-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
The performance evaluation of novices:The importance of
competence in specificwork activity clusters
Eric Molleman* and Gerben S. van der VegtUniversity of
Groningen, The Netherlands
In this study, we examine the relationships between newcomers
competence in specificwork activity clusters and the evaluation of
their performance. Longitudinal data weregathered on 92 novice
nurses from themselves and from the senior staff at three
stages:before entering the job, 6 weeks after entry and 18 months
after entry. Results showedthat, after entry, a newcomers
competence in the cluster of care activities contributedmore to a
positive performance evaluation than competence in the cluster of
non-careactivities. Competence in the non-care cluster was only
found to contribute to apositive performance evaluation, if the
newcomer also showed competence in the carecluster. Moreover,
novices showed a greater improvement in their care competencethan
their non-care competence during the first 18 months of
socialization. Finally, wefound that after 18 months competence in
the non-care cluster contributes more to apositive performance
evaluation than competence in the care cluster.
Over recent decades, an extensive body of research has been
published documenting
the factors that affect the performance of newcomers. These
factors include, for
example, recruitment practices, mentoring programmes, newcomer
values, demo-graphic characteristics and personality traits (for
overviews, see Bauer, Morrison, &
Callister, 1998; Fisher, 1986; Moreland & Levine, 2001; Saks
& Ashforth, 1997; Wanous,
Poland, Premack, & Davis, 1992). A factor that plays an
important role in the evaluation
of the overall performance of newcomers is their competence
(see, for example, Blau,
1999; Haueter, Macan, & Winter, 2003). This is perhaps not
surprising given that most
studies that consider the functioning of newcomers involve some
discussion on the
extent to which individuals have learned the tasks that are part
of the job (Dubinsky,
Howell, Ingram, & Bellenger, 1986; Feldman, 1976; Fisher,
1986; Louis, 1980; VanMaanen, 1976; Van Maanen & Schein,
1979).
Competence refers to an individuals knowledge, skills and
abilities with respect to
the work activities that have to be conducted in the full range
of situations associated
with their position (Campion, Mumford, Morgeson, & Nahrgang,
2005; Cunningham,
* Correspondence should be addressed to Professor Eric Molleman,
Faculty of Management and Organization, PO, Box 800,9700 AV
Groningen, The Netherlands (e-mail: [email protected]).
TheBritishPsychologicalSociety
459
Journal of Occupational and Organizational Psychology (2007),
80, 459478
q 2007 The British Psychological Society
www.bpsjournals.co.uk
DOI:10.1348/096317906X154469
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
1996). Depending on the occupational group under consideration,
these work activities
are usually grouped into clusters (Campion et al., 2005). Work
activity clusters provide a
unit of analysis that can precisely describe the prerequisites
for high performance in a
specific job, while remaining manageable in terms of the total
number of units necessary
to describe them. For example, for an academic, competence in
the teaching work
activity cluster might include didactic skills, the ability to
provide feedback andknowledge of ones own field, while competence
in the research work activity cluster
will include knowledge of research methodology, and statistical
and writing skills.
To date, most studies in the literature on newcomers have
examined the effects of
overall or general competence on such outcomes as stress, job
satisfaction,
organizational commitment and performance (see, for example,
Blau, 1999; Haueter
et al., 2003). Few studies have examined whether and how a
newcomers competence
in more specific work activity clusters is related to the
evaluation of their overall job
performance. Indeed, past research has ignored the fact that
most jobs requirecompetence in a mixture of different work activity
clusters, and that competence in
certain clusters may be more important in receiving a positive
overall performance
evaluation than competence in others.
Moreover, most previous studies have not done justice to the
complexity and the
dynamics of the relationship between newcomers competence in
specific work activity
clusters and the evaluation of their overall performance. That
is, most studies have
overlooked the possibility that the importance or relevance of
some of these clusters for
positive overall job performance evaluations may depend on how
newcomers, theirpeers, and their supervisors define the novices
roles immediately after entry (Morgeson,
Delaney-Klinger, & Hemingway, 2005; Morrison, 1994; Salancik
& Pfeffer, 1978; Tepper,
Lockhart, & Hoobler, 2001; Wrzesniewski, Dutton, &
Debebe, 2003). In addition, many
studies have ignored the fact that, over time, employees roles
may develop and
therefore the importance of competence in certain work activity
clusters may also
change (Barrett, Caldwell, & Alexander, 1989; Feij, Whitely,
Peiro, & Taris, 1995). For
example, it is likely that for graduates starting out on a
research career, knowledge and
mastery of research methodology is very important, while in a
later stage of theiracademic careers the ability to acquire grants
or to develop a research programme may
become more important competences.
The goal of this study is to contribute to the performance
appraisal literature by
developing a more detailed view of how newcomers competence in
specific work
activity clusters explains how their overall performance is
rated, and how this
relationship may change over time. Following Saks and Ashforths
(1997) suggestion,
we do this by examining the role of two clearly distinguishable
work activity clusters
in a specific occupational group, namely hospital nurses. By
focusing on two workactivity clusters appropriate to novice nurses
we are able to gain a more precise
insight into how competence in these clusters relates to the
evaluation of their
performance and to obtain more accurate assessments of how their
competence in
these clusters develops over time. This may not only increase
our understanding of
the relationships between competence and the evaluation of a
novices overall job
performance over time, but also provide important inputs that
can be used in the
development of professional training programmes for hospital
nurses and support
managerial interventions to improve the functioning and
development of newcomers.Further, it may also provide additional
insights into how newcomers may improve the
socialization process themselves.
460 Eric Molleman and Gerben S. van der Vegt
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Theory and hypotheses
The importance of competence in specific work activity
clustersAlthough it might seem obvious that, in general, a
newcomers competence will berelated positively to their
performance, past research has shown that this relationship is
in fact quite complex. Other factors such as motivation,
personality, expectations, work
design characteristics, mentoring systems, social support,
norms, values and attitudes
may mediate or moderate the competenceperformance relationship
or directly affect
performance (see, for example, Decker, 1985; Elbright, Urden,
Patterson, &
Chalko, 2004; Fisher, 1985; Forgas & George, 2001; Hancock,
Campbell, Ramprogus,
& Kilgour, 2005; Wanous et al., 1992; While, 1994). Thus,
even if newcomers have the
knowledge, skills and abilities to potentially perform well,
this does not necessarilymean that they will actually perform at
high levels. Therefore, examining the
relationship between novices competences in specific activity
clusters and overall job
performance is not as trivial as it first might sound. Moreover,
while logical work activity
clusters can be identified for most jobs and positions,
competence in all of these clusters
is not necessarily important for obtaining positive overall
performance evaluations.
Depending on ones specific role within a work-group or
organization, competence in
some clusters may be considered more important or relevant than
in others (Kammeyer-
Mueller & Wanberg, 2003). This is implicitly acknowledged in
several studies that havetried to identify and evaluate core
clusters for a number of professions. Zaccaro and
Banks (2004), for example, emphasized leader visioning and
adaptability as the most
important activity clusters for managers during a change in the
project. Van Leuven
(1999) identified several work activity clusters that were seen
as the most important for
entry-level practitioners in the public relations
profession.
Competence in specific work activity clusters for novice
nursesWithin the nursing literature, several work activity clusters
are distinguished, including
clinical care, managerial tasks and communication skills (see,
for example, Clinton,Murrells, & Robinson, 2005; Fitzpatrick,
While, & Roberts, 1997; Norman, Watson,
Murrells, Calman, & Redfern, 2002; Redfern, Norman, Calman,
Watson, & Murrells,
2002; Tzeng & Ketefian, 2003; Wandelt & Stewart, 1975;
Watson, Stimpson, Topping, &
Porock, 2002; Zhang, Luk, Arthur, & Wong, 2001). Competence
in such work activity
clusters is acquired through training and education in nursing
schools, and is included as
a major learning objective in most curricula (see, for example,
Clinton et al., 2005;
Gardner, Gardner, & Proctor, 2004; Lee-Hsieh, Kao, Kuo,
& Tseng, 2003). However, it is
unlikely that competence in all of the suggested clusters is
necessary for a positiveoverall performance evaluation of nurses
entering their first job. Given that the primary
task of novice nurses is to provide high-quality care to
patients, competence in
providing patient care will generally be considered as more
important for achieving a
high performance evaluation than competence in other clusters
(Clinton et al., 2005;
Ramritu & Barnard, 2001; Woods, 1999). Therefore, we argue
that competence in the
patient care work activity cluster will be of greatest
importance in achieving a high
performance rating. This cluster encompasses patient-related
care activities, such as
changing an infusion, bandaging a patient, supporting a patients
self-care, helping apatient cope with the consequences of illness
or informing a patient about a threatening
medical examination that will come (see, for example,
Fitzpatrick et al., 1997; Tzeng &
Ketefian, 2003; Wandelt & Stewart, 1975). In the remainder
of this article, we refer to a
novices mastery of such activities as their care competence.
Performance of novices 461
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
For the purposes of this study, and based on nursing literature,
we also distinguish a
second work activity cluster for the nursing profession that is
only weakly related to care
activities. This cluster includes activities such as
contributing to the health care quality
system, being able to define new working roles, providing
guidance to other nurses and
being able to come up with innovative working methods (see
Fitzpatrick et al., 1997;
Norman et al., 2002; Tzeng & Ketefian, 2003; Wandelt &
Stewart, 1975). In theremainder of this article, we will refer to a
novices mastery of such activities as their
non-care competence. We admit that by using this simple
classification, we do not
include all the work activity clusters that could possibly be
identified for the nursing
profession. Nevertheless, this general distinction is
appropriate for the purposes of our
study since we wish to examine the relationship between novices
competence in
specific but differentially important activity clusters and
their overall performance
evaluations over time.
Importance of work activity clusters on novice performanceThat
work activity clusters differ in their importance for high job
performance has
implications for the relationship between novices competence in
these clusters and theevaluation of their overall job performance
(Watson et al., 2002). Since the objective of a
nursing ward is first and foremost to provide high-quality
patient care, we assume that
when novice nurses indicate to have a high care competence, then
their contribution
to the performance of the ward is greater. Therefore, we would
expect their care
competence just after entry to be more strongly and positively
related to their overall
performance evaluation than their non-care competence. Moreover,
there may be
indirect ways in which care competence contributes to a higher
overall performance
rating. It is likely that those who contribute most to good
quality patient care, due totheir care competence, will receive the
greatest support from their peers and
supervisors. Receiving such social support will, in-turn, help
novices to improve their
performance still further (Cable & Parsons, 2001; Chen &
Klimoski, 2003; Haueter et al.,
2003; Moreland, 1985; Moreland & Levine, 1980; Moreland
& Levine, 2001). If during
the first period after entry, the care competence of novices is
indeed more important for
their higher overall job performance than their non-care
competence, then care
competence should be a stronger predictor of how their overall
performance is
evaluated than their non-care competence.
Hypothesis 1: Just after entry, novices competence in the care
cluster contributes more to apositive overall job performance
evaluation than their competence in the non-care cluster.
The above line of reasoning does not imply that non-care
competence is
unimportant for novice nurses during their first period after
entry. We accept that
competence in this cluster may be also a predictor of their
performance evaluations, but
expect that the strength and direction of this relationship will
also depend on their care
competence. Indeed, one could argue that novice nurses who have
shown competence
in care activities will be given more latitude to demonstrate
and develop their other
talents and will therefore, be considered ready at an earlier
stage for transfers to other
roles in which non-care competence is more critical (Berger,
Rosenholtz, & Zelditch,1980; Berger, Webster, Ridgeway, &
Rosenholtz, 1986; Chen & Klimoski, 2003;
Moreland & Levine, 2001). Consistent with this assertion,
Feldman (1976, p. 446) found
that newcomers first have to feel on top of their jobs before
they will make suggestions
about altering work-related activities. Indeed, before they are
given sufficient credit
462 Eric Molleman and Gerben S. van der Vegt
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
(or idiosyncrasy credits according to Hollander, 1985) to
manifest their non-care
competence, novice nurses will first have to live up to
expectations (Berger et al., 1980;
Feldman, 1976).
In contrast, novices who indicate to be less competent in the
care cluster may not be
given opportunities to expose their hidden competence in other
activity areas and,
even if they do expose them, they might be evaluated negatively.
Senior nurses willgenerally disapprove, if novices start to use
their non-care competences before they
have shown themselves to be sufficiently competent in the care
cluster. Thus, care
competence can be considered as a threshold for the employment
of competence in
other areas (Zhang et al., 2001). Any attempt to broaden ones
role prior to showing
sufficient care competence is likely be viewed as untimely and
inappropriate (Feij et al.,
1995). Based on these arguments, we would assume that just after
entry, novices care
competence would moderate the relationship between their
non-care competence and
the evaluation of their overall job performance.
Hypothesis 2: Just after entry, there will be a positive
relationship between competence in thenon-care cluster and overall
job performance evaluation provided a novices competence in thecare
cluster is high. When competence in the care cluster is low, we
expect this relationship tobe negative.
Changes in activity cluster competence over timeThe initial
period after entering their first job is generally seen as a phase,
during which
novices have to learn to perform their jobs effectively and to
increase their task-relevant
knowledge, skills and abilities. This implies that novices
competence can improve overtime. The fact that the importance for
high overall job performance of the various work
activity clusters may differ, could also have consequences for
what is learned by novices
and how this is achieved. Important work activity clusters,
those that form a central part
of ones job, will be deployed relatively often (Gibson, 2004).
This offers newcomers the
opportunity to learn the ropes by imitating their colleagues,
and provides
opportunities to evaluate and compare their own competence with
those of relevant
others. As a result, they will receive more accurate information
about their own
performance, which can be expected to stimulate learning and
effective behaviouralself-management (Saks & Ashforth, 1996).
Moreover, increasing competence in
important clusters will contribute to uncertainty reduction and
to self-esteem (Ramritu
& Bernard, 2001). If care competence is indeed more
important for novices job
performance than their non-care competence, then one would
expect to see a greater
increase over time in novices reported care competence than in
their reported non-care
competence. The time frame that is most commonly used to study
such developments
in a nursing context is 12 years (Carnwell & Daly, 2003;
Woods, 1999), and, therefore,
we will use a time frame of 18 months.
Hypothesis 3: Initially, novices competence in the care cluster
will increase more rapidly thantheir competence in the non-care
cluster.
The foregoing arguments also suggest that, after a certain time,
most novice nurses
will attain what may be called a maintenance stage, where care
competence will
become more or less self-evident (Deadrick, Bennett, &
Russell, 1997). If the nurses
care competences become high and more similar, it is likely that
these competences will
become less useful for senior nurses to discriminate between
poor and good performing
nurses, and, thus, will be less informative for determining
overall job performance
Performance of novices 463
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
(Deadrick et al., 1997). This suggests that the relationship
between care competence
and the evaluation of a novices overall job performance will
weaken over time (see also
Feij et al., 1995).
At the same time, it seems likely that when novices indicate to
be sufficiently
competent in providing care, they will feel more secure and
self-confident. This will
stimulate them to start to broaden their roles (Bauer et al.,
1998; Morgeson et al., 2005;Morrison, 1994). Such changes may occur
not only because the novice actively searches
for new challenges and learning objectives, but also because the
expectations of
colleagues and supervisors regarding the novices jobs and tasks
may change (Gibson,
2004). Moreover, it is reasonable to assume that provided nurses
demonstrate their care
competence, they will obtain more leeway to develop and expand
their roles (cf. Berger
et al., 1980). This increases the likelihood that they will be
given greater responsibilities,
with the result that competence in work activity clusters that
were less important in the
career stages immediately after entry becomes more important in
their new roles.Studies in the field of dynamic job performance do
indeed indicate that, as roles develop,
new work activity clusters may become important for high
performance (Barrett et al.,
1989; Deadrick et al., 1997). There is no reason why such role
development processes
should not also occur in nursing. Indeed, research has shown
that, over time, nurses
develop their roles from patient-related tasks to activities for
which competence in the
non-care cluster is required (Carnwell & Daly, 2003; Woods,
1999). Noyes (1995) has
argued that if novice nurses get greater clinical experience,
then they are better able to
place their job in a wider organizational context and,
therefore, their non-carecompetence will be more significant in
achieving a high overall job performance.
Novices on a nursing ward who have shown to be competent in the
care activities
cluster may, for example, be given the new task of mentoring
less-experienced nurses or
may be asked to participate in an organizational change
project.
Hypothesis 4: After 18 months, competence in the non-care
cluster contributes more to apositive overall job performance
evaluation than competence in the care cluster.
Method
DesignWe set up a panel of six head nurses to advise us with
respect to the design, content and
execution of the study. We used a longitudinal approach and
collected data at threestages: just before entry (T0), 6 weeks
after entry (T1) and 18 months after entry (T2).
Such a time-span is not unusual in socialization studies (for an
overview, see Bauer et al.,
1998) and was also supported by our panel of head nurses. At T0
and T2, the novices
completed a questionnaire. The questionnaires included items
that referred to the way
they perceived their own competence in the care and non-care
clusters. At T1 and T2,
three senior colleagues, including the head nurse and the nurse
who was assigned to
mentor the novice, were asked to evaluate the performance of the
novice. We chose to
measure self-assessed competence in both clusters just before
entry (T0), rather thanafter a short period (e.g. T1), because
research has shown that the entry phase is quite
stressful and this can make novices feel uncertain and doubt
their own competence,
which is then likely to result in biased survey responses (cf.
Fisher, 1985; Moreland &
Levine, 1980; Morrison, 1994). Naturally, we could not ask
senior nurses to evaluate the
performance of the novice nurses before entry. However, we
wanted to make the
interval between T0 and T1 as short as possible and our panel of
head nurses indicated
464 Eric Molleman and Gerben S. van der Vegt
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
that 6 weeks after entry was the earliest date to make reliable
performance assessments
(see also Bauer et al., 1998). At T1 and T2 the novices were
interviewed as part of the
regular human resource management policy of the hospitals
personnel department. We
took advantage of this by adding, to the standard interview
protocol, some open-ended
questions pertaining to the mastery and use of the two
identified work activity clusters
and to the social integration process in general. Transcriptions
of this part of theinterview were sent to the researchers. Some of
these are used as illustrative examples in
the Results section.
RespondentsThe study was conducted in the early 1990s in a
university hospital in the Netherlands
with just over 1200 beds. All the novice nurses with less than 3
months work experienceafter completing their vocational training (N
97) were asked to participate in the study.These novices entered
the hospital over a period of 19 months. Five novices refused
to
participate in the study or did not respond to any of the
questionnaires. The response rate
was 86 at T0 and 68 at T2. Consequently, depending on which time
interval is included in
a specific analysis, the number of observations differs to some
extent. The most common
reasons for non-response were unknown (12) having moved to
another ward (8),
resignation (6) and sickness (2). Multivariate analyses of
variance revealed that non-
response was not significantly related to age, gender,
department (e.g. surgery, internalmedicine) or to any of the other
study variables. Our response rates are not unusual for
longitudinal studies in healthcare settings. Adkins (1995) and
Fisher (1985), for example,
report response rates of 74 and 71%, respectively, in the final
round of their studies, some
69 months after the first. The mean age of the novices in our
study was 22.8 years
(SD 2:73) and just over 85% were female. The wards where the
novices started workingwere: Surgery (N 21), Internal Medicine (N
20), Gynaecology and Obstetrics(N 24), Paediatrics (N 8), Neurology
(N 9) and other specialties (N 15). Wereceived assessments of 84
novices from at least one senior colleague at T1, and at T2
wereceived evaluations of 60 novices1.
Measures
Competence in specific work activity clustersThis variable was
measured by asking novices to indicate to what extent they had
mastered each of the 16 activities (from 1 not at all to 5 very
well) that wereidentified as relevant in a previous study in the
same setting2. Since competences refer to
the potential to perform well and are generally not directly
observable, we have chosen tomake use of self-report measurements.
Such measurements have shown to be relatively
good proxies of true competences (Spenner, 1990). An exploratory
factor analysis
revealed four unrotated factors with eigenvalues above 1 (4.93,
1.99, 1.37 and 1.20).
Cattells SCREE test gives the best indication for the number of
factors to retain (Ford,
MacCallum, & Tait, 1986; Zwick & Velicer, 1982) and this
suggested a two-factor solution
that explained 43.24% of the variance. The loadings after
varimax rotation are presented
1More precisely, at T1 we received 1 evaluation for 1 novice, 2
evaluations for 28 novices and 3 evaluations for 55 novices,which
in total sums up to 222 evaluations by senior staff (i.e., 1 1 2 28
3 55). At T2 we received 1 evaluation for 6novices, 2 evaluations
for 48 novices and 3 evaluations for 6 novices, which sums up to
120 (i.e., 6 1 2 48 3 6).2 The results of this validation study are
reported in Aukes, Baving, and Molleman (1987). Additional
information can beobtained from the lead author.
Performance of novices 465
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
in Table 1. The items loading on the first factor reflect the
non-care activities and those
loading on the second factor pertain to care activities.
Although some of the specific items
might be more relevant for some wards than for others, our panel
of head nurses agreed
that these items did have a general relevance. Further, for our
study, we are not interested
in investigating differences between wards. To see whether the
factor structure at Time 2
replicated the structure at Time 0, we correlated the factor
loadings at Time 0 with theloadings at Time 2 (see, for example,
Van der Vegt & Janssen, 2003, for a more elaborate
explanation of this procedure). For the first factor (non-care)
this correlation was 0.80
(N 16, p , :001) and for the second one the correlation was 0.69
(N 16, p , :01),providing evidence for the invariance of the factor
structure over time. Values of
Cronbachs as for the scales measuring care competence were 0.79
at T0 and 0.68 at T2.The scale measuring non-care competence had a
:82 at T0 and.63 at T2.
Overall performance evaluationSince no adequate performance
evaluation measure was available for this specific group
of nurses, a new scale had to be developed. Evaluating overall
performance by using more
of a distal measure than specific performance items is
recommended by several authors
and, further, helps to distinguish our rather specific
competence predictors from our
performance evaluation measure (see, for example, Bauer &
Green, 1998; Sturman,
2003). In co-operation with our panel of head nurses, we
established an inventory of
criteria that define high-standard nurse performance. Then, in a
series of extensive
discussions with these same head nurses, a scale with six
overall performance evaluationitems was created. The items referred
to dedication, communication, self-reliance,
demonstrating accountability, administrative work and planning
of work. Overall
performance evaluation was measured by asking up to three senior
colleagues (including
the novices mentor and the head nurse) to indicate how satisfied
they were with the
novices performance in terms of these six global performance
items (from 1 very
Table 1. Factor analysis: items that had a high loading (shown
italics) on the same factor were assigned
to the same scale
Item Non-care Care
Inform a patient about a coming unpleasant medical examination
0.04 0.74Change an infusion 0.13 0.71Care for a patient with a
pressure sore 0.05 0.62Help a patient to cope with anxiety 0.24
0.61Talk with a patient about the consequences of illness and
treatment 0.23 0.58Monitor heart rhythm and blood pressure 0.14
0.58Inform a patients family about a patients condition 0.27
0.56Update a patients file 0.03 0.52Motivate colleagues to
participate in a ward change project 0.71 0.14Contribute to the
design and organization of the ward 0.73 0.11Discuss professional
developments with colleagues 0.69 20.06Comment on a colleagues
behaviour towards a patient 0.68 0.10Contribute to the introduction
of innovative work methods 0.62 0.35Contribute to a study on
optimizing patient admissions 0.61 0.18Contribute to the
development of healthcare quality policies 0.57 0.16Express a view
on the functioning of the ward 0.49 0.35
466 Eric Molleman and Gerben S. van der Vegt
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
dissatisfied to 5 very satisfied). For T1, the inter-rater
reliability (rWG, see James,Demaree, & Wolf, 1984) for the set
of six parallel items varied from 0.87 to 1.00
(M 0:99, SD 0:01) and for T2, the range was 0.971.00 (M 0:99, SD
0:01),indicating that the scores of the individual raters could be
combined. Next, for every
novice the evaluation scores were averaged for each of the six
items, separately for T1 and
T2. After that we conducted an exploratory factor analysis on
the six averaged items. Theeigenvalues of the first two unrotated
factors were 4.45 and 0.65 for T1, and 4.59 and 0.52
for T2, clearly supporting a one-dimensional solution. The
values of Cronbachs a for theoverall performance evaluation scale
were 0.93 at T1 and 0.94 at T2.
Results
Descriptive statistics and correlationsTable 2 presents the
means, standard deviations and Pearson zero-order correlations
among the variables in this study. This shows that the
competences in the care and non-
care clusters, measured at both T0 and T2 were only moderately
related to each other
(Pearsons r between the two clusters was .43 at T0 and .35 at
T2). Moreover,
the autocorrelations between the competence clusters were 0.53
for care and 0.26 for
non-care. Off-diagonal correlations were 0.14 and 0.22, thereby
showing discriminantvalidity.
Testing the hypothesesHypothesis 1 states that novices care
competence is a stronger predictor of their overall
job performance evaluation than their non-care competence. We
carried out hierarchicallinear regression analyses using novice
performance rated by senior staff 6 weeks after
entry as the dependent variable, and self-evaluated competence
in the two-work activity
clusters just before entry as the predictor variables. Column 2
in Table 3 shows that care
competence was significantly related to the performance rated by
senior staff, whereas
non-care competence was not. Moreover, the difference between
the two regression
weights was significant (t 3:94, df 68, p , :001). The beta
weight for carecompetence indicates that the higher the claimed
competence in this cluster, the more
positively their performance was evaluated by senior colleagues.
This supports
Table 2. Means, standard deviations and intercorrelations of the
study variables
M SD (1) (2) (3) (4) (5) (6) (7)
(1) Gender 1.86 0.35(2) Age 22.81 2.73 0.03(3) Care competence
T0 4.22 0.53 20.03 20.05(4) Non-care competence T0 3.46 0.61 20.01
0.02 0.43***(5) Care competence T2 4.51 0.33 0.11 20.11 0.53***
0.22(6) Non-care competence T2 3.49 0.48 0.10 20.13 0.14 0.26*
0.35**(7) Performance rating T1 3.91 0.51 0.01 20.05 0.35** 0.13
0.32* 0.09(8) Performance rating T2 4.12 0.58 0.14 20.09 0.02 20.07
20.06 0.19 0.39**
Notes. For gender, male was coded as 1 and female as 2.T0
pre-entry; T1 6 weeks after entry; T2 18 months after entry.*p ,
:05; **p , :01; ***p , :001.
Performance of novices 467
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Hypothesis 1. During the interviews 6 weeks after entry, the
novices also stressed the
importance of care competence, which is illustrated by the
following quotes:
Patient care is such a central issue and valued so much by
colleagues that I first want to
meet their expectations in this field. Other sides of the
profession are completely secondary
at this moment.
Possessing practical caring skills is what primarily counts when
the head nurse evaluates
my performance.
The best way to become a full team member is to show your team
mates that you make a
good contribution to patient care.
Practical experience is what really counts in my job.
Hypothesis 2 states that there will be a positive relationship
between non-care
competence and overall job performance evaluation if a novices
care competence is
high. Conversely, if a novices competence in the care cluster is
low, then we expect this
relationship to be negative. To test this interaction effect we
followed the procedure
recommended by Aiken and West (1991): (1) standardize the
predictors to reducemulticollinearity between these variables and
their interaction term, (2) multiply the
two variables to calculate their interaction term and (3)
include the main effect in the
model to prevent a biased estimate of the interaction effect.
The third column in Table 3
shows that, after including the main effects in the regression
model, the interaction
between care and non-care competence is significant.
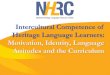
To interpret the pattern of the interaction effect, we plotted
the relationship between
non-care competence and performance rated by senior staff for
individuals with low (1 SD
below the mean) and high (1 SD above the mean) levels of
competence in the care cluster,following the procedures outlined by
Aiken and West (1991). Figure 1 shows that for
those novices who score high on competence in the care cluster,
higher scores on non-
care competence are associated with more favourable performance
evaluations. For
novices with a low score on competence in the care cluster,
non-care competence is
negatively related to performance evaluations. Thus, these
results support Hypothesis 2.
The following quotes from the interviews 6 weeks after entry
reflect the above-
mentioned findings:
I have to improve my clinical knowledge and skills to make my
colleagues value my work. It
makes no sense to interfere in other matters if the quality of
the care you provide is
Table 3. Regression of performance by senior staff (T1, 6 weeks
after entry) on care and non-care
competence and their interaction term (T0, just before
entry)
Predictors (T0) Step 1 (df 4, 68) Step 2 (df 5, 67)
Gender 20.02 20.07Age 0.04 0.04Care competence 0.38**
0.43**Non-care competence 20.05 0.02Care Non-care competence 0.22*F
2.37* 2.49*Model R2 0.12* 0.16**R2 Change 0.12* 0.04*
Note. Beta weights are presented; *p , :05; **p , :01
(one-tailed tests).
468 Eric Molleman and Gerben S. van der Vegt
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
insufficient. Most patients we care for have very serious
physical problems and you wont
be taken seriously if, for example, you do not know how to deal
with all types of drains and
infusions.If you cannot fulfil the patients basic care needs you
are missing the essence of working
here. Once you can adequately take care of the patients, there
is leeway to explore and
develop other sides of the work.Last week I made suggestions how
to improve teamwork. My peers didnt appreciate that at
all. They simply sent me back to work.Deep inside, I have many
ideas about how to improve our work setting. However, I find it
risky to suggest them now.
Hypothesis 3 states that, initially, novices care competence
increases more rapidly than
their non-care competence. A multivariate analysis of variance
with competence in both
activity clusters (two levels: care and non-care) and time (two
levels: just before entry
and after 18 months) as factors showed a significant main effect
for work activity
clusters (F1; 61 250:32, p , :001), a significant main effect
for time(F1; 61 9:65, p , :01) and a significant work activity
cluster time interactioneffect (F1; 61 11:96, p , :001). The main
effect of work activity clusters reflectedthat, regardless of the
measurement time, novices reported possessing more care
competence (M 4:35) than non-care competence (M 3:47). The main
effect of timewas that novices assessed their overall competence
level more favourably at T2 (4.03)
than at T0 (3.84), indicating an overall learning effect.
Finally, the time work activitycluster interaction effect indicates
that the competences in the two specific activity
clusters change at different rates over time. Paired t tests
showed that novices perceived
their care competence to have increased substantially over time
(t 5:48, df 61,p , :001), whereas their perceived non-care
competence did not change significantlyover the 18 months (t 0:70,
df 61, ns). These results support Hypothesis 3. Thefollowing quotes
illustrate how novices expressed themselves on this point during
the
interviews, 18 months after entry (T2):
The first months were extremely exhausting. I had just left my
parents house, and my
family and friends were far away. Everything was new and at the
end of each day I was
completely exhausted. To make me feel secure during this first
period, I only focused on
mastering direct patient care activities. At that time I had no
other concerns. Now I have
mastered all the regular patient care activities relevant to the
ward.
Figure 1. Relationship between non-care competence and
performance evaluations for novices who
score low and high on care competence.
Performance of novices 469
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
If I look back, I really started as a greenhorn. I am glad I
concentrated on clinical practice.
What nursing school had taught me in that field was really
rudimentary. I have learned a
lot and I think that patients see that I am now a competent
nurse.
School gave me a thoroughly professional attitude. In order to
survive in actual practice
however, I set most of these ideas aside and focused upon
patient care.
In Hypothesis 4 we stated that 18 months after entry, competence
in the non-carecluster contributes more to a positive overall job
performance than competence in the
care cluster. To test this hypothesis we carried out
hierarchical linear regression analyses
using novice performance rated by senior staff 18 months after
entry as the dependent
variable, self-evaluated competence in the two work activity
clusters at that time as the
predictor variables, and gender and age as control variables.
The weight for non-care
competence was .23 and for care competence it was 2 .13. These
weights differsignificantly (t 2:60, df 55, p , :05). This supports
Hypothesis 4. The followingquotations illustrate our findings
relating to Hypotheses 4:
In my first year I found it difficult to give feedback to
colleagues. Now I feel much more
confident in doing so.
I dont feel like a novice anymore. What really counts now is to
be a reliable and trusted
colleague who contributes to all issues that are relevant for
our ward.
During the first months I was completely focused on myself. My
main concern was to do
my job properly. When colleagues assisted me I experienced it as
a personal failure. Now I
value that I can help team mates and that they help me. There is
mutuality and I have
become a respected team player who is allowed to come up with
good ideas to improve our
work.
Recently I have organized a meeting to discuss our team
functioning. A year ago that would
have been completely out of order
Exploratory analysesPlaying the role of the devils advocate, one
could argue that the above findings were
influenced by our decision to apply Cattels SCREE test to
determine the appropriatenumber of factors and to extract only two
factors. The use of alternative criteria (e.g. the
Kaiser criterion; see, for example, Zwich & Velicer, 1982)
might have favoured a
solution with three or four factors and could have resulted in
different findings. In order
to address this possibility, we explored the relevance of the
three- and four-factor
solutions, and the possible consequences for our results and
conclusions.
When we tried a three-factor solution, the non-care factor
remained the same (i.e.
the first factor in Table 1), whereas the care items split into
two factors with four items
in each. The first of these two factors included the items
related to communicationissues (e.g. Inform a patient about a
forthcoming unpleasant medical examination) and
the second factor covered the items related to technical
competences (e.g. Change an
infusion). The reliabilities of these two scales were 0.74 and
0.67, respectively. If we
opted for a four-factor structure, then the non-care and
communication factors
remained unchanged, while the four technical items split further
into two factors.
However, the fourth factor included only one item (Update a
patients file). Given this
result, we concluded that it was only sensible to test the
hypotheses using the scales
resulting from the three-factor solution.When testing our
hypotheses using the technical competence and communication
competence scales instead of the original care competence scale,
the results for
Hypotheses 1, 3 and 4 remained essentially the same or became
somewhat stronger.
That is, in all of the regression analyses, the beta weights for
the communication and
470 Eric Molleman and Gerben S. van der Vegt
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
technical competences scales were very close to those of the
original care competence
scale. For Hypothesis 2, however, the findings were somewhat
different: the beta
weights for the interaction of non-care competence with
technical competences and
with communication competences were 0.33 (p , :05) and 0.18 (p ,
:10),respectively, compared with 0.22 (p , :05) for the original
care competence scale.Overall, however, given the small differences
between these and our original findings,we have concluded that our
decision to apply Cattels SCREE test has not substantially
influenced our conclusions, and that the two-factor solution,
resulting in the most
parsimonious set of results, was valid.
Discussion
The goal of this study was to examine the relationships between
novices competence in
specific work activity clusters, learning and the evaluation of
their overall performance.
We found that, 6 weeks after entry, novices care competence
contributed more to apositive performance evaluation by the senior
staff than their non-care competence.
Being able to contribute substantially to the care of patients
may make a novice feel
confident and valued. Moreover, it may instantly ease the
workload of colleagues and
add to team performance, which is likely to be highly
appreciated by ones team mates.
Additionally, we found that, 6 weeks after entry, the effect of
non-care competence
on a novices performance evaluation was linked to their care
competence. Our results
show that for novices whose care competence is relatively low,
there is a negative
relationship between non-care competence and performance
evaluation, whereas thisrelationship is positive if they have high
levels of care competence. Since making use of
non-care competence entails the expression of ideas, opinions
and criticism, it is
possible that colleagues will not appreciate such behaviour
shortly after entry if the
novice lacks competence in the field of patient care, because it
challenges the status
quo that is deeply anchored in the norms and value systems of
the ward. It seems that as
long as one is unable to help patients adequately, giving
feedback to colleagues or
bringing up ideas or suggestions regarding working methods will
be negatively valued.
Consistent with our expectations, our findings also revealed
that the importance ofcompetence in the specific work activity
clusters changed over time. First of all, we
found that novices reported a greater increase in their care,
than in their non-care
competence. It seems that novices focus on learning care
activities because gaining
competence in this cluster of activities most reduces
uncertainty and enhances feelings
of self-confidence. Moreover, it is especially care competences
that contribute directly
to ward performance with respect to the primary task, i.e.
patient care.
We predicted and indeed found that the relative contribution of
competence in
specific activity clusters to performance evaluations changes
over time. Our resultsshowed that while 6 weeks after entry care
competences contribute more to a positive
performance evaluation than non-care competences, 18 months
after entry we found
the opposite, i.e. competence in the non-care cluster
contributes more to a positive
performance evaluation than competence in the care cluster.
Eighteen months after
entry, competence in the care activity cluster may have become
self-evident and,
therefore, may be no longer predictive of overall
performance.
Practical implicationsOur findings may have several practical
implications. Our study makes clear that
acquiring knowledge, skills and abilities in the area of patient
care during the initial
Performance of novices 471
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
vocational training of nurses is critical. Once novices have
shown competence in this
area, they will get leeway to demonstrate competence in other
work activity clusters, or
to move to other occupational roles in which other work activity
clusters are more
important. Although patient care activities might be the major
concern of nursing
schools, we would not want the reader to infer from our findings
that other areas are
unimportant. Other activities, such as managerial and
professional development, forman integral part of the nursing
profession. Adequate basic knowledge and skills in these
areas may be necessary in later stages of nurses careers. Care
competences are
immediately relevant, but are also likely to be rather
context-specific so that it is nearly
impossible to learn all possible care competences for all
possible health care settings
during initial vocational training. On-the-job learning of
several of the care competences
seems inevitable and to some extent such additional on-the-job
training might be
required again if nurses move to another ward or health care
setting in a later stage of
their careers. The value of competence in non-care areas is less
context-dependent andcan be more easily transferred to other role
settings (Cunningham, 1996; Tschan & Von
Cranach, 1996). Therefore, learning about and mastering
activities in other areas than
patient care during initial vocational training remains
useful.
Nevertheless, it seems important to develop realistic
expectations about a nurses
first job (see, for example, Dean & Wanous, 1984; Meglino
& DeNisi, 1988) and to clarify
during the initial training of nurses that, when they do start
work, it is wise to focus
primarily on patient care and to set aside their competences in
other areas for use at a
later stage. If they approach work in this tactical way, novices
might move moresmoothly through the initial stages of working life,
and the amount of time required from
their supervisors and mentors for successful socialization might
decrease, thereby
enhancing both performance and satisfaction. This might also
reduce the number of
novices leaving the profession and so save time and money.
Theoretical implicationsThe results of this study contribute to
knowledge in the field of organizational and
occupational psychology in several ways. First, our study
contributes to the
performance evaluation literature by showing that the
interrelationship between
competence and the evaluation of a novices performance is
complex. Most previous
performance evaluation studies have not considered the role of
specific knowledge,
skills and abilities, nor have they examined the changing
importance of particular work
activity clusters over time (Chao, Olearykelly, Wolf, Klein,
& Gardner, 1994; Saks &
Ashforth, 1997). Our study shows that competences in different
work activity areas mayjointly affect the evaluation of a novices
performance. Moreover, our findings suggest
that, possibly due to learning effects, the predictive power of
some activity clusters
changes over time and that, as a result, the relationship
between competence in specific
activity clusters and performance evaluation is not
constant.
Second, our results have implications for the socialization
literature. Although there
are many factors that affect the socialization of newcomers, it
is clear that one of the
factors that plays an important role is the mastery of
job-relevant competences (for
overviews, see Bauer et al., 1998; Saks & Ashforth, 1997).
For example, Fisher (1986)posited learning to perform the required
work task is obviously a critical part of
socialization (p. 107). Haueter et al. (2003) have shown the
importance of task
socialization, which they define as acquiring task knowledge,
learning how to perform
relevant task behaviours and learning how to interact with
others in the course of
472 Eric Molleman and Gerben S. van der Vegt
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
performing specific tasks (p. 24). Our study shows that it is
important for newcomers to
realize that in the first period after entrance, some
competences might be more
important than others and contribute more directly to their
overall performance. So,
being aware which competences are most important during
different socialization
phases seems to be very important for newcomers. Also from a
managerial perspective,
our insights may help to develop interventions directed to the
socialization ofnewcomers such as training programmes and
mentorship policies.
Third, our results are important for theory and research dealing
with extra-role
behaviour in organizations (e.g. Miles, Borman, Spector, &
Fox, 2002). Extra-role
activities are generally considered to be positive and desirable
for organizational
effectiveness. However, it has been indicated that such
activities are sometimes also
perceived as counterproductive (Miles et al., 2002; Sackett,
2002; Staw & Boettger,
1990; Wrzesniewski & Dutton, 2001). Consistent with this
evidence, our study suggests
that extra-role activities of nurses in terms of non-care
competences will be valued onlyif their care activities are
positively evaluated. Newcomers will have to acquire credit by
showing high-quality in-role activities before extra-role
efforts are appreciated (see also
Werner, 1994).
Finally, authors who have used a social information-processing
approach to role
theory have indicated that there is no clear boundary between
in- and extra-role activities
and that roles are socially constructed phenomena that may
change over time (Morrison,
1994; Tepper et al., 2001; Wrzesniewski et al., 2003). Role
development entails that roles
are redefined and that activities that were considered to be
extra-role or evencounterproductive before, become in-role and
valued (Morrison, 1994). The findings
from our study support such a dynamic view on role development.
It is likely that when
novices have learned to master the in-role activities
adequately, they will feel more secure
and less uncertain, which may enhance perceptions of
self-efficacy and self-esteem (e.g.
Ramritu & Barnard, 2001). Our findings suggest that this
makes them eager to start to
broaden their roles (Bauer et al., 1998; Morgeson et al., 2005;
Morrison, 1994).
Strengths and limitationsWe would argue that our study has
several strengths. First, we used self-reporting to
assess competence and ratings by senior staff to measure
performance, thereby
reducing the likelihood of mono-method bias. Further, using both
qualitative and
quantitative information contributed to our understanding of the
role of competence in
specific work activity clusters and the evaluation of overall
job performance. Moreover,
the longitudinal design of our study helped in gaining a better
insight into the dynamicnature of the relationship between
competence in specific work activity clusters and
the evaluation of performance. And finally, our focus on one
particular occupational
group enabled us to examine the role of novices competence in a
more specific way
than it is possible in a more general study. As Saks and
Ashforth (1997, p. 270) stated
most past socialization research has lumped together different
occupational groups
and according to them, targeting specific occupations will
contribute to the elaboration
of the socialization literature.
Apart from these strengths, our study inevitably has a few
limitations. First, the careand non-care competences of novices
were only measured using self-reporting
instruments. It would have been better if we had used
more-objective measures of their
competence in specific work activity clusters. The addition of
assessments by peers or
supervisors, for example, might help to improve the measurement
of competences.
Performance of novices 473
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Second, with respect to the outcome variables, we included only
one measure: the
overall performance evaluation of a novice. In future research,
it might be useful to
include other outcome variables, such as job satisfaction,
acceptance by the group and
intention to stay or leave. Third, the number of respondents in
this study was rather
small. However, obtaining large samples of one particular and
highly specific
occupational group is difficult. Fourth, although the main
purpose of the interviewswas to support the novices in becoming
full and respected members of the organization,
it is possible that some novices felt constrained by the
HR-mandated nature of the
interview. Since we have used the qualitative data only for
illustrative purposes, this
might be less critical. Finally, although we found that
competence can develop over
time, we did not investigate the possible underlying mechanisms.
It might, for example,
well be that changes in role content or changes in performance
expectations affect the
development of certain competences and might also explain the
dynamic relationship
between a specific competence and performance evaluation. Such
underlyingmechanisms would be an interesting subject for future
research.
Although the generalizability of our findings is, strictly
speaking, limited to hospital
nurses, it is nevertheless relatively easy to imagine how
similar processes might occur in
other occupational groups. For example, for mechanics entering
their first job, the
ability to diagnose and repair engine defects is likely to be
more relevant and critical
than possessing good communication skills or having an insight
into the automotive
market. Of course, the ability to communicate to the owner of a
car, the details of a
problem and the necessary repairs may become important, but
these skills are rathermeaningless if one does not have the
competence to diagnose the defects in the first
place. Similarly, knowledge of the automotive market might
become an important
competence at a later stage of mechanics careers, if they become
involved in sales
activities. To give another example, it is critical for a young
academic to have writing
skills and to be able to retrieve the relevant literature. The
competence to write high-
quality review reports, however, will be less relevant during
the initial stage of such a
career. Such generalizations from our findings are, however,
only speculative and
require further support. Therefore, future research should
examine similar relationshipsto those described in this article
using occupational groups from other industries.
ConclusionThe performance of relative novices and new employees
without work experience is
crucial in determining organizational effectiveness. Focusing
first on the competence ofnovices in the most important work
activity clusters, and only later on others, will ease
their socialization and may have positive and lasting effects on
learning and adjustment,
person-job fit, person-organization fit, job satisfaction and
performance (Haueter et al.,
2003: 21). The findings of our study suggest that taking into
account the relative
importance of specific work activity clusters, and also the
changes in their importance
over time, may help novices, as well as their managers, in
facilitating the process of
becoming a full and valued member of the organization.
References
Adkins, C. L. (1995). Previous work experience and
organizational socialization - A longitudinal
examination. Academy of Management Journal, 38, 839862.
Aiken, L. S., & West, S. G. (1991). Multiple regression:
Testing and interpreting interactions.
Newbury Park: Sage publications.
474 Eric Molleman and Gerben S. van der Vegt
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Aukes, L. C., Baving, J. E., & Molleman, E. (1987). Het
nieuwkomersonderzoek. [Study among
novices] Unpublished document, University Hospital, University
of Groningen, Groningen.
Barrett, G. V., Caldwell, M. S., & Alexander, R. A. (1989).
The predictive stability of ability
requirements for task performance: A critical reanalysis. Human
Performance, 2, 167181.
Bauer, T. N., & Green, S. G. (1998). Testing the combined
effects of newcomer information seeking
and manager behavior on socialization. Journal of Applied
Psychology, 83, 7283.
Bauer, T. N., Morrison, E. W., & Callister, R. R. (1998).
Organizational socialization: A review and
directions for future research. In G. R. Ferris (Ed.), Research
in personal and human resource
management ( Vol. 16, pp. 149214). Stamford, CT: JAI.
Berger, J., Rosenholtz, S. J., & Zelditch, M. (1980). Status
organizing processes. Annual Review of
Sociology, 6, 479508.
Berger, J., Webster, M., Ridgeway, C., & Rosenholtz, S. J.
(1986). Status cues, expectations and
behavior. In E. J. Lawler (Ed.), Advances in group processes
(Vol. 3). Greenwich, CT: Jai Press.
Blau, G. (1999). Early-career job factors influencing the
professional commitment of medical
technologists. Academy of Management Journal, 42, 687695.
Cable, D. M., & Parsons, C. K. (2001). Socialization tactics
and person-organization fit. Personnel
Psychology, 54, 123.
Campion, M. A., Mumford, T. V., Morgeson, F. P., & Nahrgang,
J. D. (2005). Work redesign: Eight
obstacles and opportunities. Human Resource Management, 44,
367390.
Carnwell, R., & Daly, W. M. (2003). Advanced nursing
practitioners in primary care settings:
An exploration of the developing roles. Journal of Clinical
Nursing, 12, 630642.
Chao, G. T., Olearykelly, A. M., Wolf, S., Klein, H. J., &
Gardner, P. D. (1994). Organizational
socialization - Its content and consequences. Journal of Applied
Psychology, 79, 730743.
Chen, G., & Klimoski, R. J. (2003). The impact of
expectations on newcomer performance in
teams as mediated by work characteristics, social exchanges, and
empowerment. Academy of
Management Journal, 46, 591607.
Clinton, M., Murrells, T., & Robinson, S. (2005). Assessing
competency in nursing: A comparison
of nurses prepared through degree and diploma programmes.
Journal of Clinical Nursing, 14,
8294.
Cunningham, J. W. (1996). Generic job descriptors: A likely
direction in occupational analysis.
Military Psychology, 8, 247262.
Deadrick, D. L., Bennett, N., & Russell, C. J. (1997). Using
hierarchical linear modeling to examine
dynamic performance criteria over time. Journal of Management,
23, 745757.
Dean, R. A., & Wanous, J. P. (1984). Effects of realistic
job previews on hiring bank tellers. Journal
of Applied Psychology, 69, 6168.
Decker, F. H. (1985). Socialization and interpersonal
environment in nurses affective reactions to
work. Social Science and Medicine, 20, 499509.
Dubinsky, A. J., Howell, R. D., Ingram, T. N., & Bellenger,
D. N. (1986). Salesforce socialization.
Journal of Marketing, 50, 192207.
Elbright, P. R., Urden, L., Patterson, E., & Chalko, B.
(2004). Themes surrounding novice nurse-
miss and adverse-event situations. Journal of Nursing
Administration, 34, 531538.
Feij, J. A., Whitely, W. T., Peiro, J. M., & Taris, T. W.
(1995). The development of career-enhancing
strategies and content innovation - A longitudinal-study of new
workers. Journal of Vocational
Behavior, 46, 231256.
Feldman, D. C. (1976). Contingency theory of socialization.
Administrative science quarterly, 21,
433452.
Fisher, C. D. (1985). Social support and adjustment to work - A
longitudinal-study. Journal of
Management, 11, 3953.
Fisher, C. D. (1986). Organizational socialization: An
integrative review. In G. R. Ferris & K. M.
Rowland (Eds.), Research in personal and human resource
management ( Vol. 4,
pp. 101145). Greenwich, CT: JAI.
Performance of novices 475
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Fitzpatrick, J. M., While, A. E., & Roberts, J. D. (1997).
Measuring clinical nurse performance:
Development of the kings nurse performance scale. International
Journal of Nursing
Studies, 34, 222230.
Ford, J. K., MacCallum, R. C., & Tait, M. (1986). The
application of exploratory factor analysis in
applied psychology: A critical review and analysis. Personnel
Psychology, 39, 291314.
Forgas, J. P., & George, J. M. (2001). Affective influences
on judgments and behavior in
organizations: An information processing perspective.
Organizational Behavior and Human
Decision Processes, 86, 334.
Gardner, G., Gardner, A., & Proctor, M. (2004). Nurse
practitioner education: A research-based
curriculum structure. Journal of Advanced Nursing, 47,
143152.
Gibson, D. E. (2004). Role models in career development: New
directions for theory and research.
Journal of Vocational Behavior, 65, 134156.
Hancock, H., Campbell, S., Ramprogus, V., & Kilgour, J.
(2005). Role development in health care
assistants: The impact of education on practice. Journal of
Evaluation of Clinical Practice,
11, 489498.
Haueter, J. A., Macan, T. H., & Winter, J. (2003).
Measurement of newcomer socialization:
Construct validation of a multidimensional scale. Journal of
Vocational Behavior, 63, 2039.
Hollander, E. P. (1985). Leadership and power. In G. Lindzey
& E. Aronson (Eds.), The handbook of
social psychology. New York: Random House.
James, L. R., Demaree, R. G., & Wolf, G. (1984). Estimating
within-group interrater reliability with
and without response bias. Journal of Applied Psychology, 69,
8598.
Kammeyer-Mueller, J. D., & Wanberg, C. R. (2003). Unwrapping
the organizational entry process:
Disentangling multiple antecedents and their pathways to
adjustment. Journal of Applied
Psychology, 88, 779794.
Lee-Hsieh, J., Kao, C. H., Kuo, C. L., & Tseng, H. F.
(2003). Clinical nursing competence of RN-to-
BSN students in a nursing concept-based curriculum in Taiwan.
Journal of Nursing
Education, 42, 536545.
Louis, M. R. (1980). Surprise and sense making - What newcomers
experience in entering
unfamiliar organizational settings. Administrative Science
Quarterly, 25, 226251.
Meglino, B. M., & DeNisi, A. S. (1988). Realistic job
previews: Some thoughts on their more
effective use in managing the flow of human resources. Human
Resource Planning, 10,
157167.
Miles, D. E., Borman, W. E., Spector, P. E., & Fox, F.
(2002). Building an integrative model of extra
role work behaviours: A comparison of counterproductive work
behaviour with
organizational citizenship behaviour. International Journal of
Selection and Assessment,
10, 5157.
Moreland, R. L. (1985). Social categorization and the
assimilation of new group members. Journal
of Personality and Social Psychology, 48, 11731190.
Moreland, R. L., & Levine, J. M. (1980). Newcomers and
oldtimers in small groups. In P. B. Paulus
(Ed.), Psychology of group influence. Hillsdale, NJ: Erlbaum
Associates.
Moreland, R. L., & Levine, J. M. (2001). Socialization in
organizations and work groups. In
M. Turner (Ed.), Groups at work: Theory and research. Mahwah:
Erlbaum.
Morgeson, F. P., Delaney-Klinger, K., & Hemingway, M. A.
(2005). The importance of job autonomy,
cognitive ability, and job-related skill for predicting role
breadth and job performance. Journal
of Applied Psychology, 90, 399406.
Morrison, E. W. (1994). Role definitions and organizational
citizenship behaviour: The importance
of the employees perspective. Academy of Management Journal, 37,
15431567.
Norman, I. J., Watson, R., Murrells, T., Calman, L., &
Redfern, S. (2002). The validity and reliability
of methods to assess the competence to practice of
pre-registration nursing and midwifery
students. International Journal of Nursing Studies, 39,
133145.
Noyes, J. (1995). An explanation of the differences between
expert and novice performance in the
administration of intramuscular injection of an analgesic agent
to a patient in pain. Journal of
Advanced Nursing, 22, 800807.
476 Eric Molleman and Gerben S. van der Vegt
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Ramritu, P. L., & Barnard, A. (2001). New nurse graduates
understanding of competence.
International Nursing Review, 48, 4757.
Redfern, S., Norman, I., Calman, L., Watson, R., & Murrells,
T. (2002). Assessing competence to
practice in nursing: A review of the literature. Research Papers
in Education, 17, 5177.
Sackett, P. R. (2002). The structure of counterproductive work
behaviours: Dimensionality and
relationships with facets of job performance. International
Journal of Selection and
Assessment, 10, 511.
Saks, A. M., & Ashforth, B. E. (1996). Proactive
socialization and behavioral self-management.
Journal of Vocational Behavior, 48, 301323.
Saks, A. M., & Ashforth, B. E. (1997). Organizational
socialization: Making sense of the past and
present as a prologue for the future. Journal of Vocational
Behavior, 51, 234279.
Salancik, G. R., & Pfeffer, J. (1978). A social information
processing approach to job attitudes and
task design. Administrative Science Quarterly, 23, 224253.
Spenner, K. I. (1990). Skills: Meanings, methods, and
measurements. Work and Occupations, 17,
399421.
Staw, B. M., & Boettger, R. D. (1990). Task revision - A
neglected form of work performance.
Academy of Management Journal, 33, 534559.
Sturman, M. C. (2003). Searching for the inverted U-shaped
relationship between time and
performance: Meta-analyses of the experience/performance,
tenure/performance, and
age/performance relationships. Journal of Management, 29,
609640.
Tepper, B. J., Lockhart, D., & Hoobler, J. (2001). Justice,
citizenship, and role definition effects.
Journal of Applied Psychology, 86, 789796.
Tschan, F., & Von Cranach, M. (1996). Group task structure,
processes and outcome. In M. A. West
(Ed.), Handbook of work group psychology (pp. 95121). New York:
Wiley.
Tzeng, H. M., & Ketefian, S. (2003). Demand for nursing
competencies: An exploratory study in
Taiwans hospital system. Journal of Clinical Nursing, 12,
509518.
Van der Vegt, G. S., & Janssen, O. (2003). Joint impact of
interdependence and group diversity on
innovation. Journal of Management, 29, 729751.
Van Leuven, J. (1999). Four new course competencies for majors.
Public Relations Review, 25(1),
7785.
Van Maanen, J. (1976). Breaking in: Socialization to work. In R.
Dubin (Ed.), Handbook of work,
organization, and society (pp. 67130). Chicago: Rand
McNally.
Van Maanen, J., & Schein, E. H. (1979). Toward a theory of
organizational socialization. In B. Staw
(Ed.), Research in organizational behavior ( Vol. 1, pp.
209264). Greenwich, CT: JAI Press.
Wandelt, M. A., & Stewart, D. S. (1975). Slater nursing
competencies rating scale. New York:
Appleton-Century Crofts.
Wanous, J. P., Poland, T. D., Premack, S. L., & Davis, K. S.
(1992). The effects of met expectations
on newcomer attitudes and behaviors - A review and
meta-analysis. Journal of Applied
Psychology, 77, 288297.
Watson, R., Stimpson, A., Topping, A., & Porock, D. (2002).
Clinical competence assessment in
nursing: A systematic review of the literature. Journal of
Advanced Nursing, 39, 421431.
Werner, J. M. (1994). Dimensions that make a difference:
Examining the impact of in-role and
extrarole behaviours on supervisory ratings. Journal of Applied
Psychology, 79, 98107.
While, A. E. (1994). Competence versus performance: Which is
more important? Journal of
Advanced Nursing, 20, 525531.
Woods, L. P. (1999). The contingent nature of advanced nursing
practice. Journal of Advanced
Nursing, 30, 121128.
Wrzesniewski, A., & Dutton, J. E. (2001). Crafting a job:
Revisioning employees as active crafters of
their work. Academy of Management Review, 26, 179201.
Wrzesniewski, A., Dutton, J. E., & Debebe, G. (2003).
Interpersonal sensemaking and the meaning
of work. Research in Organizational Behavior, 25, 93135.
Performance of novices 477
-
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Zaccaro, S. J., & Banks, D. (2004). Leader visioning and
adaptability: Bridging the gap between
research and practice on developing the ability to manage
change. Human Resource
Management, 43(4), 367380.
Zhang, Z. X., Luk, W., Arthur, D., & Wong, T. (2001).
Nursing competencies: Personal
characteristics contributing to effective nursing performance.
Journal of Advanced Nursing,
33, 467474.
Zwick, W. R., & Velicer, W. F. (1982). Factors influencing
four rules for determining the number of
components to retain. Multivariate Behavioral Research, 17,
253269.
Received 15 September 2005; revised version received 31 August
2006
478 Eric Molleman and Gerben S. van der Vegt