Embed Size (px)
Citation preview
COLLEGE EXAMINATION
The MRCGP examination and its methods.II: MCQ paperJ. H. WALKER, frccp
I. M. STANLEY, frccp
T. L. VENABLES, frccp
E. C. CAMBRILL, frccp
G. K. H. HODGKIN, frccp
'T'HE multiple choice question (MCQ) paper is direct--* ed to sampling the candidate's abilities in the cogni¬
tive domain (mainly at the level of (a) in the Charvat,McGuire and Parson's classification; rarely reachingand never exceeding (d). See part I, page 662, Octoberissue of the Journal.) Thus it is almost entirely con¬
cerned with testing factual recall.Until 1982 the MCQ paper in the MRCGP examin¬
ation consisted of 90 questions of the independent true-false format, in which an opening statement or stem isfollowed by five items, each of which may be correct or
is a plausible distractor. As negative marking operatesfor incorrect responses, the candidate is provided withthe option of answering 'don't know'.The subject matter of the 90-question paper con-
formed approximately, to the proportions shown inTable 1. From the autumn of 1982 the number ofquestions was reduced to 60 and the proportion isshown in Table 2.Marking is performed automatically by the optical
scanning of sheets on which the candidate has enteredhis preferred completions. The mark awarded to thecandidate for each question is the result of the positiveand negative scores of the items; the 'don't know' or
uncompleted response attracting no score. This raw
score is subsequently amended (see below).Questions are constructed by the MCQ compilers, by
a group of examiners and recently by a group composedof invited Members who have performed outstandinglyin the examination. To be accepted, all questions mustbe supported by substantial references.
J. H. Walker, Professor of Family and Community Medicine, New¬castle upon Tyne; I. M. Stanley, Lecturer in General Practice,University of Leeds; T. L. Venables, General Practitioner, Notting¬ham; E. C. Gambrill, General Practitioner, Crawley, Sussex; G. K. H.Hodgkin, General Practitioner, Great Ayton, Cleveland.
© Journal of the Royal College of General Practitioners, 1983, 33,732-737.
These draft questions are looked at briefly by a smallgroup of examiners before being circulated more widelyto members ofthe Panel of Examiners. Each question indraft form is submitted to at least four examiners infull-time general practice. They are asked to commentspecifically on relevance, clarity of wording, level ofdifficulty and acceptability for the examination. Thisprocess results in the rejection of some questions andthe amendment of many others.
Table 1. The number of questions allocated to each subjectin the 90-question paper.General medicinePsychiatryObstetrics and gynaecologyTherapeuticsPaediatricsSurgical diagnosisENT, opthalmology,dermatology
Community medicine
20181210105
105
Table 2. The number of questions allocated to each subjectin the 60-question paper.General medicineTherapeuticsObstetrics and gynaecologyPaediatricsPsychiatrySurgical diagnosisENTDermatologyEyesSocial and legal aspectsEpidemiology and statisticsPractice organization
1286664443322
732 Journal of the Royal College of General Practitioners, November 1983
J. H. Walker et al.
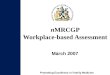
Figure 1. Examples of multiple choice questions and answers.
Journal of the Royal College of General Practitioners, November 1983 733
J. H. Walker et al.
At all stages from draft to printer's proofs thesvording of questions is scrutinized for ambiguity. Al¬though more care goes into the construction and evalua¬tion of questions, there is no substitute for the processof testing them in the examination setting. At thepresent time the MCQ paper contains roughly equalnumbers of new and previously used questions.As a by-product of computer marking, aconsiderable
amount of statistical information becomes availablesoon after each examination. This information is im¬portant in two areas. The first of these is the calculationof a correlation coefficient for each question. Thecoefficients are used to derive the final (or amended)percentage mark of each candidate. The details need notconcern us, but the effect of this is to reduce theweighting of questions which do not discriminate be¬tween high-scoring and low-scoring candidates. This is agood example of peer referencing. Data from the com¬
puter are also used to scrutinize the discriminatingpower of questions and items, in order to improve themfor future use. Some questions with low overall correla¬tion are rejected; the majority need attention to one or
more items. Item analysis like that of questions is basedon correlation with overall score, but provides in addi¬tion information on the distribution of candidates be¬tween 'correct', 'incorrect' and 'don't know'. Thusdifficulty and discrimination may be assessed. Thisprocess of question refinement is protracted and timeconsuming, but is an essential complement to the pro¬cess of question construction. With the present systemof amending candidate scores, correlation coefficients
of a high order of significance must remain the aim ofthe MCQ compilers.The large number of candidates and the use of
automatic marking means that the MCQ paper is inher-ently reliable. Content validity is potentially high also,but (like all questions of validity) requires judgements tobe made on matters such as relevance or difficulty, if itis to be optimal. In the MRCGP examination, as we
have seen, these judgements are shared between thecompilers of the paper and about 20 members of thePanel of Examiners. If, despite this, some questions oflow discriminating power are used, their weighting inthe final mark is reduced by a process involving peerreferencing.
This balanced arrangement is not of course perfeet.Examiners may disagree about relevance. A poorlydiscriminating question may have other functions, forexample, to extend the curriculum into areas not seen bythe candidates as relevant. It has been known for sometime that the process of amending scores tends toincrease the difficulty of assessing factual knowledgeseen as peripheral by the majority of candidates. Thishas led other examining bodies to abandon the process.While a significant proportion of new, and thereforeuntested, questions was in use, the amended score
provided an important safeguard for the candidate. Theissue is now being reconsidered because of the more
efficient use of questions in a smaller 60-question paper.Examples of current multiple choice questions and
answers, provided by Dr Andrew Belton, the presentMCQ Coordinator, are shown in Figure 1.
Ill: TEQ or short notes paper'T'HE MRCGP examination has contained traditional*- essay questions (TEQ) since its inception. These are
designed to test candidates in the cognitive domain butalso to a lesser extent assess attitudes. The technique hastwo main advantages: the questions provide the oppor¬tunity to test the candidate's abilities in organizing hisknowledge and expressing it in written form and are
comparatively easy to construct.The main disadvantages include the fact that con-
straints of time limit the number of questions, and thusthe range of content which can be tested, and thatmarking is time consuming, and to a considerable extent
subjective and less reliable than that of some otherwritten techniques. English expression and legibility are
important, and most doctors who wish to express theirknowledge logically in written form find this difficult toachieve without the opportunity for redrafting.im¬possible in the context of an examination.The College has made several attempts to minimize
these disadvantages. Content validity has been increasedby careful selection of questions from the five areas ofclinical practice. Of the three questions, one is usuallyselected from area 1.clinical practice, health and dis¬ease. By subdividing the question and at times using theshort notes format, a single question can be based on
areas 2 or 3.human development or human behaviour,and the third on areas 4 or 5.medicine and society or
the practice.Questions are constructed by members ofthe Panel of
Examiners and are refined and edited at examiners'workshops by subgroups who also construct and weightthe marking schedules. Each script is marked by two
independent examiners using schedules which allocateapproximately 70 per cent of the marks to content. Upto 30 per cent of the marks are available at the examin-er's discretion, and the process is facilitated by the use
of marking grids. The marks for each candidate are
collated by the computer, which produces a printout
734 Journal of the Royal College of General Practitioners, November 1983
J. H. Walker et al.
identifying any discrepancy between examiners. When a
discrepancy is capable of affecting a candidate's perfor¬mance overall, the script can be assessed by a thirdexaminer.The validity of the TEQ is satisfactory. Its reliability
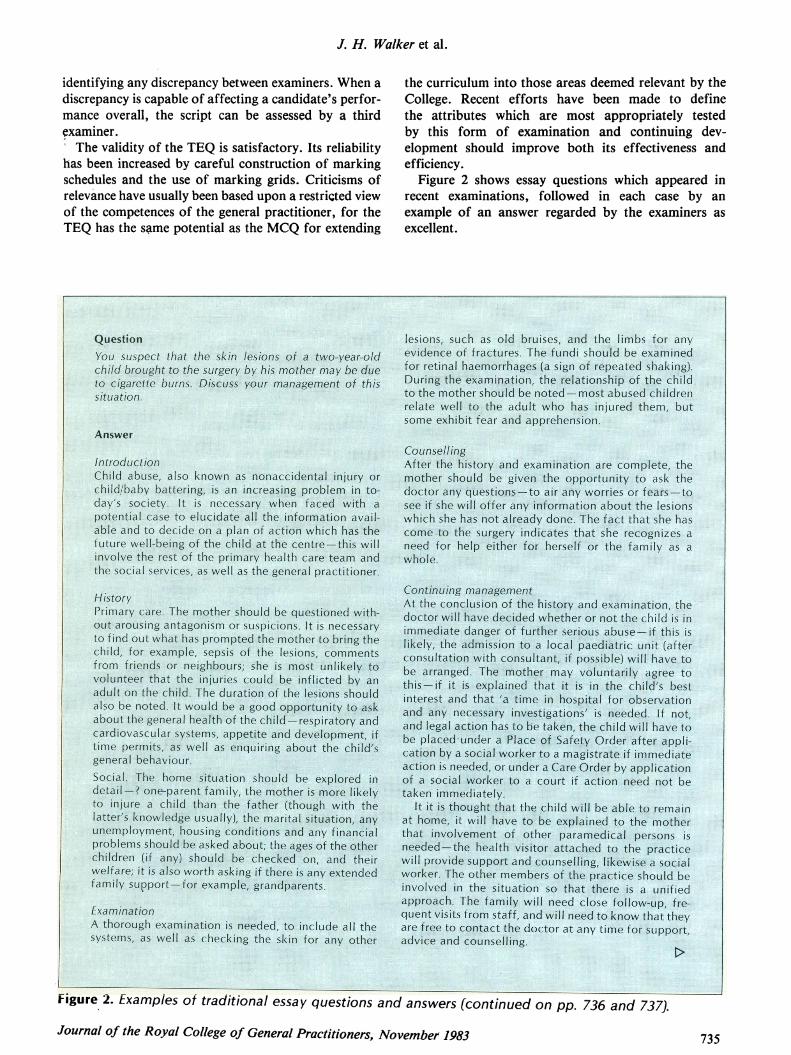
has been increased by careful construction of markingschedules and the use of marking grids. Criticisms ofrelevance have usually been based upon a restricted viewof the competences of the general practitioner, for theTEQ has the s^me potential as the MCQ for extending
the curriculum into those areas deemed relevant by theCollege. Recent efforts have been made to definethe attributes which are most appropriately testedby this form of examination and continuing dev¬elopment should improve both its effectiveness andefficiency.
Figure 2 shows essay questions which appeared inrecent examinations, followed in each case by an
example of an answer regarded by the examiners as
excellent.
!-:V:f::iifS:?:-'!-^#:i;Vi-: ¦Viffi;^¦::.;::.-5-.:i;:!:;:'. :.¦;. ^ife; ;¦ ¦.:¦¦¦
,-¦«¦,.,.¦.., .,,,«::,. .«^- .,:;:;.:.::-.,,,«,,,,: :.,^ *^
=: ="v*.I:fv:-":"¦:=""-¦" '..*"':'::::^::--^ ''"::V:*." 11*111= -=_=
Answer.-',.'' ¦'''¦*¦v'' J-^.'T'\\'.?.~'.'.,,-"£.-:' ''7?*7.''\'.''-:7' 'B7.':' ^^'''¦'¦'Jfr^- '^:f-:-:'':?^- "'^ "'''^ ''^7''
¦ftmarl^il^
iJilavetp
§8:'' -:-^$^^#.^i^»^Hi iriiiiiihiillrig. «;¦
;:jhiSfti|;:v':
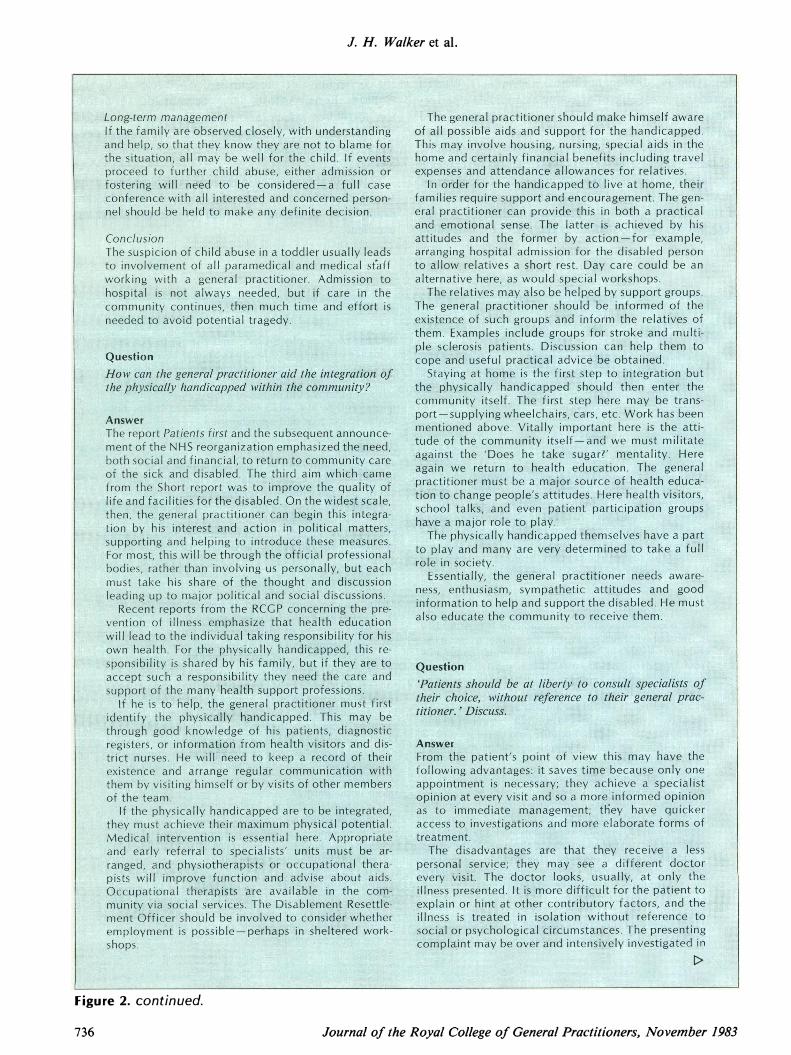
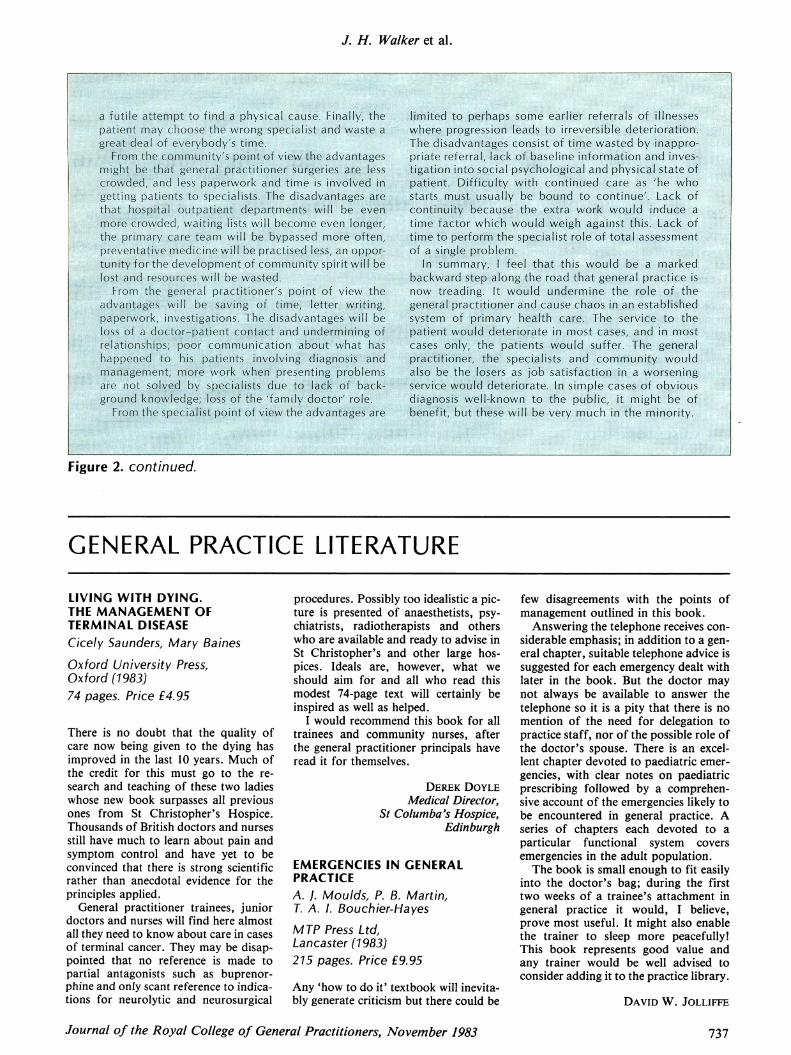
Figure 2. Examples of traditional essay questions and answers (continued on pp. 736 and 737).Journal of the Royal College of General Practitioners, November 1983 735
J. H. Walker et al.
Lonf-term marnggmmtIftt^f^niJyaref"andJ^elp,;#o thM -th*the stoattoh, all m*proceed tp
osely, with understandingHm itey #re fipt to Wamt Iori wMf for t^ ctttld; f '""'"
ConclusionThe suspicion of chiid abuse in a toddler usually leadsto involvement of all paramedical and medical staffworking with a general practitioner. Admission to
The general practitioner should make himself awareof all possible aids and support for the handicapped.hSme aritf certiMiirY finan^totfterlrflts including travel
families require support and <
«fifrprrt^it|Ji(B#W» -: ?§w*'#<tlwde-?W* >in i-balfe a practicalajpiifrjaotional ?«*$* The -Jattfr4s achieved by hisattitudes and tHe former by action.for example,arranging hospital admission for the disabled personto allow relatives a short rest, Day care could be analternative here, as woutd special workshops.
then effter^ :thfe
j^wer'-*"'--1^Tr« reporty^lSV**"¥ ^°^f here * *?i£^"¦..¦*.... ftiitem*N community itself.and we must mmtate
the 'Does he take sugar?' mentality. Herereturn to IwsLlt:^ ^cfaiuCj^tort-. The general'""'"'. "|Cah
ment ofthe NHS reorganlzatiteths<
¦¦¦¦Ilfeii
''^¦bociiesfS
vehtidto'cjwrirtead^
.JiMi^ awar# ¦¦;W^M^i^^i 'ii^^0SiSi^^^^'-»^.. goodiiirSrtatiQri to help*nd^^^lB&^i£iIi$d^ He rhUst;
:tr)a|ii«|existenceth^-i%*iof the teanv
,.jh|fy:^|i|f.
'j'T'^'-'VlV^'^ <;~;
.lii!^
WtestigatwpS-:.
Figure 2. continued.
736 Journal of the Royal College of General Practitioners, November 1983
J. H. Walker et al.
-::::--,:.:....: -::...:. :...... .......-.....:......:.. t.:.. .......,i.t!T:i,.:1. ...i: <..::-....--,-. ... ,..: ,.:.%.,,.:.,,,.::,%... .:,:,.Fi_z ..,;-t;::Z:::;:- .:.%;: ...::::_:.. .:.:....,. .,.... .:..::::.:...%%. :. .": ::......::%% ::-::!-: ,: .., ..:.t :" -,-...: ...;".%..N.,:%t:%:,........-::-. ,.:.... .: .:...:- -1......:...-:..:-:::.:. .-.-.. .-.: ,:. .. ...:...:......... :... .....:%..:.... .: :....:.,,.i;%i--,.--iL,..., :!. -:.,.;.ii.,7,!,.--,,..j, :i, ...- .. .t,.. i..--------,ii: !.,-,!!;....4..- .......... ...........%-, ..i. .,,V.*iNai .i .. ,.,%::4 .:. ..::::" ..::, .,. .i. t.A!.:i1--1,,1,.i:: .. -.:., ;:.!!--!!..: .::.!!..:::.
:,.:.:-:....:.... ..:,.....: .R%. i.-MN. :..:,- :.,! ,:,.:.. ,:,: ..... ::..%:::: ::.,.. ...., -::: ::.:,":.. :... ..%.::..,.... .-.t".,-'i "."'s. it1i,.-.,:i ..:.:-:::.:."',...... ...-.-..........,..:.:.::-.- -.-::... ..-.-. :-:: ,: :. --.....::,":......::..."'..t-.-... :.. .,: ....;,,,....
.!Iij .:: %.:%:t,,f:2,,, .,,..iT::.. :..: "" 3.%:M, :...."z.,.si;...?...."..:..ji...,I:i.....:j':.-.. :,--,
.:". ,. ,F: -:. -::4:. -. .: ,, :, .,,,,L-,,,--.-i ..e,..:."...-,.!ZWi..Z, W:ai Tv K.::x:.i:,-.j-..-I ..;.i iki.-,, -,,;..f::iio%..:I. x .5f?.J:?..I. ,,..%,.1;........ ..... .: .:. :.:: .:.::c .::::,.:::: ::.::.Hs,.,,.:--.. iii-k, ,,--,..::.:.;::i-..- .,-:..:---- -.:..t.....t :;;.:.:-.1. .... ., ...:. ..............., C'I'i..
-",,:,"%:........ ::".: i..:...%.,..-,-,;.-.-,...,-V;- -X .---..:..... :%,I.:... -t.:-..::,:.:.1..1......:.. :1. .%. ",". ". i,,.:, "' ....:.....:.....,.1 ... .., ... .. g,.,,-,-- 77. -,:--...,", ,,-,---:- ..;I-1.. .... :.. .....: .....-.......-I..: .:. :.:I.: ,. :..:...1.t......-.:..-..:..I-;'.... ..: .-..:: :.:2 .,..,..,....,:U:......I-,.- -,st%!.My.... :,!,.--- ,;,... e., :", :7.t'.. .,: :r.,%.:%--.: 4-. .:.1.,., ..-:;"C ..,,.'...z. -...-... :,-I.-.......:%.......... .!.:.:... .-,,-,-. -..,%. ,............% .,,.,,.t:. ,. .,.%:::. ,.:.% ...- 4%M....I...... .., .:.....r,.-... ......:.......;...-.: -:: .::. ..M.. ......:..t.-...-.. .,:.: ......: "... -:.,.,: %.....: %... ....,.7.!,--......:,....:.:." :... :', ,... -,..,.. ....,..%..
,.:.::t. :::... .... .....:-....N. ..:.............:....:% .:: :t..:.... :-......1..- ..:.......-"........ .. :-.... ..-:: .....,..........,......:..:.. %..%...... .:::-- .: .....-.....: -..A: .:.: ........,1'. :1: :%.--..:: .:...::-- -`-.,-t.;:;;;! i.!..I.,-,.,..;:::..:.:: ....,4,.. .......-,.. .....:- %.............-"...........
,:.::: -:;?:!.:::, ., i, :,:::.:,:: ::: :::.."....'.%:t;,;.::,::,:::.,:, -.-::-.i.:::t;i:,xI: .::... :,,,,"",,".%94:. .-Y. %::..:. %. .: 1% .: ......",,,-, ,, ""....::::::...:-::::. -..;;..-i;..i ii:.:: -;;.:..:::!.:,,;: "', ::,:.: ... ..:;-.;.., .. .:. --.::!%-!!.-.%:!-, ,:i.,: ..%..:...:: ,,::L.:..i.lt:.;, ......:.....I.:......%........... ....:i:: !!!:.-Iii..*,ii;i4..i, --:4:i ,-......,.- .: .....:......,..:ji:!.::,.."i.%:7::,: .:: .'. .:,.%,t-:::..P,,?,,i,:. ... :..... -.. -,:x.l.., ::% x:-i!:: ::,...-:: ..;:::.%;.::- .,. t:,! ,i....,.-,- :.t -4:.-.::%W......._-.%:.:........-.:-.:-.ip..i; .. "'... .,X.-..... .....:......::F::-?;.i:: .. .-: it;:. ........,.,.::::.2!:;i :... .,,..1....:....I...: .! i! ..: :.i i..; i.i im.TiiU.: i: .;!%ihi.i!i..i! :.: :s:; :1.;%.i. :.,-.'..'.ir-,...'.'.i?'..f...ii.?.:.: !.-.. ..::::. :,,. ....... ... .:;;-.: i!i::::jl...:I.l..'-.,:.:i.....'.: i:::..'4..::...";:..:i.i:.'.'., ..:,.:.
it N:... .1,....... .;.:.!...:i.:%::.. ,::. M....,.,:!:...:......V::,-$4. f..:.: i.: ii.::1 ::: ... ...,,, -X:44 --. :...... ::;::::,%:: .....:.. :i;.;; .,,,;x::I1,:i. .:::
.., t.. :. !. -: N.. .::
-.X::--.:i:::.::.ii.H...I.... I.-..::.,.:...:..::.,%:.%-:--%. ..:,-,,,.;..: -.. ,. ::: ,.,-,:: ...,,........:.. -::
.:4.:. ..::.-. -son.. ...... --erra, ...:--..:.. :::- 4..:et.-tI --n:..:"Ni.P,,,--... i!...::,.,.:.i...;:..i..,..l:...i..:.'..iiiss.i...i..ll..::.il:,.",.::i":::.::..i....:iiii ..... i;.F-.,:,,.H:;iii%:,--: ... ::".,%:"::, .:''QW, .!0!!::.,.!!,. i:-,.S --:.-..i.s:l.:ip.%.::::i:;,;..i, -, .---.A.V. .N.
.... ".--'-'ilfl ",--:- '--"-'--.: :!% :,: ......,,%4,6.--'$..,4 ... .:.
.:,--:6 ----- -,'':,:::" ,:,`...;i.!..:-:_,ii.i..."...'i"...6;.......,.,,.ij:t.,.---..j*.. ..-,: ... ...."'.,i:.,% ... ;. ..:.:::!.!-:: i:::::: ... .."',," , , '':..::::4 ...:i,,,-,--i.gi ....i;;..I!.:.j: 14.',-' -,,,.,,.i ils'. ..f:::- V:Y. --:: ""....:,,,,,,it'....... :....... ----.: J.j.iI.!.I.
AL]ta1'.... Je..:::::.: ...
"P.:...-::%-,.i::e..-,,,,,. ........44-H.."I .jwqld."'I,''ifi:......es
....I.!--X::-.- :jN::!..::::.. ii:c :.:i.?.:.:;":..!;..,i.:.'i:,.i. .:;...E!..!!.!i..;11) ''
...,: ": .:%.:...: :,X:.: .::. .:: ..... :.: ..:..... .....-......'',...,.....-.:,-,,;,:..- .. ..:. ........-...::-
"of fiii..... .."..'N.1 ...M'.,%:..:!::..i:.i.:::i;..f..i...I.::.ii---:ii.:..:.. -,:.,:!..:...'.''..-.-...
... ,:!-:,,,,.,1.11. .. hi-i'll,iii.-t.ii: ......:Ti..:.,? ::. s::-,!.:..`!::.:,!!.:.!!::. .:.%-.............X:..."...-:X--:M..,::,:,. .:..., ....: %iii.i:i...!:;..f:''.....i,,'f...,::ii.l:..lli,::;::..'.... -.....-....:t,:,.:::
:-. -j' F,:,: ......xN--.,- ........,,"',.... I........N.:..:-I......:%..: ....:::."..,:..1.:.:.I .:... --.:.... -:'to i'',,:rsible"Aetefl-646-'' "', !......:--.::,:.-:::--.. .......0e...:,.: i.:: ,-, 'a.,- -..%,,:.- .,, ..:. t--`..,,`-.!i--,,-----,--.I.7:U,hie 11-.-4 .......---
-:1le '' '" 'd '" 11" ': ,% ,,, ,, ,,, ,.,, "", :::.::::: ::: ...::-.."---'":.:..::::..e. .%._Y..._,,..,t...r.:: ..,,j,,..:!:... .. r- ---,-....::, :.: -.:-. -,;:.I%.Y..-.---:n. W... e.:,a..:.. .-'-'..-'. ----,-.-----,,.i:!M-,,:-I.....,- ....:t 09- ..-srreveI...I.. ...i---w lig-,.!$-,,p,III....:he.'6n.111I I... -S. .......i."., ...": 1: 4d':: .:.:%. am, ..:.% .:."",.-.......:j. ..::..,P0.K*..,...- .t...-.: .::....,.....,... ....:-.I-,:,::4-.:. .....I..... .:. :.%.:. ....%......7,:.-1 ::", -I-,- -Iwi._...:.::..::,...: -.-'.. ..... ... ... ...... ... ... ..... ....t,'". .........4.::".'.
:::....:-- :. er........ ..-- .. ''':..,.. .......%
.: %.-
:,,..,-,-.,..,---V!-.......: .:..:::::":::-S-... .N... -:--.:.t,,.:..-::.:t.::. -..," t of -titne. wasted:-by... :.s tmiie-:. .."-,0- -. - --
::::::..,. ""i. ..- ----...:: ..:: L, -.::-:::-:::,- .: 1f.". --,,,.,,: ,::.,.A"f.a! ....::,::M-:::.:....:,..-...... .::The Ab vant' Si ,PE -..x::-,:::-%..:1:,-...11 .... je....owi.,..!:!,......z.ial;.:..,....".I .,%,.,.....:.. ...... -. .........ws ..::-:: ....:.:-W....... ....- :.,..:..................:..::.': %,!v ..:::-:i;::7..;;Xji.::: -:... :.: .:::.: .... ...... ....:,,:1 -:::".--. .:.:.... ...... F:I.i.i:::Iii: ...---,: :.... ..... .......4. %..%:!i...-....i...i;iiii!;.i!i.:!!:.i.:!i:-:!i!..i:!;i....,,.... :.:j&:..:N .:: -:......:....:--1-.::X!-ji,,:::..i.-1.h:t 1%t .:4:.:!l ..::. .-,.,-.,.1;-:::!i;j.ii ,,,.... .- %. .:: ,.i::,-i:!,,..... .......
...:. IN.%,,,-.....:.- .!Iir .:-:.......,!;.H. ...:.. .AX:4.4F.;;;;... :.. !e""'It ,-, ---:!. '" ,: "'IF6 .. ...e... .,-:. .... .': -i;:!Ii-:`1411,, ".'s .vr :.:.:.. ''"-:-;m---;;.:i:::-- -% -i .1, --.A--.qq!i---%r-, ::::.. -:-i,i9t. .1-S J I .iiih r.M-11'...'-A 16 -", ,,:........iA. -, ,,i!i il!..i:i! .!.:i!!!
-....I............ .....%. .i. ..ii...Y:............... .....
,::..,
i:.!,,..I...., le .10-11., ....... .. .... ...,,i".k: .."" """,
.w i.1,11-"-- - `- -- -i.. i:!....,:..."".l...ifi.li...:i....;,'ij...!.?!.. :10i ....,"...,.,.... .., r........" I.tite" wo, -s -1.Wf.i!1416 -61---P!. -',',",.a..... -,
N----d.'.i.t...."'91..'.:::I:...::..!...-S::..ii.::i.:!:...':i i:..,.'..:...,i:i:.z.iii;:...i::...i:.l:i.:,:.,:, ,..;i:ii., ..:.:.:::bii::...iiel,.:.",.."fli%:.':i.:ii- t:, ,: [..i--,..`.,i,-1.i.:i-e "'.11', A.6. ef..:...
.:,.:; ::: V-V. ,"I..:::,M;::..::.::. .: ... .::".,., .!.i..!.ii..,1::-.:::-: :- :.-- --:-: --::.
:.:..:fle,,..5---,,i ::..%.,..--;;...;.....::.::::::-:::-- 1c...1 :: ...:-: .N.---n .. ....---,,- ....
GENERAL PRACTICE LITERATURE
LIVING WITH DYING.THE MANAGEMENT OFTERMINAL DISEASECicely Saunders, Mary Baines
Oxford University Press,Oxford (1983)74 pages. Price £4.95
There is no doubt that the quality ofcare now being given to the dying hasimproved in the last 10 years. Much ofthe credit for this must go to the re-search and teaching of these two ladieswhose new book surpasses all previousones from St Christopher's Hospice.Thousands of British doctors and nursesstill have much to learn about pain andsymptom control and have yet to beconvinced that there is strong scientificrather than anecdotal evidence for theprinciples applied.
General practitioner trainees, juniordoctors and nurses will find here almostall they need to know about care in casesof terminal cancer. They may be disap-pointed that no reference is made topartial antagonists such as buprenor-phine and only scant reference to indica-tions for neurolytic and neurosurgical
procedures. Possibly too idealistic a pic-ture is presented of anaesthetists, psy-chiatrists, radiotherapists and otherswho are available and ready to advise inSt Christopher's and other large hos-pices. Ideals are, however, what weshould aim for and all who read thismodest 74-page text will certainly beinspired as well as helped.
I would recommend this book for alltrainees and community nurses, afterthe general practitioner principals haveread it for themselves.
DEREK DOYLEMedical Director,
St Columba's Hospice,Edinburgh
EMERGENCIES IN GENERALPRACTICEA. J. Moulds, P. B. Martin,T. A. 1. Bouchier-HayesMTP Press Ltd,Lancaster (1983)215 pages. Price £9.95
Any 'how to do it' textbook will inevita-bly generate criticism but there could be
few disagreements with the points ofmanagement outlined in this book.Answering the telephone receives con-
siderable emphasis; in addition to a gen-eral chapter, suitable telephone advice issuggested for each emergency dealt withlater in the book. But the doctor maynot always be available to answer thetelephone so it is a pity that there is nomention of the need for delegation topractice staff, nor of the possible role ofthe doctor's spouse. There is an excel-lent chapter devoted to paediatric emer-gencies, with clear notes on paediatricprescribing followed by a comprehen-sive account of the emergencies likely tobe encountered in general practice. Aseries of chapters each devoted to aparticular functional system coversemergencies in the adult population.The book is small enough to fit easily
into the doctor's bag; during the firsttwo weeks of a trainee's attachment ingeneral practice it would, I believe,prove most useful. It might also enablethe trainer to sleep more peacefully!This book represents good value andany trainer would be well advised toconsider adding it to the practice library.
DAVID W. JOLLIFFE
Journal of the Royal College of General Practitioners, November 1983 737
![Tel e: 2698894 Fax: 2695188 E-mail: cgpsl@sltnet.lk ...cgpsl.org/wp-content/uploads/newsletters/Newsletter-March-April... · MRCGP [INT] OSCE Examination Ø ofSuccessful Academic](https://img.pdfslide.us/doc/110x75/5afc18c47f8b9a32348fddb5/tel-e-2698894-fax-2695188-e-mail-cgpsl-cgpslorgwp-contentuploadsnewslettersnewsletter-march-aprilmrcgp.jpg)


![EXAMINATION FOR MEMBERSHIP OF THE ROYAL …mitshs.org/Download/Syllabus.pdf · examination for membership of the royal college of general practitioners mrcgp [int] syllabus for the](https://img.pdfslide.us/doc/110x75/5b2b398d7f8b9a45198b51a1/examination-for-membership-of-the-royal-examination-for-membership-of-the-royal.jpg)

![MRCGP [INTERNATIONAL] BRUNEI - ihs.ubd.edu.bnihs.ubd.edu.bn/wp-content/uploads/2017/02/MRCGP-INT-BRUNEI...Module 2: OSCE 4. MRCGP International Examination Fee 10 5. Payment Procedures](https://img.pdfslide.us/doc/110x75/5aa66f037f8b9a1d728e6aa7/mrcgp-international-brunei-ihsubdedubnihsubdedubnwp-contentuploads201702mrcgp-int-bruneimodule.jpg)



![MRCGP [INTERNATIONAL] BRUNEI - ihs.ubd.edu.bnihs.ubd.edu.bn/wp-content/uploads/2018/03/MRCGP-INT-BRUNEI... · Module 2 Objective Structured Clinical Examinations (OSCE) – to be](https://img.pdfslide.us/doc/110x75/5afc18c47f8b9a32348fdd9f/mrcgp-international-brunei-ihsubdedubnihsubdedubnwp-contentuploads201803mrcgp-int-bruneimodule.jpg)