-
8/13/2019 The Management of Mental Illness Among Maharashtrian
Families
1/20
The Management of Mental Illness Among Maharashtrian Families: A
Case Study of a
Mahanubhav Healing TempleAuthor(s): Vieda SkultansSource: Man,
New Series, Vol. 22, No. 4 (Dec., 1987), pp. 661-679Published by:
Royal Anthropological Institute of Great Britain and IrelandStable
URL: http://www.jstor.org/stable/2803357
Accessed: 16/11/2010 09:26
Your use of the JSTOR archive indicates your acceptance of
JSTOR's Terms and Conditions of Use, available at
http://www.jstor.org/page/info/about/policies/terms.jsp. JSTOR's
Terms and Conditions of Use provides, in part, that unless
you have obtained prior permission, you may not download an
entire issue of a journal or multiple copies of articles, and
you
may use content in the JSTOR archive only for your personal,
non-commercial use.
Please contact the publisher regarding any further use of this
work. Publisher contact information may be obtained at
http://www.jstor.org/action/showPublisher?publisherCode=rai.
Each copy of any part of a JSTOR transmission must contain the
same copyright notice that appears on the screen or printed
page of such transmission.
JSTOR is a not-for-profit service that helps scholars,
researchers, and students discover, use, and build upon a wide
range of
content in a trusted digital archive. We use information
technology and tools to increase productivity and facilitate new
forms
of scholarship. For more information about JSTOR, please contact
[email protected].
Royal Anthropological Institute of Great Britain and Irelandis
collaborating with JSTOR to digitize, preserve
and extend access toMan.
http://www.jstor.org
http://www.jstor.org/action/showPublisher?publisherCode=raihttp://www.jstor.org/stable/2803357?origin=JSTOR-pdfhttp://www.jstor.org/page/info/about/policies/terms.jsphttp://www.jstor.org/action/showPublisher?publisherCode=raihttp://www.jstor.org/action/showPublisher?publisherCode=raihttp://www.jstor.org/page/info/about/policies/terms.jsphttp://www.jstor.org/stable/2803357?origin=JSTOR-pdfhttp://www.jstor.org/action/showPublisher?publisherCode=rai
-
8/13/2019 The Management of Mental Illness Among Maharashtrian
Families
2/20
THE MANAGEMENT OF MENTAL ILLNESS AMONGMAHARASHTRIAN FAMILIES: A
CASE STUDY OF A
MAHANUBHAV HEALING TEMPLEVIEDASKULTANSUniversityofBristol
Fieldwork was carried out in a Mahanubhav healing temple in
Maharashtra. Women'sresponsibility for the health andwell-being of
the family is given a novel andliteralinterpretationin this
setting. Women come as care givers accompanying a mentally ill
family member. Butalthough they arrive as care givers and, indeed,
continue to fulfil that function, they becomeafflicted by trance
soon after their arrival. Women see this transformation into
patienthood asresulting from their devotion to their families.
Indeed, they pray that the illness be transferredfrom their sons,
husband or daughtersto themselves. It is thought thatregulartrance
will channelthe force of the earlierafflictionaway from the
original patient. Thus women cultivate trance as asacrificial
device to ensure the health andwell-being of the rest of the
family. This view of tranceisvigorously contested by the temple
experts, however, who see trance assymptomatic of femininepollution
and character weakness. This lack of consensus regarding the nature
of trance and thedistribution of affliction has cautionary
implications for a monistic approach to religious andmedical
institutions.
Women, illness and treatmentopportunitiesFieldwork was
carriedout in a Mahanubhav temple in Maharashtrarenownedfor its
trance inducing propertiesand its therapeuticpowers in relation to
mentalillness. This setting was chosen because it was
anticipatedthat large numbers ofpeople who considered themselves,
or were considered by others, to bementally ill would gather there.
The research had two kinds of distinct butinterrelated aims: one
being of a psychiatric epidemiological nature and theother
socio-anthropological. The psychiatric questions were prompted
bythe apparentcontrast between the sex distributionof psychiatric
disorderin thewest and in traditional societies. Western mental
health surveys, admission andconsultation figures all point to the
greater psychiatric morbidity of women.Psychiatric surveys in
developing countries do not follow this trend.Epidemiological
studies in non-industrialised societies do not appear toconfirm the
excess psychiatric morbidity found among women in the westernworld.
Although the field of cross-cultural psychiatry is large and
flourishing,however, and although women's mental health is a topic
of concern, theinteresting apparent difference between women's
mental health in westernindustrialised societies and
non-industrialised societies has not been investi-gated. A review
of population surveys in India suggests the direction ofresearch.
Incidentally, 'more population surveys for psychiatric illness
havebeen conducted in India than in any other developing country'
(Leff I98 I:90). A
Man (N.S.) 22, 66I-79
-
8/13/2019 The Management of Mental Illness Among Maharashtrian
Families
3/20
662 VIEDA SKULTANSstudy of the prevalence and type of mental
disorder in a village of West Bengalfound a lower rate of
psychiatricmorbidity for women than for men (Elnagaretal. I97I:
50I). Astudy ooking attheprevalence f mental
llnessamongfamiliesregistered with an urban health centreat Lucknow
again found women to haveslightly lower rates of mental illness
than men (Thacore et al. I975: 365). Thework of Carstairs and Kapur
in Karnataka State in south India provides anexception in that
their survey found a slight excess of female psychiatricmorbidity:
only 6o per cent. of women in their sample were symptom free,
asopposed to 68 per cent. of men (Kapur I975: 37). However, this
slight biastowards women in no way approachesthe situation
obtaining in the west (seeCarstairs& Kapur 976: I04).
Epidemiologicalindings must, of course,beapproached with caution,
since each survey employs different criteria forassessing mental
illness, but it remains true that whatever the threshold levelused,
a more equal male/female ratio is found than western findings would
leadone to expect.Hospital in-patient andout-patient figures show
that men outnumber womenby 3 to I (Kynch& Sen 983: 372)
andpsychiatric dmissioniguresappear obein line with general
hospital figures. It therefore seemed to be important toestablish
the psychiatric morbidity of supplicants seeking indigenous forms
ofcure at a healing temple, particularlysince there appears to be
an implicit andwidely held assumption that 'neurotic' women form
the bulk of the clientele oftraditional healersandhealing temples.
Although unforeseenpracticalproblemsmeant that psychiatric
assessments using the Present State Examination
(astandardisedpsychiatric interview schedule, see Wing et al. I974)
could not bemade, the anthropological interviews throw some light
on the direction inwhich answers to the epidemiological puzzles
might be sought.It is generally recognised that Indian women are
held responsible for thefamily'shealth see,forexample,Abdullah&
Zeidenstein982: 52). Moreover,health and, in
particular,mentalhealth, may be viewed as aproperty of
familiesratherthan individuals: 'South Asian ruralfamily members
may not have anyclear perception of individual welfare, having
instead some unsplittable com-pound notion of family well-being'
(Kynch & Sen I983: 364). However, datafrom the Mahanubhav
temple suggest that this compound notion of familywell-being
remains intact when mental illness of a male family member
isinvolved whereas when women encounter mental healthproblems the
notion offamily wellbeing is not as 'unsplittable'as Kynch and Sen
imply. It may be thatthe threat of separation from the family as
well as the active role assigned towomen in the promotion of family
health all contribute towards a lower rate ofmental disorder among
Indian women.
Mysticalaccounts f illnessCommon to Maharashtrianpopular culture
is a set of beliefs regarding illnessand misfortune: namely, that
they are frequently the result of possession by aspirit or
bhutbhada. n general, little interestis shown in discovering the
identityof the bhutor its characteristics.Possession by bhutmay
sometimes give rise totrancing, but more often it results in
ill-health or bad luck. Often possessed
-
8/13/2019 The Management of Mental Illness Among Maharashtrian
Families
4/20
VIEDA SKULTANS 663persons are not aware of suffering from bhut
bhadauntil they come into thevicinity of ahealing temple. Here the
power of the God or saint associated withthe temple or shrineis
thought to draw out the possessing spirit, thus encourag-ing
trance. In most cases of bhutbhada,karanis involved. Literally
translatedtheword means 'things done' and there is an implicit
understandingthat the thingsdone are bad. Stanley, in a paper on
possession in Maharashtra,has translatedkaranias black magic
(Stanley n.d.: 3). Perhaps the more general word witch-craft best
covers the several uses of the term karani. tis thought that
bhutbhadasusually brought about by means of karani. In such
instances an angered orenvious person will either ask God to send a
bhutupon their enemy, or else willrequest a mantrik magician)or
devrishi shaman)to do so. Again, there appearsto be little interest
in the technical details of karani,although the reasons for thebad
feelings will be spelt out in some detail. Thus there exists a set
of commonbeliefs about the spiritual provenance of illness which
underpinthe widespreadresort to healing centres. Throughout
Maharashtra many healing templesspecialise in the management and
cure of spiritual afflictions. The Muslimshrines or dargahs n
Bombay and Pune cater for many thousands a weekwho present with a
wide variety of afflictions. The temples of the HinduMahanubhav
panth (sect) also cater for spiritualafflictions, in
particular,thosewhich give rise to mental illness.The Mahanubhav
sect arose in the thirteenthcentury forming part of a widermovement
of the time which emphasisedbhaktior devotion. The
characteristicsof this sect which set it apartfrom orthodox
Hinduism have been describedbyother scholars (Raeside I976;
Feldhaus I983). Feldhaus cites the rejection ofcaste and the
worship of idols, the refusal to acknowledge the
scripturalauthority of the Brahmins, the creation of a female order
of sannyasis andthe belief in a single God Parmeshwar as evidence
of the heterodoxy of theMahanubhavs (Feldhaus n.d.: i) Despite
doctrinal differences, however, theMahanubhav temples are
frequented by all Hindus in times of trouble and atthe major
Mahanubhav festivals. Temple users have in common poverty
andilliteracy rather than sect affiliation.Feldhaus describes the
Mahanubhav God as one who 'can be addressed in thelanguage of the
people, not just in the Sanskritof the erudite and the
religiousprofessionals, and can be approached by members of all
castes and both sexes'(I984: 4). Thus the Mahanubhav temples
provide the setting for a directexperience of and dialogue with
God. Given the nature of the problemsbesetting many of the
supplicants the immediacy of this relationship is impor-tant.
Individuals and theirfamilies are drawn to the temples because they
can getdetailed and personal information and advice about their
particular health orfamily problems. Here unconventional and
uncontrolled behaviour is toleratedand even encouraged. For
example, dialogues with God take place duringtrance. Indeed, there
is a divine precedentfor outrageous behaviour. Accordingto
Mahanubhavbelief, Parmeshvar hastaken five avatars rhuma-n
ncarnations:Krishna, Dattatreya, Cakradhara, Govindaprabhu, also
known as GundamRaul, and Cangdev Raul. The biography of Gundam Raul
portrays him asbreaking all the social and religious rules
regarding proper behaviout. Feldhauswrites: 'The text shows that
God transcends not only the rules of ritual and
-
8/13/2019 The Management of Mental Illness Among Maharashtrian
Families
5/20
664 VIEDA SKULTANSmorality and the hierarchiesof caste, sex and
learning, but the conventions ofpoliteness and sanity as well. For
the text shows that Gundam Raul was God,and it shows thathe was
mad' (I984: 4). Indeed, that madness is itself evidence ofhis
divinity. Thus the Mahanubhav writings suggest that their temples
areparticularlywell suited to the management of madness.
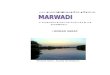
The Mahanubhav empleOne such centre which attracts large numbers
of people considered mad isPhaltan. Phaltan is a small town with a
population of about 40,000 in districtSatara. In terms of the
religious geography of the Mahanubhavs, Phaltanoccupies animportant
position. Itis thebirthplaceof Cakradhara, he founderofthe sect.
There are three Mahanubhav temples in the town. One of these,
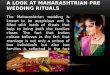
theAbbasai temple catersfor the mentally ill. Here accommodation is
provided forpatients and their families. Thirty-five small open
dormitories surround thetemple (see fig. i). Each family is
assigned a space measuring about 4' X IO'where they can store their
cooking pots, bed rolls and other belongings.Families come from the
whole of Maharashtraalthough most are from districtSatara.The
average stay lasts threeto four months, although families
areusuallypreparedto stay until the sick person is cured. Whatever
the turnover of templeresidents, the temple remains full at all
times. During the period of the study(November I984 to April I985)
there were forty-one 'cases' for which aspiritualresolution or cure
was being sought. All the caseswere investigated by
lengthyinterviews with the patients and their families.The
following picture emerged: therewere fifty-six women and
twenty-eightmen supplicants. These figures appear to confirm both
the anthropologists'account of healing temples and trancing and the
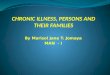
views of priests and localtownspeople. However, when each case was
looked at more closely a differentpicture emerged (see fig. 2).
Twenty-two families came on behalf of a man,twelve came on behalf
of a woman and nine women came alone. There weremore women than men
accompanying the sick person. The greaternumber offemale caretakers
and the fact that middle-aged and older women were
oftenunaccompanied accounts for the greater overall number of women
in thetemple. This might prompt a casual observer to conclude that
the temple caterslargely for women's needs. In fact, the temple
answers the needs of two quitedifferent categories of persons. In
one category are women who come to thetemple because of some major
upheaval or conflict in family relationships.Nearly all the women
in this category aredivorced, widowed or childless andthey come to
the temple alone. Frequently, their husbands have remarried.They
come to the temple feeling depressed and tired. Without exception
allthese women learn to trance at the temple. In a few cases women
who appeartobe expressing family problems through
theirtrancingareaccompaniedby otherfamily members. Although
psychiatric interviews were not carriedout,1 it wasmy impression
that many of these women would not score high on neuroticism.These
women come to the temple, not so much because their symptoms
areintolerable, as because their social situation is intolerable:
they have failed toattainor have lost a respectable position in the
family. In these cases the temple
-
8/13/2019 The Management of Mental Illness Among Maharashtrian
Families
6/20
VIEDA SKULTANS 665
provides a refuge which in some cases becomes a permanent
home.In the other category are people brought by their families
because theirbehaviour has become intolerable and unmanageable.
Many of them have spentlong periods in psychiatric hospitals and
have been discharged as incurable.Everyone in this category
manifests behaviour which falls far beyond thebounds of the
socially acceptable. Quite how madness is defined, and the
22 21 20 19 18 1700 0 0 0 0 0 0 0 0 0 0
VU CY 0lEE < s
C1
-. i 1 D [ OT
' INNERTREE WTANKTML
Lnz o z
Cy 0 0 -
z ~ z Az
(.) INNER COURTYARDEY EAcS
13.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~TREEITHUREI-
CY PLATFORM 0-mc
gc] 0u0
71 ~~~~~~~OTHA 0o 0
INN ERSANCTUARY O0N
O-'Cd) ~~~~~~~~~~~~~~~~ENTRYrum forwU FROM pry0 0 0 0 NORTH
pae
0 0 0 0 PLATFORMC.) 00 0 0zI 0 Lamp ree
C.) 0 0 0~~~~~~~TH 0 of stones0~~~~~~~13. ~~0 0 INNER 0 0Cd)
~~~~~~TEMPLE0 0 0 0
0 0 0 0 0 0
0 0 0 0 0 0ENTRY FROM EAST
FIGURE I.
-
8/13/2019 The Management of Mental Illness Among Maharashtrian
Families
7/20
666 VIEDA SKULTANSbounds of social acceptability delineated, is
not made altogether explicit.Although there is no dispute over who
is designated as mad, the criteriadetermining madness do not
appearto be given much thought. Given that thetemple is considered
the appropriate refuge for the mad, there is a curiousabsence of
reflection or theorising about madness. Answers to questions
abouthow madness was recognised were hesitant and it became clear
that there wereno explicit and detailed theories of the kind that
anthropologists often expect.
e- - + + L~J 2.> co , 2 .. J
J 20~~~~~~~~~~~0> w~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~40a)
co. ~ ~ Z- )a
> Li U)+ c c u -4- C)~~~~~-
Li n 'aEz a,) L< co C) P - t- %~ ~ 5 Cz >. a,
a,'-'-~~~~~~~~~~~~~~)2 CO < LL 0 rz) >M~~,~C ..a, , E< ~a-
E E.~~~~~~~~~~~~~~~a,DO~~~~~~~~~~~I) c
0 CL~~~~~~~~+~ . ~ 'crLi H 0 +
c-i N + -'Z-'~~~~~~~~~~~~~~~~~~~~~~~~+
a,~~~~~~~~~~~~~~~~~~~~~~
< C0DD~~~~~~~~ a,< ). E(Liij
m E + 0 cu.0 , acu CD =~~~~~~~~~~a +C) C,~~~~~~~~~~~~~~cC >f.
cu -0 - CD f..~~~0 a,
C: a) + C) ~ a a, ou .0 I- a) - I CO a, a,
0 C:)~~~~~~~~~~~~~,o ~~~~~~~~~ C-~~~~~~~~~~~~~~~~IoN .-
-~~~~~~~~~~~~~~~~~~~, m L< Z CU CU$Ma,L'u. .O a ..
a,u~a 0u ~ 0 Oa..C H 1 CoUi