Embed Size (px)
Citation preview
The Influence of Type 2 Diabetes on Cardiovascular
Disease and Glycemic Treatment Options
Rocky Mountain/ACPInternal Medicine Conference
Banff, ABNovember 22, 2012
David C.W. Lau, MD, PhD, FRCPCDepts. of Medicine, Biochem. & Molec. Biol.
Julia McFarlane Diabetes Research CentreUniversity of [email protected]
Program Faculty
• Dr. Ronald Goldenberg, MD, FRCPC, FACEConsultant Endocrinologist, North York General Hospitaland LMC Endocrinology Centers, Thornhill, Ontario
• Dr. Mansoor Husain MD, FRCPCDirector, Toronto General Hospital Research Institute and Heart and Stroke Richard Lewar Centre for ExcellenceSenior Scientist, Division of Experimental TherapeuticsProfessor of Medicine, University of Toronto
• Dr. David C. W. Lau MD, PhD, FRCPCProfessor of Medicine, Biochemistry and Molecular BiologyJulia McFarlane Diabetes Research CentreUniversity of Calgary
Disclosures: David C. W. Lau
Research funding:
• AHFMR, Alberta Cancer Board, CIHR, AstraZeneca, Boehringer-Ingelheim, BMS, Dainippon, Eli Lilly, Novo Nordisk, Pfizer and sanofi
Consultant or advisory board member:
• Abbott, Allergan, Amgen, AstraZeneca, Bayer, Boehringer-Ingelheim, BMS, Eli Lilly, Merck, Novartis, Novo Nordisk, Pfizer, Roche, sanofi
Speaker bureau:
• CDA, HSFC, AstraZeneca, Abbott, Bayer, Boehringer-Ingelheim, BMS, Eli Lilly, Merck, Novo Nordisk, sanofi
Some slides are selected from accredited CHE programs sponsored by Novo Nordisk and AstraZeneca/BMS
Objectives
At the end of the presentation, the participant will be able to:• Understand the cardiovascular burden in diabetes• Review the mechanisms of actions of incretin-
based therapies for diabetes • Compare the cardiovascular effects of incretins and
other glucose-lowering agents• Review current and ongoing data on incretin-based
therapies and cardiovascular disease outcomes
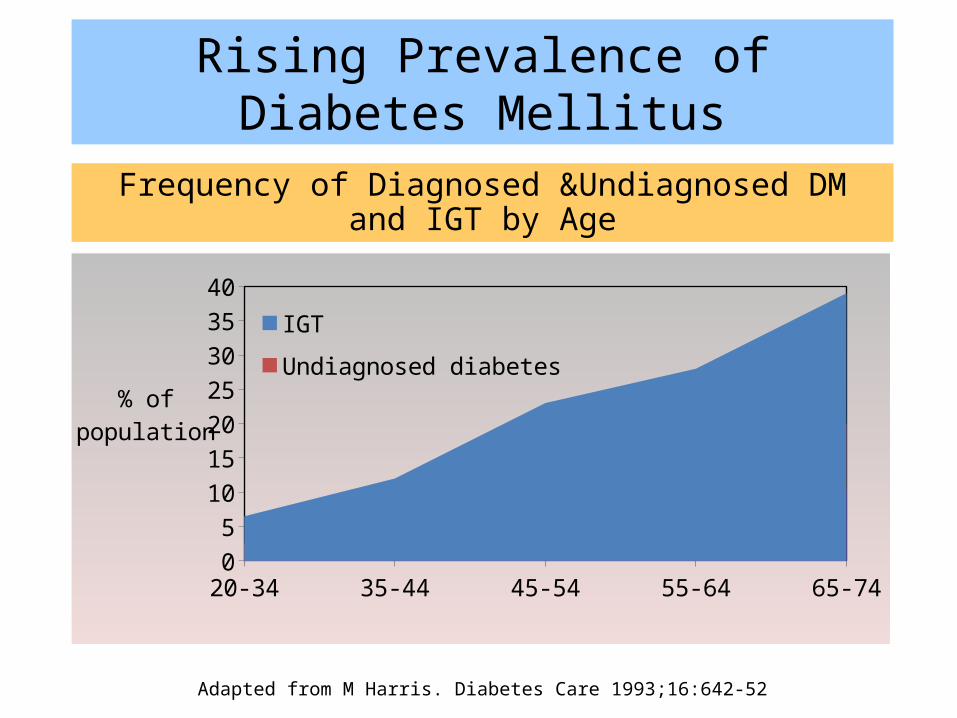
Frequency of Diagnosed &Undiagnosed DM and IGT by Age
Rising Prevalence of Diabetes Mellitus
20-34 35-44 45-54 55-64 65-7405
10152025303540
IGTUndiagnosed diabetesDiagnosed diabetes
% ofpopulation
Adapted from M Harris. Diabetes Care 1993;16:642-52
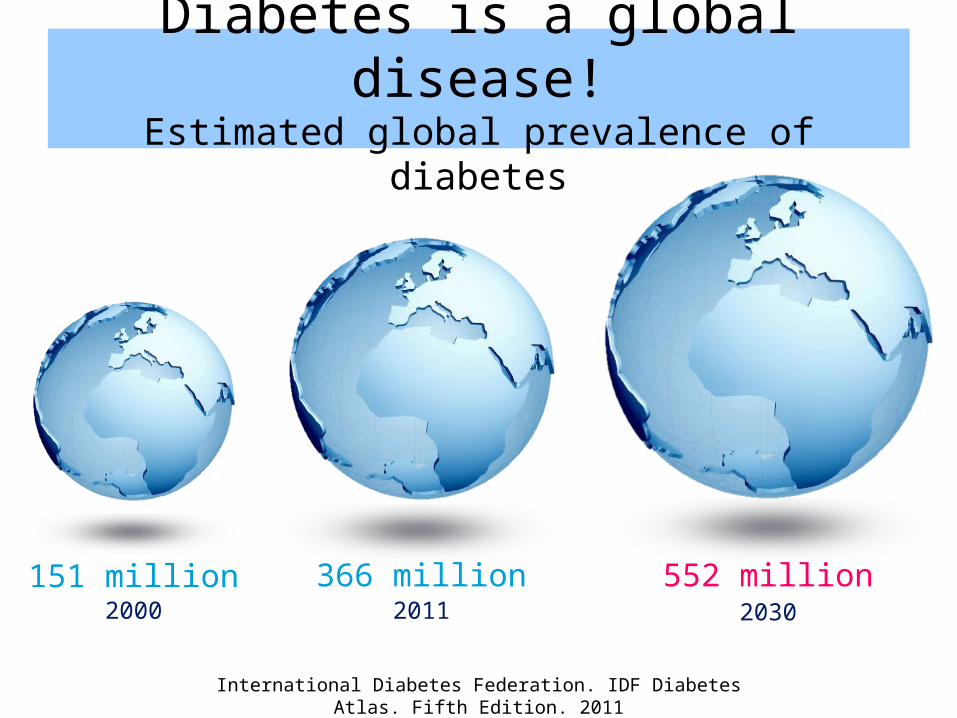
Diabetes is a global disease!Estimated global prevalence of diabetes
International Diabetes Federation. IDF Diabetes Atlas. Fifth Edition. 2011
2000 2011 2030151 million 366 million 552 million
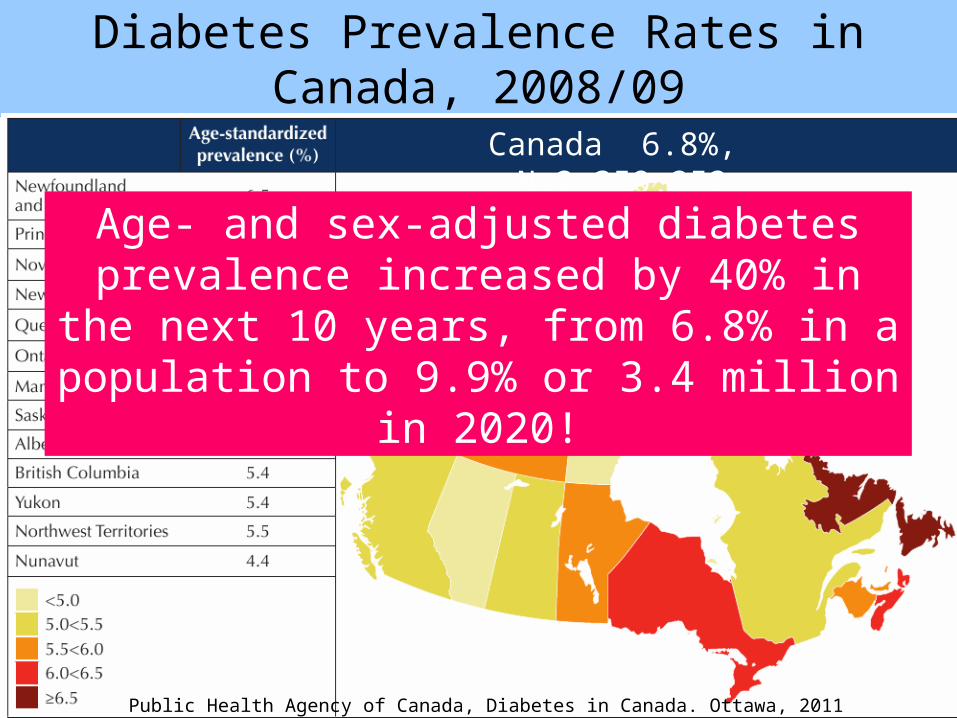
Diabetes Prevalence Rates in Canada, 2008/09
Canada 6.8%, N=2,359,252
Age- and sex-adjusted diabetes prevalence increased by 40% in the next 10 years, from 6.8%
in a population to 9.9% or 3.4 million in 2020!
Public Health Agency of Canada, Diabetes in Canada. Ottawa, 2011
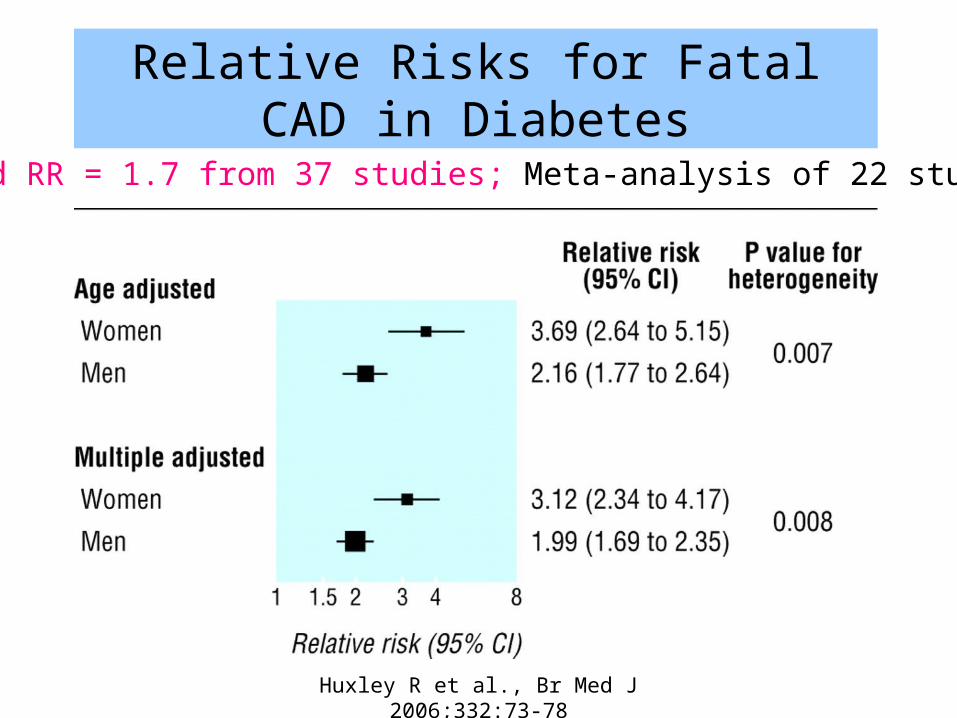
Relative Risks for Fatal CAD in Diabetes
Huxley R et al., Br Med J 2006;332:73-78
Pooled RR = 1.7 from 37 studies; Meta-analysis of 22 studies
People with DM2 and CVD Derive Less Benefit from Preventive and Interventional Therapies
• Patients with diabetes treated with antiplatelet treatments continue to have a higher risk of adverse CV events compared with nondiabetic patients 1
Reduced antiplatelet drug responsiveness may play a role in these worse outcomes
• Diabetes may abolish the beneficial effect of primary percutaneous coronary intervention on long-term risk of reinfarction after acute ST-segment elevation MI 2
1. Angiolillo DJ. Diabetes Care 2009;32:531-540; 2. Madsen MM, et al. Am J Cardiol 2005;96:1469-1475. 9
CV, cardiovascular; CVD, cardiovascular disease; MI, myocardial infarction
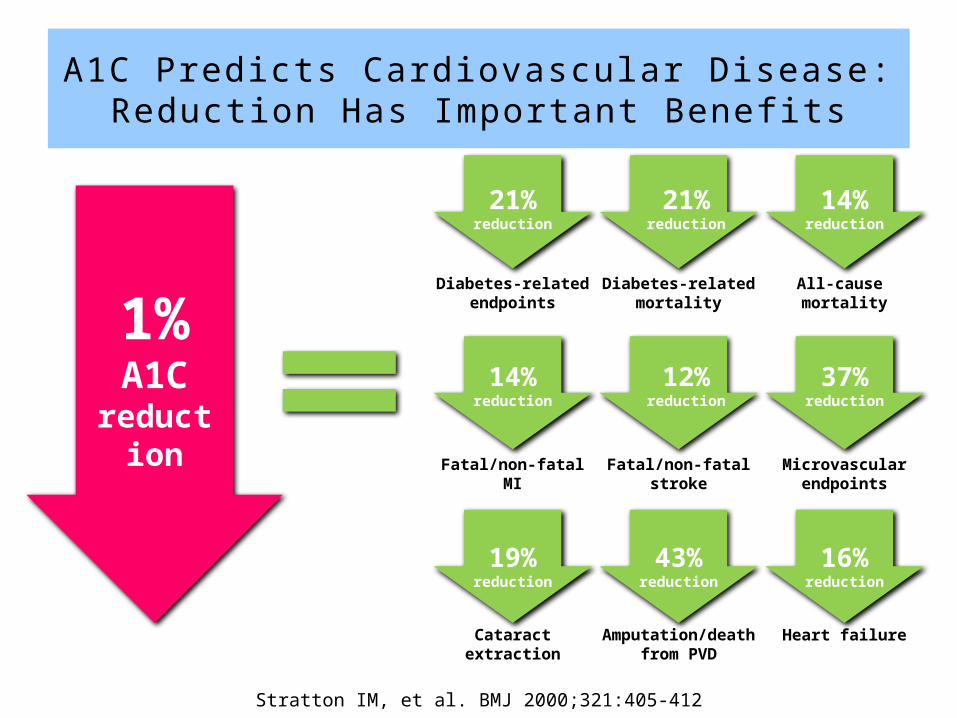
Stratton IM, et al. BMJ 2000;321:405-412
1%A1C
reduction
21%reduction
21%reduction
14%reduction
14%reduction
12%reduction
37%reduction
19%reduction
43%reduction
16%reduction
Diabetes-related endpoints
Cataract extraction
Diabetes-related mortality
All-cause mortality
Fatal/non-fatal MI Fatal/non-fatal stroke Microvascular endpoints
Amputation/death from PVD
Heart failure
A1C Predicts Cardiovascular Disease:Reducti on Has Important Benefi ts
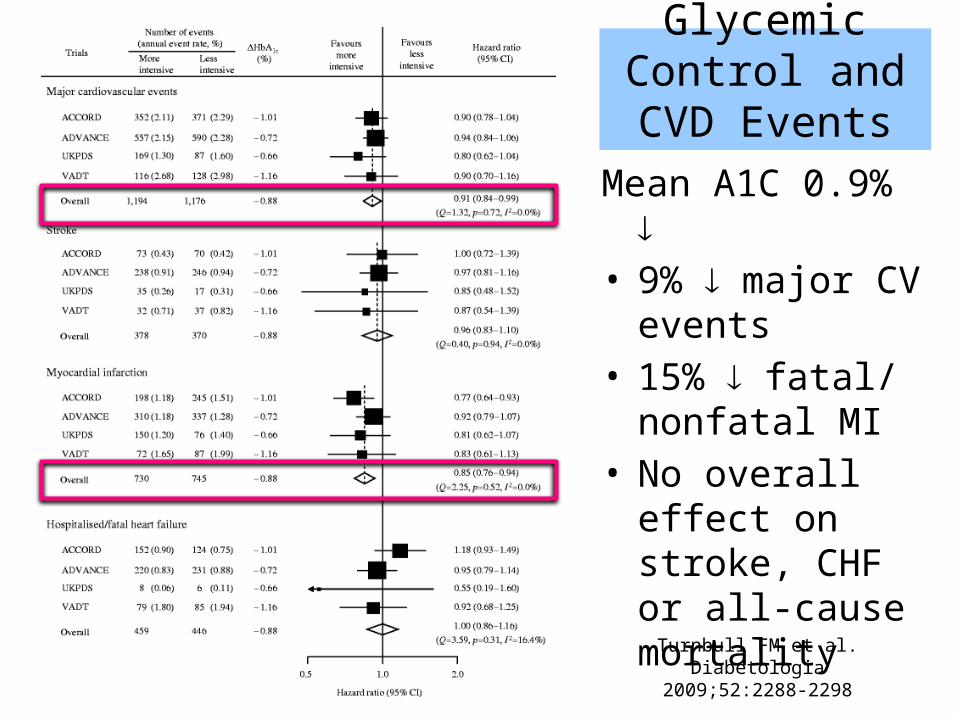
Glycemic Control and CVD Events
Mean A1C 0.9% • 9% major CV
events• 15% fatal/
nonfatal MI• No overall effect
on stroke, CHF or all-cause mortality
Turnbull FM et al. Diabetologia 2009;52:2288-2298
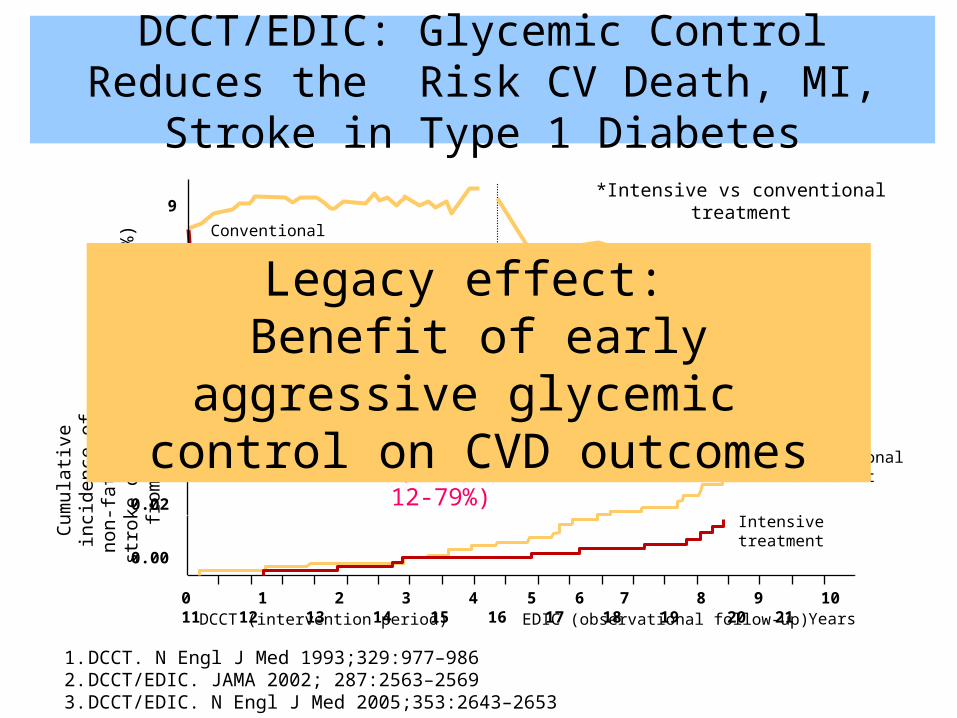
DCCT/EDIC: Glycemic Control Reduces the Risk CV Death, MI, Stroke in Type 1 Diabetes
Conventional treatment
Intensive treatment
*Intensive vs conventional treatment
Cum
ulati
ve in
cide
nce
of n
on-fa
tal M
I, st
roke
or
dea
th fr
om C
VD
Conventionaltreatment
Intensivetreatment
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21Years
0.06
0.04
0.02
0.00
DCCT (intervention period) EDIC (observational follow-up)
07
1 6
A1C
(%)
9
8
2 3 4 5 7 8 9 11 12 13 14 15 16 1710DCCT (intervention period) EDIC (observational follow-up)
Years
1. DCCT. N Engl J Med 1993;329:977–9862. DCCT/EDIC. JAMA 2002; 287:2563–25693. DCCT/EDIC. N Engl J Med 2005;353:2643–2653
CVD death, MI & StrokeRR 57% (p = 0.02, 95%CI 12-79%)
Legacy effect: Benefit of early aggressive glycemic
control on CVD outcomes
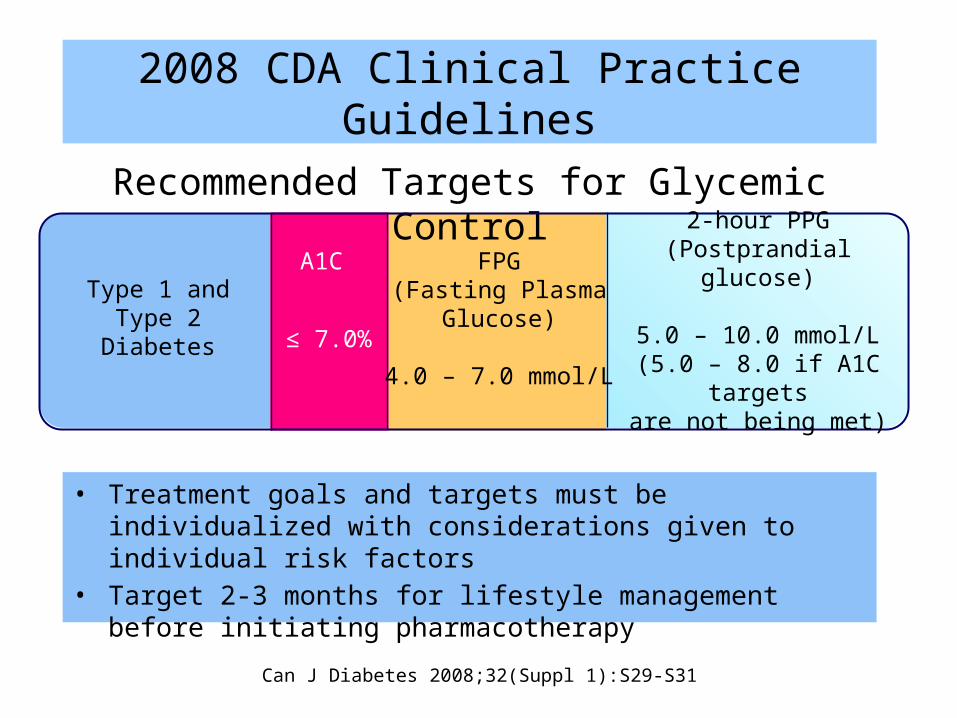
• Treatment goals and targets must be individualized with considerations given to individual risk factors
• Target 2-3 months for lifestyle management before initiating pharmacotherapy
Recommended Targets for Glycemic Control
Can J Diabetes 2008;32(Suppl 1):S29-S31
FPG(Fasting Plasma
Glucose)
4.0 – 7.0 mmol/L
2-hour PPG(Postprandial glucose)
5.0 – 10.0 mmol/L(5.0 – 8.0 if A1C targets
are not being met)
A1C
≤ 7.0%Type 1 and Type 2
Diabetes
2008 CDA Clinical Practice Guidelines
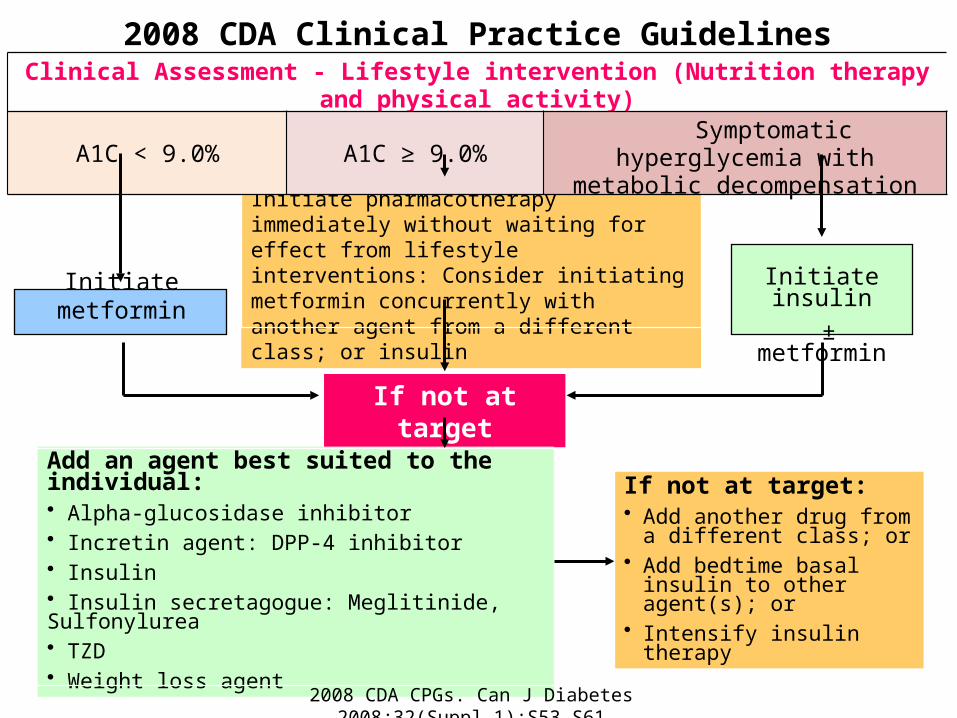
Initiate metformin
Initiate pharmacotherapy immediately without waiting for effect from lifestyle interventions: Consider initiating metformin concurrently with another agent from a different class; or insulin Initiate insulin
± metformin
If not at target
Add an agent best suited to the individual:• Alpha-glucosidase inhibitor• Incretin agent: DPP-4 inhibitor• Insulin• Insulin secretagogue: Meglitinide, Sulfonylurea• TZD• Weight loss agent
If not at target:• Add another drug from a
different class; or • Add bedtime basal insulin to
other agent(s); or • Intensify insulin therapy
2008 CDA Clinical Practice GuidelinesClinical Assessment - Lifestyle intervention (Nutrition therapy and physical activity)
A1C < 9.0% A1C ≥ 9.0% Symptomatic hyperglycemia with metabolic decompensation
2008 CDA CPGs. Can J Diabetes 2008;32(Suppl 1):S53–S61
How do glucose-lowering drugs work?
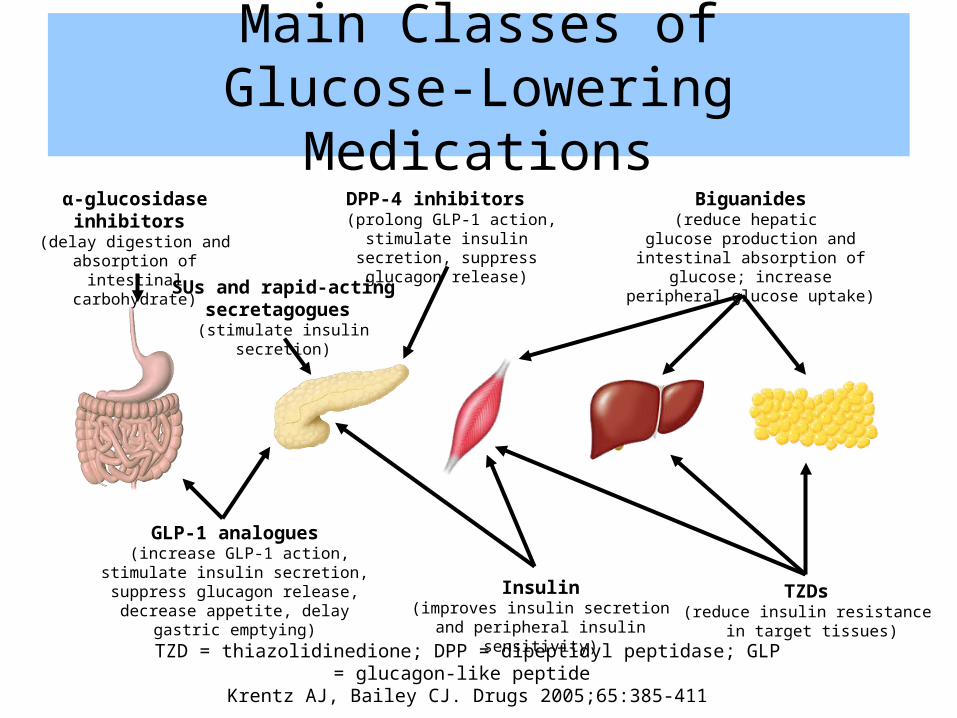
Main Classes ofGlucose-Lowering Medications
TZD = thiazolidinedione; DPP = dipeptidyl peptidase; GLP = glucagon-like peptide Krentz AJ, Bailey CJ. Drugs 2005;65:385-411
SUs and rapid-acting secretagogues
(stimulate insulin secretion)
Biguanides(reduce hepatic
glucose production and intestinal absorption of glucose; increase
peripheral glucose uptake)
α-glucosidase inhibitors (delay digestion and
absorption of intestinal carbohydrate)
TZDs (reduce insulin resistance
in target tissues)
DPP-4 inhibitors (prolong GLP-1 action, stimulate
insulin secretion, suppress glucagon release)
GLP-1 analogues (increase GLP-1 action, stimulate insulin
secretion, suppress glucagon release, decrease appetite, delay gastric emptying) Insulin
(improves insulin secretion and peripheral insulin sensitivity)
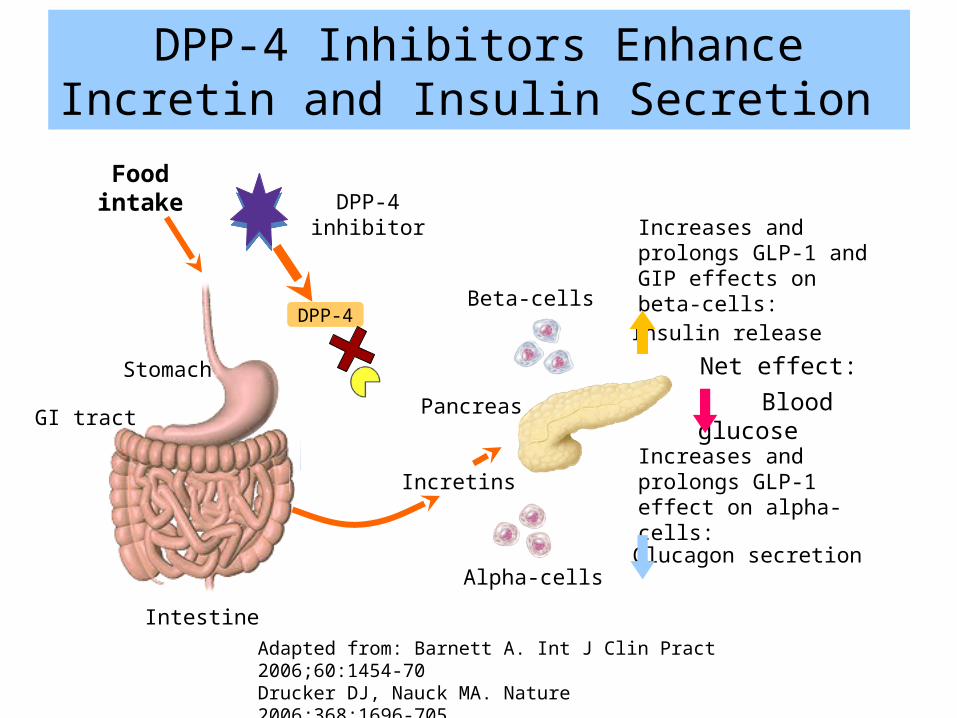
Food intake
Stomach
GI tract
Intestine
Increases and prolongs GLP-1 effect on alpha-cells:
Alpha-cells
Pancreas
Insulin release
Net effect: Blood glucose
Beta-cells
Increases and prolongs GLP-1 and GIP effects on beta-cells:
DPP-4 inhibitor
Glucagon secretion
Incretins
DPP-4
DPP-4 Inhibitors Enhance Incretin and Insulin Secretion
Adapted from: Barnett A. Int J Clin Pract 2006;60:1454-70 Drucker DJ, Nauck MA. Nature 2006;368:1696-705Idris I, Donnelly R. Diabetes Obes Metab 2007;9:153-65
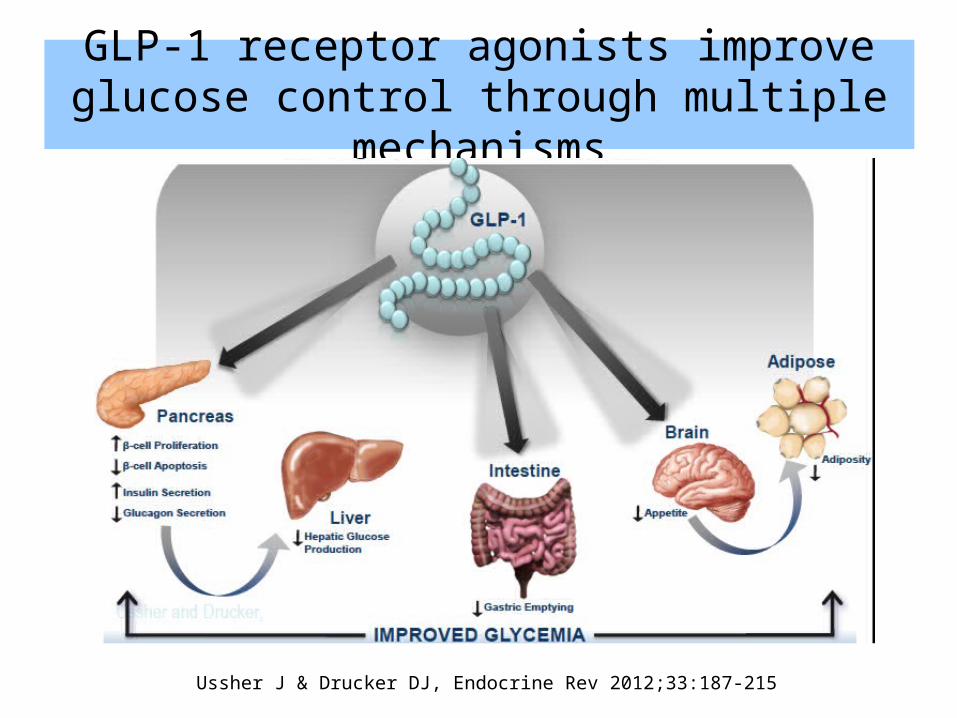
GLP-1 receptor agonists improve glucose control through multiple mechanisms
Ussher J & Drucker DJ, Endocrine Rev 2012;33:187-215
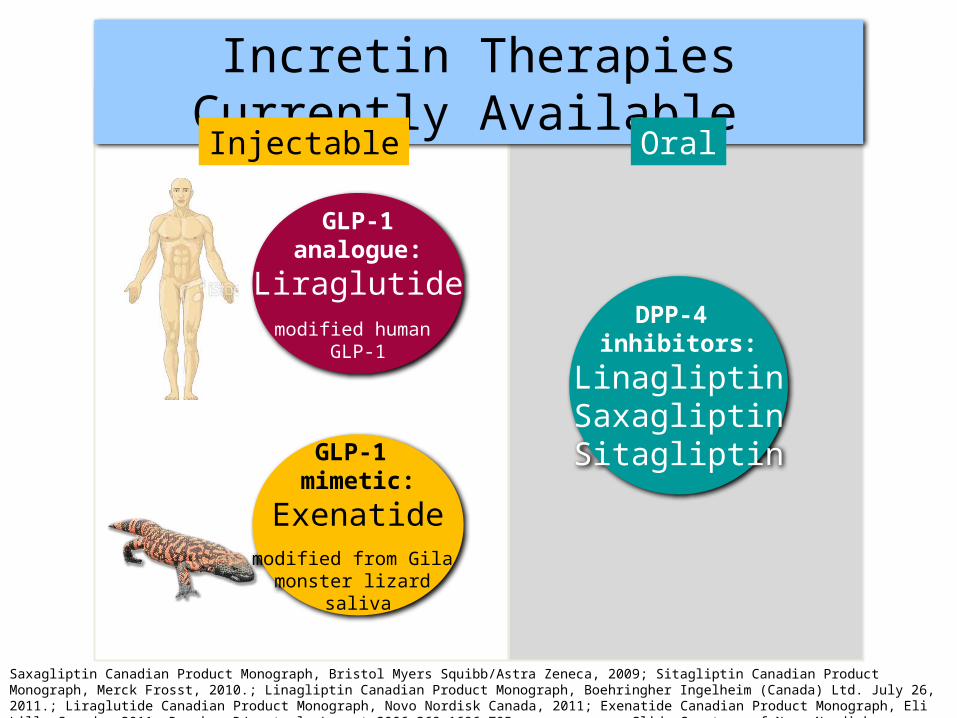
Saxagliptin Canadian Product Monograph, Bristol Myers Squibb/Astra Zeneca, 2009; Sitagliptin Canadian Product Monograph, Merck Frosst, 2010.; Linagliptin Canadian Product Monograph, Boehringher Ingelheim (Canada) Ltd. July 26, 2011.; Liraglutide Canadian Product Monograph, Novo Nordisk Canada, 2011; Exenatide Canadian Product Monograph, Eli Lilly Canada, 2011. Drucker DJ, et al. Lancet 2006;368:1696-705 Slide Courtesy of Novo Nordisk sponsored accredited CHE program
GLP-1analogue:
Liraglutidemodified human
GLP-1
GLP-1 mimetic:
Exenatidemodified from Gila
monster lizard saliva
DPP-4 inhibitors:
LinagliptinSaxagliptinSitagliptin
Incretin Therapies Currently Available
Injectable Oral
Questions to consider when choosing a glucose-lowering agent
• What is the efficacy in A1C reduction?• What is the glycemic durability?• Is the patient at risk for hypoglycemia?• Is weight a concern?• What are the long-term side-effects?• Does the patient have a drug plan?• What is your prescribing comfort level?• What is your patient’s preference?
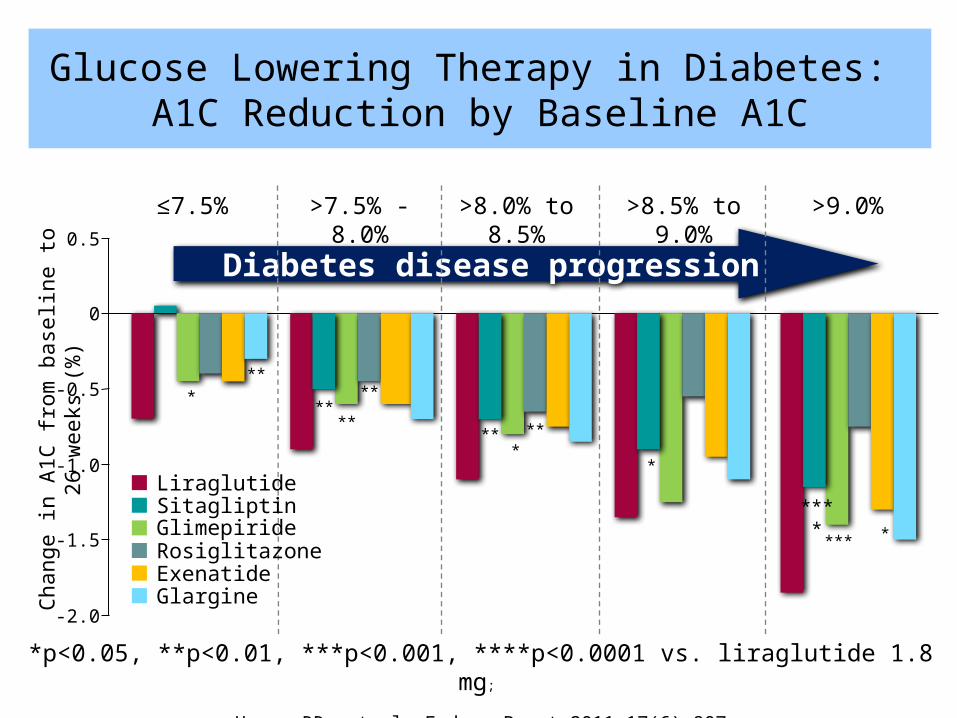
*p<0.05, **p<0.01, ***p<0.001, ****p<0.0001 vs. liraglutide 1.8 mg ;
Henry RR, et al. Endocr Pract 2011;17(6):907
Diabetes disease progression
≤7.5% >7.5% - 8.0% >8.0% to 8.5% >8.5% to 9.0% >9.0%
***
****
**
** ***
*
****
****
0.5
0
-0.5
-1.0
-1.5
-2.0Chan
ge in
A1C
from
bas
elin
e to
26
wee
ks (%
)
Exenatide
LiraglutideSitagliptin GlimepirideRosiglitazone
Glargine
Glucose Lowering Therapy in Diabetes: A1C Reduction by Baseline A1C
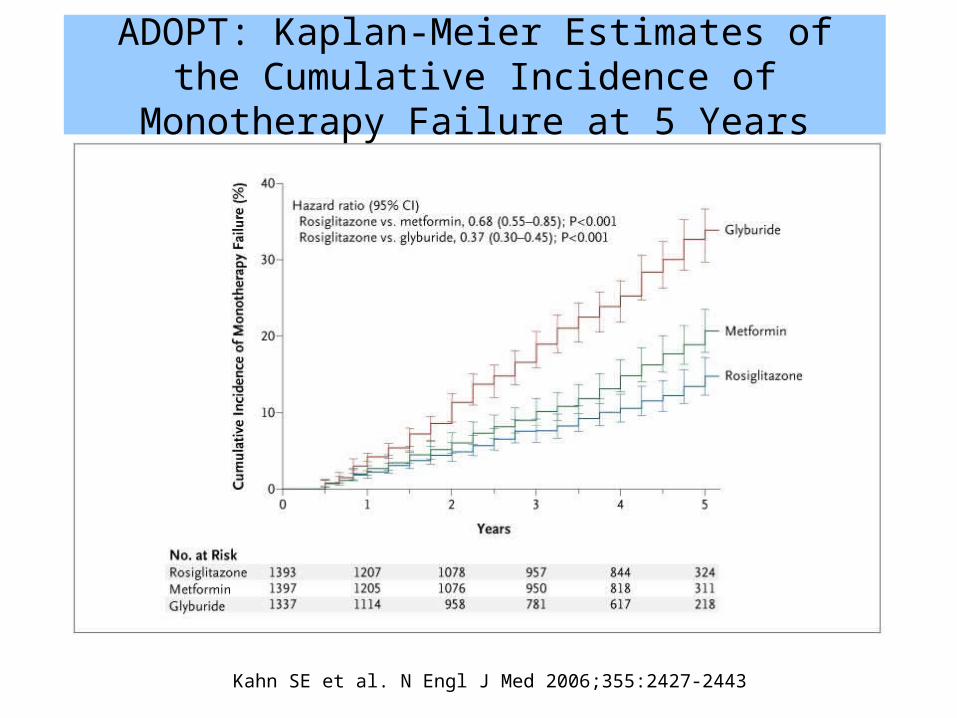
Kahn SE et al. N Engl J Med 2006;355:2427-2443
ADOPT: Kaplan-Meier Estimates of the Cumulative Incidence of Monotherapy Failure at 5 Years
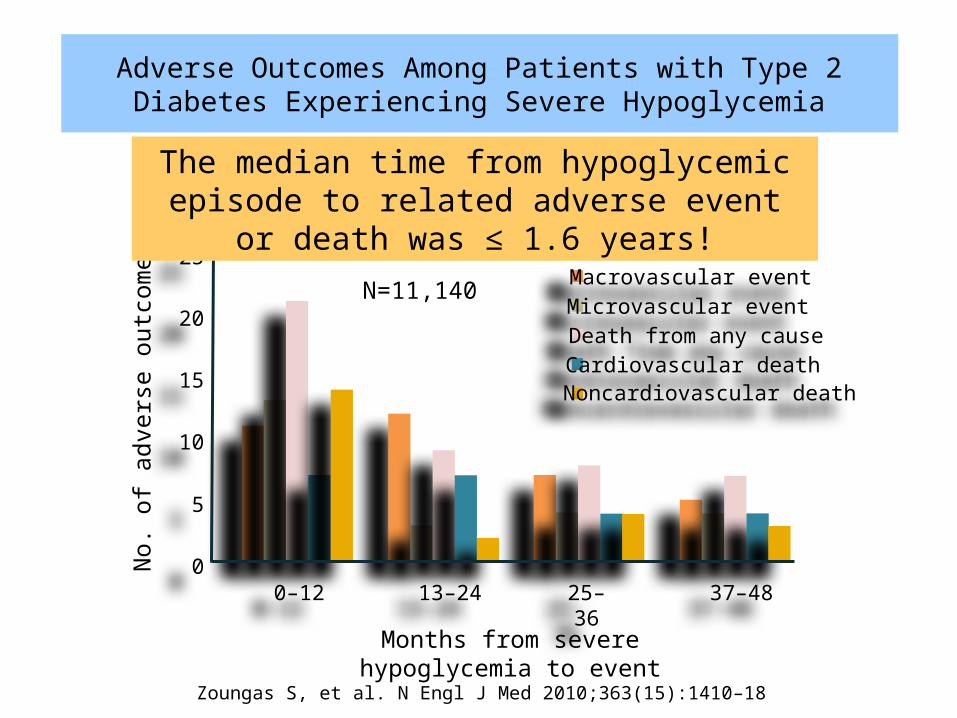
Adverse Outcomes Among Patients with Type 2 Diabetes Experiencing Severe Hypoglycemia
25
No.
of a
dver
se o
utco
mes
Months from severe hypoglycemia to event
20
15
10
5
00–12 13–24 25–36 37–48
Macrovascular eventMicrovascular eventDeath from any causeCardiovascular deathNoncardiovascular death
Zoungas S, et al. N Engl J Med 2010;363(15):1410–18
The median time from hypoglycemic episode to related adverse event or death was ≤ 1.6 years!
N=11,140
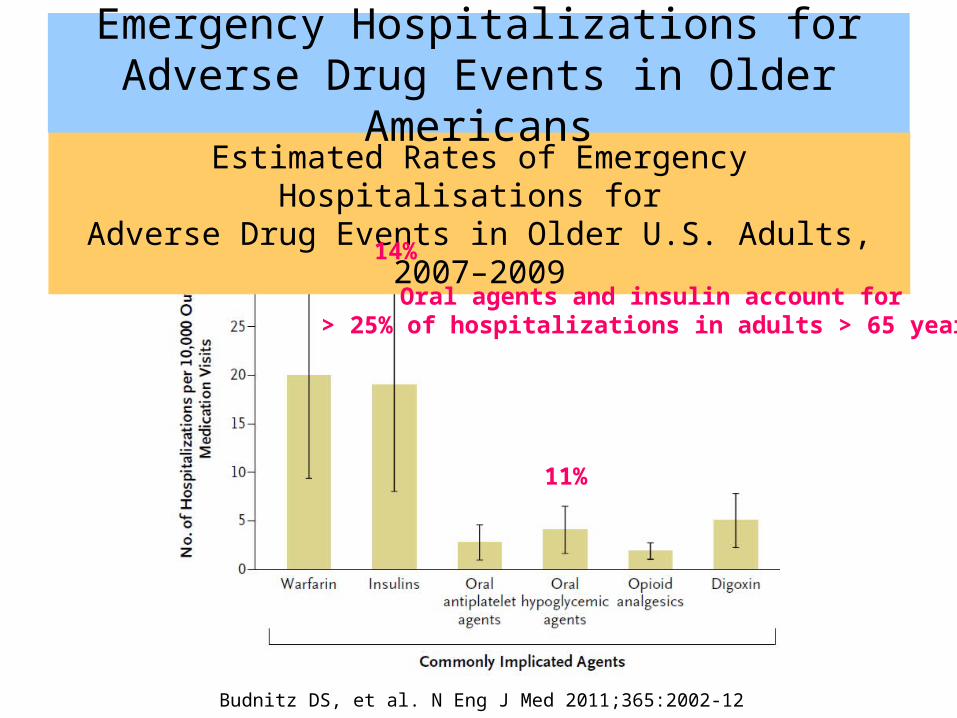
Estimated Rates of Emergency Hospitalisations for Adverse Drug Events in Older U.S. Adults, 2007–2009
Budnitz DS, et al. N Eng J Med 2011;365:2002-12
14%
11%
Emergency Hospitalizations forAdverse Drug Events in Older Americans
Oral agents and insulin account for > 25% of hospitalizations in adults > 65 years!
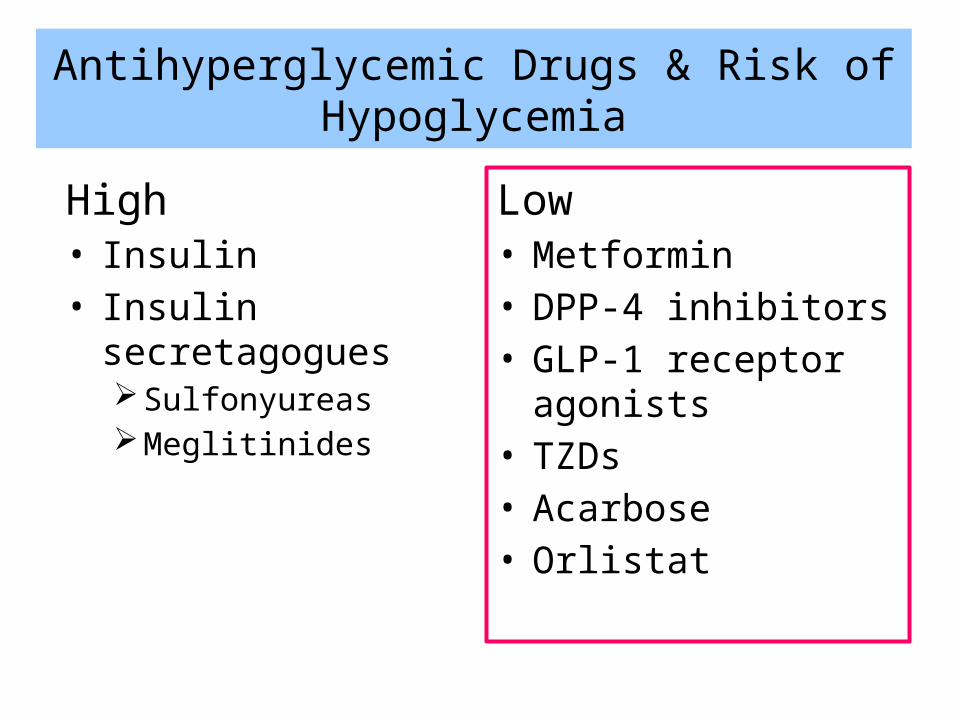
Antihyperglycemic Drugs & Risk of Hypoglycemia
High• Insulin• Insulin secretagogues
SulfonyureasMeglitinides
Low• Metformin• DPP-4 inhibitors• GLP-1 receptor agonists• TZDs• Acarbose• Orlistat
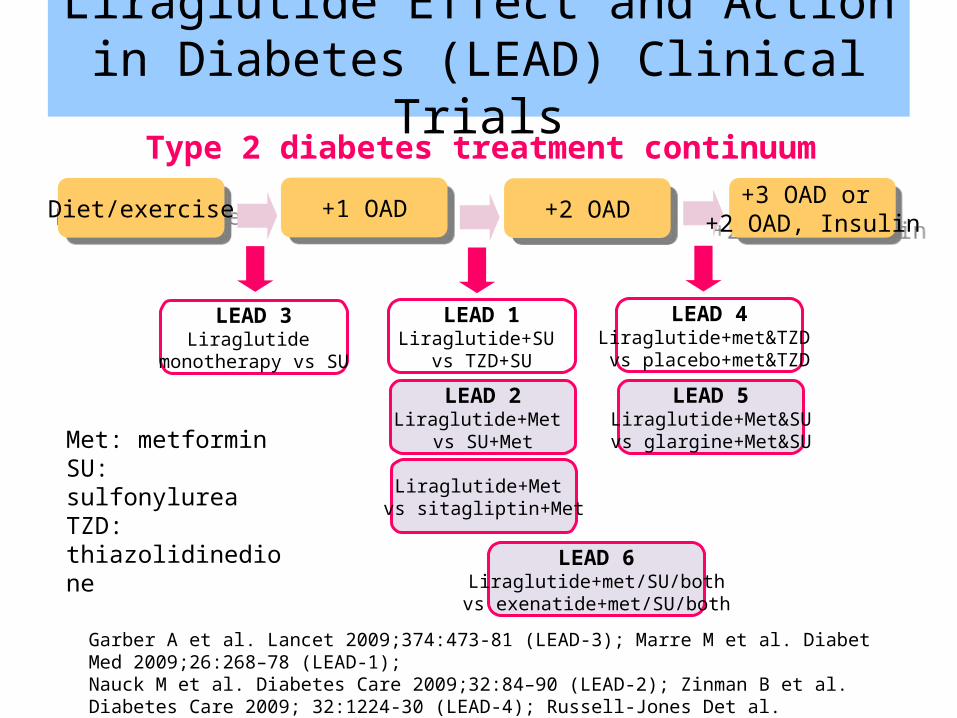
Garber A et al. Lancet 2009;374:473-81 (LEAD-3); Marre M et al. Diabet Med 2009;26:268–78 (LEAD-1); Nauck M et al. Diabetes Care 2009;32:84–90 (LEAD-2); Zinman B et al. Diabetes Care 2009; 32:1224-30 (LEAD-4); Russell-Jones Det al. Diabetologia 2009;52:2046-55 (LEAD-5); Buse J et al. Lancet 2009;374:39-47 (LEAD-6); Pratley R et al. Lancet 2010;375:1447-1456 (Lira vs. sitagliptin)
LEAD 3Liraglutide
monotherapy vs SU
Diet/exerciseDiet/exercise
Met: metformin SU: sulfonylurea TZD: thiazolidinedione
+1 OAD+1 OAD +2 OAD+2 OAD +3 OAD or +2 OAD, Insulin
+3 OAD or +2 OAD, Insulin
LEAD 2Liraglutide+Met
vs SU+Met
LEAD 1Liraglutide+SU
vs TZD+SU
LEAD 6Liraglutide+met/SU/both
vs exenatide+met/SU/both
LEAD 4Liraglutide+met&TZD vs placebo+met&TZD
LEAD 5Liraglutide+Met&SUvs glargine+Met&SU
Type 2 diabetes treatment continuum
Liraglutide Effect and Action in Diabetes (LEAD) Clinical Trials
Liraglutide+Met vs sitagliptin+Met
-0.51%
-0.97%-1.00%-0.98%
-0.4%
-0.5%
-1.09%
-0.79%
-0.9%-0.84%*
-1.14%*-1.1%* -1.1%*
-1.5%* -1.5%*
-1.33%*
-1.12%*
-1.2%*
-1.5%*-1.60%
-1.40%
-1.20%
-1.00%
-0.80%
-0.60%
-0.40%
-0.20%
0.00%
Chan
ge in
A1C
% fr
om b
asel
ine
Liraglutide 1.2mg Liraglutide 1.8mg Glimepiride Rosiglitazone Placebo Glargine Exenatide Sitagliptin
MonotherapyLEAD-3
MET Combination
LEAD-2
SU Combination
LEAD-1
MET + TZD Combination
LEAD-4
MET + SU Combination
LEAD-5
MET ± SU Combination
LEAD-6
MET + SitagliptinNN2211-1860
p=0.0014
p<0.0001p<0.0001 p<0.0001
p=0.0015
p<0.0001
p<0.0001
p<0.0001p<0.0001 p<0.0001
Garber A et al, Lancet 2009;373:473–81 (LEAD-3); Nauck M et al, Diabetes Care 2009;32:84-90 (LEAD 2); Marre M et al. Diabetic Med 2009;26:268-78 (LEAD 1); Zinman B et al. Diabetes Care 2009;32:1224-30 (LEAD 4); Russell-Jones D et al. Diabetes 2009;52:2046-55 (LEAD 5); Buse J et al. Lancet 2009;374:39-47 (LEAD 6); Pratley R et al. Lancet 2010;375:1447-1456
*significant vs. comparator
LEAD Program: A1C Lowering with Liraglutide
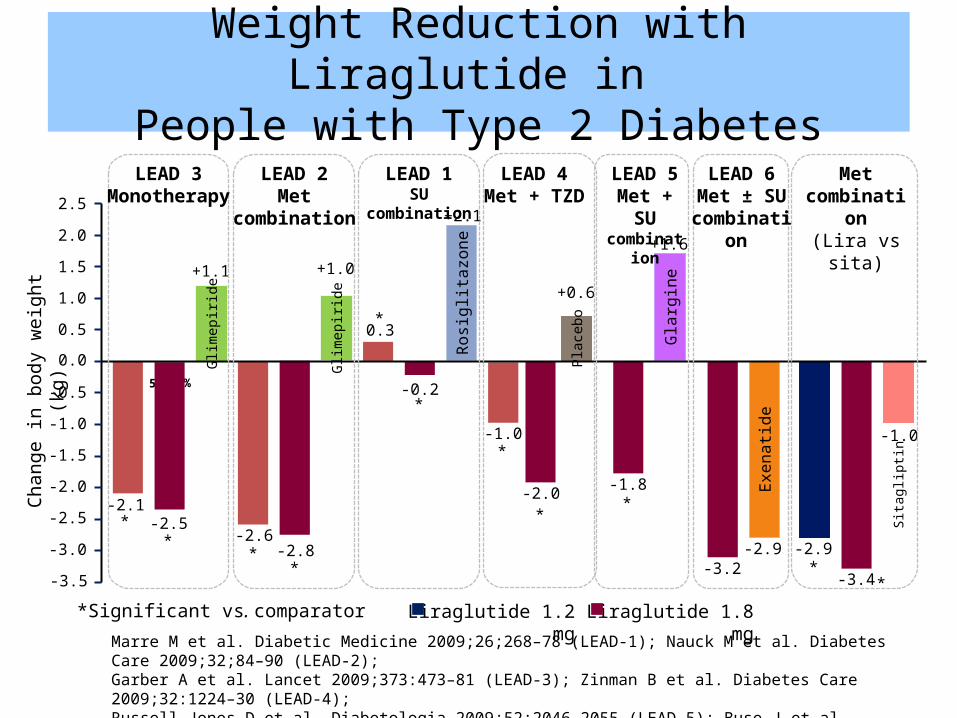
Weight Reduction with Liraglutide in People with Type 2 Diabetes
Chan
ge in
bod
y w
eigh
t (kg
)
0.0
-0.5
-1.0
-1.5
-2.0 -1.8-2.0
51%43%
-2.5
-2.8
-2.5
-3.0-3.2
-3.5
2.5
2.0
1.5
1.0
0.5
-0.2
Exen
atide
-2.9
Plac
ebo
Glim
epiri
de
Rosi
glita
zone
Gla
rgin
e
Glim
epiri
de
+1.1
+1.6
+0.6+1.0
+2.1
Liraglutide 1.8 mg*Significant vs. comparator
-2.1
-2.6
0.3
-1.0
**
*
*
*
*
**
Liraglutide 1.2 mg
*
-2.9
-3.4
-1.0
Sita
glip
tin
**
LEAD 1SU combination
LEAD 2Met
combination
LEAD 4Met + TZD
LEAD 5Met + SU
combination
LEAD 3Monotherapy
LEAD 6Met ± SU
combination
Met combination(Lira vs sita)
Marre M et al. Diabetic Medicine 2009;26;268–78 (LEAD-1); Nauck M et al. Diabetes Care 2009;32;84–90 (LEAD-2); Garber A et al. Lancet 2009;373:473–81 (LEAD-3); Zinman B et al. Diabetes Care 2009;32:1224–30 (LEAD-4); Russell-Jones D et al. Diabetologia 2009;52:2046-2055 (LEAD-5); Buse J et al. Lancet 2009;374 (9683):39–47 (LEAD-6); Pratley R et al. Lancet 2010;375:1447-56 (Lira vs sitagliptin)
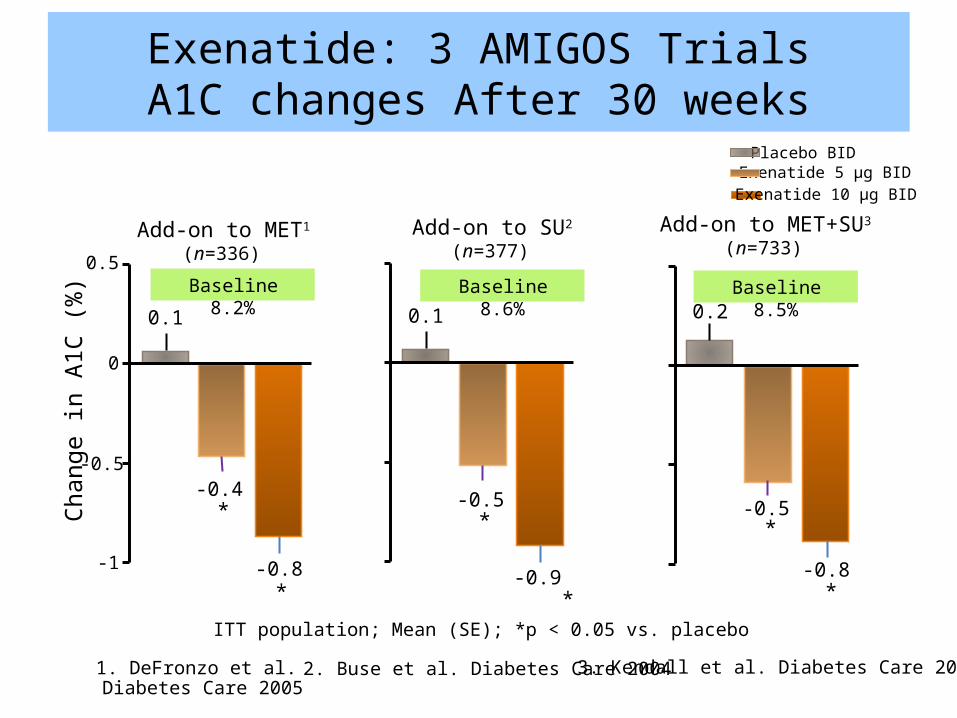
Exenatide: 3 AMIGOS TrialsA1C changes After 30 weeks
Chan
ge in
A1C
(%)
Placebo BID
-0.4*
-0.8*
-1
-0.5
0
0.5
0.1
Add-on to MET1
(n=336)
1. DeFronzo et al. Diabetes Care 2005
ITT population; Mean (SE); *p < 0.05 vs. placebo
Baseline 8.2%
Exenatide 5 µg BID
Add-on to SU2
(n=377)
*
0.1
-0.5*
-0.9
Baseline 8.6%
2. Buse et al. Diabetes Care 2004
Exenatide 10 µg BID
Add-on to MET+SU3
(n=733)
*
0.2
-0.5*
-0.8
Baseline 8.5%
3. Kendall et al. Diabetes Care 2005
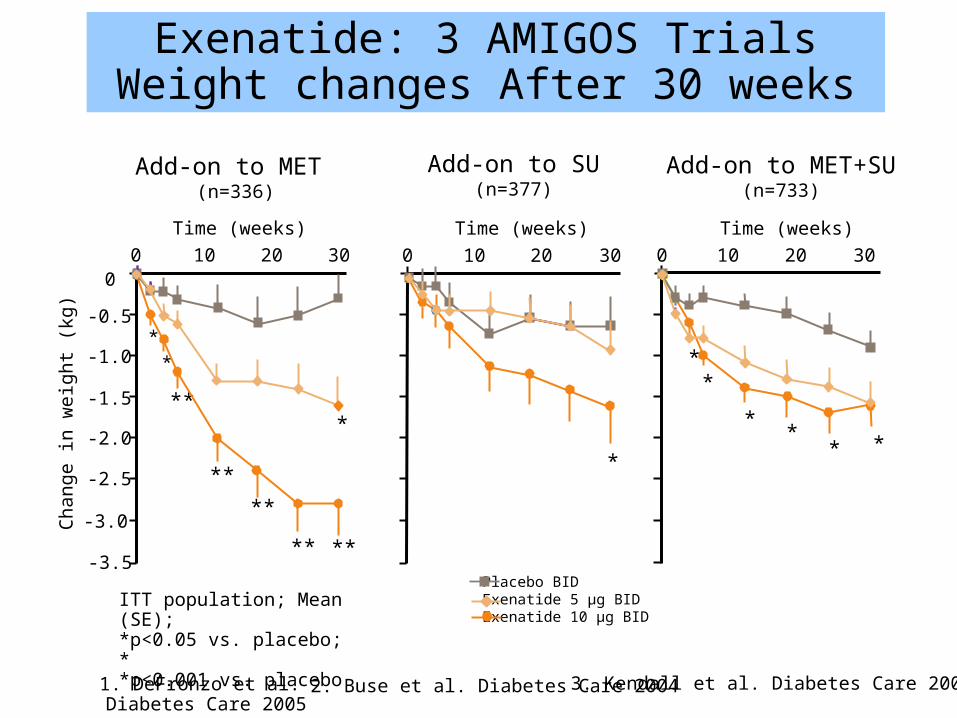
Add-on to MET (n=336)
0 10 20
-3.0
-2.5
-2.0
-1.5
-1.0
-0.5
030
**
**
****
** **-3.5
*
Cha
nge
in w
eigh
t (kg
)
Time (weeks)
ITT population; Mean (SE); *p<0.05 vs. placebo; **p<0.001 vs. placebo
Exenatide: 3 AMIGOS TrialsWeight changes After 30 weeks
1. DeFronzo et al. Diabetes Care 2005
Add-on to SU(n=377)
0 10 20 30
*
Time (weeks)
2. Buse et al. Diabetes Care 2004
Placebo BIDExenatide 5 µg BIDExenatide 10 µg BID
Add-on to MET+SU(n=733)
0 10 20 30
*
*
*
** *
Time (weeks)
3. Kendall et al. Diabetes Care 2005
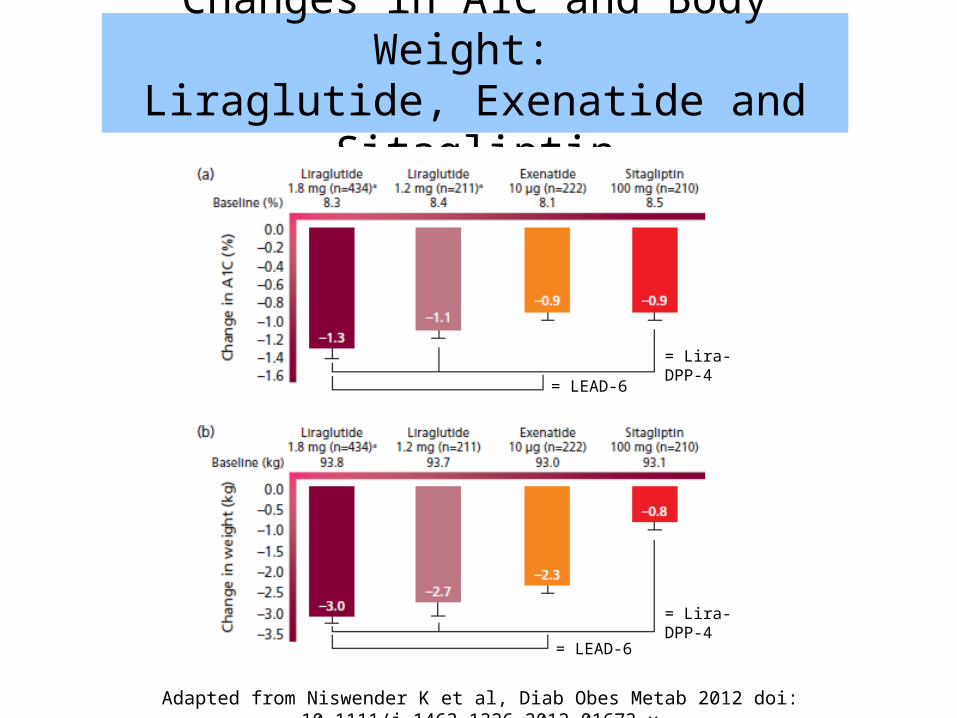
Changes in A1C and Body Weight: Liraglutide, Exenatide and Sitagliptin
= LEAD-6
= LEAD-6
= Lira-DPP-4
= Lira-DPP-4
Adapted from Niswender K et al, Diab Obes Metab 2012 doi: 10.1111/j.1463-1326.2012.01673.x
Glucose-lowering Drugs and CVD Risk
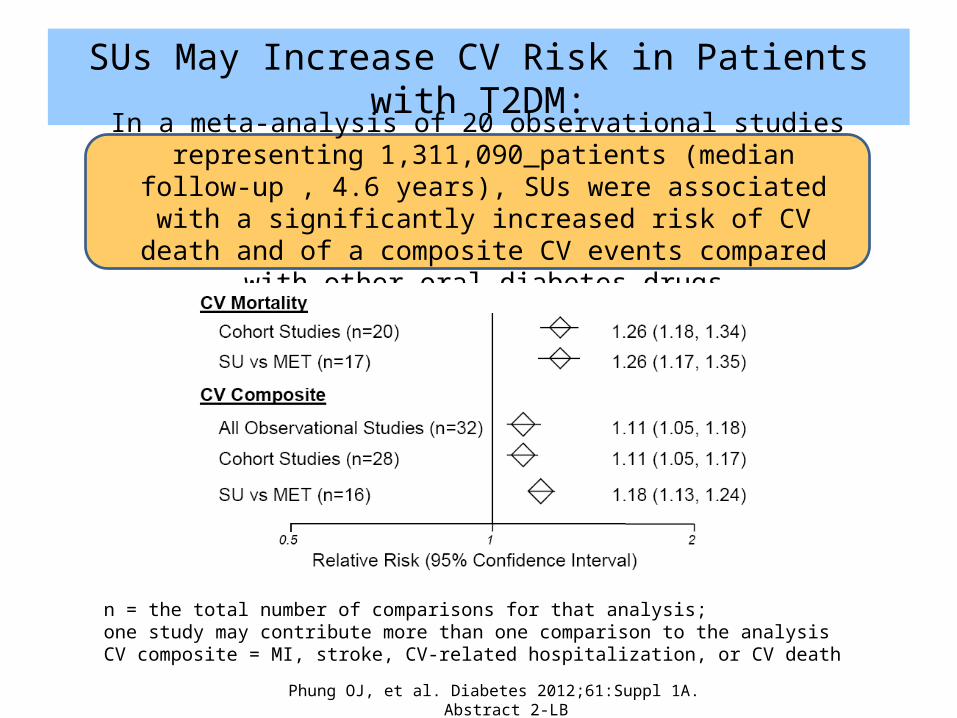
SUs May Increase CV Risk in Patients with T2DM:
34
In a meta analysis of 20 observational studies representing 1,311,090‐ patients (median follow-up , 4.6 years), SUs were associated with a
significantly increased risk of CV death and of a composite CV events compared with other oral diabetes drugs
Phung OJ, et al. Diabetes 2012;61:Suppl 1A. Abstract 2-LB
n = the total number of comparisons for that analysis; one study may contribute more than one comparison to the analysisCV composite = MI, stroke, CV-related hospitalization, or CV death
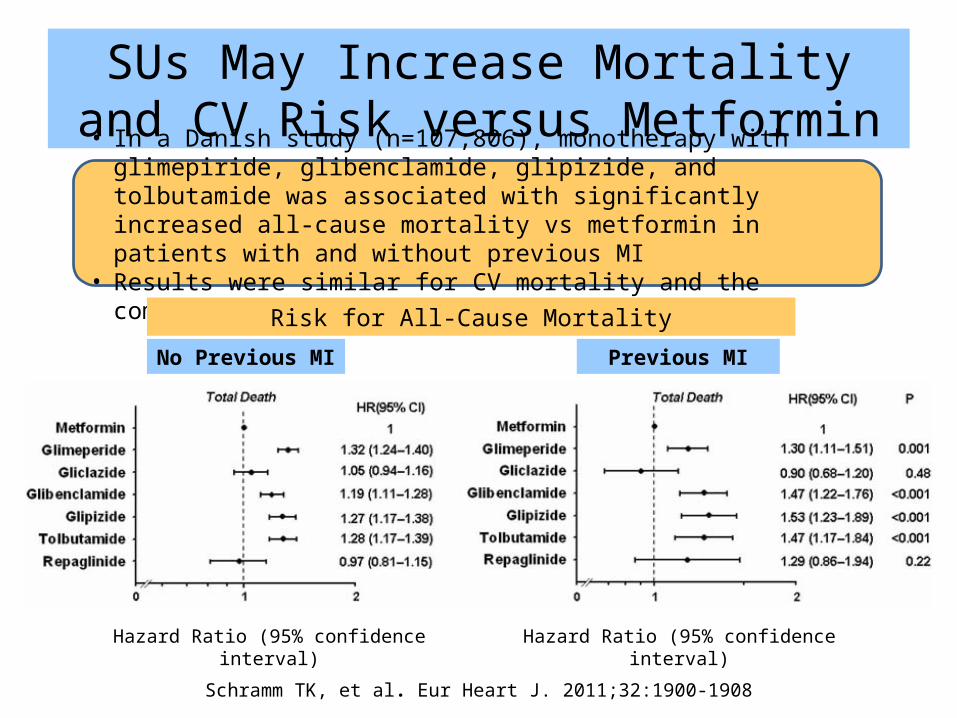
SUs May Increase Mortality and CV Risk versus Metformin
35
• In a Danish study (n=107,806), monotherapy with glimepiride, glibenclamide, glipizide, and tolbutamide was associated with significantly increased all-cause mortality vs metformin in patients with and without previous MI
• Results were similar for CV mortality and the composite CV end point
Schramm TK, et al. Eur Heart J. 2011;32:1900-1908
Hazard Ratio (95% confidence interval) Hazard Ratio (95% confidence interval)
No Previous MI Previous MI
Risk for All-Cause Mortality
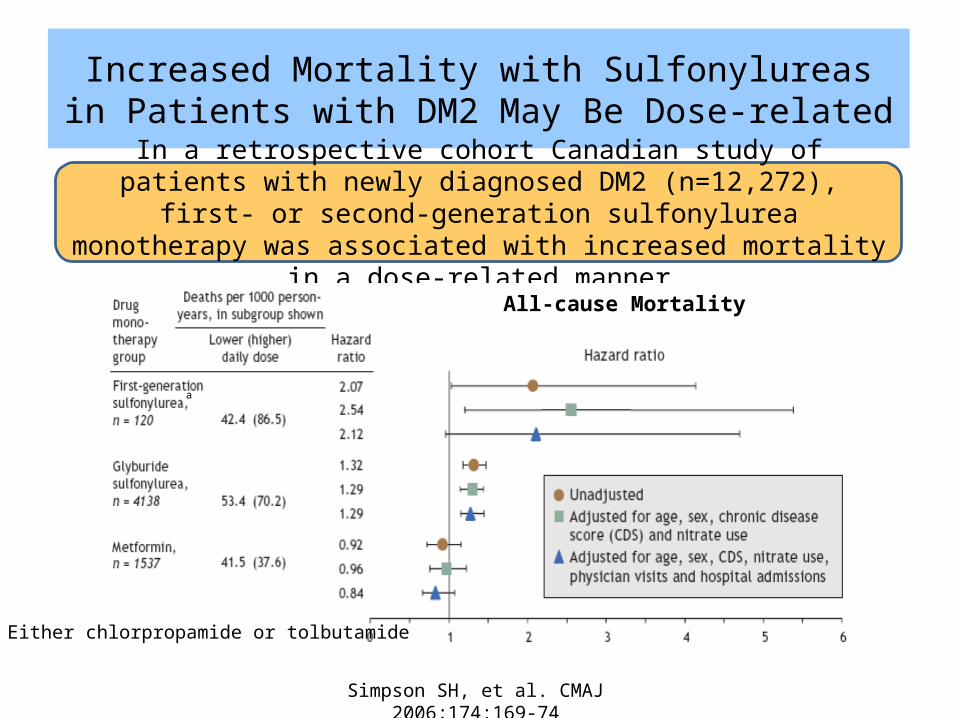
Increased Mortality with Sulfonylureas in Patients with DM2 May Be Dose-related
In a retrospective cohort Canadian study of patients with newly diagnosed DM2 (n=12,272), first- or second-generation sulfonylurea monotherapy was
associated with increased mortality in a dose-related manner
Simpson SH, et al. CMAJ 2006;174:169-74 36
All-cause Mortality
a
a Either chlorpropamide or tolbutamide
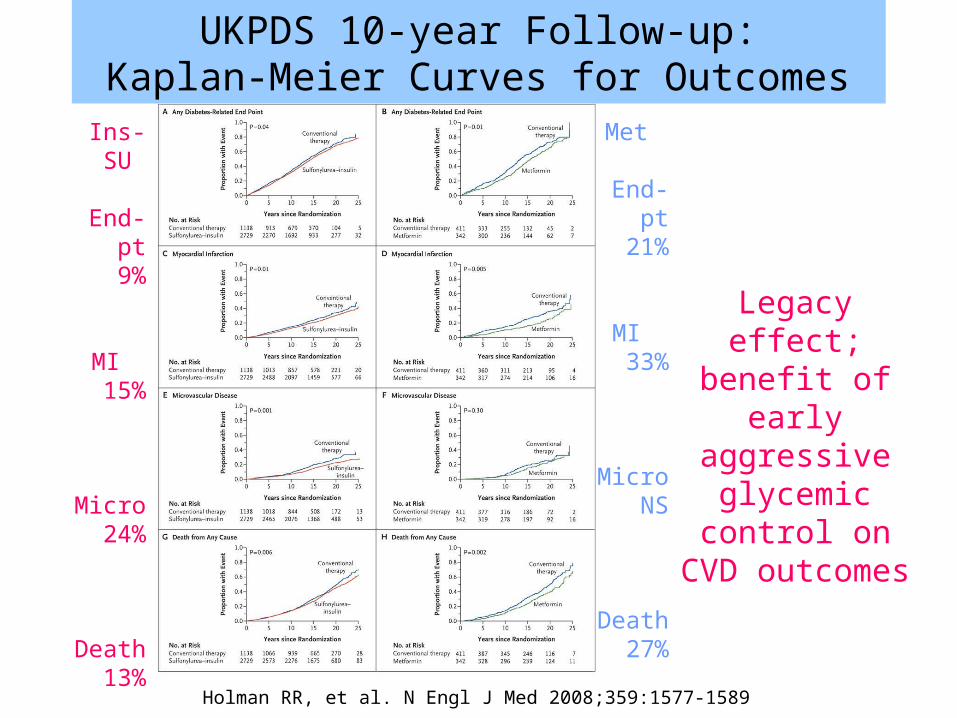
Holman RR, et al. N Engl J Med 2008;359:1577-1589
UKPDS 10-year Follow-up:Kaplan-Meier Curves for Outcomes
Legacy effect; benefit of early
aggressive glycemic control on CVD
outcomes
Holman RR, et al. N Engl J Med 2008;359:1577-1589
Ins-SU
End-pt9%
MI15%
Micro24%
Death13%
Met
End-pt21%
MI33%
MicroNS
Death27%
Cardioprotective Effects of GLP-1
• GLP-1 improves cardiac function in heart failure 1,2
• GLP-1 increases myocardial glucose uptake 3 • GLP-1 improves functional recovery following
myocardial ischemia 4-6
• Incretins reduce infarct size 7-9
• GLP-1 improves endothelium dysfunction 10,11
1 Nikolaidis et al. Circulation 2004;110:955–61 2 Poornima I et al. Circ Heart Fail. 2008;1:153-1603 Zhao et al. J Pharmacol Exp Ther 2006;317:1106–13 4 Nikolaidis et al. J. Pharm Exp Ther 2005;312:303 5 Nikolaidis et al. Circulation 2004;109:962 6 Ban et al. Circulation 2008;117:2340 7 Bose A et al. Diabetes 2005;54:146 8 Noyan-Ashraf et al. Diabetes 2009;58:975 9 Sauve et al. Diabetes 2010;59:1063–73 10 Basu et al. Am J Physiol Endocrinol Metab 2007;293:E1289–95 11 Nyström et al. Am J Physiol Endocrinol Metab 2004;287:E1209–15
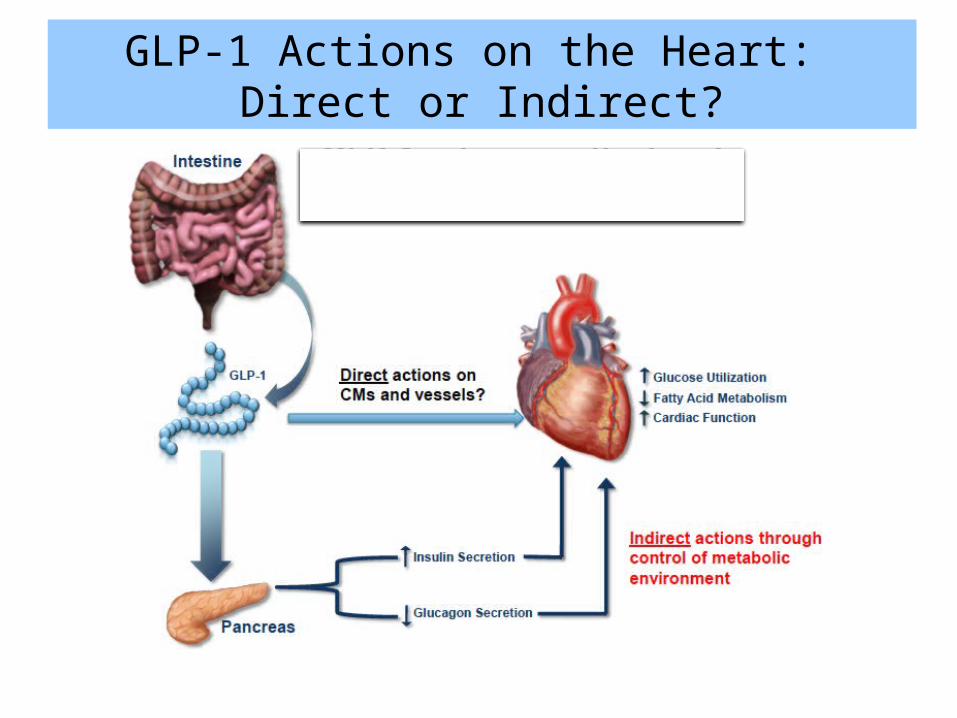
GLP-1 Actions on the Heart: Direct or Indirect?
Ussher J, Drucker DJ, Endocrine Rev. 2012 Apr;33(2):187-215.
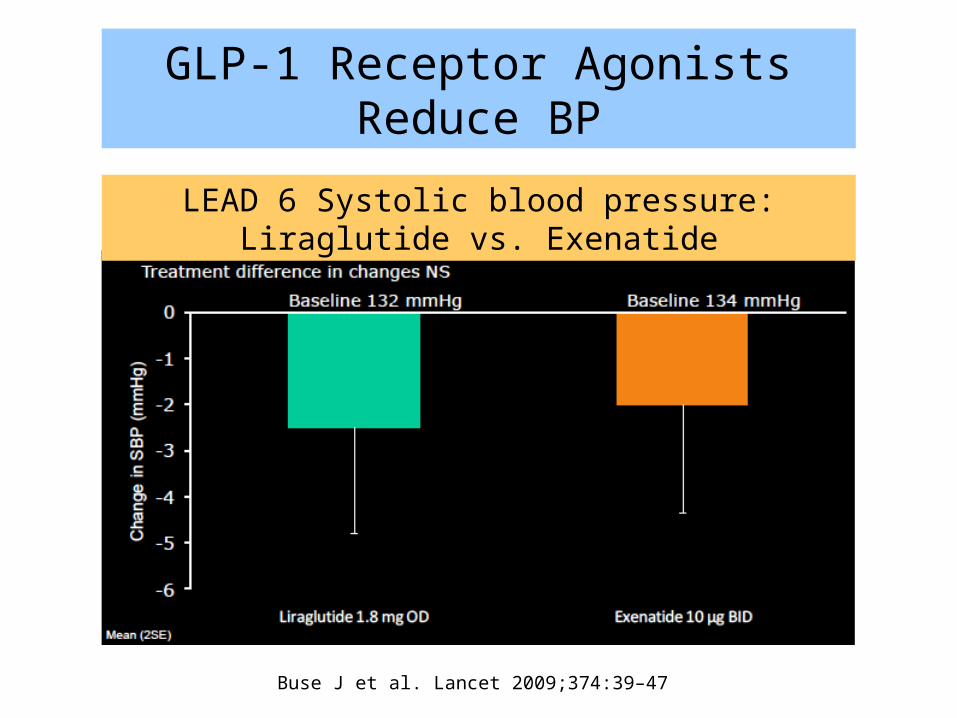
GLP-1 Receptor Agonists Reduce BP
LEAD 6 Systolic blood pressure: Liraglutide vs. Exenatide
Buse J et al. Lancet 2009;374:39–47
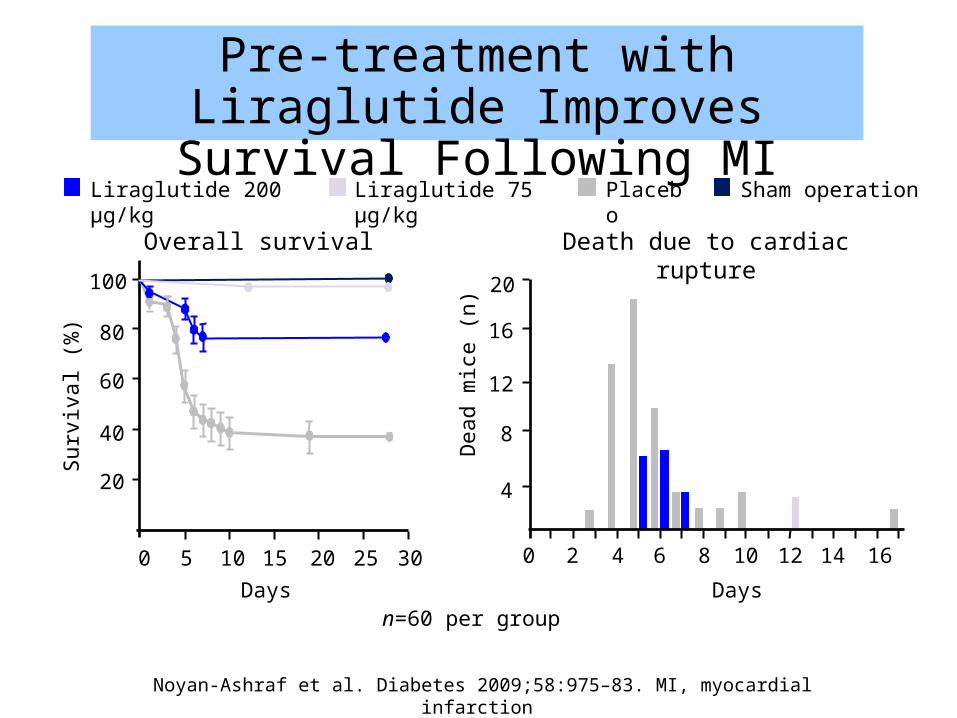
n=60 per group
Liraglutide 200 µg/kg Placebo Sham operation
50 10 15 20 25 30
20
40
60
80
100
Surv
ival
(%)
20 4 6 8 10 12 14 16
DaysDays
Overall survival Death due to cardiac rupture
4
8
12
16
20
Dea
d m
ice
(n)
Liraglutide 75 µg/kg
Pre-treatment with Liraglutide Improves Survival Following MI
Noyan-Ashraf et al. Diabetes 2009;58:975–83. MI, myocardial infarction
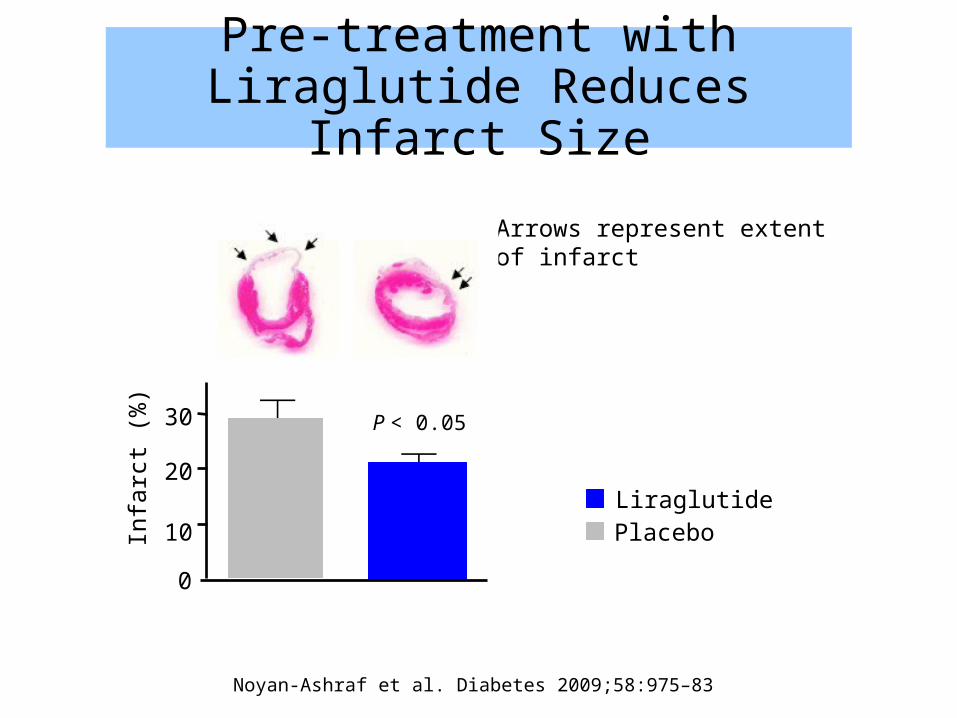
Liraglutide Placebo
Arrows represent extent of infarct
Pre-treatment with Liraglutide Reduces Infarct Size
Noyan-Ashraf et al. Diabetes 2009;58:975–83
Infa
rct (
%)
0
10
20
30 P < 0.05
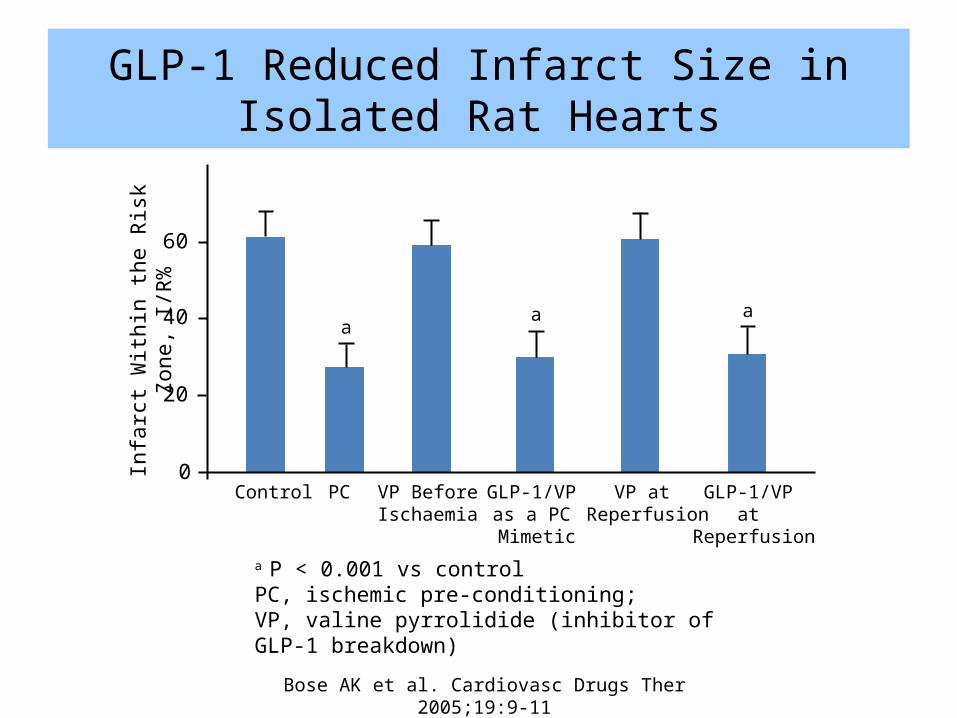
GLP-1 Reduced Infarct Size in Isolated Rat Hearts
44
a P < 0.001 vs control PC, ischemic pre-conditioning; VP, valine pyrrolidide (inhibitor of GLP-1 breakdown)
Infa
rct W
ithin
the
Risk
Zon
e, I/
R%
0
20
40
60
Control PC VP Before Ischaemia
GLP-1/VP as a PC Mimetic
VP at Reperfusion
a
GLP-1/VP at
Reperfusion
a a
Bose AK et al. Cardiovasc Drugs Ther 2005;19:9-11
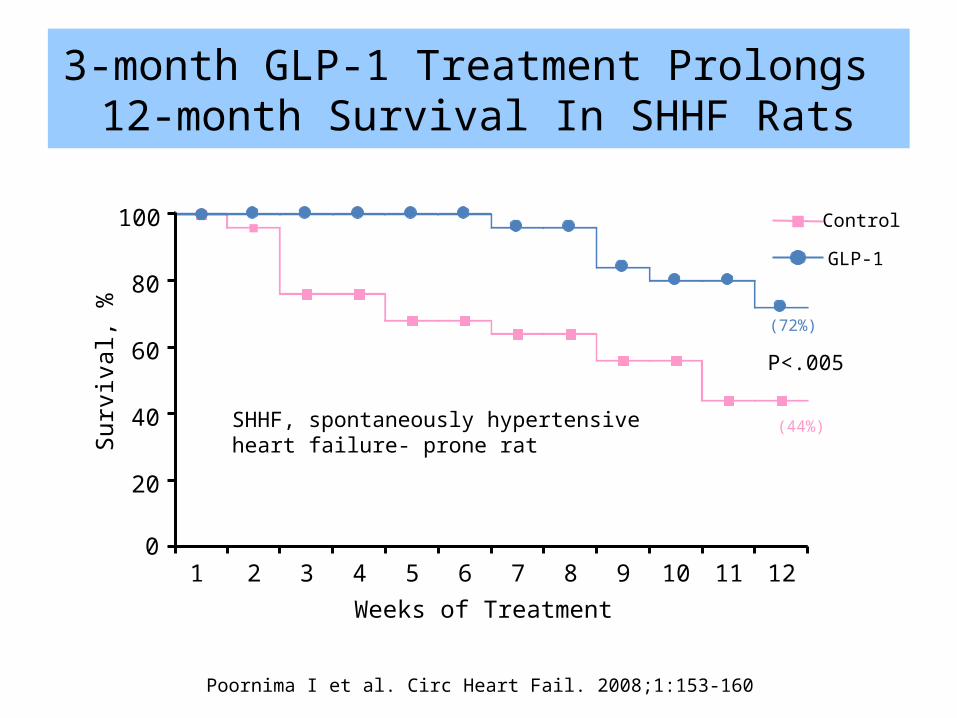
3-month GLP-1 Treatment Prolongs 12-month Survival In SHHF Rats
Poornima I et al. Circ Heart Fail. 2008;1:153-160
Weeks of Treatment1 2 3 4 5 6 7 8 9 10 11 12
0
20
40
60
80
100
P<.005
(72%)
(44%)
Surv
ival
, %
Control
GLP-1
SHHF, spontaneously hypertensive heart failure- prone rat
45
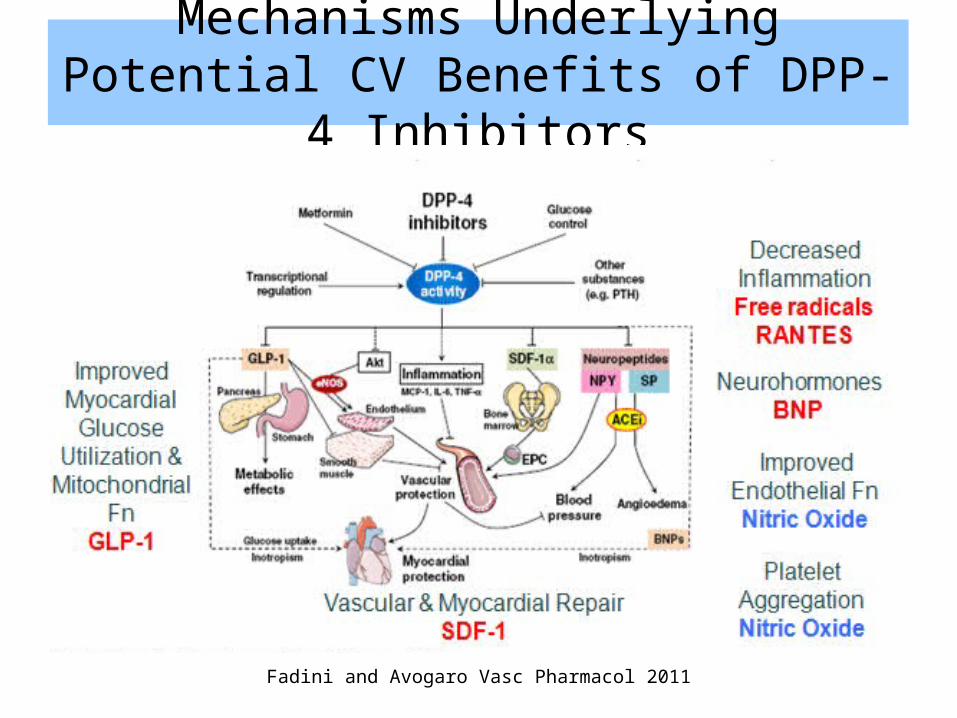
Mechanisms Underlying Potential CV Benefits of DPP-4 Inhibitors
Fadini and Avogaro Vasc Pharmacol 2011
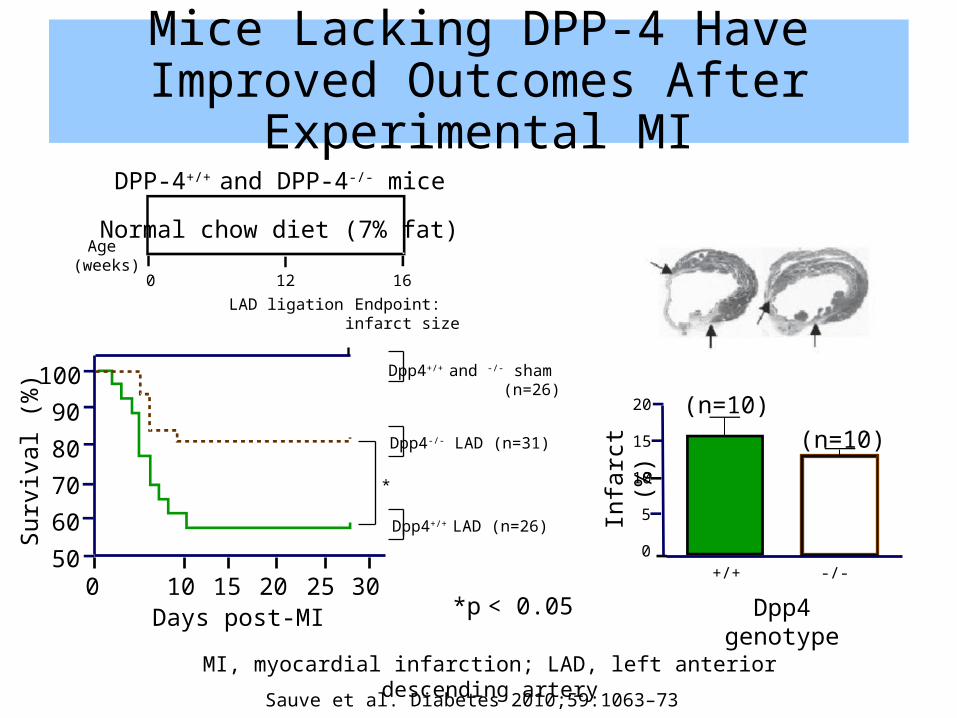
Mice Lacking DPP-4 Have Improved Outcomes After Experimental MI
Sauve et al. Diabetes 2010;59:1063–73
*
0 10 15 20 25 30Days post-MI
60
100
90
80
70
Surv
ival
(%)
50
Dpp4+/+ and -/- sham (n=26)
Dpp4-/- LAD (n=31)
Dpp4+/+ LAD (n=26)
DPP-4+/+ and DPP-4-/- mice
Normal chow diet (7% fat)
0 12 16
Age (weeks)
LAD ligation Endpoint: infarct size
5
20
15
10
Infa
rct (
%)
0
(n=10)(n=10)
Dpp4 genotype
+/+ -/-
*p < 0.05
MI, myocardial infarction; LAD, left anterior descending artery
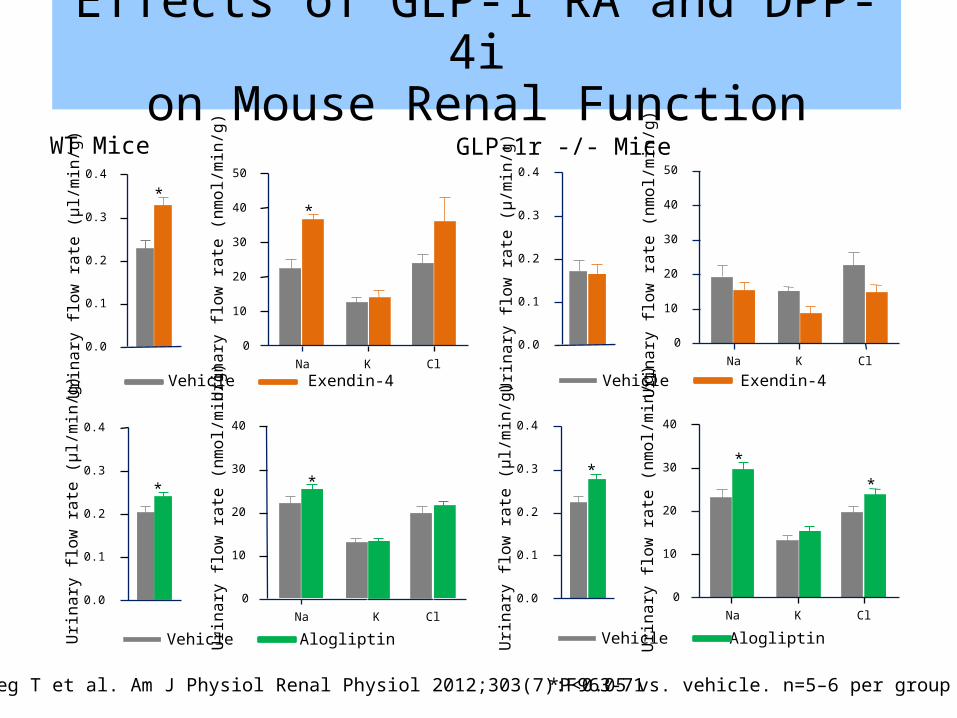
Rieg T et al. Am J Physiol Renal Physiol 2012;303(7):F963-71 *P<0.05 vs. vehicle. n=5–6 per group
0.0
0.1
0.2
0.3
0.4
WT Mice
Urin
ary
flow
rate
(µl/
min
/g)
*
0
10
20
30
50
Urin
ary
flow
rate
(nm
ol/m
in/g
)40
Na K Cl
*
Vehicle Exendin-4
0.0
0.1
0.2
0.3
0.4
GLP-1r -/- Mice
Urin
ary
flow
rate
(µ/m
in/g
)
0
10
20
30
50
Urin
ary
flow
rate
(nm
ol/m
in/g
)
40
Na K Cl
Vehicle Exendin-4
0.0
0.1
0.2
0.3
0.4
Urin
ary
flow
rate
(µl/
min
/g)
*
0
10
20
30
40
Urin
ary
flow
rate
(nm
ol/m
in/g
)
Na K Cl
*
*
Vehicle Alogliptin
0.0
0.1
0.2
0.3
0.4
Urin
ary
flow
rate
(µl/
min
/g)
*
0
10
20
30
40
Urin
ary
flow
rate
(nm
ol/m
in/g
)
Na K Cl
*
Vehicle Alogliptin
Effects of GLP-1 RA and DPP-4ion Mouse Renal Function
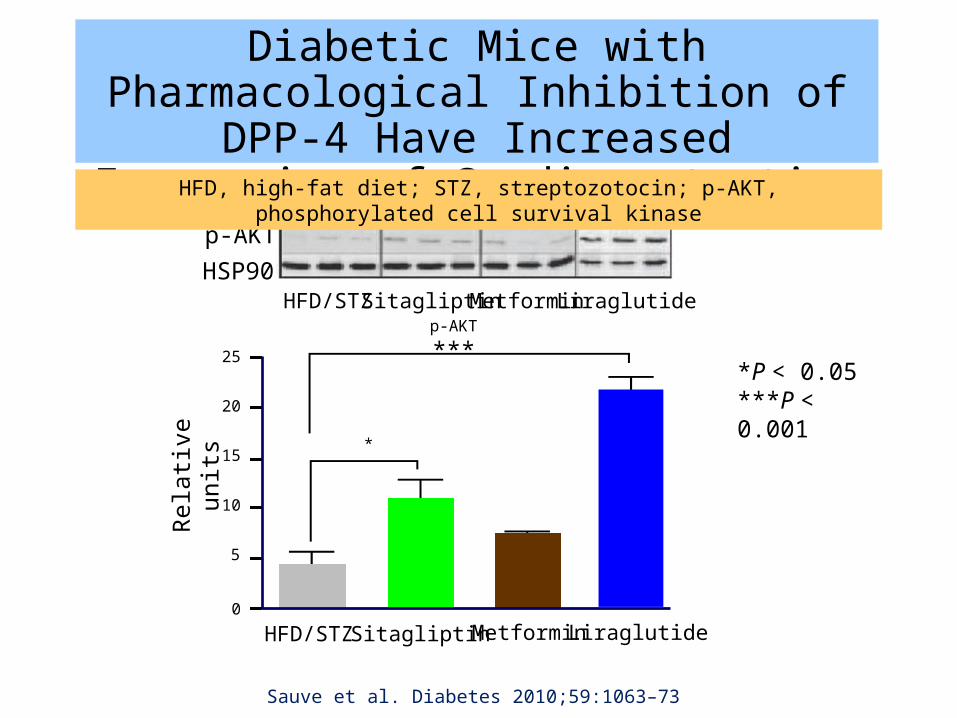
Diabetic Mice with Pharmacological Inhibition of DPP-4 Have Increased
Expression of Cardioprotective Proteins
Sauve et al. Diabetes 2010;59:1063–73
0
Rela
tive
units
HFD/STZ Sitagliptin Metformin Liraglutide
HFD/STZ Sitagliptin Metformin Liraglutide
p-AKTHSP90
p-AKT
***
25
15
10
5
*
20
*P < 0.05 ***P < 0.001
HFD, high-fat diet; STZ, streptozotocin; p-AKT, phosphorylated cell survival kinase
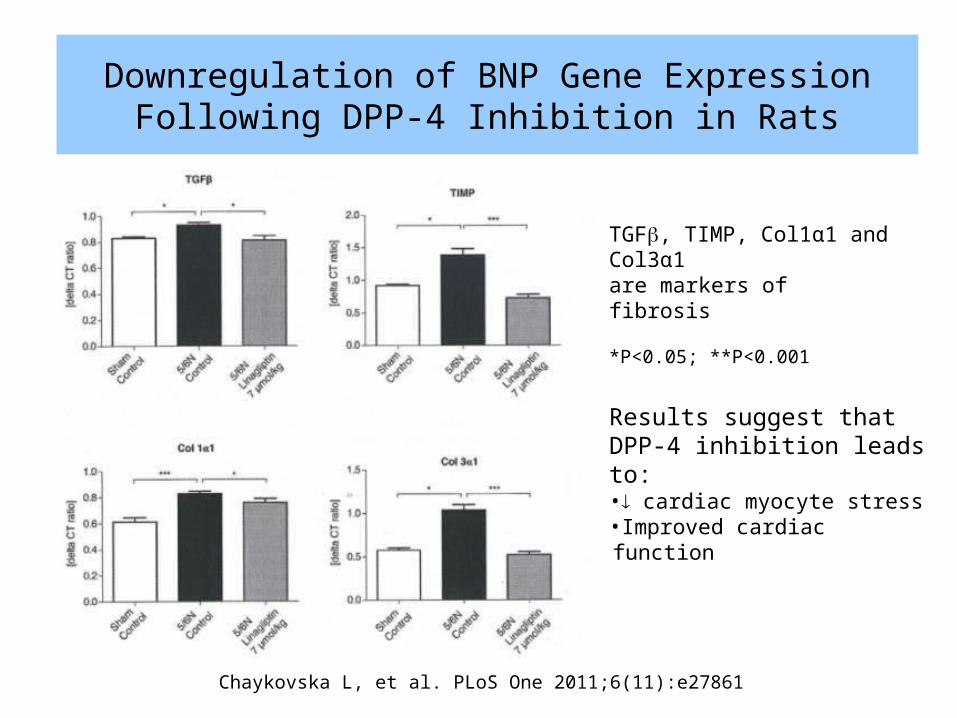
Downregulation of BNP Gene Expression Following DPP-4 Inhibition in Rats
50Chaykovska L, et al. PLoS One 2011;6(11):e27861
Results suggest that DPP-4 inhibition leads to:• cardiac myocyte stress•Improved cardiac function
TGFb, TIMP, Col1α1 and Col3α1 are markers of fibrosis
*P<0.05; **P<0.001
Effects of DM2 on Endothelial Progenitor Cells (EPCs)
• The quantity and function of EPCs are diminished in patients with type 2 diabetes 1,2
EPCs play an important role in cardiac tissue repair following ischemic events 3
• Preclinical data in animals show the homing of EPCs to sites of vascular injury is impaired in diabetes 4
• In patients with ischemic heart disease, there are a decreased number of bone marrow-derived circulating progenitor cells with further reductions in those with diabetes 5
51
1. Hill JM, et al. N Engl J Med 2003;348:593-6002. Tepper OM, et al. Circulation 2002;106(22):2781-278663. Zaruba M-M, et al. Cell Stem Cell 2009;4:313-3234. Li M, et al. Circ Res. 2006 Mar 17;98:697-704 5. Bozdag-Turan I, et al. Cardiovasc Diabetol 2011;10(1):107
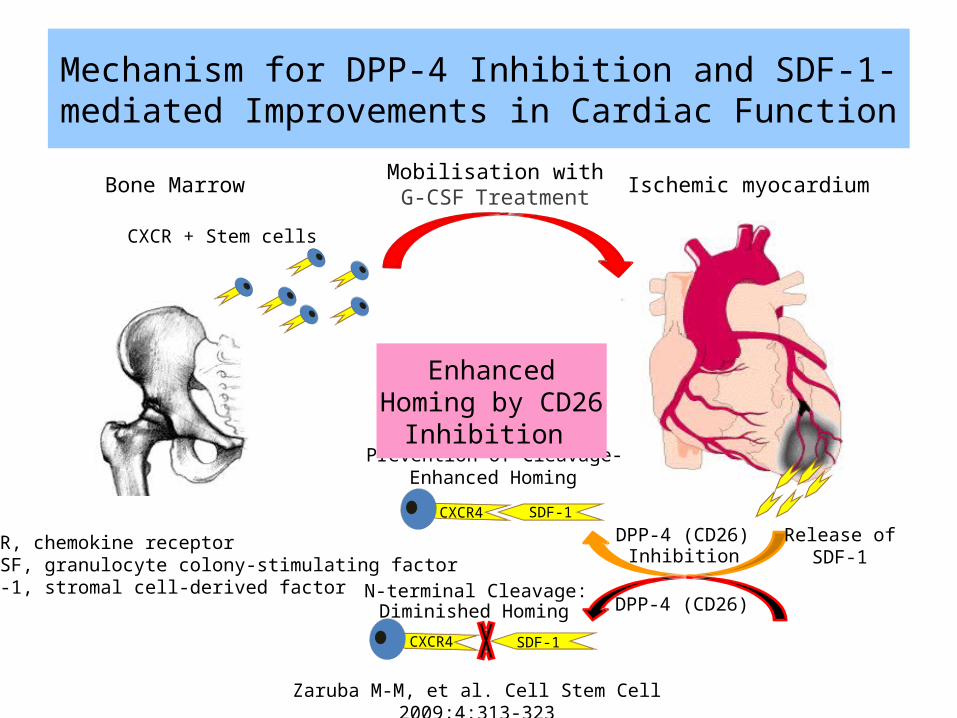
Mobilisation withG-CSF Treatment Ischemic myocardiumBone Marrow
Release ofSDF-1
CXCR + Stem cells
SDF-1CXCR4
DPP-4 (CD26)N-terminal Cleavage:Diminished Homing
DPP-4 (CD26)Inhibition
SDF-1CXCR4
Prevention of Cleavage-Enhanced Homing
Enhanced Homing by CD26 Inhibition
CXCR, chemokine receptor G-CSF, granulocyte colony-stimulating factorSDF-1, stromal cell-derived factor
52
Mechanism for DPP-4 Inhibition and SDF-1-mediated Improvements in Cardiac Function
Zaruba M-M, et al. Cell Stem Cell 2009;4:313-323
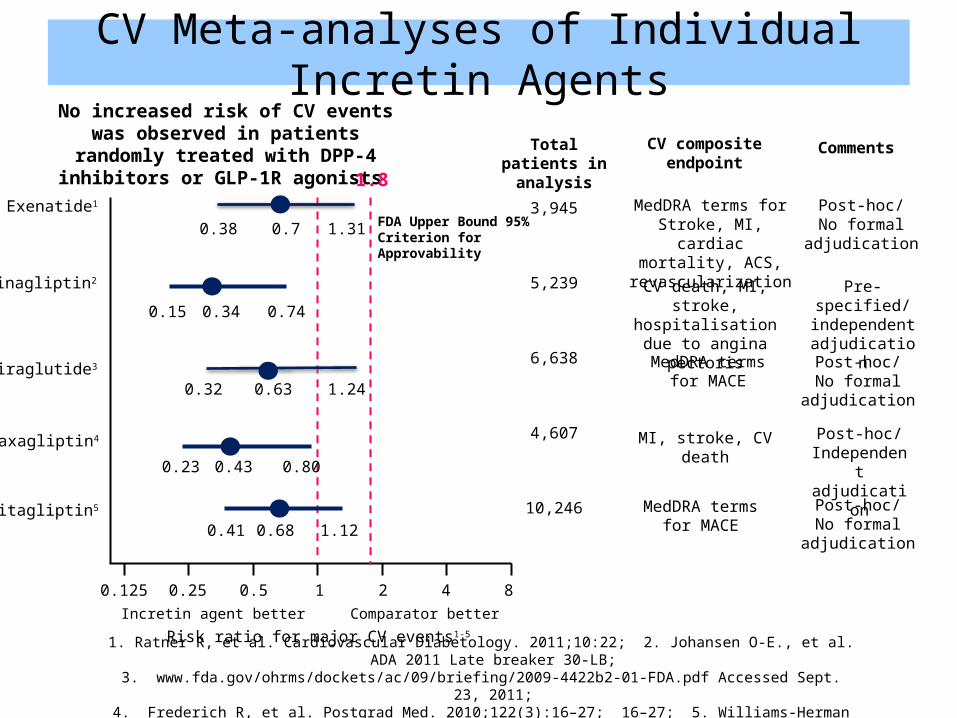
Risk ratio for major CV events1-5
1. Ratner R, et al. Cardiovascular Diabetology. 2011;10:22; 2. Johansen O-E., et al. ADA 2011 Late breaker 30-LB;3. www.fda.gov/ohrms/dockets/ac/09/briefing/2009-4422b2-01-FDA.pdf Accessed Sept. 23, 2011;
4. Frederich R, et al. Postgrad Med. 2010;122(3):16–27; 16–27; 5. Williams-Herman D, et al. BMC Endocr Disord. 2010;10:7
Total patients in analysis
CV compositeendpoint
Comments
Incretin agent better Comparator better
10.50.250.125 2 4 8
MedDRA termsfor MACE
Post-hoc/No formal
adjudication
Sitagliptin5
0.680.41 1.12
MI, stroke, CV death Post-hoc/Independent adjudication
Saxagliptin4
0.430.23 0.80
No increased risk of CV events was observed in patients randomly treated with DPP-4
inhibitors or GLP-1R agonists
Exenatide1
0.70.38 1.31MedDRA terms for Stroke, MI, cardiac mortality, ACS,
revascularization
Post-hoc/No formal
adjudication
1.8
Liraglutide3
0.630.32 1.24
Post-hoc/No formal
adjudication
MedDRA termsfor MACE
CV death, MI, stroke,hospitalisation due to
angina pectoris
Pre-specified/independent adjudication
0.15 0.74
Linagliptin2
0.34
3,945
5,239
6,638
4,607
10,246
FDA Upper Bound 95%Criterion for Approvability
CV Meta-analyses of Individual Incretin Agents
1. Golden SH. Am J Cardiol 2011;108 (Suppl):59B-67B2. Fonseca V. Am J Cardiol 2011;108 (supp):52B–58Bl
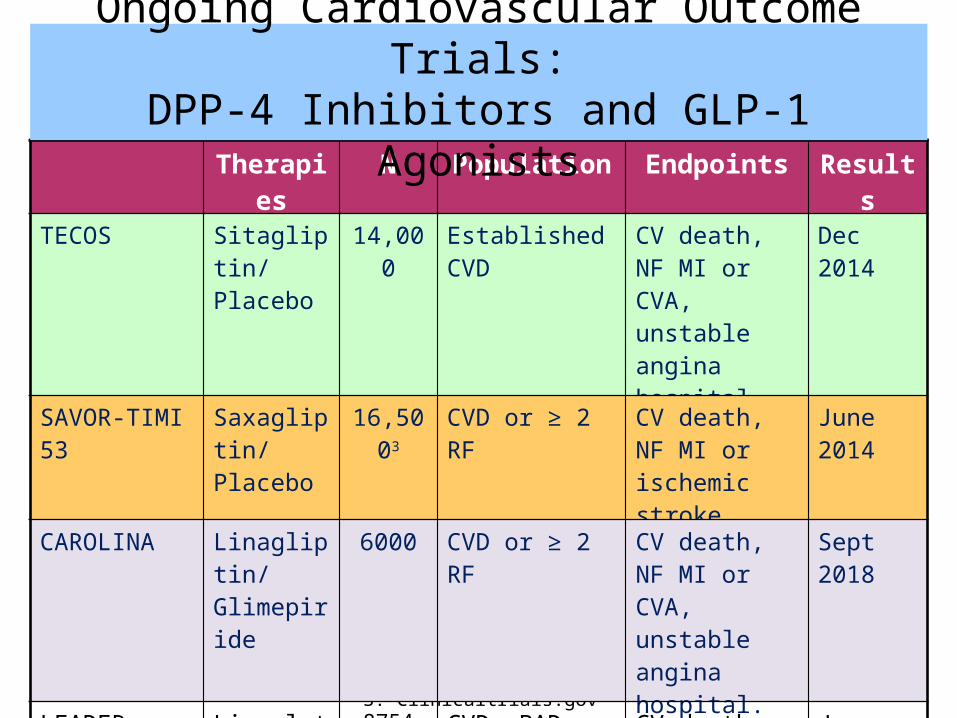
3. Clinicaltrials.gov
Therapies N Population Endpoints Results
TECOS Sitagliptin/ Placebo
14,000 Established CVD CV death, NF MI or CVA, unstable angina hospital.
Dec 2014
SAVOR-TIMI 53 Saxagliptin/ Placebo
16,5003 CVD or ≥ 2 RF CV death, NF MI or ischemic stroke
June 2014
CAROLINA Linagliptin/ Glimepiride
6000 CVD or ≥ 2 RF CV death, NF MI or CVA, unstable angina hospital.
Sept 2018
LEADER Liraglutide/ Placebo
8754 CVD, PAD, CKD, CHF or RF if >60yrs
CV death, NF MI or stroke, revasc
Jan 2016
EXSCEL Exenatide LAR/Placebo
9500 Not specified CV death, NF MI or stroke
Mar 2017
Ongoing Cardiovascular Outcome Trials:DPP-4 Inhibitors and GLP-1 Agonists
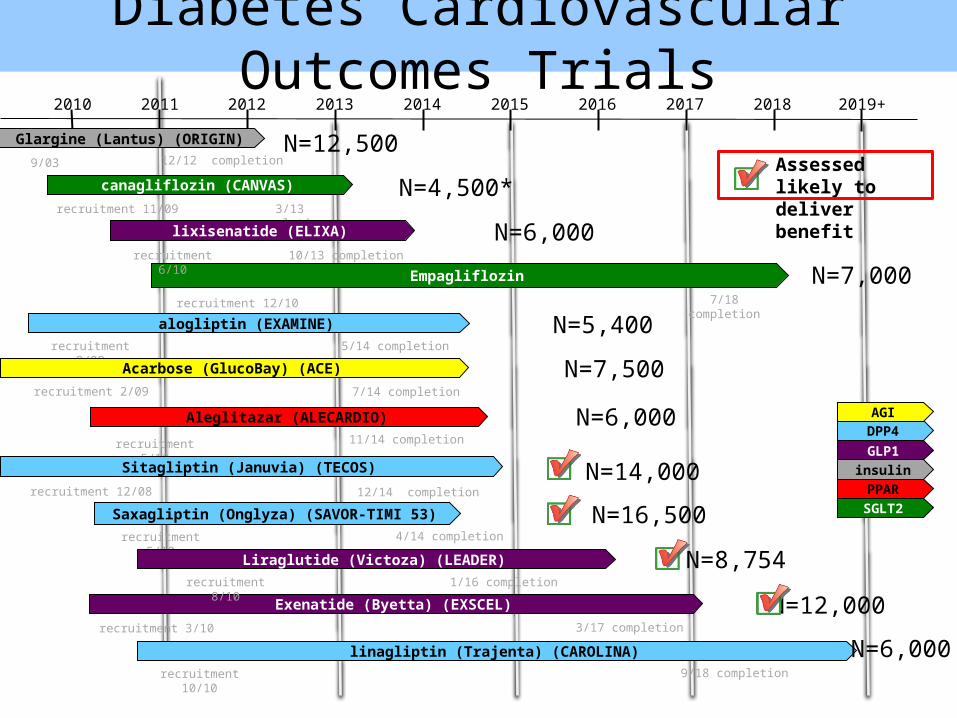
Diabetes Cardiovascular Outcomes Trials2010 2011 2012 2013 2014 2015 2016 2017 2018 2019+
recruitment 11/09
canagliflozin (CANVAS)
3/13 completion
recruitment 9/09
alogliptin (EXAMINE)5/14 completion
recruitment 5/10
Aleglitazar (ALECARDIO)11/14 completion
9/03
Glargine (Lantus) (ORIGIN)12/12 completion
7/14 completion
Acarbose (GlucoBay) (ACE) recruitment 2/09
recruitment 5/10
Saxagliptin (Onglyza) (SAVOR-TIMI 53)4/14 completion
insulin
SGLT2
GLP1DPP4AGI
PPAR
recruitment 3/10
Exenatide (Byetta) (EXSCEL)3/17 completion
recruitment 12/08
Sitagliptin (Januvia) (TECOS)
12/14 completion
Empagliflozin
recruitment 12/10 7/18 completion
1/16 completionrecruitment 8/10
Liraglutide (Victoza) (LEADER)
10/13 completionrecruitment 6/10
lixisenatide (ELIXA)
recruitment 10/10
linagliptin (Trajenta) (CAROLINA)9/18 completion
N=12,500
N=4,500*
N=6,000
N=7,000
N=5,400
N=7,500
N=6,000
N=14,000
N=16,500
N=8,754
N=12,000
N=6,000
Assessed likely to deliver benefit
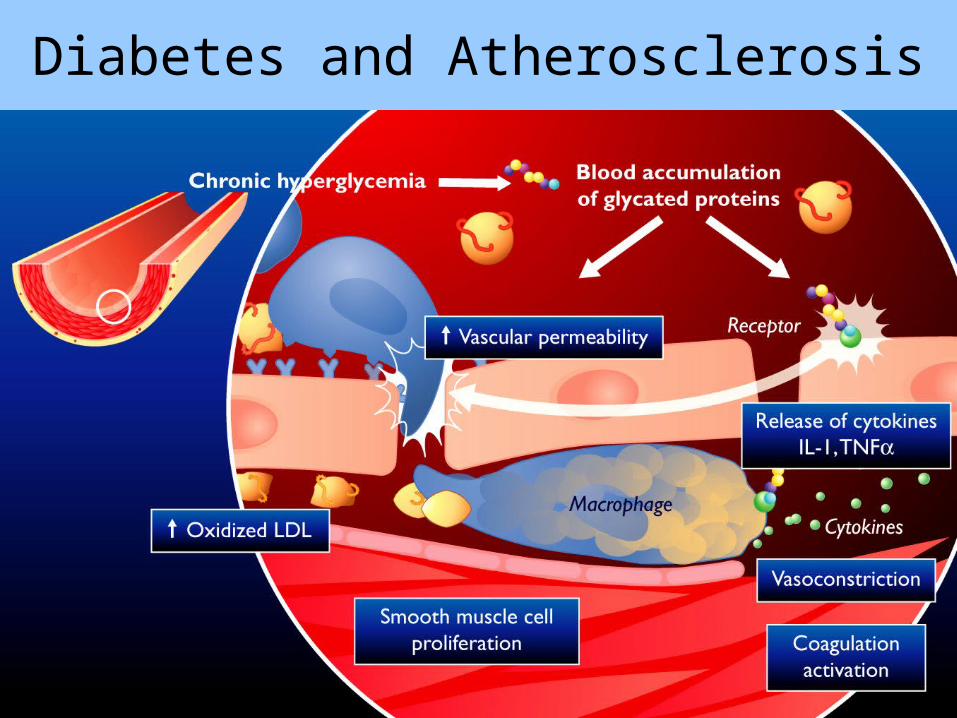
Diabetes and Atherosclerosis
CVD Management in Diabetes
Benefits of multiple CVD risk factor management on CVD outcomes
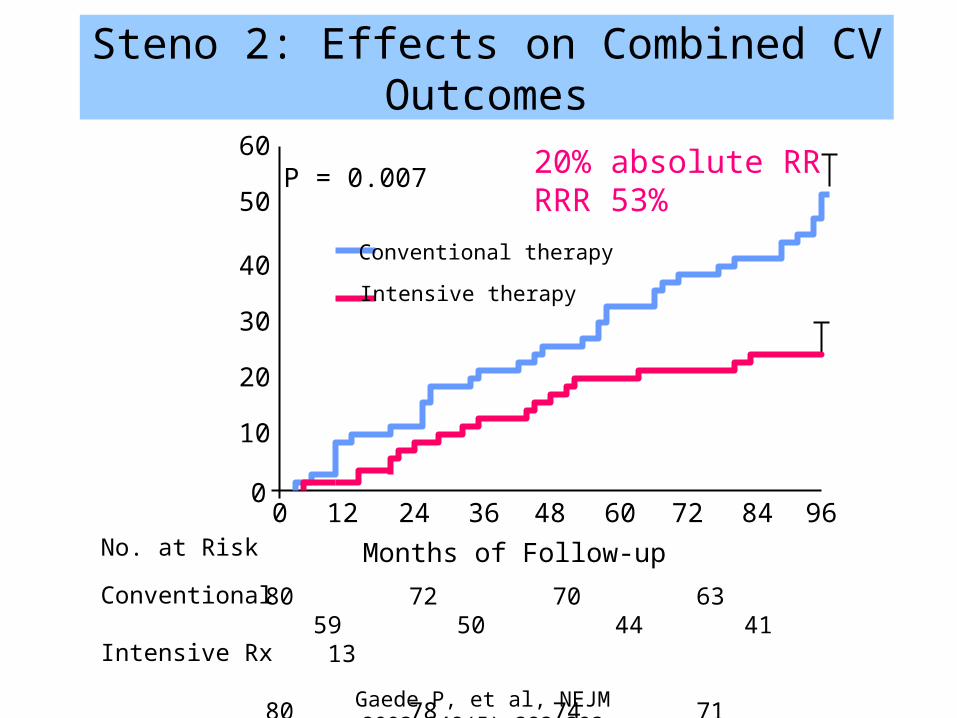
Steno 2: Effects on Combined CV Outcomes
Gaede P, et al, NEJM 2003;348(5):383-393
0 12 24 36 48 60 72 84 960
10
20
30
40
50
60P = 0.007
Conventional therapy
Intensive therapy
Months of Follow-up
80 72 70 63 59 50 44 41 13
80 78 74 71 66 63 61 59 19
No. at Risk
Conventional
Intensive Rx
20% absolute RRRRR 53%
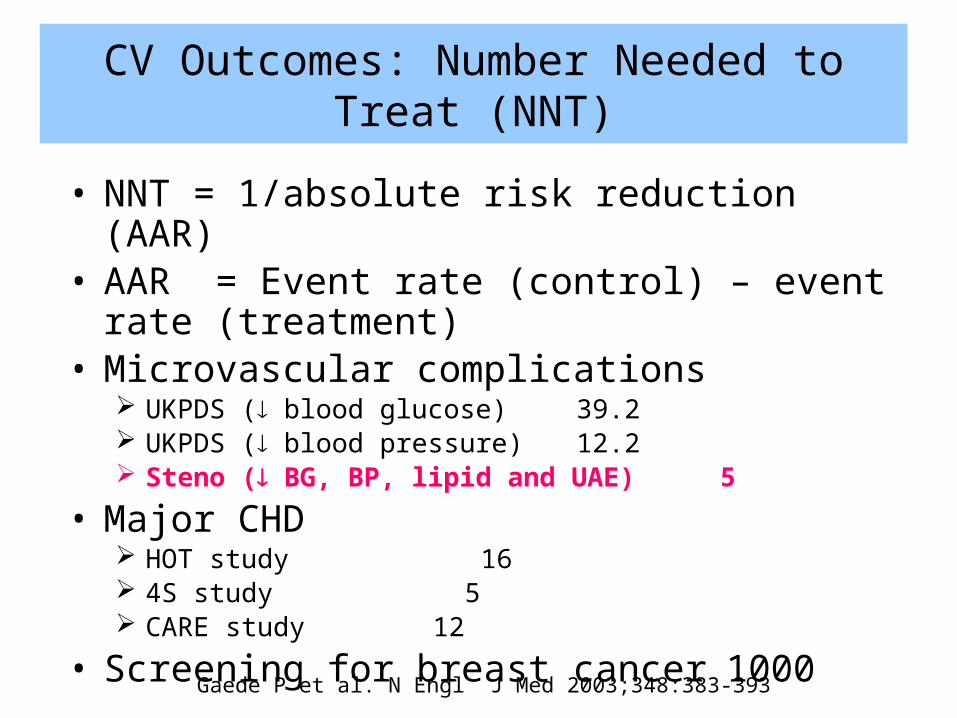
CV Outcomes: Number Needed to Treat (NNT)
• NNT = 1/absolute risk reduction (AAR)• AAR = Event rate (control) – event rate (treatment)• Microvascular complications
UKPDS ( blood glucose) 39.2 UKPDS ( blood pressure) 12.2 Steno ( BG, BP, lipid and UAE) 5
• Major CHD HOT study 16 4S study 5 CARE study 12
• Screening for breast cancer 1000
Gaede P et al. N Engl J Med 2003;348:383-393
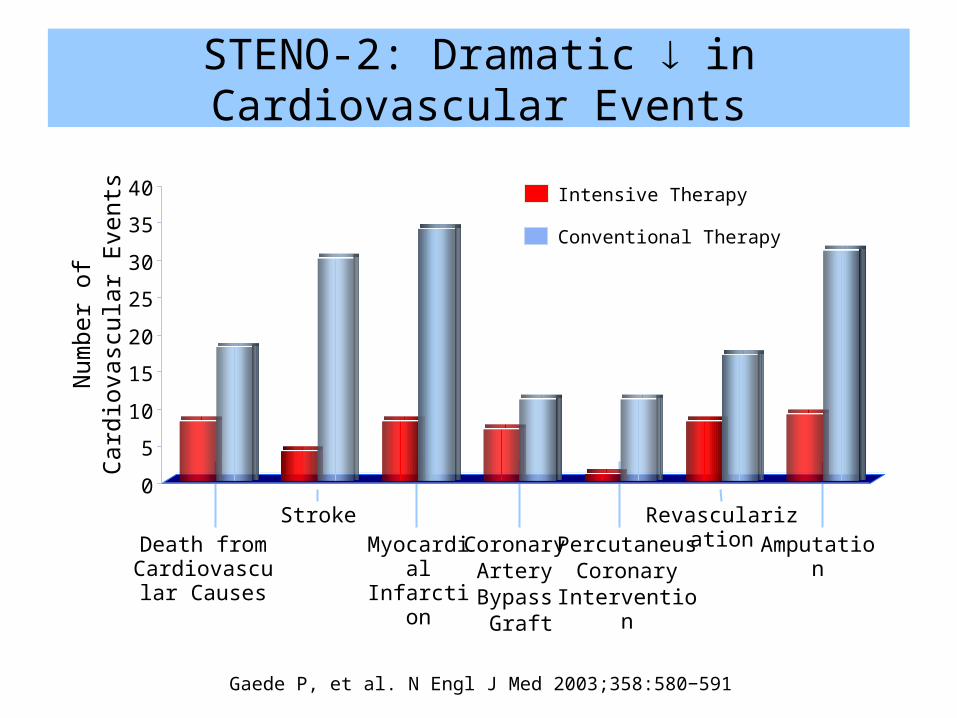
Intensive Therapy
Conventional Therapy
Num
ber o
f Car
diov
ascu
lar E
vent
s
AmputationRevascularization
PercutaneusCoronary
Intervention
Myocardial Infarction
StrokeDeath from
Cardiovascular Causes
Coronary Artery Bypass
Graft
Gaede P, et al. N Engl J Med 2003;358:580−591
0
5
10
15
20
25
30
35
40
STENO-2: Dramatic in Cardiovascular Events
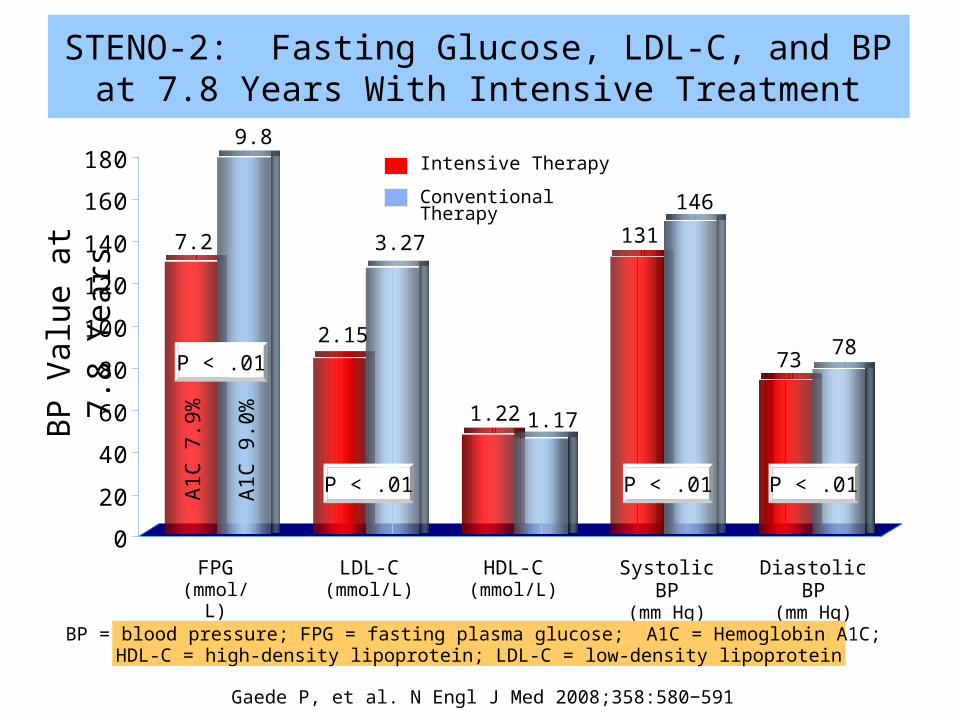
0
20
40
60
80
100
120
140
160
180 Intensive Therapy
Conventional Therapy
BP V
alue
at 7
.8 Y
ears
FPG(mmol/L)
LDL-C(mmol/L)
HDL-C(mmol/L)
Systolic BP(mm Hg)
Diastolic BP(mm Hg)
7.2
9.8
2.15
3.27
1.22 1.17
131
146
73 78
A1C
7.9%
A1C
9.0%
P < .01
P < .01
P < .01 P < .01
Gaede P, et al. N Engl J Med 2008;358:580−591
BP = blood pressure; FPG = fasting plasma glucose; A1C = Hemoglobin A1C; HDL-C = high-density lipoprotein; LDL-C = low-density lipoprotein
STENO-2: Fasting Glucose, LDL-C, and BP at 7.8 Years With Intensive Treatment
Gaede P, et al. N Engl J Med 2008;358:580-591
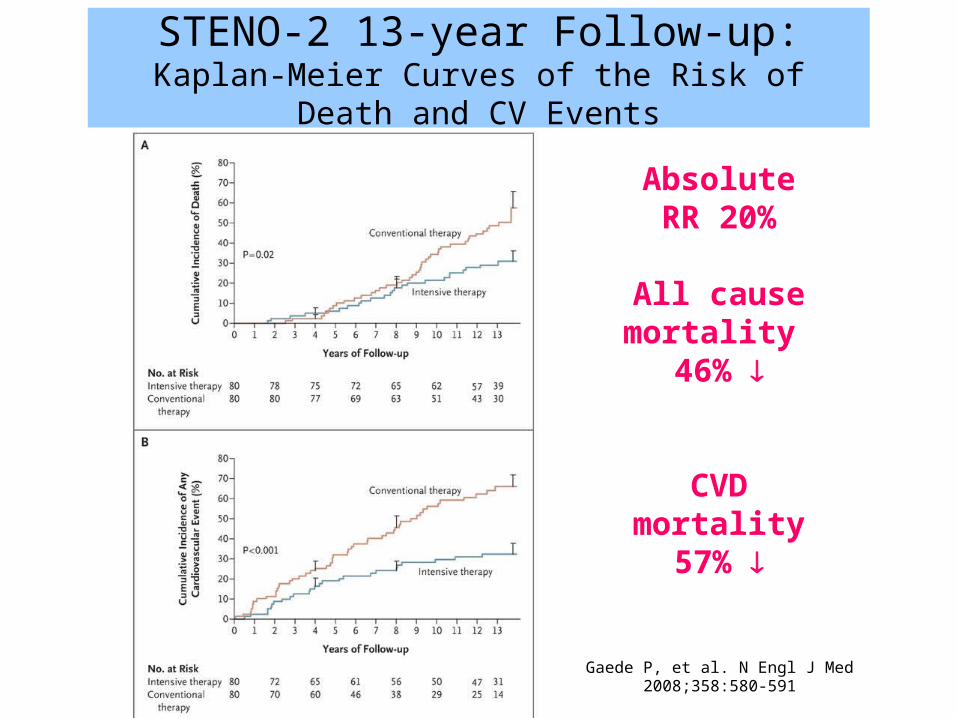
STENO-2 13-year Follow-up:Kaplan-Meier Curves of the Risk of Death and CV Events
Absolute RR 20%
All causemortality
46%
CVDmortality
57%
Global CVD Risk Reduction in Diabetes
CVD risk estimates in diabetes should be patient-centred and not disease-based:1. Identify individual CVD risk factors 2. Consider all risk factors in estimating particular
patient’s CVD risk3. Appropriate therapies should be evidence-based4. Integrate all therapies to optimize best
management for global CVD risk reduction
Gerstein HC Diabetologia 2011;54:230–232
Guidelines on Vascular Protection: Summary of Diabetes Management
• Achieve healthy weight and exercise regularly• Treat to glycemic target
BG 4-10 mmol/L A1C ≤ 7%, ≤ 6.5% to reduce nephropathy in DM2 Regular surveillance for complications
• Treat lipid and BP to goal targets: LDL-C ≤ 2.0 mmol/L or 50% reduction, or ApoB < 0.8g/L TC/HDL-C ratio < 4 BP < 130/80 mmHg
• ACE inhibition (ACEi or ARB) for vascular protection• ECASA in patients with stable CAD• Smoking cessation and moderate alcohol intake
Can J Diabetes 2008;32(Suppl 1):S102-S118
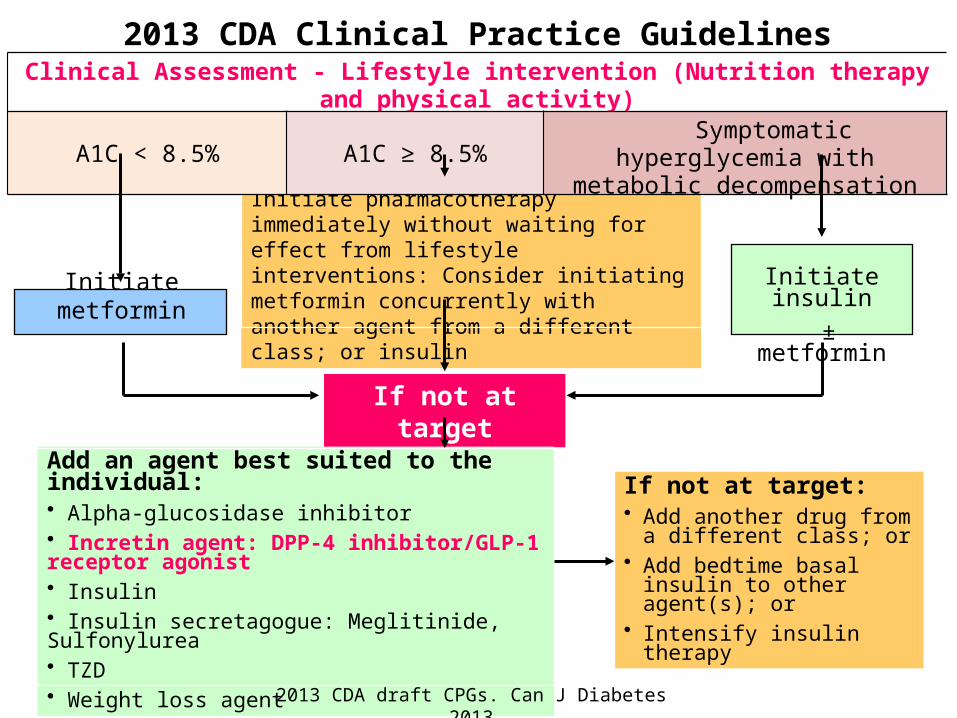
Initiate metformin
Initiate pharmacotherapy immediately without waiting for effect from lifestyle interventions: Consider initiating metformin concurrently with another agent from a different class; or insulin Initiate insulin
± metformin
If not at target
Add an agent best suited to the individual:• Alpha-glucosidase inhibitor• Incretin agent: DPP-4 inhibitor/GLP-1 receptor agonist• Insulin• Insulin secretagogue: Meglitinide, Sulfonylurea• TZD• Weight loss agent
If not at target:• Add another drug from a
different class; or • Add bedtime basal insulin to
other agent(s); or • Intensify insulin therapy
2013 CDA Clinical Practice GuidelinesClinical Assessment - Lifestyle intervention (Nutrition therapy and physical activity)
A1C < 8.5% A1C ≥ 8.5% Symptomatic hyperglycemia with metabolic decompensation
2013 CDA draft CPGs. Can J Diabetes 2013
Summary
• Glycemic control reduces macro- and microvascular complications of both type 1 and type 2 diabetes
• In choosing antihyperglycemic agents, select drugs that do not cause hypoglycemia, as severe hypoglycemia is associated with adverse CV outcomes
• Metformin and incretins (DPP-4 inhibitors and GLP-1 receptor agonists) are associated with lower CV risk
• Sulfonylureas and TZDs are associated with increased CV risk
• Definitive CV effects of antihyperglycemic agents in DM2 will await the results of ongoing CV trials
“Superior Doctors Prevent the Disease.Mediocre Doctors Treat the Disease Before Evident.
Inferior Doctors Treat the Full Blown Disease.”
Huang Dee, 2600 B.C. In Nai Ching, 1st Chinese Medical Text
Thank you
Questions?