Embed Size (px)
DESCRIPTION
Check out the second issue of The Muse, a platform for the personal stories and reflections of healthcare providers.
Citation preview

THE MUSE • WINTER 2016
1
ISSUE 2 • WINTER 2016

ContentsFrom the Editor
The WHO Diaries
Saving an Unknown Life
Interview with Dr. Alan Neville
MacMed
Paramedic
Community Spotlight: Health, Aging, and Society Student Association
Childhood Cancer: Ready or Not
Emergency First Response Team Interview Series: Sachin Doshi, Director
What is Health?
Just Observe
The Emotional Aspect of Patient Care: A Volunteer’s
Perspective
Staff
3
4
6
8
11
14
15
17
19
23
25
28
29

THE MUSE • WINTER 2016
3
FROM THE EDITOR
(Photo courtesy of Irina Sverdlichenko)
To the reader:
You’d think it were a simple thing.
There is a lot of dialogue about the importance of integrating humanistic care into the health professions. While there is no single, universally agreed upon model of what is it that constitutes humanistic care, there are a number of qualities that pop up frequently in the dis-cussion—an example being integrity. Communication. Respect. Empathy.
It’s unfortunate that the fundamental tenets of hu-manistic healthcare seem fairly obvious at first glance. However, to miss the nuances is to have an incomplete understanding of the entire concept. Let’s take commu-nication as an example. In his interview, Dr. Alan Nev-ille, oncologist and Associate Dean (Health Professional Education) of the Faculty of Health Sciences, offers his perspective on what meaningful dialogue with patients and their families entails:
What does the patient want to know at that time? Is that what the family wants to know and what they think the patient thinks or needs to know? You’ve got to keep an eye on everyone in the room.
Ultimately, these kinds of intricate complexities pervade the patient-provider relationship and this is what the guidelines and courses modeling humanistic care attempt to teach. And perhaps this is what renders teaching humanistic healthcare in such a way so chal-lenging. But thankfully, research papers and courses ar-en’t the only way to learn.
Read about Noa Lashevsky’s Locks for Love cam-paign in tribute to Angel, the young girl to whom she was a Big Sister through an afterschool program and who was diagnosed with leukemia. Read about Ham-ilton Paramedic Steve Kawamura’s fond musings about the inspiration he drew from a couple that he met on one of his calls. Turn the pages and you’ll see many in-stances of raw humanity demonstrated across a diverse range of times, places, and situations. Read and you’ll find that things start to make sense.
I’m not here to debate the semantics of which spe-cific qualities comprise humanistic care and how they should be defined; our goal as a team bringing this issue to you is not to convince you of a particular set of beliefs or practices. All we hope to do is share these stories with you as they’ve been shared with us, and let you come to your own conclusions. Whether or not you intend on pursuing a career in healthcare, the premise upon which all of these stories are founded is humanity, and that rings true to all of us.
As always, I’d like to express my appreciation of the many contributors that invest their time, skills, and ex-periences in an effort to realize the vision of The Muse. It is courtesy of you that The Muse represents what it does now and, hopefully, will continue to do so for many years to come: amongst struggles and successes, the best of humanity.
Anna GoshuaEditor-In-Chief

THE MUSE • WINTER 2016
4
THE WHO DIARIESExcerpts from the musings of a World Health Organization internDisclaimer: Everything I’ve written is based on my own observations and my interpretations of them. There may be things that I don’t know, and things that I haven’t considered, but full disclosure so you can form your own opinions.WEEK 1Before I say anything more about my experience at the WHO, let me just give you a heads-up. I know I’m at the WHO, I know it could be a great stepping stone, I know it will look great on my CV, and I know I’m lucky to be here. But I want you to know that I didn’t come here with big expectations. I’ve heard and read time and time again about how the WHO is in shambles, and about the bureaucracy and poli-tics that colour these institutions. I came here because I wanted to see it for myself, I wanted to understand, and I wanted specific stories that illustrated these vague accusations that get tossed around.
WEEK 2 Yesterday I attended a techni-cal briefing about Ebola. Techni-cal briefings are side events at the World Health Assembly that focus on specific issues (like Ebola, cli-mate change, malaria, WHO re-form, etc.) where you hear from a panel of speakers who speak to their experiences in that topic. To be completely honest, most of it was a snoozefest. The speakers sounded bored. They were reporting statis-tics and dropping buzzwords, and it was painfully evident that they
were all figureheads. Just as I was ready to walk out, a lady from the Liberian delegation began to speak. She spoke with such conviction and pride (Liberia had reached zero Eb-ola cases), it was clear that she had been on the ground as it happened and not in an office giving orders. It was no surprise that she received the loudest and longest applause. Do you know how I knew she was genuine? It was clear that she was proud of her nation’s accomplish-ments, but she by no means took the credit. “It’s the communities in Li-beria that have turned the corner,” she said. She didn’t tout the govern-ment response or higher-level poli-cies, but instead credited the people that showed the most resilience in the face of the crisis. In comparison, there was a level of restraint in how the other delegates spoke. So many of them said, “[Insert country name here] thinks…”, or “[insert country name here] has done…”, as though they were somehow removed from their country. This woman always said “we”.
WEEK 2Based on what I’ve read so far, to be completely honest, the WHO’s work all seems like a bunch of lin-go and overarching frameworks
that prescribe a one-size-fits-all approach to different issues. That’s the thing: the WHO acknowledges that approaches need to be tailored and modified to specific contexts, but they still can’t let go of publish-ing vague, broad-based guidelines that aren’t really all that useful to anybody who might actually use them. But I’ll sift through them. I don’t expect to make any big chang-es during my time here, it’s just too unrealistic (and it’s too big of a mess), but I’ll be damned if I choose to be apathetic. I guess I’ll start with questioning things that don’t make sense to me, and see where that takes me.
WEEK 3One incredibly humbling part about working at the WHO is feeling like the whole world is here. Today, as I was waiting outside of the Human Resources office to submit some paperwork, I heard an exchange that made my heart happy. A lady was picking up something from her mailbox and as a man passed her, he said “Habari yako”. She smiled back and replied, “Mzuri sana”. Hearing this, I laughed and said, “It’s been so long since I’ve heard those words.” She smiled and said, “Then you must have been to....”
THE WHO DIARIESThe WHO Diaries
ARTISTAmy Ajay

THE MUSE • WINTER 2016
5“Tanzania,” I finished for her. And I started, and she joined me in sing-ing “Jambo, jambo bwana, habari gani, mzuri sana”, right there in the middle of the HR hallway with ev-eryone watching. It made my day.
WEEK 4The WHO doesn’t have the power to propose resolutions, side-events, or technical briefings during the World Health Assembly - only states have this power. So, despite being the supposed global author-ity on health, and despite hosting some of the world’s best technical experts, the WHO and other non-state bodies can only make rec-ommendations and lobby national governments. If countries aren’t receptive, then the potential res-olution falls through the cracks. I had always thought that a state-based system was the most dem-ocratic way to govern. Part of me still does, but it’s becoming more and more apparent that there needs to be more of a role for IGOs and NGOs in global decision-mak-ing.
WEEK 7…I told her that it’s hard for me to understand—much less debate—abstract concepts when I’m so far removed from the ground. I told her that I’m used to being closer to the work that I’m doing, and that I work best when my work is put into context. I told her that it’s hard for me to be doing work on communi-ty-based rehabilitation when I don’t know the communities we’re sup-porting, or whether or not this work is helpful at all. I told her that, from my limited experience, I don’t know whether the products we’re putting out will even be used by people on the ground.
WEEK 8…He stressed the need for adapt-able employees. He reminded us that the WHO works for and is ac-countable to its Member States, so when their priorities change, our work changes. We can’t just keep a project going because we’ve be-come attached to it. If it needs to be
dropped, we drop it and move on. It took a few seconds for it to sink in. There are 194 Member States and most of them have an election every 4-6 years, meaning that priorities in each country change at least every 4-6 years. Probably more. “Adapt-able” doesn’t even begin to cover it.
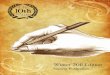
WEEK 9 WHO (Geneva Headquarters) Em-ployee Quotas by Nationality (as of Summer 2015)What? How can there be more American employees at the WHO than any other nationality, and yet, the USA is still underrepresented?
How are these quotas determined and who decides them? It turns out the quotas are directly correlated with each country’s contribution to the WHO’s budget. Bingo. It’s frus-trating to see how deep-seated the politics are, especially considering that your country’s quota status influences your chances of being hired by the WHO. The countries that have the most money can es-sentially buy their way into and out of everything. All things considered, the fact that each Member State only has one vote in the Assembly seems like a superficial democracy. It doesn’t mean much when votes can be bought.
WEEK 10 A colleague’s response to my dec-laration that the WHO is merely a puppet for Member States: “I see it more as a dance between WHO and Member States. We’re dance partners. Yes, we can’t tell them to do anything, but we can move with them and nudge them. So we nudge. We can’t propose resolutions, so we
find Member States who have been front runners in certain areas (e.g. health systems strengthening, HIV/AIDS prevention, universal health coverage, etc.), praise them as champions of the cause, and nudge them to propose the resolution. Yes, WHO ends up doing a lot of the work for the resolution and lets the Member States take all of the credit, but if the resolution passes, it’s all worth it. It’s a dance and we have to move with them to get things done.” The analogy made sense, and I apologized for oversimplify-ing what was actually an extremely nuanced relationship.
WEEK 11 The WHO has limited resources and it needs to focus its energies where its Member States want it to. Nobody cared about outbreaks before H1N1(swine flu) and Ebola, and the WHO wouldn’t have got-ten any pats on the back for invest-ing time into creating a stronger pandemic preparedness plan when there were other pressing needs to attend to. But now that the global
interest is there, it makes sense to invest resources into strengthen-ing this emergency response. Not the most proactive way to go about doing things, but it’s what works in the system we have now.
WEEK 12At the end of the day, I feel incred-ibly privileged to have had the op-portunity to be here, frustrations and all. Yesterday’s speaker encour-aged us [interns] to go out and get some field experience. “Geneva’s not the place for young people,” he said. “I mean it’s really nice and the lake is really cute, but go out and do life and then come here to see the lake.” And I can recognize the truth in his words as they apply to me – I need to be closer to the ground to believe in the work that I’m do-ing. Maybe that’ll change one day, but I’ll cross that bridge when I get there. So wherever this “field” may be, I guess that’s where I’m headed.
ABOUT THE AUTHOR - Mathura Mahendren is a recent graduate of the BHSc program, Global Health Specialization, at McMaster University. During the summer of 2015, Mathura had the privilege of complet-ing an internship at the World Health Organization (Geneva Headquarters) in the Department of Disability and Rehabilitation. She is currently working as a Health Promotion and Education Officer at the Nova Scotia Gambia Association in The Gambia. Email: [email protected]
CountryEmployee
QuotaRange
Actual # ofEmployees Status
Canada
United Kingdom
United States of America
28-39
39-54
188-255
47
99
144
Over-represented
Under-represented
Over-represented
THE WHO DIARIESThe WHO Diaries

THE MUSE • WINTER 2016
6
Tel Aviv, Israel
It was 3 AM on a Friday when we got called to do CPR. A cab driver
had fallen on the road from a heart attack after loading his passengers’ luggage into the trunk.
We got to the location within three minutes. As we pulled up, the only source of light was from our ambulance’s headlights, which brightly lit the middle of the road. From the back of the ambulance I looked through the windshield to see a man doing compressions on the fallen driver. I grabbed the ambulance kit and got out through the back. I stopped for a second as the realization of what I was about to do hit me.
The paramedic told me calmly that I should take over and do the compressions, so I found the Cardio-Pump and started. Meanwhile,
the paramedic was setting up the defibrillator and the medic was preparing the oxygen pump. My sense of time was skewed, so I don’t recall if I did compressions for two minutes or for ten.
At some point, another medic showed up on a motorcycle and took over doing compressions, while I switched to give breaths every five seconds. I also watched the time on the defibrillator, announcing when two minutes had passed, meaning we had to give a shock.
We gave a total of three shocks, which I later learned were considered to be quite a few. Our patient’s pulse returned before we gave him any medications, so we loaded him into the ambulance and I continued pumping oxygen until the hospital nurse took over for me.
On Monday morning, I saw the same paramedic from Friday at the
station. She told me that our patient was alive and in the hospital. I asked her if we could visit him, and she said that we could. We went upstairs to the cardiac centre. There is an entire world above the Emergency Department, which I had never seen before. Ambulance workers are foreigners in all other areas of the hospital, filled with restaurants, clinics, and offices.
We entered a room to find a man in his 60s, sitting up in the hospital bed eating his lunch. He looked up and asked who we were. We told him that we were part of the team that had brought him to the hospital. All he could say, repeatedly, was that he was at a loss for words.
But so was I. I remember feeling my cheeks hurt from smiling. It was all I could do. He started to cry and shake his head and strain for words.
Saving an Unknown Lifeby Michal Coretcoretam@mcmaster. ca
Saving an Unknown Life
ARTISTNikesh Pandey

THE MUSE • WINTER 2016
7
He told me that I had saved his life. Yet even now as I write this, I don’t feel that I saved his life. I helped. As the volunteer First Aid Provider, I did what the paramedic needed me to do. There was no feeling of heroism, only joy.
As I was standing at the foot of his bed, a woman walked in. She asked us who we were and we told her. She screamed a little and started crying, hugging and kissing us. She said that we didn’t just save his life, but also all the lives connected to him.
And then she showed us his phone, which had a picture of a sweet little girl as the wallpaper.
This, she explained, was his granddaughter who loved him dearly. She said that the two were inseparable, and that we gave her husband the chance to watch their granddaughter grow up.
I left the hospital not knowing the cab driver’s name, nor any details about him, except for the fact that he was alive.
~~~
This experience affected me in profound ways that I cannot begin to explain. To be so involved in an
individual’s existence is shocking, humbling, and unforgettable. There is a strange tension I cannot ignore between the closeness I feel to a life I helped save, as well as the distance between myself and this anonymous stranger.
There is a sense of humanity in every healthcare profession: to help whoever needs your help, regardless of who they are. Our paths will likely never cross again. All I have left now is to move on, carrying the satisfying notion that one day I might get into a cab and recognize the driver.
“To be so involved in an individual’s existence is
shocking, humbling, and unforgettable.”
ABOUT THE AUTHOR - Hi! Thanks for reading The Muse! My name is Michal and I’m a second year BHSc student at McMaster University. That’s what I am, sort of. What else am I? Who knows? I love used books, reading and writing poetry, playing music, over-thinking, learning math, swing dancing, and... so much more.
“There is a sense of humanity in every healthcare profession: to help whoever needs your help,
regardless of who they are. ”

THE MUSE • WINTER 2016
8
EXCLUSIVE
DR. ALAN NEVILLE Interviewed by Anna Goshua & Irina Sverdlichenko
Dr. Alan Neville, M.D.is an oncologist at the Juravinski Cancer Centre and Associate Dean (Health Professional Education) of the Faculty of Health Sciences at McMaster University.
AnnA & IrInA: What is a typical clinical day like?
Dr. nEVILLE: I work in an outpatient clinic at the Ju-ravinski Cancer Centre two half-days each week. I also take my turn on call. My area of work is with genitouri-nary cancers, though I do have a few brain tumour pa-tients as well. Genitourinary cancers are predominantly malignancies of the testicles, kidney, prostate, or urinary bladder. The clinic is very busy and has numerous pa-tients. The waittimes for a new consultation are short, simply due to the pressing nature of the health issues with which these patients are contending. Patients are fitted into one-hour new consultation and 15-minute follow-up visit timeslots. Follow-up appointments are sometimes double booked, which adds a sense of pres-sure when it comes to allocating time per patient. There is a very brief timeframe to see the patient and complete the medical note.
Dr. Alan Neville

THE MUSE • WINTER 2016
9Many of our patients, especially the young ones, have a high survival rate, though there are survivorship, fertil-ity, and psychosocial effects that must be dealt with. In the elderly, with bladder or prostate cancer, the situation is more complex and the prognosis tends to be worse due to cancer metastasis, less effective treatment, and pre-existing comorbidities.
It’s hard for me to describe a “typical” clinical day. Each patient interaction is unpredictable. No matter how ex-perienced and adept you think you are, a curveball can be thrown at you at any point. And you simply don’t have the opportunity to take endless time to mull over a pa-tient. You have to work efficiently with your team. I have a nurse who works with me directly, as we have a prima-ry nursing system. Healthcare is moving more and more toward team function. It’s inevitable, and it’s for the bet-ter.
A&I: Why did you choose to specialize in medi-cal oncology (lung and genitourinary cancers)?
Dr. n: Essentially, it was exposure to the specialty. As a clinical clerk and a first year resident, I was initially assigned to the main clinical teaching ward of the uni-versity hospital, which contained the Internal Medicine and Hematology-Oncology services. In those days in the United Kingdom, there were no structured cancer clinics. Patients who were receiving medical oncology care for leukemia or lymphoma actually came into the hospital for treatment. To receive chemotherapy, they were given the beds of inpatients that were well enough to get out of the bed for the morning. Mind you, we didn’t have che-motherapy nurses to administer or mix the drugs prop-erly. This work was all done by the residents.
You should note that the junior British training system is different from the system in place in Canada. We spent six months to one year at a time on a service, so that estab-lished a sense of continuity. I’ve spent hours and hours starting the IVs on a patient, and sitting and chatting with them while the chemotherapy was being administered. Not many of the leukemia patients had long survivals, but these experiences and the opportunities I had to spend time with them gradually drew me into oncology.
A&I: What do you appreciate the most about your patients?
Dr. n: Seeing them as people. They come in as pa-tients and I have the opportunity, however brief, to sit down and talk with them as people. I encourage indi-viduals who aspire to be physicians to engage with the arts and literature. A student who only knows physi-
ology and biochemistry is really not well educated, as far as I’m concerned. You have to be able to relate to people in order to talk to them. I often see a patient or their family members with a novel, for example, and just a brief comment acknowledging the book can be a conversation-starter.
It is important to discuss the medical issues, certainly, but it’s not all about the CT scan results or the blood count. I don’t talk to my patients as a medical expert in a white coat. My aim is to be able to converse with my patients should I see them on the street. It’s really hard to do that if you have no sense of other cultures, and what’s current…how do you prepare yourself to be able to relate to other people? Well, don’t be so focused on yourself. Sometimes my patient needs Dr. Neville and other times, they need Dr. Neville’s nurse. If I can’t see a patient often enough to adequately monitor how well pain and other symptoms are being managed, that is when I start thinking about referral, getting a social worker involved, and figuring out the family situation.
A&I: How have your patients shaped your de-velopment as a physician?
Dr. n: Variety being the spice of life, each patient in-teraction diversifies and enriches your perspective. It’s not just another patient with prostate cancer. It adds another facet to the impression of the wide panorama of cancer patients.
“As I’ve gotten older, I’ve grown increasingly concerned by how older cancer patients struggle with other chronic ill-
nesses as a simple con-sequence of them being
older.”You may have a 75-year old with bladder cancer, for which there is a specific drug treatment. However, he also happens to be diabetic, hypertensive, a lifelong smoker, taking a non-steroidal anti-inflammatory drug
Dr. Alan Neville

THE MUSE • WINTER 2016
10such as ibuprofen for his constant headaches, and had a heart attack three years ago. When you examine the blood work and observe that their kidney function is insufficient, you realize that the standard treatment would kill them. Patient comorbidities are challeng-ing to deal with and it has helped me develop a holistic treatment approach.
A&I: I imagine that you must engage in end-of-life discussion quite often. How do you ap-proach this type of discussion?
Dr. n: Good question. I imagine that’s what everyone thinks about this profession: cancer is an inevitable terminal disease. To be honest, medical oncology is more of a chronic care specialty. It is critical to develop a rapport with patients in order to hold dialogue with them. Choosing the right moment to deliver news is an important aspect of these discussions. What does the patient want to know at that time? Is that what the family wants to know and what they think the patient thinks or needs to know? You’ve got to keep an eye on everyone in the room.
It is tricky when the patient and family are not on the same page. Perhaps the patient is scared to know the news, or has already figured it out and doesn’t want to know. Either way, if, for example, you communicate with a patient’s daughter and say nothing to the moth-er, and the mother begins to suspect this sidebar com-munication is going on, tension can develop between everyone. Patients go through stages of wanting and being ready to receive information. It is important to be upfront and acknowledge the situation.
A&I: What about what you do makes you afraid?
Dr. n: My biggest fear isn’t a matter of whether or not I have prescribed the appropriate treatment. I’m not being a smartass saying this, by the way — years of experience give you a certain sense of reassurance that you’re capable of doing the right thing. Besides, we have a lot of checks and balances. I can easily consult with other physicians on the service, and the oncologic treatment opinion tends to be fairly uniform among all of us. Most of the time, my main concern is whether I’ve said the right thing. For example, I might think, was the patient ready to hear this aspect of their prog-nosis at this time?
A&I: Who was your mentor as you were train-ing to become a physician and how did they in-fluence your course within healthcare?
Dr. n: There were probably several of them. In med-ical school, there were two inspiring senior physicians on the same ward that I was assigned to. They were good at clinical medicine, of course. But beyond that, what they were really hot on-and this is what inspired my passion-was what we call clinical skills. They were sticklers for teaching the art of the history and physical examination to students.
The other notable mentor I had was a senior oncologist at the Juravinski Cancer Centre whom I trained under as a resident. Back then, it was still called the Hender-son Hospital. He had been there for quite a while prior to my stint there as chief medical resident. He had a wonderfully British sense of humour-very facetious- that stands out in my mind.
A&I: What’s the most important piece of advice that you pass on to your students?
Dr. n: Engage with the humanities. We are just com-ing out of an era where it was felt that medicine was becoming very technology based and that healthcare improvements were going to come from technological innovation. Better care needs not only that, but the hu-manities. This entails empathy, professionalism, good communication, and, above all, the ability to prioritize the patient and their needs.
“Medical education should be holistic.” In my academic life, I used to run the MD program, through which I became involved in national curricula initiatives; we have an Aboriginal health curriculum in Canada, for instance, which let me work closely with Aboriginal peoples and physicians. Or take the medical program at McMaster University as an example. The medical students are taken to the Hamilton Art Gallery and made to describe drawings, which helps them with describing symptoms. These aspects of the program are implemented so as to help teach the students that they are learning the patient’s narrative, rather than just their history.
Dr. Alan Neville

THE MUSE • WINTER 2016
12
The medical school application process is a gruelling experi-
ence. You spend a great deal of time working through the application and even more time just waiting to hear about interviews and admis-sions results. At the end of it all, if you find yourself with one or more offers of admission from medical school, you’re faced with the inevi-table question: where do I go?
Whether you are at the begin-ning of the process and are debating applying to McMaster, or at the end of the process and wrestling with the decision to actually choose McMas-ter, I hope this article will provide you with insight into the program and its unique style of learning. I did not have a clear appreciation of how the mechanics of Problem Based Learning (PBL) worked until I immersed myself in this style of learning. To me, entering McMas-ter’s medical program required a leap of faith. Despite being a little concerned about the learning style and how it would suit me, I am now firmly convinced that PBL is an ex-cellent way to learn and am excited to be able to take the useful skills I gained with me as I move through the rest of my training into clinical practice.
The bulk of learning during the pre-clerkship phase (one and a half years) at McMaster’s medical school takes place in and around tu-torial, of which we have two blocks each week that are three hours long. The group is comprised of around seven students and a faculty mem-ber, whose role is to sit in during the session and ensure we are meet-ing the curriculum’s learning objec-tives through our discussion. The tutorial begins with a novel case, from which the group identifies the information needed to understand the case properly. The group then sets up a list of learning objectives. Between tutorial sessions, each group member does their individ-ual preparation, from textbooks,
journal articles, websites, and var-ious other resources. It is common for group members to converge upon the same learning objectives using completely different resourc-es, adding variety to the upcoming tutorial discussion. At the following tutorial, the case is taken up and everyone shares their findings and understandings before setting ob-jectives for the next case. There is ample opportunity for questions, discussion, and formulation of key concepts. In fact, these are encour-aged. I find the moments where one tutorial member explains a concept to clear up the confusion from a probing question asked by another particularly educational. Given this set up, students visit the concepts at least twice – once before tutorial in the preparation phase and once during tutorial.
To illustrate how PBL works, allow me to invoke a hypothetical patient admitted to hospital with a complicated set of symptoms. The physician is unsure of what ails the patient because the patient history, physical examination results, and the laboratory investigations do not lend themselves to a clear diagno-sis. The doctor suspects this patient may have a rare and peculiar disor-der that was not covered in medi-cal school. Our doctor decides to consult six colleagues in the hopes that they might have an idea of what is going on. The group decides it needs additional information in order to proceed with planning the patient’s care, and the members sit down together and spend some time brainstorming what they need to know. A list of learning objec-tives is generated based on the im-portant aspects of the patient’s pre-sentation. The team reconvenes the following day, each of the members having spent the last evening revis-iting some textbooks and reading some of the latest journal articles. They share their respective findings around the table and identify a few
conditions that might be afflicting the patient, as well as the relevant pathophysiology underlying these diseases, and the investigations and treatment required. Armed with this new knowledge, our doctor leaves to do the appropriate testing needed to make progress in this di-agnostic challenge.
In addition to tutorials - which are the venue for learning the work-ings of the body and the biology of disease - we have a number of other sessions. Clinical skills ses-sions are where we learn how to take good medical histories and practice physical examination ma-neuvers for different body systems. Anatomy sessions take place in the anatomy lab with the faculty anat-omists, and are reasonably self-ex-planatory. Large group sessions are presentations given by facul-ty on material that supplement our tutorial learning. Professional Competencies is where we learn about the aspects of medicine that lie outside of biology. There are so many things a physician needs to be adept at or knowledgeable about for successful patient interactions and good outcomes, in addition to having a strong biomedical founda-tion. We grow to appreciate these domains of medicine with the help of our Professional Competencies group. It is comprised of approxi-mately nine students and two facil-itators, one of whom is a physician and the other a member of an allied health profession. Group discus-sion, role-playing with simulated patients, and other activities allow for some of the richest learning ex-periences within the program.
Furthermore, there are a num-ber of unscheduled hours each week that students spend in a number of ways to round out their educational experience. Of course, the prepara-tion for tutorials and other sessions is to be completed during this time, but there is also time for other ac-tivities including but not limited
MacMed

THE MUSE • WINTER 2016
13to research, shadowing physicians, riding along with paramedics for a shift in an ambulance, organizing workshops for high school students interested in medicine, hobbies, and anything else you may be inter-ested in. The schedule is as busy as you decide to make it. Every week can be different - some weeks I have a lot going on, and other weeks I cut back a little.
The remaining time of the three-year program is spent in clerkship where students complete core rotations and electives in a variety of specialties and practice settings with physician mentors. Every day brings a new experience. No amount of textbook reading can prepare you for each unique patient encounter, but the skills acquired from working through problems with your classmates transfer nicely to the clinical environment. Simi-lar elements of collaboration and learning are in play; however, you are now working with your precep-tor and a team of interdisciplinary professionals. The virtual case be-comes a real patient.
Overall, McMaster allows stu-dents to focus on learning the key concepts in medicine and con-necting these together, rather than memorizing extraneous de-tails that one can look up on their smartphone. This style of learning
encourages me to work hard not to achieve a particular mark on my test, but further my interest in learning and my aim to be a good physician.
I am very fortunate to be a medical student at McMaster. I can monitor my learning, be sur-rounded by wonderful colleagues who are also good friends, and ev-ery week is new and exciting. The program is challenging, but it is im-mensely rewarding. If you are con-cerned about whether or not PBL is right for you, let me assure you that anyone can do well given the right environment, an open mind, a willingness to work hard, and the determination to succeed. McMas-ter does an excellent job of building the right environment. If you bring the remaining elements to the table, they will be fostered and you will do well here.
ABOUT THE AUTHOR - Ammar Khairullah is a third year medical student at McMaster University. As part of the Waterloo Regional Campus, he enjoys sharing his experiences at a distributed medical education site with people interested in pursuing medicine.
MacMed

artistSama anvari
Paramedicby Steve [email protected]
Being a paramedic, you get to know and serve your community well. I’ve
been on the job for 14 years now, and still enjoy racing to the scene to help some-one in need. The need may be physical, mental, or virtually anything imaginable. Early on in my career, I focused on the technical and clinical aspects of the job.
Bettering my IV starts, intubations, and field diagnoses were important to me. I was so afraid of making a mistake that I wrote all of my significant calls down in a diary to improve my patient care. As time went on, I gained experience and confidence in my skills. After a few years, I was able to take a step back from the action and appreciate the human aspects of my calls. This was something I lacked early on in my career.
I remember a call that really touched my heart. At 0300hrs in the morning, a call came in for an uncontrolled bleed. We ar-rived at the apartment, where an elderly female answered the door. Very concerned, she directed us to her husband, who was sitting at the kitchen table holding his ear. He explained to us that the abscess in his
ear that was scheduled for removal start-ed bleeding around 11:00pm and hadn’t stopped. Visibly frustrated, he apologized for calling us, telling us that he’d tried ev-erything but couldn’t stop the bleeding. We assured him that that we were here to take care of him, and that he should have called earlier. I bandaged his ear and made some small talk with the couple. They told us proudly that they had been married 60 years. I was only 22 at the time, and couldn’t even begin to understand the scope of what that meant. But I was old enough to know that such a thing was rare, and that it mer-ited appreciation and respect. My partner and I congratulated them and a smile broke out on all of our faces. I offered to take his wife to the hospital with us, but she re-fused politely. With a smile and a wink, she claimed that she had something “special” to do. I thought it strange at the time, but it wasn’t my job to interrogate the patient’s wife about her personal affairs. I let it be and we prepared the patient for transport. The drive to the hospital was quiet and without incident. We dropped our patient
off in the emergency department. It was a mild summer night, so I decided to do my paperwork outside. I had just finished up when I saw a cab pull up to the emergen-cy department, from which the patient’s wife emerged. She carried a big, beautiful bouquet of flowers, and was smiling from ear to ear. She must have picked them up from the 24-hour grocery store near the hospital. I could only assume that they were for her husband. Nothing else would make sense at 0430hrs in the morning.
To be witness to love like that was a privilege. It made me ponder about the future and hope to someday find a love like that. Since then, I have always taken the time to appreciate the bond between elderly couples during the calls I am on. A kiss goodbye, an “I love you”, a sincere embrace – these are examples of true love. Companionships that stand the test of time are a thing to be cherished. I wrote down this call in my diary, but not as a means to improve my patient care. For me, this was more—a memory of something to aspire to.
About the author: Steve Kawamura is a 14 year veteran of the Hamilton Para-medic Service. He resides in Hamilton, and enjoys serving his community. When he is not busy transporting patients to the hospital, he enjoys his family life and martial arts. He has been training in karate for 30 years, and has attained his blackbelt in two different styles.

THE MUSE • WINTER 2016
15
The Health, Aging and Society Student Association (HASSA)
is a student-run organization ded-icated to promoting the awareness and study of issues related to health and aging. HASSA hopes to bring together students through academ-ic, professional, and social activities both on and off campus. Through this objective, HASSA hopes to build a better understanding of health and aging as social realities while exposing students to academic, vol-unteer, and professional opportuni-ties. To date, HASSA programming, outreach, and volunteer opportuni-
ties have benefited hundreds of stu-dents in the Department of Health, Aging, and Society and have direct-ly contributed to students obtaining internship placements and employ-ment positions in the field.
I have been fortunate to be in-volved with HASSA as the 2013-2015 Academic Coordinator and the 2015-2016 President. Admit-tedly, I first applied for an executive role as a way to make connections in my department and gain leader-ship experience to include on my CV. However, volunteering with HASSA over the past three years
by helping to create opportunities for student learning beyond the classroom has shown me the value of involving oneself in efforts that benefit others. I can hardly refer to what I do with HASSA as ‘work’; or-ganizing events, collaborating with other organizations on campus, and developing relationships with community stakeholders is truly rewarding and meaningful. Volun-teering with HASSA has brought new meaning to the words of Steve Jobs, “the only way to do great work is to do what you love.”
During my 2014-2015 term as the Academic Coordinator, I focused much of my volunteer time with HASSA on creating new events. In honour of Remembrance Day, my committee and I organized the first annual Canadian War Vet-eran Speaker Event. I also invited the McMaster University History Society (MUHS) to co-host. This
Community Spotlight: Health, Aging, and Society Student Associationby Audrey [email protected]
Community Spotlight: Health, Aging, and Society Student Association

THE MUSE • WINTER 2016
16event allowed students from both the faculties of Social Sciences and Humanities to hear from a WWII Veteran and Korean War Veteran about their experiences fighting in war and how this affected their lives. The discussion of how a per-son’s life course evolves is a topic we discuss in various courses in the Department of Health, Ageing, and Society. Just this past Novem-ber, we held the 2015 version of the Veteran Speaker Event. Partnering again with the MUHS, this year we were honoured to hear from a Vet-eran from the War in Afghanistan. Major John Stewart shared frank and honest accounts of his experi-ence in Afghanistan and his strug-gles with Post-Traumatic Stress Disorder. This event gives perspec-tive to the academic theories that they learn in class, allowing them to meet living and breathing examples of people with meaningful and ap-plicable personal narratives.
Last year we heard from stu-dents who were looking for more opportunities to become involved
in the community. Thus, one of our goals for this year is to increase awareness of HASSA on and off campus, as well as to improve our relations with other health-relat-ed groups on campus. At the start of the year, I worked with my Vice-President to create a new exec-utive role for the 2015-2016 school year to help advance this goal – the Volunteer and Outreach Coordi-nator (VOC). The Volunteer and Outreach Committee has reached out to the Victorian Order of Nurs-es to participate in volunteer visit-ing with older adults and to help in their adult day centre. For the win-ter semester, the Committee hopes to expand their volunteer outreach to other organizations, such as soup kitchens and the Ronald McDonald House. Response to this new po-sition from both students and the community has been positive. A dedicated group of VOC volunteers has become involved with initia-tives such as the Victorian Order of Nurses Stocking Stuffers for older adults and the Hamilton Road 2
Hope. Furthermore, organizations such as Shalom Village, a long term care home in Hamilton, and First Place Hamilton, a senior’s resi-dence, have reached out to HASSA in search of student volunteers.
Volunteering with HASSA has given me a platform to enrich the academic experiences of students beyond their studies and to make meaningful connections with stu-dents, staff, and professors in my Department and stakeholders in the community. My involvement with HASSA has shown me that getting involved with a student organiza-tion or club is a great way to gain leadership experience, network, and contribute to a field or cause about which you are passionate – it is truly a no loss investment into your future and time at McMaster. Future submissions in in The Muse will include pieces from other stu-dents who volunteer with HASSA and who donate their time to the Association in a variety of ways.
ABOUT THE AUTHOR - Audrey is pursuing an Honours Double Major in Health Studies and Gerontology with a Minor in French and Business Certificate. She became involved with HASSA in her second year as the Academic Coordinator and continued in this role until her fourth year when she took on the role as President. Upon graduation Audrey hopes to pursue a Masters of Philosophy in Evidence-Based Social Intervention and Policy Evaluation at the University of Oxford.
If you are interested in learning more about HASSA, you are encouraged to email us at:
or visit our Facebook page at:
https://www.facebook.com/groups/healthandaging/
Community Spotlight: Health, Aging, and Society Student Association

THE MUSE • WINTER 2016
17
In high school, I was privileged to become a Big Sister to a girl
named Angel through a school pro-gram. After school, we would spend time reading books together, draw-ing, and colouring our favourite an-imals, and most importantly, danc-ing whenever we had the chance. I was supposed to be her role model, yet somehow she became mine. An-gel and I grew so close as sisters that seeing her walking down the hall would always brighten my mood, no matter how tired or stressed I was. During exams in my first se-mester of university, I found out
that my little sister was diagnosed with acute lymphoblastic leukemia, a type of cancer targeting the blood and bone marrow.
Hearing the news, I was stunned. I had no idea how to feel, what to say, or how to react. How was the eighteen-year-old me sup-posed to know any better? The only exposure I had to the reality of cancer was my two grandparents passing away from it when I was less than two years of age. I knew that it was one of the most common causes of death in the elderly, but my little sister? For her, a teenag-
er, to have to endure this sickness, sounded unimaginable to me. I asked if I could visit her during the winter break, not knowing whether I would be strong enough to see her in the hospital. When we finally set a date, the first thing I did was Goo-gle how to act when visiting a friend with childhood cancer. What do you say? What shouldn’t you say? What do you ask? What shouldn’t you ask? I was sad to find out that for the first time, Google was not able to answer my questions. In fact, no-body was able to answer them.
Childhood cancer is a topic that is rarely spoken of. We censor the idea because it is too difficult to bear. We are only willing to cope with the thought of a child suffering for the one hour and thirty minutes of The Fault in Our Stars movie… And that’s where it ends.
The problem is that when we censor discussion of childhood cancer, thinking of it as an un-imaginable tragedy, we isolate the many children who have to battle this monster daily. Instead, I firmly
Childhood Cancer: Ready or Notby Noa [email protected]
On February 8, 2016, I will be do-nating 12 inches of hair to Angel Hair for Kids.Here’s my story:
Childhood Cancer: Ready or Not

THE MUSE • WINTER 2016
18
believe that we should be taking a completely different approach, by exposing the world to the realities and struggles that these brave chil-dren must deal with. Rather than feeding this monster with our fear, we should educate ourselves and gather tools to help those who are battling it to feel empowered.
There are about 10,000 chil-dren living with cancer in Canada today. Though we are privileged to have free healthcare, we forget that subsidizing the direct costs of pur-chasing medication or having an or-gan transplant is not enough to win the war against cancer. Both social and emotional support is necessary to enable children and their fami-lies to lead healthy, ordinary lives.
Imagine a single mother with two jobs, raising four children, one of whom is diagnosed with cancer
at the age of six. The mother has to stay with her sick child overnight at the hospital and hire a nanny to care for the other three children. When the daughter has a chance, she tries to go to school to keep up with her normal life. However, she is starting to lose hair due to chemotherapy. The rest of her six-year-old friends, who have never heard of the disease, start to ask her questions. The daughter refuses to go back to school. She feels strange. Different. She wants to get a wig so that she can look like the rest of her friends. However, her mother can-not afford one, since a wig costs be-tween $800-$1,000. The daughter stops going to school because she feels like an outsider and, therefore, discontinues her education.
If there is anything you should take away from this story, it is that
we need to stop looking at child-hood cancer as a taboo and start raising awareness to give strength to these children and their families. We need to realize that the Cana-dian healthcare system only pro-vides free direct treatment, which is not enough to conquer cancer. Something as simple as wearing a wig, which is not always afford-able, can ensure that a child does not feel alienated throughout their battle. It helps children with cancer maintain their normal lives: going to school, going on playdates with their friends, and above all, feeling confident enough to race to the ice cream truck after a tiring game of hide-and-seek. Give these children an opportunity to come out of their hiding spots.
ABOUT THE AUTHOR - My name is Noa and I am a second year BHSc student at McMaster Universi-ty, specializing in Child Health. I am participating in McMaster’s annual Locks for Love event on February 8, 2016. I will be donating 12 inches of hair to Angel Hair for Kids, a non-profit program under A Child’s Voice Foundation that provides wigs for local, financially disadvantaged children suffering from medically induced hair loss. The wigs are provided at no cost to the families, which is astonishing considering that it costs $800 - $1,000 and 10-12 donated ponytails to create one hair prosthesis! Feel free to visit Angel Hair for Kids’ website to find out more about their work: http://www.acvf.ca/index.php/our-programs/angel-hair-for-kids/
If you can, please make a donation to help support this incredible cause or share this page with your friends and family. Every little bit counts! Thank you.
https://www.canadahelps.org/en/pages/locks-for-love-noa-lash/
Noa and Angel
Childhood Cancer: Ready or Not

THE MUSE • WINTER 2016
19
Emergency First Response Team Interview Series: Sachin Doshi, Director Interviewed by Samuel Wu and Joon Mun
For the next several issues, we will be profiling members of McMaster’s Emergency First Response Team (EFRT). Each piece will aim to shed light on the workings of EFRT and provide some insight into the perspectives of those mysterious yellow-backpacked individuals known as responders. Without further ado, let us present the command-er-in-chief…

THE MUSE • WINTER 2016
20
About EFRT
Sam and Joon: Can you describe EFrT in one sentence?
Sachin Doshi: Can I say no? From a responder’s per-spective, it would be a home away from home, where you’re able to grow personally and give back to the community in an interesting, unique, and engaging way.
S&J: How does EFrT work?
SD: We have two branches, the main one being our response to any sort of medical emergency on campus. A lot of people think we only respond to calls that are alcohol or drug related, but that is not the case; our most frequent calls involve musculoskeletal injuries. On top of that, we also deal with many other medical conditions, such as psychological emergencies; we’re actually putting in considerable effort into expanding our mental health services this year. The secondary branch is education. Throughout the year, we offer re-duced-rate first-aid courses, both public and private. If
anyone is interested, they can reach out to us and we can arrange that.
Our mandate is to provide better care and support for students, staff, and anyone else who steps foot on campus. In the process, we reduce the workload of the Hamilton Emergency Medical Service (EMS), which is already overloaded with calls. One of the reasons why EFRT was founded was to reduce response time for cardiac emergencies. Our average response time is two to three minutes, whereas EMS is eight to 10 minutes.
S&J: What’s one thing people don’t know about EFrT?
SD: Once you get involved, it’s interesting to see how far you get absorbed into the team, which I think is one thing that is difficult to imagine from the outside. Most people think that EFRT is just a club or a team, but everyone who joins becomes a part of our big family.
S&J: What does a typical shift look like?
SD: Our usual day shifts are eight hours, whereas our
EFRT Interview Series: Sachin Doshi, Director
Sachin Doshi:My name is Sachin and it is my third year in EFRT, thus making me a senior responder. I joined EFRT in my first year and this year, I am the director of the team.

THE MUSE • WINTER 2016
21night shifts are 16 hours (we can sleep in the office overnight). When you come in for your shift, you will do a pack check and restock supplies accordingly. After that, it’s up to the responder to decide what they want to do. They have to have the pack with them at all times on campus, as well as their bike, ready to go. One thing they cannot do is swim during their shift, as it takes too long to dry off and change if a call were to come in.
All of our calls come through campus secu-rity, so if a call comes in, a silent alarm on our pager goes off that gives us a brief head start. A few seconds thereafter, a loud tone on the radio goes off with the dispatch information. Once we have the information, we race over to the scene on our bikes and respond to the call.
After every call, the responders who attended the call debrief back at the office. It’s a great way to learn, as well as to provide support for responders who might have attended a difficult or troubling call. Along with the debrief, we write a report to document each event. Then, we go about our daily routine again, waiting for our next call. Typically, you’ll get one or two calls a shift, but I have had some shifts where I had eight calls and some where I had none.
S&J: What is the process of becoming a mem-ber of EFrT?
SD: It’s actually quite an intensive process. Written applications open up at the beginning of August and all you need to apply is Standard First Aid and CPR-HCP certification. All the training during tryouts is conduct-ed in-house to assess how well you learn and are able to apply your skills. After the written applications are reviewed, everyone is offered an interview that is MMI style [multiple mini interviews], along with a practical and knowledge test of first aid and CPR. So that’s the first round. For the next round, we narrow the pool of applicants to 40 candidates, who go through a full weekend of intensive training. Then there’s a week or two of practice nights, which are optional but highly recommended in order to practice applying these skills and gain experience. Finally, there’s an intensive week-end of evaluations that culminates in us selecting the new additions to the team.
S&J: How has the role of EFrT on campus evolved over the years?
SD: EFRT is close to 35 years old. In terms of how much it’s evolved since I’ve been here, I think it has ad-vanced in the sense of our campus awareness, as well as our first aid courses. Also, we’re constantly improv-
ing our services, an ex-ample being the addition of mental health training. I think something we’ve done well is keep up our reputation as one of the strongest first response teams in Ontario and even in North America. In fact, we went to a com-petition in the United States and ranked sec-ond. It just goes to show that the commitment to the team really pays off.
S&J: What lasting legacy do you hope EFrT can leave in the McMaster and/or Hamilton com-munity?
SD: That’s a hard question. If I think about all of the different aspects of our team that are important to me, one would be ensuring that we continue to provide an extremely high quality of care. Another thing that I am constantly working to improve upon is team relations. Not only does this improve the quality of our response, it also makes everything much more enjoyable for us responders.
EFRT: The Personal Experience
S&J: Why did you choose to join EFrT?
SD: For much of my life, I was extremely interested in applying my first aid knowledge, but I never really had the chance to. Also, coming in to my first year at Mc-Master, I wanted to find a way to give back to the com-munity. It’s funny because my roommate was applying, so I took a first aid course the week before in order to be able to apply as well. Had I not had that 30-second conversation with my roommate, I don’t know where my life would be right now.
EFRT Interview Series: Sachin Doshi, Director
“I think something we’ve done well is keep up our reputation as one of the strongest first response teams in Ontario and even in North America.”

THE MUSE • WINTER 2016
22S&J: What’s the most satisfying aspect of being a part of the EFrT team?
SD: It would probably be the amount that I can learn being part of EFRT. I think I can say that I’ve learned as much from EFRT as I have in a lot of my courses. On top of the hands-on skills that we learn, there are lots of soft skills that are gradually developed. Also, we’re all such good friends with each other; I don’t know who else I would have met had it not been for EFRT.
S&J: How important is EFrT to you? How im-portant is EFrT’s role at McMaster?
SD: I can’t quantify it, but EFRT is extremely import-ant to me. Sometimes, I’ll compromise something like academics for EFRT be-cause that’s how much it means to me. It’s given me so much that I want to give back to the team. In terms of how import-ant it is at McMaster, it’s one of those things where you don’t notice it’s there until it’s gone. I believe the sense of security and the education we provide to the McMaster community is extremely important for its well-being.
S&J: What is the most important thing you have learned from being with EFrT?
SD: The most surprising and important thing that I have realized from being with EFRT is how well a team can come together to create one cohesive unit, even though every member is unique and different from the next. It’s interesting how having a common goal or interest can bring all of us with vastly diverse back-grounds together and become so close.
The People of EFRT
S&J: What really is in one of your bags?
SD: We have three responders on call, so each pack is distributed with different equipment. The unfortu-nate thing is that we have to bring all of our equipment with us to each call because we have to anticipate any and every situation. Each pack contains an assessment kit, oxygen, trauma kit, personal protective equipment, symptom relief drugs, and more. Equipment such as an automated external defibrillator [used for diagnos-ing and treating cardiac arrhythmias] and noninvasive
blood pressure amplifier are in one kit only; we have to split up these resources accordingly when responding to multiple calls. I weighed a pack once and found that its weight ranges from 30 to 35 pounds. You get quite the workout.
S&J: What are you currently studying? Why?
SD: I switched in to the Biomedical Discovery and Commercialization (BDC) program from Bachelor of Health Sciences. I wanted to broaden my knowledge base, specifically with respect to commerce.
S&J: What’s your best timesaving shortcut?
SD: I like to multitask and do things on the go; being a huge tech person helps with that. So, I’ll have my phone, tablet, and com-puter lined up with things to do at all times. If I’m walking between places, I’ll have something to do on my phone. If I’m eat-
ing dinner, I’ll watch TV, and message a bunch of peo-ple at the same time.
S&J: What everyday thing are you better at than everyone else?
SD: Being Sachin. Personally, I don’t think that I’m better at one particular thing than anyone else. It’s more of the unique combination of skills that I can bring to the team.
S&J: What is the best advice you’ve ever re-ceived?
SD: I’ve learned, especially through my role as EFRT director, that you’re going to make a lot of difficult de-cisions that people may or may not agree with. Despite this, it’s important to stay focused on the long-term goals motivating these decisions and to be confident with your choices.
“It’s given me so much that I want to give back to the team.”
EFRT Interview Series: Sachin Doshi, Director

I had a preconceived notion of what health meant. After 15 years in the education system, I could re-
cite countless theories from my first year psychology class, as well as the names of anatomical structures. I believed that if I simply dedicated my time to un-derstanding the biology, I’d be equipped to solve problems facing modern day health issues. I trudged through late nights and long group meetings in order to satisfy my curiosity for human biology, with the hope that one day I could use it to deliver the best standard of medical care. Hence, when I began volun-teering to take patient histories in a cardiology clin-ic, I naturally repeated my cycle of questioning and learning.
Each case presented a series of disjoint puzzle pieces. What events occurred prior to the sudden chest pain? Do the results from the diagnostic tests provide any clues? Did I miss anything from their past medical history? My ability to sort through the data ultimately had an impact on people, and thus ev-ery day, I strived to learn more and more. Although I always loved hearing about other patients’ lives, I felt slightly inconvenienced when patients would diverge on tangents unrelated to the case, as it distracted me from the biology. I felt it was taking away from my ability to focus on putting these pieces together, and hence affecting the doctor’s work in delivering the most accurate diagnosis for these patients.
However, as time progressed, I noticed that a bot-tle of pills and a name to an illness was not enough. Throughout their time in the clinic, patients would give momentary glimpses into their lives. These ranged from simple things like what they were mak-ing for dinner that day, to the hardships experienced while taking care of a spouse who is also ill. Each patient carries their own story with them; their own blissful moments accompanied by immense hard-ships. And many of the patients sought for their sto-ries to be understood.
Slowly, I began to draw connections. By genuinely listening to patients’ stories, I was beginning to un-derstand why it was so difficult for certain people to alter their smoking and eating habits, despite know-ing the negative consequences. It no longer startled me to see the statistics on the news regarding hospi-tal visits from healthy, but lonely individuals seek-ing company. The burden of disease, as I witnessed first-hand, fell beyond the free nerve endings that detected pain or the biological entities that were af-fected. Disease crept into every aspect of life, includ-ing the way people interact with their loved ones or the ability to continue with activities that gave them joy. It opened my eyes to a deeper understanding of health, outside of the bounds of my textbook pages.
Health is not simply the absence of illnesses. Our health care technologies and services are centered on diseases, in order to provide the most efficient diag-noses and treatments. However, we cannot lose sight of the fact that our goal is to treat patients, not diseas-es. Each patient that enters the clinic brings along a wealth of experiences that have shaped them into the person they are today. As doctors, nurses, and volun-teers, we should take the time to understand the pa-tient as a whole, rather than only listen for risk factors of the disease and whether the symptoms line up with whatever we suspect the differential diagnosis to be.
Although this approach requires a much greater amount of patience and listening, it ultimately rings true to the pillars of humanistic healthcare. When people exhibit negative attitudes, it is important to approach the situation with the understanding that underlying hardships may greatly influence their be-haviour. People who are unable to change their un-healthy lifestyle habits don’t need to be accused of their choices. Instead, they may want someone to lis-ten to why they have been unable to change. Our goal should be to provide care, rather than simply striving to cure the disease at hand.
“ our goal is to treat patients, not diseases.”ABOUT THE AUTHOR - Jean is a second year student
in the Global Health Specialization of the Bachelor of Health Sciences Program. As part of the Advocacy Team for Engineers Without Borders, she is passionate about international development. She also enjoys play-ing piano, running, photography, and making people smile.
ARTISTAdhora Mir

THE MUSE • WINTER 2016
25
***
JUST OBSERvEby Isabella Fan
***
At William J. McCordic School, ob-servation is powerful. Though it
holds the title of a school for students with developmental disabilities, these students offer a depth of perspective that goes far beyond face value. While there, I befriended the bus driver who drove these students to and from school. Once, as I was helping wheel the kids into the classrooms, he asked me why I was helping out there rather than working in a hospital setting, since I was interested in healthcare. The truth was, I did not want to interact with chil-dren through the systematic screens of hospital rituals.
Here, even though I had to keep an eye out for physical discomforts and contact the nurse for checkups, these occurrences were infrequent. I was es-sentially free to observe and interact without distractions. Intriguing reali-zations about these children emerged, as I watched them shatter preconceived notions about individuals with disabil-ities.
Intelligence is reputably demon-strated by complex physical or verbal means. Raw intelligence, however, can be shown by engaging others through emotional communication. McCordic students do not have the privileges of physical or verbal abilities. Neverthe-less, they have demonstrated intelli-gence in its rawest form.
Two students, Evan and Ben, have particularly convinced me of this mas-tery. Whenever I asked Evan about his birds or I played his favourite Elvis song, Can’t help falling in love, he would
Just Observe
ARTISTKelly Dong

THE MUSE • WINTER 2016
26lift his head and express a powerful grin, warming even the most insensitive nerves in my body, tightened from the long, early hours. His smile appeared to have unbuckled his spirit for a mo-ment to take a blissful break from the silence in the wheelchair. And I could sense the glee he felt. With his grin, Evan showed me how he was sensitive to music, had passions and preferences, and was aware of changing surround-ings. Words were not necessary in these enlightening interactions.
Ambition can be another measure of intelligence. Ben was cleverly am-bitious, but quiet. While the teachers knew he was verbal, they rarely heard him speak. After spending time with Ben, I realized that motivation for re-ward was what broke the ice. During outings, he was always unusually alert and responsive, especially when I pushed his wheelchair at faster speeds. One day I decided to take him around a circular path in the building, and told him we were going on a race – with safety precautions in mind, of course.
He greatly enjoyed the ride. Fol-lowing the first round, I made a bargain with him. If I took him on another ride,
he would have to say something to me. The deal was miraculously accepted with a “good morning” and “thank you” – phrases he had not spoken in years! Ben possessed ambition, a quality unique to humankind. His cognisance of how to benefit from negotiations is a manifestation of the raw nature of hu-man ability. My interactions with him opened my eyes to the same clever in-telligence in other students.
I felt great joy watching these stu-dents experience the world around them, but not every moment here was pleasant. I had my frustrations in fail-ing to understand or communicate with the children. Yet even more frus-trating was how sympathy can make people less cautious with their words. One day, Evan was lying comfortably in the play area. Some of the volunteers and I were encouraging him to nudge balls with his knees, when the teach-er came over. Having known Evan for years, the teacher reflected out loud, “his legs weren’t bent like this. We got them straight three years ago. It’s a shame.” I was stunned.
At fourteen years old, and despite not being verbal and capable of ex-
pressing his emotions, Evan certainly understood the negative connotation behind the words,. He quietly looked down. I realized then that the teacher’s pity for Evan’s physical paralysis was overgeneralized to a mental paralysis. He forgot that Evan’s intelligence and emotions were still very much vibrant and present. This is the danger of sym-pathy, as a lack of caution causes words to enter the bounds of insult. At times like these, it is difficult to be empathetic since we have never experienced these students’ struggles. Even so, we must try our best to empathize with their sit-uations to avoid the slip-ups of conde-sending sympathy.
I might never be able to remove myself from the observer’s position to truly grasp what the students are ex-periencing. The best I can do is use an emotional connection to probe into their source of relief and identity. They have a lot to reveal. Their existence is raw, their essence stripped of artificial human behaviours, and they are left to cultivate the root of human nature: emotions.
ABOUT THE AUTHOR - A first year Bachelor of Health Sciences student at McMaster University, Isabella writes as a ritual, and has interests in philosophy, paintings, and classical music.
Just Observe
***“Wise men say only fools rush in”
to Den lille havfrue who by the watersideperished for the affected human soul.
Now the colours of Copenhagen remember the vibrancy of her sentiments
while the tour guide narrates her tale and Andersen whispers above the air
Be happy with who you are.***

MAKE MEMORIESMATTERTM

ABOUT THE AUTHOR - Julia Xiong is a second year student in the BHSc program. She has been volunteering as a clinical worker in her local hospital for several years.
THE MUSE • WINTER 2016
28
The Emotional Aspect of Patient Care: A volunteer’s Perspective by Julia [email protected]
Little could have prepared me for the emotional chal-lenges of my hospital volunteer placement. Going
into the experience, I expected it to be a lot more mech-anized; my training adequately prepared me for basic safety and patient care. But I had never provided care for people who were as vulnerable and fragile as hos-pital patients. My previous volunteer experiences with the children’s recreation sector were full of able-bodied human beings able to take care of themselves.
But at the hospital, the full reality of what was ex-pected of me did not sink in until my first day. What I saw were people who needed help. Easy enough, right? Their bodies were broken in some way and it was the responsibility of the doctor and the healthcare team to fix them. But what I was not expecting was the number of people that opened up to me about their worries and pains, both physical and emotional. The depth of these talks was novel to me.
At the beginning, it was difficult for me to respond. I was used to giving advice to my friends and peers who needed help, but what wisdom could I possibly of-fer to someone who has traversed so many walks of life and experienced many more obstacles than I could ever imagine? As a human being, it was natural for me to feel like I needed to fix their prob-lems in some way.
The fact-of-the-matter was that in many cases, I couldn’t. Sure, I could offer the lady who was wor-ried about not being able to reach her kids a hospital phone line free of cost. But how could I respond to patients who shared problems that were beyond the scope of my responsibilities as a volunteer?
One vignette that pops into my mind was my talk with a senior lady in my unit. She told me about how she was due out of the hospital soon. When she said this though, she did not smile; there was no happiness in her eyes like I was used to seeing with other patients.
So I asked why. She told me that she lived in a senior home and did not want to return because of the loneli-ness. At the hospital, she had healthcare professionals visiting her and volunteers to talk to her. At the senior home, she had no family and no one she could connect with. As a university student, this was not something I could fully empathize with. So I kept asking questions, partly because I wanted her to feel better and was in-terested in what she had to say, and partly because, frankly, I didn’t know what else to do.
Throughout my experience I could never remove myself from the feeling of being obligated to fix my pa-tients’ problems. But if I do the best I can, hopefully that is enough. I hope that by listening to their worries, I can connect with them and help them feel better. And I have seen this with numerous volunteers: a patient tells them that they need something, and their auto-matic reflex is to try to fix it. And the guilt the volunteer feels when they can’t help is ubiquitous. However, by being there and listening to the patient’s concerns, we
are able to give them an emotional outlet. Per-haps these patients are sharing their sto-
ries not because they think we can fix their woes, but because they know
we will listen.
ARTISTAdhora Mir

THE MUSE • WINTER 2016
29
STAFFEditor-in-chiefAnna Goshua
Managing EditorIrina Sverdlichenko
Creative DirectorMichael Sun
Financial CoordinatorLucy Luo
Community Engagement ManagerSamuel Wu
Editorial TeamDarwin ChanMichal CoretAlex FlorescuRyann Kwann Joon MunIsabella FanyBhagyashree SharmaCarolyn TanMarina WangIshan Aditya
Graphics and Layout TeamAmy AjaySama AnvariAdhora MirJess BlackwoodKelly Dong Lauren LiuAlice LuNikesh Pandey Shira Weiss
Staff

THE MUSE • WINTER 2016
30
BACK COVER