Embed Size (px)
Citation preview
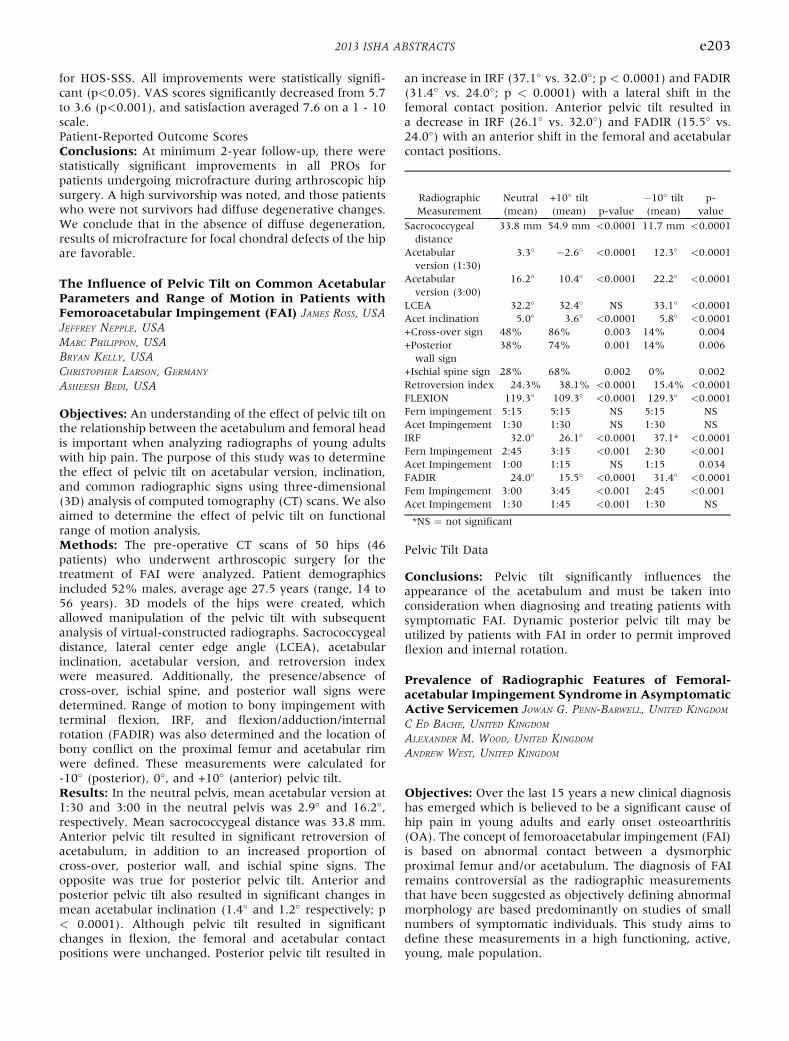
RadiographicMeasurement
Neutral(mean)
+10� tilt(mean) p-value
�10� tilt(mean)
p-value
Sacrococcygealdistance
33.8 mm 54.9 mm <0.0001 11.7 mm <0.0001
Acetabularversion (1:30)
3.3� �2.6� <0.0001 12.3� <0.0001
Acetabularversion (3:00)
16.2� 10.4� <0.0001 22.2� <0.0001
LCEA 32.2� 32.4� NS 33.1� <0.0001Acet inclination 5.0� 3.6� <0.0001 5.8� <0.0001+Cross-over sign 48% 86% 0.003 14% 0.004+Posteriorwall sign
38% 74% 0.001 14% 0.006
+Ischial spine sign 28% 68% 0.002 0% 0.002Retroversion index 24.3% 38.1% <0.0001 15.4% <0.0001FLEXION 119.3� 109.3� <0.0001 129.3� <0.0001Fern impingement 5:15 5:15 NS 5:15 NSAcet Impingement 1:30 1:30 NS 1:30 NSIRF 32.0� 26.1� <0.0001 37.1* <0.0001Fern Impingement 2:45 3:15 <0.001 2:30 <0.001Acet Impingement 1:00 1:15 NS 1:15 0.034FADIR 24.0� 15.5� <0.0001 31.4� <0.0001Fem Impingement 3:00 3:45 <0.001 2:45 <0.001Acet Impingement 1:30 1:45 <0.001 1:30 NS
*NS ¼ not significant
2013 ISHA ABSTRACTS e203
for HOS-SSS. All improvements were statistically signifi-cant (p<0.05). VAS scores significantly decreased from 5.7to 3.6 (p<0.001), and satisfaction averaged 7.6 on a 1 - 10scale.Patient-Reported Outcome ScoresConclusions: At minimum 2-year follow-up, there werestatistically significant improvements in all PROs forpatients undergoing microfracture during arthroscopic hipsurgery. A high survivorship was noted, and those patientswho were not survivors had diffuse degenerative changes.We conclude that in the absence of diffuse degeneration,results of microfracture for focal chondral defects of the hipare favorable.
The Influence of Pelvic Tilt on Common AcetabularParameters and Range of Motion in Patients withFemoroacetabular Impingement (FAI) JAMES ROSS, USAJEFFREY NEPPLE, USAMARC PHILIPPON, USABRYAN KELLY, USACHRISTOPHER LARSON, GERMANY
ASHEESH BEDI, USA
Objectives: An understanding of the effect of pelvic tilt onthe relationship between the acetabulum and femoral headis important when analyzing radiographs of young adultswith hip pain. The purpose of this study was to determinethe effect of pelvic tilt on acetabular version, inclination,and common radiographic signs using three-dimensional(3D) analysis of computed tomography (CT) scans. We alsoaimed to determine the effect of pelvic tilt on functionalrange of motion analysis.Methods: The pre-operative CT scans of 50 hips (46patients) who underwent arthroscopic surgery for thetreatment of FAI were analyzed. Patient demographicsincluded 52% males, average age 27.5 years (range, 14 to56 years). 3D models of the hips were created, whichallowed manipulation of the pelvic tilt with subsequentanalysis of virtual-constructed radiographs. Sacrococcygealdistance, lateral center edge angle (LCEA), acetabularinclination, acetabular version, and retroversion indexwere measured. Additionally, the presence/absence ofcross-over, ischial spine, and posterior wall signs weredetermined. Range of motion to bony impingement withterminal flexion, IRF, and flexion/adduction/internalrotation (FADIR) was also determined and the location ofbony conflict on the proximal femur and acetabular rimwere defined. These measurements were calculated for-10� (posterior), 0�, and +10� (anterior) pelvic tilt.Results: In the neutral pelvis, mean acetabular version at1:30 and 3:00 in the neutral pelvis was 2.9� and 16.2�,respectively. Mean sacrococcygeal distance was 33.8 mm.Anterior pelvic tilt resulted in significant retroversion ofacetabulum, in addition to an increased proportion ofcross-over, posterior wall, and ischial spine signs. Theopposite was true for posterior pelvic tilt. Anterior andposterior pelvic tilt also resulted in significant changes inmean acetabular inclination (1.4� and 1.2� respectively; p< 0.0001). Although pelvic tilt resulted in significantchanges in flexion, the femoral and acetabular contactpositions were unchanged. Posterior pelvic tilt resulted in
an increase in IRF (37.1� vs. 32.0�; p < 0.0001) and FADIR(31.4� vs. 24.0�; p < 0.0001) with a lateral shift in thefemoral contact position. Anterior pelvic tilt resulted ina decrease in IRF (26.1� vs. 32.0�) and FADIR (15.5� vs.24.0�) with an anterior shift in the femoral and acetabularcontact positions.
Pelvic Tilt Data
Conclusions: Pelvic tilt significantly influences theappearance of the acetabulum and must be taken intoconsideration when diagnosing and treating patients withsymptomatic FAI. Dynamic posterior pelvic tilt may beutilized by patients with FAI in order to permit improvedflexion and internal rotation.
Prevalence of Radiographic Features of Femoral-acetabular Impingement Syndrome in AsymptomaticActive Servicemen JOWAN G. PENN-BARWELL, UNITED KINGDOM
C ED BACHE, UNITED KINGDOM
ALEXANDER M. WOOD, UNITED KINGDOM
ANDREW WEST, UNITED KINGDOM
Objectives: Over the last 15 years a new clinical diagnosishas emerged which is believed to be a significant cause ofhip pain in young adults and early onset osteoarthritis(OA). The concept of femoroacetabular impingement (FAI)is based on abnormal contact between a dysmorphicproximal femur and/or acetabulum. The diagnosis of FAIremains controversial as the radiographic measurementsthat have been suggested as objectively defining abnormalmorphology are based predominantly on studies of smallnumbers of symptomatic individuals. This study aims todefine these measurements in a high functioning, active,young, male population.




























![Femoroacetabular%20 impingement[1]](https://img.pdfslide.us/doc/110x75/54559a24af7959d8748b6a78/femoroacetabular20-impingement1.jpg)
