Embed Size (px)
Citation preview

lable at ScienceDirect
Behaviour Research and Therapy 62 (2014) 60e73
Contents lists avai
Behaviour Research and Therapy
journal homepage: www.elsevier .com/locate/brat
The neuroscience of depression: Implications for assessment andintervention
Manpreet K. Singh a, *, Ian H. Gotlib b
a Stanford University School of Medicine, United Statesb Department of Psychology, Stanford University, United States
a r t i c l e i n f o
Article history:Received 31 March 2014Received in revised form16 August 2014Accepted 18 August 2014Available online 4 September 2014
Keywords:DepressionNeuroscienceNeuroimagingAssessmentTreatmentIntervention
* Corresponding author. Stanford University SchooPsychiatry and Behavioral Sciences, Division of Child aQuarry Road, Stanford, CA 94305-5719, United States. T650 724 4794.
E-mail address: [email protected] (M.K. Sing
http://dx.doi.org/10.1016/j.brat.2014.08.0080005-7967/© 2014 Elsevier Ltd. All rights reserved.
a b s t r a c t
Major Depressive Disorder (MDD) is among the most prevalent of all psychiatric disorders and is thesingle most burdensome disease worldwide. In attempting to understand the profound deficits thatcharacterize MDD across multiple domains of functioning, researchers have identified aberrations inbrain structure and function in individuals diagnosed with this disorder. In this review we synthesizerecent data from human neuroimaging studies in presenting an integrated neural network framework forunderstanding the impairments experienced by individuals with MDD. We discuss the implications ofthese findings for assessment of and intervention for MDD. We conclude by offering directions for futureresearch that we believe will advance our understanding of neural factors that contribute to the etiologyand course of depression, and to recovery from this debilitating disorder.
© 2014 Elsevier Ltd. All rights reserved.
Introduction
Major Depressive Disorder (MDD) is a prevalent psychiatricdisorder characterized by significant role impairment, suicide risk,economic burden, and the largest number of years lived withdisability in the US (US Burden of Disease Collaborators, 2013).Almost 20% of Americans will experience a major depressiveepisode in their lifetime (Hirschfeld, 2012); moreover, up to 80% ofthese individuals will have multiple depressive episodes (Bulloch,Williams, Lavorato, & Patten, 2014). Given its high prevalence,recurrence, and enormous personal and societal costs, it is notsurprising that the World Health Organization projects that MDDwill be the single most burdensome disease in the world in thiscentury (Moussavi et al., 2007).
In this review, we synthesize multimodal neuroimaging datathat inform the diagnosis and intervention of MDD, taking intoconsideration recent advances in the nosology and treatment ofdepression. With respect to diagnosis, we specifically consider the
l of Medicine, Department ofnd Adolescent Psychiatry, 401el.: þ1 650 723 5511; fax: þ1
h).
advantages of addressing the heterogeneity of MDD by integratinga dimensional Research Domain Criteria (RDoC) approach in eval-uating neuroimaging characteristics of depression. In terms ofintervention, we review recent research demonstrating the neuraleffects of the most evidence-based interventions, of rapid-actingantidepressants (e.g. ketamine), and the regional and global ef-fects of targeting neural networks.
According to the Diagnostic and Statistical Manual-Fifth Edition(DSM-5), a diagnosis of MDD requires a persistent disturbance ofmood (sadness, and/or in children, irritability) or a loss of interestor pleasure in virtually all activities, in addition to at least four ofthe following symptoms: sleep disturbance, guilt, loss of energy,impaired concentration, change in appetite, psychomotor agitationor retardation, and suicidal ideation (American PsychiatricAssociation, 2013). Given these varied symptoms, it is not surpris-ing that depression is a heterogeneous disorder; indeed, each ofthese symptoms has specific risk factors, severities, and trajectories(Fried, Nesse, Zivin, Guille, & Sen, 2013). Further, both MDD and itsindividual symptoms often co-occur with other psychiatric disor-ders (Curry et al., 2014); they also manifest differently both acrossdevelopmental stages (Dekker et al., 2007) and between males andfemales (Goodwin & Gotlib, 2004). This heterogeneity and comor-bidity has posed significant challenges for the diagnosis andtreatment of depression and has hindered our ability to predictlong-term outcome of MDD. Although investigators and clinicians

M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e73 61
have made significant advancements in identifying depressivesymptoms and in managing MDD with multimodal pharmacolog-ical and psychological treatments, there are wide variations in theefficacy and tolerability of interventions (Perlis, 2014), and prob-lems related to symptom relapse and medication non-adherence(Sato & Yeh, 2013). Further, despite the well-documented burdenof MDD, we do not yet understand the pathophysiology of thisdisorder.
In attempting to address this issue, researchers have begun toexamine psychobiological aspects of MDD in the context of RDoC.For example, in order to advance our understanding of the path-ophysiology and outcome of MDD, investigators have attempted todeconstruct depression along unitary psychopathological di-mensions, such as anhedonia (Downar et al., 2013) or negativeaffect (Vrieze et al., 2014). In a recent review, Dillon et al. (2014)related anhedonic behavior to deficits in psychological functionsthat rely heavily on dopamine signaling, especially cost/benefitdecision-making and reward learning, influenced negatively bothby acute threats and chronic stress. Other studies have docu-mented shared characteristics between MDD and other disordersassociated with blunted or negative affect, such as schizophrenia,by focusing on similar reduced expressive behaviors measured bycomputerized acoustic analysis of speech (Cohen, Najolia, Kim, &Dinzeo, 2012). Although these are recent efforts, these di-mensions of depression may aid in predicting treatment outcome.Researchers have also characterized cognitive impairments asso-ciated with depression. For example, Gotlib and Joormann (2010)noted that depressed individuals have been found consistentlyto be characterized by difficulties with inhibition of negative in-formation and deficits in working memory, ruminative responsesto negative mood states and life events, and the inability to usepositive stimuli to regulate negative mood.
Importantly, recent advances in brain imaging have allowedresearchers to augment studies of cognitive and behavioral im-pairments in MDD with an examination of neural circuit-levelmechanisms that may underlie these difficulties (Foland-Ross &Gotlib, 2012). Specifically, neuroimaging studies have docu-mented structural and functional neural characteristics critical tothe pathogenesis of MDD (see Hamilton, Chen, & Gotlib, 2013 for arecent review). These studies have also demonstrated that anom-alies in distributed, integrated neural networks that involve mul-tiple brain regions, linked structurally and functionally, underliethe disturbances in cognitive functioning that have been docu-mented in MDD (Sacher et al., 2012). Only recently, however, haveresearchers begun to examine explicitly the nature of the relationbetween clinical and neural network markers of MDD at variouspoints during the onset and course of the disorder, and to useneural characteristics to predict treatment outcome. We believethat neuroimaging is a promising tool for elucidating the patho-genesis of MDD; it is a safe, noninvasive procedure that is ideallysuited for simultaneously identifying aberrant behavior, brainstructure, and brain function in MDD. Indeed, with neuroimaging,we can bridge a clinical assessment of depressive symptoms withan examination of brain abnormalities to advance our under-standing of the pathophysiology of MDD.
We have three broad goals in this review. We describe anoma-lies in neural structure and function in adults and youth with MDDand discuss the implications of these abnormalities, first, for theassessment of depression, and second, for approaches to inter-vention with this disorder. Finally, we offer directions for futureresearch that we believe will advance our understanding of bio-logical factors that are implicated in the etiology and course ofMDD, and in recovery from depression. We begin by presenting abrief review of neural aspects of unipolar depression and theirimplications for assessment of MDD.
How the neuroscience of depression can inform assessment
Researchers have consistently documented impairments inemotional functioning and emotion regulation in MDD (Gotlib &Joormann, 2010). Moreover, these difficulties have been found topredict the early onset (Klein et al., 2013) and the recurrence ofdepressive episodes (Lewinsohn, Allen, Seeley, & Gotlib, 1999),suggesting that impairments in specific domains of emotionalfunctioning reflect stable vulnerabilities that place individuals atincreased risk for experiencing recurrent episodes of MDD. Neu-roimaging studies have complemented these clinical findings,documenting aberrant structure, function, and connectivity inbrain regions that subserve these aspects of emotion and emotionalregulation. Specifically, investigators have reported structuralanomalies in MDD in the amygdala and hippocampus, and func-tional abnormalities in the subgenual anterior cingulate cortex(sgACC), dorsolateral prefrontal cortex (DLPFC), amygdala, andventral striatum in MDD (Sacher et al., 2012). Further, there isgrowing recognition that depressed individuals are characterizedby abnormalities in the anatomical and functional connectionsamong these brain regions (Hamilton et al., 2013). In the followingsections we describe these neural aberrations in depressed in-dividuals, their relation to the clinical syndrome of MDD, and theirimplications for assessment of depression. Key findings from thissection are summarized in Table 1.
Structural neuroimaging in MDD
Researchers using structural magnetic resonance imaging (MRI)have reported abnormalities in specific brain regions in depressedindividuals. Using such tools as manual volumetry, voxel-basedmorphometry (VBM), and cortical thickness, investigators havedocumented differences in neural structure between individualswith depression and healthy controls, primarily involvingdepression-related reductions in brain regions important for thegeneration and regulation of emotion. Meta-analyses that havepooled structural neuroimaging data in depressed individuals haveconsistently identified focal gray matter volumetric reductions inthe rostral anterior cingulate cortex (rACC; Bora, Fornito, Pantelis,&Yücel, 2012), hippocampus (Cole, Costafreda, McGuffin,& Fu, 2011),striatum and, more broadly, basal ganglia (Bora, Harrison, Davey,Yücel, & Pantelis, 2012), insula (Liu et al., 2014), subregions of theprefrontal cortex (PFC; Kempton et al., 2011), and amygdala (Sacheret al., 2012), although reports of decreased amygdala volume indepressed individuals are less consistent in medicated samples(Hamilton, Siemer, & Gotlib, 2008). Trait-specific structural differ-ences between depressed and nondepressed individuals have beenreported as relative thickening in MDD the temporal pole, caudate,and posterior cingulate, thinning of the medial PFC (VanEijndhoven et al., 2013), and reduced volumes in the anteriorinsula (Takahashi et al., 2010) and the left anterior cingulate(Caetano et al., 2006). Larger gray matter volume in the bilateralamygdala, hippocampus, and dorsolateral PFC have been found infirst-degree relatives of patients with MDD, suggesting a mecha-nism of risk for MDD. The most consistent state-dependent struc-tural finding is reduction in hippocampal volume (Arnone et al.,2013).
Through inhibitory connections with other subcortical struc-tures, the hippocampus is involved in the appraisal and regulationof stress and in the generation of emotion. Indeed, investigatorshave demonstrated that gray matter reductions in hippocampalvolume are associated with an increased number of depressiveepisodes (Videbech & Ravnkilde, 2004), and with greater symptomseverity and longer illness duration (Cheng et al., 2010), includinglonger durations during which depressive episodes went untreated

Table 1Common neuroimaging findings that characterize individuals diagnosed withdepression relative to controls.
Finding Region/Network Reference/Review/Meta-analysis
Reduced gray mattervolume
Anterior cingulatecortex (includingsubgenual orrostral anteriorcingulate)
Bora, Fornito, et al. (2012),Bora, Harrison, et al.(2012), Vasic et al. (2008),Koolschijn et al. (2009),Singh et al. (2013),Groenewold et al. (2013),Lai (2014), Sperduti et al.(2013), Kühn et al. (2012),Kerestes et al. (2013)
Hippocampus Cole et al. (2011),Videbech and Ravnkilde(2004), Foland-Ross et al.(2013), Norbury et al.(2013), McKinnon et al.(2009), Suzuki et al. (2013)
Striatum Bora, Fornito, et al. (2012),Bora, Harrison, et al. (2012),Groenewold et al. (2013),Lai (2014)
Basal ganglia Bora, Fornito, et al. (2012),Bora, Harrison, et al. (2012)
Amgydala Sacher et al. (2012),Kerestes et al. (2013)3
Insula Liu et al. (2014), Dieneret al. (2012)
VentrolateralPrefrontal Cortex
Salvadore et al. (2011),Kerestes et al. (2012),Sperduti et al. (2013)
DorsolateralPrefrontal Cortex
Li et al. (2010), Singh et al.(2013), Choi et al. (2013),Chechko et al. (2013),Korgaonkar et al. (2013),Kerestes et al. (2012)
Orbitofrontal Cortex Koolschijn et al. (2009),Singh et al. (2013),Kerestes et al. (2013)
Reduced white matterintegrity
Limbic tracts Choi et al. (2013)Thalamic projections Choi et al. (2013)Corpus Callosum Choi et al. (2013)
Aberrant activationduring functionalMRI (*hyperactivityto positive valenceand hypoactivity tonegative valence ofstimuli presented)
Anterior cingulatecortex (includingrostral andsubgenual)
Diener et al. (2012),Nejad et al. (2013),Wagner et al. (2013)
Medial prefrontalcortex
Steele et al. (2007),Nejad et al. (2013)
Amygdala* Groenewold et al. (2013)Thalamus Lai (2014)Parahippocampalgyrus*
Groenewold et al. (2013),Lai (2014)
Cerebellum* Groenewold et al. (2013)Parietal cortex Chechko et al. (2013)
Aberrant resting statefunctional connectivity
Subgenual anteriorcingulate andthalamus
Greicius et al. (2007)
Default ModeNetwork
Marchetti et al. (2012),Tahmasian et al. (2013),Ajilore et al. (2013),Sambataro et al. (2013)
Central ExecutiveNetwork
Tahmasian et al. (2013)
Salience Network Tahmasian et al. (2013)DorsomedialPrefrontalCortex to multiplenetworks
Sheline et al. (2010),Van Tol et al. (2013)
Pregenual cingulateto thalamus,amygdalastriatum
Anand et al. (2009)
M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e7362
(Sheline, Gado, & Kraemer, 2003). Depression-associated re-ductions in gray matter volume in emotion regulatory regions ofthe PFC, which include DLPFC (Li et al., 2010) and ventrolateral PFC(VLPFC; Salvadore et al., 2011), ACC and sgACC, and orbitofrontalcortex (OFC), reflect the involvement of these structures in im-pairments in reasoning and other executive functions, regulation ofemotion and attention, and processing of rewards and motivationin MDD. In particular, reductions in ACC volume have been asso-ciated with poorer executive functioning (Vasic, Walter, H€ose, &Wolf, 2008). Some studies suggest that volumetric reductions infrontal regions, especially in the ACC and OFC, are more pro-nounced than are decreases in hippocampal and striatal volumes(e.g., Koolschijn, van Haren, Lensvelt-Mulders, Hulshoff Pol, &Kahn, 2009). In fact, in examining large-scale structural brain net-works, researchers have consistently found widespread abnor-malities in depressed individuals in gray matter in the ACC, DLPFCand dorsomedial PFC (DMPFC), and lateral and medial OFC (Singhet al., 2013).
These gray matter anomalies in prefrontal and subcortical brainregions may be associated with abnormalities within white mattertracts that connect these regions. White matter hyperintensities,areas of increased signal intensity on T2 MRI images that may beindicative of neuropathological changes in white matter tracts,have been found to be more common in depressed than in healthyindividuals (Arnone, McIntosh, Ebmeier, Munaf�o, & Anderson,2012). White matter hyperintensities may represent early signs ofdemyelination (Hajek, Carrey, & Alda, 2005), and have been re-ported to be associated with greater clinical severity (Tham, Woon,Sum, Lee, & Sim, 2011). These anatomical abnormalities are poorlyunderstood, however, and may be confused with vascular abnor-malities, particularly in late-life depression. For example, post-mortem studies of depression have documented pathology inprefrontal white matter, including decreased oligodendrocytedensity, reduced expression of genes related to oligodendrocytefunction, molecular changes in intercellular adhesion moleculeexpression levels, and ischemic changes (Tham et al., 2011). It isdifficult to distinguish, however, whether signal intensity differ-ences reflect myelin changes, reduced axon density, or an entirelydifferent process related to regional differences in vasculature.Thus, to characterize quantitatively white matter tracts betweenprefrontal and subcortical regions, researchers have used alterna-tive approaches such as diffusion tensor imaging (DTI).
DTI uses measurement of water diffusion to study white mattertracts in vivo. Water diffusion in white matter is highly anisotropic(i.e., not equal in all directions); diffusion tends to be greater par-allel than perpendicular to the fiber axis. Using DTI, investigatorshave documented abnormalities in MDD inwhite matter tracts thatconnect portions of the PFC to subcortical structures (Liao et al.,2013), suggesting that MDD is a syndrome of white matterdisconnection. Researchers have also reported lower levels of whitematter integrity in the limbic system, DLPFC, thalamic projectionfibers, corpus callosum, and other association fibers in depressedthan in nondepressed individuals (but see also Choi et al., 2013).
Functional neuroimaging in MDD
Functional MRI (fMRI) generates data regarding magnitude ofbrain activation in specific regions, as indexed by levels ofoxygenated versus de-oxygenated hemoglobin, referred to as theBlood Oxygen Level Dependent (BOLD) signal. Investigators usingfMRI have documented aberrations in regional brain activation inMDD in response to a variety of emotional and cognitive stimuli,suggesting that depression is associated with dysfunction inemotion regulation (Rive et al., 2013). Other researchers have re-ported findings that suggest more complex patterns of neural

M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e73 63
dysfunction in depression. For example, using both task-activatedand resting-state data, investigators have documented hypoactiveclusters in the anterior insula and rACC in MDD that appear to belinked to affectively biased information processing and poorcognitive control (Diener et al., 2012). In addition, frontal brainareas have been found to show both under- and over-activationduring cognitive-emotional challenges in MDD and, subcortically,thalamic and striatal activations are associated with biased pro-cessing of emotional stimuli (Hamilton et al., 2012). Similar to thestructural neuroimaging studies described above, some in-vestigators argue that aberrant activations in medial prefrontalcortex (mPFC) show larger effect sizes than do limbic activations(Steele, Currie, Lawrie,& Reid, 2007). ThemPFC and rACC have beenimplicated in self-referential processing and are emphasized intheoretical models of MDD that posit biases toward negativeemotional processing and increased self-focus (Nejad, Fossati, &Lemogne, 2013). We now describe specific tasks used in fMRIstudies of depression, discussing cognitive and emotional func-tioning and their interplay in MDD.
Researchers have examined neural responses as depressed in-dividuals complete an emotional Stroop task in the scanner toexamine neural aspects of the interference in cognitive processingassociated with this task. Wagner et al. (2013) found that patientswith MDD are characterized by an inability to deactivate the rACCduring cognitive processing, leading to a compensatory prefrontalhyperactivation and interfering with cognitive control. This inter-action between affective and cognitive circuitry may contribute tothe reduced capacity for affect regulation and cognitive control inMDD. Interestingly, the rACC was activated during negative self-referential processing, and this activation was related to theseverity of patients' depressive symptoms. Other investigators havefound hypoactivity in MDD during an emotional Stroop task inregions important for conflict resolution, including the DLPFC, pa-rietal, and extrastriate cortices combined with amygdala hyperac-tivity (Chechko et al., 2013).
Given memory difficulties that often characterize depressedindividuals, researchers have also examined neural aspects ofworking memory (WM) in MDD. Anomalous activations in bilateralhippocampus during verbal WM tasks have been documented inunmedicated and remitted depressed patients compared to con-trols, suggesting that both depression and a vulnerability torecurrence of depression are characterized by a reduced capacity toignore task-irrelevant stimuli (Foland-Ross et al., 2013; Norbury,Godlewska, & Cowen, 2013). Other investigators have reportedhypoactivation in the DLPFC and hyperactivation in the DMPFCduring WM tasks (Korgaonkar, Grieve, Etkin, Koslow, & Williams,2013). When a WM task is combined with emotional distracterstimuli, remitted depressed individuals show hyperactivation ofthe DLPFC in response to negative emotional distracters buthypoactivation of the DLPFC and VLPFC in response to positiveemotional distracters, suggesting an attentional bias toward nega-tively valenced information (Kerestes et al., 2012).
Several researchers have examined reward-related brain func-tions and deficits in depressed individuals. A recent meta-analysisfound that a reward network is characterized in MDD bydecreased striatal and limbic activity and increased cortical activity(Zhang, Chang, Guo, Zhang, & Wang, 2013). More specifically,depressed individuals consistently show reduced caudate responseto anticipation and outcome of monetary rewards, and increasedactivation in themiddle frontal gyrus and dorsal ACC (dACC) duringanticipation of reward. Variability in tasks and mood states werefound to contribute to heterogeneity across studies, highlightingthe importance in future investigations of carefully specifying thetypes of reward used and the different components of rewardprocessing that are being examined.
It appears, therefore, that emotional processing in MDD ischaracterized by hyperactivity in the amygdala and ACC, andhypoactivity in the striatum and DLPFC. Findings in this area havebeen inconsistent, however, due in part to valence-related effects. Arecent meta-analysis found that depressed individuals show hy-peractivity in the amygdala, striatum, parahippocampal gyrus,cerebellum, fusiform gyrus, and ACC in response to positive stimuli,but hypoactivity in these regions in response to negative stimuli(Groenewold, Opmeer, de Jonge, Aleman, & Costafreda, 2013). Inaddition, activation in the ACC appears to be modulated both byvalence and by facial versus non-facial stimuli. These findingssuggest that emotional valence moderates neural abnormalities indepression and is a critical factor in understanding emotionaldysfunction in depression. Indeed, a recent meta-analysis of fMRIstudies using emotional faces found that whereas depressed pa-tients have significantly increased activations in the striatum andparahippocampal gyrus, nondepressed controls have increasedactivations in the medial and middle frontal gyrus, thalamus, ACC,and superior frontal gyrus (Lai, 2014).
Other cognitive functions are also affected in MDD. Given thedocumented deficits in inhibitory control in MDD, researchers havealso examined patterns of response inhibition in depression usingtasks such as the Go/NoGo task. Depressed individuals have beenfound to show greater neural activation than do controls in frontal,limbic, and temporal regions during successful response inhibition(Langenecker et al., 2007). Other cognitive functions includingresponse flexibility, reversal learning, and emotional reactivityhave similarly been examined to understand the pathophysiologyof depression. Theorists have suggested that depressed individualsshift from episodic to semantic autobiographical memory retrievalin which they overgeneralize and, consequently, reduce executiveresources that lead to a pervasive negative self-representation(Watson, Berntsen, Kuyken, & Watkins, 2013). Interestingly,healthy persons with a rigid negative self-image mimic patterns ofaltered neurobehavioral functioning found in depression, includinghypoactivity of the VLPFC and ACC (Sperduti et al., 2013). Theselatter findings suggest that a negative self-image represents a riskfactor for depression. Importantly, aberrations in any of thesecognitive functions may represent important targets forintervention.
The functional imaging studies that we described above all usedtasks that target specific brain regions and functions. Task-independent spontaneous resting-state functional connectivity(RSFC) has recently been used to gain a better understanding ofintrinsic brain activity and relations among prefrontal andsubcortical structures at rest. Researchers have postulated thatabnormal resting-state activity may affect stimulus-induced neuralactivity in core medial prefrontal systems important for self-representation as well as for interactions with external stimulisuch as stress (Northoff, Wiebking, Feinberg, & Panksepp, 2011).Indeed, unlike task-activation studies, RSFC can directly assessneural systems without the confound of differences in performancethat might increase variability within study groups. RSFC isassessed by correlating this activity temporally; such patterns arebelieved to reflect synchronous interactions among brain regions.Using RSFC, researchers have found depressed individuals toexhibit broad abnormalities in interhemispheric connectivity(Wang, Li, Zhang, Zeng, Jin, et al., 2013), as well as focal deficits inconnectivity at rest. One specific RSFC network is the default modenetwork (DMN), which includes the ACC and a large portion ofmPFC extending inferiorly into the OFC. This network is posited tobe involved with internally generated thought and is inhibitedwhen individuals attend to external stimuli that require attentionand cognition. The first RSFC finding in depression reportedincreased connectivity between the DMN and the sgACC and the

M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e7364
thalamus (Greicius et al., 2007). Given these and similar subsequentfindings, the DMN has been hypothesized to play a critical role inthe pathophysiology and recurrence of depression (Marchetti,Koster, Sonuga-Barke, & De Raedt, 2012). In fact, the saliencenetwork (SN) and central executive network (CEN) have also beenfound to be disrupted in MDD (Tahmasian et al., 2013). Depressedindividuals exhibit increased intrinsic connectivity between bilat-eral dorsal medial PFC and each of cognitive control, default mode,and affective networks, suggesting that a coordinated engagementof diverse networks might explain the development and expressionof specific symptoms of depression (Sheline, Price, Yan, & Mintun,2010). A recent analysis of subsystems of the DMN suggest thatpatients with MDD exhibit more focal increased within-networkconnectivity in posterior, ventral, and core DMN subsystems(Sambataro,Wolf, Pennuto, Vasic,&Wolf, 2013). Other studies havedocumented decreased intrinsic corticolimbic connectivity,including between the pregenual ACC and the thalamus, amygdala,and pallidostriatum, in depressive and bipolar mood disorders(Anand, Li, Wang, Lowe, & Dzemidzic, 2009). These findings high-light the possibility that mood-state and treatment-related factorssuch as treatment status (Anand, Li, Wang, Gardner, & Lowe, 2007)and treatment response (Guo et al., 2013), and exposure to early lifestress (Cisler et al., 2013), influence the nature of the relation be-tween MDD and neural activation. Despite the specific directionaldiscrepancies, these findings collectively suggest that depression isa disorder of disrupted global and focal connectivity.
Recent advances in analytic techniques have increased ourability to use RSFC to inform the assessment of MDD. For example,RSFC has been used in conjunction with support vector machine(SVM) classification methods, which have discriminated MDD pa-tients from healthy controls with 84e93% accuracy, based on con-nectivity in key areas of the DMN and SN (Zeng, Shen, Liu, & Hu,2013). Cortical thinning in the DMPFC has been found to directlyand selectively affect RSFC to the precuneus in depressed in-dividuals (Van Tol et al., 2013), and reductions in RSFC have beenfound to overlap with volume reductions in the ACC and rightinferior frontal gyrus that are correlated with rumination (Kühn,Vanderhasselt, De Raedt, & Gallinat, 2012). Finally, investigatorshave recently tried to bridge data from RSFC and white matterbased structural connectivity data to construct the resting-statestructural connectome. In a small sample of seven depressed in-dividuals and seven matched controls, function-by-structure hier-archical mapping demonstrated that depressed individuals hadstronger associations in bilateral posterior cingulate and rightprecuneus than did controls, both regions important for self-referential functions (Ajilore et al., 2013). These studies illustratethe increased sensitivity gained by using integrative multimodalimaging data and analyses to examine aberrations in brain con-nectomes that characterize MDD.
Although researchers may disagree about the specific di-mensions or brain regions that are most relevant to the onset andmaintenance of depressive symptoms, there is general consensusthat altered interactions between key prefrontal and subcorticalregions contribute to dysfunctional cognition and regulation ofemotion in MDD. Importantly, altered interactions among theseregions may be a developmental phenomenon. For example, intypical neurodevelopment, subcortical gray matter developmentprecedes prefrontal development and pruning, and there appearsto be a shift in functional dependence from subcortical to prefrontalstructures around puberty (Thompson et al., 2000). Consequently,puberty may represent a critical sensitive period when such func-tional shifts are vulnerable to alterations and the development ofpsychopathology (Casey, Jones, & Hare, 2008). Perhaps not coinci-dentally, the onset of depression occurs most commonly inadolescence (Shanahan, Copeland, Costello, & Angold, 2011).
Neuroimaging findings indicate that reductions in hippocampalvolume (Chen, Hamilton, & Gotlib, 2010) and blunted striatal acti-vation (Sharp et al., 2014) may precede the onset of MDD, sug-gesting that certain neural features are endophenotypic for MDD.Further, the results of several studies suggest that chronic depres-sion can lead to neurodegeneration, highlighting the potential forearly intervention to prevent neuronal loss and regenerate neuraltissue to restore function (Bewernick & Schlaepfer, 2013). Specif-ically, experiencing a greater number of depressive episodes in-fluences the organization of striatal networks (Meng et al., 2014)and may be associated with impaired hippocampal activationduring a recollection memory task (Milne, MacQueen,&Hall, 2012)and with selective deficits in down-regulating amygdala responsesto negative emotional stimuli using reappraisal (Kanske, Heissler,Sch€onfelder, & Wessa, 2012), factors that also contribute to riskfor relapse. Vulnerability for recurrence of depressive episodes hasbeen found to be associated with poorer outcomes in patients withearlier onset of depression, with increased number and length ofdepressive episodes (Moylan, Maes, Wray, & Berk, 2013), and withhistory of childhood trauma (Barnhofer, Brennan, Crane, Duggan, &Williams, 2014). Thus, in such patients, longer and more frequentdepressive episodes appear to increase vulnerability for furtherepisodes, precipitating an accelerating and progressive course ofillness, leading to functional decline.
By studying youth with MDD, we can examine the neurobio-logical features of depression without the confounds associatedwith chronic illness course, including medication exposure andcomorbidities, and can investigate etiological factors associatedwith the onset, early stages, and progression of MDD. Althoughmeta-analytic data in adults suggest that hippocampal volume re-ductions occur only after the onset of depression (McKinnon, Yucel,Nazarov, & MacQueen, 2009), studies of youth with MDD indicatethat reductions in hippocampal volume are a consequence ofdepressive symptoms detected as early as the preschool years(Suzuki et al., 2013), and in young offspring of mothers withdepression even before the onset of symptoms (Chen et al., 2010).Across tasks assessing emotion processing, cognitive control, af-fective cognition, reward processing, and resting state, researchershave found elevated neural activity in the ACC, VMPFC and OFC, andamygdala in children and adolescents with MDD (Kerestes, Davey,Stephanou, Whittle, & Harrison, 2013). Longitudinal studies thatcontextualize functional activation patterns according to neuro-developmental changes and pubertal maturation will be critical inproviding a more comprehensive picture of the trajectories ofanomalies in neural development in depression.
How the neuroscience of depression can inform intervention
Investigators have begun to use imaging techniques to examineneural aspects of different interventions in individuals diagnosedwith MDD. Across most imaging studies, treatment such as anti-depressants, and especially those affecting the serotonergic system,have been shown to modulate the volumes, functions andbiochemistry of brain regions implicated in MDD, including theDLFPC, ACC and amygdala (Bellani, Dusi, Yeh, Soares, & Brambilla,2011). In the following sections, we describe changes in neuralstructure and function in MDD in response to a variety of in-terventions, and discuss how these changes can inform the devel-opment of more effective treatments for this disorder. Key findingsfrom this section are summarized in Table 2.
Structural MRI and intervention for MDD
As we described above, MDD is characterized by structural ab-normalities that are associatedwith clinical features of the disorder.

Table 2Neuroimaging findings that characterize response to treatment for depression.
Finding Region/Network Reference/Review/Meta-analysis
Antidepressantsincrease gray mattervolume
Hippocampus MacQueen et al. (2008),Fu et al. (2007),Delaveau et al. (2011)
Orbitofrontal cortex Kong et al. (2014),Lisiecka et al. (2011),Delaveau et al. (2011)
Anterior cingulatecortex
Chen et al. (2007),Lisiecka et al. (2011), Fuet al. (2013), Fu et al.(2008)
Middle frontal gyrus Kong et al. (2014)Antidepressants
normalize fMRIactivation
Anterior cingulatecortex (includingsubgenual and rostral)
Chen et al. (2007),Lisiecka et al. (2011), Fuet al. (2013), Fu et al.(2008), Delaveau et al.(2011), Mayberg et al.(2005), Langeneckeret al. (2007), Brody et al.(1999); Miller et al.(2008)
Hippocampus MacQueen et al. (2008),Fu et al. (2007),Delaveau et al. (2011)
Parahippocampus Delaveau et al. (2011)Amygdala Rosenblau et al. (2012),
Victor et al. (2013),Delaveau et al. (2011),Miller et al. (2008)
Striatum (includingcaudate, nucleusaccumbens)
Samson et al. (2011),Lisiecka et al. (2011),Langenecker et al.(2007), Stoy et al.(2012)
Insula Samson et al. (2011),Rizvi et al. (2013),Langenecker et al.(2007), Delaveau et al.(2011)
Prefrontal cortex(including ventrolateraland dorsolateral)
Fitzgerald et al. (2008),Samson et al. (2011),Delaveau et al. (2011),Rosenblau et al. (2012),Victor et al. (2013),Langenecker et al.(2007), Brody et al.(1999), Carlson et al.(2013), Drevets (1998),Van Wingen et al.(2010)
Superior frontal gyrus Samson et al. (2011)Posterior cingulatecortex
Samson et al. (2011),Rizvi et al. (2013)
Antidepressantsimprove functionalconnectivity
Prefrontal-subcorticalnetworks
Wang, Li, Zhang, Zeng,Dai, et al. (2013)
Anterior cingulatecortex
Salvadore et al. (2010),Delaveau et al. (2011)
Posterior cingulatecortex
Delaveau et al. (2011)
Precuneus Delaveau et al. (2011)Inferior parietal lobe Delaveau et al. (2011)Thalamus Lisiecka et al. (2011)Cerebellum Lisiecka et al. (2011)
Structuredpsychotherapynormalizes fMRIactivation
Anterior cingulatecortex (including dorsaland subgenual)
Siegle et al. (2006),Chen et al. (2007), Fuet al. (2008), Buchheimet al. (2012)
Medial prefrontalcortex
Buchheim et al. (2012)
Amygdala Siegle et al. (2006),Buchheim et al. (2012)
Medial temporal lobe Buchheim et al. (2012),Amsterdam et al.(2013)
Table 2 (continued )
Finding Region/Network Reference/Review/Meta-analysis
Electroconvulsivetherapy increasesbrain connectivity
Increased fiber integrityof dorsal fronto-limbicpathways
Lyden et al. (2014)
Transcranial magneticstimulationimproves function attarget andtransynapticallyconnected networks
Subgenual anteriorcingulate
Pascual-Leone et al.(1998), Liston et al.(2014)
Connectivity betweencentral executive andsalience networks anddefault mode network
Chen et al. (2013)
Deep brain stimulationreduces symptoms insignificantlytreatment refractorypatients
Subgenual anteriorcingulate
Anderson et al. (2012)
M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e73 65
Recently, researchers have examined whether these abnormalitiescan be reversed with intervention. Using multivariate pattern an-alyses of structural MRI data to predict treatment response indepressed individuals, researchers have distinguished treatment-resistant from treatment-sensitive individuals with 82e91% accu-racy (Liu et al., 2012). Researchers have also found greater volumesof the hippocampal body in medicated than in unmedicateddepressed individuals (Malykhin, Carter, Seres, & Coupland, 2010).Further, researchers have found that greater baseline hippocampalvolumes predict remission of MDD following eight weeks of anti-depressant treatment (MacQueen, Yucel, Taylor, Macdonald, &Joffe, 2008). Other studies have shown no effects of treatment onhippocampal volume (Vythilingam et al., 2004), but have reportedthat hippocampal memory function improves with treatment.Kong et al. (2014) found increased gray matter volume in the leftmiddle frontal gyrus and right OFC in depressed individuals relativeto controls following eight weeks of fluoxetine administration, andChen et al. (2007) reported that faster rates of improvement insymptoms and lower residual symptom scores in depressed in-dividuals were associated with greater gray matter volume in theACC. Interestingly, patients with treatment-responsive MDDcontinue to have abnormalities in white matter tracts in the pro-jection fibers and corpus callosum (Guo et al., 2012); similarly,white matter hyperintensities have been found to predict failure torecover following antidepressant therapy (Sneed et al., 2011). Theselatter findings suggest that white matter abnormalities associatedwithMDD are less responsive to pharmacological intervention thanare gray matter abnormalities. Other investigators, however, havefound that four weeks of guided imagery psychotherapy not onlysignificantly reduces depressive symptoms, but also increasesprefrontal fractional anisotropy, suggesting that psychotherapycontributes to white matter remodeling through a topedown reg-ulatory mechanism (Wang et al., 2013). Discrepant findings acrossstudies may be due to differences in treatment targets across in-terventions, to heterogeneous levels of depression severity acrossstudies, or to other factors that influence treatment response.
fMRI and intervention for MDD
Many of the cross-sectional functional neuroimaging studies inMDD reviewed above were confounded by varying levels of expo-sure of participants to psychotropic medications at the time of thescan. A growing number of researchers are now examining theeffects of intervention on neural function in depression. Across arange of tasks, depressed individuals have been found to exhibitpatterns of limbic hyperactivity and prefrontal hypoactivity thatreverse with intervention (Fitzgerald, Laird, Maller, & Daskalakis,

M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e7366
2008). For example, as early as four weeks after treatment withmirtazapine or venlafaxine, depressed individuals show increasedactivations in the DMPFC, posterior cingulate cortex, superiorfrontal gyrus, caudate, and insula during an emotion perceptiontask (Samson et al., 2011). Other researchers have found that rela-tive to controls, depressed individuals had less activity in theamygdala and PFC during the explicit processing of negative pic-tures after eight weeks of escitalopram (Rosenblau et al., 2012), andduring the implicit processing of emotional faces after eight weeksof sertraline (Victor, Furey, Fromm, €Ohman, & Drevets, 2013). Se-lective serotonin reuptake inhibitors (SSRIs) may bemost beneficialfor patients who are less able to engage cognitive control networkswhile they process negative stimuli (Miller et al., 2013) or whilethey perform verbal WM tasks (Walsh et al., 2007). Indeed, re-searchers have reported that after eight weeks of fluoxetine,depressed individuals have reversed attenuated activations in thehippocampus and extrastriate visual regions as they process posi-tively valenced facial stimuli (Fu et al., 2007). Interestingly, treat-ment with SSRIs in depressed individuals has also been shown toattenuate a bias toward attending to masked sad faces and to leadto a positive bias toward masked happy faces, along with corre-sponding mood-congruent amygdala activation (Victor, Furey,Fromm, Ohman, & Drevets, 2010). Further, using an inhibitorycontrol task, Langenecker et al. (2007) found that activation duringsuccessful inhibition in bilateral inferior frontal, left amygdala,insula, and nucleus accumbens, and during unsuccessful inhibitionin the rACC, predicted improvement in depressive symptomsfollowing treatment with escitalopram; Stoy et al. (2012) foundescitalopram to also normalize ventral striatal hypoactivity duringreward processing. In another study researchers showed that aftereight weeks of SSRI treatment, depressed individuals no longerdiffered from controls in either DLPFC or amygdala activity duringan emotional interference task (Fales et al., 2009). Baseline activa-tions in posterior cingulate cortex, anterior insula, and premotorcortex while processing affective images have been found to predictresponse to combination pharmacotherapies such as fluoxetine andolanzapine (Rizvi et al., 2013). Researchers have also demonstratedthat fMRI can be used to distinguish neural responses to in-terventions that have different mechanisms of action in the brainthan do SSRIs (Wagner et al., 2010).
Studies using positron emission tomography (PET) and singlephoton emission computed tomography (SPECT) have yielded in-formation about the effect of specific neurochemical challenges onregional brain function at rest or under activation. Different PETmethods demonstrate consistent abnormalities in depressed in-dividuals in the prefrontal, cingulate, and amygdala regions(Kennedy, Javanmard, & Vaccarino, 1997). For example, symptomimprovement from paroxetine is correlated with normalized infe-rior frontal gyrus and VLPFC metabolism, and lower metabolism inthe left ventral anterior cingulate gyrus is associated with bettertreatment response (Brody et al., 1999). These studies also provideinformation about the activity of neurotransmitters and theregional expression of specific molecular targets in depression,including their modulation by drug treatment, and the kinetics ofdrug disposition and activity directly in the target organ (Moresco,Matarrese, & Fazio, 2006). For example, lower pretreatment sero-tonin (5-HTT) binding by PET may predict non-remission fromMDD following one year of naturalistic antidepressant treatment,demonstrating the power of functional PET to distinguish treat-ment remitters from nonremitters (Miller, Oquendo, Ogden, Mann,& Parsey, 2008).
In this context, functional neuroimaging has been used todocument changes in neural activation in response to newerpharmacological agents for depression such as scopolamine (Fureyet al., 2013) and ketamine (Carlson et al., 2013). Imaging markers
have the potential to provide a powerful assay to investigate hownovel therapies work, and have validated the function of ketamineas an N-methyl-D-aspartate receptor antagonist (Doyle et al., 2013)that leads to decreased metabolism in the right habenula and theextended medial and orbital prefrontal networks in associationwith rapid antidepressant response (Carlson et al., 2013).Ketamine-related symptom improvement is predicted by pre-treatment functional connectivity between the pgACC and the leftamygdala during a working-memory task (Salvadore et al., 2010).The rapid and long-lasting (up to 10 days) antidepressant responseto ketamine has been demonstrated consistently in treatment-resistant patients (Bortolozzi, Celada, & Artigas, 2013; Hayley &Litteljohn, 2013), in electroconvulsive therapy (ECT) and non-ECTstudies (Fond et al., 2014), and in unipolar and bipolar depression(McGirr et al., 2014).
Increased functional connectivity between prefrontal (e.g., OFCor ACC) and other emotion processing regions including thecaudate, thalamus, and cerebellum, has also been found to predictresponse to antidepressant therapy (Lisiecka et al., 2011). Further, inthe only fMRI study to examine changes in brain activity withtreatment in pediatric depression, (Tao et al., 2012) documentedthat overactivation in prefrontal and temporal regions in depressedyouth normalized after eight weeks of fluoxetine treatment.
In sum, therefore, most studies have found normalizing effectson neural activation in response to emotional stimuli followingantidepressant treatment. In a recent meta-analysis, (Delaveauet al., 2011) found treatment-related increases in activation inDLFPC, DMPFC, and VLPFC and decreases in activation in limbicstructures such as the amygdala, hippocampus, parahippocampus,sgACC, OFC, and insula. This meta-analysis also found decreasedactivation in the anterior and posterior cingulate cortices, pre-cuneus, and inferior parietal lobule, suggesting restored deactiva-tion of the DMN in MDD following antidepressant treatment. In adifferent meta-analysis of studies of participants who weremedication-free before their initial scan, Fu, Steiner, and Costafreda(2013) found distinct regional activations that predicted antide-pressant response. Specifically, Fu et al. found that increasedbaseline activity in the ACC predicted a higher likelihood ofimprovement, whereas increased baseline activation in the insulaand striatum was associated with poorer clinical response. Indeed,anomalous activation in the sgACC has been a treatment target forpatients with refractory depression (Mayberg et al., 2005) and hasbeen found to predict treatment response (Korb, Hunter, Cook, &Leuchter, 2011). Although it is difficult to disentangle whetherimproved fMRI response following treatment is due to symptomreduction or to the intervention itself, these findings highlight thepromise of fMRI data to provide prognostic markers of clinicalresponse to treatment in MDD. Further, there are limited neurobi-ological data to guide treatment choices for individuals withdepression, and even fewer data that are not biased by treatmenthistories (Dunlop et al., 2012). Studies in which depressed patientsare selected or stratified on the basis of these neural characteristicsand that accurately predict which patients respond to treatmentwill advance the field significantly. Similarly, large controlledstudies of individuals who were previously naïve to any interven-tion will increase our knowledge of the specific effects of antide-pressant treatment on neural activation.
Functional neuroimaging is limited by its relative sensitivity tostate-dependent features of depression, which are often difficult todistinguish from trait-related phenomena. Importantly, however,the results of a recent meta-analysis investigating three neurobio-logical models of depression, including limbic-cortical, cortico-striatal, and the DMN, suggest that state and trait neural markers ofdepression can be distinguished based on the responsiveness ofactivations in these neural regions to intervention (Graham et al.,

M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e73 67
2013). This meta-analysis found broad support for limbic-corticaland cortico-striatal models of depression, and noted that lateralfrontal areas were most sensitive to treatment. In contrast, subcor-tical regions appeared relatively insensitive to treatment, suggestingthat they are indicators of trait vulnerability rather than state ortreatment-sensitive markers of depression. Other studies suggestthat aberrant amygdala activation in response to sad faces (Arnone,McKie, et al., 2012) and memory formation and retrieval (VanWingen et al., 2010) are specific to the depressed state and areresponsive to treatment. Portions of the prefrontal cortex are alsoresponsive to treatment (Drevets, 1998; Van Wingen et al., 2010). AsStuhrmann, Suslow, and Dannlowski (2011) note, it is likely thatinconsistencies among studies are due to the heterogeneity of pa-tient samples and paradigms. Changes in resting-state function inresponse to eight weeks of escitalopram also support a prefrontal-subcortical model of depression (Wang, Li, Zhang, Zeng, Dai, et al.,2013), suggesting that biomarkers of treatment response are notlimited to task-based fMRI studies.
Although psychotherapy is a mainstay intervention for depres-sion, relatively few studies have examined the effects of structuredpsychotherapy on neural function. One early study found thatdepressed individuals with low sustained reactivity to emotionalstimuli in the sgACC and high reactivity in the amygdala exhibitedthe strongest improvement following 16 weeks of cognitivebehavioral therapy (CBT) (Siegle, Carter, & Thase, 2006). Anotherstudy found that depressed individuals with higher levels ofbaseline dACC activity during an affect recognition task had betterclinical response to 16 weeks of CBT (Fu et al., 2008), suggestingthat ACC activity is an important predictor of treatment responsefor both psychotherapeutic and pharmacological interventions(Chen et al., 2007). Using SPECT, Amsterdam et al. (2013) found thatlow pretreatment serotonin transporter binding in the medialtemporal lobe bilaterally increased over time in depressed in-dividuals who experienced symptom improvement with 12 weeksof CBT. Neural benefits of psychotherapy seem to be sustained evenbeyond the acute phase of treatment. Depressed patients who hadincreased activation in the left anterior hippocampus/amygdala,sgACC, and mPFC before treatment with psychodynamic psycho-therapy showed reduction in activation in these areas after 15months of treatment, which was associated with improvement indepressive symptoms (Buchheim et al., 2012). Importantly, re-searchers who directly compared psychotherapy with pharmaco-therapy found dissociable patterns of treatment response. Forexample, whereas response to CBT was associated with a reciprocalmodulation of cortical-limbic connectivity, pharmacological treat-ment with venlafaxine engaged additional cortical and striatal re-gions (Kennedy et al., 2007). It appears that, much likepharmacological interventions, CBT affects clinical recovery bymodulating the functioning of specific sites in limbic and corticalregions; however, unique directional changes in frontal cortex,cingulate, and hippocampus with CBT relative to paroxetine mayreflect modality-specific effects (Goldapple et al., 2004). These re-sults suggest that neuroimaging can identify treatment-specificbiomarkers (McGrath et al., 2013), a formulation that is particu-larly important for a disorder that is typically characterized byequivalent responses to different kinds of intervention.
Neuromodulation
Aberrant functional activations in key brain regions have led tothe development of neuromodulatory treatment options for severeand treatment refractory depression (Kennedy & Giacobbe, 2007).In contrast to medications that putatively work by altering neuro-chemistry throughout the brain, neuromodulation offers a moretargeted approach to treatment thatmodulates specific networks in
the brain (Schlaepfer & Bewernick, 2014). Neuromodulatory in-terventions include ECT, magnetic seizure therapy, repetitivetranscranial magnetic stimulation (rTMS), transcranial direct cur-rent stimulation (tDCS), vagal nerve stimulation (VNS), and deepbrain stimulation (DBS). ECT is considered the first-line treatmentfor more severe forms of depression (Kellner et al., 2014). RecentMRI studies indicate that ECT may increase brain connectivity indepression, demonstrated by neuroplasticity of white mattermicrostructure suggesting increased fiber integrity of dorsal fronto-limbic pathways involved in mood regulation (Lyden et al., 2014).Further, depressed individuals who do not respond to ECT arecharacterized by a poorer overall clinical response, more sustainedreported depressionwith anxiety features, and higher left temporalregional cerebral blood flow (Berggren, Gustafson, H€oglund, &Johanson, 2014). Unfortunately, extant data reveal considerablevariations among studies, which limits our understanding of aunified mechanism by which ECT might achieve its positive clinicaleffects (Bolwig, 2014).
rTMS and tDCS have comparable effects to antidepressant drugs,but have a relatively benign profile of side effects (Brunoni et al.,2010). Importantly, the effects of rTMS are not limited to thecortical area that is targeted directly, but affect a wider neuralnetwork transynaptically (Pascual-Leone et al., 1998). For example,although targeted modulation of subgenual cingulate connectivityhas been shown to play an importantmechanistic role in alleviatingdepression (Liston et al., 2014), rTMS has also been shown toselectively modulate functional connectivity both within and be-tween the broader CEN and DMN. Chen et al. (2013) recentlycombined TMS with functional MRI to causally excite or inhibitTMS-accessible prefrontal nodes within the CEN or SN to determinethe effects on the DMN. Single-pulse excitatory stimulationsdelivered to only the CEN node induced negative DMN connectivitywith the CEN and SN, consistent with the hypothesized negativeregulation of the DMN by the CEN and the SN. Conversely, low-frequency inhibitory repetitive TMS to the CEN node resulted in ashift of DMN signal from its normally low-frequency range to ahigher frequency, suggesting disinhibition of DMN activity. More-over, the CEN node exhibited this causal regulatory relation pri-marily with the medial prefrontal portion of the DMN. Thesefindings advance our understanding of the causal mechanisms bywhich major brain networks coordinate information processing,and how these systems might be aberrant in MDD.
DBS and VNS are invasive strategies with a possible role intreatment-resistant depression (Brunoni et al., 2010). In fact, DBShas yielded significant reductions in depressive symptomatologyand high rates of remission in severely treatment-resistant patients(Anderson et al., 2012). Some researchers have suggested thatneuromodulation would be more efficacious if used early to alterthe developmental course of dysfunctional neurocircuitry; how-ever, safety and tolerability are important concerns, especially forpediatric populations (Croarkin et al., 2010). Some researchers havefound benefit for anterior cingulotomy in treatment refractorypatients, demonstrating that a stronger clinical response wasassociated with more anterior lesions and with smaller lesionvolumes (Steele, Christmas, Eljamel, & Matthews, 2008). Otherinvestigators have proposed trigeminal nerve stimulation as apromising adjunct to pharmacotherapy in depression (Cook et al.,2013). Additional comparative studies are needed to determinethe relative advantages of each of these approaches and how best tomatch patients to specific neuromodulation strategies.
Limitations and directions for future research
In this article we have described implications of neuroimagingfor assessment and treatment of MDD. There are several challenges

M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e7368
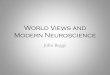
for research in this field. For example, patients are diagnosed andtreated on the basis of symptom clusters that are heterogeneousand are likely to be caused by numerous and divergent biologicalfactors. Two patients can exhibit non-overlapping clusters ofsymptoms, but share the same diagnosis and treatment recom-mendation. Another challenge involves distinguishing depressionfrom other commonly co-occurring disorders such as anxiety. Pa-tients may be better served by a diagnostic system that is based onunderlying genetic and neurobiological factors that define subtypesof broad syndromes instead of on symptom clusters. One way toapply this concept would be to identify biomarker signatures thataccompany specific domains of behavioral abnormalities and thatpredict distinct treatment responses. The identification of newbiomarker targets based on disease mechanisms has the potentialto significantly improve the treatment of depression. In Fig. 1 wepresent a conceptual framework for developing new models ofdepression grounded in neuroscience.
Given the complexity of the depressed brain, it is also importantto integrate neuroimaging findings with results of gene and proteinexpression analyses that suggest that depression involves disrup-tions in various components of a complex signaling network(Villanueva, 2013). Components of this network include the hypo-thalamicepituitaryeadrenal axis; the production of neurotrophinsand growth factors; the expression of miRNAs; the production ofproinflammatory cytokines; and the abnormal delivery of gastro-intestinal signaling peptides, all of which may contribute to sig-nificant alterations in mood. Indeed, cytokines have beenimplicated in early-onset depression in adolescents, suggestingimportant developmental vulnerabilities in the immune and in-flammatory systems (Mills, Scott, Wray, Cohen-Woods, & Baune,2013). Similarly, animal models of stress exposure have been usedto advance our understanding of the pathophysiology of depression(Abelaira, R�eus, & Quevedo, 2013). These factors also modulateneurogenesis in brain regions involved in MDD, and are function-ally interconnected in a fashion that creates cascading abnormal-ities. Neuroimaging findings are also being associated with specificgenotypes (Flint& Kendler, 2014). Advances in genetic and imagingtechnologymay enable us to gain a better understanding of the roleof genetics in contributing to brain abnormalities that increase riskfor the development of depression.
Fig. 1. Conceptual framework for developin
Some investigators have argued that progress in assessment andintervention for depressive disorders has been limited by a lack ofvalid diagnostic and treatment biomarkers (Niciu et al., 2013). Inaddition to integrating macro- and micro-level information aboutneural systems, there are several additional solutions that mightstrengthen the impact of studies of depression on our under-standing of assessment and intervention. For example, many neu-roimaging studies have used univariate analytic techniques toexamine single structures and specific task-based neural functions,which has limited our ability to integrate neurobiological findingsacross modalities. A multivariate analytic approach, using tech-niques such as graph theory and multivariate pattern analyses, islikely to be more sensitive to subtle neurobiologic changes than aretraditional univariate analyses, and can be used to develop a moresophisticated model of depression based on neural networkdysfunction. Similarly, as we noted above, investigators haveassessed clinically heterogeneous samples cross-sectionally (e.g.,variable pubertal status, ages, gender, medication exposures,number of episodes, and comorbidities). While informative, find-ings of these studies are limited in furthering our understanding ofthe neural consequences of MDD, which are likely to be bettermodeled with longitudinal study designs. Finally, researchersshould integrate approaches across biological systems includinggenetics, peripheral measures, proteomics/metabolomics, multi-modal neuroimaging, neuropsychopharmacological challenge par-adigms, and clinical predictors. These systems can be integrated toexplore potential predictor and mediator/moderator biomarkersfor novel intervention approaches, which could then be selected fora priori use in larger multisite controlled studies.
Other challenges associated with fMRI research in MDD includethe appropriate selection of cognitive tasks and the use of stan-dardized tasks that take into account differences in performance ofindividuals at different life stages. Future studies will benefit fromcareful selection of tasks and from generating a priori hypothesesabout specific mechanisms of dysfunction to advance our under-standing of functional impairments in depression. Additionalfunctional and resting state connectivity studies are important toevaluate networks involved in clinical and neurocognitive aspectsof depression, such as executive function, self-monitoring, andemotion regulation. In addition, paradigms that highlight core
g neuroscience models of depression.

M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e73 69
symptoms of depression, such as anhedonia, could expand howweconceptualize subtypes of depression. In addition, more studies areneeded assessing symptomatic and never-ill youth at familial riskfor depression to determine whether there is functional impair-ment prior to the onset of depression (e.g., Gotlib, Joormann, &Foland-Ross, 2014). Neuroimaging studies of healthy and sub-syndromal youth at risk for depression can aid in determiningendophenotypes of depression.
As we noted above, studies of youth at familial risk for depres-sion indicate that structural and functional neural changes precedeonset of depressive symptoms, stressing the importance of earlyidentification of risk factors to prevent disease onset and progres-sion. Compared to low-risk counterparts, healthy daughters ofdepressed mothers selectively attend to negative facial expressionsafter a negative mood induction (Joormann, Talbot,& Gotlib, 2007),interpret ambiguous words and stories more negatively (Dearing &Gotlib, 2009), and have poorer accuracy in identifying sad facialexpressions (Joormann, Gilbert, & Gotlib, 2010). These negativecognitive biases in high-risk youth have been coupled withincreased stress reactivity (Gotlib, Joormann, Minor, & Hallmayer,2008) and with abnormalities in brain structure and function,including reduced hippocampal volumes (Chen et al., 2010),amygdala and VLPFC hyperactivity during negative mood inductioncombined with DLPFC and dACC hypoactivity during automaticmood regulation (Joormann, Cooney, Henry, & Gotlib, 2012), pu-tamen and right insula hypoactivity while anticipating rewards(Gotlib et al., 2010), and aberrant frontolimbic responses toemotional faces (Monk et al., 2008). Other studies have found fa-milial risk for depression to be associated with cortical thinning(Peterson et al., 2009), altered white matter integrity (Huang, Fan,Williamson, & Rao, 2011), and lower levels of intrinsic connectiv-ity at rest (Clasen, Beevers, Mumford, & Schnyer, 2014). Impor-tantly, these abnormalities in neural function in high-risk youthmimic those found in depressed adults and, consequently, mayrepresent risk factors for the development of MDD. Studies of high-risk populations may also suggest clues for resilience factors thatmay be important in preventing the onset of illness, but longitu-dinal observations are required for this purpose.
Less is known about how abnormalities in structure and func-tion in depression are directly related to each other on a networklevel. Nor do we understand how depression-associated impair-ment in specific brain regions affect other areas to which they arefunctionally and structurally connected to form neural networks.Indeed, we do not yet understand precisely how these anomaliesare related to MDD. Inconsistent results across studies may be dueto variations in how brain volume was measured and non-uniformscaling across brain regions. To correct for this variation, moststructural studies provide volumetric measurements as a ratio tooverall brain volume. Variation in whole brain measurements be-tween groups is therefore an important consideration when eval-uating specific brain regions (Barnes et al., 2010). Nevertheless,these studies collectively demonstrate structural and functionaldeficits in multiple cortical and subcortical brain regions that maylead to emotional dysfunction during critical periods of neuro-development. Further, volumetric changes in portions of PFC mayhave a significant impact on cognitive development and the regu-lation of emotion, and suggest vulnerability factors that affectchronicity of the course of depressive illness.
We are also limited in our understanding of how the neuralcharacteristics of depression described above can be useful inpredicting treatment response and long-term prognosis. Some re-searchers attribute the lack of progress in this area to the gap be-tween current clinical nosology and classification suggested byneuroimaging (Farah & Gillihan, 2012). Other investigators havebegun to link neurobiological assessments to an understanding of
treatment response (Fu & Costafreda, 2013), which may be an earlyproxy for prognosis. Clearly, we need to conduct more innovativeexaminations of MDD that integrate structural and functionalproperties of the brain in order to provide a strong empirical basisfor the development of effective early and lasting interventions thatprevent progression and recurrence of MDD.
Finally, despite the progress that we have made in under-standing the neurobiological basis of depression, longitudinalcontrolled studies are needed to examine more explicitly the na-ture of the relation between depression and neuroimaging findings,to identify neurobiomarkers in order to establish rational treatmentstrategies in individuals with and at risk for developing depression,and to elucidate the mechanisms that contribute to illness onset.Through such investigations, we should be better able to clarify thecomplex etiopathophysiology of depression in order to diagnosemore accurately, and treat more effectively, depressed individuals.Given the enormous costs of MDD and themodest effects of currentinterventions for depression, it is imperative that we develop amore comprehensive and integrative neural conceptualization ofthis debilitating disorder.
Conflict of interest
Drs Singh and Gotlib report no known conflicts of interestassociated with this publication.
Acknowledgments
Preparation of this article was facilitated by National Institute ofMental Health Grants MH085919 to MKS and MH074849,MH101495, and MH101545 to IHG.
References
Abelaira, H. M., R�eus, G. Z., & Quevedo, J. (2013). Animal models as tools to study thepathophysiology of depression. Revista Brasileira de Psiquiatria (S~ao Paulo, Brazil:1999), 35(Suppl. 2), S112eS120.
Ajilore, O., Zhan, L., Gadelkarim, J., Zhang, A., Feusner, J. D., Yang, S., et al. (2013).Constructing the resting state structural connectome. Frontiers in Neuro-informatics, 7, 30.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mentaldisorders: DSM-5 (5th ed.). Washington, D.C: American Psychiatric Association.
Amsterdam, J. D., Newberg, A. B., Newman, C. F., Shults, J., Wintering, N., & Soeller, I.(2013). Change over time in brain serotonin transporter binding in majordepression: effects of therapy measured with [(123) I]-ADAM SPECT. Journal ofNeuroimaging: Official Journal of the American Society of Neuroimaging, 23,469e476.
Anand, A., Li, Y., Wang, Y., Gardner, K., & Lowe, M. J. (2007). Reciprocal effects ofantidepressant treatment on activity and connectivity of the mood regulatingcircuit: an FMRI study. The Journal of Neuropsychiatry and Clinical Neurosciences,19, 274e282.
Anand, A., Li, Y., Wang, Y., Lowe, M. J., & Dzemidzic, M. (2009). Resting state cor-ticolimbic connectivity abnormalities in unmedicated bipolar disorder andunipolar depression. Psychiatry Research, 171, 189e198.
Anderson, R. J., Frye, M. A., Abulseoud, O. A., Lee, K. H., McGillivray, J. A., Berk, M.,et al. (2012). Deep brain stimulation for treatment-resistant depression: effi-cacy, safety and mechanisms of action. Neuroscience and Biobehavioral Reviews,36, 1920e1933.
Arnone, D., McIntosh, A. M., Ebmeier, K. P., Munaf�o, M. R., & Anderson, I. M. (2012).Magnetic resonance imaging studies in unipolar depression: systematic reviewand meta-regression analyses. European Neuropsychopharmacology: The Journalof the European College of Neuropsychopharmacology, 22, 1e16.
Arnone, D., McKie, S., Elliott, R., Juhasz, G., Thomas, E. J., Downey, D., et al. (2013).State-dependent changes in hippocampal grey matter in depression. MolecularPsychiatry, 18, 1265e1272.
Arnone, D., McKie, S., Elliott, R., Thomas, E. J., Downey, D., Juhasz, G., et al. (2012).Increased amygdala responses to sad but not fearful faces in major depression:relation to mood state and pharmacological treatment. The American Journal ofPsychiatry, 169, 841e850.
Barnes, J., Ridgway, G. R., Bartlett, J., Henley, S. M. D., Lehmann, M., Hobbs, N., et al.(2010). Head size, age and gender adjustment in MRI studies: a necessarynuisance? NeuroImage, 53, 1244e1255.
Barnhofer, T., Brennan, K., Crane, C., Duggan, D., & Williams, J. M. G. (2014).A comparison of vulnerability factors in patients with persistent and remitting

M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e7370
lifetime symptom course of depression. Journal of Affective Disorders, 152e154,155e161.
Bellani, M., Dusi, N., Yeh, P. H., Soares, J. C., & Brambilla, P. (2011). The effects ofantidepressants on human brain as detected by imaging studies. Focus on majordepression. Progress In Neuro-Psychopharmacology & Biological Psychiatry, 35,1544e1552.
Berggren, A., Gustafson, L., H€oglund, P., & Johanson, A. (2014). A long-termfollow-up of clinical response and regional cerebral blood flow changes indepressed patients treated with ECT. Journal of Affective Disorders, 167,235e243.
Bewernick, B. H., & Schlaepfer, T. E. (2013). Chronic depression as a model diseasefor cerebral aging. Dialogues in Clinical Neuroscience, 15, 77e85.
Bolwig, T. G. (2014). Neuroimaging and electroconvulsive therapy: a review. TheJournal of ECT, 30, 138e142.
Bora, E., Fornito, A., Pantelis, C., & Yücel, M. (2012). Gray matter abnormalities inMajor Depressive Disorder: a meta-analysis of voxel based morphometrystudies. Journal of Affective Disorders, 138, 9e18.
Bora, E., Harrison, B. J., Davey, C. G., Yücel, M., & Pantelis, C. (2012). Meta-analysis ofvolumetric abnormalities in cortico-striatal-pallidal-thalamic circuits in majordepressive disorder. Psychological Medicine, 42, 671e681.
Bortolozzi, A., Celada, P., & Artigas, F. (2013). Novel therapeutic strategies in majordepression: focus on RNAi and ketamine. Current Pharmaceutical Design, 20,3848e3860.
Brody, A. L., Saxena, S., Silverman, D. H., Alborzian, S., Fairbanks, L. A., Phelps, M. E.,et al. (1999). Brain metabolic changes in major depressive disorder from pre- topost-treatment with paroxetine. Psychiatry Research, 91, 127e139.
Brunoni, A. R., Teng, C. T., Correa, C., Imamura, M., Brasil-Neto, J. P., Boechat, R., et al.(2010). Neuromodulation approaches for the treatment of major depression:challenges and recommendations from a working group meeting. Arquivos deNeuro-Psiquiatria, 68, 433e451.
Buchheim, A., Viviani, R., Kessler, H., K€achele, H., Cierpka, M., Roth, G., et al. (2012).Changes in prefrontal-limbic function in major depression after 15 months oflong-term psychotherapy. PloS one, 7, e33745.
Bulloch, A., Williams, J., Lavorato, D., & Patten, S. (2014). Recurrence of majordepressive episodes is strongly dependent on the number of previous episodes.Depression and Anxiety, 31, 72e76.
Caetano, S. C., Kaur, S., Brambilla, P., Nicoletti, M., Hatch, J. P., Sassi, R. B., et al.(2006). Smaller cingulate volumes in unipolar depressed patients. BiologicalPsychiatry, 59, 702e706.
Carlson, P. J., Diazgranados, N., Nugent, A. C., Ibrahim, L., Luckenbaugh, D. A.,Brutsche, N., et al. (2013). Neural correlates of rapid antidepressant response toketamine in treatment-resistant unipolar depression: a preliminary positronemission tomography study. Biological Psychiatry, 73, 1213e1221.
Casey, B.j., Jones, R. M., & Hare, T. A. (2008). The adolescent brain. Annals of the NewYork Academy of Sciences, 1124, 111e126.
Chechko, N., Augustin, M., Zvyagintsev, M., Schneider, F., Habel, U., & Kellermann, T.(2013). Brain circuitries involved in emotional interference task in majordepression disorder. Journal of Affective Disorders, 149, 136e145.
Chen, M. C., Hamilton, J. P., & Gotlib, I. H. (2010). Decreased hippocampal volumein healthy girls at risk of depression. Archives of General Psychiatry, 67,270e276.
Chen, A. C., Oathes, D. J., Chang, C., Bradley, T., Zhou, Z.-W., Williams, L. M., et al.(2013). Causal interactions between fronto-parietal central executive anddefault-mode networks in humans. Proceedings of the National Academy ofSciences of the United States of America, 110, 19944e19949.
Chen, C. H., Ridler, K., Suckling, J., Williams, S., Fu, C. H. Y., Merlo-Pich, E., et al.(2007). Brain imaging correlates of depressive symptom severity and predictorsof symptom improvement after antidepressant treatment. Biological Psychiatry,62, 407e414.
Cheng, Y. Q., Xu, J., Chai, P., Li, H.-J., Luo, C.-R., Yang, T., et al. (2010). Brain volumealteration and the correlations with the clinical characteristics in drug-naïvefirst-episode MDD patients: a voxel-based morphometry study. NeuroscienceLetters, 480, 30e34.
Choi, K. S., Holtzheimer, P. E., Franco, A. R., Kelley, M. E., Dunlop, B. W., Hu, X. P., et al.(2013). Reconciling variable findings of white matter integrity in majordepressive disorder. Neuropsychopharmacology: Official Publication of theAmerican College of Neuropsychopharmacology, 39, 1332e1339.
Cisler, J. M., James, G. A., Tripathi, S., Mletzko, T., Heim, C., Hu, X. P., et al. (2013).Differential functional connectivity within an emotion regulation neuralnetwork among individuals resilient and susceptible to the depressogenic ef-fects of early life stress. Psychological Medicine, 43, 507e518.
Clasen, P. C., Beevers, C. G., Mumford, J. A., & Schnyer, D. M. (2014). Cognitive controlnetwork connectivity in adolescent womenwith and without a parental historyof depression. Developmental Cognitive Neuroscience, 7, 13e22.
Cohen, A. S., Najolia, G. M., Kim, Y., & Dinzeo, T. J. (2012). On the boundaries of bluntaffect/alogia across severe mental illness: implications for Research DomainCriteria. Schizophrenia Research, 140, 41e45.
Cole, J., Costafreda, S. G., McGuffin, P., & Fu, C. H. Y. (2011). Hippocampal atrophy infirst episode depression: a meta-analysis of magnetic resonance imagingstudies. Journal of Affective Disorders, 134, 483e487.
Cook, I. A., Schrader, L. M., Degiorgio, C. M., Miller, P. R., Maremont, E. R., &Leuchter, A. F. (2013). Trigeminal nerve stimulation inmajor depressive disorder:acute outcomes in an open pilot study. Epilepsy & Behavior: E&B, 28, 221e226.
Croarkin, P. E., Wall, C. A., McClintock, S. M., Kozel, F. A., Husain, M. M., &Sampson, S. M. (2010). The emerging role for repetitive transcranial magnetic
stimulation in optimizing the treatment of adolescent depression. The Journal ofECT, 26, 323e329.
Curry, J. F., Aubuchon-Endsley, N., Brancu, M., Runnals, J. J., & , VA Mid-AtlanticMirecc Women Veterans Research Workgroup, VA Mid-Atlantic Mirecc Regis-try Workgroup, Fairbank, J. A. (2014). Lifetime major depression and comorbiddisorders among current-era women veterans. Journal of Affective Disorders,152e154, 434e440.
Dearing, K. F., & Gotlib, I. H. (2009). Interpretation of ambiguous information in girlsat risk for depression. Journal of Abnormal Child Psychology, 37, 79e91.
Dekker, M. C., Ferdinand, R. F., van Lang, N. D. J., Bongers, I. L., van der Ende, J., &Verhulst, F. C. (2007). Developmental trajectories of depressive symptoms fromearly childhood to late adolescence: gender differences and adult outcome.Journal of Child Psychology and Psychiatry, and Allied Disciplines, 48, 657e666.
Delaveau, P., Jabourian, M., Lemogne, C., Guionnet, S., Bergouignan, L., & Fossati, P.(2011). Brain effects of antidepressants in major depression: a meta-analysis ofemotional processing studies. Journal of Affective Disorders, 130, 66e74.
Diener, C., Kuehner, C., Brusniak, W., Ubl, B., Wessa, M., & Flor, H. (2012). A meta-analysis of neurofunctional imaging studies of emotion and cognition in majordepression. NeuroImage, 61, 677e685.
Dillon, D. G., Rosso, I. M., Pechtel, P., Killgore, W. D. S., Rauch, S. L., & Pizzagalli, D. A.(2014). Peril and pleasure: an rdoc-inspired examination of threat responsesand reward processing in anxiety and depression. Depression and Anxiety, 31,233e249.
Downar, J., Geraci, J., Salomons, T. V., Dunlop, K., Wheeler, S., McAndrews, M. P., et al.(2013). Anhedonia and reward-circuit connectivity distinguish nonrespondersfrom responders to dorsomedial prefrontal repetitive transcranial magneticstimulation inmajor depression.Biological Psychiatry, 76(3),176e185, 2014Aug 1.
Doyle, O. M., De Simoni, S., Schwarz, A. J., Brittain, C., O'Daly, O. G., Williams, S. C. R.,et al. (2013). Quantifying the attenuation of the ketamine pharmacologicalmagnetic resonance imaging response in humans: a validation using antipsy-chotic and glutamatergic agents. The Journal of Pharmacology and ExperimentalTherapeutics, 345, 151e160.
Drevets, W. C. (1998). Functional neuroimaging studies of depression: the anatomyof melancholia. Annual Review of Medicine, 49, 341e361.
Dunlop, B. W., Binder, E. B., Cubells, J. F., Goodman, M. M., Kelley, M. E., Kinkead, B.,et al. (2012). Predictors of remission in depression to individual and combinedtreatments (PReDICT): study protocol for a randomized controlled trial. Trials,13, 106.
Fales, C. L., Barch, D. M., Rundle, M. M., Mintun, M. A., Mathews, J., Snyder, A. Z., et al.(2009). Antidepressant treatment normalizes hypoactivity in dorsolateral pre-frontal cortex during emotional interference processing in major depression.Journal of Affective Disorders, 112, 206e211.
Farah, M. J., & Gillihan, S. J. (2012). The puzzle of neuroimaging and psychiatricdiagnosis: technology and nosology in an evolving discipline. AJOB Neurosci-ence, 3, 31e41.
Fitzgerald, P. B., Laird, A. R., Maller, J., & Daskalakis, Z. J. (2008). A meta-analytic studyof changes in brain activation in depression.Human Brain Mapping, 29, 683e695.
Flint, J., & Kendler, K. S. (2014). The genetics of major depression. Neuron, 81,484e503.
Foland-Ross, L. C., & Gotlib, I. H. (2012). Cognitive and neural aspects of informationprocessing in major depressive disorder: an integrative perspective. Frontiers inPsychology, 3, 489.
Foland-Ross, L. C., Hamilton, J. P., Joormann, J., Berman, M. G., Jonides, J., &Gotlib, I. H. (2013). The neural basis of difficulties disengaging from negativeirrelevant material in major depression. Psychological Science, 24, 334e344.
Fond, G., Loundou, A., Rabu, C., Macgregor, A., Lançon, C., Brittner, M., et al. (2014).Ketamine administration in depressive disorders: a systematic review andmeta-analysis. Psychopharmacology. http://dx.doi.org/10.1007/s00213-014-3664-5.
Fried, E. I., Nesse, R. M., Zivin, K., Guille, C., & Sen, S. (2013). Depression is more thanthe sum score of its parts: individual DSM symptoms have different risk factors.Psychological Medicine, 1e10.
Fu, C. H. Y., & Costafreda, S. G. (2013). Neuroimaging-based biomarkers in psychi-atry: clinical opportunities of a paradigm shift. Canadian Journal of Psychiatry.Revue Canadienne de Psychiatrie, 58, 499e508.
Fu, C. H. Y., Steiner, H., & Costafreda, S. G. (2013). Predictive neural biomarkers ofclinical response in depression: a meta-analysis of functional and structuralneuroimaging studies of pharmacological and psychological therapies. Neuro-biology of Disease, 52, 75e83.
Fu, C. H. Y., Williams, S. C. R., Brammer, M. J., Suckling, J., Kim, J., Cleare, A. J., et al.(2007). Neural responses to happy facial expressions in major depressionfollowing antidepressant treatment. The American Journal of Psychiatry, 164,599e607.
Fu, C. H. Y., Williams, S. C. R., Cleare, A. J., Scott, J., Mitterschiffthaler, M. T.,Walsh, N. D., et al. (2008). Neural responses to sad facial expressions in majordepression following cognitive behavioral therapy. Biological Psychiatry, 64,505e512.
Furey, M. L., Drevets, W. C., Hoffman, E. M., Frankel, E., Speer, A. M., & Zarate, C. A., Jr.(2013). Potential of pretreatment neural activity in the visual cortex duringemotional processing to predict treatment response to scopolamine in majordepressive disorder. JAMA Psychiatry, 70, 280e290.
Goldapple, K., Segal, Z., Garson, C., Lau, M., Bieling, P., Kennedy, S., et al. (2004).Modulation of cortical-limbic pathways in major depression: treatment-specificeffects of cognitive behavior therapy. Archives of General Psychiatry, 61, 34e41.
Goodwin, R. D., & Gotlib, I. H. (2004). Gender differences in depression: the role ofpersonality factors. Psychiatry Research, 126, 135e142.

M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e73 71
Gotlib, I. H., Hamilton, J. P., Cooney, R. E., Singh, M. K., Henry, M. L., & Joormann, J.(2010). Neural processing of reward and loss in girls at risk for major depres-sion. Archives of General Psychiatry, 67, 380e387.
Gotlib, I. H., & Joormann, J. (2010). Cognition and depression: current status andfuture directions. Annual Review of Clinical Psychology, 6, 285e312.
Gotlib, I. H., Joormann, J., & Foland-Ross, L. C. (2014). Understanding familial risk fordepression: a 25-year perspective. Perspectives on Psychological Science, 9,94e108.
Gotlib, I. H., Joormann, J., Minor, K. L., & Hallmayer, J. (2008). HPA axis reactivity: amechanism underlying the associations among 5-HTTLPR, stress, and depres-sion. Biological Psychiatry, 63, 847e851.
Graham, J., Salimi-Khorshidi, G., Hagan, C., Walsh, N., Goodyer, I., Lennox, B., et al.(2013). Meta-analytic evidence for neuroimaging models of depression: state ortrait? Journal of Affective Disorders, 151, 423e431.
Greicius, M. D., Flores, B. H., Menon, V., Glover, G. H., Solvason, H. B., Kenna, H., et al.(2007). Resting-state functional connectivity in major depression: abnormallyincreased contributions from subgenual cingulate cortex and thalamus. Bio-logical Psychiatry, 62, 429e437.
Groenewold, N. A., Opmeer, E. M., de Jonge, P., Aleman, A., & Costafreda, S. G. (2013).Emotional valence modulates brain functional abnormalities in depression:evidence from a meta-analysis of fMRI studies. Neuroscience and BiobehavioralReviews, 37, 152e163.
Guo, W., Liu, F., Xue, Z., Gao, K., Liu, Z., Xiao, C., et al. (2013). Abnormal resting-statecerebellar-cerebral functional connectivity in treatment-resistant depressionand treatment sensitive depression. Progress In Neuro-Psychopharmacology &Biological Psychiatry, 44, 51e57.
Guo, W., Liu, F., Xue, Z., Gao, K., Wu, R., Ma, C., et al. (2012). Altered white matterintegrity in young adults with first-episode, treatment-naive, and treatment-responsive depression. Neuroscience Letters, 522, 139e144.
Hajek, T., Carrey, N., & Alda, M. (2005). Neuroanatomical abnormalities as riskfactors for bipolar disorder. Bipolar Disorders, 7, 393e403.
Hamilton, J. P., Chen, M. C., & Gotlib, I. H. (2013). Neural systems approaches tounderstanding major depressive disorder: an intrinsic functional organizationperspective. Neurobiology of Disease, 52, 4e11.
Hamilton, J. P., Etkin, A., Furman, D. J., Lemus, M. G., Johnson, R. F., & Gotlib, I. H.(2012). Functional neuroimaging of Major Depressive Disorder: a meta-analysisand new integration of baseline activation and neural response data. AmericanJournal of Psychiatry, 169, 693e703.
Hamilton, J. P., Siemer, M., & Gotlib, I. H. (2008). Amygdala volume in majordepressive disorder: a meta-analysis of magnetic resonance imaging studies.Molecular Psychiatry, 13, 993e1000.
Hayley, S., & Litteljohn, D. (2013). Neuroplasticity and the next wave of antide-pressant strategies. Frontiers in Cellular Neuroscience, 7, 218.
Hirschfeld, R. M. A. (2012). The epidemiology of depression and the evolution oftreatment. The Journal of Clinical Psychiatry, 73(Suppl. 1), 5e9.
Huang, H., Fan, X., Williamson, D. E., & Rao, U. (2011). White matter changes inhealthy adolescents at familial risk for unipolar depression: a diffusion tensorimaging study. Neuropsychopharmacology: Official Publication of the AmericanCollege of Neuropsychopharmacology, 36, 684e691.
Joormann, J., Cooney, R. E., Henry, M. L., & Gotlib, I. H. (2012). Neural correlates ofautomatic mood regulation in girls at high risk for depression. Journal ofAbnormal Psychology, 121, 61e72.
Joormann, J., Gilbert, K., & Gotlib, I. H. (2010). Emotion identification in girls at highrisk for depression. Journal of Child Psychology and Psychiatry, and Allied Disci-plines, 51, 575e582.
Joormann, J., Talbot, L., & Gotlib, I. H. (2007). Biased processing of emotional in-formation in girls at risk for depression. Journal of Abnormal Psychology, 116,135e143.
Kanske, P., Heissler, J., Sch€onfelder, S., &Wessa,M. (2012). Neural correlates of emotionregulation deficits in remitted depression: the influence of regulation strategy,habitual regulation use, and emotional valence. NeuroImage, 61, 686e693.
Kellner, C. H., Kaicher, D. C., Banerjee, H., Knapp, R. G., Shapiro, R. J., Briggs, M. C.,et al. (2014). Depression severity in Electroconvulsive Therapy (ECT) versuspharmacotherapy trials. The Journal of ECT. http://dx.doi.org/10.1097/YCT.0000000000000135.
Kempton, M. J., Salvador, Z., Munaf�o, M. R., Geddes, J. R., Simmons, A., Frangou, S.,et al. (2011). Structural neuroimaging studies in major depressive disorder.Meta-analysis and comparison with bipolar disorder. Archives of General Psy-chiatry, 68, 675e690.
Kennedy, S. H., & Giacobbe, P. (2007). Treatment resistant depression e advances insomatic therapies. Annals of Clinical Psychiatry: Official Journal of the AmericanAcademy of Clinical Psychiatrists, 19, 279e287.
Kennedy, S. H., Javanmard, M., & Vaccarino, F. J. (1997). A review of functionalneuroimaging in mood disorders: positron emission tomography and depres-sion. Canadian Journal of Psychiatry. Revue Canadienne De Psychiatrie, 42,467e475.
Kennedy, S. H., Konarski, J. Z., Segal, Z. V., Lau, M. A., Bieling, P. J., McIntyre, R. S.,et al. (2007). Differences in brain glucose metabolism between responders toCBT and venlafaxine in a 16-week randomized controlled trial. The AmericanJournal of Psychiatry, 164, 778e788.
Kerestes, R., Davey, C. G., Stephanou, K., Whittle, S., & Harrison, B. J. (2013). Func-tional brain imaging studies of youth depression: a systematic review. Neuro-Image: Clinical, 4, 209e231.
Kerestes, R., Ladouceur, C. D., Meda, S., Nathan, P. J., Blumberg, H. P., Maloney, K.,et al. (2012). Abnormal prefrontal activity subserving attentional control of
emotion in remitted depressed patients during a working memory task withemotional distracters. Psychological Medicine, 42, 29e40.
Klein, D. N., Glenn, C. R., Kosty, D. B., Seeley, J. R., Rohde, P., & Lewinsohn, P. M.(2013). Predictors of first lifetime onset of major depressive disorder in youngadulthood. Journal of Abnormal Psychology, 122, 1e6.
Kong, L., Wu, F., Tang, Y., Ren, L., Kong, D., Liu, Y., et al. (2014). Frontal-subcorticalvolumetric deficits in single episode, medication-naïve depressed patients andthe effects of 8 weeks fluoxetine treatment: a VBM-DARTEL study. PloS One, 9,e79055.
Koolschijn, P. C. M. P., van Haren, N. E. M., Lensvelt-Mulders, G. J. L. M., HulshoffPol, H. E., & Kahn, R. S. (2009). Brain volume abnormalities in major depressivedisorder: a meta-analysis of magnetic resonance imaging studies. Human BrainMapping, 30, 3719e3735.
Korb, A. S., Hunter, A. M., Cook, I. A., & Leuchter, A. F. (2011). Rostral anteriorcingulate cortex activity and early symptom improvement during treatment formajor depressive disorder. Psychiatry Research, 192, 188e194.
Korgaonkar, M. S., Grieve, S. M., Etkin, A., Koslow, S. H., & Williams, L. M. (2013).Using standardized fMRI protocols to identify patterns of prefrontal circuitdysregulation that are common and specific to cognitive and emotional tasks inmajor depressive disorder: first wave results from the iSPOT-D study. Neuro-psychopharmacology, 38, 863e871.
Kühn, S., Vanderhasselt, M.-A., De Raedt, R., & Gallinat, J. (2012). Why ruminatorswon't stop: the structural and resting state correlates of rumination and itsrelation to depression. Journal of Affective Disorders, 141, 352e360.
Lai, C. H. (2014). Patterns of cortico-limbic activations during visual processing ofsad faces in depression patients: a coordinate-based meta-analysis. The Journalof Neuropsychiatry and Clinical Neurosciences, 26, 34e43.
Langenecker, S. A., Kennedy, S. E., Guidotti, L. M., Briceno, E. M., Own, L. S., Hooven, T.,et al. (2007). Frontal and limbic activation during inhibitory control predictstreatment response in major depressive disorder. Biological Psychiatry, 62,1272e1280.
Lewinsohn, P. M., Allen, N. B., Seeley, J. R., & Gotlib, I. H. (1999). First onset versusrecurrence of depression: differential processes of psychosocial risk. Journal ofAbnormal Psychology, 108, 483e489.
Li, C. T., Lin, C. P., Chou, K. H., Chen, I. Y., Hsieh, J. C., Wu, C. L., et al. (2010). Structuraland cognitive deficits in remitting and non-remitting recurrent depression: avoxel-based morphometric study. NeuroImage, 50, 347e356.
Liao, Y., Huang, X., Wu, Q., Yang, C., Kuang, W., Du, M., et al. (2013). Isdepression a disconnection syndrome? Meta-analysis of diffusion tensorimaging studies in patients with MDD. Journal of Psychiatry & Neuroscience,38, 49e56.
Lisiecka, D., Meisenzahl, E., Scheuerecker, J., Schoepf, V., Whitty, P., Chaney, A., et al.(2011). Neural correlates of treatment outcome in major depression. The In-ternational Journal of Neuropsychopharmacology, 14, 521e534.
Liston, C., Chen, A. C., Zebley, B. D., Drysdale, A. T., Gordon, R., Leuchter, B., et al.(2014). Default mode network mechanisms of transcranial magnetic stimula-tion in depression. Biological Psychiatry. http://dx.doi.org/10.1016/j.biopsych.2014.01.023.
Liu, F., Guo, W., Yu, D., Gao, Q., Gao, K., Xue, Z., et al. (2012). Classification of differenttherapeutic responses of major depressive disorder with multivariate patternanalysis method based on structural MR scans. PloS One, 7, e40968.
Liu, C. H., Jing, B., Ma, X., Xu, P. F., Zhang, Y., Li, F., et al. (2014). Voxel-basedmorphometry study of the insular cortex in female patients with current andremitted depression. Neuroscience, 262, 190e199.
Lyden, H., Espinoza, R. T., Pirnia, T., Clark, K., Joshi, S. H., Leaver, A. M., et al. (2014).Electroconvulsive therapy mediates neuroplasticity of white matter micro-structure in major depression. Translational Psychiatry, 4, e380.
MacQueen, G. M., Yucel, K., Taylor, V. H., Macdonald, K., & Joffe, R. (2008). Posteriorhippocampal volumes are associated with remission rates in patients withmajor depressive disorder. Biological Psychiatry, 64, 880e883.
Malykhin, N. V., Carter, R., Seres, P., & Coupland, N. J. (2010). Structural changes inthe hippocampus in major depressive disorder: contributions of disease andtreatment. Journal of Psychiatry & Neuroscience, 35, 337e343.
Marchetti, I., Koster, E. H. W., Sonuga-Barke, E. J., & De Raedt, R. (2012). The defaultmode network and recurrent depression: a neurobiological model of cognitiverisk factors. Neuropsychology Review, 22, 229e251.
Mayberg, H. S., Lozano, A. M., Voon, V., McNeely, H. E., Seminowicz, D., Hamani, C.,et al. (2005). Deep brain stimulation for treatment-resistant depression. Neuron,45, 651e660.
McGirr, A., Berlim, M. T., Bond, D. J., Fleck, M. P., Yatham, L. N., & Lam, R. W. (2014).A systematic review and meta-analysis of randomized, double-blind, placebo-controlled trials of ketamine in the rapid treatment of major depressive epi-sodes. Psychological Medicine, 1e12.
McGrath, C. L., Kelley, M. E., Holtzheimer, P. E., Dunlop, B. W., Craighead, W. E.,Franco, A. R., et al. (2013). Toward a neuroimaging treatment selectionbiomarker for major depressive disorder. JAMA Psychiatry, 70, 821e829.
McKinnon, M. C., Yucel, K., Nazarov, A., & MacQueen, G. M. (2009). A meta-analysisexamining clinical predictors of hippocampal volume in patients with majordepressive disorder. Journal of Psychiatry & Neuroscience, 34, 41e54.
Meng, C., Brandl, F., Tahmasian, M., Shao, J., Manoliu, A., Scherr, M., et al. (2014).Aberrant topology of striatum's connectivity is associated with the number ofepisodes in depression. Brain, 137, 598e609.
Miller, J. M., Oquendo, M. A., Ogden, R. T., Mann, J. J., & Parsey, R. V. (2008). Serotonintransporter binding as a possible predictor of one-year remission in majordepressive disorder. Journal of Psychiatric Research, 42, 1137e1144.

M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e7372
Miller, J. M., Schneck, N., Siegle, G. J., Chen, Y., Ogden, R. T., Kikuchi, T., et al. (2013).fMRI response to negative words and SSRI treatment outcome in majordepressive disorder: a preliminary study. Psychiatry Research, 214, 296e305.
Mills, N. T., Scott, J. G., Wray, N. R., Cohen-Woods, S., & Baune, B. T. (2013). Researchreview: the role of cytokines in depression in adolescents: a systematic review.Journal of Child Psychology and Psychiatry, 54, 816e835.
Milne, A. M. B., MacQueen, G. M., & Hall, G. B. C. (2012). Abnormal hippocampalactivation in patients with extensive history of major depression: an fMRI study.Journal of Psychiatry & Neuroscience: JPN, 37, 28e36.
Monk, C. S., Klein, R. G., Telzer, E. H., Schroth, E. A., Mannuzza, S., Moulton, J. L., 3rd,et al. (2008). Amygdala and nucleus accumbens activation to emotional facialexpressions in children and adolescents at risk for major depression. TheAmerican Journal of Psychiatry, 165, 90e98.
Moresco, R. M., Matarrese, M., & Fazio, F. (2006). PET and SPET molecular imaging:focus on serotonin system. Current Topics in Medicinal Chemistry, 6, 2027e2034.
Moussavi, S., Chatterji, S., Verdes, E., Tandon, A., Patel, V., & Ustun, B. (2007).Depression, chronic diseases, and decrements in health: results from the WorldHealth Surveys. Lancet, 370, 851e858.
Moylan, S., Maes, M., Wray, N. R., & Berk, M. (2013). The neuroprogressive nature ofmajor depressive disorder: pathways to disease evolution and resistance, andtherapeutic implications. Molecular Psychiatry, 18, 595e606.
Nejad, A. B., Fossati, P., & Lemogne, C. (2013). Self-referential processing, rumina-tion, and cortical midline structures in major depression. Frontiers in HumanNeuroscience, 7, 666.
Niciu, M. J., Mathews, D. C., Nugent, A. C., Ionescu, D. F., Furey, M. L., Richards, E. M.,et al. (2013). Developing biomarkers in mood disorders research through theuse of rapid-acting antidepressants. Depression and Anxiety, 31, 297e307.
Norbury, R., Godlewska, B., & Cowen, P. J. (2013). When less is more: a functionalmagnetic resonance imaging study of verbal working memory in remitteddepressed patients. Psychological Medicine, 1e7.
Northoff, G., Wiebking, C., Feinberg, T., & Panksepp, J. (2011). The “resting-statehypothesis” of major depressive disorder e a translational subcortical-corticalframework for a system disorder. Neuroscience and biobehavioral reviews, 35,1929e1945.
Pascual-Leone, A., Tormos, J. M., Keenan, J., Tarazona, F., Ca~nete, C., & Catal�a, M. D.(1998). Study and modulation of human cortical excitability with transcranialmagnetic stimulation. Journal of Clinical Neurophysiology: Official Publication ofthe American Electroencephalographic Society, 15, 333e343.
Perlis, R. H. (2014). Pharmacogenomic testing and personalized treatment ofdepression. Clinical Chemistry, 60, 53e59.
Peterson, B. S., Warner, V., Bansal, R., Zhu, H., Hao, X., Liu, J., et al. (2009). Corticalthinning in persons at increased familial risk for major depression. Proceedingsof the National Academy of Sciences of the United States of America, 106,6273e6278.
Rive, M. M., van Rooijen, G., Veltman, D. J., Phillips, M. L., Schene, A. H., & Ruh�e, H. G.(2013). Neural correlates of dysfunctional emotion regulation in majordepressive disorder. A systematic review of neuroimaging studies. Neuroscienceand Biobehavioral Reviews, 37, 2529e2553.
Rizvi, S. J., Salomons, T. V., Konarski, J. Z., Downar, J., Giacobbe, P., McIntyre, R. S.,et al. (2013). Neural response to emotional stimuli associated with successfulantidepressant treatment and behavioral activation. Journal of Affective Disor-ders, 151, 573e581.
Rosenblau, G., Sterzer, P., Stoy, M., Park, S., Friedel, E., Heinz, A., et al. (2012).Functional neuroanatomy of emotion processing in major depressive disorder isaltered after successful antidepressant therapy. Journal of Psychopharmacology,26, 1424e1433.
Sacher, J., Neumann, J., Fünfstück, T., Soliman, A., Villringer, A., & Schroeter, M. L.(2012). Mapping the depressed brain: a meta-analysis of structural and func-tional alterations in major depressive disorder. Journal of Affective Disorders, 140,142e148.
Salvadore, G., Cornwell, B. R., Sambataro, F., Latov, D., Colon-Rosario, V., Carver, F.,et al. (2010). Anterior cingulate desynchronization and functional connectivitywith the amygdala during a working memory task predict rapid antidepressantresponse to ketamine. Neuropsychopharmacology: Official Publication of theAmerican College of Neuropsychopharmacology, 35, 1415e1422.
Salvadore, G., Nugent, A. C., Lemaitre, H., Luckenbaugh, D. A., Tinsley, R.,Cannon, D. M., et al. (2011). Prefrontal cortical abnormalities in currentlydepressed versus currently remitted patients with major depressive disorder.NeuroImage, 54, 2643e2651.
Sambataro, F., Wolf, N. D., Pennuto, M., Vasic, N., & Wolf, R. C. (2013). Revisitingdefault mode network function in major depression: evidence for disruptedsubsystem connectivity. Psychological Medicine, 1e11.
Samson, A. C., Meisenzahl, E., Scheuerecker, J., Rose, E., Schoepf, V., Wiesmann, M.,et al. (2011). Brain activation predicts treatment improvement in patients withmajor depressive disorder. Journal of Psychiatric Research, 45, 1214e1222.
Sato, S., & Yeh, T. L. (2013). Challenges in treating patients with major depressivedisorder: the impact of biological and social factors. CNS Drugs, 27(Suppl. 1),S5eS10.
Schlaepfer, T. E., & Bewernick, B. H. (2014). Neuromodulation for treatment resistantdepression: state of the art and recommendations for clinical and scientificconduct. Brain Topography, 27, 12e19.
Shanahan, L., Copeland, W. E., Costello, E. J., & Angold, A. (2011). Child-, adolescent-and young adult-onset depressions: differential risk factors in development?Psychological Medicine, 41, 2265e2274.
Sharp, C., Kim, S., Herman, L., Pane, H., Reuter, T., & Strathearn, L. (2014). Majordepression in mothers predicts reduced ventral striatum activation in adoles-cent female offspring with and without depression. Journal of Abnormal Psy-chology, 123, 298e309.
Sheline, Y. I., Gado, M. H., & Kraemer, H. C. (2003). Untreated depression and hip-pocampal volume loss. The American Journal of Psychiatry, 160, 1516e1518.
Sheline, Y. I., Price, J. L., Yan, Z., & Mintun, M. A. (2010). Resting-state functional MRIin depression unmasks increased connectivity between networks via the dorsalnexus. Proceedings of the National Academy of Sciences of the United States ofAmerica, 107, 11020e11025.
Siegle, G. J., Carter, C. S., & Thase, M. E. (2006). Use of FMRI to predict recovery fromunipolar depression with cognitive behavior therapy. The American Journal ofPsychiatry, 163, 735e738.
Singh, M. K., Kesler, S. R., Hadi Hosseini, S. M., Kelley, R. G., Amatya, D.,Hamilton, J. P., et al. (2013). Anomalous gray matter structural networks inmajor depressive disorder. Biological Psychiatry, 74, 777e785.
Sneed, J. R., Culang-Reinlieb, M. E., Brickman, A. M., Gunning-Dixon, F. M.,Johnert, L., Garcon, E., et al. (2011). MRI signal hyperintensities and failure toremit following antidepressant treatment. Journal of Affective Disorders,135(1e3), 315e320.
Sperduti, M., Martinelli, P., Kalenzaga, S., Devauchelle, A.-D., Lion, S., Malherbe, C.,et al. (2013). Don't be too strict with yourself! Rigid negative self-representationin healthy subjects mimics the neurocognitive profile of depression for auto-biographical memory. Frontiers in Behavioral Neuroscience, 7, 41.
Steele, J. D., Christmas, D., Eljamel, M. S., & Matthews, K. (2008). Anterior cingu-lotomy for major depression: clinical outcome and relationship to lesioncharacteristics. Biological Psychiatry, 63, 670e677.
Steele, J. D., Currie, J., Lawrie, S. M., & Reid, I. (2007). Prefrontal cortical functionalabnormality in major depressive disorder: a stereotactic meta-analysis. Journalof Affective Disorders, 101, 1e11.
Stoy, M., Schlagenhauf, F., Sterzer, P., Bermpohl, F., H€agele, C., Suchotzki, K., et al.(2012). Hyporeactivity of ventral striatum towards incentive stimuli in un-medicated depressed patients normalizes after treatment with escitalopram.Journal of Psychopharmacology, 26, 677e688.
Stuhrmann, A., Suslow, T., & Dannlowski, U. (2011). Facial emotion processing inmajor depression: a systematic review of neuroimaging findings. Biology ofMood & Anxiety Disorders, 1, 10.
Suzuki, H., Botteron, K. N., Luby, J. L., Belden, A. C., Gaffrey, M. S., Babb, C. M., et al.(2013). Structural-functional correlations between hippocampal volume andcortico-limbic emotional responses in depressed children. Cognitive, Affective &Behavioral Neuroscience, 13, 135e151.
Tahmasian, M., Knight, D. C., Manoliu, A., Schwerth€offer, D., Scherr, M., Meng, C.,et al. (2013). Aberrant intrinsic connectivity of hippocampus and amygdalaoverlap in the fronto-insular and dorsomedial-prefrontal cortex in majordepressive disorder. Frontiers in Human Neuroscience, 7, 639.
Takahashi, T., Yücel, M., Lorenzetti, V., Tanino, R., Whittle, S., Suzuki, M., et al. (2010).Volumetric MRI study of the insular cortex in individuals with current and pastmajor depression. Journal of Affective Disorders, 121, 231e238.
Tao, R., Calley, C. S., Hart, J., Mayes, T. L., Nakonezny, P. A., Lu, H., et al. (2012). Brainactivity in adolescent major depressive disorder before and after fluoxetinetreatment. The American Journal of Psychiatry, 169, 381e388.
Tham, M. W., Woon, P. S., Sum, M. Y., Lee, T.-S., & Sim, K. (2011). White matterabnormalities in major depression: evidence from post-mortem, neuroimagingand genetic studies. Journal of Affective Disorders, 132, 26e36.
Thompson, P. M., Giedd, J. N., Woods, R. P., MacDonald, D., Evans, A. C., & Toga, A. W.(2000). Growth patterns in the developing brain detected by using continuummechanical tensor maps. Nature, 404, 190e193.
US Burden of Disease Collaborators. (2013). The state of US health, 1990e2010:burden of diseases, injuries, and risk factors. Journal of the American MedicalAssociation, 310, 591e608.
Van Eijndhoven, P., van Wingen, G., Katzenbauer, M., Groen, W., Tepest, R.,Fern�andez, G., et al. (2013). Paralimbic cortical thickness in first-episodedepression: evidence for trait-related differences in mood regulation. TheAmerican Journal of Psychiatry, 170, 1477e1486.
Van Tol, M.-J., Li, M., Metzger, C. D., Hailla, N., Horn, D. I., Li, W., et al. (2013). Localcortical thinning links to resting-state disconnectivity in major depressivedisorder. Psychological Medicine, 1e13.
Van Wingen, G. A., van Eijndhoven, P., Cremers, H. R., Tendolkar, I., Verkes, R. J.,Buitelaar, J. K., et al. (2010). Neural state and trait bases of mood-incongruentmemory formation and retrieval in first-episode major depression. Journal ofPsychiatric Research, 44, 527e534.
Vasic, N., Walter, H., H€ose, A., & Wolf, R. C. (2008). Gray matter reduction associatedwith psychopathology and cognitive dysfunction in unipolar depression: avoxel-based morphometry study. Journal of Affective Disorders, 109, 107e116.
Victor, T. A., Furey, M. L., Fromm, S. J., Ohman, A., & Drevets, W. C. (2010). Rela-tionship between amygdala responses to masked faces and mood state andtreatment in major depressive disorder. Archives of General Psychiatry, 67,1128e1138.
Victor, T. A., Furey, M. L., Fromm, S. J., €Ohman, A., & Drevets, W. C. (2013). Changes inthe neural correlates of implicit emotional face processing during antidepres-sant treatment in major depressive disorder. The International Journal of Neu-ropsychopharmacology, 16, 2195e2208.
Videbech, P., & Ravnkilde, B. (2004). Hippocampal volume and depression: a meta-analysis of MRI studies. The American Journal of Psychiatry, 161, 1957e1966.

M.K. Singh, I.H. Gotlib / Behaviour Research and Therapy 62 (2014) 60e73 73
Villanueva, R. (2013). Neurobiology of major depressive disorder. Neural Plasticity,2013, 873278.
Vrieze, E., Demyttenaere, K., Bruffaerts, R., Hermans, D., Pizzagalli, D. A., Sienaert, P.,et al. (2014). Dimensions in major depressive disorder and their relevance fortreatment outcome. Journal of Affective Disorders, 155, 35e41.
Vythilingam, M., Vermetten, E., Anderson, G. M., Luckenbaugh, D., Anderson, E. R.,Snow, J., et al. (2004). Hippocampal volume,memory, and cortisol status inmajordepressive disorder: effects of treatment. Biological Psychiatry, 56, 101e112.
Wagner, G., Koch, K., Schachtzabel, C., Peikert, G., Schultz, C. C., Reichenbach, J. R.,et al. (2013). Self-referential processing influences functional activation duringcognitive control: an fMRI study. Social Cognitive and Affective Neuroscience, 8,828e837.
Wagner, G., Koch, K., Schachtzabel, C., Sobanski, T., Reichenbach, J. R., Sauer, H., et al.(2010). Differential effects of serotonergic and noradrenergic antidepressantson brain activity during a cognitive control task and neurofunctional predictionof treatment outcome in patients with depression. Journal of Psychiatry &Neuroscience, 35, 247e257.
Walsh, N. D., Williams, S. C. R., Brammer, M. J., Bullmore, E. T., Kim, J., Suckling, J.,et al. (2007). A longitudinal functional magnetic resonance imaging study ofverbal working memory in depression after antidepressant therapy. BiologicalPsychiatry, 62, 1236e1243.
Wang, T., Huang, X., Huang, P., Li, D., Lv, F., Zhang, Y., et al. (2013). Early-stagepsychotherapy produces elevated frontal white matter integrity in adult majordepressive disorder. PloS One, 8, e63081.
Wang, L., Li, K., Zhang, Q., Zeng, Y., Dai, W., Su, Y., et al. (2013). Short-term effects ofescitalopram on regional brain function in first-episode drug-naive patientswith major depressive disorder assessed by resting-state functional magneticresonance imaging. Psychological Medicine, 44, 1417e1426.
Wang, L., Li, K., Zhang, Q. E., Zeng, Y. W., Jin, Z., Dai, W. J., et al. (2013). Interhemi-spheric functional connectivity and its relationships with clinical characteristicsin major depressive disorder: a resting state fMRI study. PloS One, 8, e60191.
Watson, L. A., Berntsen, D., Kuyken, W., & Watkins, E. R. (2013). Involuntary andvoluntary autobiographical memory specificity as a function of depression.Journal of Behavior Therapy and Experimental Psychiatry, 44, 7e13.
Zeng, L. L., Shen, H., Liu, L., & Hu, D. (2013). Unsupervised classification of majordepressionusing functionalconnectivityMRI.HumanBrainMapping,35,1630e1641.
Zhang, W. N., Chang, S. H., Guo, L. Y., Zhang, K. L., & Wang, J. (2013). The neuralcorrelates of reward-related processing in major depressive disorder: a meta-analysis of functional magnetic resonance imaging studies. Journal of AffectiveDisorders, 151, 531e539.