Embed Size (px)
Citation preview

The Path to Clinical Enterprise Maturity
DEVELOPING A CLINICALLYINTEGRATED NETWORK

Kevin [email protected]
Michael StrileskySENIOR [email protected]
Danny [email protected]
dhgllp.com/healthcare

page 3The Path to Clinical Enterprise Maturity: Developing a Clinically Integrated NetworkCENTER FOR INDUSTRY TRANSFORMATION
Industry Forces Encouraging Clinical IntegrationThe healthcare industry is undergoing significant transformation. Providers are challenged to do more while being paid less, in part due to the increase in uncompensated care and more recently the shift in risk attributed to payment for value. The shift to value-based payment is causing hospitals, physicians, payers and employers to plan and execute strategies that include performance incentives and outcome measures that have rarely been included in prior contracts. While the strategies and tactics may vary, the end-in-mind objective is clear, our industry will move toward a payment mechanism that is attributed to enhancing quality and outcomes for the cost of care provided. The pathway for most health systems and physicians to begin meeting this objective is through the integration of both parties in a Clinically Integrated Network (CIN).
Clinical Integration is commonly defined as a network of providers working together, using proven protocols and measures, to coordinate patient care, improve quality, decrease cost, and demonstrate value to the market. This will represent an evolutionary performance pathway to achieve Clinical Enterprise Maturity (CEM) as more providers and facilities are integrated in the network. Once the CIN is confident it can demonstrate a value proposition, the network will approach payers and employers to contract with the network based on shared incentives aligned with defined quality and economic goals.
The concept of clinical integration has been around since 1996 when the Department of Justice and the Federal Trade Commission (FTC) defined it as “an active and ongoing program to evaluate and modify practice patterns by the networks’ physician participants to create a high degree of interdependence and cooperation among the physicians to control costs and ensure quality.” Generally, the FTC considers a program to be clinically integrated if it performs the following:
1) Common information technology to ensure exchange of all relevant patient data
2) Clinical protocols that are developed and adopted by providers
3) Care review based on the implementation of protocols
4) Mechanisms to ensure adherence to protocols.
While there are a number of details aligned with each of these criteria, FTC approval for a CIN is no longer required as long as the design of the CIN meets the above criteria. The FTC guidance and subsequent advisory opinions have resulted in a clear set of conditions for CIN development. However, there continues to be common misconceptions about what a CIN is and what it is not. The following chart outlines some of these misconceptions.
CLINICAL INTEGRATION IS NOT: CLINICAL INTEGRATION IS:
• Simply physician employment • A hospital only led initiative • Reduction of choice or limiting services • Only based on a new electronic medical records
system • Simply a mechanism to gain negotiating leverage
over payers • A stand-alone IPA / PHO messenger contract
Model • A return to capitation of the ‘90s
• A network led by select employed and private practice physicians typically working with a hospital to improve quality and efficiency of care
• Increased coordination between providers, supported by reliable data, to improve outcomes and reduce waste
• A legal structure that allows members of the network to be financially rewarded for demonstrated performance
• A vehicle that allows the network to collectively negotiate contracts on behalf of its members
• A model that lays the foundation for the future realities of accountable care
Although uncertainties regarding the post-reform environment remain, providers agree they must address three key challenges moving forward. CI provides a flexible model to respond to these challenges in a manner that positions providers for short- and long-term success.

page 4The Path to Clinical Enterprise Maturity: Developing a Clinically Integrated NetworkCENTER FOR INDUSTRY TRANSFORMATION
A New World Order: Clinical IntegrationOnce the CIN is confident it can demonstrate a value proposition, the network approaches payers and employers to contract with the network and provide other incentives that are based on achieving defined results. In many cases, development of the network and initial conversations with payers are initiated by health systems; however, once deployed, CINs become physician-led, professionally managed organizations.
CHALLENGE NUMBER ONE: SHIFTING RISK FROM PAYER TO PROVIDERHealthcare reform is shifting risk to providers by economically incentivizing hospitals / health systems and physicians to manage the populations they serve. This is a logical proposal to curb healthcare spending, but it creates challenges when developing the mechanics of risk-based programs. Early reports indicate mixed results regarding the effectiveness of ACOs. However, commercial payers are aggressively following suit and implementing incentive - and risk-based payment models. This transition to performance-based payments as it pertains to population health management requires transformational change in how providers deliver care and forces hospitals and physicians to accelerate efforts to more closely align.
WHY CLINICALLY INTEGRATED NETWORKS?Successful CINs facilitate significant interaction between a health system, its employed medical staff and its independent physician participants in the program. Regular communication, sharing of patient data and adherence to clinical pathways allow the CIN to achieve the increased coordination of care needed to succeed under a risk-based model where efficiency is rewarded and duplicative or unnecessary procedures are penalized.
CHALLENGE NUMBER TWO: MOVING FROM VOLUME TO VALUEPhysicians and health systems are being affected by recent cuts to fee-for-service reimbursement. Questions surrounding the fiscal cliff as well as uncertainty related to Medicaid expansion and Health Insurance Exchanges and a louder cry for a permanent Sustainable Growth Rate (SGR) solution have fueled additional concern in recent months. Payers are moving from a volume-based fee-for-service model, to a value-based model which pays based on performance and population management. Hospitals are concerned about their margins; physicians are concerned about their survival. Both are recognizing the need for closer collaboration to ease mutual financial pressures.
WHY CLINICALLY INTEGRATED NETWORKS?A CIN allows providers in the network to define the network’s quality initiatives and the metrics that will be tracked to measure that quality.
CHALLENGE NUMBER THREE: COMPETING ON QUALITYThe pursuit of quality in healthcare has been limited by (1) clear definition and adoption of quality metrics and (2) access to and transparency of performance data. Providers are beginning to solve both challenges by offering their own definition(s) of quality and by collecting, analyzing, and sharing performance data.
As health IT systems proliferate, patients, payers, and providers gain a greater understanding of cost and outcomes data and quality becomes a necessity. As insurance exchanges and tiered insurance products gain traction, quality has become a competitive priority for hospital and health system senior leadership.

page 5The Path to Clinical Enterprise Maturity: Developing a Clinically Integrated NetworkCENTER FOR INDUSTRY TRANSFORMATION
Market Conditions Dictating the Pace of AdoptionAll markets are different and are moving toward integrated networks at varying speeds. Unique market characteristics, including organizational profile, competitor strategies, physician profile, payer readiness, and employer dynamics will play a significant role in determining how fast or slow a market will transition toward integrated networks.
Each of the following market characteristics should be assessed to determine the pace at which the market is transitioning to an integrated environment where a CIN should be considered.
HOSPITAL PROFILE
Location, access, inpatient volume and market share, EBITDA, profit margin, quality scores, asset distribution, IT infrastructure
MARKET CHARACTERISTICS
Supply and demand of beds, outpatient facilities, demographics, population growth, CON requirements, payer mix, uninsured
COMPETITIVE LANDSCAPE
Competitive intensity, history of irrationality, pursuit of new strategies and/or payment models, alignment with physicians
PHYSICIAN PROFILE
Mix of independent, employed, multispecialty or super groups, historical hospital- physician and physician-physician relationships
PAYER PROFILEMarket share, rate parity, willingness to offer P4P or risk-based contracts
EMPLOYER PROFILE
Large employers (>1,000 employees) pursuing contracts with providers; small employers likely to abandon plans for Exchanges
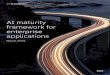
CIN Emerging as a Preferred Alignment Model
TACTICAL
LOW HIGH Degree of Alignment
Pay for Call
Physician Advisory Council
Directorship Management Services Organization
Joint Venture Professional Services Arrangement
Physician Hospital Organization
Gainsharing
Institute
Employment
STRATEGIC TRANSFORMATIONAL
IT Deployment
Physician Enterprise Foundation
Hospital Efficiency Program PCMH
Clinically Integrated Network Accountable Care Organization
Res
ourc
es R
equi
red
LOW
H
IGH
Co-Marketing
Co-Management Independent
Practice Association
The chart above depicts the alignment and integration efforts hospitals and health systems are pursuing with its physicians in response to the changing healthcare environment. As DHG defines it, a CIN qualifies as a “Transformational” model, meaning there is a high degree of organizational integration and high level of time, human and financial resources needed to implement. Much of the appeal of a CIN is that these programs are initially constructed internally whereas a bundled payment or ACO model is regulated by a government or commercial payer. Once tested and mature, a CIN can be used as a way to transition into a value-based model without the inherent risk involved in many of the other transformational models. Because a CIN is an evolutionary and ever-changing model, it creates an agile and flexible organization which is, in a sense, can be seen as resistant to future legislative changes that may occur.

page 6The Path to Clinical Enterprise Maturity: Developing a Clinically Integrated NetworkCENTER FOR INDUSTRY TRANSFORMATION
Hospitals & Health Systems
Payers & Employers
Physicians
• Enhance reimbursement for demonstrated quality
• Respond to market pressures• Provide right care in the right
setting• Align independent, employed,
and specialist physicians• Maintain / expand referral base
• Enhance value• Manage high cost
chronic conditions more effectively
• Increase collaboration with patients and providers
• Attain more attractive payer contracts
• Access patient information across the continuum
• Implement data-driven, clinical best practice guidelines
• Increase input in health system decisions
• Share in performance related savings
Patients & Communities
• Improve coordination of care
• Improve higher satisfaction
• Improve quality & outcomes
• Enhance cost efficiency
ALL
• Improve quality / patient satisfaction
• Enhance value
• Create greater coordination of care
• Align incentives
CI Creating Value for All StakeholdersCINs provide value to all involved parties—Hospitals & Health Systems, Physicians, Patients & Communities, and Payers & Employers. Engaging stakeholders early in the development process will enable the CIN to begin tracking, measuring and monitoring relevant information; establishing the value proposition as to why each stakeholder should participate in the network.

page 7The Path to Clinical Enterprise Maturity: Developing a Clinically Integrated NetworkCENTER FOR INDUSTRY TRANSFORMATION
CLINICALLYINTEGRATED
NETWORK
Structure & Governance
Infrastructure & Funding
Participation Criteria
Performance Objectives
Physician Leadership
Distribution of Funds
Contracting
Information Technology
Key Components of a CINA CIN is made up of various components, each equally important to its legality and success. To effectively implement, the network should understand the definition, relevance, and possible options for each of the components. Broad education and engagement of independent and employed physicians, with significant administrative direction and support, will aid in accelerating implementation. Additionally, clear understanding and communication will create consensus and buy-in across the community regarding the importance of positioning the providers for success in the midst of constant and continuous change. A CIN, as DHG defines it, is made up of the following components:
CI COMPONENT DEFINITIONS
Structure & Governance
With the exception of an employment-only model, a CIN can only be structured as a wholly-owned subsidiary, PHO or an IPA. The right structure depends on the desired speed to implement, ideal level of control, and willingness to take on risk.
Infrastructure & Funding
The CIN is a separate Business Entity with:
Participation Criteria
Member physicians or groups in the CIN must sign an agreement outlining the expectations and requirements for participation in the program.
Performance Objectives
CINs identify metrics and targets designed to meaningfully impact the clinical practice of all network physicians to improve and demonstrate value across the entire continuum of care.
Physician Leadership
Health systems must empower physicians to have an influence on the future direction of the network. This will help integrate physicians’ clinical expertise into hospital operations and increase cooperation and credibility of the CIN.
Information Technology
CINs use IT-dependent performance improvement architecture with data-based mechanisms and processes to monitor and track utilization of healthcare services to control costs, ensure quality, and demonstrate value.
Distribution of Funds
The CIN establishes a flow of funds to distribute rewards based on measureable performance. The design should reduce the complexity of the distribution methodology and increase transparency across the network
ContractingA CIN may utilize a wide range of contracts including fee for service, bundled payments for episodes of care, management of a chronic conditions, and/or disease management programs, and population based payments including shared risk arrangements or capitated payments.
• Distinct Identity, Mission, and Vision • Dedicated Leadership and Staff
• Sustainable Sources of Revenue • Participating Agreements with Providers

page 8The Path to Clinical Enterprise Maturity: Developing a Clinically Integrated NetworkCENTER FOR INDUSTRY TRANSFORMATION
Success Factors Creating Short Term WinsAs previously discussed, CINs are emerging as a response to changing healthcare dynamics that are holding providers more accountable for quality and outcomes. As the CIN becomes a strategic imperative in some markets, organizations should keep the following critical success factors in mind to implement a successful and sustainable network:
• ALIGN HEALTH SYSTEM OBJECTIVES WITH THE CIN VISION AND STRATEGY TO AVOID CONFLICTING MESSAGES IN THE LOCAL MARKET. As previously discussed, the CIN is a transformational change in the way a health system operates. Along these lines, prior to implementing a CIN, hospital and health system leadership must ensure that the local goals align with the vision and strategy of the network. Failing to do so can cause confusion as to the direction of the health system and prevent any short-term successes that can be useful for gaining momentum.
• INVOLVE PHYSICIAN LEADERS IN THE NETWORK DEVELOPMENT PROCESS TO GAIN PHYSICIAN BUY-IN FOR PROGRAM OBJECTIVES. Integration in the post-reform era requires a higher degree of physician-hospital alignment that is based on trust and transparency. Health systems willing to pursue a CIN must empower physician leaders to have an influence in the future direction of the network. This is critical in the development of a CIN and to achieving buy-in within the medical staff.
• EXPRESS A WILLINGNESS TO CREATE A NEW PARTNERSHIP MODEL WITH YOUR EMPLOYED AND INDEPENDENT PHYSICIANS THAT INCLUDES DEFINED ROLES FOR PHYSICIAN LEADERS. CINs are built on partnerships between the stakeholders – the hospital, its employed physicians, and independent practitioners. A true partnership requires a high level of interdependence among the groups. This means that leadership positions with decision-making responsibilities need to be reserved or created for independent and employed physicians to increase the level of ownership and accountability throughout the organization.
• MAINTAIN SYSTEMS THAT CAN TRACK AND MONITOR CLINICAL DATA ACROSS THE CONTINUUM OF AMBULATORY, ACUTE AND POST-ACUTE SERVICES. Investing in technical infrastructure such as EHR’s or patient registries that can measure quality outcomes across a broad spectrum of providers and locations is a quality imperative. In some markets, payment models are beginning to shift. Developing an infrastructure that shares vital patient information, and facilitates communication between providers is imperative to managing complex patients.
• DEVELOP A COMPREHENSIVE LIST OF METRICS THAT PROVIDE VALUE TO MULTIPLE STAKEHOLDERS AND POSITIONS THE CIN FOR GREATER LEVELS OF ACCOUNTABILITY. Due to the large number of stakeholders with varying interests it is important to understand that not all metrics will appeal to every stakeholder. With this in mind, it is vital to select metrics that not only align with the CIN vision and strategy but also appeal to the broad range of physicians within the network.
• CREATE AN EFFECTIVE COMMUNICATION STRATEGY ACROSS ALL STAKEHOLDERS TO INCREASE UNDERSTANDING OF THE KEY ISSUES IN CI. Clear understanding of CIN goals and initiatives by all network stakeholders will encourage dialogue and partnership formation as the strategy is implemented. A communication plan should be developed and implemented to maintain consistency between the tactical elements of the program within the business entity, and the broader system communication to the physicians and hospital staff.
• COMMIT TO APPROACH PAYERS AND EMPLOYERS IN THE MARKET AS A COMBINED NETWORK. Committing to jointly contract with payers and employers will require greater trust and transparency that can only occur if the physicians and health system are integrated. To realize sustained or improved reimbursement through this integration, hospitals and physicians will need to be confident in the value their network can provide in the market through higher quality and reduced costs. Creating a network for the sole purpose of negotiating better rates is not the purpose of a CIN, but financial rewards could most certainly be the byproduct of a network that creates savings and value to payers in the market.

page 9The Path to Clinical Enterprise Maturity: Developing a Clinically Integrated NetworkCENTER FOR INDUSTRY TRANSFORMATION
Call to ActionWe would estimate that over 20% of the hospitals in the United States have initiated their journey to either form, or participate in a Clinically Integrated Network. The most mature networks have gone through a process that includes:
1) Assessing their market need and opportunity for development of a CIN.
2) Creating an independent legal entity together with employed and independent physicians to deliver care.
3) Contracting with the related hospital through a contractual Hospital Efficiency Program to go “at risk” for managing hospital employee medical care.
4) Developing risk based contracts with independent payers.
5) Distributing shared savings to physicians who achieve quality and cost metrics aligned with the CIN’s contractual payer relationship.
The process to complete the above five steps must include a joint commitment between a hospital and its physicians to work collaboratively on this initiative. Following a commitment, there must be a shared sense of urgency (based on either a perception of opportunity or burning platform) for the two organizations to progress from one step to the next. On one level this may seem methodical and process driven, however our experience shows that developing a CIN is evolutionary in nature because the magnitude of change is so significant.
Delaying the evaluation and development of a CIN could prove to be a mistake if the payer market is quick to move to risk-based contracting and competitors in your market move faster than your organization to position themselves with their own CIN. Absent the pressure from payers and competitors, you may see the benefit of methodically assessing and navigating your way through the process to strategically align your health system with the physicians in your market. One significant advantage today is the ability to apply multiple lessons learned from other organizations that have gone through this before you and if need be, accelerate the development process associated with the five steps outlined in this article.

dhgllp.com/healthcare
CENTER FOR INDUSTRY TRANSFORMATION