Embed Size (px)
Citation preview

The molecular pathologist’s view: how to satisfy increasing demand for multiple biomarker testing from limited sample size? Luca Quagliata Institute for Medical Genetics and Pathology University Hospital of Basel, Switzerland

Disclosure The data presented here are the sole property of the author and his institution. The idea and concepts proposed are based on his experience and are not influenced by any means by Novartis or Thermo Fisher Scientific. Novartis covered conference registration, travel, accommodation, and honorarium expenses for the speaker.
Disclosure – Year 2017 (research support, travel sponsor, honorarium)

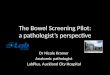
NSCLC molecular subtypes Extensive genomics studies resulted in clinically relevant findings
Tsao AS, et al. J Thorac Oncol. 2016;11:613-38.
Unknown oncogenic
driver detected
31%
KRAS 25%
EGFR-sensitizing
17%
ALK 7%
EGFR other 4%
MET 3%
HER2 2%
ROS1 2%
BRAF 2%
RET 2%
NTRK1 1%
PIK3CA 1%
MEK1 1%
ALK, anaplastic lymphoma kinase; BRAF, B-Raf proto-oncogene; EGFR, epidermal growth factor receptor; HER2, human epidermal growth factor receptor 2; MEK1, mitogen-activated protein kinase 1; MET, mesenchymal-epidermal transition; NTRK1, neurotrophic tyrosine kinase receptor 1; RET, rearranged during transfection; PIK3CA, phosphatidylinositol-4,5-bisphosphate 3-kinase, catalytic subunit alpha; ROS1, ROS1 proto-oncogene receptor tyrosine kinase.
Key 1 - Phase 1 2 - Phase 2 3 - Phase 3 4 - Approved
EGFR-sensitizing • Gefitinib4
• Erlotinib4
• Afatinib4
• Osimertinib4
ALK • Crizotinib4
• Alectinib4
• Ceritinib4
• Lorlatinib2
• Brigatinib2
MET • Crizotinib2
• Cabozantinib2
HER2 • Trastuzumab
• Afatinib2
• Dacomitinib2
ROS1 • Crizotinib4
• Cabozantinib2
• Ceritinib2
• Lorlatinib2
• DS-6051b1
BRAF • Vemurafenib2
• Dabrafenib2
RET • Cabozatinib2
• Alectinib2
• Apatinib2 • Vandetanib2
• Ponatinib2
• Lenvatinib2
NTRK1 • Entrectinib2
• LOXO-1012
• Cabozantinib2
PIK3CA • LY30234142
• PQR 3091
MEK1 • Trametinib2
• Selumetinib3
• Cobimetinib1

NCCN testing guidelines A pressing demand for comprehensive molecular diagnostics
National Comprehensive Cancer Network. Non-Small Cell Lung Cancer Guidelines (Version 8.2017). Available from. https://www.nccn.org/professionals/physician_gls/PDF/nscl.pdf. Accessed September 2017. NCCN, National Comprehensive Cancer Network.

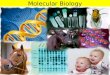
Molecular pathology has faced a sustained growth Historical trend of analysed samples (Basel)
CAGR, compound annual growth rate.
0
500
1,000
1,500
2010 2011 2012 2013 2014 2015 2016
Sam
ples
“Investments made within the Molecular Unit turned into a constant and substantial growth over the past years with an overall CAGR of 10.42%”
n = 750 n = 887 n = 907
n = 980
n = 1,156 n = 1,255
n = 1,501
Property of the University Hospital of Basel.

Examples of analysed sample types Heterogeneous source of starting material
Property of the University Hospital of Basel.
Tissue punch
Biopsy Resected Cytology Biopsy
Laser microdissection Liquid Biopsy

How to proceed with molecular testing – 2014 Swiss Lung Pathology Group recommendations (2014)
AC, adenocarcinoma; Amp, amplification; FISH, fluorescence in situ hybridization; KRAS, Kirsten rat sarcoma viral oncogene homologue; PD-L1, programmed death ligand 1; TAT, turn-around time. Courtesy of Prof Lukas Bubendorf - University Hospital of Basel
If negative
ALK FISH
ROS FISH If negative
RET FISH If negative
If positive If positive
Desirable TAT 1 day
Desirable TAT 10 days
AC/AC phenotype Stage IIIB/IV
Immunohistochemistry
ALK ROS1
Mutation analysis covering at least: EGFR KRAS HER2 BRAF – e.g. Sanger combination
Additional tests • Resistance mutations • PD-L1 IHC • EGFR IHC • MET Amp • METex14 Effective but
too complex!

How to proceed with molecular testing – 2017 Internal guidelines at the USB
Desirable TAT 1 day
Desirable TAT 5 days
AC/AC phenotype Stage IIIB/IV
Immunohistochemistry
ALK ROS1 PD-L1 MET
Mutation analysis covering: Oncomine™ Solid Tumour DNA kit
(EGFR KRAS HER2 BRAF)
Oncomine™ Solid Tumour Fusion panel (ALK ROS1 RET NTKR1)
If negative Additional tests: MET Amp METex14
If negative
Courtesy of Prof Lukas Bubendorf - University Hospital of Basel USB: University Hospital of Basel
Unidirectional, simplified and very effective!

Technological breakthrough in molecular pathology NGS is changing routine practice in pathology

Next generation sequencing (NGS) evolution NGS is a kind of revolution
Sanger Few base pairs A few hotspots One exone
One gene Whole exome Entire genome NGS

NGS workflow overview: an established path Is that compatible with our work?
QC, quality control. Modified from Quagliata L, et al. 2017, Schweizer Krebsbulletin, Nr. 1/2017, ISSN 2297-0703 . From the initial sample to the final report within 5-7 working days
Sample sources
DNA/RNA extraction Sequencing Data
generation Report
Small tissue biopsy
Cytology specimen
Liquid biopsy
Tumour-specific panel of genes
Library preparation
DNA/RNA extraction
Sequencing platform preparation
0% No template 33,811,202 100%
Enrichment
10% Empty wells 33,811,833 90%
Loading
38% Polyclonal 21,115,607 62%
Clonal
Bioinformatic analysis Variant calling
and classification
Signal processing
Alignment QC
Read filter
Base caller
Classification
DAT processing
L858R DEL18
INS9 G719A G719S L861Q INS12 V600E G12V G12A G12D
E545K
EGFR
ERBB2 BRAF
KRAS
PIK3CAC

Fusion variants described in the Cosmic database as related to lung cancer plus some additional variants identified by the OncoNetwork Consortium.
ALK translocation/ceritinib/crizotinib: approved ROS1 translocation/crizotinib: approved RET translocation/vandetanib: phase 33 clinical trial NTKR1: early clinical evidence
EGFR approved BRAF approved KRAS highly clinical relevant ERBB2 highly clinical relevant
What currently matters is there
NGS for NSCLC: a robust solution Covering all clinically relevant variants
NA, not applicable. Modified from the web info of

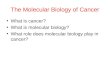
Sequencing of NSLCL: 2015–2016 results Sanger vs NGS: any winner? No need to fight
Quagliata L, et al. Unpublished data.
Sanger vs NGS sample distribution
No major differences in the incidence of driver gene alterations, as detected by the two methods. However, NGS intercepts a slightly higher number of EGFR and BRAF mutations
40.24% biopsy 59.76% cytology
Sanger (n = 1,225) N = 1,805
(n = 732)
(n = 493)
(n = 259)
(n = 312)
44.65% biopsy 55.35% cytology
NGS (n = 580)
Independent of the methods used, about 50% of samples still do not have driver gene mutations
n = 1,225
52.4% Driver-negative 29.5% KRAS (+) 13.0% EGFR (+) 3.8% BRAF (+) 1.0% HER2 (+) 0.2% EGFR + KRAS 0.2% KRAS + BRAF 0.1% EGFR + BRAF 0% EGFR + HER2 0% KRAS + HER2
Driver mutations distribution with Sanger 48.6% Driver-negative 30.0% KRAS (+) 14.1% EGFR (+) 6.2% BRAF (+) 0.5% HER2 (+) 0.2% EGFR + KRAS 0.2% KRAS + BRAF 0.2% EGFR + BRAF 0% EGFR + HER2 0% KRAS + HER2
Driver mutations distribution with NGS
n = 580

Molecular diagnostics: no tissue is left behind Make the best out of the limited resources
Property of the University Hospital of Basel.
For DNA extraction
(If needed) for RNA extraction
(If needed) for confirmation FISH
NSCLC samples overall rejection rate

Molecular diagnostics: no tissue is left behind It is a kind of Magic
Property of the University Hospital of Basel.

Molecular diagnostics: no tissue is left behind It is not just a matter of how much
Quagliata L, et al. Unpublished data.
Minimal additional time burden!

Mutually exclusive variants
Top mutated genes
NGS of NSLCL: what can we learn? NGS provides a handful of information
Quagliata L, et al. Unpublished data.
Agents Status Agents Status Agents Status Agents Status AKT1 On trial FGFR3 On trial EGFR Approved PIK3CA On trial ALK On trial KRAS Clin relevant ERBB2 Approved PTEN Clin relevant
BRAF Approved MET Approved FBXW7 Clin relevant STK11 Clin relevant DDR2 On trial NRAS Clin relevant FGFR1 On trial TP53 Clin relevant
Data highlights that 52% of patients are eligible for targeted therapy (in/off label Data also highlights that 71% has some mutations that might be clinically relevant

Not all is bright and shining Criticisms to precision medicine – how bad can it be?

The causes and consequences of genetic heterogeneity in cancer evolution
NSCLC are indeed heterogeneous entities How can we sort out the problem of tumour heterogeneity? Listen to the next talk…
Burrell RA, et al. Nature. 2013;501:338-45.
Lars Grimm, MD, MHS | December 22, 2015, Medscape
Imaging suspect
Tumour biopsy
Traditional histology-based classification

Acknowledgements
Contact: [email protected]
Institute of Medical Genetics and Pathology
Molecular Team:
Alexandra, Anja, Barbara, Claudia, Linda, Tanja, Sybille I, Sybille II, Valeria
R&D Unit:
PD Dr C Ruiz, Dr I Bratic Hech, Dr C NG, Dr S Piscuoglio, Dr P Jermann, Dr S Nicolet
Molecular Pathologists:
Prof L Terracciano, PD Dr M Bihl, Dr M Matter, PD Dr S Holler
Lung Specialists:
Prof L Bubendorf, PD Dr S Savic

Lung tumour classification Large vs small specimens – an open issue
Modified from Gridelli C, et al. Nat Rev Dis Primers. 2015;1:15009.
Adenocarcinoma • Mixed subtypes • Lepidic (non-mucinous or mucinous) • Acinar • Papillary • Micropapillary • Solid
Large-cell carcinoma • Large-cell neuroendocrine
carcinoma
Squamous Non-squamous
Small-cell lung cancer Non-small-cell lung cancer
Lung cancer
15% 85%
70%
90%
30%
10%

Living in the personalized-medicine era The concept in a nutshell
Modified from Quagliata L, et al. 2017, Schweizer Krebsbulletin, Nr. 1/2017, ISSN 2297-0703 . Available from: www.aboutcancer.com/lung_CT_BMC_Feb_2007.jpg. Available from: business.inquirer.net/122469/first-endobronchial-ultrasound-procedures-in-ph.
Clinical suspect and investigation
DRUG TARGET MANUFACTURER Erlotinib (Tarceva) EGFR Roche
Dacomitinib/PF-00299804 EGFR Pfizer Gefitinib (Iressa) EGFR AstraZeneca Afatinib (Gilotrif) EGFR Boehringer Ingelheim
Rociletinib/CO-1686 EGFR T790M Clovis AZD9291 EGFR T790M AstraZeneca Icotinib EGFR Beta Pharma, Inc
Necitumumab/IMC-11F8 EGFR (Mab) Lilly Trastuzumab (Herceptin) ERBB2 Roche
T-DM1 (Kadcyla) ERBB2 Roche MM-121 ERBB3 Merrimack
Crizotinib (Xalkori) ALK, ROS Pfizer LDK378/ceritinib (Zykadia) ALK Novartis
Alectinib/RO5424802/ ALK Roche, Chugai PF-06463922 ALK, ROS Pfizer
RXDX-101 ALK, ROS, NTRK1 Ignyta Cabozantinib/XL184 MET, RET Exelixis
INC280 MET Novartis, Incyte Vandetanib/ZD6474 RET AstraZeneca

Living in the personalized-medicine era The concept in a nutshell
Modified from Quagliata L, et al. 2017, Schweizer Krebsbulletin, Nr. 1/2017, ISSN 2297-0703 . Available from: www.aboutcancer.com/lung_CT_BMC_Feb_2007.jpg. Available from: business.inquirer.net/122469/first-endobronchial-ultrasound-procedures-in-ph.
Clinical suspect and investigation
Sample extraction and molecular profiling
Data analysis and reporting
Sample collection and assessment
Treatment decision

Our working frame: precision medicine A shifting paradigm in medicine