Upload
others
View
1
Download
0
Embed Size (px)
Citation preview
May 2003 Vol 19, No 5
The monthly publication for OR decision makers
In this issueConference features OR designand construction . . . . . . . . . . . . .5
Are you confident aboutscope reprocessing? . . . . . . . . . .8
TOP 100 HOSPITALS.Hospital finds savings byoutsourcing cataracts . . . . . . . .11
PATIENT SAFETY.A blame-free culture in thereal world . . . . . . . . . . . . . . . . . .18
PATIENT SAFETY.Analyzing OR incidents ina just culture . . . . . . . . . . . . . . .20
FORUM . . . . . . . . . . . . . . . . . . . .22
AMBULATORY SURGERY.ASC list a mix of wins,disappointments . . . . . . . . . . . .23
AMBULATORY SURGERY.U S accuses HealthSouth of massive fraud . . . . . . . . . . . . .24
AMBULATORY SURGERY.Complying with HIPAAssecurity rule . . . . . . . . . . . . . . . .25
WORKPLACE . . . . . . . . . . . . . .27
HEALTH POLICY& POLITICS . . . . . . . . . . . . . . . .30
AT A GLANCE . . . . . . . . . . . . .32
ASC section on page 23.
Homeland Security is heighteningawareness of the need for disas-ter planning. The reality is amajor disaster can hit any communi-tywitness the Feb 20 nightclub fire inRhode Island.
While some communities are wellalong in disaster planning, others arestill waiting for someone to call the firstmeeting, says Joint Commission onAccreditation of Healthcare Organiza-tions president, Dennis OLeary, MD.
The hard fact is most communitieswill be on their own for the first 24 to72 hours until federal aid arrives.
The Joint Commission issued awhite paper about the urgent need oflocal, state, and federal authorities toaddress vulnerabilities in the health
care system (www.jcaho.org).Three materials management soci-
eties issued a blueprint for disaster-related supply planning in March. Theblueprint urges facilities to anticipatesupply needs and work out a logisticalplan with suppliers and with localauthorities.
Theres a temptation to buy andhoard, but that isnt the most effectiveresponse, says Al Cook, chief resourceofficer at St Francis Hospital, Monroe,La, who chaired the committee thatdeveloped the blueprint.
Hoarding ties up dollars and stor-age space and can leave hospitals withoutdated supplies. With todays lean
In a disaster, will your OR supply chain handle a wave of casualties?
Continued on page 6
Materials management
Creating a blame-free culture isconsidered basic to improvingpatient safety. Why would a nursedisclose a medication error that mighthave harmed a patient if she fears losingher job and her license? If such errorsarent disclosed, how can we learn howto prevent similar errors in the future?
A blame-free culture is intended toencourage people to come forward witherrors so systems can be improved. Butdoes a blame-free culture mean employ-ees arent disciplined? How can you bal-ance the need not to blame with theneed to hold people accountable fortheir actions?
David Marx, a human error consul-tant to hospitals, air carriers, regulators,
and NASA, describes what he calls thejust culture.
To me, a just culture is a culturethat is in between a blame-free cultureand a punitive culture, he says.
A just culture is one that encourages
How building a ‘just culture’ helpsan organization learn from errors
Patient safety
Medicare updatesASC list
Medicare published on March 28 a long-awaited
update to the list of procedures approved for
ambulatory surgery centers.Please see article on p 23.
Continued on page 14
2
Full Page Ad
2
Please see the ad for KIMBERLY-CLARK CORPORATIONin the OR Manager print version.
It may serve the cause of patient safe-ty not to punish caregivers whomake mistakes.In a blame-free culture, clinicians are
more likely to come forward abouterrors.
But how do patients feel?Will patients accept that the person
who committed a serious error wont bepunished?
The issue was highlighted in thecase of Linda McDougal, a Minnesotawoman who mistakenly had a doublemastectomy last year when a patholo-gist confused her biopsy specimen withsomeone elses.
In a blame-free culture, the patholo-gist wouldnt be disciplined becausethe mix-up was inadvertent. Thepathologist wasnt reckless or necessari-ly negligent. The problem was theworkflow didnt have the proper safe-guards.
But McDougal was understandablyangry.
I think that pathologist has got tobe penalized, she told the MinneapolisStar Tribune. Hes got to be heldaccountable. She was taking legalaction.
Balancing demand for justiceHow do you balance her demand for
justice with the blame-free culture?We asked the team from Missouri
Baptist Medical Center in St Louis thisquestion when we interviewed themfor the article on page 18 about theirnonpunitive culture. Their efforts haveearned a national award.
I was extremely distressed when Iread about this case, Max Cohen, MD,Missouri Baptists vice president andchief medical officer, told us.
First, they should have gone to thepatient and apologized, he said. Thereshould have been an immediate confes-sion, an expression of compassion, andan offer to help as far as possible to makeit better.
But Dr Cohen was equally out-raged at the suggestion that thepathologist should be punished. Itsour opinion that unless someone is con-sistently or flagrantly violating stan-dards, punishment achieves nothing. After apologizing, he suggested, thehospital should tell her there will be a
thorough investigation to find the rootof the problem and take steps so itdoesnt happen again.
New research indicates patients arelikely to respond positively to thatapproach.
In the study reported in the Feb 26JAMA, researchers conducted 13 focusgroups with patients and physiciansabout their attitudes toward disclosingerrors. More than half of the MDs weresurgeons.
Not surprisingly, patients over-whelmingly wanted to be told abouterrors. Physicians were more circum-spect, partly because of the fear of liti-gation.
What patients wanted, the authorsfound, was an explanation of why theerror occurrednot to fix blame but tounderstand what happened and knowthose involved had learned from theevent. At least four studies have foundmany patients file lawsuits to keep sim-ilar errors from being repeated.
Patients also want an apology. In McDougals case, it didnt help
that the pathologist and hospital didntgo to her and apologize. The head ofthe pathology group issued a statementto the media, saying the group wasexceedingly sorry for her pain.
But McDougal was angry they hadnot apologized in person.
The Joint Commission on Accredita-tion of Healthcare Organizationsrequires organizations to have a systemthat assures patients are informedabout outcomes of their careinclud-ing errors.
Theres no standard requiring anapology. But its a simple gesture thatmight help break through the fear andmistrust that keep errors hidden. ❖
Pat Patterson
Salary/career survey coming
Look for our annual salary/careersurvey. The survey will be sent to a ran-dom sample of OR Manager subscribersthis month. Now in its 13th year, thesurvey tracks trends in staffing, skillmix, salaries, benefits, and other ORmanagement issues. Results will bepublished this fall.
3May 2003
May 2003 Vol 19, No 5OR Manager is a monthly publication forpersonnel in decision-making positions inthe operating room.
Elinor S. Schrader: PublisherPatricia Patterson: EditorJudith M. Mathias, RN, MA:
Clinical editorBillie Fernsebner, RN, MSN:
Consulting editorJanet K. Schultz, RN, MSN:
Consulting editorKathy Shaneberger, RN, MSN, CNOR:
Consulting editorOR Manager (USPS 743-010), (ISSN
8756-8047) is published monthly by ORManager, Inc, 1807 Second St, Suite 61,Santa Fe, NM 87505-3499. Periodicalspostage paid at Santa Fe, NM and addi-tional post offices. POSTMASTER: Sendaddress changes to OR Manager, PO Box5303, Santa Fe, NM 87502-5303.
OR Manager is indexed in the CumulativeIndex to Nursing and Allied HealthLiterature, the Hospital Literature Index, andthe National Library of Medicines HealthPlanning and Administration Database.
Copyright © 2003 OR Manager, Inc. All rightsreserved. No part of this publication may bereproduced without written permission.
Subscription rates: $86 per year. Canadian,$98. Foreign, $108. Single issues $10.Address subscription requests to PO Box5303, Santa Fe, NM 87502-5303. Tele:800/442-9918 or 505/982-0510. Web site:www.ormanager.com
Editorial Office: PO Box 5303, Santa Fe, NM87502-5303. Tele: 800/442-9918. Fax: 505/983-0790. E-mail: [email protected]
Advertising Manager: Anthony J. Jannetti,Inc, East Holly Ave/Box 56, Pitman, NJ08071. Telephone: 856/256-2300; Fax:856/589-7463. John R. Schmus, nationaladvertising manager. [email protected]
The monthly publication for OR decision makers
UpcomingNew energy modalities
New devices using RF energy, ultra-sound, cryotherapy, and other waveformsare arriving in the OR. What you need toknow to manage the new technology.
Physician buy-in Advice from a national study on get-
ting physicians involved in your costreduction projects.
Joint venturesWhat you need to know if your
organization is embarking on a jointventure with physicians.
OR Manager Vol 19, No 5
Editorial
4
Please see the ad for OLYMPUS ENDOSCOPYin the OR Manager print version.
OR design and construction andthe role of the business managerin surgical services are high-lights of the OR Business ManagementConference June 4 to 6 at the CapitalHilton in Washington, DC. The two-dayconference is on Thursday and Fridaywith an opening reception onWednesday.
The meeting also features sessionson materials management, periopera-tive information systems, and using SixSigma for process improvement.
OR construction andrenovation
Health care construction rose bynearly 17% in 2002, according toPriceWaterhouseCoopers.
The conference offers a track of twohalf-day seminars and two breakout
sessions to assist those involved in ORconstruction projects: Equipping the New OR
In this breakout, Walt Justice of BDConsulting and Services will discusspurchasing equipment for a new suite.He will address questions such aswhether the new ORs should be all-purpose or specialty rooms andwhether equipment will be standard-ized. He will also discuss coordinatingequipment shipments and contingencyplanning.
Creating a Healing EnvironmentBeverly Anderson and Jo Ulrich of
Bronson Healthcare, Kalamazoo, Mich,will describe Bronsons award-winninghospital, opened in 2000, which rein-forces Bronsons commitment to well-ness and integrative medicine.Anderson, Bronsons director of surgi-cal services, will discuss the surgicalenvironment, including the flow ofinpatients and outpatients and waitingareas for families. Technology and the Integrated OR
Darko Spoljaric, a popular speakerat last year s conference, and TrudyKenyon, both from ConMed IntegratedSystems, will present a half-day work-shop on the design of an integrated OR.They will focus on perspectives of theOR team, the facility, and the patient.Video routing, monitor placement,lighting, flexibility, and upgradeabilitywill be explored. Working Through Construction
Jayne Byrd, Rex Healthcare, Raleigh,NC, and James Jepson and Jane Stuckeyof consultants FreemanWhite will giveadvice on how an OR can continuefunctioning during construction. Thisteam, which has worked through sever-al construction projects, will discussissues such as scheduling, traffic pat-terns, supply distribution, infectioncontrol, and codes and regulations.
Evolving business manager roleThe demands of billing compliance,
patient confidentiality, exploding tech-nology, and shrinking reimbursementare among factors driving the need formore focused business management insurgery. How is the OR business man-ager s role changing to meet theseincreasing demands?
In a session devoted to the businessmanagers role, Judy Canfield, associateadministrator, and Bill Anton, businessdirector for surgical services and direc-tor of the value analysis program at theUniversity of Washington, Seattle, willtalk about these forces and describehow and why the role is changing tomeet these new demands. ❖
For a brochure or to register online, goto the OR Manager web site at www.ormanager.com. Click on OR BusinessManagement conference. Or call 800/442-9918.
Conference features OR design and construction
5OR Manager Vol 19, No 5May 2003
Gail Avigne, RN, BA, CNORNurse managerShands Hospital at the University of Florida, Gainesville
Mark E. Bruley, EITDirectorAccident & Forensic Group, ECRIPlymouth Meeting, Pa
Judith Canfield, RNC, MNA, MBAAssociate administrator of surgical servicesUniversity of Washington MedicalCenter, Seattle, Wash
Michele Chotkowski, RN, MSHADirector of perioperative servicesLawrence Hospital/Healthstar NetworkBronxville, NY
DeNene G. Cofield, RN, BSN, CNORDirector of surgical servicesMedical Center EastBirmingham, Ala
Larry Creech, RN, MBA, CDTVice president, perioperative servicesClarian Health SystemIndianapolis, Ind
Cheryl Dendy, RNAdministrative director, AmbulatorySatellites, St John Hospital and MedicalCenter, Detroit
Franklin Dexter, MD, PhDAssociate professorDepartment of AnesthesiaUniversity of Iowa, Iowa City
Aileen Killen, RN, PhD, CNORDirector of nursing, perioperative servicesMemorial Sloan-Kettering Cancer CenterNew York City
Robert V. Rege, MDProfessor and chairmanDepartment of SurgeryUT Southwestern Medical CenterDallas, Tex
Marimargaret Reichert, RN, MAAdministrator, Surgical Care CenterSouthwest General Health CenterMiddleburg Heights, Ohio
Kathy E. Shaneberger, RN, MSN, CNORDirector, perioperative services andortho/neuro service lineMercy General Health PartnersMuskegon, Mich
Shelly Schwedhelm, RN, BSNDirector, perioperative servicesNebraska Health System, Omaha
Sallie Walker, RN, BA, CGRNBaptist Physicians Surgery CenterLexington, Ky
Allen WarrenBusiness manager, surgical servicesMission St Josephs HospitalAsheville, NC
Anny Yeung, RN, MPA, CNOR, CNAAAssistant vice president for perioperative services & associate hospital directorSUNY Downstate Medical CenterNew York City
Advisory Board
OR Design & Construction
inventories, hospitals dont have thefunds and capacity to build a big stash.
Instead, hospitals need to coordinatewith their suppliers, other local facilities,and emergency management officials sothey are able to respond quickly.
Disaster formulariesThe supply blueprint, intended as a
starting point, has formularies for coresupplies plus supplies for five disasterscenarioschemical, biological, radio-logical, nuclear, and explosive events.(The formularies do not cover radiolo-gy and pharmacy supplies.)
In the event of a disaster, every hos-pital in the area will be calling for sup-plies, and coordination is essential toprevent chaos, notes Cook. The blue-print was developed by the Associationfor Healthcare Resource & MaterialsManagement (AHRMM), the HealthIndustry Distributors Association(HIDA), and the Health Industry GroupPurchasing Association (HIGPA).
Another association, AdvaMed(www.advamed.org), which representsmedical device companies, has issuedthe Guide to Local Emergency Response:Medical Supplies to help local officialsunderstand the supply chain.
A bioterrorism expert echoes thatadvice.
It would behoove OR directors toget a baseline idea on their communi-tys state of readiness and ability tomove things, Monica Schoch-Sana,PhD, senior fellow at the Johns
Hopkins Center for Civil BiodefenseStrategies in Baltimore, told ORManager.
Its going to be a challenge to strikethe right balance between planning foran institutions temporary needs andcoordinating with local agencies on acommunity-wide plan.
Worry about resourcesA lot of attention has been focused
on terrorism, but not much funding hastrickled down to the state or local level.Even with a federal response, local sup-port and logistics will be critical,experts say.
Schoch-Sana has great concern aboutthe added burden placed on the publichealth systems limited resources.
In a federally declared disaster, theCenters for Disease Control andPrevention (CDC) has a national stock-pile of medical supplies that can bedrawn on to help. The CDC can send a50-ton push pack from its stockpile ofstores at ten locations around the coun-try. The pack isnt intended as a first-response stock but as reinforcement.
Push packs are giant pallets of sup-plies that arrive by truck or jumbo jet,usually in two phasesa 12-hour deliv-ery of general supplies and a seconddisaster-specific delivery later. TheCDC sends along a team of five or sixadvisors to guide local authorities ondistribution. The shipment takes atleast 5,000 sq ft of warehouse space,according to a report in the Wall StreetJournal.
Its one thing for these supplies toarrive, but it can be a scramble to movethe inventory off the tarmac and get itinto the hands of patients, saysSchoch-Sana.
Logistics are crucial, agrees HIDAspokesperson Amanda Forster.
You will need someone at the air-
port with logistics expertise, such as adistributor, to divvy up the suppliesand transport them.
HIDA encourages distributors towork out plans with local emergencyresponse teams.
We want our members to getinvolved so they can be included in thefirst response. They need to knowwhos in charge so they can get sup-plies through, says Forster.
After the Sept 11, 2001, attacks dis-
6 OR Manager Vol 19, No 5 May 2003
“Local supportand logistics
will be critical.
“
Continued from page 1
Materials management
Supply planningfor disasters
Key points in blueprint for supplyplanning for disasters:
Identify departments or units inthe hospital that might beclosed in a large-scale disasterand identify supplies thatcould be diverted to first-response areas.
Determine from your suppliershow long it would take to berestocked.
Consider the maximum num-ber of casualties your facilitymight handle in that time, whatsupplies you could divert, andwhat additional supplies youneed to have on hand until youare restocked.
Use the suggested disaster for-mularies to develop formula-ries specific to your facility.
Establish pre-event orders withsuppliers that can be activatedwith a single phone call or e-mail.
Identify other resources in yourimmediate areanot just otherhospitals but discount stores,local pharmacies, home healthagencies, and other placeswhere basic supplies could beobtained quickly.
Identify a single contact in thecommunity for requesting sup-plies and coordinating supplyflow.
Source: AHRMM, HIDA, HIGPA.Medical-surgical supply formulary bydisaster scenario. www.ahrmm.org.
New disasterplanning manualfrom AORN
The Association of periOperativeRegistered Nurses has a new manualon disaster preparedness for periop-erative services. The manual is aresource for those who are develop-ing a plan for surgical areas to sup-plement the hospitals disaster plan.The manual addresses natural as wellas man-made disasters.
The manual can be purchased bycalling AORN at 800/755-2676 oronline at www.aorn.org
tributors found roads closed into NewYork City and had to arrange for heli-copter delivery, which took extra time.
Community readiness varies aroundthe country, according to the Journal.
Live drills with the CDCs pushpacks have been held in five states:Arizona, Oklahoma, Kentucky, Nevada,and Florida. Other states plan drillslater this year. Some states have heldtheir own drills, and others have sentteams to a federal training site inAnniston, Ala.
Night club fire tests responseHospitals in the Northeast had their
supply response tested after the Feb 20nightclub fire in West Warwick, RI.
Area hospitals were flooded withburn victims. Kent Hospital in War-wick, the nearest community facility,which has a stockless inventory system,immediately called its regional distribu-tor, Claflin, which had a warehouseabout 5 miles away.
Our disaster plan includes having a24-7 pager number for Claflin, saysTom Gardner, director of materialsmanagement for Care New England, towhich Kent belongs. We paged andgot a call back within 10 minutes.
Working through the night, Kentsstaff coordinated with the warehouse,which had three trucks out by 6 am.
Without that, we would have beenscrambling, Gardner says.
Having supply formularies, such asthose recommended by AHRMM,HIDA, and HIGPA would be helpful,comments Claflins director of sales andmarketing, Alexandra Caldwell. Whenhospitals call in a crisis, there can bequestions about exactly what items areneeded. Having a disaster formularyset up in advance not only enables thedistributor to plan ahead but also torespond quickly and accurately.
Another lesson learnedhow quick-ly hospitals respond to the needs ofother facilities. Claflin was able toround up specialty items, such as burngloves, from hospitals around the area.There was an outpouring, saysCaldwell. No one questioned why wewere calling. They just made the sup-plies available. ❖
ResourcesAdvaMed. Guide to Local Emergency
Response: Medical Supplies. www.advamed.org
AHRMM, HIDA, HIGPA. Medical-SurgicalSupply Formulary by Disaster Scenario.www.ahrmm.org
Association of periOperative RegisteredNurses. Disaster Preparedness ResourceManual. Order by calling 800/755-2676
or online at www.aorn.org
Centers for Disease Control and Preven-tion. Strategic National Stockpile.www.bt.cdc.gov/stockpile/
Joint Commission on Accreditation ofHealthcare Organizations. Health Careat the Crossroads: Strategies for Creatingand Sustaining Community-wideEmergency Preparedness Systems. www.jcaho.org
7OR Manager Vol 19, No 5May 2003
Materials management
Labor is the largest single driverof hospital spending for goodsand servicesa reflection ofthe personnel shortage.
For the first time in a decade in2001, hospital wage increases out-paced those in private industry,according to a report byPriceWaterhouseCoopers for theAmerican Hospital Association andFederation of American Hospitals.
Hospitals also are absorbing otherexpenses to help retain nursestuition reimbursement, bonuses,and the like.
Nonlabor expenses also are ris-ing. These include items such assupplies, drugs, devices, technolo-gy, and liability insurance. Thoughthese costs havent risen as fast aslabor spending, most hospitalsreported double-digit increases forcertain drugs and supplies between1997 and 2001, the report says.
Productivity gains hospitals sawin the 1990s from reduced length ofstay and so forth are not likely tocontinue. Instead, hospitals say theywill have to focus on creating a bet-ter work environment for nurses.They also face more paperworkdemands from government and pri-vate payers.
Overall, volumemore peopleusing more servicesaccounts formost of the growth in nationalspending for hospital care. Morethan half55%of the spendinggrowth is volume related, with theremaining 45% from goods and ser-vices, including labor, supplies,drugs, and so on.
Reasons for higher volumesinclude an aging population, crowd-
ed ERs, and less restrictive insuranceplans. ❖
What’s driving hospital costs?
0 Construction 1%Other/efficiency -5%
Regulatory changes 4%
Technology 5%
Other supplies & services 18%
Pharmaceuticals 3%
Labor costs 38%
Increased use rates 16%
Populationgrowth 20%
Share of hospitalspending growth
2002 to 2003 projected
Source: PriceWaterhouseCoopersanalysis for American HospitalAssociation and Federation ofAmerican Hospitals, February 2003.
8 OR Manager Vol 19, No 5 May 2003
Are you confident about scope reprocessing?
How much confidence do youhave in your endoscope repro-cessing?A report from California earlier this
year underlines the difficulties that canarise if reprocessing is inadequate.
Two Sacramento-area hospitals con-tacted more than 3,000 patients whohad colonoscopies at their facilities ear-lier this year and advised them to betested for hepatitis and HIV.
The hospitals recommended the test-ing after finding they had contaminatedendoscopes. Though the chances of apatient being infected were small, theydecided to recommend the testingbecause of previous reports of blood-borne pathogens being transmitted inendoscopy.
The contamination became apparentwhen the staff at one of the hospitalsnoticed material leaking from a scopeas it was about to be used on a patient.The second hospital discovered a simi-lar problem.
The scopes were Olympus, but thebrand is not important, noted JonRosenberg, MD, epidemiologist withthe California Department of HealthServices. He said the incident was unre-lated to a recall of Olympus endoscopeslast year because of a defective port.
This was not a question of any faultwith the endoscopes design, he said.
The problem was that the scopeswere not properly cleaned before beingdisinfected.
The health department wrote toabout 1,000 health facilities in the statereinforcing that every organization thatreprocesses flexible endoscopes needs: policies and procedures on how to
clean and disinfect all endoscopesaccording to the manufacturers rec-ommendations
training for staff on the policies andprocedures
a quality assurance (QA) programfor monitoring of endoscope clean-ing and disinfection.What does a good QA program for
scopes consist of? We asked PauletteSmith, RN, BSN, CGRN, president ofthe Society of Gastroenterology Nursesand Associates (SGNA).
SGNA has standards for reprocessingof GI endoscopes, including a samplecompetency checklist for personnel, avideo, and a chart to help teach and rein-
force the standards. (See Resources.) Expected soon is a new consensus
standard from the American Society forGastrointestinal Endoscopy and theSociety for Healthcare Epidemiology ofAmerica. That standard is not expectedto change the fundamentals of repro-cessing described in the SGNA stan-dard.
Q. What would you like toemphasize about quality moni-toring for flexible endoscopy?
Smith: Supervision is particularlyimportant. Our recommendation is thatthe supervisor of the endoscopy areaeither be certified in GI endoscopy orhave a solid background in this special-ty. The supervisor needs a good under-standing of infection control as well asthe design and function of endoscopes.
Because so many staff hired for theGI lab do not have formal education inGI endoscopy or endoscope reprocess-ing, its all on-the-job training. Itsimperative to have a knowledgeable,well-trained RN or associate to closelymonitor and precept new employees.The supervisor needs to monitor newemployees until they feel comfortablewith all phases of reprocessing.
SGNA recommends that each staffmember who reprocesses endoscopesand accessories have documented: initial orientation in infection control
and reprocessing
annual competency review
annual infection control update.SGNA advises that temporary per-
sonnel not be allowed to clean or disin-fect instruments either in manual orautomated reprocessing systems.
Training also is needed when newmodels of endoscopes or reprocessorsare introduced into your facility. Even if
a new scope is of the same brand andmodel as those you already use, therecan be subtle changes that make a dif-ference in reprocessing.
Q. What’s needed for policiesand procedures?
Smith: You dont need to reinventthe wheel. Resources are available tohelp you. Some GI labs take the SGNAstandards and use them as a step-by-step process. Manufacturers providedetailed manuals on each type of endo-scope.
We recommend that you reviewyour policies annually to make surethey are still current and are followedconsistently. Before making any policychanges, consult with an infection con-trol advisor. Be sure to document thereview process and any modificationsyou make.
As part of your policies and proce-dures, be sure you monitor concentra-tions of reusable high-level disinfec-tants and sterilants every single day.Keep a log of the results. In our lab, wekeep logs for several years. A lot ofambulatory centers are closed on theweekends, and you need to do monitor-ing before putting the liquids back intouse the next week. Also, be sure youadhere to the disinfectants or sterilantsexpiration date. Even if the concentra-tion is all right, if the expiration datehas arrived, the liquid needs to bechanged.
Q. What about culturing ofendoscopes? Is this somethingwe should do?
Smith: SGNA doesnt recommendroutine culturing of endoscopes. Wedetermined that GI departments donthave the ability to properly culture thescopes, and previous environmentalcontamination could give erroneousreadings.
Q. What are the biggest trou-ble spots you see in endoscopereprocessing?
Smith: Cleaning endoscopes is a keystep. This seems to have been what wasoverlooked in the California situation.Cleaning reduces the microbial burden.Scopes that arent properly cleanedmay have debris left behind that will
“The staff noticedmaterial leakingfrom the scope.
“
interfere with the chemicals used inreprocessing. Meticulous manual clean-ing is needed even if an automatedendoscope reprocessor is used.
All of the reprocessing steps need tobe followed each time after an endo-scope enters a body cavity. That meanscleaning all channels, even if a channelwas not used on that case.
Two other areas we hear about: Biopsy forceps. It is recommended
that biopsy forceps be steam steril-ized because they penetrate amucous membrane. It has takenawhile for that message to getthrough.
Water bottles. At a minimum, waterbottles must be manually cleanedand high-level disinfected daily. Afresh bottle with sterile water shouldbe used the next day. Some peopleare still in the habit of leaving thebottle overnight.
Q. Do the same standards thatapply to GI endoscopes applyto bronchoscopes?
Smith: Yes, the SGNA standards doapply to bronchoscopy. We find someGI labs are given the responsibility forrespiratory equipment. Even thoughbronchoscopes are similar to GI scopes,there are differences in the number ofchannels and accessories. As with GIscopes, it is important that all of theports be accessed and cleaned.
ASTM has published a standard,updated in 2000, that applies to allfiberoptic endoscopes.
It is important to note that theSGNA and ASTM standards recom-mend a final step in reprocessing thatincludes purging all channels with airand flushing all channels, includingaccessory channels, with alcohol.SGNA recommends the alcohol flusheseven when sterile water is being usedfor rinsing. ❖
ResourcesAmerican Society for Testing and
Materials. ASTM Standard Practice forCleaning and Disinfection of FlexibleFiberoptic and Video Endoscopes Used inExamination of the Hollow Viscera(F1518-00). W Conshohocken, Pa: 2000.www.astm.org
Association for Professionals in InfectionControl and Epidemiology. APICGuideline for Infection Prevention and
Control in Flexible Endoscopy. www.apic.org/pdf/gdendosc.pdf
Association of periOperative RegisteredNurses. Recommended practices foruse and care of endoscopes. 2002Standards, Recommended Practices, andGuidelines. Denver: AORN, 2002.
Food and Drug Administration. FDA andCDC public health advisory: Infectionsfrom endoscopes inadequately reprocessedby an automated endoscope reprocessingsystem. www.fda.gov/cdrh/safety/endoreprocess.html
Society of Gastroenterology Nurses andAssociates. Guideline for Use of High-Level Disinfectants and Sterilants forReprocessing of Flexible GastrointestinalEndoscopes. www.sgna.org
Society of Gastroenterology Nurses andAssociates. Standards of InfectionControl in Reprocessing of FlexibleGastrointestinal Endoscopes. Also avail-able: Video and chart with reprocess-ing steps. Call 800/245-7462 or visitwww.sgna.org
9OR Manager Vol 19, No 5May 2003
NominateOR Managerof Year
As surgical services managers anddirectors juggle departments,cope with staffing, and strive tokeep quality of patient care high, theydeserve to be recognized.
Each year at the Managing TodaysOR Suite conference, a manager or direc-tor is named OR Manager of the Year.
This years conference will be heldSept 17 to 19 in San Diego.
The OR Manager of the Year willreceive an expense-paid trip to themeeting, including air fare, hotel, meals,and registration.
In recognizing an individual manag-er, the award honors all OR nurses fortheir important role. It is a way of cele-brating nursing management in surgicalservices.
Readers of OR Manager are invited tonominate a manager for the award.Simply write a letter of about 300 wordsdescribing what makes the managerdeserving of the award.
Specific accomplishmentsAddress specific accomplishments
such as leading the staff, inspiring oth-ers, improving recruitment and reten-tion, stimulating quality improvement,and encouraging collaboration amongdisciplines. The letter may be accompa-nied by letters from colleagues, includ-ing physicians, administrators, staff,and other managers.
Send the letter to OR Manager, Inc,OR Manager of the Year Award, PO Box5303, Santa Fe, NM 87502-5303. Thedeadline for entries is July 1.
Nominations are judged by membersof the OR Manager advisory board. Thewinner will be notified in August. ❖
A conference brochure has been mailed toall OR Manager subscribers. The brochure isalso available at www.ormanager.com or call800/442-9918.
Check our web site for the latest news,
meeting announcements,and other practical help.
www.ormanager.com
Billing in full whenteaching MDs aren’tpresent can be fraud
Billing Medicare in full for services ofteaching physicians who arent presentduring key phases of surgical patientscare can constitute fraud, a federal courthas ruled.
Two coders at Washington Universityin St Louis filed suit under the FalseClaims Act alleging the institutionimproperly billed Medicare and otherpublic programs for attending physi-cians services actually performed by res-idents or nurses.
Specifically, the coders alleged super-vising physicians were not present dur-ing preoperative and postoperative care,though their services were billed. Theuniversity contended the teaching physi-cians did not have to be present becausethese services are billed globally underthe surgical procedure itself. But thecourt, in examining the history ofMedicare rules, found that when the gov-ernment went to global billing in 1996, itdid not intend to change its requirementthat teaching physicians had to be pre-sent during key portions of the serviceto bill for the full amount. The courtdenied the motions to dismiss the case. ❖
US ex re Schuhardt v Washington Univ.,228 F Supp 2d 1018 (E.D. Mo 2002)
10
Please see the ad for BOVIE MEDICALin the OR Manager print version.
A series featuring ideas from periopera-tive leaders at Top 100 Hospitals.
How do you make cataract sur-gery affordable when your facil-ity doesnt have a high volumeof these cases?
Maintaining a margin and keepingsurgeons satisfied are tough because
ophthalmol-ogy equip-ment is ex-pensive andc h a n g e srapidly. Itsalso a chal-lenge tokeep thestaff s pro-ficiency up
when the procedure volume is small.For 110-bed St Francis Hospital in
Federal Way, Wash, the solution hasbeen to outsource cataract surgery.
It is one way St Francis has keptcosts under control, notes PatriciaEverett, RN, MSN, manager of periop-erative services. St Francis has been oneof the nations Top 100 Hospitals for 3years. The Top 100 Hospital study rec-ognizes hospitals that outperform theirpeers clinically as well as financially.
Latest technologyBy outsourcing, a facility can offer
eye surgery with the latest technologyand a specialized staff without the costsof capital equipment. It allows a facilityto hedge its bets in case ophthalmolo-gists decide to leave and start their owneye center.
Its a good deal for small hospitalsbecause its a way to avoid the capitalcosts and at the same time meet theneeds of the surgeons, says DaveHarmon, whose firm, MarketScope, StLouis, conducts market research incataract and refractive surgery. His datashows that 56% of cataract surgery isdone in surgery centers, and 44% isdone in hospitals.
St Francis contracts with an indepen-dent vendor, Northwest MedicalServices of Beaverton, Ore, which pro-vides all of the equipment, supplies,lenses, and a surgical technologist (ST)for a set fee per case.
On days cataract surgery is sched-uled, Northwests ST pulls up in a vanwith the microscope, phacoemulsifica-tion machine, and instruments. Thetech sets up the equipment and mayscrub in if that is part of the contract.
In addition to saving on the capitalequipment cost, with outsourcing thecare is the same, perhaps betterbecause the vendor s STs staff onlyophthalmology cases, notes Sue Brown,RN, MBA, regional director of perioper-ative services for the Tacoma, Wash-based Franciscan Health System, ofwhich St Francis is a part. She findsthats a satisfier for the OR staff as wellbecause they may not be experts in eyesurgery.
A lot of times people worry theywill lose control and money if they out-source, says Corey Jensen, North-wests owner and president. Actually,they maintain better control. We canhelp them free up staff positions so theycan redirect their resources.
Adds Everett, Its one less thing Ihave to worry aboutacquiring thelenses, making sure the staff is compe-tent, and the efficiency issues.
The outsourcing businessOutsourcing of cataract surgery got
its start about 15 years ago when salesreps who sold intraocular lenses begantheir own mobile services, primarily inrural areas.
Since then, the business has consoli-dated as regional firms were acquiredby national companies. The largestcataract outsourcing company isMidwest Surgical Services (MSS),Bloomington, Minn, a unit of TLCVision Corporation. MSS has about 300accounts in 40 states, most of which are
hospitals or multispecialty ambulatorysurgery centers that do not have largevolumes of cataract surgery. There alsocontinue to be some regional vendors,such as Northwest.
For a facility performing 35 to 40cataract procedures a month, MSSs feeis about $550 to $750 per procedure,which leaves the facility with a marginover the Medicare reimbursement,which with coinsurance is $1,000 to$1,300 a case, says Dick Minors, MSSsvice president of sales. He said the com-panys capitated fee includes all of thecataract supplies, equipment, and thesurgical technologist. The fee variesdepending on the choice of lens, vis-coelastic, equipment manufacturer, andvolume of procedures done. He main-tains larger facilities can also benefitfrom outsourcing because they donthave the capital equipment cost.
Facilities benefit in areas wherethere is still competition in the out-sourcing business because they havethe ability to bargain for the mostfavorable rates. ❖
The Top 100 Hospital study is conduct-ed by Solucient. For more information, goto www.solucient.com
11OR Manager Vol 19, No 5May 2003
Hospital finds savings by outsourcing cataracts
Top 100 Hospitals
St Francis HospitalFederal Way, Wash
Nonprofit community hospitalBeds: 110 ORs: 4 ambulatory, 4 main Surgical volume: 6,000 Services: Most specialties except
cardiac Years in Top 100: 3
“It’s one less thing I have to worry
about.
“
12
Please see the ad for DUPONTin the OR Manager print version.
13
Please see the ad for DUPONT
in the OR Manager print version.
14 OR Manager Vol 19, No 5 May 2003
Patient safety
people to raise their hands and say theymade a mistake, yet still holds themaccountable if they choose behavior thatknowingly puts someone at risk.
He says it is similar to the atmosphereloving parents try to establish for theirchildrenyou want the child to comeforward and admit she stole some candyfrom a store, but thats no guaranteethere wont be consequences.
Generally, human error is not ourchoicewe dont intend to make mis-takesbut what we do intend is the
underlyingb e h a v i o r ,which mightsignificantlyincrease therisk, Marxexplains. Ane x t r e m eexample is aperson whohas an acci-
dent while driving drunk. The driverdoesnt intend to have an accident butmakes an accident much more likely bybeing intoxicated.
We dont send a drunk driver to jailbecause he had an accident but becausewhat he did unnecessarily increased therisk, he says.
Marx described his concepts of thejust culture in a primer available on theInternet at www.mers-tm.net/support/Marx_Primer.pdf
To see how the concepts apply to theOR, read about the two OR incidents onp 15. Think about how you as a managerwould respond. Then turn to p 20 to readMarxs analysis.
See the accompanying article to readhow one organization, Missouri BaptistMedical Center, put the principles intopractice.
The “four evils”Marx says four behavioral concepts
or four evils (sidebar)are necessaryto understanding the interrelationshipbetween discipline and patient safety: human error
negligence
reckless conduct
intentional rule violations.The question is: Do all or only some
of these concepts warrant disciplinary
action after an adverse incident?Marx notes that research on discipli-
nary systems shows we react more strong-ly to risk-taking behavior of others than towhether they are adhering to rules or poli-cies. Consider the driver you see weavingin and out of traffic. Do you react to a vio-lation of traffic rules or to the risk the dri-ver is taking? If you are like most people,you perceive the risk-taking behavior to bemore culpable than whether the person isbreaking the speed limit.
Understanding the four evils pro-vides a framework for understandingjustice and deciding when disciplinaryaction is called for.
In the primer, Marx applies the fourconcepts to three types of disciplinary sys-tems that organizations typically have:
Outcome-based disciplineIn this system, disciplinary decision
making hinges on the outcome of thebehavior. An example is a disciplinarypolicy that scores nurses who make med-ication errors based on a number of fac-tors including the outcome of the error: 5points for no harm, 15 points for moder-ate harm, 25 points for severe injury, and70 points for death.
The problem with this system, saysMarx, is that, theoretically, an intoxicatednurse who made a drug error thatcaused no harm would score lower thana well-meaning nurse who killed apatient.
This is a fundamentally flawed sys-tem based on the notion that we cantotally control our outcomes, says Marx.
In managing human error, we canonly control our intended behaviors toreduce the likelihood of a mistake, butwe cannot truly control when and wherea human error will strike.
Rule-based disciplineRule-based discipline is the easiest to
“What do you do about the
negligentemployee?
“
Continued from page 1
The “four evils”Human error
A person did other than what heor she should have done and inad-vertently caused an undesirable out-come. Though we use the term todescribe everyday behaviormiss-ing an exit on the freeway, pickingup strawberry ice cream instead ofchocolateerrors in health care canhave more dire consequences. Forexample, a physician prescribes awrong dosage of a medication. Thephysician did not intend the erroreven though the consequences couldbe life threatening.
Negligent conductNegligence is conduct we consider
more culpable than human error.Negligence is a legal term that inmost states is defined as failure toexercise the skill, care, and learningexpected of a reasonably prudenthealth care provider. Criminal negli-gence involves an objective determi-nation that a person should havebeen aware he or she was taking asubstantial and unjustifiable risktoward causing an undesirable out-come.
Reckless conductReckless conduct, also called gross
negligence, involves a higher degreeof culpability than negligence.Reckless conduct differs from negli-gent conduct in intent; negligence isthe failure to recognize a risk, andrecklessness is a conscious disregardof a visible, significant risk. Forexample, the term reckless drivingconnotes a much higher degree ofculpability than mere human error.
Intentional rule violationsAn intentional rule violation
occurs when an individual knowing-ly chooses to violate a rule whileperforming a task. The concept isnot necessarily related to risk takingbut merely shows an individualknew of or intended to violate a rule,procedure, or duty while performinga task.
Source: David Marx.
understand. Most high-risk industrieshave rules, policies, and proceduresintended to prevent mishaps.
Two questions to ask about a rule orpolicy violation: Did the person violate the rule?
Did the person intentionally violatethe rule?In many organizations today, disci-
plinary action is possible for any ruleviolationintended or not, says Marx.Organizations that have revised theirpolicies to encourage learning frommishaps have raised the disciplinarythreshold to intentional rule violations.
There are some difficulties with a rule-based disciplinary system. First, not allintentional violations are bad. There aretimes in patient care when rules dont fitthe circumstances of a professional givingcare. Also, intentional violation of somerules occurs every day. Some of these vio-lations become normal behavior.
The important point is that rule vio-lations in themselves are crucial learningopportunities for improving safety.Much can be learned through under-standing why certain violations becomethe norm, Marx says.
In a system that takes action againstevery intentional deviation from policy,employees will report they were follow-ing the ruleseven when the facts arepossibly quite different.
Risk-based disciplineThis system, which is the basis for our
civil liability system, considers theemployees intent with regard to anundesirable outcome. Negligence, grossnegligence, and recklessness are all con-cepts related to risk creation.
Many organizations that adopt a cul-ture of reporting mistakes have raised thethreshold for possible disciplinary actionto reckless conduct, using discipline onlyto deter intentionally or knowingly unsafeacts. Thus, if an act is inadvertent, a per-son would feel safe reporting it.
I am aware of no organization in theworld, even those professing to beblame-free, that will not discipline anindividual who has been reckless towardthe safety of others, he says.
What about negligence?What to do about the negligent
employee? That question lies squarely in the
middle of disciplinary decision making,Marks says.
Negligence means the employeeshould have known but was unaware ofthe risk he was taking. The doctor writesa prescription for 100 mg of a drug ratherthan the intended 10 mg. Was he awareof what he did? No. Should he have beenaware? Yes.
In medicine, negligence is the thresh-old for compensating victims of harm.
To that end, it is important to distin-guish negligence and human error fromreckless conduct, says Marx.
Negligence and human error are bothviewed as inadvertentthe person didnot intend the error or negligence. Ingeneral, states allow punitive damagesonly when the individual was recklessacting in conscious disregard for sub-stantial and unjustifiable risk.
Is it more beneficial to punish the neg-ligent health care provider, hoping theperson will pay better attention to avoidfuture punishment? Or is it more benefi-
cial to allow the person to come forwardso the system can learn from the individ-uals mistake?
Data to answer this question havebeen growing in industries outsidehealth care.
Aviation and other industries withinjury prevention programs have seengreat reductions in adverse events bycreating a culture where safe behaviorsare reinforced, and disciplinary systemsallow erring employees to come forwardand report their mistakes. ❖
David Marx can be reached at [email protected]
15OR Manager Vol 19, No 5May 2003
Patient safety
As a manager, how would you ana-lyze these two OR incidents andmake a decision about discipline?Think about the incidents. Then turnto page 20 for an analysis of howthese incidents would be handled in ajust culture.
Incident 1A baby rolls off of an OR table dur-
ing emergence from anesthesia after aminor procedure. Neither the circulat-ing nurse nor the anesthesiologist wasat the babys side, which is the usual
practice. There is not a written policyrequiring this, however. The baby wasnot injured.
Incident 2After open-heart surgery, a patient
develops complications. The patient isbrought back to the OR, and it is dis-covered that a small retractor was leftin the wound. The retractor did notshow up on an x-ray taken after theprocedure. The hospital does not havea policy requiring instrument counts.The patient recovered.
JCAHO will shift tounannounced surveysby January 2006
The Joint Commission on Accredi-tation of Healthcare Organizations(JCAHO) will conduct all regularaccreditation surveys on an unan-nounced basis beginning January 2006.The unannounced surveys will be pilot-tested in volunteer organizations dur-ing 2004 and 2005.
The new process, dubbed SharedVisionsNew Pathways, providesstrong incentives for organizations toprovide safe, high-quality care at alltimes, according to the JCAHO. Child-rens Memorial Hospital, Chicago, is thefirst hospital to seek an unannouncedreview, to take place in 2004. One hun-dred hospitals have volunteered forpilot testing of the unannounced trien-nial survey process. Four multi-hospitalsystems and alliancesAscensionHealth, Tenet Healthcare, VeteransHealth Administration, and NorthShore-Long Island Jewish HealthSystemhave committed to having anumber of their hospitals participate inunannounced surveys in 2004 or 2005.
The commission will continue volun-tary unannounced surveys on a limitedbasis in 2005 until the transition to a com-pletely unannounced survey program in2006. It will also continue one-day ran-dom, unannounced surveys in an annual5% sample of the health care organiza-tions it accredits through the end of 2005.After that time, it will discontinue ran-dom unannounced surveys. ❖
www.jcaho.org
OR incidents and a just culture
16
Please see the ad for CARDINAL HEALTHin the OR Manager print version.
17
Please see the ad for CARDINAL HEALTH
in the OR Manager print version.
Having a just culture wherepeople arent blamed for makingmistakes is a laudable concept.How does it work in the real world?For the past 2 1/2 years, Missouri
B a p t i s tM e d i c a lCenter in StLouis hasbeen build-ing a blame-free cultureas part of itspatient safe-ty program.The hospital
was recognized for its efforts with theAmerican Hospital Associations firstQuest for Quality Prize, which cited thehospital for leadership and innovationin patient care quality and safety.
A team from the hospitals surgicalservices department put the just cul-ture concepts into practice recently asit analyzed and learned from two inci-dents of retained sponges after surgery.The team was able to fine-tune itscounting policies, making the processsafer.
More than words The hospitals vice president and
chief medical officer, Max Cohen, MD,has taken a leadership role in fosteringthe blame-free environment.
We realized that to make improve-ments in patient safety, we would firsthave to change our culture, he says.Weve put a tremendous amount ofeffort into that.
Among steps Missouri Baptist hastaken to keep the blame-free culturefrom being more than words: Define the philosophy
All employees receive a brochure thatexplains Missouri Baptists philosophy.The brochure says that the hospital rec-ognizes that competent and caring pro-fessionals will make mistakes. Therefore,we do not intend to instill fear or punish-ment for reporting these events, as theyoften result from inadequate or complexsystems within the hospital.
The brochure says the hospital willprovide staff who are involved inevents with a nonpunitive and sup-
portive environment to report eventsas well as near misses.
Its our opinion that unless some-one is consistently or flagrantly violat-ing policies or standards, punishmentachieves nothing, Dr Cohen says. Itdoesnt make the hospital safer.
Everyone in the organization has tobelieve it is their job to keep patientssafe. The staff must believe in theirhearts that the way to make care safer isto tell someone about errors.
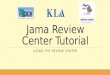
A blame-free environment does notmean no one is ever disciplined. Tohelp staff and managers sort out whichbehaviors fall under the nonpunitiveumbrella, which are exceptions, andwhich are in a gray area, the hospitaldeveloped a chart titled AssessingUnsafe Acts (illustration). For behav-iors in the gray area, there are threequestions managers can ask in deter-mining how to handle a situation:Was the act or omission reckless?
Was the act or omission repeated orvery similar to others?
Did the act or omission underminepatient safety initiatives?
Educate leaders and staffEducation began at the executive
level. We first had to retrain the execu-
tives, then the directors, Dr Cohennotes.
Leaders spent time at retreats andeven acted out skits to show how theywould handle errors and employee dis-cipline in a blame-free culture. Onlyafter the directors were trained did edu-cation take place for managers andstaff. Appoint a full-time patient safety
officer.
As safety officer, Nancy Kimmel,RPh, develops and carries out pro-grams such as: a Patient Safety Hotline that fields
about 200 calls a month, up 900%from when it began operation.Employees are encouraged to call ifthey are aware of an accident or nearmiss. They can report anonymously.They can file a written report insteadif they wish. Physicians can also usethe hotline, which is accessible fromoutside the organization.
We Heard You, We Acted e-mailnewsletter that describes how prob-lems that were reported wereaddressed.
cultural surveys to measureemployees opinion about the cultur-al changes.
random chart reviews that use trig-gers to monitor patterns andtrends. Kimmel says these reviewsshow that potentially harmful inci-dents have declined since reportingbegan.
A blame-free culture insurgical services
Nancy Hesselbach, RN, BSN, direc-tor of surgical services, receives all hot-line reports that concern her depart-ment.
It really helps alert me to thingsemployees are concerned about, shesays.
Hesselbach then decides whetherthe incident needs to be analyzed insurgical services or referred to anotherdepartment.
Recently, the surgical services teamapplied the nonpunitive concepts aftersponges were retained after surgery.
After the first incident occurred, wesat down with the team that had beenin the room and talked about what hap-pened. Then we started a root causeanalysis, says Linda Daake, RN, nursemanager for the OR.
The staff came into my office andsaid, Were not in trouble? she recalls.I said, No. We need to discuss this soit doesnt happen again. Surgeonsparticipated as well.
The team spent about 4 monthsrevising the counting policy. Then
18 OR Manager Vol 19, No 5 May 2003
Patient safety
A blame-free culture in the real world
“The team appliednonpunitive conceptsafter sponges were
retained.
“
another incident happened on anotherservice. Once again, Daake sat downwith the team from that service.
The staff felt comfortable sayingthey had made a mistake. They weremore attuned to looking at what hap-pened because they werent worriedabout losing their jobs, she says. Afterthe second incident was analyzed, fur-ther policy revisions were made.
From their analysis, the team learnedthat one incident happened when the cir-culating nurse left the room, and theanesthesiologist got laparotomy spongesfor the surgeon. The scrub nurse wasbusy, and the sponges were opened butnot recorded. The patient was large, andthe fact that the count was incorrect wasmissed. The sponge was discovered later.
As a result of analyzing these inci-dents, the team made a change in itssponge counting practices, which wasadopted by all departments wheresurgery is performed.
As a check on the sponge count, whennew sponges are added to the field, thecirculating nurse takes the label from thesponge package and places it on the clip-board used for recording counts. The
same is done when sponges are addedfrom custom packs.
This gives them a way of verifyingthe count, Daake says. The labels arehelpful, for example, when a new circu-lating nurse comes in to provide reliefat 3 pm for an ongoing case.
Nurses got the idea from needlecounting, where the scrub nurse leavesthe needle package on the field as away of double checking the number ofneedles used.
X-rays are performed whenever theteam has a question about the count.
This is a matter of professionaljudgment, Daake says. It adds a littletime to the case, but its a safety issue inmy opinion. ❖
19OR Manager Vol 19, No 5May 2003
Patient safety
Intention-ally causesharm ortampers
with errorreportingprocess
Recklessor
intentionaldisregard
forpatientsafety
Repeatedlyviolateshospitalpolicies,
processesor
standards
Failure toparticipatein patient
safetyinitiative
Near missor erroroccurreddue tominor
deviationfrom
process orpolicy
Carelessnessin
providingpatientcare or
adherenceto policy
or process
Employeemade errorin judgment
when nopolicy orprocess in place
Employeemade error
byincorrectly
interpretingambiguouspolicy orprocess
Employeemade error
whilefollowinghospitalpolicy orprocess
Gray Area
Key "gray area" questions:
NonpunitiveExceptions
1. Was the act or omission reckless?2. Was the act or omission repeated or very similar to others?3. Did the act or omission undermine patient safety initiatives?
Source: Missouri Baptist Medical Center, St Louis. Reprinted with permission.
Assessing unsafe acts
Survey confirmsurgent need forliability reform
A survey by the Englewood, Colo-based Medical Group ManagementAssociation (MGMA) suggests recentincreases in liability insurance premiumsare beginning to severely limit patientaccess to health care.
Responses from 700 group practicesemploying 16,800 physicians found MDsfaced an average premium increase of53% between 2002 and 2003. In all, 26%of practices say their physicians wouldretire, relocate, or restrict services overthe next 3 years. Some 14% of practicessay they no longer treat certain high-riskpatients.
MGMA calls for Congress to pass leg-islation to halt the rapid increases in pre-miums.
www.mgma.com
Have an idea?Do you have a topic you’d like to see
covered in OR Manager?
Have you completed a project youthink would be of help to others?
We’d be glad to consider your sug-gestions. Please e-mail Editor Pat
Patterson at [email protected]
This analysis by David Marx, JD,illustrates how the OR incidentsdescribed on page 15 would beconsidered in a just culture.
Incident 1: A baby fallsLeaving the baby unattended is an
error that placed the baby at risk. In ajust culture, the analysis would focusnot only on the error but also on whythe error occurred. Did something drawthe clinicians attention away from thebaby, such as an urgent phone call?How often does this happen? Is there asystem in place to assure a baby is notleft unsecured?
In situations where human error ispossible, high-risk industries like avia-tion build in a safety net. If there is abackup system, they may avoid losingan aircraft. Backups also provide a safe-ty net in health care. For example, ifthere is a strap to hold the baby on thetable, the baby wont fall if the nurse iscalled away.
In terms of discipline, would this beconsidered negligent or reckless behav-ior?
Many would argue that remaining atthe side of a baby emerging from anes-thesia is expected professional conductand thus not doing so could be consid-ered negligent or even reckless. But thereal issue is one level deeper: Whatbehavior led up to the incident? Whywere the nurse and anesthesiologist notat the babys side?
One way to explore this would be togather a group of peers from this hospi-tal and ask them what they would havedone in that situation. Is the norm atthat hospital always to stay by a babysside? Or is there a norm that says itsOK to leave in certain situations, suchas an urgent phone call asking for vitalpatient information?
The bottom line: Unless you dig intothe reasons why the error occurred, youdont know how to judge it. It is not themistake you judge but the behavior thatled up to the mistake. There are choicespeople make. In this case, they chose toleave the baby. Why did they leave?What was the rationale?
What if there is a double standardfor judging nurse and physician behav-ior? Is that a just culture?
In a just culture, recklessness is the
evil. We judge on individual behavior,Marx responds. In this type of situation,he favors a group investigation, whereincidents are analyzed by a multidisci-plinary team.
Incident 2: The retainedretractor
This situation is not a reason for dis-cipline but for the hospital to under-stand where at-risk behavior is occur-ring and whether it could adopt strate-gies to reduce the risk.
The risk of a retained object is notzero. You never have a perfect system.There is some risk, and the hospitalshould have a sense of what the risk is.Is it one incident in 15 years? Is it one in1,000 cases?
A study by Atul Gawande and col-leagues published earlier this year inthe New England Journal of Medicineindicated that an item is retained inabout 1 in 9,000 to 1 in 19,000 cases, theequivalent of about one case a year fora typical large hospital. Increased riskswere associated with emergencysurgery, an unplanned change in opera-tion, or obesity.
In this case, the hospital did nothave an instrument count policy. Thiswas an organizational decision. By nothaving a policy, did they appreciate therisk? Is there an alternative that wouldhave made the system safer?
A hospital pays through the tort sys-tem for the system it has designed. Itsup to the hospital to decide: What lia-bility do we want? Thats not meant tobe punitive, but thats our system.
It doesnt help just to put the respon-sibility on the nurse not to make a mis-take. Expecting people to be perfect isnot realistic. If you consider people tobe perfect, you dont need a robust sys-tem. You have a system with highaccountability but poor reliability.
In a just culture, we look at thebehavior we want. What are ways tomake the system more robust andsafer? Are there better ways to keeptrack of instruments? How do we teachthe OR staff to conduct counts? Arethere situations in which x-rays shouldbe done to verify that an instrument hasnot been left in? ❖
20 OR Manager Vol 19, No 5 May 2003
Patient safety Managing Today’s OR Suite to offer eight all-day seminars
Juliet Liposky, MD, director of ambula-tory anesthesia and recovery atMassachusetts General Hospital inBoston, has joined the faculty for theManaging Todays OR Suite conferenceSept 17 to 19 in San Diego.
She will speak with Janet Quigley, RN,MSN, nurse manager of Mass GeneralsSame-Day Surgery Unit, at an all-dayseminar, Clinical Management of theAmbulatory Surgery Patient. The semi-nar is one of eight preconference semi-nars scheduled for Wednesday, Sept 17.
Among strategies Dr Liposky andQuigley will share: how study findings can be used to
refine preadmission screening, patienteducation, and discharge planning
how to manage credentialing for careof the patient having IV sedation andtrack patient outcomes
changes needed to accommodate afast-tracking program for the post-anesthesia phase of care
advantages of various pain manage-ment strategies with costs and out-comes.
Other all-day seminarsTopics of other seminars include:
Keys to Retaining Todays OR Work-force, with Jennifer Ahmad, of JWTSpecialized Communications
Patient Safety: Tools to Make it Hap-pen and Measure Success, withPatrice Spath
Succession Leadership: Preparing forthe Future, with Tim Porter-OGrady
Tools for New Managers, withSuzanne Moss Richins of KadlecMedical Center, Richland, Wash
The Big Picture: Working Together,with Marcia Peterson and Judith A.Pins of Cardinal Health and surgicalservices leaders Barbara Pankratz andJoann Rickley
Lean Thinking and Rapid ProcessImprovement, with Jeff McAuliffe andKate Rogers of Swedish MedicalCenter, Seattle
Creating a Healthy, Healing Work-place with Bonnie Wesorick.
For a conference brochure, visitwww.ormanager.com or phone 800/442-9918. You may register online. ❖
Analyzing OR incidents in a just culture
S I X T E E N T H A N N U A L
Discover, discuss, debate the latest in OR managementAll-day workshops, general sessions, breakout sessions, exhibits, and networking provide you with the information you need to manage your OR today.
Highlights:• Track for those who manage an ambulatory surgery center• Track for those involved with purchasing for the OR• Track for new managers
You may register online. For a conference brochure, visit www.ormamager.com or phone 800/442-9918.
ManagingToday’s ORSuiteT H E P R E M I E R C O N F E R E N C E O N O R M A N A G E M E N T
San DiegoSeptember 17-19, 2003Manchester Grand Hyatt San Diego
To the Editor:
I read with great interest your Marcharticle regarding Pseudomonas aerugi-nosarelated infections at AlleghenyGeneral Hospital (OR Manager, Vol 19,No 3).
We would like to take this opportu-nity to provide clarification to the infor-mation reported in this article, as Sterispersonnel have first-hand knowledge ofsome of the events at Allegheny (AGH).
Its important to remember thatthere are three fundamental elements inthe disinfection or sterilization of bron-choscopesthe bronchoscopes them-selves, the processes and proceduresused by the health care facility, and thereprocessing devicesand each ofthese elements must be considered inthe investigation of the Alleghenyevents.
First, bronchoscopes must be consid-ered as possible contributors to contam-ination (even if not subject to recall) iftheir design, age, or condition preventseffective disinfection or sterilization.Allegheny General dismisses the possi-bility that poor maintenance or otherfactors relating to the bronchoscopescontributed to the infections. Based oninformation obtained from the compa-nys review at AGH, Steris questionsAGHs assessment.
Second, the cleaning and disinfect-ing or sterilization processes and proce-dures followed by a hospitals staffmust be considered. For any manufac-turers process to work effectively, facil-ities must vigilantly articulate andobserve their infection control practices.Among these practices, practitionersmust use only the proper manufacturer-approved accessories and must main-tain the cleaning times, temperatures,and procedures as defined in each com-panys FDA 510(k) clearance.
In the Allegheny case, on Oct 18,prior to being notified of an infectionoutbreak, Steris conducted an assess-ment of the facilitys reprocessing pro-cedures and raised several concernsincluding the selection of the properconnectors and compliance with Sterisreprocessing instructions. The System1® Sterile Processing System isdesigned for just-in-time use, meaning
bronchoscopes should be reprocessedimmediately before use, as recommend-ed in guidelines of AORN (Associationof periOperative Registered Nurses).
Finally, the reprocessing device itselfmust be considered. Since its introduc-tion in 1988, the System 1 has sterilizedhundreds of millions of medical devicessafely and effectively. With more than16,000 units installed in more than 5,000US facilities, System 1s validated steril-ization process has become the industrystandard for reprocessing endoscopes,providing the highest reprocessingstandard for patients versus alternativetechniques.
There was discussion of thereprocessors sterile water quality in theAllegheny incident. However, ourunderstanding is that the method usedto collect a water sample for testing atAllegheny violated the reprocessor ssterile barrier seal and was otherwiseincapable of obtaining an aseptic sam-
ple. It is no surprise that the Centers forDisease Control and Prevention foundcontamination in these questionablesamples as the collection process mostcertainly contaminated them. In 15years of use of the Steris System 1, therehas never been a reported filter break-down. Indeed, these are the same gradeof filters that are used in the productionof injectable drugs, diagnostic reagents,and aseptically filled medical devices.
Steris has fully supported and coop-erated with the FDA and other interest-ed parties throughout the investigationprocess. As are infection control practi-tioners, we are absolutely confident inour product and the assurance of a ster-ile process when proper operatinginstructions and clinical guidelines arefollowed.
Richard (Ric) RumbleVice President, Global Marketing
HealthcareSteris Corporation
22 OR Manager Vol 19, No 5 May 2003
Forum
Preventing back injuries in nursesThough hospitals have spent a lot of
time and effort to prevent back injuries innurses, the incidence or severity of suchinjuries has improved little over theyears.
In a two-part article beginning in theFebruary American Journal of Nursing,experts advocated abandoning ineffec-tive or unproven measures such as backbelts.
Instead, they believe efforts should bedirected to: performing an ergonomic assess-
ment of patient care areas
providing engineering controls suchas ceiling-mounted mechanical lift-ing devices
having a standardized protocol forassessing patient handling and mov-ing
developing algorithms for determin-ing the number of personnel andequipment needed to move patientssafely
using a new education model with atrain-the-trainer approach in whichunit leaders teach coworkers to useequipment competently.Engineering controls focus on bring-
ing the activity to the patient rather thanthe reverse. For example, nurses couldsubstitute a lower-risk task such as later-al transfer for a higher-risk task such astransfer from bed to chair through theuse of new equipment.
For more information, visit www.patientsafetycenter.com ❖
Nelson A et al. AJN. February2003;103:32-40.
Call for abstractsfor poster display
Posters are invited for theManaging Todays OR Suite confer-ence Sept 17 to 19 at the ManchesterGrand Hyatt, San Diego. Topics suit-able for posters include research stud-ies, process improvement projects,and clinical innovations.
If you are interested in displayinga poster, please submit an abstract toOR Manager, Inc, by July 15.
For more information, includingan abstract submission form, checkthe OR Manager website at www.ormanager.com or call 800/442-9918.
ASC list a mix of wins, disappointments
Along-awaited update in Medi-cares list of approved proceduresfor ambulatory surgery centers(ASCs) was published March 28. The listadds about 280 procedures to the list of2,306 already approved and deletes 140.The list is effective July 1.
Though the list is final, the Centers forMedicare and Medicaid Services (CMS)is seeking comments on 58 of the addi-tions. Comments are due by May 27.
Among key procedures added werearthroscopic rotator cuff repair andwrist endoscopy for carpal tunnelrelease.
Though pleased the new list wasfinally released, the ASC communitywas disappointed. Fewer procedureswere added than had been proposed,and there was no change in the criteriafor adding procedures to the list, as hadbeen hoped.
In a victory for ASCs, several painmanagement codes proposed for dele-tion were kept on the list. These include64420 and 64421 (injection for nerveblock) and 64622 and 64623 (destruc-tion of paravertebral nerve).
CMS cited patient safety as a reasonthese procedures should continue to bedone in ASCs rather than doctorsoffices, noting that patients require car-
diac and respiratory monitoring. Paininjections also require fluoroscopicguidance as well as meticulous atten-tion to infection control.
Also a victory was retaining threekey urodynamic procedures51726(complex cystometrogram), 51772 (ure-thra pressure profile), and 51785(anal/urinary muscle study), theAmerican Association of AmbulatorySurgery Centers notes.
The ASC community was dismayedCMS decided not to add laparoscopiccholecystectomy to the list.
Were disappointed, particularlybecause CMS acknowledges this isbeing done without problems for non-Medicare patients, says Kathy Bryant,executive director of the FederatedAmbulatory Surgery Association
(FASA), which has lobbied to expandthe list since 1995.
CMS says its medical advisors deter-mined that lap choles in the ASC settingwouldnt be appropriate for Medicarepatients because some patients need anovernight stay.
Among highlights in surgical spe-cialties:
GynecologyAnother disappointment was CMSs
decision not to add most codes forlaparoscopic-assisted vaginal hysterec-tomy. Only one code was added58550for the most minimal type oflap-assisted hysterectomy.
Several other gynecology procedureswere not added, including 57288 (stressincontinence) and 57460 (colposcopy),because a physicians group comment-ed that these should be done in the hos-pital. But CMS did keep on the list19318 (large breast reduction) and19340 (immediate breast prosthesis).
ENT surgeryAdded to the list were codes in the
40700 series for repair cleft lip/nasaland 42415 for parotid surgery. In addi-tion, CMS included four codes forremoval of tonsils and adenoids.
But two more extensive procedureswere not added because they are con-sidered hospital procedures. Thesewere 60220 and 60225 (total thyroidlobectomy) and 48242 and 42844 (exten-sive throat surgery).
EndoscopySome 23 codes were added for GI
endoscopy, ranging from esophagusendoscopy to ileostomy with stent toanoscopy. CMS is seeking comment on14 of these added since the 1998 pro-posal. Most are endoscopies that entailan additional procedure, such asesophagoscopy or upper GI endoscopywith ultrasound-guided biopsy.
Gwendolyn Grothouse, RNAdministrative directorApple Hill Surgical CenterYork, Pa
Barbara Harmer, RN, BSN, MHASenior consultantHealthCare Consultants, IncCelebration, Fla
Jerry Henderson, RN, BS, CNOR, CASCExecutive directorThe SurgiCenter of BaltimoreOwings Mills, Md
Diana Procuniar, RN, BA, CNORNursing administratorWinter Haven Ambulatory Surgical
CenterWinter Haven, Fla
Donna Gelardi-Slosburg, RN, BSN, CASCNational surgery specialistHealthSouthSt Petersburg, Fla
Rhonda Tubbe, RN, CNORAdministratorThe Surgery Center of NacogdochesNacogdoches, Tex
Ambulatory Surgery Advisory Board
Continued on page 24
“Fewer procedureswere added
than proposed.
“
23OR Manager Vol 19, No 5May 2003
24 OR Manager Vol 19, No 5 May 2003
Neurosurgery/orthopedicsA noteworthy addition is 29827
(arthroscopic rotator cuff repair), whichCMS is seeking comments on. Alsoadded were 29848 (wrist endoscopy/surgery) and some hip and ankle ar-throscopy codes. Percutaneous diskec-tomy (62287) was added to the list, aswere five codes for implanting neuro-electrodes.
UrologyTwo treatments for benign prostate
disease were included: 52647 and 52648(laser surgery of the prostate) and 53850(prostate microwave thermotherapy).Penile repair and prosthesis proceduresalso can now be done in the ASC. Thenew list adds eight new cystoscopycodes, such as 52341 (cysto with treat-ment of ureteral stricture).
Though commenters argued that anumber of codes, such as 53600, 53601,and 53621 (dilate ureteral strictures),should be added, CMS said these dontqualify because data show these proce-dures are performed most of the time inphysicians offices. Several codes in the50570 series (renal endoscopy) wereremoved because they dont meet crite-ria for the list. Extracorporeal shock-wave lithotripsy (ESWL) was not addedbecause of a 1992 court decision.
A long processThough the ASC list by law is sup-
posed to be updated every 2 years, theprocess for this version began in 1998.CMS attributed the long delay to itspreoccupation with Y2K and imple-mentation of the hospital outpatientprospective payment system, amongother developments.
Before the next scheduled update in2005, CMS says it will consider propos-ing revised criteria for determiningwhich procedures should be on the list.
Though a number of people advo-cate dropping the list all together, say-ing the decision about where to dosurgery is best made by the patient and
physician, CMS says the list is requiredby law.
To be added to the list, proceduresmust:
not be performed more than 50% ofthe time in a doctors office
be considered safe or appropriate for
Medicare patients in the ASC setting.
Procedures are not added if theywould have a payment rate significant-ly lower than the lowest ASC paymentgroup.
ASC groups already are working onadditions for the next update. FASA hascollected 119 suggested additionsthrough its web site at www.fasa.org.Bryant noted that CMS must start theprocess soon to meet the 2-year sched-ule. ❖
The final rule and ASC list were pub-lished in the March 28 Federal Registeravailable at www.access.gpo.gov/su_docs/aces/aces140.html
Additional information is on the FASAsite at www.fasa.org and the AAASC site atwww.aaasc.org
AmbulatorySurgery
Continued from page 23
“A disappointmentwas not adding
lap chole.
“
HealthSouth fired its CEO and chair-man, Richard M. Scrushy, March31 after the Securities and Ex-change Commission (SEC) charged thecompany with massive accounting fraud.The SEC alleges HealthSouth inflatedearnings by as much as $2.5 billion.
Eight executives had pled guilty tofederal charges as of April 8, includingtwo former CFOs.
HealthSouth, the nations largestprovider of outpatient surgery and rehabservices, has some 1,700 facilities, includ-ing more than 200 surgery centers.
The SEC charges Scrushy certifiedfinancial statements he knew or shouldhave known were false and misleadingand personally profited from inflatedearnings.
Scrushys lawyers say he is innocentand has done nothing wrong.
Inflated earnings chargedThe SEC contends that shortly after
HealthSouth went public in 1986, atScrushys instruction, the companybegan inflating earnings to match WallStreet expectations and keep the stockprice up.
If quarterly earnings looked like they
would fall short, Scrushy would tellmanagers to fix it by recording falseearnings.
In August 2002, when senior officersconvinced Scrushy to take steps to lowerWall Street expectations, he authorized ascheme to blame a Medicare billing rule.The rule required rehab therapists treat-ing more than one patient at a time to billat the group rate rather than an individ-ual rate. HealthSouth said it had notunderstood the ruling and was reducingexpected earnings by $175 millionbecause of the lower reimbursementrates. The SEC alleges this was a smokescreen to reduce the companys need toartificially inflate earnings. But the SECalleges Scrushy and others still certifiedunder oath that its SEC filings were true.
Though the company said it wascontinuing to conduct business normal-ly, the April 5 Wall Street Journal report-ed that physician partners in Health-South surgery centers were worriedabout the companys image and whatmight happen to their interests if thecompany files for bankruptcy. Surgerycenters generated about one quarter ofthe companys revenue in 2002, accord-ing to the Journal. ❖
U S accuses HealthSouth of “massive fraud”
Youre not finished with HIPAAyet. Most organizations havegeared up for the privacy rule,which went into effect April 14.
But another regulationthe finalsecurity rulewas published Feb 20. Itis another major rule to carry out theHealth Insurance Portability andAccountability Act.
The security rule requires organiza-tions to take steps to safeguard patientselectronic protected health information(EPHI).
The security rule will not beenforced for most entities until 2005.But because the security rule overlapswith the privacy rule, its a good idea toaddress some of the security rulesrequirements now.
Here is a rundown on the securityrule from Robert Tennant, a HIPAAexpert and government affairs directorfor the Medical Group ManagementAssociation (MGMA).
Who does the rule cover? The security rule applies to covered
entitieshealth plans, health careclearinghouses, and health careproviders, (such as doctors, hospitals,and surgery centers) who transmit anyprotected health information in elec-tronic form.
What’s the scope of this rule? The security rule requires organiza-
tions to safeguard the integrity, confi-dentiality, and availability of patientsEPHI. Information must be protectedwhile it is received, created, stored, andtransmitted.
The standard covers only computer-ized information. It does not coverpaper-to-paper faxes, phone calls, videoconferencing, or voice mail messages.
The standard does, however, covercomputer-generated faxes even if youreceive them on paper and fax-backsystems that allow a person to requestinformation from a computer usingvoice or a keypad.
What are the rule’s basicrequirements?
In brief, the rule requires you to: 1. Conduct a risk analysis for security
gaps.
2. Take steps to mitigate the risks youidentified.The rule has a host of requirements
that will require policies and proce-dures for three major areas: Administrative safeguards: Exam-
ples: Assigning responsibility forsecurity, providing security aware-ness and training.
Physical safeguards. Example:Limiting access to information systemsand places where they are housed.
Technical safeguards: Example:Having procedures to verify thatpersons authorized to have access toEPHI are who they claim to be.
Two concepts to be aware of: The rule has both required and
addressable components. Requi-red components obviously must beimplemented. Addressable compo-nents give you flexibility in how toaddress an issue.
If you elect not to implement anaddressable component, you need todocument why it was not imple-mented. The good news is that the final rule
is more flexible than the proposed ruleissued in 1998.
Says Tennant, This is very different
from other HIPAA rules and the pro-posed security rule in that it says anorganization can take cost into accountin its decision about whether to imple-ment certain measures.
Significantly, the rule lets you weighnot only the cost of security but also thesize of your organization, your capabili-ties, and the potential threats. Forexample, if you are a cosmetic surgerycenter in Beverly Hills, you may needto protect against snooping reporters. Ifyour center has good firewalls to pro-tect against external threats, you maydetermine that your key threats areinternal, say, from employees.
You can look at all of these factorsand decide on the best strategies to fityour organization, Tennant says.
What’s involved in the riskassessment?
A good risk assessment is the key tomeeting the security rule. The rulestates that covered entities must con-duct an accurate and thorough assess-ment of the potential risks and vulnera-bilities to the confidentiality, integrity,and availability of EPHI held by thecovered entity.
Risk is defined in the rule as a spe-cific threat that will exploit a flaw orweakness in your system and theimpact of that event. The threats areusually rated as high, medium, or low.
Examples of threats are: natural disasters like floods or earth-
quakes
human problems like accidentaldeletion of data or intentional inva-sion of the system
environmental events like powerfailures or a hazardous materialspill.The first step in the risk assessment
is taking an inventory of EPHI and theinformation systems in your ASC.Among items the inventory wouldinclude are:
25OR Manager Vol 19, No 5May 2003
AmbulatorySurgery
Complying with HIPAA’s security rule
Continued on page 26
“The good news isthe final rule ismore flexible.
“
hardware and software
internal and external interfaces withthe information system
primary users of the informationsystem and EPHI
the basic function and purpose ofthe EPHI and the information sys-tem
technical controls for protectingEPHI, such as passwords andencryption
nontechnical controls, such as secu-rity policies and employee training.Based on the risks you identify, you
need to take steps to mitigate them.Most of these are things you should
already be doing anyway, saysTennant.
Examples are systematic data stor-age and backup and controlling accessto electronic information.
The rule says you can use the riskassessment as a tool to assess safe-guards you already employ anddemonstrate how they meet the rulesrequirements. If the assessment showsyou already have appropriate securityprotections, you only need to make surethose are documented. You also need toreassess periodically to make sure theprotections are appropriate and areactually being followed.
Can we rely on our softwarevendor to help us out withthis?
Vendors are not covered entitiesunder HIPAA, so they are under noobligation to comply with the regula-tions. But most have security measuresbuilt into their systems, says Tennant.
As part of the risk assessment, con-sider how closely your current informa-tion system meets the security rule andwhere there are gaps. If you find gaps,talk to your IS vendor to see how theycan be addressed.
If you plan to upgrade your infor-mation system, make compliance withthe security rule part of your requestfor proposal.
How does the security rulerelate to the privacy rule?
The security rule is more limitedthan the privacy rule because it appliesto electronic information. The privacyrule applies to protected health infor-mation in any form (eg, oral conversa-tions and paper).
If the privacy and securityrules overlap, are there thingswe should be doing now?
In my mind, security is an exten-sion of privacy, says Tennant. Ifsomeone hacks into your computer sys-tem, and patient information is dis-closed, it will be hard to argue that youstill had 2 years to comply with thesecurity rule.
He advises ASCs to take steps toprotect electronic data now, especiallyits physical security.
Walk around your center and see ifthere are places where an unauthorizedperson could have access to your com-puter system, Tennant says.
Do you have passwords or othersecurity mea