Embed Size (px)
DESCRIPTION
Presented at Optimizing Medications workshop in Vancouver by Johanna Trimble
Citation preview

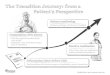
Community • Professional Academic
Detailing in GP offices Medication knowledge • Polypharmacy Medication review
Hospital • MedRec Best possible medication history • 48/6 Assess 6 areas w/i 48 hr • Polypharmacy Medication review
Residential Care
• MedRec Best possible medication history • CLeAR Appropriate antipsychotic use • Polypharmacy Medication review
Transition in Care
Patient

Optimizing Medications: Time to bring the pieces together
January 16-17, 2014 (BCPSQC)
Is Your Mom on Drugs? Johanna Trimble
Polypharmacy Initiative (Shared Care): Steering Committee Call for Less Anti-Psychotics in Residential Care: CLeAR Faculty
Fraser Health Authority, Polypharmacy Initative

Let’s work together to change how we care for elders
• Realize the impact of multiple medications on frequent hospitalizations, loss of function & inability to live independently
• Schedule medication reviews that help lessen the burden of multiple medications and improve quality of life
• Involve the family as part of your team – ask them for input and act on their concerns

Who was Fervid Trimble?

Teacher (MEd, U. of Idaho) Wife, mother, grandmother, family matriarch

Fervid Trimble, age 86 years, enjoying her apartment in a senior’s residence she’d carefully chosen for herself.

Fervid’s “family care team” Johanna, Dale, Fervid and Kathie

Fervid experienced a precipitous mental decline

• Her problems came on quite quickly
• Didn’t fit her diagnosis or her history
• Several new drugs had been prescribed
• We researched drug interactions, and then…
• We requested a medication review with facility staff
Why we decided to intervene:

• Pay attention to your loved one: watch, ask, listen, write it down
• Research: identify REPUTABLE internet and other resources to research drugs, side effects and treatments
• Compare: symptoms with adverse effects or interactions of current, and especially new, drugs
• Communicate: first as a family – then with the staff
• Timing: delays can cost precious time in reversing adverse effects
• Be respectful but persistent
The family team

“Assume that any new symptom you
develop upon starting a new drug may be caused by the drug. If you have a new
symptom, psychiatric or otherwise,
report it to your doctor” Public Citizen, Health Research Group
www.worstpills.org

Do the professionals know the patient’s baseline? The family probably does…
Everyone intends well, but they may not be seeing the big picture (or the frail person) in front of them0.

Symptoms of Serotonin Syndrome:
1. Cognitive/behavioral changes: confusion, agitation, lethargy
2. Autonomic instability: rapid heart rate, sweating
3. Neuromuscular changes: myoclonus (twitching a muscle or group of muscles)
Self-limited if recognized early, it can be fatal
if left unrecognized and untreated.


SSRI antidepressant (citalopram)
+ serotonergic pain medication
to replace Vioxx (tramadol)
= Serotonin Syndrome

• Donepezil (Aricept), often prescribed for Alzheimer’s, was suggested by the facility’s consulting Psychiatrist whose diagnosis was “vascular dementia”.
• We declined, after reviewing the Therapeutics Initiative’s recommendations regarding the medication – and asked that no additional drugs be prescribed without family consent and without a medication review of all medications.
MORE drugs had been suggested!

“Ask about changes in your loved one even if no one asks.” http://thisisnotmymom.ca

Delirium
• Drugs and bugs (infections) most likely causes • Polypharmacy plus advanced age can often result
in delirium. • Delirium can be mistaken for Alzheimer’s or
dementia if the baseline isn’t known • A minor change (in drugs) can precipitate a crisis
among vulnerable elders (ask Dr. Sloan!). • Delirium is a serious health threat -- but also
largely preventable. • “After an episode of delirium, one year mortality
among frail elderly can be as high as 35 to 40%” - Delirium Prevention Training program: IPPOD
Sunnybrook Health Sciences Centre, Toronto ON

Definition of Polypharmacy
When the theoretical benefits of multiple
medications are outweighed by the negative
effect of the sheer number of medications,
regardless of class of medication or
“appropriateness” thereof.

Much prescribing for the elderly is an “evidence-free zone”.
A Bitter Pill: How the Medical Systemis Failing the Elderly
by Dr. John Sloan

Polypharmacy is a stand-
alone risk factor for
morbidity

Polypharmacy & admissions to acute care
• 5 or more drugs 10% • 7 or more drugs 20% • 9 or more drugs 30%
Percentage increase in transfers to acute care per year

Loss of function • 1 in 3 frail elders admitted
to hospital is discharged at a higher level of disability
• Can lose up to 5% of functional muscle strength for every day in bed.
• Delirium will keep a patient in bed and result in loss of function, even when the illness necessitating the hospitalization is successfully treated.

Fervid recovered cognitively from a diagnosis of “vascular dementia” after some drugs were stopped
Enjoying white wine and oysters with her family at her favourite restaurant.

Many weeks in bed resulted in loss of function. Fervid could not return to independent living.

The result of Fervid’s “drugectomy”
• Normal mental status (as bright as ever!)
• Physical improvement • Fervid returned to
“training” care aides she thought needed it
• Formed close relationships with staff
• Joined us for family outings • Lived 4 more years • But…she could not return to
independent living

My Question: Is there an epidemic of Alzheimer’s and dementia?
• We constantly hear of the “epidemic” of Alzheimer’s and dementia.
• Is there an epidemic of over-medication (with resulting hospital admissions – often the worst place for a frail elder to be?)
• How do I want it to be when I get there?

Alzheimer’s is often misdiagnosed
"It's a real problem. If you're older and you get a label of Alzheimer's — even a hint that you have Alzheimer's — there's no more critical thinking about it. The difficulty in pinning down Alzheimer's makes misdiagnosis too easy."
Peter Lichtenberg,
Head of the Institute of Gerontology
Wayne State University

Polypharmacy & c. difficile
• Fervid had many antibiotic treatments for suspected UTI’s
• 5 other residents had it
• Cleaning & infection protocols substandard or inconsistent
• Frequent transfer of staff and patients
• 5 courses of vancomycin weakened Fervid

A picture is worth a thousand words…
Over-medicated Life after the “drugectomy”

“It’s (about) quality of life…for my residents. I've seen dramatic differences in the quality of their life when the burden of their medication is reduced...”

What our family learned from Fervid

“Life’s too precious — we’ve enjoyed each other so much. I think [love] will grow. That’s the ticket into the next world. We will always be together, our love is always there and we will be part of the great growing field of love.
…I’ll be out there watching you”.
Fervid Trimble, August 2008

Fervid died blessing us.
If she had died 4 years earlier
of her drug interaction,
she would have died
not even recognizing us.
Let us work together to give our elders the chance for a leave-taking that has profound meaning both for their loved ones and themselves.
The meaning for all of us…

A picnic in the garden with Fervid
Dedicated to Fervid Trimble 1917 - 2008