Embed Size (px)
Citation preview

D I A G N O S I S A N D T R E A T M E N T
The Patient's Story: Integrating the Patient- and Physician-centered Approaches to Interviewing Robert C. Smith, MD, and Ruth B. Hoppe, MD
• Patients produce biopsychosocial stories that integrate material from the medical and personal aspects of their lives. Capturing the personal aspect of the story requires that a patient-centered approach to clinical interviewing complement the equally important physician-centered approach. Patient-centered interviewing actively involves the patient and ensures that his or her perceptions, needs, and concerns are articulated during the physician-patient interaction. In our article, we define patient-centered interviewing and provide a rationale for using it. We also describe how patient-centered interviewing is done, how it is integrated with the physician-centered approach, and how to understand the product of this complementary approach to clinical interviewing, the patient's biopsychosocial story.
Annals of Internal Medicine. 1991;115:470-477.
From Michigan State University, East Lansing, Michigan. For current author addresses, see end of text.
According to the biopsychosocial model (1, 2), every patient has a story that demonstrates the interaction among the biologic, psychologic, and social components of his or her life. Gestalt theory posits that people are continuously developing a story that portrays what is most important in their lives (3-6). The patient's story emerges in a meaningful, integrated, and complete way. The physician's task is to elicit and understand this story, for it provides an introduction to who the person is and why he or she is seeing the physician. The story also provides clues to diagnostic and therapeutic issues relevant to the patient's problem. The primary means for eliciting the story is clinical interviewing, the core skill of the clinician (7-9) and a skill that has long been central to the clinical method (10).
Unfortunately, physicians frequently do not emerge from an interview with an understanding of the complete story because current interviewing practices often eschew the human dimension in favor of a purely biologic story (11-15). To elicit the full biopsychosocial story, physicians must complement the current physician-centered practices with patient-centered interviewing (1, 2, 11-16). Our aim in this article is to briefly describe what patient-centered interviewing is and why it is important. We then describe how to perform patient-centered interviewing and how to integrate it with presently isolated physician-centered practices.
What Is a Patient-centered Approach to Interviewing?
The patient's concerns, comfort, and desire for information are the physician's foremost considerations during the patient-centered interview (16-20). The need for comfort can often be addressed easily, whereas the need for information can usually be met only after the story has been understood. A top priority in patient-centered interviewing, therefore, is eliciting and understanding the patient's concerns (symptoms, fears, and ideas, for example). Using open-ended and emotion-handling responses, the interviewer actively facilitates the patient's expression of concerns.
In the patient-centered interview, patients lead the exchange. The patient generates ideas and controls the direction of the conversation. The physician follows the patient, much as one follows a dance partner. When an interview becomes physician-centered, which it must in later parts, ideas originate in the physician's mind and the physician's questions or statements focus the patient. In an ideal interview integrating the patient-centered and physician-centered approaches, the patient leads in areas where he or she is the expert (on symptoms, concerns, preferences, and values) and then the physician leads in his or her domain of expertise (details of organic disease and estimating probabilities of disease) (10, 18, 21-24). The following examples show how both the lead and the interview content differ in each approach. Regarding a woman's complaint of "chest pain since my mother's heart seizure," a patient-centered response might be, 'Tell me more about that." The response is patient-centered because it follows the patient's lead and adds no new idea to the conversation. A physician-centered response to the same question might be, "Does it make you short of breath?" This response is physician-centered because it adds an idea of interest to the physician (shortness of breath) that the patient had not previously introduced. The physician has taken the lead away from the patient and established a new direction.
The Rationale for Patient-centered Interviewing
Patient-centered interviewing produces a more humanistic interaction because patients are heard and understood in a different way (25). Patients' responsibility, involvement in care, and self-sufficiency increase as sharing of power occurs and patient autonomy grows (10, 18, 21-26). In a patient-centered interview, physicians can fully express such humanistic attributes as respect, humility, empathy, and sensitivity (26-28). In addition, a patient-centered approach seems important for developing a sense of connectedness between patient and physician, which is a part of the spiritual or
470 © 1991 American College of Physicians
Downloaded From: http://annals.org/ by a Michigan State University Libraries User on 11/12/2013

transcendent dimension of medicine (29). A patient-centered approach is also involved with healing (27-31), placebo effects (32), patient satisfaction (33, 34), and physician satisfaction (29).
Research data support a patient-centered approach and have also revealed the limitations of isolated physician-centered interviewing. Beckman and Frankel (11) found that physicians did not allow patients to complete their opening statement of concerns in 69% of visits, interrupting patients after a mean time of 18 seconds; information was sought almost exclusively through the use of closed-ended, physician-centered questions. Once interrupted, fewer than 2% of patients went on to complete their statements. Premature termination of the patient's initial statement had the effect of making early clinical material the primary diagnostic focus. Burack and Carpenter (35) found that this approach prevented physicians from learning about all but 6% of primary problems that were ultimately determined to be psychosocial. Frankel (12) found that 94% of physician interruptions resulted in the physician's taking charge of the conversation. This finding is consistent with results from a study by Piatt and McMath (13), who found that an incomplete database was occasioned by the omission of patient-centered information and a "high control" style. Data are thus very much physician-determined, skewed toward problems that are biomedical in nature and directed away from the psychosocial or personal domain. Because of this imbalance, it has been proposed that current interviewing practices are at odds with scientific requirements: They produce biased, incomplete data about the patient (11-13, 35, 36).
Careful and extensive descriptive work first suggested that a patient-centered approach had superior qualities; generally, it was found that more complete patient information led to more humane care (25, 37-39). This work fostered the distinction of illness from disease and of caring from curing and established the centrality of communication and language in medicine. These approaches also showed the need for integrating the biomedical and psychosocial (personal) aspects of medicine. Although the inherent richness of this information speaks for itself (40), many systematic studies further support the superiority of patient-centered interviewing.
From a diagnostic perspective, patient-centered interviewing produces more psychosocial data and emotional responses through its use of open-ended inquiry and emotion-handling responses (for example, sympathy) (41-43). Investigators have also shown that a few closed-ended questions might enhance the quantity and quality of personal data, but a controlling style greatly reduced it. Perhaps surprising in these studies was that open-ended inquiry elicited much data ordinarily obtained by systematic, closed-ended questioning and that it also generated some biomedical data that did not arise during systematic questioning (6). No studies have yet compared patient-centered and physician-centered techniques with regard to consistency of data.
Research regularly shows that patient-centered interviewing is associated with increased patient satisfaction when compared with physician-centered interviewing (33, 34, 44-50). However, many studies have been plagued by methodologic diversity, multiple variables,
inconstant coding schemata, and the absence of hypothesis testing (34). In a meta-analysis of 41 studies, Hall and colleagues (34) extracted all results, whether statistically significant or not, and consolidated many definitions into a few comprehensive categories. Satisfaction was still highly correlated with a patient-centered approach. Roter and colleagues (33) also showed a statistically significant association between satisfaction and patient-centered interactions when testing a specific hypothesis and when using systematic rating procedures; both simulated patients and trained judges were used as raters. A teaching intervention did not produce a change in the satisfaction of patients who received care from residents; satisfaction ratings were too high initially to detect a change (51). An important by-product is that satisfaction is related to diminution of malpractice suits (52) and "doctor-shopping" (53). By personally interviewing a sample of upper- and lower-income patients who had changed doctors, Kasteler and colleagues (53) found that, in part, dissatisfaction and change were related to inattention to socioemotional factors.
Although it is not as strong, a distinct association between patient-centered interviewing and compliance has also been shown (20, 34, 44, 45, 50, 54). Furthermore, patient knowledge and recall are greater with patient-centered communication (33, 34, 44, 55, 56). Because recall and satisfaction are closely linked with compliance (54, 57, 58) and, in turn, compliance is closely linked with health status outcomes (54, 56-58), patient-centered interviewing is likely to be important in both treatment and health promotion. For instance, a patient-centered approach should allow physicians to better understand and involve patients in choosing acceptable treatments (for example, an antihypertensive agent not associated with impotence); discussing prognosis (for example, the adverse effect of the family myth that all men die before 60 years of age); and accepting preventive strategies (for example, beginning a tobacco cessation program when many of one's coworkers smoke). Studies have also shown that patients have better blood pressure and diabetic control when they participate more and take more control in their care (59); improved perinatal outcome when they are provided with continuity of care and an "attitudinal contract" (60); and shortened, less complicated postoperative courses when they receive support and instruction (61). Nevertheless, a health status benefit from patient-centered interviewing itself has not yet been conclusively shown (20, 51).
Performing the Patient-centered Interview and Integrating It with the Physician-centered Interview
Patient-centered Interviewing: Nondirective Dimension
Several excellent resources provide more detailed information on patient-centered interviewing (24, 28, 37, 62-65), and an annotated transcript of an integrated interview is available on request from the authors.
The interviewer sets the stage for a successful interview by showing the following courtesies at the outset (66): knowing and using the patient's name, introducing
15 September 1991 • Annals of Internal Medicine • Volume 115 • Number 6 471
Downloaded From: http://annals.org/ by a Michigan State University Libraries User on 11/12/2013

Table 1. Specific Open-Ended Interviewing Responses*
Silence Nonverbal responses (hand gesture or facial expression to
encourage talking) Neutral utterances or continuers ("Uh-huh."; "Mmm . . ." ;
"Yes.") Reflection or echoing ("The pain is in my [the patient's]
back."; Interviewer's response: "Your back." Open-ended questions or requests ("Tell me more."; "Go
on.") Short summaries or paraphrasing ("So you had many tests
over the weekend but still don't know anything?")
* See References 24, 28, 37, 62-65.
oneself, and welcoming the patient; putting the patient at ease, often with seemingly aimless talk (for example, about the weather), and ensuring privacy and comfort (37); attempting to correct barriers to communication (for example, moving to a quieter area); establishing the patient's understanding of the situation; and clarifying the time available, negotiating plans for its use, and setting an agenda (23, 67, 68).
The interviewer starts with an open-ended question or statement such as "How are things?" or "You're new here." This does not dictate the patient's response and allows the patient to begin wherever he or she likes. The major initial goal is to encourage a free flow of information (69). The interviewer also observes nonverbal data such as gestures, facial expression, and style of dress, as well as clinical manifestations such as dyspnea or weakness.
As long as the patient begins talking, the interviewer says little for the first 30 seconds or so (6, 37) and is content with any type of information, whether personal or medical. The specific open-ended responses of silence, nonverbal facilitations, and neutral utterances are used to facilitate the free flow of information from and about the patient (Table 1). This period helps establish that the interviewer is interested and will listen.
Occasionally, patients present so many problems that their exploration would exceed the time available. If the interviewer has not already done so, he or she negotiates an agenda for the encounter, deferring less pressing problems to a subsequent visit (23, 67, 68). This allows the patient to develop what is most important and the interviewer to meet her or his needs in a timely fashion as well. On the other hand, the patient may say little and may ask what to do rather than produce a free flow of information. The interviewer remains open-ended, using such responses as "Start wherever you like." If the patient keeps asking for direction, the interviewer provides guidance and focus (42); for example, the interviewer might say "You're here in the hospital [clinic] ." After this initial period, or sooner if the patient does not begin to speak spontaneously (42), the interviewer becomes more active by using the additional open-ended responses noted in Table 1 (reflection, requests, and summaries).
Two cautionary notes should be interjected regarding this early stage: First, the interviewer follows initial open-ended statements with additional open-ended responses and must not be deterred by a seeming lack of responsiveness or a belief that the patient is not ame
nable to this approach. Second, the interviewer avoids behaviors that can prematurely interrupt the free flow of data: exploring physician-centered hypotheses, interrupting inappropriately, or changing the topic of conversation (nontracking). If interrupting is necessary because of a failure to understand, it is explained with a statement such as, "Excuse me, I didn't quite follow that." Closed-ended questioning can be used for purposes of clarification after the patient has established the focus (for example, "When did all this occur?"). Care must be taken, however, to return the lead to the patient and not prematurely focus on the physician's agenda.
Sometimes, open-ended questions are not appropriate. An immature person, an adolescent, a demented patient, a severely distressed patient, or a severely ill patient is often made uncomfortable by open-ended questions. In such instances, it is better to directly address the need for clarity and structure (70).
During the initial phase of the interview (usually about 1 minute), the interviewer's facilitating, open-ended responses are used wherever the patient seems to have the most interest. This is the "nondirective" dimension because the interviewer is not guiding the content or course of the interview. Rather, he or she is establishing a relationship and a flow of information as well as generating hypotheses.
Patient-centered Interviewing: Directive Dimension
The interviewer becomes more active and channels the flow of data in specific directions by selective emphasis on the conversation of most concern to the patient, typically the personal dimension. Therefore, the directive phase often tests hypotheses about the personal meaning of the patient's story. Open-ended statements (Table 1) are still used, but the physician now exerts more influence by deciding what aspects of the story require a response.
In the usual instance, the interviewer avoids focusing on the diagnosis of possible organic disease or specific laboratory data related to organic disease. Such topics are elaborated in the later physician-centered aspect of the interview. Nevertheless, data relevant to diagnoses of organic disease are commonly verbalized during the patient-centered part of the interview. Rather than asking about details of physical symptoms or laboratory data, physicians learn what patients were doing when the symptoms occurred, what else was going on in their lives, and who else was involved. Thus, information about the patient's life setting and physical symptoms is often developed simultaneously.
There are exceptions to the generalization that the interviewer should avoid eliciting medical information at this stage. Occasionally, he or she learns through initial open-ended inquiry that a patient wants to discuss only physical symptoms, and this is appropriate from a patient-centered perspective; typically, these patients return to personal data later. On other occasions, usually in cases of severe or acute organic disease, patients will be able to focus only on physical symptoms (for example, the patient with terminal cancer who has severe pain and nausea). At still other times, the physician
472 15 September 1991 • Annals of Internal Medicine • Volume 115 • Number 6
Downloaded From: http://annals.org/ by a Michigan State University Libraries User on 11/12/2013

may recognize physical symptoms that indicate a life-threatening condition (crushing substernal pain radiating to the arm). Because the symptom is of the utmost importance to the patient, the immediate follow-up of this lead is appropriate from a patient-centered perspective, even though the patient may present other issues. Therefore, in focusing the encounter, the physician is guided by both his or her own clinical acumen and the patient's concerns (23).
Clues to the Personal Story Identifying the clues to the patient's personal story is
the interviewer's next task in the directive dimension (37). Some patients, however, are reluctant initially to express personal, psychological material (35, 71), particularly when they have been conditioned to give only information on organic disease. Nevertheless, the first step in recognizing personal material is knowing that such material is almost always communicated and that it can be expressed as either a statement or an emotion.
Personal statements do not directly refer to physical symptoms or to other information about organic disease, but they usually emerge in conjunction with and reflect the context of such data. The personal statements are italicized in the following examples. Suggested open-ended responses for beginning the development of the underlying personal story are given subsequently; open-ended questions that would encourage a focus on the patient's biomedical story are shown for contrast.
Example 1: "the day after my husband lost his job, my ankles got swollen and my fever went to
Suggested responses are "Lost his job?" (personal) and "Ankles were swollen?" (biomedical).
Example 2: the large lymph nodes and hoarseness were only the beginning; then was the angina and
Suggested responses are "Only the beginning?" (personal) and "Lymph nodes?" (biomedical).
Personal statements unrelated to medical events occur much less frequently in a medical setting unless the patient has previously experienced a physician's interest in the personal domain. These references are similar to what one hears from nonpatients and can be about any life circumstance, as in the following example. Patient: "My wife died 4 months ago." Physician: "Your wife died" or "How have things been?"
Certain responses are probably more important clues than others. We propose the following hierarchy of increasingly important personal responses (72): 1) statements unrelated to the present, to the interviewer, or to emotions ("In 1983 my friend came . . . " ) ; 2) statements about the interviewer ("You're younger than I expected") or to present circumstances ("It's hot in here"); 3) statements about emotions, feelings, or affect ("She made me angry"); 4) nonverbal expression of emotion (depressed facies, sighing, helplessness gesture) (73); and 5) the actual expression of emotion (crying, joy). The open-ended skills described in Table 1 are Used for develooine the first three tvnes of ner^nnal
statement into a story. Pursuing the development of verbal or nonverbal emotional expression (the last three types of personal responses given above) to the underlying story also requires facility with the basically similar emotion-handling skills described below.
Emotional expression is perhaps the most vital clue to the personal database (72). In addition, by addressing affect, the interviewer can also make the patient feel better and greatly enhance rapport. It is important to anticipate affect even when it is not verbally expressed. Nonverbal expression can occur in many ways: For example, glistening of the eyes may signify sadness or joy, and abruptness or impatience may signify anger. After understanding the nonverbal message (for example, a sigh indicating discouragement), the interviewer can develop the message further by directly feeding it back to the patient ("You're sighing, you seem discouraged.") or by making an open-ended inquiry about affect ("How was that for you?"). Such responses are similar to open-ended feedback addressing patients' verbal material and are not biasing.
When a particularly difficult situation is described without affect, the interviewer also inquires about emotional responses (for example, "How does that make you feel?"). After hearing a long litany of physical symptoms, hospitalizations, and laboratory data, the interviewer might respond, "That 's a lot to happen in just 5 weeks. How's that affected you personally?" Inquiring about the underlying emotion in situations where patients focus entirely on physical symptoms and laboratory data is a good way to open discussion of the personal dimension.
In responding to verbally or nonverbally expressed affect, the first step is to become aware of one's own emotional reaction and not to be alarmed or frightened. Patients can be allowed to express their emotions, and physicians must guard against the impulse to shut them off or change the subject. Interviewers often fear losing control of the interview when feelings are expressed, especially through crying, but feelings are not harmful and, when addressed in an open-ended way, patients will control how far they go in discussing them.
Managing verbally or nonverbally expressed emotions involves the emotion-handling (relationship-building) skills presented in Table 2 (66-68, 74, 75). Rehearsing these can be helpful to prepare for tense moments in the interview. The mnemonic NURS (naming, understanding, respecting, supporting) aids in their recall.
Hypothesis Testing: Developing the Personal Story Hypothesis testing as it relates to the personal story
is accomplished in the directive dimension by selectively focusing on the highest-ranking personal clues
Table 2. Emotion-handling Skills*
Naming or labeling the emotion ('That seems sad for you.") Understandability or legitimation ("I can imagine that must
have been quite upsetting.") Respect ("You've really dealt remarkably well with this.") Support or partnership ("Together, I think we can get on top
of this.")
* See References 66-68, 74, 75.
15 September 1991 • Annals of Internal Medicine • Volume 115 • Number 6 473
Downloaded From: http://annals.org/ by a Michigan State University Libraries User on 11/12/2013

with an open-ended comment or an emotion-handling response. Such responses usually prompt the patient to provide additional personal data. The interviewer then responds, in a similar open-ended way, for clarification and further elaboration. More personal material follows, yielding new and more accurate hypotheses. This process eventually reveals the patient's personal story or "hidden agenda" (76). One does not have to be a psychiatrist to conduct such exploration. "Following your nose" is all that is required to understand most stories (69). If the interviewer allows it, the patient will do the work. It has been suggested by Lipkin (66) that the interviewer should function like a conductor, "orchestrating" the interview using the skills that have been described. Furthermore, there is not a right or wrong personal issue to pursue. There is usually only one personal story at a given moment; the higher-ranking hierarchical clues simply take the interviewer more quickly to it (28).
When patients redirect conversation away from the personal dimension and begin to give data related to organic disease, the interviewer should try to refocus the patient on the already-developed personal reference or emotion, as in the following example: "Before going into your hospitalizations, tell me more about what that was like for you to be scared." If the patient resists redirection, the interviewer should respect the patient's wishes and understand that the avoidance of further personal material may be important information in its own right.
The story is completed when a sense of understanding develops (37, 77-79) and when later occurring data reinforce this impression. The physician must check with the patient to verify his or her understanding (67, 68). When such corroboration is received, then the patient-centered part of the interview can be completed. Nevertheless, related stories or sequels often occur. The amount of time available determines whether the interviewer addresses them. The benefits of the patient-centered part of the interview, however, accrue just from hearing what may be only the first chapter of a longer story.
Transition Because the patient has been accustomed to express
ing needs and personal concerns, the interviewer indicates that a change in style is about to occur ("I appreciate your sharing these things; we're going to have to shift gears now and I'll ask you some different types of questions about your symptoms.") (25, 28). Otherwise, the abrupt change to the physician-centered part of the interview could confuse and upset the patient.
Physician-centered Interviewing: Nondirective and Directive Dimensions
The interviewer proceeds to the equally important (6, 41, 42) physician-centered part of the interview to further evaluate earlier hypotheses and develop new ones. Although hypotheses may be about partially stated personal issues or about psychiatric diagnoses, most concern possible organic disease. Although the interviewer initiates inquiry by nondirective, open-ended medical
questions ("Now, what about the pain you mentioned earlier?"), much time is devoted to directive, progressively more closed-ended responses ("When did the pain begin?", "Does it go anywhere?"). Using this style of inquiry to refine the information on each symptom, the interviewer focuses on the pertinent specifics of the patient's possible organic disease problem.
Closed-ended interviewing can introduce considerable bias into the patient's medical story. Bias is minimized by proceeding from the general to the specific; using single questions; not suggesting a response by wording of a question, tone, or nonverbal communication; giving equal weight to alternative answers; not interpreting data while gathering it; giving balanced attention to all aspects of the story; not confusing the patient with technical language or rapid shifts; and making the conversation congruent with the patient's education, language, cultural, social, and stylistic capabilities (24, 28, 62, 64, 65, 70).
Physician-centered interviewing is required for the definitive categorization of most organic diseases and for decisions about disease probability and diagnostic procedures (6, 41, 42). Although it is usual to obtain information related to organic disease during patient-centered interviewing, the data are seldom complete enough to be diagnostic.
When serious personal or psychiatric problems are suspected on the basis of earlier patient-centered interviewing, more specific data are obtained during physician-centered interviewing (25). More directed, closed-ended questions are used for refining hypotheses developed earlier ("How long did you feel blue and down?") and for eliciting therapeutic information ("What was the dose of doxepin?") and other information ("When was the divorce?").
If additional personal needs or emotions are expressed by the patient during physician-centered interviewing, the physician must revert to the use of patient-centered techniques (16) (for example, a discussion of a past illness triggers an unanticipated emotional response in the patient). Generally, however, this situation does not arise because the most pressing needs have been addressed during the initial patient-centered interview (80).
After completing the physician-centered part of the interview it is important, before proceeding to the physical examination, to return the encounter to a patient-centered atmosphere. To achieve this, the interviewer should forewarn the patient that the interview will end shortly; briefly summarize what he or she has understood; inquire whether the patient has anything additional to discuss; and determine how the interaction has gone.
Understanding, Categorizing, and Using the Patient's Story
Although each patient is unique, awareness of common personal themes among medical patients prepares interviewers for issues they are likely to encounter. Common themes include fear of death, mutilation, or disability; dislike, distrust, or disbelief of the medical system or physician; concern about loss of function,
474 15 September 1991 • Annals of Internal Medicine • Volume 115 • Number 6
Downloaded From: http://annals.org/ by a Michigan State University Libraries User on 11/12/2013

"wholeness," role, status, and independence; denial of reality-based medical problems; separation, grief, and losses; leaving home and becoming independent; discomfort with retirement; and uniquely personal issues.
The meaning of the illness to the patient and her or his beliefs and explanations about the illness are also important features of the story (39, 81-84). In addition, the interviewer will often have learned other essential components of the story: the patient's goals and expectations and other information specifically requested of the physician (84, 85). When either type of information does not arise during patient-centered interviewing, it is identified during the physician-centered part of the interview. These data ensure that the patient will be adequately understood during negotiations about future medical care (23, 70, 84, 85).
Although the personal and organic-disease dimensions are sufficient to categorize the biopsychosocial story, we teach learners to look for two additional psychosocial features: a psychiatric diagnosis (if relevant) and characteristics of the patient's personality style. Both, however, require additional expertise, the discussion of which falls outside the purview of this article. However, with some review (66, 86-88), most interviewers can effectively address these issues.
We then ask interviewers to systematically categorize the dimensions of the biopsychosocial story according to the mnemonic POPP: personal dimension, organic-disease dimension, psychiatric diagnosis (if any), and personality features. Such categorization provides an integrated biopsychosocial summary of the patient. The formulation of the mnemonic POPP has been useful to ensure that all dimensions of the story are obtained. Learners are taught to summarize their interaction with patients using the mnemonic, to record the POPP dimensions in patients' medical records, and to appreciate that the biopsychosocial story is very different from the routine personal and social history because it highlights what is most important to the patient at any given time. Two patients' stories or POPP designations are given in Table 3. The more multidimensional classification system used in the Diagnostic and Statistical Manual of Mental Disorders can also be used (86).
The integrated interviewing process reviewed in this article is the first and primary tool for developing the biopsychosocial story (7-9). The story is updated after physical examination, acquisition of laboratory data, observation of the patient's clinical course, and more interviewing. Additional interpersonal communication skills (the ability to educate, inform, and motivate the patient) are needed during the treatment phase, so that patients can participate fully in their care (67, 68, 74, 75).
The integrated approach incorporating both patient-and physician-centered interviewing is applicable in all settings, from the encounter with a new patient to the return visit and from ward rounds to the outpatient clinic or emergency room. The only difference concerns the total amount of time available. As a rule of thumb, the interviewer can obtain pertinent patient-centered data in approximately 5% to 20% of the time available. The magnitude of the patient's immediate personal concerns is the major determinant of the time required.
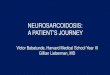
Table 3. Two Biopsychosocial Stories from Integrated Patient- and Physician-centered Interviewing*
1. (P) The recent death of spouse has left a 73-year-old patient sad, having to move in with a daughter he dislikes and believing that his plight is due to sexual transgressions committed many years before. (O) He complains of paralysis of the left side since a stroke several years ago, the development of decubiti since the death of his caretaker wife, and recent worsening of typical angina pectoris. (P) He shows appropriate expression of affect in a usually sad situation. There is no psychiatric disease. (P) He has a slightly controlling (obsessive) personality style, which is within the normal range.
2. (P) A recent unwanted divorce, finalized 4 days ago, has left a 27-year-old patient unable to support herself and her two children; her mother will not let her move back home again. She believes it is "normal" for men to keep deserting her, citing three similar previous experiences. (O) She has intermittent chest pain of 4 days duration that sounds musculoskeletal in origin. (P) She is sad and has felt depressed for several weeks. A diagnosis of major depression is made. (P) She also has a dependent personality (trait).
* Each story is categorized according to the POPP profile: (P) personal content, (O) organic-disease data, (P) psychiatric diagnosis (if any), and (P) personality. Note the interaction among the component parts of each story, how the personal and medical domains often are interdependent.
We have developed our approach in conjunction with teaching medical students and residents for many years. It reflects considerable input from them, is well accepted by them, and has been a useful teaching method. We propose that obtaining the patient's relevant biopsychosocial story is the objective of every encounter and that facility with the patient-centered approach will enable interviewers to achieve this. By integrating the patient's needs with those of the physician, medicine will have taken a significant step on the path toward becoming more humanistic and more scientific.
Acknowledgments: The authors thank Arnold Werner, Howard Brody, Howard Beckman, William Clark, Mack Lipkin, Jr., Valerie Shebroe, and Alicia Wilson for helpful comments on the manuscript; Timothy Quill for his extensive review and many useful suggestions; both The Task Force on Doctor and Patient (Society of General Internal Medicine) and the University of Rochester's programs in biopsychosocial medicine for their strong influence; the Fetzer Institute of Kalamazoo, Michigan, for their generous support; the many residents and students for their active participation and many helpful suggestions; and Theresa Ryan for her valuable help in manuscript preparation.
Requests for Reprints: Robert C. Smith, MD, B220 Life Sciences Building, Michigan State University, East Lansing, MI, 48824.
Current Author Addresses: Drs. Smith and Hoppe: B220 Life Sciences Building, Michigan State University, East Lansing, MI, 48824.
References 1. Engel GL. The clinical application of the biopsychosocial model.
Am J Psychiatry. 1980;137:535-44. 2. Engel GL. The need for a new medical model: a challenge for
biomedicine. Science. 1977;196:129-36. 3. Koffka K. Principles of Gestalt Psychology. New York: Harcourt,
Brace and World Inc.; 1935. 4. Kohler W. Gestalt Psychology: An Introduction To New Concepts
in Modern Psychology. New York: Liveright; 1947. 5. Lewin K. Field Theory in Social Science: Selected Theoretical Pa
pers. Cartwright D, ed. New York: Harper and Row; 1951. 6. Cox A, Rutter M, Holbrook D. Psychiatric interviewing techniques
V. Experimental study: eliciting factual information. Br J Psychiatry. 1981;139:29-37.
7. Weston WW, Lipkin M. Doctors learning communication skills: developmental issues. In: Stewart M, Roter D, eds. Communicating With Medical Patients. London: Sage Publications; 1989:43-57.
15 September 1991 • Annals of Internal Medicine • Volume 115 • Number 6 475
Downloaded From: http://annals.org/ by a Michigan State University Libraries User on 11/12/2013

8. Lipkin M Jr . The medical interview as core clinical skill: the problem and the opportunity. J Gen Intern Med. 1987;2:363-5.
9. Lipkin M, Quill TE, Napodano RJ. The medical interview: a core curriculum for residencies in internal medicine. Ann Intern Med. 1984;100:277-84.
10. Stoeckle JD, Billings JA. A history of history-taking: the medical interview. J Gen Intern Med. 1987;2:119-27.
11. Beckman HB, Frankel RM. The effect of physician behavior on the collection of data. Ann Intern Med. 1984;101:692-6.
12. Frankel RM. From sentence to sequence: understanding the medical encounter through microinteractional analysis. Discourse Process. 1984;7:135-70.
13. Piatt FW, McMath JC. Clinical hypocompetence: the interview. Ann Intern Med. 1979;91:898-902.
14. Duffy DL, Hamerman D, Cohen MA. Communication skills of house officers: a study in a medical clinic. Ann Intern Med. 1980;93:354-7.
15. Waitzkin H. Doctor-patient communication. Clinical implications of social scientific research. JAMA. 1984;252:2441-6.
16. Levenstein JH, McCracken EC, McWhinney IR, Stewart MA, Brown JB. The patient-centered clinical method. 1. A model for the doctor-patient interaction in family medicine. Fam Pract. 1986;3:24-30.
17. McWhinney I. The need for a transformed clinical method. In: Stewart M, Roter D, eds. Communicating with Medical Patients. London: Sage Publications; 1989:25-42.
18. Levenstein JH, Brown JB, Weston WW, Stewart M, McCracken EC, McWhinney I. Patient centered clinical interviewing. In: Stewart M, Roter D, eds. Communicating with Medical Patients. London: Sage Publications; 1989:107-20.
19. McWhinney IR. An Introduction To Family Medicine. New York: Oxford University Press; 1981.
20. Stewart MA. What is a successful doctor-patient interview? A study of interactions and outcomes. Soc Sci Med. 1984;2:167-75.
21. Tate P. Doctors' style. In: Pendleton D, Hasler J, eds. Doctor-Patient Communication. Orlando, Florida: Academic Press; 1983: 75-85.
22. Freeling P. The doctor-patient relationship in diagnosis and treatment. In: Pendleton D, Hasler J, eds. Doctor-Patient Communication. Orlando, Florida: Academic Press; 1983; 161-75.
23. Quill TE. Partnerships in patient care: a contractual approach. Ann Intern Med. 1983;98:228-34.
24. Morgan WL, Engel GL. The Clinical Approach To The Patient. Philadelphia: W.B. Saunders Company; 1969.
25. Mishler EG. The Discourse of Medicine. Norwood, New Jersey: Ablex Publishing Corporation; 1984.
26. Rogers CR. Client-Centered Therapy. Boston, Massachusetts: Houghton Mifflin Company; 1951.
27. Lipp MR. Respectful Treatment—The Human Side of Medical Care. New York: Harper and Row; 1977.
28. Reiser DE, Schroder AK. Patient Interviewing—The Human Dimension. Baltimore, Maryland: Williams & Wilkins; 1980.
29. Suchman AL, Matthews DA. What makes the patient-doctor relationship therapeutic? Exploring the connexional dimension of medical care. Ann Intern Med. 1988;108:125-30.
30. Greene WA, Conron G, Schalch DS, Schreiner BF. Psychologic correlates of growth hormone and adrenal secretory responses of patients undergoing cardiac catheterization. Psychosom Med. 1970; 32:599-614.
31. Singer MT. Presidential address. Engagement-involvement: a central phenomenon in psychophysiological research. Psychosom Med. 1974;36:1-17.
32. Brody H. The lie that heals: the ethics of giving placebos. Ann Intern Med. 1982;97:112-8.
33. Roter DL, Hall JA, Katz NR. Relations between physicians' behaviors and analogue patients' satisfaction, recall, and impressions. Med Care. 1987;25:437-51.
34. Hall JA, Roter DL, Katz NR. Meta-analysis of correlates of provider behavior in medical encounters. Med Care. 1988;26:657-75.
35. Burack RC, Carpenter RR. The predictive value of the presenting complaint. J Fam Pract. 1983;16:749-54.
36. Engel GL. Physician-scientists and scientific physicians. Am J Med. 1987;82:107-11.
37. Cassel EJ. Talking with Patients. Cambridge, Massachusetts: The MIT Press; 1985.
38. Kleinman A. Explanatory models in health-care relationships: a concep.ual frame for research on family-based health-care activities in relation to folk and professional forms of clinical care. In: Stoeckle JD, ed. Encounters Between Patients and Doctors. Cambridge, Massachusetts: The MIT Press; 1987:273-83.
39. Kleinman A, Eisenberg L, Good B. Culture, illness and care: clinical lessons from anthropologic and cross-culture research. Ann Intern Med. 1978;88:251-8.
40. Roter DL, Hall JA, Katz NR. Patient-physician communication: a descriptive summary of the literature. Patient Education and Counseling. 1988;12:99-119.
41. Cox A, Holbrook D, Rutter M. Psychiatric interviewing techniques
VI. Experimental study: eliciting feelings. Br J Psychiatry. 1981; 139:144-52.
42. Hopkinson K, Cox A, Rutter M. Psychiatric interviewing techniques III. Naturalistic study: eliciting feelings. Br J Psychiatry. 1981; 138: 406-15.
43. Cox A, Rutter M, Holbrook D. Psychiatric interviewing techniques. A second experimental study: eliciting feelings. Br J Psychiatry. 1988;152:64-72.
44. Roter D. Which facets of communication have strong effects on outcome—a meta-analysis. In: Stewart M, Roter D, eds. Communicating With Medical Patients. London:Sage Publications; 1989: 183-96.
45. Freemon B, Negrete VF, Davis M, Korsch BM. Gaps in doctor-patient communication: doctor-patient interaction analysis. Pediatr Res. 1971;5:298-311.
46. Korsch BM, Gozzi EK, Francis V. Gaps in doctor-patient communication. I. Doctor-patient interaction and patient satisfaction. Pediatrics. 1968;42:855-71.
47. Francis V, Korsch BM, Morris MF. Gaps in doctor-patient communication: patients' response to medical advice. In: Stoeckle JD, ed. Encounters Between Patients and Doctors. Cambridge, Massachusetts: The MIT Press; 1987:259-72.
48. DiMatteo MR, Hays R. The significance of patients' perceptions of physician conduct: a study of patient satisfaction in a family practice center. J Community Health. 1980;6:18-34.
49. Putnam SM, Stiles WB, Casey-Jacob M, James SA. Patient exposition and physician explanation in initial medical interviews and outcomes of clinic visits. Med Care. 1985;23:74-83.
50. Carter WB, Inui TS, Kukull WA, Haigh VH. Outcome-based doctor-patient interaction analysis. II. Identifying effective provider and patient behavior. Med Care. 1982;20:550-66.
51. Putnam SM, Stiles WB, Casey-Jacob M, James SA. Teaching the medical interview. J Gen Intern Med. 1988;3:38-47.
52. Vacarinno JM. Malpractice—the problem in perspective. JAMA. 1977;238:861-3.
53. Kasteler J, Kane RL, Olsen DM, Thetford C. Issues underlying prevalence of "doctor-shopping" behavior. J Health Soc Behav. 1976;17:328-39.
54. Eraker SA, Kirscht JP, Becker MH. Understanding and improving patient compliance. Ann Intern Med. 1984;100:258-68.
55. Bartlett EE, Grayson M, Barker R, Levine DM, Golden A, Libber S. The effects of physician communications skills on patient satisfaction; recall, and adherence. J Chronic Dis. 1984;37:755-764.
56. Ley P, Whitworth MA, Skilbeck CE. Improving doctor-patient communication in general practice. J R Coll Gen Pract. 1976;26:720-4.
57. Gillum RF, Barsky AJ. Diagnosis and management of patient noncompliance. JAMA. 1974;228:1563-7.
58. Haynes RB, Mattson ME, Chobanian AV, et al. Management of patient compliance in treatment of hypertension—report of the NHLBI Working Group. Hypertension. 1982;4:415-23.
59. Kaplan SH, Greenfield S, Ware JE. Impact of the doctor-patient relationship on the outcomes of chronic disease. In: Stewart M, Roter D, eds. Communicating With Medical Patients. London:Sage Publications; 1989:228-45.
60. Shear CL, Gipe BT, Mattheis JK, Levy MR. Provider continuity and quality of medical care—a retrospective analysis of prenatal and perinatal outcome. Med Care. 1983;21:1204-10.
61. Egbert LD, Battit GE, Welch CE, Bartlett MK. Reduction of postoperative pain by encouragement and instruction of patients—a study of doctor-patient rapport. N Engl J Med. 1964;270:825-7.
62. Billings JA, Stoeckle JD. The Clinical Encounter—A Guide To The Medical Interview and Case Presentation. Chicago: Year Book Medical Publishers; 1989.
63. Lipkin M, Putnam SM, Lazare A, eds. The Medical Interview—A Textbook on Medical Interviewing. New York: Springer-Verlag; 1990 [In press].
64. Enelow AJ, Swisher SN. Interviewing and Patient Care. New York: Oxford University Press; 1986.
65. Coulehan JL, Block MR. The Medical Interview: A Primer For Students of The Art. Philadelphia: F.A. Davis Co.; 1987.
66. Lipkin M. The medical interview and related skills. In: Branch WT, ed. Office Practice of Medicine. Philadelphia: W.B. Saunders; 1987: 1287-306.
67. Cohen-Cole SA. The Medical Interview: The Three Function Approach. St. Louis, Missouri: Mosby-Year Book, Inc.; 1991.
68. Bird J, Cohen-Cole SA. The three-function model of the medical interview: an educational device. In: Hale M, ed. Models of Teaching Consultation-Liaison Psychiatry. Basel: Karger; 1991:65-88.
69. Oxman TE, Rosenberg SD, Schnurr PP, Tucker GJ. Diagnostic classification through content analysis of patients' speech. Am J Psychiatry. 1988;145:464-8.
70. Quill TE. Recognizing and adjusting to barriers in doctor patient communication. Ann Intern Med. 1989;111:51-7.
71. Katon W, Kleinman A, Rosen G. Depression and somatization: a review (part 1). Am J Med. 1983;72:127-35.
72. Cohen-Cole SA, Bird J. Interviewing the cardiac patient: II. A
4 7 6 15 Sep tember 1991 • Annals of Internal Medicine • Volume 115 • N u m b e r 6
Downloaded From: http://annals.org/ by a Michigan State University Libraries User on 11/12/2013

practical guide for helping patients cope with their emotions. Quality of Life and Cardiovascular Care. 1986;3:53-65.
73. Engel GL. The care of the patient: art of science? Johns Hopkins Med J. 1977;140:222-32.
74. Bird J, Cohen-Cole SA, Boker J, Freeman A. Teaching psychiatry to nonpsychiatrists: I. The application of educational methodology. Gen Hosp Psych. 1983;5:247-53.
75. Lazare A. Three functions of the medical interview. In: Lipkin M, Putnam S, Lazare A, eds. The Medical Interview—A Textbook on Medical Interviewing. New York: Springer-Verlag; 1990 [In press].
76. Barsky AJ. Hidden reasons why some patients visit doctors. Ann Intern Med. 1981;94:492-8.
77. Slavney PR, McHugh PR. Life stories and meaningful connections: reflections on a clinical method in psychiatry and medicine. Per-spect Biol Med. 1984;27:279-88.
78. Schwartz MA, Wiggins O. Science, humanism, and the nature of medical practice: a phenomenological view. Perspect Biol Med. 1985;28:331-61.
79. Wallace ER 4th. What is "truth?' ' Some philosophical contributions to psychiatric issues. Am J Psychiatry. 1988;145:137-47.
80. Frankel R, Beckman H. Evaluating the patient's primary problem(s). In: Stewart M, Roter D, eds. Communicating With Medical Patients. London: Sage Publications; 1989:86-98.
81. King J. Health beliefs in the consultation. In: Pendleton D, Hasler J, eds. Doctor-Patient Communication. Orlando, Florida: Academic Press; 1983:110-25.
82. Snow LF. Traditional health beliefs and practices among lower class black Americans. West J Med. 1983;139:820-8.
83. Jaspars J, King J, Pendleton D. The consultation: a social psychological analysis. In: Pendleton D, Hasler J, eds. Doctor-Patient Communication. Orlando, Florida: Academic Press; 1983:139-57.
84. Lazare A, Eisenthal S, Frank A, Stoeckle JD. Studies on a negotiated approach to patienthood. In: Stoeckle JD, ed. Encounters Between Patients and Doctors. Cambridge: The MIT Press; 1987: 413-32.
85. Lazare A, Eisenthal S, Wasserman L. The customer approach to patienthood: attending to patient requests in a walk-in clinic. Arch Gen Psychiatry. 1975;32:552-8.
86. American Psychiatric Association. Diagnostic Manual of Mental Disorders. Third edition. Washington, DC: American Psychiatric Association 1986.
87. Kahana RJ, Bibring GL. Personality types in medical management. In: Zaiberg NE, ed. Psychiatry and Medical Practice In A General Hospital. New York: International University Press; 1964:108-23.
88. Shapiro D. Neurotic Styles. New York: Basic Books, Inc.; 1965.
15 September 1991 • Annals of Internal Medicine • Volume 115 • Number 6 477
Downloaded From: http://annals.org/ by a Michigan State University Libraries User on 11/12/2013