Embed Size (px)
Citation preview

Endocrine-RelatedCancer
ReviewM C Bruce et al. Kinome associated with
ER-positive status21 :5 R357–R370
The kinome associatedwith estrogenreceptor-positive status in humanbreast cancer
M Christine Bruce, Danielle McAllister and Leigh C Murphy
Department of Biochemistry and Medical Genetics, Manitoba Institute of Cell Biology, University of Manitoba
and CancerCare Manitoba, 675 McDermot Avenue, Winnipeg, Manitoba, Canada R3E 0V9
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
Published by Bioscientifica Ltd.
Correspondence
should be addressed
to L C Murphy
Leigh.Murphy@
med.umanitoba.ca
Abstract
Estrogen receptor alpha (ERa) regulates and is regulated by kinases involved in several
functions associated with the hallmarks of cancer. The following literature review strongly
suggests that distinct kinomes exist for ERa-positive and -negative human breast cancers.
Importantly, consistent with the known heterogeneity of ERa-positive cancers, different
subgroups exist, which can be defined by different kinome signatures, which in turn are
correlated with clinical outcome. Strong evidence supports the interplay of kinase networks,
suggesting that targeting a single node may not be sufficient to inhibit the network.
Therefore, identifying the important hubs/nodes associated with each clinically relevant
kinome in ERC tumors could offer the ability to implement the best therapy options at
diagnosis, either endocrine therapy alone or together with other targeted therapies,
for improved overall outcome.
Key Words
" estrogen receptors
" breast cancer
" phosphorylation
" kinases
" endocrine therapy sensitivity
" biomarker
Endocrine-Related Cancer
(2014) 21, R357–R370
Introduction
The idea of personalized approaches to therapy in breast
cancer based on the molecular nature of the tumor can be
traced back to the late 1960s and early 1970s, when it was
discovered that some but not all human breast tumors
express estrogen receptors (ERs; Jensen et al. 1971). This
heralded the beginning of an era of targeted therapies for
breast cancer, identified the first biomarker used clinically
to predict the biological behavior of breast cancer, and
established the beginnings of understanding molecular
mechanisms by which the ovarian hormone, estrogen,
drives the growth and survival of the majority of human
breast cancers (Jensen & Jordan 2003), at least initially.
Inhibiting the activity of ERs with the antiestrogen
tamoxifen was the first targeted therapy in breast cancer.
Although the knowledge that female hormones were
involved in breast cancer and the hormonal/endocrine
therapy was used for breast cancer at least in the form of
ablation surgery such as ovariectomy dates back well over
a century, the identification of ERs in breast cancers
provided a molecular mechanism and rationale for the use
of hormonal therapies (Jensen & Jordan 2003). This led
directly to the development of the successful modern
endocrine therapies such as tamoxifen and other selective
estrogen receptor modulators (SERMs), which bind to the
ERs and induce conformational changes that modify and
in some cases inactivate the ERs (Jensen & Jordan 2003).
The newer endocrine therapies, the aromatase inhibitors
(AIs), which inhibit the aromatase enzyme, eliminate the
production of estrogen and therefore inhibit estrogen’s
proliferative action (Goss et al. 2011).
It was evident from the start that not all ERC breast
tumors were created equal. Although a little more than

Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R358
70% of all breast tumors express ER, only about half of
patients with ERC tumors respond to tamoxifen. There-
fore, ERC breast cancers exhibit heterogeneity associated
with prognosis and treatment outcomes. The first step to
resolve this heterogeneity came from the idea that the
measurement of a downstream target of estrogen-
dependent ER signaling such as the progesterone receptor
(PR) would increase confidence that the pathway was
intact (Horwitz et al. 1975). This increased the accuracy of
treatment prediction, but was obviously still imprecise as
some 20–30% of ERC/PRC tumors are de novo resistant to
the endocrine therapies. Furthermore, initial response to
endocrine therapies is often followed by acquired resist-
ance despite the continued expression of ER (Encarnacion
et al. 1993, Bachleitner-Hofmann et al. 2002).
The next significant insight into the heterogeneity of
ERC breast cancer came with the identification of HER2
(ERBB2) amplification. Approximately 20% of all breast
cancers have amplified, overexpressed HER2, and 40–50%
of these will also be ERC. Interestingly, ERC/HER2C
tumors are more likely to be resistant to endocrine
therapy, in particular tamoxifen, thus providing
important insight into the relevance of crosstalk of
signaling pathways initiated at the level of the plasma
membrane with many aspects of the ER signaling
pathway. This may cause ligand-independent activation
of ER signaling and hormone therapy resistance.
The molecular detailing that has become possible
through the Human Genome Project and new high-
throughput/high-content technologies in the last decade
initially established five intrinsic molecular subgroups
(Sorlie et al. 2003) of which three were significantly
populated with ERC tumors. Most recently, at least ten
molecular subgroups of human breast cancer have been
described (Curtis et al. 2012) and eight of these appeared to
be significantly populated with ERC tumors (Curtis et al.
2012). Associated with these studies has been the frequent
identification of kinases, either mutated and/or structurally
altered in large cohorts of breast tumors (Banerji et al. 2012,
Curtis et al. 2012, Shah et al. 2012, Stephens et al. 2012).
Some of these have also been found frequently altered and
associated with AI sensitivity (Ellis et al. 2012).
ER and its many coactivators are regulated by
phosphorylation as well as other post-translational
modifications (PTMs; Rowan et al. 2000, York et al. 2010,
Le Romancer et al. 2011, Zhang et al. 2013). The discovery
that the ER and its coactivators are substrates of several
kinases (enzymes causing phosphorylation of specific
substrates), which are regulated by signaling pathways
frequently mutated or structurally altered in breast cancer
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
(Yamnik et al. 2009, Yamnik & Holz 2010, Murphy et al.
2011), as well as the demonstration that a clinically
relevant phosphorylation profile of ERs can be identified
in human breast cancer (Skliris et al. 2010a), suggests that
kinases and/or phosphatases associated with ERC breast
cancer could provide a wealth of potential drug targets to
complement existing endocrine therapies or generate new
endocrine therapies. The following is a review of kinases
that have been identified as associated with ER status in
breast tumors or those that have been implicated in the
regulation of estrogen signaling and/or modifying sensi-
tivity to estrogen and its antagonists in breast cancer.
Kinases identified as mutated or structurallyaltered in breast cancer in large breast cancercohorts
Genome-wide analyses of large cohorts of breast cancer
cases are providing detailed, comprehensive analyses of
genomic aberrations in breast cancer at a population level.
Some studies have also provided data concerning their
impact on clinical characteristics. These studies have
shown that many of the frequently altered (amplified,
fused, deleted, or mutated) genes encode kinases. Some of
these frequently altered genes, such as HER2, were
previously known but others, such as MAP3K1 and its
substrate MAP2K4, have not previously been identified to
have functional roles in breast cancer. However, given that
enzymes, kinases in particular, have proven to be clinically
efficacious therapeutic targets, a wealth of data has now
been generated not only to understand the complex
biology of the disease but also to identify new treatments
for specific cohorts.
The recently published METABRIC cohort of breast
cancers, in which 2000 individual breast cancers were
interrogated, identified ten integrative clusters, each with
distinct molecular characteristics associated with clinical
outcome (Curtis et al. 2012). Often, altered genes encoding
kinases and phosphatases dominate individual clusters
(Table 1). Furthermore, the original intrinsic subtypes, in
particular the ERC luminal A and luminal B (Perou et al.
2000, Ignatiadis & Sotiriou 2013) subtypes, have been
further subdivided due to the METABRIC study (Curtis et al.
2012, Dawson et al. 2013). Therefore, a brief description of
this follows as it relates to clusters that have significant
ERC components.
METABRIC integrative cluster 1 (IntClust1), represent-
ing 7% of breast cancer (Curtis et al. 2012, Dawson et al.
2013), contains predominantly ERC tumors with luminal B
features and is characterized by amplification of the
Published by Bioscientifica Ltd.

Table 1 Kinases and phosphatases altered in ERC-dominated
breast cancer clusters from METABRIC (Curtis et al. 2012,
Dawson et al. 2013)
METABRIC
integrative clusters
Kinases or phosphatases
identified Alteration
IntClust1 Ribosomal protein S6kinase 1 (RPS6KB1)
Amplification/overexpression
Protein phosphatase1D (PPM1D)
Amplification/overexpression
IntClust2 PAK1 Amplification/overexpression
PIK3CA MutationIntClust3 PIK3CA Mutation
MAP3K1 MutationIntClust5 HER2 Amplification/
overexpressionPIK3CA Mutation
IntClust6 FGFR1 AmplificationIntClust7 PI3K Mutation
MAP3K1 MutationIntClust8 MAP2K4 Mutation
PI3K MutationIntClust9 Regulatory subunit B
of proteinphosphatase 2alpha (PPP2R2A)
Deletion
Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R359
17q23 region. Two genes in this amplicon associated with
increased expression are ribosomal protein S6 kinase beta 1
(RPS6KB1 and p70S6K1) and protein phosphatase 1D
(PPM1D). Interestingly, expression of both of these genes
has been shown to be regulated by estrogen in ERC breast
cancer cells at the transcriptional level (Han et al. 2009,
Yamnik et al. 2009, Yamnik & Holz 2010). In addition,
the protein product of RPS6KB1 (p70S6K1) has
been shown to phosphorylate ERa (Yamnik & Holz 2010)
and under IGF1 stimulation p70S6K1 can be
co-immunoprecipitated with ERa in ERC breast cancer
cells (Becker et al. 2011). PPM1D/Wip1 is known for its p53
inhibitory effects and, in ERC MCF7 cells, has been shown
to be regulated by estrogen and to increase the transcrip-
tional activity of ERa (ESR1) as well as other steroid hormone
receptors (Proia et al. 2006), possibly by modulating
phosphorylation of coactivators such as SRC1 and/or
p300/CBP (Proia et al. 2006).
Integrative cluster 2 (IntClust2), representing 4% of
breast tumors, is also dominated by ERC tumors with
characteristics of both luminal A and luminal B subtypes
(Dawson et al. 2013). Amplification of chromosome region
11q13/14 characterizes this cluster and high expression of
another kinase, PAK1, known to affect ERa phosphory-
lation and activity (Wang et al. 2002, Mazumdar & Kumar
2003, Holm et al. 2009, Kok et al. 2010) is associated with
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
its amplification in this region. A high frequency (w50%)
of PI3K catalytic subunit p110a (PIK3CA) mutations is also
observed in this group.
ERC tumors with luminal A characteristics predo-
minate integrative cluster 3 (IntClust3), which represents
15% of all breast tumors (Dawson et al. 2013). Tumors in
this cluster tend to have few structural alterations, low
genomic instability, and usually an excellent prognosis.
Interestingly, they also have the highest frequency of
PIK3CA mutations (w58%). As well, similar to other
clusters dominated by ERC tumors, a high level of
MAP3K1 mutations (w15%) is observed in IntClust3.
IntClust5 represents 10% of all breast tumors and is
characterized by HER2 amplification with w42% of them
also expressing ERa (Dawson et al. 2013). Approximately
30% of tumors in this cohort also have PIK3CA mutations.
ERC tumors with overexpressed HER2 are more likely to
be resistant to endocrine therapies. One reason for this is
thought to be the constitutive activation of several kinases
downstream of HER2, such as ERK1/2, PI3K, and AKT, all
of which can phosphorylate ERa and several ER coacti-
vators to enhance the ligand-independent activity of ERa
as well as to enhance the agonist activity of tamoxifen
(Wu et al. 2005, Le Romancer et al. 2011).
IntClust6, representing 4% of breast tumors, is another
predominantly ERC group with both luminal A and
luminal B characteristics (Dawson et al. 2013). Tumors of this
group show amplification of the chromosome 8p12 locus and
are genomically unstable with an intermediate prognosis.
Less than 20% of tumors in this group have PIK3CA
mutations, which is low compared to other ERC groups.
The gene for FGFR1 is located in the chromosome 8p12
region. FGFR1 amplification and overexpression have been
directly linked to endocrine therapy resistance (Turner et al.
2010, Balko et al. 2012). FGFR1 also regulates several kinases
such as PI3K and AKT, which are known to phosphorylate
ERa and its coactivators (Le Romancer et al. 2011).
IntClust7 (10% of breast tumors) and IntClust8 (15%
of breast tumors) are mainly ERC groups and while similar
in many ways tumors in Intclust8 display higher genomic
instability, with an associated inferior prognosis than
tumors in IntClust7 (Dawson et al. 2013). Interestingly,
both again have a high frequency of PI3K (PIK3CA)
mutations. IntClust7 has a high frequency of MAP3K1
mutations and IntClust8 has the highest frequency of
MAP2K4 mutations, a downstream target of MAP3K1.
The structural alterations usually found in MAP3K1
and MAP2K4 are deletions and mutations associated
with loss of function (Teng et al. 1997, Pham et al. 2013),
suggesting that the pathways they regulate have
Published by Bioscientifica Ltd.

Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R360
tumor-suppressor function. Steroid hormone receptor
signaling, including estrogen and androgen receptors,
shows crosstalk with MAP3K1 in some systems, and it is
the ERC tumors, in particular luminal A type, that have
the highest level of mutation and/or deletion of the
MAP3K1/MAP2K4 pathway (Pham et al. 2013). This
pathway has been implicated in cell death pathways,
which under normal conditions is important for mam-
mary gland involution, hence its loss of function in many
ERC breast cancers may in part be responsible for the
dissociation of estrogen-induced proliferative and survival
pathways from growth-inhibiting differentiation
pathways (Pham et al. 2013). This pathway has been
described as having a molecular switch type function
between survival and cell death, possibly dependent on
cell-type background, subcellular localization, and caspase
3 activity (Pham et al. 2013). Increased ERa expression
combined with a decreased activity of the MAP3K1/
MAP2K4 pathway may, in part, underlie the change in
the balance of estrogen signaling regulation of survival/
proliferation vs cell cycle inhibition that is often
associated with differentiation.
IntClust9 (7% of breast tumors) is characterized by
a high frequency of PPP2R2A deletions (Dawson et al.
2013). PPP2R2A is the regulatory subunit B of protein
phosphatase 2 alpha (PP2A). While IntClust9 contains a
mixture of intrinsic subtypes, its ERC members are mainly
of the luminal B type, and loss of PPP2R2A expression is
associated with a high mitotic index. Interestingly, PP2A
also has been implicated in the regulation of ERa
phosphorylation and activity (Lu et al. 2003a).
The above data underscore that distinctly altered
kinase and phosphatase mutation patterns occur frequently
in ERC breast cancer subgroups with altered clinical
outcome. This would support the idea that combining
endocrine therapies with other targeted therapies informed
by each subgroup’s distinct kinase pattern could provide
better clinical outcome for breast cancer patients.
Kinases associated with the PI3K/AKT/mTORand ER-positive breast cancer
METABRIC and similar studies (Curtis et al. 2012, Ellis et al.
2012, Stephens et al. 2012) as well as previous smaller scale
studies (Miller et al. 2010, 2011a,b) have identified the
frequent structural and mutational alterations in the
PI3K/AKT/mTOR pathway that occur in ERC breast cancer.
IntClust1, IntClust2, IntClust3, and IntClust5 (Dawson
et al. 2013) have w25, 50, 58, and 30% frequencies of
PIK3CA mutations respectively. IntClust7 and IntClust8
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
also have a high frequency of PIK3CA mutations while by
contrast IntClust6 has less than a 20% frequency of PI3K
pathway mutations (Dawson et al. 2013).
Experimental and clinical data suggest that hyper-
activation of the PI3K/AKT/mTOR pathway is associated
with endocrine resistance. However, gain-of-function
PIK3CA mutations in ERC tumors are often associated
with good prognosis (Miller et al. 2011a). Such apparently
contradictory results may be due to complexities associ-
ated with feedforward and feedback mechanisms involved
in the PI3K/AKT/mTOR pathway and other alterations
co-occurring in regulators of the pathway. This latter idea
is supported by the finding that most often the associ-
ations of PIK3CA mutations with good outcome in ERC
tumors are restricted to those tumors that are also HER2
negative (Fu et al. 2013).
As discussed above, the PIK3CA gene, encoding the
PI3K catalytic subunit p110a, is one of the most frequently
mutated genes in ERC breast cancers (Dawson et al. 2013).
Many of the mutations occur in ‘hot spots’ with the most
frequent mutations being E542K, E545K (both in the
helical domain), and H1047R (in the kinase domain)
(Barbareschi et al. 2007). Generally, the mutations result in
constitutive activation of the kinase (Di Cosimo & Baselga
2009). As mentioned above, the published data largely
suggest that mutations in PIK3CA occur more frequently
in ERC breast cancer with good prognosis and may also be
associated with better clinical outcome in patients treated
with endocrine therapy (Di Cosimo & Baselga 2009, Miller
et al. 2011a). However, this is not a universal finding
(Cuorvo et al. 2014). Recent reviews have discussed this
aspect in detail (Fu et al. 2013).
AKT1 mutations, often associated with PI3K-inde-
pendent constitutive activity, occur in w4% of breast
cancers and are often associated with ERC tumors.
However, the relationship of AKT expression and/or
activation to outcome in breast cancer is inconsistent
(Badve et al. 2010, Aleskandarany et al. 2011). Consi-
dering that the different AKT isoforms have distinct
functions (Dillon & Muller 2010) and that a recent study
using proximity ligation assay (PLA) to distinguish
between pAKT1 and pAKT2 (Spears et al. 2012)
determined the former to be associated with poor
prognosis and the latter with better prognosis, it seems
possible that the relative levels of each isoform may
determine the final read out. Furthermore, the inability
to distinguish the different pAKT isoforms may, at least in
part, underlie the previous lack of consistency (Badve
et al. 2010, Aleskandarany et al. 2011) around their
association with breast cancer outcome.
Published by Bioscientifica Ltd.

Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R361
Owing to the frequency with which components of the
PI3K/AKT/mTOR pathway are altered in ERC tumors, and
the fact that the pathway is a central hub receiving growth
and survival signals from many factors, the detailed
molecular nature of the pathway in different ERC tumors
may be important to guide appropriate therapy options.
Kinases associated with ER status byexpression analyses
Several studies have now been published in which different
kinase expression patterns were found in ERC vs other
clinical subtypes of breast cancer. Using publically available
RNA expression databases, Bianchini et al. (2010) identified
16 kinases that were overexpressed in ERC/HER2K breast
cancer biopsy samples. These were IGF1R, STK32B, ERBB4,
FGFR3, BMPR1B, MAST4, HSPB8, IKBKB, DCLK1, ERBB3,
STK39, MAP3K1, PTK6, PLK2, TEX14, and MST1. Kinases
uniquely overexpressed in ERK and HER2C breast cancer
subtypes were also identified. Two robust kinase clusters
were recognized: a mitosis metagene cluster (12 distinct
kinases) and an immune kinase cluster (15 distinct kinases),
which were present inall clinical subgroups. Overexpression
of kinases composing the mitosis metagene cluster was
mostly found in ERK tumors and was not prognostic in this
subgroup. However, ERC/HER2K tumors that presented a
high mitosis kinase score were associated with a worse
prognosis but showed a higher frequency of pathological
complete response (pCR)toneoadjuvantchemotherapy.On
the other hand, overexpression of kinases from the immune
kinase cluster was associated with better survival in
ERC/HER2K and HER2C subgroups. Interestingly, the
authors also observed that in ERC tumors, many of the
overexpressed kinases were transmembrane growth factor
receptors, while ERK tumors mostly overexpressed intra-
cellular kinases associated with cell proliferation (Bianchini
et al. 2010).
Finetti et al. (2008) undertook a genome-wide
expression analysis of a cohort of primary human breast
tumors focusing mainly on the basal and luminal A
intrinsic breast cancer subtypes. From this analysis, they
extracted kinase genes whose differential expression was
associated with a clinical outcome. Not unexpectedly,
there were substantial differences in the pattern of kinase
gene expression between the basal and the luminal
A intrinsic subtypes. Of more interest, however, was the
discovery that 16 kinases were overexpressed in most of
the basal group and in a few luminal A tumors. These
kinases were AURKA, AURKB, BUB1, BUB1B, CDC2 (CDK1),
CDC7, CHEK1, MASTL, MELK, NEK2, PBK, PLK1, PLK4,
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
SRPK1, TTK, and VRK1. Many of these kinases have been
previously reported to be involved in the G2 and M phases
of the cell cycle (Malumbres & Barbacid 2009, Knight et al.
2010). Notably, these kinases include the 12 kinases
making up the mitosis metagene cluster identified by
Bianchini et al. (2010). Similarly, Finetti et al. (2008) found
that overexpression of kinases from this 16-kinase
signature in luminal A (ERC) tumors was associated with
a poor clinical outcome. The association of mitosis and
proliferation signatures with poorer prognosis in the
luminal breast cancer subgroups is a consistent theme
(Ribelles et al. 2013).
Unique kinases associated with ER status in breast
cancer cell lines have also been reported (Michalides et al.
2002, Finetti et al. 2008, Midland et al. 2012), some of
which show overlap with studies in tumors (Finetti et al.
2008, Midland et al. 2012), therefore potentially providing
models of ERC breast cancer kinomes in vitro. These data
support the existence of distinct kinomes, not only
associated with ER status per se, but also further define
heterogeneity within ERC breast tumors.
Kinase overexpression associated withsensitivity to endocrine therapies
There are many different kinases that when either over-
expressed or underexpressed in ERC breast cancer cells
lead to altered cell growth and survival responses to both
SERMs such as estrogen and tamoxifen, and AIs. Many of
these are listed in Table 2.
Such data underscore the importance of kinase net-
works, as many of the kinases listed in Table 2 converge on
common hubs associated with cell growth, survival and
cell death. It is not surprising that the interaction of
multiple kinases with ER signaling is observed in breast
cancer, as many of these kinases are key components of
proliferation, survival and cell death pathways and would
be expected to be regulated by estrogen, through the ER,
which is the primary mitogenic/survival signal in the
majority of breast cancers, at least initially (Musgrove &
Sutherland 2009, Osborne & Schiff 2011).
In ERC breast cancer, gene signatures that are based on
proliferation often strongly correlate with Ki67 expression
(Gao et al. 2014), a well-known marker of proliferation.
Furthermore, in ERC breast tumors in particular, it is
Ki67 and not pCR that is the early correlative endpoint
for predicting efficacy of both hormonal therapy or
chemotherapy in ERC breast cancer (Yerushalmi et al.
2010, Dowsett et al. 2011, Ellis et al. 2011,
von Minckwitz et al. 2012, Gao et al. 2014). Recently, using
Published by Bioscientifica Ltd.

Table
2Kinasesexp
erimentallymanipulatedandshownto
influence
tamoxifen(Tam)oraromatase
inhibitor(A
I)sensitivity
Kinase
sGain
offu
nction
Loss
offu
nction
Refe
rence
sEffects
Clinicalco
rrelation
EGFR
Ectopic
ove
rexp
ression
Agthove
netal.(1992)
Tam-resistantgrowth
Yes(G
iltnaneetal.2007
HER2
Ectopic
ove
rexp
ression
Benzetal.(1992)
Tam-resistantgrowth
Yes(O
sborneetal.2003)
AKT
Ectopic
ove
rexp
ression
Campbelletal.(2001),
deGraffenriedetal.(2004)
andSilvaetal.(2007)
Tam-resistantgrowth
Yes(Perez-Te
norioetal.2002)
Akt3
Ectopic
ove
rexp
ression
Faridietal.(2003)
E2-independent,
Tam-stimulated
growth
asxe
nograft
Yes(N
akatanietal.1999)
ERK1/2
MAPK
Yes(G
eeetal.2001)
PKCa
Ectopic
ove
rexp
ression
Chisamore
etal.(2001)and
Frankeletal.(2007)
Tam-resistantgrowth
Yes(Kalstadetal.2010)
PKCd
Ectopic
ove
rexp
ression
Nabhaetal.(2005)
Tam-resistantgrowth
PKA
Ove
rexp
ressionbyreducing
exp
ressionofnegative
regulatory
subunit
PKA-RIalpha
Michalidesetal.(2004)
Tam-resistantgrowth
Yes(M
ichalidesetal.2004)
MKP3
Ectopic
ove
rexp
ression
Cuietal.(2006)
Tam-resistantgrowth
Yes(Cuietal.2006)
CDK10
siRNA
Iornsetal.(2008)
Tam-resistantgrowth
inhibition
Yes(Iornsetal.2008)
CRK7
siRNA
Iornsetal.(2009)
Tam-resistantgrowth
inhibition
No
IKK3
Ectopic
ove
rexp
ression
Guoetal.(2010)
Protectionagainst
Tam-inducedcell
death
No
SphK1
Ectopic
ove
rexp
ression
Sukoch
eva
etal.(2009)
Tam-resistantgrowth
inhibition
Yes(Ruckhaberleetal.2008)
c-ABL
siRNA
Zhaoetal.(2010)
Sensitize
scellsto
Tam
inhibition
Yes(Zhaoetal.2010)
Ronreceptortyrosine
kinase
(MST
1R)
Ectopic
ove
rexp
ression
McC
laineetal.(2010)
Tamoxifenresistance
No
EphA2receptortyrosine
kinase
(EPHA2)
Ectopic
ove
rexp
ression
Luetal.(2003b)
Tamoxifenresistance
Yes(Brantley-Sieders
etal.2011)
cRET
siRNA
Plaza
-Menach
oetal.(2010)
Increasedsensitivity
toTa
mYes(M
orandietal.2013)
HSP
B8
Ectopic
ove
rexp
ression
Gonza
lez-Malervaetal.(2011)
Tam
resistance
Yes(G
onza
lez-Malervaetal.
2011)
LMTK3
siRNA
Giamasetal.(2011)
Increasedsensitivity
toTa
mYes(G
iamasetal.2011)
IGF-R1
Ectopic
ove
rexp
ression
Zhangetal.(2011)
Tam
andfulvestrant
resistance
Yes(Foxetal.2011,W
inder
etal.2014)
FGFR
3Ectopic
ove
rexp
ression
Tomlinsonetal.(2012)
Tam
andfulvestrant
resistance
Yes(Tomlinsonetal.2012)
TBK1
Ectopic
ove
rexp
ression
Weietal.(2014)
Tam
resistance
Yes(W
eietal.2014)
Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R362
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
Published by Bioscientifica Ltd.

A/B
1
S46/47Y52
Y537S102 S118 S167 S236 T311S104 S212 S305
S559
S554
S282S154S106 Y219 S294
180 263 302 595
C D FE
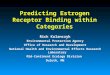
Figure 1
Known phosphorylation sites on estrogen receptor a. Sites identified by
stars are those that have been determined in ERaC breast cancer cases in
the Manitoba Breast Tumor Bank (MBTB) and are the basis of the P7-ERa
score. The black stars are those residues which when phosphorylated are
associatedwith a good clinical outcome in patients treated with tamoxifen.
The open/white stars are those residues which when phosphorylated are
Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R363
neoadjuvant antiestrogen therapy (particularly AIs), it
was observed that decreased detection of survival pathway
activation markers (e.g. phosphorylated AKT and phos-
phorylated mTOR) in tumors after treatment, compared
with pretreatment levels, was predictive of a better clinical
outcome (Generali et al. 2008, 2011), suggesting that
estrogen via the ER was regulating these pathways, directly
or indirectly in vivo. Many preclinical models have shown
that estrogen, via ER signaling, at least in part, regulates the
activities of PI3K/AKT/mTOR, p38MAPK, and MAPK/
ERK1/2 (Zhang et al. 2002, Lee et al. 2005, Yu & Henske
2006, Kazi et al. 2009, Maruani et al. 2012). This suggests that
the use of hormonal therapies in combination with the
most appropriately targeted kinase inhibitors may be more
beneficial at the onset of therapy than application in a
sequential fashion. Indeed, there are ongoing clinical trials
evaluating the use of combination therapies with endo-
crine therapies as first-line approaches (Ciruelos 2014).
A major challenge of using kinase inhibitors is that
kinase networks especially those associated with growth and
survival are often interconnected and inhibition of one may
have effects beyond the immediate targets. Adaptive
reprogramming of cancer kinomes due to single kinase
inhibitors has been demonstrated (Duncan et al. 2012) and
an argument for targeted combination therapy approaches
initially has been put forward (Stuhlmiller et al. 2014). The
development of resistance to hormonal therapies most
often occurs despite the continued expression of ERa
(Encarnacion et al. 1993, Bachleitner-Hofmann et al.
2002). In addition, many laboratory studies suggest that
adaptive responses of breast cancer cells, rather than
selection of existing ER-negative cells in the original
heterogeneous population, frequently occur (Santen et al.
2003, Browne et al. 2013). In such cases, increased
expression/activity of kinases also frequently occurs (Coutts
& Murphy 1998, Santen et al. 2003, 2004), supportive of the
concept that adaptive reprogramming of the breast cancer
kinome, in part, underlies some mechanisms of estrogen
independence and anti-estrogen resistance (Stuhlmiller
et al. 2014). The challenge will be to understand this and
its potential plasticity within the underlying heterogeneity
of ERC breast cancers and at the individual patient level.
associated with a poor clinical outcome in patients treated with tamoxifen
(Skliris et al. 2010a). It should be noted that others have determined that
S305 when phosphorylated is associated with a poor clinical outcome in
tamoxifen-treated patients (Le Romancer et al. 2011) and we have found
that tyrosine (Y) 537 when phosphorylated is also associated with a poor
clinical outcome in tamoxifen-treated patients (Skliris et al. 2010b). These
latter two results (textured stars) are consistent with our observation that
phosphorylation in N-terminal residues is associated with a good clinical
outcome, but phosphorylation in C-terminal residues is associated with a
poor clinical outcome.
Kinases known to phosphorylate ERa
In addition to ER signaling regulating kinase pathway
expression and/or activity, ER activity can also be
regulated by kinases.
ERa can be phosphorylated on many residues (Fig. 1)
and ERa has been identified as a substrate for several
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
kinases with known functions in breast cancer develop-
ment and progression. Dysregulation including mutation
and structural alterations of kinases themselves or the
signaling pathways in which they function is thought, in
part, to contribute to the dysregulation of ER signaling
that is associated with the development of breast cancer as
well as its progression to endocrine resistance in vivo.
Multiple aspects of ER activity can be affected by
phosphorylation; however, the focus of the majority of
studies addressing this issue has been on the transcrip-
tional activity (Le Romancer et al. 2011) and, not
surprisingly, it has been observed that differential phos-
phorylation of ERa (e.g. PKA activation) can alter the
chromatin-binding pattern (cistrome) of the receptor, in
turn altering the ERa transcriptome (de Leeuw et al. 2013).
The function of phosphorylation on ER activity and that
of other steroid hormone receptors have been recently
extensively reviewed (Le Romancer et al. 2011, Trevino &
Weigel 2013) and will not be reviewed herein.
Multiple different kinases can phosphorylate the same
ERa residue (e.g. serine amino acid residue 167 (S167) can
be phosphorylated by AKT, p70S6K, Aurora A, and
p90RSK) (Le Romancer et al. 2011). Similarly, one kinase
can phosphorylate several different residues on ERa
(e.g. MAPK can phosphorylate S104/106, S118, and S167)
(Le Romancer et al. 2011). Many kinases known to
phosphorylate ERa can also phosphorylate various
Published by Bioscientifica Ltd.

Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R364
coactivators and coregulators (Wu et al. 2005), impacting
ER (ESR1) transcriptional activity. This provides a
potential mechanism allowing the integration of multiple
pathways to regulate the biology and/or patho-biology of
ERa in the mammary gland. Support for this idea, at least
in breast cancer, is provided by the existence of a
phosphorylation code for ERa (Skliris et al. 2010a) and at
least one of its coactivators, SRC3/AIB1 (Wu et al. 2004,
York et al. 2010). As ERa can undergo several other types of
PTMs, e.g. acetylation, methylation, ubiquitylation, etc.
(Le Romancer et al. 2011), one can envisage a broader ERa
PTM or epigenetic-like code.
The identification of kinases phosphorylating ERa has
been achieved using multiple methods, alone or in
combination: in vitro studies using recombinant proteins,
mass spectroscopy, the use of selective small-molecular-
weight kinase activators or inhibitors, and overexpression
or knockdown of expression using cells in culture or as
xenografts. Furthermore, it is reasonable to assume, while
not proving, that if ER can be directly phosphorylated by a
kinase, the two proteins would directly bind under
appropriate circumstances. Table 3 lists a number of kinases
that have been found to undergo protein:protein
interactions with ERa using different methodologies,
e.g. co-immunoprecipitation (Wierer et al. 2013) and
other pull-down-type assays (Kanaujiya et al. 2013), PLA
(Poulard et al. 2012), yeast-2-hybrid assay (Paul et al. 2014),
Table 3 Kinases shown to interact directly with estrogen receptor
Kinases Assays
ERK1/2 CoIP; ChIP/reChIPp70S6K1 Co-IPGSK3 Co-IPCDK2 GST pull-down, in vitro kinase assIKKa Co-IP ChIP-reChIPCDK7 In vitro Co-IPAKT In vitro kinase assayPI3K Proximity ligation assay Co-IPpp90RSK1 In vitro kinase assays Co-IPPKA FRET in vitro kinase assayILK GST-down experiments Co-IPEGFR Co-IP in vitro kinase assayIGFR Co-IPDNA-PK Co-IPcAbl Co-IP in vitro kinase assayCK2 In vitro kinase assayIKK3 Co-IP in vitro kinase assayPAK1 In vitro kinase assay GST-pull-dow
experiments Co-IPc-SRC Proximity ligation assay Co-IP in v
kinase assayp38 MAPK Immunocomplex kinase assay in v
kinase assay shows no phosphoPLK1 Co-IP ChIP/reChIP
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
and fluorescence resonance energy transfer (FRET) (Zwart
et al. 2007a,b). Direct interaction of ERa with kinases can
occur in the cytoplasm (Poulard et al. 2012), at the plasma
membrane (Poulard et al. 2012), as well as in the nucleus on
chromatin (Madak-Erdogan et al. 2011, 2014, Wierer et al.
2013), with some methodologies, such as PLA, allowing the
determination of the subcellular localization of any
interactions that occur (Poulard et al. 2012).
There is no doubt that phosphorylation and other
PTMs (Wu et al. 2007, Le Romancer et al. 2011) are
important for the regulation of ER highlighted by the
existence of a phosphorylation code for ERa in human
breast tumors (Skliris et al. 2010a). However, it is still
unclear as to which kinases and phosphatases are involved
in regulating ERa in vivo. Correlations of expression and/or
activity of some kinases with ER or its phosphorylated
forms in human breast tumors have been reported,
supporting a possible role in vivo (Murphy et al. 2004,
Gee et al. 2005, Jiang et al. 2007, Shrivastav et al. 2014).
Many of the kinases that can directly phosphorylate
ERa and its coregulators can also be regulated by estrogen
signaling under some circumstances. Many such kinases are
components of key signaling pathways involved in
development/differentiation, proliferation, cell cycle,
motility/invasion, and cell death. Whether or not they are
regulated by estrogen or in turn regulate ERa may depend on
levels of expression of both substrate and kinase, and on
a
References
Madak-Erdogan et al. (2011)Becker et al. (2011)Medunjanin et al. (2005)
ay Rogatsky et al. (1999)Park et al. (2005)Chen et al. (2000)Campbell et al. (2001) and Sun et al. (2001)Sun et al. (2001) and Poulard et al. (2012)Joel et al. (1998)Chen et al. (1999), Zwart et al. (2007a,b)Acconcia et al. (2006)Marquez et al. (2001)Mendez et al. (2003)Medunjanin et al. (2010)He et al. (2010)Williams et al. (2009)Guo et al. (2010)
n Wang et al. (2002)
itro Arnold et al. (1995b, Poulard et al. (2012) andSun et al. (2012))
itrorylation
Lee & Bai (2002)
Wierer et al. (2013)
Published by Bioscientifica Ltd.

Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R365
mutations or structural alterations that may eliminate or
introduce new regulatory factors. The ability of the
estrogen/ERa complex to activate kinases that in turn
can phosphorylate ER and modify function provides a
powerful feed-forward amplification system that may
drive many human breast cancers. Understanding how
this occurs and how it can be perturbed to drive
progression to therapy resistance would provide funda-
mental information to inform early combination
approaches, for preventing and/or treating resistant tumors.
Interestingly, although in primary breast tumors, few
ERa mutations have been found, one known mutation
K303R changes the amino acid lysine that can be
acetylated (another type of PTM) to an arginine residue
that cannot be acetylated. This in turn alters regulation of
S305 phosphorylation on ERa, a site of ERa phosphory-
lation with established relevance in vivo and in AI
resistance (Herynk & Fuqua 2004, Barone et al. 2010).
There are also other examples of the co-regulation of
phosphorylation with other PTMs to regulate ERa
expression and/or activity. For example, c-Src can phos-
phorylate ERa at Y537 that in turn facilitates its
interaction with E3 ubiquitin ligases such as E6AP,
resulting in ubiquitin-dependent degradation of ERa
(Zhou & Slingerland 2014). Most recently, however,
frequent somatic mutations in ERa have been identified
in metastases from ERC breast cancer. This is more
frequently associated with metastases that occur during
or following endocrine therapy (Zhang et al. 1997,
Robinson et al. 2013, Jeselsohn et al. 2014, Segal & Dowsett
2014). The most frequent mutation identified was at Y537
or the residue beside it, D538; therefore, affecting directly
or indirectly a well-known phosphorylation site on ERa
(Arnold et al. 1995a, Nettles et al. 2008, Skliris et al. 2010b)
with known clinical relevance (Skliris et al. 2010b). Such
data underscore the importance of ERa phosphorylation
and other PTMs to breast cancer progression.
Our understanding of estrogen-regulated ERa signaling
in human breast cells comes from model systems that are all
cancer cells. Moreover, all ERC and ERK cell lines were
originally obtained from breast cancer metastases usually
pleural and ascitic effusions (Soule et al. 1973, Lippman
et al. 1976). We have little if any understanding of ERa
signaling in normal human breast epithelial cells, mainly
due to the lack of appropriate ERC models. This remains a
large gap in our understanding, potentially limiting the
development of more efficacious prevention strategies. This
is especially important as increased ERa expression in
normal human breast is associated with an increased cancer
risk (Khan et al. 2005) and elevated ERa expression is one of
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
the earliest alterations occurring in ‘precursors’ of breast
cancer (Shoker et al. 1999, Lee et al. 2006). ERa is highly
expressed in most atypical ductal hyperplasia (ADH), ductal
carcinoma in situ (DCIS), and invasive breast cancers
(Shoker et al. 1999, Allred et al. 2001). However, the
mechanisms leading to increased ERa expression during
tumorigenesis are poorly understood. Interestingly, beside
alterations in ER gene transcription (Muscat et al. 2013),
altered kinase expression affecting ERa protein stability has
been suggested (Henrich et al. 2003, Antoon et al. 2013)
and, therefore, highlights the potential link between
phosphorylation and estrogen signaling.
The challenge now is to identify those kinases and
their associated networks that phosphorylate and regulate
ERa function in ERC tumors and potentially normal
breast in vivo, as such information will identify the most
efficacious targeted treatment approaches upfront and
may inform better prevention approaches.
Conclusions
ERa regulates and is regulated by kinases involved in several
functions associated with the hallmarks of cancer (Hanahan
& Weinberg 2011). The presence of a phosphorylation code
for ERa in breast cancers associated with clinical outcome
(Skliris et al. 2010a) and the knowledge that there are also
other PTMs associated with ERa (Le Romancer et al. 2011)
in vivo suggest that there is an epigenetic-like code for ERa,
which can regulate and is in part regulated by distinct
kinomes. The literature reviewed above strongly suggests that
distinct kinomes exist for ER-positive and -negative breast
cancers. Even within ERC cancers, different subgroups exist,
defined by different kinome signatures, which can be
correlated with clinical outcome. Strong evidence supports
the interplay of kinase networks, suggesting that targeting a
single node may not be sufficient to inhibit the network.
Therefore, identifying the important hubs/nodes associated
with each clinically relevant kinome in ERC tumors could
offer the ability to implement the best therapy options at
diagnosis, either endocrine therapy alone or together with
other targeted therapies for an improved overall outcome.
Declaration of interest
The authors declare that there is no conflict of interest that could be
perceived as prejudicing the impartiality of the review.
Funding
This work was made possible through grant support to L C Murphy from the
Canadian Institutes of Health Research (CIHR), the Canadian Breast Cancer
Foundation (CBCF), and the Canadian Cancer Society Research Institute
Published by Bioscientifica Ltd.

Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R366
(CCSRI). M C Bruce is funded by a CBCF-Prairies/NWT region Postdoctoral
Fellowship. Morerover, some of published works referred to in this review
used breast tumor samples from theManitoba Breast Tumor Bank, a member
of the Canadian Tumor Repository Network, which are funded in part by the
CancerCare Manitoba Foundation (CCMF) and CIHR, respectively.
References
Acconcia F, Manavathi B, Mascarenhas J, Talukder AH, Mills G & Kumar R
2006 An inherent role of integrin-linked kinase-estrogen receptor a
interaction in cell migration. Cancer Research 66 11030–11038.
(doi:10.1158/0008-5472.CAN-06-2676)
van Agthoven T, van Agthoven TL, Portengen H, Foekens JA & Dorssers LC
1992 Ectopic expression of epidermal growth factor receptors induces
hormone independence in ZR-75-1 human breast cancer cells. Cancer
Research 52 5082–5088.
Aleskandarany MA, Rakha EA, Ahmed MA, Powe DG, Ellis IO & Green AR
2011 Clinicopathologic and molecular significance of phospho-Akt
expression in early invasive breast cancer. Breast Cancer Research and
Treatment 127 407–416. (doi:10.1007/s10549-010-1012-y)
Allred D, Mohsin S & Fuqua S 2001 Histological and biological evolution of
human premalignant breast disease. Endocrine-Related Cancer 8 47–61.
(doi:10.1677/erc.0.0080047)
Antoon JW, Martin EC,Lai R, SalvoVA,TangY, NitzchkeAM, Elliott S,Nam SY,
Xiong W, Rhodes LV et al. 2013 MEK5/ERK5 signaling suppresses estrogen
receptor expression and promotes hormone-independent tumorigenesis.
PLoS ONE 8 e69291. (doi:10.1371/journal.pone.0069291)
Arnold S, Vorojeikina D & Notides A 1995a Phosphorylation of tyrosine
537 on the human estrogen receptor is required for binding to an
estrogen response element. Journal of Biological Chemistry 270
30205–30212. (doi:10.1074/jbc.270.4.1850)
Arnold S, Obourn J, Jaffe H & Notides A 1995b Phosphorylation of the
human estrogen receptor on tyrosine 537 in vivo and by Src family
tyrosines in vitro. Molecular Endocrinology 9 24–33.
Bachleitner-Hofmann T, Pichler-Gebhard B, Rudas M, Gnant M, Taucher S,
Kandioler D, Janschek E, Dubsky P, Roka S, Sporn E et al. 2002 Pattern of
hormone receptor status of secondary contralateral breast cancers in patients
receiving adjuvant tamoxifen. Clinical Cancer Research 8 3427–3432.
Badve S, Collins NR, Bhat-Nakshatri P, Turbin D, Leung S, Thorat M, Dunn SE,
Geistlinger TR, Carroll JS, Brown M et al. 2010 Subcellular localization of
activated AKT in estrogen receptor- and progesterone receptor-expressing
breast cancers: potential clinical implications. American Journal of Path-
ology 176 2139–2149. (doi:10.2353/ajpath.2010.090477)
Balko JM, Mayer IA, Sanders ME, Miller TW, Kuba MG, Meszoely IM,
Wagle N, Garraway LA & Arteaga CL 2012 Discordant cellular response
to presurgical letrozole in bilateral synchronous ERC breast cancers
with a KRAS mutation or FGFR1 gene amplification. Molecular Cancer
Therapeutics 11 2301–2305. (doi:10.1158/1535-7163.MCT-12-0511)
Banerji S, Cibulskis K, Rangel-Escareno C, Brown KK, Carter SL, Frederick AM,
Lawrence MS, Sivachenko AY, Sougnez C, Zou L et al. 2012 Sequence
analysis of mutations and translocations across breast cancer subtypes.
Nature 486 405–409. (doi:10.1038/nature11154)
Barbareschi M, Buttitta F, Felicioni L, Cotrupi S, Barassi F, Del Grammastro M,
Ferro A, Dalla Palma P, Galligioni E & Marchetti A 2007 Different
prognostic roles of mutations in the helical and kinase domains of the
PIK3CA gene in breast carcinomas. Clinical Cancer Research 13
6064–6069. (doi:10.1158/1078-0432.CCR-07-0266)
Barone I, Iacopetta D, Covington KR, Cui Y, Tsimelzon A, Beyer A, Ando S &
Fuqua SA 2010 Phosphorylation of the mutant K303R estrogen
receptor a at serine 305 affects aromatase inhibitor sensitivity. Oncogene
29 2404–2414. (doi:10.1038/onc.2009.520)
Becker MA, Ibrahim YH, Cui X, Lee AV & Yee D 2011 The IGF pathway
regulates ERa through a S6K1-dependent mechanism in breast cancer
cells. Molecular Endocrinology 25 516–528. (doi:10.1210/me.2010-0373)
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
Benz CC, Scott GK, Sarup JC, Johnson RM, Tripathy D, Coronado E,
Shepard HM & Osborne CK 1992 Estrogen-dependent, tamoxifen-
resistant tumorigenic growth of MCF-7 cells transfected with HER2/neu.
BreastCancerResearchandTreatment2485–95. (doi:10.1007/BF01961241)
Bianchini G, Iwamoto T, Qi Y, Coutant C, Shiang CY, Wang B, Santarpia L,
Valero V, Hortobagyi GN, Symmans WF et al. 2010 Prognostic and
therapeutic implications of distinct kinase expression patterns in
different subtypes of breast cancer. Cancer Research 70 8852–8862.
(doi:10.1158/0008-5472.CAN-10-1039)
Brantley-Sieders DM, Jiang A, Sarma K, Badu-Nkansah A, Walter DL, Shyr Y
& Chen J 2011 Eph/ephrin profiling in human breast cancer reveals
significant associations between expression level and clinical outcome.
PLoS ONE 6 e24426. (doi:10.1371/journal.pone.0024426)
Browne BC, Hochgrafe F, Wu J, Millar EK, Barraclough J, Stone A, McCloy RA,
Lee CS, Roberts C, Ali NA et al. 2013 Global characterization of
signalling networks associated with tamoxifen resistance in breast
cancer. FEBS Journal 280 5237–5257. (doi:10.1111/febs.12441)
Campbell RA, Bhat-Nakshatri P, Patel NM, Constantinidou D, Ali S &
NakshatriH 2001Phosphatidylinositol3-kinase/AKT-mediatedactivation
of estrogen receptor a: a new model for anti-estrogen resistance. Journal of
Biological Chemistry 276 9817–9824. (doi:10.1074/jbc.M010840200)
Chen D, Pace P, Coombes R & Ali S 1999 Phosphorylation of human
estrogen receptor a by protein kinase A regulates dimerization.
Molecular and Cellular Biology 19 1002–1015.
Chen D, Washbrook E, Sarwar N, Pace P, Coombes R, Egly J & Ali S 2000
Activation of estrogen receptor a by S118 phosphorylation involves a
ligand-dependent interaction with TFIIH and participation of CDK7.
Molecular and Cellular Biology 6 127–137.
Chisamore MJ, Ahmed Y, Bentrem DJ, Jordan VC & Tonetti DA 2001 Novel
antitumor effect of estradiol in athymic mice injected with a T47D
breast cancer cell line overexpressing protein kinase Ca. Clinical Cancer
Research 7 3156–3165.
Ciruelos G 2014 Targeting the PI3K/AKT/mTOR pathway in estrogen
receptor-positive breast cancer. Cancer Treatment Reviews 40 862–871.
(doi:10.1016/j.ctrv.2014.03.004)
Coutts A & Murphy L 1998 Elevated mitogen activated protein kinase
activity in estrogen non-responsive human breast cancer cells. Cancer
Research 58 4071–4074.
Cui Y, Parra I, Zhang M, Hilsenbeck SG, Tsimelzon A, Furukawa T, Horii A,
Zhang ZY, Nicholson RI & Fuqua SA 2006 Elevated expression of
mitogen-activated protein kinase phosphatase 3 in breast tumors: a
mechanism of tamoxifen resistance. Cancer Research 66 5950–5959.
(doi:10.1158/0008-5472.CAN-05-3243)
Cuorvo LV,VerderioP,CiniselliCM,Girlando S, DecarliN,LeonardiE, FerroA,
Caldara A, Triolo R, Eccher C et al. 2014 PI3KCA mutation status is of
limited prognostic relevance in ER-positive breast cancer patients
treated with hormone therapy. Virchows Archiv: An International
Journal of Pathology 464 85–93. (doi:10.1007/s00428-013-1500-7)
Curtis C, Shah SP, Chin SF, Turashvili G, Rueda OM, Dunning MJ, Speed D,
Lynch AG, Samarajiwa S, Yuan Y et al. 2012 The genomic and
transcriptomic architecture of 2,000 breast tumours reveals novel
subgroups. Nature 486 346–352. (doi:10.1038/nature10983)
Dawson SJ, Rueda OM, Aparicio S & Caldas C 2013 A new genome-driven
integrated classification of breast cancer and its implications.
EMBO Journal 32 617–628. (doi:10.1038/emboj.2013.19)
Di Cosimo S & Baselga J 2009 Phosphoinositide 3-kinase mutations in
breast cancer: a “good” activating mutation? Clinical Cancer Research 15
5017–5019. (doi:10.1158/1078-0432.CCR-09-1173)
Dillon RL & Muller WJ 2010 Distinct biological roles for the akt family in
mammary tumor progression. Cancer Research 70 4260–4264.
(doi:10.1158/0008-5472.CAN-10-0266)
Dowsett M, Nielsen TO, A’Hern R, Bartlett J, Coombes RC, Cuzick J, Ellis M,
Henry NL, Hugh JC, Lively T et al. 2011 Assessment of Ki67 in breast
cancer: recommendations from the International Ki67 in Breast Cancer
working group. Journal of the National Cancer Institute 103 1656–1664.
(doi:10.1093/jnci/djr393)
Published by Bioscientifica Ltd.

Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R367
Duncan JS, Whittle MC, Nakamura K, Abell AN, Midland AA, Zawistowski JS,
Johnson NL, Granger DA, Jordan NV, Darr DB et al. 2012 Dynamic
reprogramming of the kinome in response to targeted MEK inhibition in
triple-negative breast cancer. Cell 149 307–321. (doi:10.1016/j.cell.
2012.02.053)
Ellis MJ, Suman VJ, Hoog J, Lin L, Snider J, Prat A, Parker JS, Luo J,
DeSchryver K, Allred DC et al. 2011 Randomized phase II neoadjuvant
comparison between letrozole, anastrozole, and exemestane for
postmenopausal women with estrogen receptor-rich stage 2 to 3 breast
cancer: clinical and biomarker outcomes and predictive value of the
baseline PAM50-based intrinsic subtype – ACOSOG Z1031. Journal of
Clinical Oncology 29 2342–2349. (doi:10.1200/JCO.2010.31.6950)
Ellis MJ, Ding L, Shen D, Luo J, Suman VJ, Wallis JW, Van Tine BA, Hoog J,
Goiffon RJ, Goldstein TC et al. 2012 Whole-genome analysis informs
breast cancer response to aromatase inhibition. Nature 486 353–360.
(doi:10.1038/nature11143)
Encarnacion CA, Ciocca DR, McGuire WL, Clark GM, Fuqua SA &
Osborne CK 1993 Measurement of steroid hormone receptors in breast
cancer patients on tamoxifen. Breast Cancer Research and Treatment 26
237–246. (doi:10.1007/BF00665801)
Faridi J, Wang L, Endemann G & Roth RA 2003 Expression of constitutively
active Akt-3 in MCF-7 breast cancer cells reverses the estrogen and
tamoxifen responsivity of these cells in vivo. Clinical Cancer Research 9
2933–2939.
Finetti P, Cervera N, Charafe-Jauffret E, Chabannon C, Charpin C,
Chaffanet M, Jacquemier J, Viens P, Birnbaum D & Bertucci F 2008
Sixteen-kinase gene expression identifies luminal breast cancers with
poor prognosis. Cancer Research 68 767–776. (doi:10.1158/0008-5472.
CAN-07-5516)
Fox EM, Miller TW, Balko JM, Kuba MG, Sanchez V, Smith RA, Liu S,
Gonzalez-Angulo AM, Mills GB, Ye F et al. 2011 A kinome-wide screen
identifies the insulin/IGF-I receptor pathway as a mechanism of escape
from hormone dependence in breast cancer. Cancer Research 71
6773–6784. (doi:10.1158/0008-5472.CAN-11-1295)
Frankel LB, Lykkesfeldt AE, Hansen JB & Stenvang J 2007 Protein kinase Ca
is a marker for antiestrogen resistance and is involved in the growth of
tamoxifen resistant human breast cancer cells. Breast Cancer Research
and Treatment 104 165–179. (doi:10.1007/s10549-006-9399-1)
Fu X, Osborne CK & Schiff R 2013 Biology and therapeutic potential of PI3K
signaling in ERC/HER2-negative breast cancer. Breast 22 (Suppl 2)
S12–S18. (doi:10.1016/j.breast.2013.08.001)
Gao Q, Patani N, Dunbier AK, Ghazoui Z, Zvelebil M, Martin LA & Dowsett M
2014 Effect of aromatase inhibition on functional gene modules in
oestrogen receptor positive breast cancer and their relationship with
antiproliferative response. Clinical Cancer Research 20 2485–2494.
(doi:10.1158/1078-0432.CCR-13-2602)
Gee J, Robertson J, Ellis I & Nicholson R 2001 Phosphorylation of ERK1/2
mitogen-activated protein kinase is associated with poor response to
anti-hormonal therapy and decreased patient survival in clinical breast
cancer. International Journal of Cancer 95 247–254. (doi:10.1002/
1097-0215(20010720)95:4!247::AID-IJC1042O3.0.CO;2-S)
Gee J, Robertson J, Gutteridge E, Ellis I, Pinder S, Rubini M & Nicholson R
2005 Epidermal growth factor receptor/HER2/insulin-like growth
factor receptor signalling and oestrogen receptor activity in clinical
breast cancer. Endocrine-Related Cancer 12 (Suppl 1) S99–S111.
(doi:10.1677/erc.1.01005)
Generali D, Fox SB, Brizzi MP, Allevi G, Bonardi S, Aguggini S, Milani M,
Bersiga A, Campo L, Dionisio R et al. 2008 Down-regulation of
phosphatidylinositol 3 0-kinase/AKT/molecular target of rapamycin
metabolic pathway by primary letrozole-based therapy in human breast
cancer. Clinical Cancer Research 14 2673–2680. (doi:10.1158/
1078-0432.CCR-07-1046)
Generali D, Symmans WF, Berruti A & Fox SB 2011 Predictive immuno-
histochemical biomarkers in the context of neoadjuvant therapy for
breast cancer. Journal of the National Cancer Institute. Monographs 2011
99–102. (doi:10.1093/jncimonographs/lgr030)
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
GiamasG,FilipovicA, Jacob J,MessierW,ZhangH,YangD,ZhangW,ShifaBA,
Photiou A, Tralau-Stewart C et al. 2011 Kinome screening for regulators of
theestrogenreceptor identifies LMTK3asanewtherapeutic target inbreast
cancer. Nature Medicine 17 715–719. (doi:10.1038/nm.2351)
Giltnane JM, Ryden L, Cregger M, Bendahl PO, Jirstrom K & Rimm DL 2007
Quantitative measurement of epidermal growth factor receptor is a
negative predictive factor for tamoxifen response in hormone receptor
positive premenopausal breast cancer. Journal of Clinical Oncology 25
3007–3014. (doi:10.1200/JCO.2006.08.9938)
Gonzalez-Malerva L, Park J, Zou L, Hu Y, Moradpour Z, Pearlberg J, Sawyer J,
Stevens H, Harlow E & LaBaer J 2011 High-throughput ectopic
expression screen for tamoxifen resistance identifies an atypical kinase
that blocks autophagy. PNAS 108 2058–2063. (doi:10.1073/pnas.
1018157108)
Goss PE, Ingle JN, Ales-Martinez JE, Cheung AM, Chlebowski RT,
Wactawski-Wende J, McTiernan A, Robbins J, Johnson KC, Martin LW
et al. 2011 Exemestane for breast-cancer prevention in postmenopausal
women. New England Journal of Medicine 364 2381–2391. (doi:10.1056/
NEJMoa1103507)
deGraffenried LA, Friedrichs WE, Russell DH, Donzis EJ, Middleton AK,
Silva JM, Roth RA & Hidalgo M 2004 Inhibition of mTOR activity
restores tamoxifen response in breast cancer cells with aberrant Akt
activity. Clinical Cancer Research 10 8059–8067. (doi:10.1158/1078-
0432.CCR-04-0035)
Guo JP, Shu SK, Esposito NN, Coppola D, Koomen JM & Cheng JQ 2010
IKKepsilon, phosphorylation of estrogen receptor a Ser-167 and
contribution to tamoxifen resistance in breast cancer. Journal of
Biological Chemistry 285 3676–3684. (doi:10.1074/jbc.M109.078212)
Han HS, Yu E, Song JY, Park JY, Jang SJ & Choi J 2009 The estrogen receptor a
pathway induces oncogenicWip1phosphatase geneexpression.Molecular
Cancer Research 7 713–723. (doi:10.1158/1541-7786.MCR-08-0247)
Hanahan D & Weinberg RA 2011 Hallmarks of cancer: the next generation.
Cell 144 646–674. (doi:10.1016/j.cell.2011.02.013)
He X, Zheng Z, Song T, Wei C, Ma H, Ma Q, Zhang Y, Xu Y, Shi W, Ye Q et al.
2010 c-Abl regulates estrogen receptor a transcription activity
through its stabilization by phosphorylation. Oncogene 29 2238–2251.
(doi:10.1038/onc.2009.513)
Henrich L, Smith J, Kitt D, Errington T, Nguyen B, Traish A & Lannigan D
2003 Extracellular signal-regulated kinase 7, a regulator of hormone-
dependent estrogen receptor destruction. Molecular and Cellular Biology
23 5979–5988. (doi:10.1128/MCB.23.17.5979-5988.2003)
Herynk M & Fuqua S 2004 Estrogen receptor mutations in human disease.
Endocrine Reviews 25 869–898. (doi:10.1210/er.2003-0010)
Holm C, Kok M, Michalides R, Fles R, Koornstra RH, Wesseling J,
Hauptmann M, Neefjes J, Peterse JL, Stal O et al. 2009 Phosphorylation
of the oestrogen receptor a at serine 305 and prediction of tamoxifen
resistance in breast cancer. Journal of Pathology 217 372–379.
(doi:10.1002/path.2455)
Horwitz KB, McGuire WL, Pearson OH & Segaloff A 1975 Predicting
response to endocrine therapy in human breast cancer: a hypothesis.
Science 189 726–727. (doi:10.1126/science.168640)
Ignatiadis M & Sotiriou C 2013 Luminal breast cancer: from biology to
treatment. Nature Reviews. Clinical Oncology 10 494–506. (doi:10.1038/
nrclinonc.2013.124)
Iorns E, Turner NC, Elliott R, Syed N, Garrone O, Gasco M, Tutt AN, Crook T,
Lord CJ & Ashworth A 2008 Identification of CDK10 as an important
determinant of resistance to endocrine therapy for breast cancer. Cancer
Cell 13 91–104. (doi:10.1016/j.ccr.2008.01.001)
Iorns E, Martens-de Kemp SR, Lord CJ & Ashworth A 2009 CRK7 modifies
the MAPK pathway and influences the response to endocrine therapy.
Carcinogenesis 30 1696–1701. (doi:10.1093/carcin/bgp187)
Jensen E & Jordan V 2003 The estrogen receptor: a model for molecular
medicine. Clinical Cancer Research 9 1980–1989.
Jensen E, Block G, Smith S, Kyser K & DeSombre E 1971 Estrogen receptors
and breast cancer response to adrenalectomy. Journal of the National
Cancer Institute. Monographs 34 55–70.
Published by Bioscientifica Ltd.

Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R368
Jeselsohn R, Yelensky R, Buchwalter G, Frampton G, Meric-Bernstam F,
Gonzalez-Angulo AM, Ferrer-Lozano J, Perez-Fidalgo JA, Cristofanilli M,
Gomez H et al. 2014 Emergence of constitutively active estrogen
receptor-a mutations in pretreated advanced estrogen receptor-positive
breast cancer. Clinical Cancer Research 20 1757–1767. (doi:10.1158/
1078-0432.CCR-13-2332)
Jiang J, Sarwar N, Peston D, Kulinskaya E, Shousha S, Coombes R & Ali S 2007
Phosphorylation of estrogen receptor-a at Ser167 is indicative of longer
disease-free and overall survival in breast cancer patients. Clinical Cancer
Research 13 5769–5776. (doi:10.1158/1078-0432.CCR-07-0822)
Joel PB, Smith J, Sturgill TW, Fisher TL, Blenis J & Lannigan DA 1998
pp90rsk1 regulates estrogen receptor-mediated transcription through
phosphorylation of Ser-167. Molecular and Cellular Biology 18 1978–1984.
Kalstad G, Cornmark L, Zahirovic I, Landberg G, Jirstrom K & Larsson C
2010 PKCa expression is a marker for breast cancer aggressiveness.
Molecular Cancer 9 76–90. (doi:10.1186/1476-4598-9-76)
Kanaujiya JK, Lochab S, Kapoor I, Pal P, Datta D, Bhatt ML, Sanyal S, Behre G
& Trivedi AK 2013 Proteomic identification of Profilin1 as a corepressor
of estrogen receptor a in MCF7 breast cancer cells. Proteomics 13
2100–2112. (doi:10.1002/pmic.201200534)
Kazi AA, Molitoris KH & Koos RD 2009 Estrogen rapidly activates the
PI3K/AKT pathway and hypoxia-inducible factor 1 and induces
vascular endothelial growth factor A expression in luminal epithelial
cells of the rat uterus. Biology of Reproduction 81 378–387. (doi:10.1095/
biolreprod.109.076117)
Khan SA, Bhandare D & Chatterton RT Jr 2005 The local hormonal
environment and related biomarkers in the normal breast. Endocrine-
Related Cancer 12 497–510. (doi:10.1677/erc.1.00732)
Knight Z, Lin H & Shokat K 2010 Targeting the cancer kinome through
polypharmacology. Nature Reviews. Cancer 10 130–137. (doi:10.1038/
nrc2787)
Kok M, Zwart W, Holm C, Fles R, Hauptmann M, Van’t Veer LJ, Wessels LF,
Neefjes J, Stal O, Linn SC et al. 2010 PKA-induced phosphorylation of
ERa at serine 305 and high PAK1 levels is associated with sensitivity to
tamoxifen in ER-positive breast cancer. Breast Cancer Research and
Treatment 125 1–12. (doi:10.1007/s10549-010-0798-y)
Lee H & Bai W 2002 Regulation of estrogen receptor nuclear export by ligand-
induced and p38-mediated receptor phosphorylation. Molecular and
Cellular Biology22 5835–5845. (doi:10.1128/MCB.22.16.5835-5845.2002)
Lee YR, Park J, Yu HN, Kim JS, Youn HJ & Jung SH 2005 Up-regulation of
PI3K/Akt signaling by 17b-estradiol through activation of estrogen
receptor-a, but not estrogen receptor-b, and stimulates cell growth in
breast cancer cells. Biochemical and Biophysical Research Communications
336 1221–1226. (doi:10.1016/j.bbrc.2005.08.256)
Lee S, Mohsin SK, Mao S, Hilsenbeck SG, Medina D & Allred DC 2006
Hormones, receptors, and growth in hyperplastic enlarged lobular
units: early potential precursors of breast cancer. Breast Cancer Research
8 R6. (doi:10.1186/bcr1367)
de Leeuw R, Flach K, Bentin Toaldo C, Alexi X, Canisius S, Neefjes J,
Michalides R & Zwart W 2013 PKA phosphorylation redirects ERa to
promoters of a unique gene set to induce tamoxifen resistance.
Oncogene 32 3543–3551. (doi:10.1038/onc.2012.361)
Le Romancer M, Poulard C, Cohen P, Sentis S, Renoir JM & Corbo L 2011
Cracking the estrogen receptor’s posttranslational code in breast
tumors. Endocrine Reviews 32 597–622. (doi:10.1210/er.2010-0016)
Lippman M, Bolan G & Huff K 1976 Effects of estrogens and antiestrogens
on hormone-responisve human breast cancer in long-term tissue
culture. Cancer Research 36 4595–4601.
Lu Q, Surks H, Ebling H, Baur W, Brown D, Pallas D & Karas R 2003a
Regulation of estrogen receptor a-mediated transcription by a direct
interaction with protein phosphatase 2A. Journal of Biological Chemistry
278 4639–4645. (doi:10.1074/jbc.M210949200)
Lu M, Miller KD, Gokmen-Polar Y, Jeng MH & Kinch MS 2003b EphA2
overexpression decreases estrogen dependence and tamoxifen
sensitivity. Cancer Research 63 3425–3429.
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
Madak-Erdogan Z, Lupien M, Stossi F, Brown M & Katzenellenbogen BS
2011 Genomic collaboration of estrogen receptor a and extracellular
signal-regulated kinase 2 in regulating gene and proliferation programs.
Molecular and Cellular Biology 31 226–236. (doi:10.1128/MCB.00821-10)
Madak-ErdoganZ,VentrellaR, PetryL &KatzenellenbogenBS2014Novel roles
for ERK5 and cofilin as critical mediators linking ERa-driven transcription,
actin reorganization and invasiveness in breast cancer. Molecular Cancer
Research 12 714–727. (doi:10.1158/1541-7786.MCR-13-0588)
Malumbres M & Barbacid M 2009 Cell cycle, CDKs and cancer: a changing
paradigm. Nature Reviews. Cancer 9 153–166. (doi:10.1038/nrc2602)
Marquez DC, Lee J, Lin T & Pietras RJ 2001 Epidermal growth factor
receptor and tyrosine phosphorylation of estrogen receptor. Endocrine
16 73–81. (doi:10.1385/ENDO:16:2:073)
Maruani DM, Spiegel TN, Harris EN, Shachter AS, Unger HA, Herrero-
Gonzalez S & Holz MK 2012 Estrogenic regulation of S6K1 expression
creates a positive regulatory loop in control of breast cancer cell
proliferation. Oncogene 31 5073–5080. (doi:10.1038/onc.2011.657)
Mazumdar A & Kumar R 2003 Estrogen regulation of Pak1 and FKHR
pathways in breast cancer cells. FEBS Letters 535 6–10. (doi:10.1016/
S0014-5793(02)03846-2)
McClaine RJ, Marshall AM, Wagh PK & Waltz SE 2010 Ron receptor
tyrosine kinase activation confers resistance to tamoxifen in breast
cancer cell lines. Neoplasia 12 650–658.
Medunjanin S, Hermani A, Servi BD, Grisouard J, Rincke G & Mayer D 2005
Glycogen synthase kinase-3 interacts with and phosphorylates estrogen
receptor a and is involved in the regulation of receptor activity. Journal of
Biological Chemistry 280 33006–33014. (doi:10.1074/jbc.M506758200)
Medunjanin S, Weinert S, Schmeisser A, Mayer D & Braun-Dullaeus RC
2010 Interaction of the double-strand break repair kinase DNA-PK
and estrogen receptor-a. Molecular Biology of the Cell 21 1620–1628.
(doi:10.1091/mbc.E09-08-0724)
Mendez P, Azcoitia I & Garcia-Segura LM 2003 Estrogen receptor a forms
estrogen-dependent multimolecular complexes with insulin-like
growth factor receptor and phosphatidylinositol 3-kinase in the adult
rat brain. Brain Research. Molecular Brain Research 112 170–176.
Michalides R, van Tinteren H, Balkenende A, Vermorken JB, Benraadt J,
Huldij J & van Diest P 2002 Cyclin A is a prognostic indicator in early
stage breast cancer with and without tamoxifen treatment. British
Journal of Cancer 86 402–408. (doi:10.1038/sj.bjc.6600072)
Michalides R, Griekspoor A, Balkenende A, Verwoerd D, Janssen L, Jalink K,
Floore A, Velds A, van’t Veer L & Neefjes J 2004 Tamoxifen resistance by
a conformational arrest of the estrogen receptor a after PKA activation
in breast cancer. Cancer Cell 5 597–605. (doi:10.1016/j.ccr.2004.05.016)
Midland AA, Whittle MC, Duncan JS, Abell AN, Nakamura K, Zawistowski JS,
Carey LA, Earp HS III, Graves LM, Gomez SM et al. 2012 Defining
the expressed breast cancer kinome. Cell Research 22 620–623.
(doi:10.1038/cr.2012.25)
Miller TW, Hennessy BT, Gonzalez-Angulo AM, Fox EM, Mills GB, Chen H,
Higham C, Garcia-Echeverria C, Shyr Y & Arteaga CL 2010 Hyperacti-
vation of phosphatidylinositol-3 kinase promotes escape from hormone
dependence in estrogen receptor-positive human breast cancer.
Journal of Clinical Investigation 120 2406–2413. (doi:10.1172/JCI41680)
Miller TW, Balko JM & Arteaga CL 2011a Phosphatidylinositol 3-kinase and
antiestrogen resistance in breast cancer. Journal of Clinical Oncology 29
4452–4461. (doi:10.1200/JCO.2010.34.4879)
Miller TW, Rexer BN, Garrett JT & Arteaga CL 2011b Mutations in the
phosphatidylinositol 3-kinase pathway: role in tumor progression and
therapeutic implications in breast cancer. Breast Cancer Research 13 224.
(doi:10.1186/bcr3039)
von Minckwitz G, Untch M, Blohmer JU, Costa SD, Eidtmann H, Fasching PA,
Gerber B, Eiermann W, Hilfrich J, Huober J et al. 2012 Definition and
impact of pathologic complete response on prognosis after neoadjuvant
chemotherapy in various intrinsic breast cancer subtypes. Journal of
Clinical Oncology 30 1796–1804. (doi:10.1200/JCO.2011.38.8595)
Morandi A, Martin LA, Gao Q, Pancholi S, Mackay A, Robertson D, Zvelebil M,
Dowsett M, Plaza-Menacho I & Isacke CM 2013 GDNF-RET signaling in
Published by Bioscientifica Ltd.

Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R369
ER-positive breast cancers is a key determinant of response and
resistance to aromatase inhibitors. Cancer Research 73 3783–3795.
(doi:10.1158/0008-5472.CAN-12-4265)
Murphy LC, Cherlet T, Adeyinka A, Niu Y, Snell L & Watson P 2004
Phospho-serine-118 estrogen receptor-a detection in human breast
tumors in vivo. Clinical Cancer Research 10 1354–1359. (doi:10.1158/
1078-0432.CCR-03-0112)
Murphy LC, Seekallu SV & Watson PH 2011 Clinical significance of
estrogen receptor phosphorylation. Endocrine-Related Cancer 18
R1–R14. (doi:10.1677/ERC-10-0070)
Muscat GE, Eriksson NA, Byth K, Loi S, Graham D, Jindal S, Davis MJ, Clyne C,
Funder JW, Simpson ER et al. 2013 Research resource: nuclear receptors as
transcriptome: discriminant and prognostic value in breast cancer.
Molecular Endocrinology 27 350–365. (doi:10.1210/me.2012-1265)
Musgrove EA & Sutherland RL 2009 Biological determinants of endocrine
resistance in breast cancer. Nature Reviews. Cancer 9 631–643.
(doi:10.1038/nrc2713)
Nabha SM, Glaros S, Hong M, Lykkesfeldt AE, Schiff R, Osborne K & Reddy KB
2005 Upregulation of PKC-delta contributes to antiestrogen resistance
in mammary tumor cells. Oncogene 24 3166–3176. (doi:10.1038/sj.onc.
1208502)
Nakatani K, Thompson DA, Barthel A, Sakaue H, Liu W, Weigel RJ & Roth RA
1999 Up-regulation of Akt3 in estrogen receptor-deficient breast
cancers and androgen-independent prostate cancer lines. Journal of
Biological Chemistry 274 21528–21532. (doi:10.1074/jbc.274.31.21528)
Nettles KW, Bruning JB, Gil G, Nowak J, Sharma SK, Hahm JB, Kulp K,
Hochberg RB, Zhou H, Katzenellenbogen JA et al. 2008 NFkB selectivity of
estrogen receptor ligands revealed by comparative crystallographic
analyses. Nature Chemical Biology 4 241–247. (doi:10.1038/nchembio.76)
Osborne CK & Schiff R 2011 Mechanisms of endocrine resistance in breast
cancer. Annual Review of Medicine 62 233–247. (doi:10.1146/annurev-
med-070909-182917)
Osborne C, Bardou V, Hopp T, Chamness G, Hilsenbeck S, Fuqua S, Wong J,
Allred D, Clark G & Schiff R 2003 Role of the estrogen receptor
coactivator AIB1 (SRC-3) and HER-2/neu in tamoxifen resistance in
breast cancer. Journal of the National Cancer Institute 95 353–361.
(doi:10.1093/jnci/95.5.353)
Park K, Krishnan V, O’Malley B, Yamamoto Y & Gaynor R 2005 Formation
of an IKKa-dependent transcription complex is required for estrogen
receptor-mediated gene activation. Molecular Cell 18 71–82.
(doi:10.1016/j.molcel.2005.03.006)
Paul A, Garcia YA, Zierer B, Patwardhan C, Gutierrez O, Hildenbrand Z,
Harris DC, Balsiger HA, Sivils JC, Johnson JL et al. 2014 The
cochaperone SGTA (small glutamine-rich tetratricopeptide repeat-
containing protein a) demonstrates regulatory specificity for the
androgen, glucocorticoid and progesterone receptors. Journal of
Biological Chemistry 289 15297–15308. (doi:10.1074/jbc.M113.535229)
Perez-Tenorio G, Stal O & Group MotSSBC 2002 Activation of AKT/PKB in
breast cancer predicts a worse outcome among endocrine treated patients.
British Journal of Cancer 86 540–545. (doi:10.1038/sj.bjc.6600126)
Perou CM, Sorlie T, Eisen MB, van de Rijn M, Jeffrey SS, Rees CA, Pollack JR,
Ross DT, Johnsen H, Akslen LA et al. 2000 Molecular portraits of human
breast tumors. Nature 406 747–752. (doi:10.1038/35021093)
Pham TT, Angus SP & Johnson GL 2013 MAP3K1: genomic alterations in
cancer and function in promoting cell survival or apoptosis. Genes &
Cancer 4 419–426. (doi:10.1177/1947601913513950)
Plaza-Menacho I, Morandi A, Robertson D, Pancholi S, Drury S, Dowsett M,
Martin LA & Isacke CM 2010 Targeting the receptor tyrosine kinase RET
sensitizes breast cancer cells to tamoxifen treatment and reveals a role
for RET in endocrine resistance. Oncogene 29 4648–4657. (doi:10.1038/
onc.2010.209)
Poulard C, Treilleux I, Lavergne E, Bouchekioua-Bouzaghou K, Goddard-
Leon S, Chabaud S, Tredan O, Corbo L & Le Romancer M 2012 Activation
of rapid oestrogen signalling in aggressive human breast cancers. EMBO
Molecular Medicine 4 1200–1213. (doi:10.1002/emmm.201201615)
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
Proia DA, Nannenga BW, Donehower LA & Weigel NL 2006 Dual roles for the
phosphatase PPM1D in regulating progesterone receptor function.
Journal of Biological Chemistry 281 7089–7101. (doi:10.1074/jbc.
M511839200)
Ribelles N, Perez-Villa L, Jerez JM, Pajares B, Vicioso L, Jimenez B, de Luque V,
Franco L, Gallego E, Marquez A et al. 2013 Pattern of recurrence of early
breast cancer is different according to intrinsic subtype and proliferation
index. Breast Cancer Research 15 R98. (doi:10.1186/bcr3559)
Robinson DR, Wu YM, Vats P, Su F, Lonigro RJ, Cao X, Kalyana-Sundaram S,
Wang R, Ning Y, Hodges L et al. 2013 Activating ESR1 mutations in
hormone-resistant metastatic breast cancer. Nature Genetics 45
1446–1451. (doi:10.1038/ng.2823)
Rogatsky I, Trowbridge J & Garabedian M 1999 Potentiation of human
estrogen receptor a transcriptional activation through phosphorylation
of serines 104 and 106 by the cyclin A–CDK2 complex. Journal of
Biological Chemistry 274 22296–22302. (doi:10.1074/jbc.274.32.22296)
Rowan B, Weigel N & O’Malley B 2000 Phosphorylation of steroid
receptor coactivator-1. Journal of Biological Chemistry 275 4475–4483.
(doi:10.1074/jbc.275.6.4475)
Ruckhaberle E, Rody A, Engels K, Gaetje R, von Minckwitz G, Schiffmann S,
Grosch S, Geisslinger G, Holtrich U, Karn T et al. 2008 Microarray
analysis of altered sphingolipid metabolism reveals prognostic signi-
ficance of sphingosine kinase 1 in breast cancer. Breast Cancer Research
and Treatment 112 41–52. (doi:10.1007/s10549-007-9836-9)
Santen RJ, Song RX, Zhang Z, Kumar R, Jeng MH, Masamura S, Yue W &
Berstein L 2003 Adaptive hypersensitivity to estrogen: mechanism for
superiority of aromatase inhibitors over selective estrogen receptor
modulators for breast cancer treatment and prevention. Endocrine-
Related Cancer 10 111–130. (doi:10.1677/erc.0.0100111)
Santen R, Song R, Zhang Z, Yue W & Kumar R 2004 Adaptive
hypersensitivity to estrogen: mechanism for sequential responses to
hormonal therapy in breast cancer. Clinical Cancer Research 10
337S–345S. (doi:10.1158/1078-0432.CCR-031207)
Segal CV & Dowsett M 2014 Estrogen receptor mutations in breast cancer-
new focus on an old target. Clinical Cancer Research 20 1724–1726.
(doi:10.1158/1078-0432.CCR-14-0067)
Shah SP, Roth A, Goya R, Oloumi A, Ha G, Zhao Y, Turashvili G, Ding J, Tse K,
Haffari G et al. 2012 The clonal and mutational evolution spectrum of
primary triple-negative breast cancers. Nature 486 395–399.
(doi:10.1038/nature10933)
Shoker BS, Jarvis C, Sibson DR, Walker C & Sloane JP 1999 Oestrogen
receptor expression in the normal and pre-cancerous breast. Journal of
Pathology 188 237–244. (doi:10.1002/(SICI)1096-9896(199907)188:3
!237::AID-PATH343O3.0.CO;2-8)
Shrivastav A, Bruce M, Jaksic D, Bader T, Seekallu S, Penner C, Nugent Z,
Watson P & Murphy L 2014 The mechanistic target for rapamycin is
related to the phosphorylation score for estrogen receptor a in human
breast tumors, in vivo. Breast Cancer Research 16 R49. (doi:10.1186/
bcr3660)
Silva J, Cavazos DA, Donzis E, Friedrichs WE, Marciniak R &
deGraffenried LA 2007 Akt-induced tamoxifen resistance is associated
with altered FKHR regulation. Cancer Investigation 25 569–573.
(doi:10.1080/07357900701513538)
Skliris GP, Nugent ZJ, Rowan BG, Penner CR, Watson PH & Murphy LC
2010a A phosphorylation code for oestrogen receptor-a predicts
clinical outcome to endocrine therapy in breast cancer. Endocrine-
Related Cancer 17 589–597. (doi:10.1677/ERC-10-0030)
Skliris GP, Nugent ZJ, Watson PH & Murphy LC 2010b Estrogen receptor a
phosphorylated at tyrosine 537 is associated with poor clinical
outcome in breast cancer patients treated with tamoxifen. Hormones &
Cancer 1 215–221. (doi:10.1007/s12672-010-0049-z)
Sorlie T, Tibshirani R, Parker J, Hastie T, Marron J, Nobel A, Deng S, Johnsen H,
Pesich R, Geisler S et al. 2003 Repeated observation of breast tumor
subtypes in independent gene expression data sets. PNAS 100
8418–8423. (doi:10.1073/pnas.0932692100)
Published by Bioscientifica Ltd.

Endocrine-RelatedCancer
Review M C Bruce et al. Kinome associated withER-positive status
21 :5 R370
Soule HD, Vazguez J, Long A, Albert S & Brennan M 1973 A human cell line
from a pleural effusion derived from a breast carcinoma. Journal of the
National Cancer Institute 51 1409–1416.
SpearsM,CunninghamCA,TaylorKJ,MallonEA,Thomas JS,KerrGR, JackWJ,
Kunkler IH, Cameron DA, Chetty U et al. 2012 Proximity ligation assays
for isoform-specific Akt activation in breast cancer identify activated
Akt1 as a driver of progression. Journal of Pathology 227 481–489.
(doi:10.1002/path.4022)
Stephens PJ, Tarpey PS, Davies H, Van Loo P, Greenman C, Wedge DC,
Nik-Zainal S, Martin S, Varela I, Bignell GR et al. 2012 The landscape of
cancer genes and mutational processes in breast cancer. Nature 486
400–404. (doi:10.1038/nature11017)
Stuhlmiller TJ, Earp HS & Johnson GL 2014 Adaptive reprogramming of the
breast cancer kinome. Clinical Pharmacology and Therapeutics 95
413–415. (doi:10.1038/clpt.2014.8)
Sukocheva O, Wang L, Verrier E, Vadas MA & Xia P 2009 Restoring
endocrine response in breast cancer cells by inhibition of the
sphingosine kinase-1 signaling pathway. Endocrinology 150 4484–4492.
(doi:10.1210/en.2009-0391)
Sun M, Paciga J, Feldman R, Yuan Z, Coppola D, Lu Y, Shelley S, Nicosia S &
Cheng J 2001 Phosphatidylinositol-3-OH kinase (PI3K)/AKT2, activated
in breast cancer, regulates and is induced by estrogen receptor a (ERa)
via interaction between ERa and PI3K. Cancer Research 61 5985–5991.
Sun J, Zhou W, Kaliappan K, Nawaz Z & Slingerland JM 2012 ERa
phosphorylation at Y537 by src triggers E6-AP-ERa binding, ERa
ubiquitylation, promoter occupancy, and target gene expression.
Molecular Endocrinology 26 1567–1577. (doi:10.1210/me.2012-1140)
TengDH, Perry WL III, HoganJK, Baumgard M,Bell R, Berry S, Davis T, FrankD,
FryeC,HattierT etal.1997Humanmitogen-activatedproteinkinasekinase
4 as a candidate tumor suppressor. Cancer Research 57 4177–4182.
Tomlinson DC, Knowles MA & Speirs V 2012 Mechanisms of FGFR3 actions
in endocrine resistant breast cancer. International Journal of Cancer 130
2857–2866. (doi:10.1002/ijc.26304)
Trevino LS & Weigel NL 2013 Phosphorylation: a fundamental regulator of
steroid receptor action. Trends in Endocrinology and Metabolism 24
515–524. (doi:10.1016/j.tem.2013.05.008)
Turner N, Pearson A, Sharpe R, Lambros M, Geyer F, Lopez-Garcia MA,
Natrajan R, Marchio C, Iorns E, Mackay A et al. 2010 FGFR1
amplification drives endocrine therapy resistance and is a therapeutic
target in breast cancer. Cancer Research 70 2085–2094. (doi:10.1158/
0008-5472.CAN-09-3746)
Wang RA, Mazumdar A, Vadlamudi RK & Kumar R 2002 P21-activated
kinase-1 phosphorylates and transactivates estrogen receptor-a and
promotes hyperplasia in mammary epithelium. EMBO Journal 21
5437–5447. (doi:10.1093/emboj/cdf543)
Wei C, Cao Y, Yang X, Zheng Z, Guan K, Wang Q, Tai Y, Zhang Y, Ma S, Ge X
et al. 2014 Elevated expression of TANK-binding kinase 1 enhances
tamoxifen resistance in breast cancer. PNAS 111 E601–E610. (doi:10.
1073/pnas.1316255111)
Wierer M, Verde G, Pisano P, Molina H, Font-Mateu J, Di Croce L & Beato M
2013 PLK1 signaling in breast cancer cells cooperates with estrogen
receptor-dependent gene transcription. Cell Reports 3 2021–2032.
(doi:10.1016/j.celrep.2013.05.024)
Williams CC, Basu A, El-Gharbawy A, Carrier LM, Smith CL & Rowan BG
2009 Identification of four novel phosphorylation sites in estrogen
receptor a: impact on receptor-dependent gene expression and
phosphorylation by protein kinase CK2. BMC Biochemistry 10 36.
(doi:10.1186/1471-2091-10-36)
Winder T, Giamas G, Wilson PM, Zhang W, Yang D, Bohanes P, Ning Y,
Gerger A, Stebbing J & Lenz HJ 2014 Insulin-like growth factor receptor
http://erc.endocrinology-journals.org q 2014 Society for EndocrinologyDOI: 10.1530/ERC-14-0232 Printed in Great Britain
polymorphism defines clinical outcome in estrogen receptor-positive
breast cancer patients treated with tamoxifen. Pharmacogenomics
Journal 14 28–34. (doi:10.1038/tpj.2013.8)
Wu RC, Qin J, Yi P, Wong J, Tsai SY, Tsai MJ & O’Malley BW 2004 Selective
phosphorylations of the SRC-3/AIB1 coactivator integrate genomic
reponses to multiple cellular signaling pathways. Molecular Cell 15
937–949. (doi:10.1016/j.molcel.2004.08.019)
Wu RC, Smith CL & O’Malley BW 2005 Transcriptional regulation by
steroid receptor coactivator phosphorylation. Endocrine Reviews 26
393–399. (doi:10.1210/er.2004-0018)
Wu RC, Feng Q, Lonard DM & O’Malley BW 2007 SRC-3 coactivator
functional lifetime is regulated by a phospho-dependent ubiquitin time
clock. Cell 129 1125–1140. (doi:10.1016/j.cell.2007.04.039)
Yamnik RL & Holz MK 2010 mTOR/S6K1 and MAPK/RSK signaling pathways
coordinately regulate estrogen receptor a serine 167 phosphorylation.
FEBS Letters 584 124–128. (doi:10.1016/j.febslet.2009.11.041)
Yamnik RL, Digilova A, Davis DC, Brodt ZN, Murphy CJ & Holz MK 2009 S6
kinase 1 regulates estrogen receptor a in control of breast cancer cell
proliferation. Journal of Biological Chemistry 284 6361–6369.
(doi:10.1074/jbc.M807532200)
Yerushalmi R, Woods R, Ravdin PM, Hayes MM & Gelmon KA 2010 Ki67 in
breast cancer: prognostic and predictive potential. Lancet Oncology 11
174–183. (doi:10.1016/S1470-2045(09)70262-1)
York B, Yu C, Sagen JV, Liu Z, Nikolai BC, Wu RC, Finegold M, Xu J &
O’Malley BW 2010 Reprogramming the posttranslational code of SRC-3
confers a switch in mammalian systems biology. PNAS 107
11122–11127. (doi:10.1073/pnas.1005262107)
Yu J & Henske EP 2006 Estrogen-induced activation of mammalian target
of rapamycin is mediated via tuberin and the small GTPase Ras
homologue enriched in brain. Cancer Research 66 9461–9466.
(doi:10.1158/0008-5472.CAN-06-1895)
Zhang Q-X, Borg A, Wolf D, Oesterreich S & Fuqua S 1997 An estrogen
receptor mutant with strong hormone independent activity from a
metastatic breast cancer. Cancer Research 57 1244–1249.
Zhang Z, Maier B, Santen RJ & Song RX 2002 Membrane association of
estrogen receptor a mediates estrogen effect on MAPK activation.
Biochemical and Biophysical Research Communications 294 926–933.
(doi:10.1016/S0006-291X(02)00348-0)
Zhang Y, Moerkens M, Ramaiahgari S, de Bont H, Price L, Meerman J &
van de Water B2011Elevated insulin-likegrowth factor1 receptor signaling
induces antiestrogen resistance through the MAPK/ERK and PI3K/Akt
signaling routes. Breast Cancer Research 13 R52. (doi:10.1186/bcr2883)
Zhang F, Wang Y, Wang L, Luo X, Huang K, Wang C, Du M, Liu F, Luo T &
Huang D 2013 Poly(ADP-ribose) polymerase 1 is a key regulator of
estrogen receptor a-dependent gene transcription. Journal of Biological
Chemistry 288 11348–11357. (doi:10.1074/jbc.M112.429134)
Zhao H, Ou-Yang F, Chen IF, Hou MF, Yuan SS, Chang HL, Lee YC, Plattner R,
Waltz SE, Ho SM et al. 2010 Enhanced resistance to tamoxifen by the
c-ABL proto-oncogene in breast cancer. Neoplasia 12 214–223.
Zhou W & Slingerland JM 2014 Links between oestrogen receptor
activation and proteolysis: relevance to hormone-regulated cancer
therapy. Nature Reviews. Cancer 14 26–38. (doi:10.1038/nrc3622)
Zwart W, Griekspoor A, Berno V, Lakeman K, Jalink K, Mancini M, Neefjes J
& Michalides R 2007a PKA-induced resistance to tamoxifen is
associated with an altered orientation of ERa towards co-activator
SRC-1. EMBO Journal 26 3534–3544. (doi:10.1038/sj.emboj.7601791)
Zwart W, Griekspoor A, Rondaij M, Verwoerd D, Neefjes J & Michalides R
2007b Classification of anti-estrogens according to intramolecular FRET
effects on phospho-mutants of estrogen receptor a. Molecular Cancer
Therapeutics 6 1526–1533. (doi:10.1158/1535-7163.MCT-06-0750)
Received in final form 9 July 2014Accepted 23 July 2014Made available online as an Accepted Preprint23 July 2014
Published by Bioscientifica Ltd.



![Study of Estrogen Receptor, Progesterone Receptor, …...[CANCER RESEARCH 49,4298-4304, August 1. 1989] Study of Estrogen Receptor, Progesterone Receptor, and the Estrogen-regulated](https://img.pdfslide.us/doc/110x75/5f95792bbdbd5e0915333803/study-of-estrogen-receptor-progesterone-receptor-cancer-research-494298-4304.jpg)