Embed Size (px)
Citation preview

The neck is not designed to be a weight-bearing part of the body.
The neck is not designed to be a weight-bearing part of the body.
IT IS IN THE SPORT
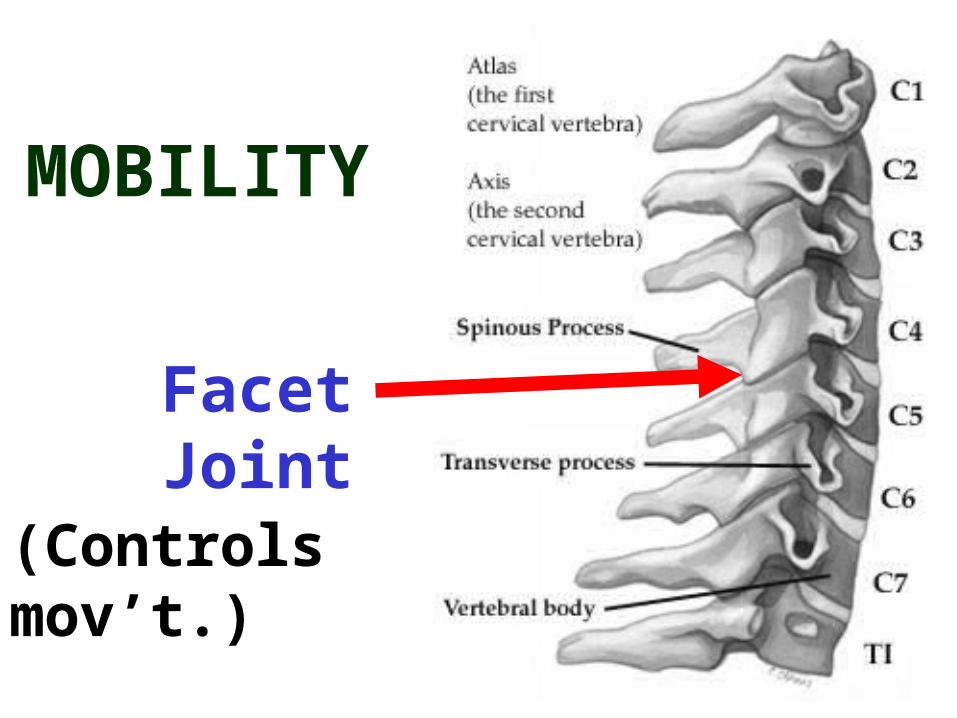
MOBILITY
Facet Joint
(Controls mov’t.)
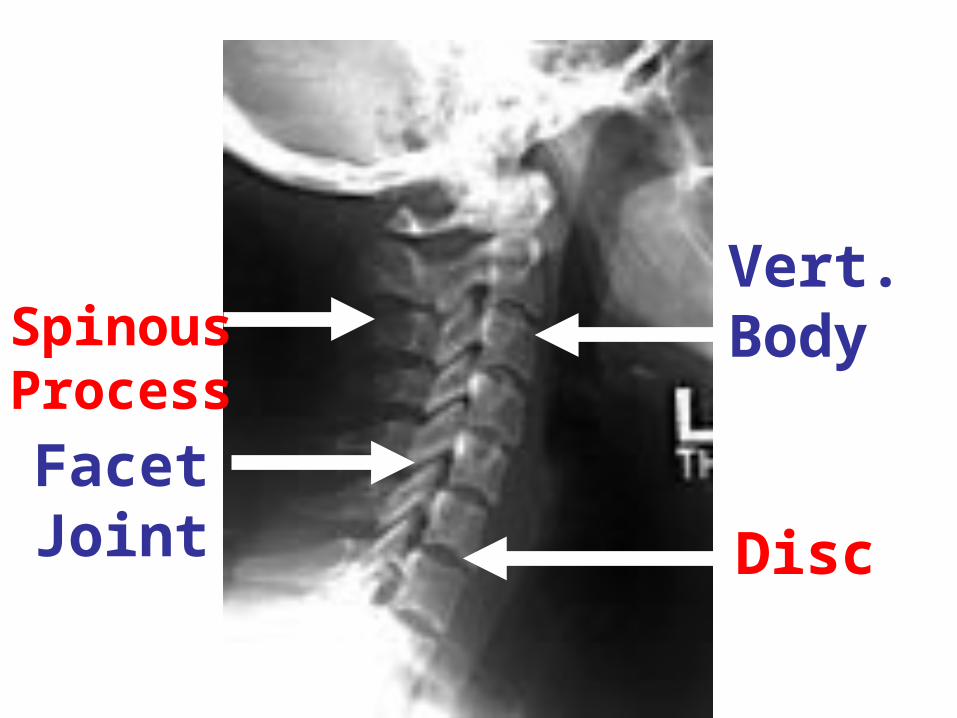
Spinous ProcessFacet Joint
Vert. Body
Disc
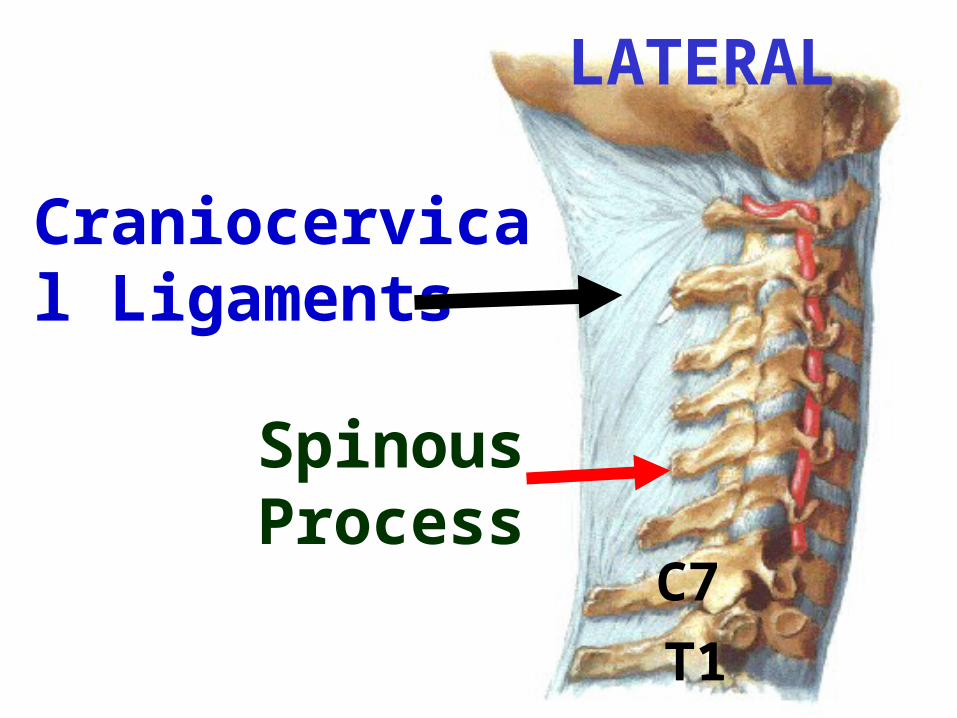
LATERAL
C7
T1
Craniocervical Ligaments
Spinous Process
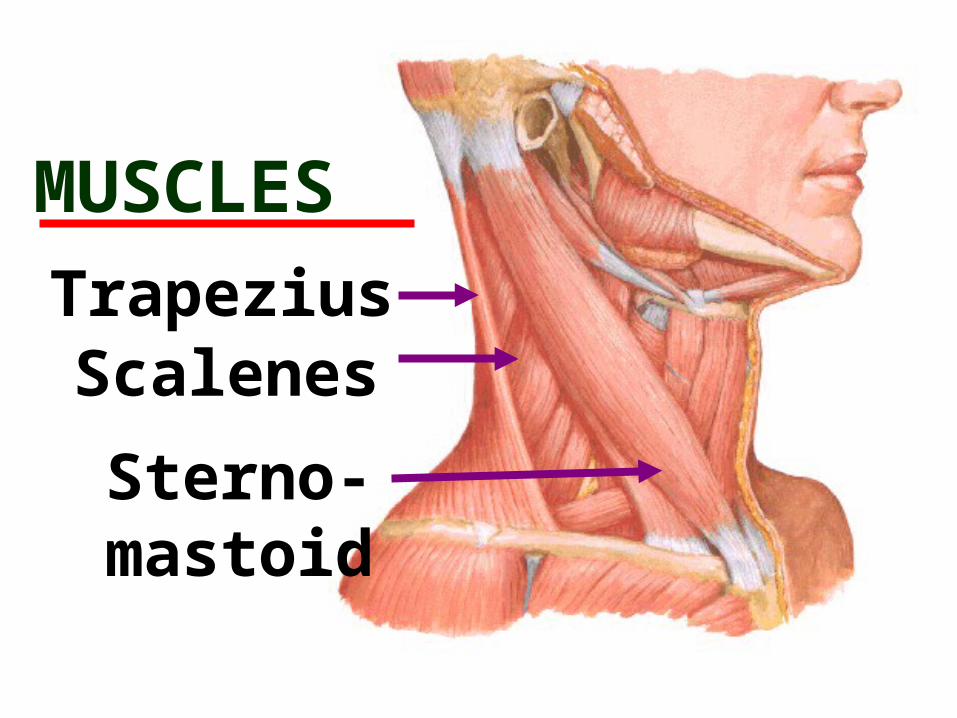
MUSCLESTrapeziusScalenes
Sterno-mastoid
TYPES OF NECK INJURIES
• Strains
• Sprains
• Fractures/ Disloc.
• Nerve
MECHANISMS OF CERVICAL
INJURY
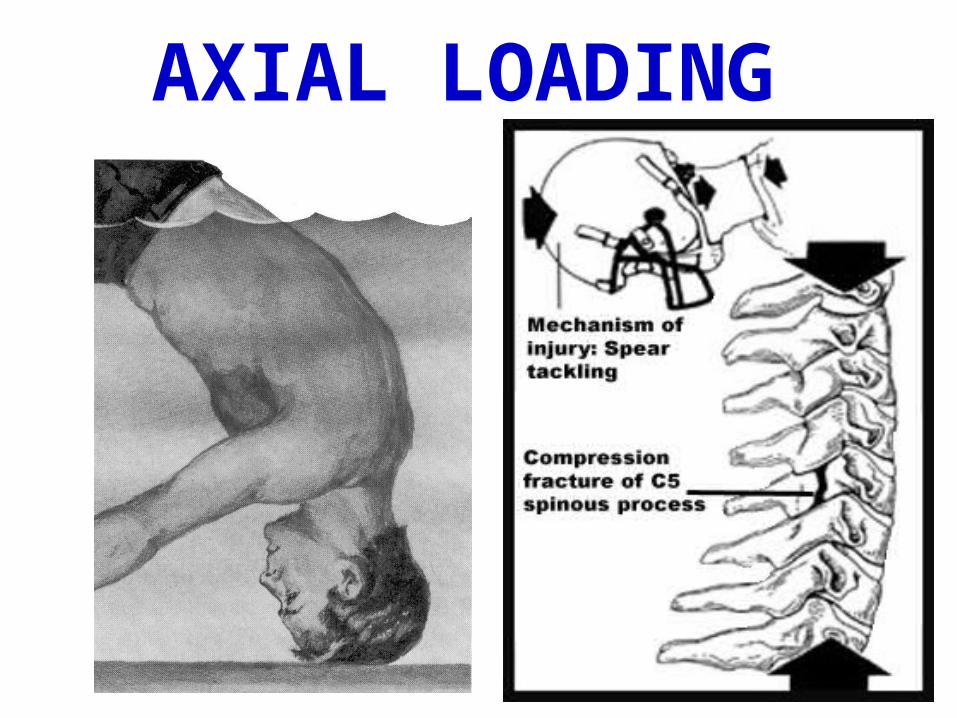
AXIAL LOADING
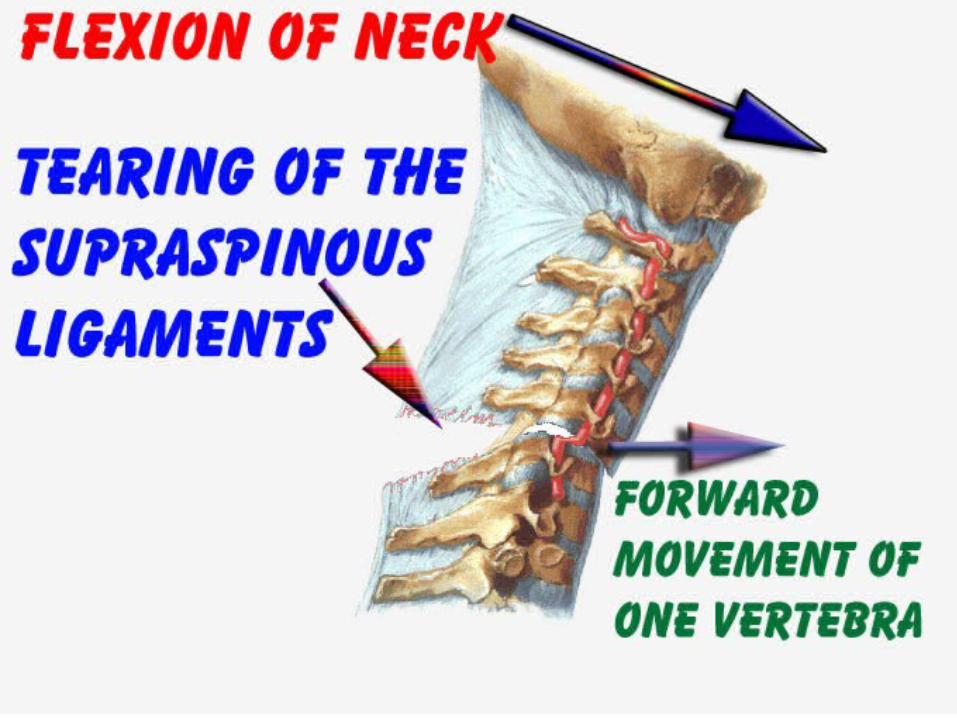
FLEXION
FLEXION AND ROTATION(Most fractures)
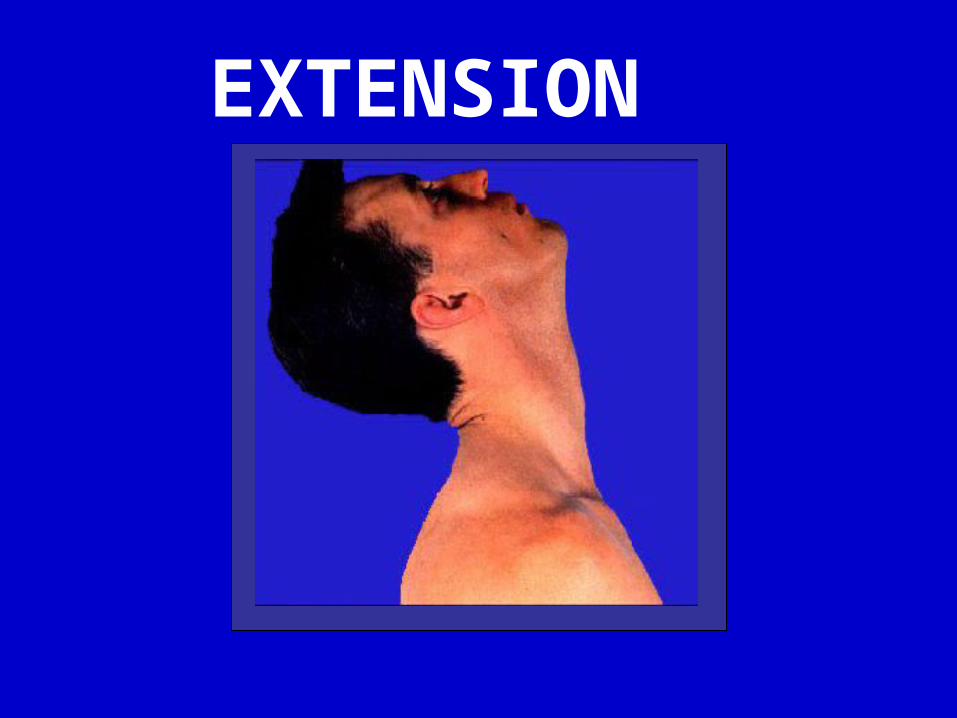
EXTENSION

IN

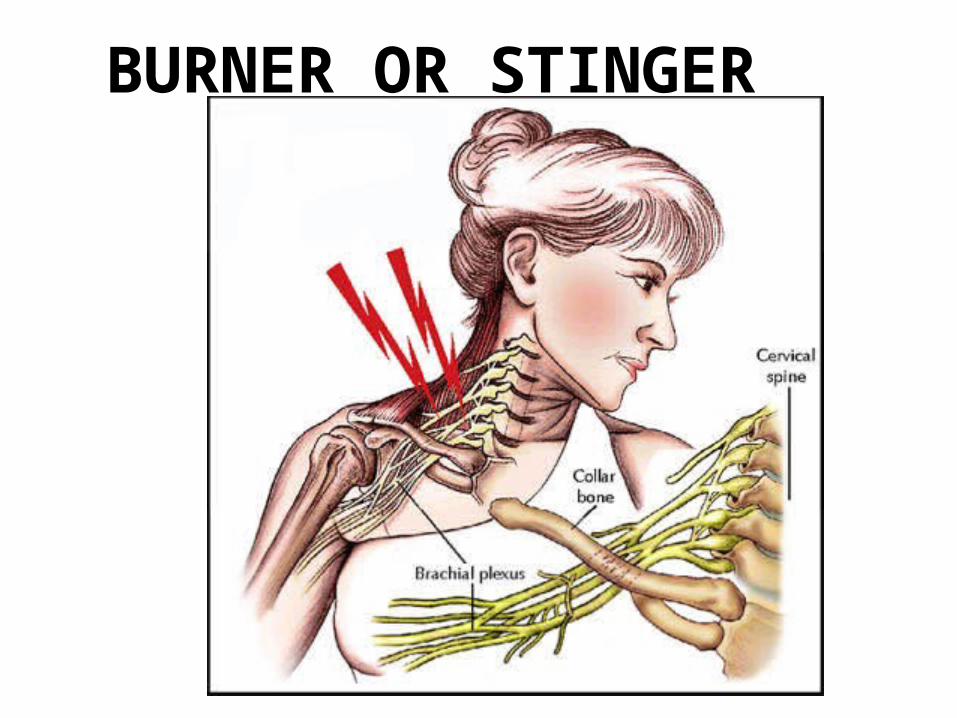
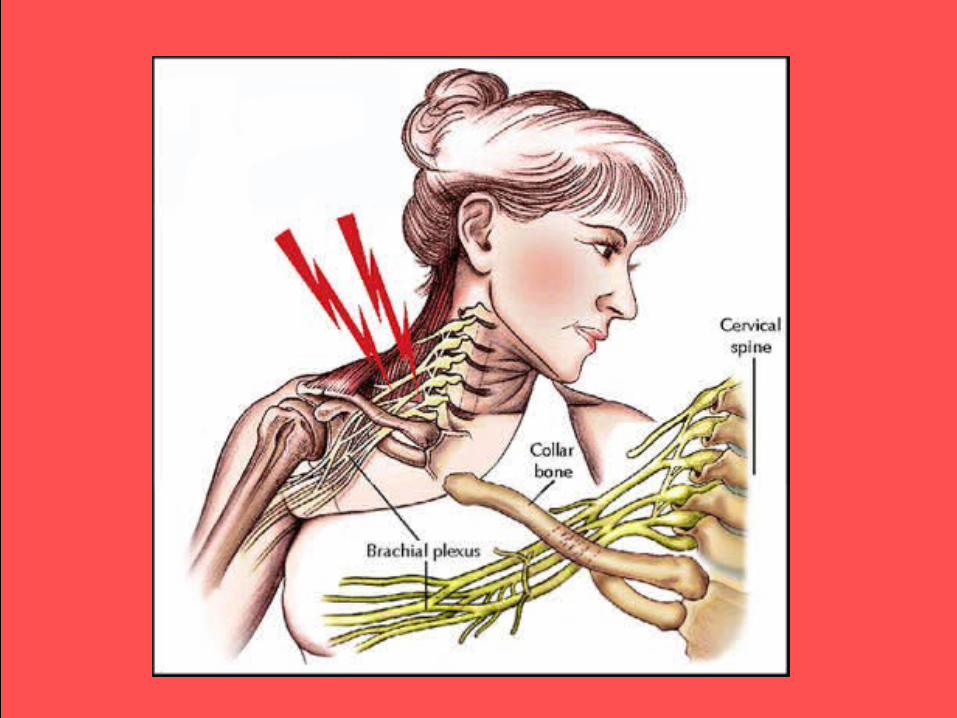
BURNER OR STINGER
MECHANISM OF INJURY
Head tilted away.
Head rotated away.
Shoulder depressed.
Posture of the arm after a burner. Pain is burning and it radiates down to the arm. Tenderness on Brachial Plexus
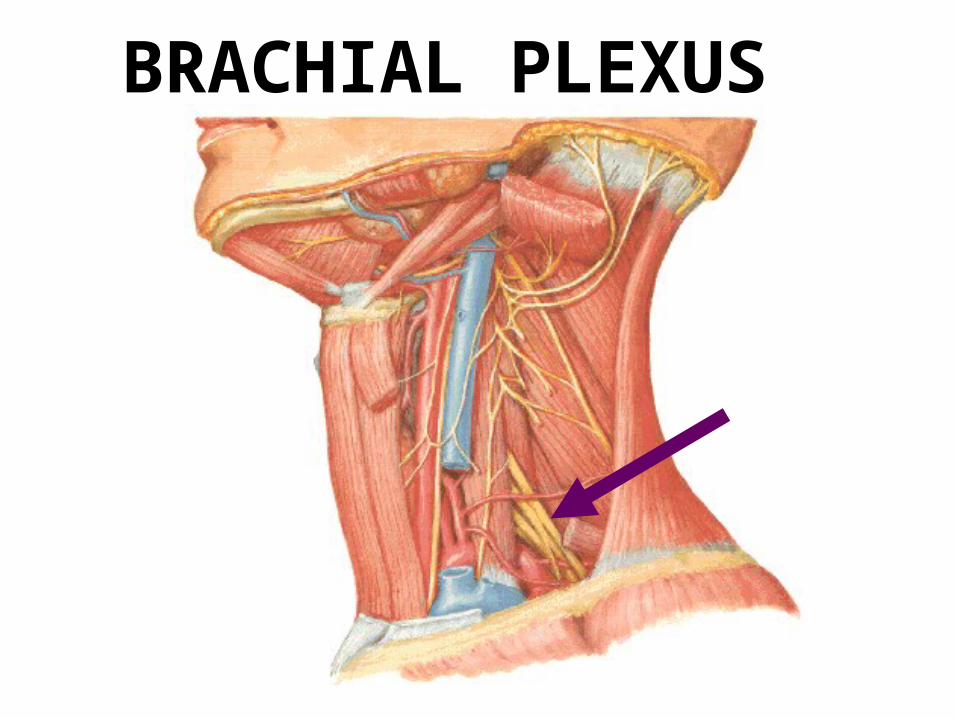
BRACHIAL PLEXUS
PINCHED NERVE
Mechanism of Injury (M.O.I.) ….
Axial loading to the extended, side-flexed neck.
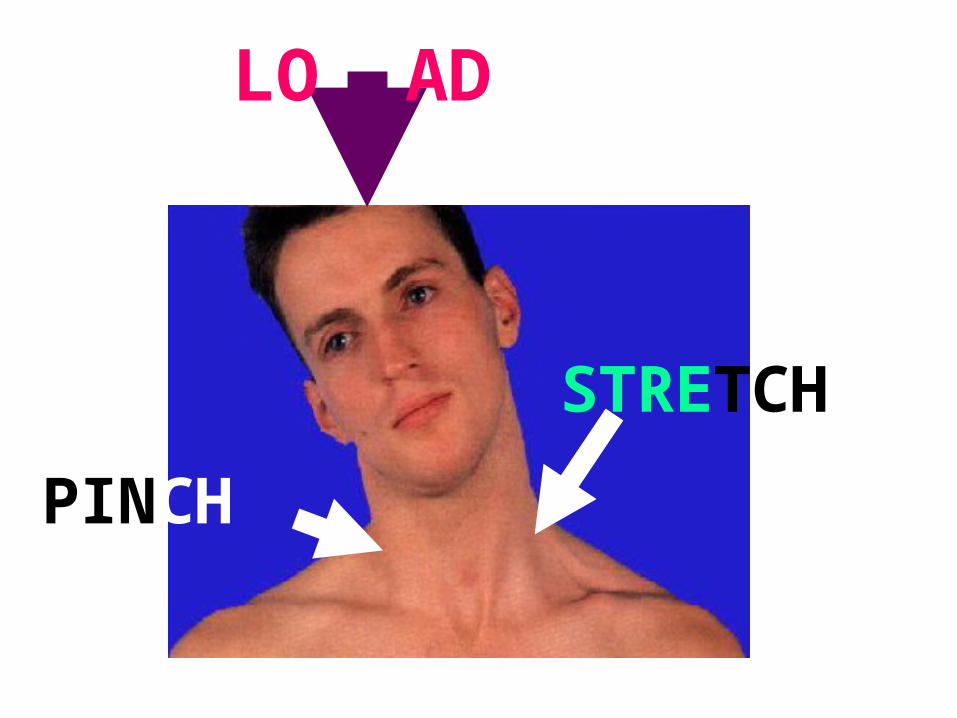
LO AD
STRETCH
PINCH
ASSESSMENT OF THE HEAD-NECK
INJURED ATHLETE ON THE PLAYING
SURFACE
NEUROLOGICAL SIGNS
Disruption of nerve functionWeakness
Reduced Sensation
Reduced Reflexes
Muscle Atrophy

PAIN IS NOT A
NEUROLOGICAL
SIGN!!!!!
NerveCover
Touching Nerve

FIELD APPROACH
TO
THE INJURED ATHLETE

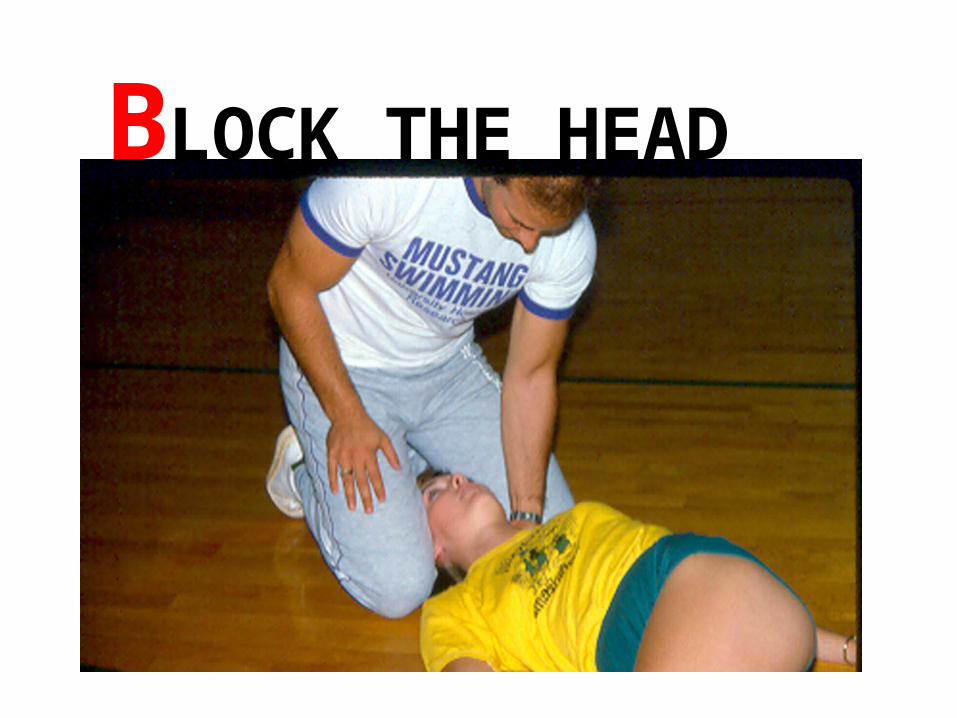
BLOCK THE HEAD

No Helmet
Removal

C.P.R.
Look Listen Feel

ANY UNCONSCIOUS ATHLETE MUST BE
TREATED AS A POTENTIAL SPINAL
CORD INJURY!!!
Athlete unconscious.
Athlete conscious with loss of movement or sensation. Complains of central neck pain.
FIELD MONITORING
Re-check vitals.
Reassure athlete.
Observe for Shock.
Be prepared to treat for shock.
SHOCK
Collapse of the c.v. system, or failure of the system to provide an adequate blood supply to all body tissues.
CAUSES OF SHOCK
Blood vessels dilated so widely that there is a
poor venous return.
There is loss of blood.
Heart fails to circulate the blood properly.
TYPES AND CAUSE OF SHOCK
Hemorrhagic – Internal and/or External Bleeding
Respiratory – reduce O2 in blood. (sucking wound, airway obstruction, spinal cord injury).
Neurogenic – loss of control by the nervous
system.
Psychogenic – reaction of nervous system to fear, bad news etc.
Cardiogenic – inadequate function of
the heart
Septic – severe infection resulting in vasodilation.
Metabolic – loss of fluids through diarrhea, or urination.Anaphylactic – caused by allergic reactions. Extreme emergency.
SIGNS AND SYMPTOMS
Eyes dull, lackluster
Pupils dilated
Face pale
Shallow, irregular respirations
Pulse rapid and weak 2
… 2
Skin cool and clammy
May have nausea, fainting, anxiety, thirst
Blood pressure is low
TREATMENT FOR SHOCK
Control bleeding.
Elevate lower extremities if no chest or head injury.
Prevent loss of body heat.
Lie athlete down. N.P.O.
Primary Survey
Initial scan done by the ‘at head’ person. Feeling for deformity etc.Secondary Survey
Someone else holds head and you check lower ext.
Initial Questions
What happen?
Pain? Present or after accident.
Feelings: burning/tingling
Head pain/ache?
Orientation to time and place.
Observations of pupils.
Observe for any CSF or blood coming from nose or ears.
Look for bruising.
Test motor and sensory of upper extremity.
Do gross motor of feet.
Test grip strength of the upper extremity.
Continue to ask about headache and nausea.
Removal from FieldSupine lying. Sitting.
Four Point Kneeling. Three Point Kneeling. Standing (with support). Slowly walk to sideling.
Sideline Testing.
SIDE LINE TESTING
Subjective
Question about their feelings (headache, tingling, nausea)
ObjectiveMotor skills, verbal skills

HEEL TO SHIN
1 2
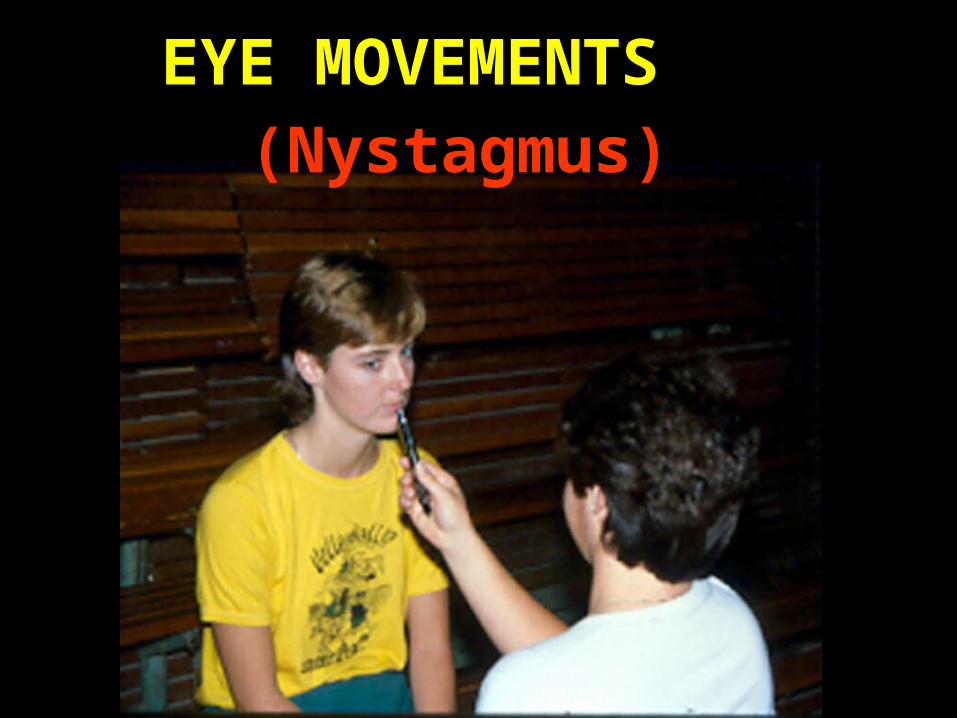
EYE MOVEMENTS(Nystagmus)
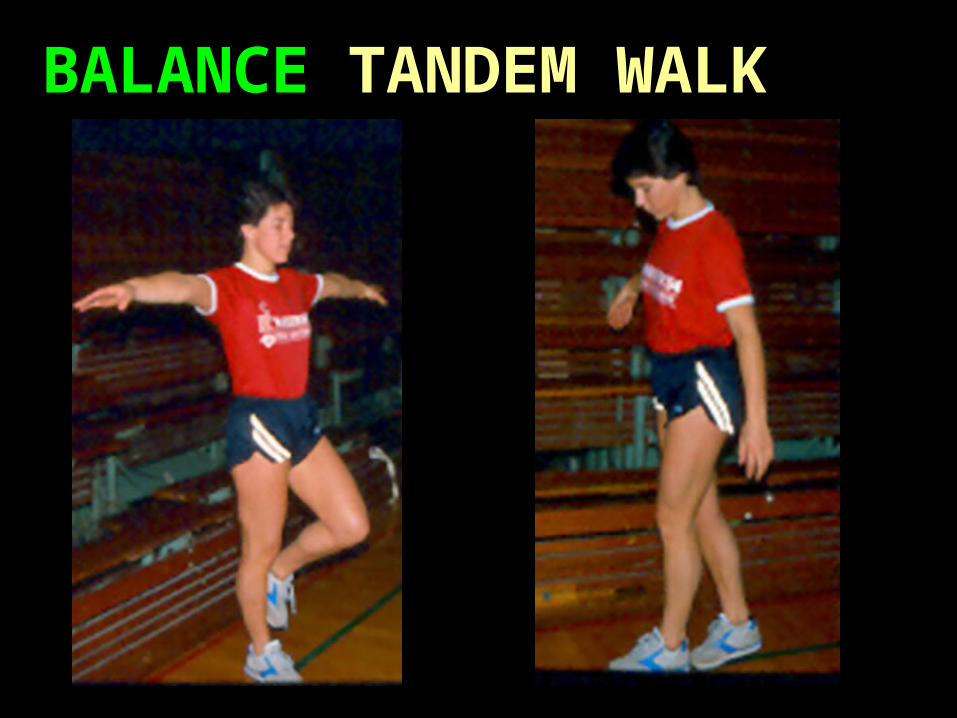
BALANCE TANDEM WALK
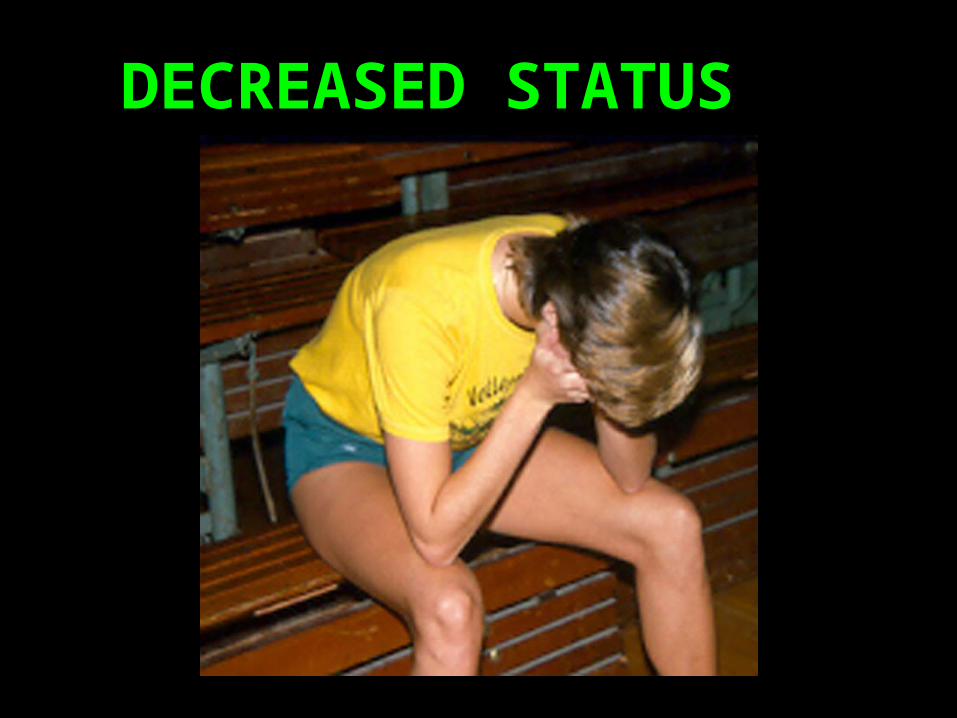
DECREASED STATUS
GUIDELINES FOR CONTINUED
MONITORING
Grade II should be sent to the hospital.
Grade I monitored at home. We give instructions.
No A.S.A. One drink!

MINOR NECK TRAUMA
SIDELINE MANAGEMENT
Minor Neck Trauma is an injury that has no arm pain, no loss of neck motion and no central pain during movement. The following should be tested……
General test of the myotomes (specific
nerves that innervate specific muscles) to determine if there is gross weakness. If
weakness; no return.
SIDE LIGHT… ‘Motion Talk’
..ors – muscles doing the movement.
..ion – direction of mov’t.
..ed – end position.
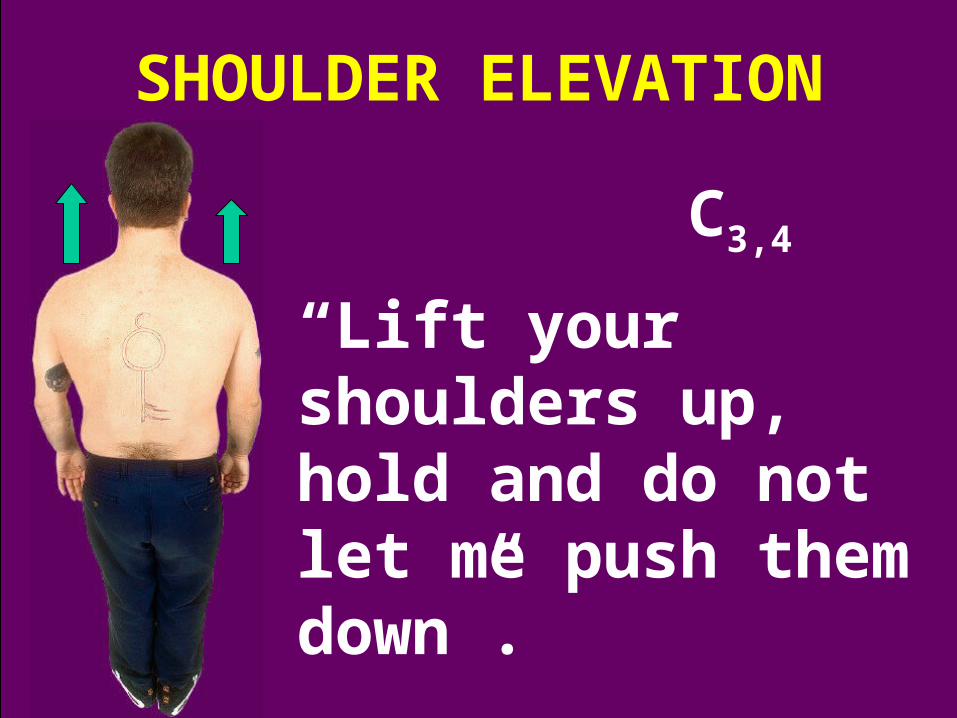
SHOULDER ELEVATION
C3,4
“Lift your shoulders up, hold and do not let me push them down”.
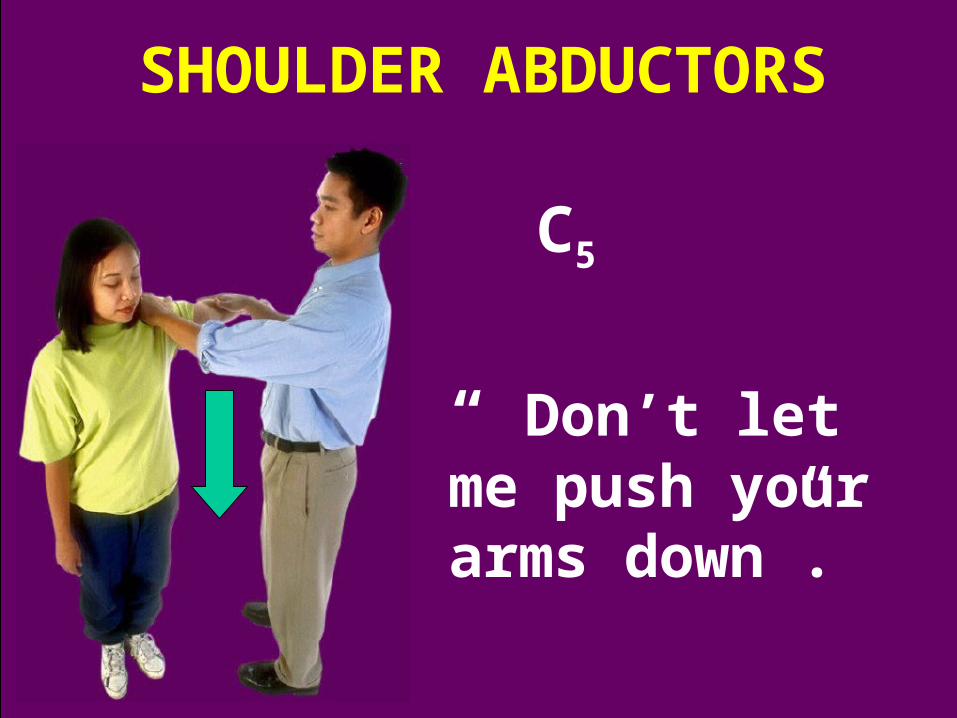
“ Don’t let me push your arms down”.
SHOULDER ABDUCTORS
C5
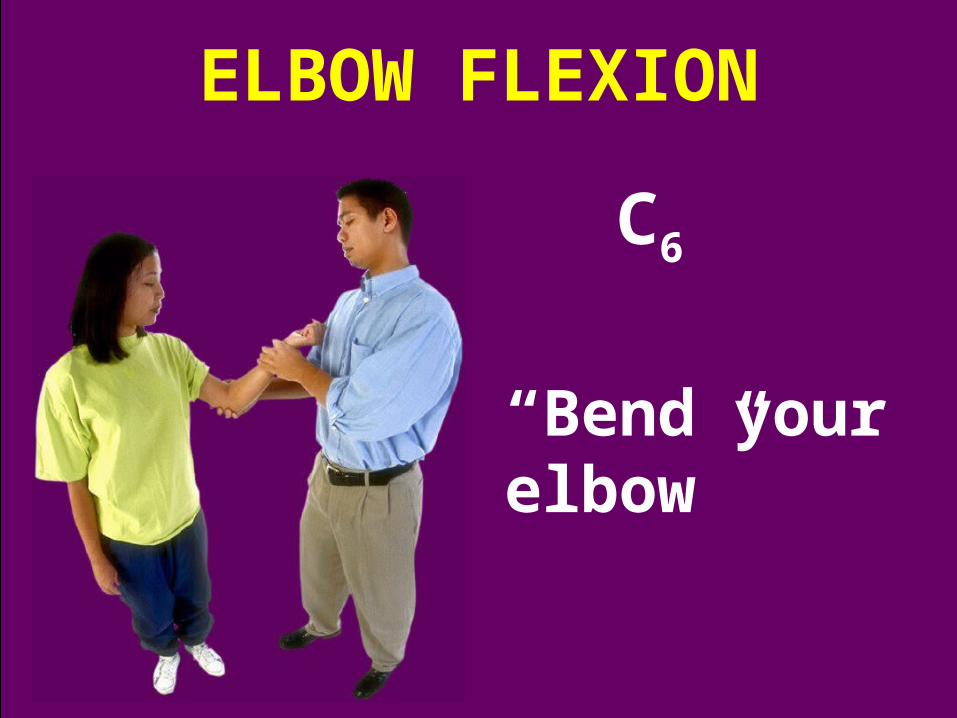
ELBOW FLEXION
C6
“Bend your elbow”
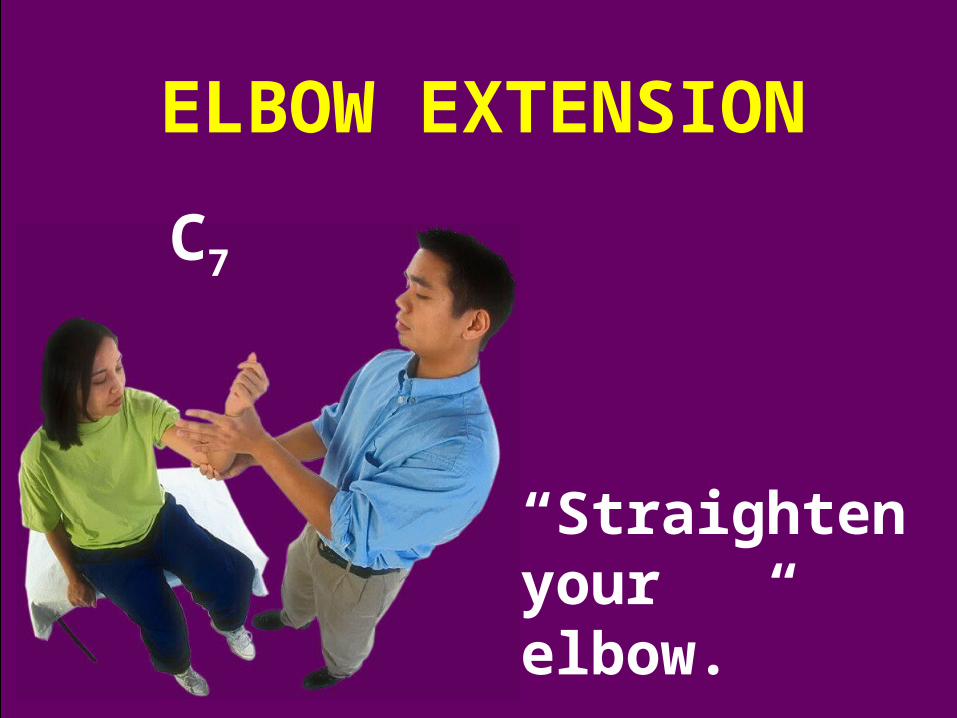
ELBOW EXTENSION
C7
“Straighten your elbow.”
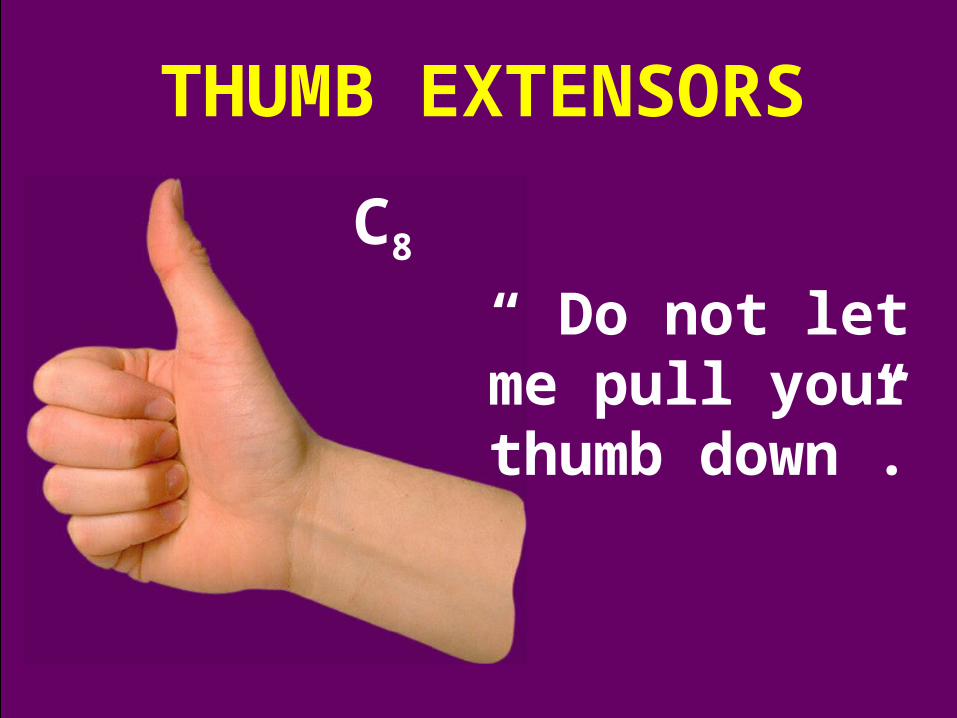
THUMB EXTENSORS
C8
“ Do not let me pull your thumb down”.
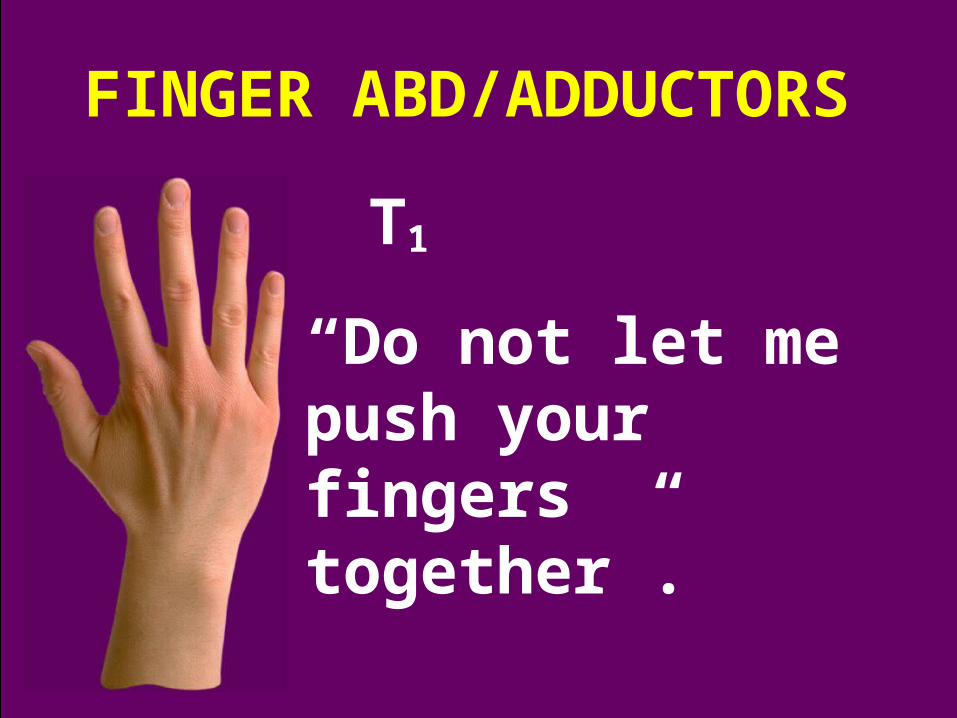
FINGER ABD/ADDUCTORS
T1
“Do not let me push your fingers together”.
If the neck motion is good, there is no neck/arm pain and the strength in the extremities is good, it is decision time!
If in doubt, don’t!
If the tests are good and you tested long and often enough, then do!
RETURN





























