Embed Size (px)
Citation preview

European Journal of Heart Failure (2020) RESEARCH ARTICLEdoi:10.1002/ejhf.1783
The impact of palliative care on clinical andpatient-centred outcomes in patients withadvanced heart failure: a systematic review ofrandomized controlled trialsNick Sahlollbey1,2, Christopher Kai Seng Lee1, Afraah Shirin1, and Philip Joseph1,2*1McMaster University, Hamilton, Canada; and 2Population Health Research Institute (PHRI), Hamilton Health Sciences and McMaster University, Hamilton, Canada
Received 29 September 2019; revised 16 February 2020; accepted 18 February 2020
Aims To examine the impact of palliative care on acute care hospitalizations, survival, symptoms, and quality of life (QOL)in patients with advanced heart failure.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Methodsand results
We conducted a systematic search of publications through CENTRAL, CINAHL, EMBASE, and MEDLINE originallyup to July 2017, and then updated to June 2019. The study was registered (PROSPERO ID: CRD42017069685)prior to its initiation. Randomized controlled trials (RCTs) were included that tested an interdisciplinary palliativecare intervention (compared to usual care) primarily in a heart failure population. Main outcomes assessed werehospitalizations, mortality, QOL, and symptom burden. Ten independent RCTs were selected, representing a total of1050 participants (921 with a diagnosis of heart failure). Compared with usual care, palliative care interventions wereassociated with a substantial reduction in hospitalizations [odds ratio 0.56 (0.33–0.94); four trials; I2 = 27%], modestimprovement in QOL [standardized mean difference (SMD) 0.25; 95% con!dence interval (CI) 0.06–0.45; seventrials; I2 = 15%], and modest reduction in symptom burden (SMD !0.29; 95% CI !0.54–0.03; three trials; I2 = 15%).There was no clear adverse impact on mortality. Most studies had methodological limitations that increased the riskof biases.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Conclusion Compared to usual care, palliative care interventions substantially reduce hospitalizations, with no clear adverse effect
on survival. Effects on QOL and symptom burden appear to be modest, and indicate that further efforts to improvethese patient centred outcomes are needed.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Keywords Palliative care • Heart failure • Systematic review • Cardiovascular disease
IntroductionDespite advances in treatment, approximately half of patients diag-nosed with heart failure will die within 5 years.1 Advanced heartfailure is highly symptomatic, associated with a poor quality of life(QOL), and patients often require acute care hospitalizations forsymptom management.1,2 Given the growing burden of heart failureand its overall poor long-term prognosis, there is a need to bet-ter understand how to best manage patients with advanced heart
*Corresponding author. Population Health Research Institute, Hamilton Health Sciences and McMaster University, C3 110 DBCVSRI, Hamilton General Hospital, 237 Barton StEast, Hamilton, Ontario, L8L 2X2, Canada. Tel: +1 905 521-2100 ext. 40743, Fax: +1 905 297-3789, Email: [email protected]
....
....
....
....
....
....
...
failure. While palliative care was initially reserved for relieving suf-fering at the end-of-life, it is being increasingly integrated earlier inchronic disease management to improve symptoms and QOL.3–6
Palliative care strategies commonly utilize an interdisciplinaryapproach that focus on eight domains: structural processes, physi-cal, psychological, social, spiritual, cultural, ethical/legal, and care ofthe immediately dying.4 Compared to its use in some chronic dis-ease (i.e. cancer), the impact of palliative care in patients with heart
© 2020 European Society of Cardiology

2 N. Sahlollbey et al.
failure is less clear, with fewer randomized controlled trials (RCTs)conducted. Recent systematic reviews have also attempted to sum-marize the current data, but have reported varying results as to thebene!ts of palliative care on either objective (e.g. hospitalizations)or subjective (e.g. QOL) outcomes. Some reviews had includedboth observational and randomized trial data in their analyses,while in others the quanti!cation of effects for some outcomeswas limited, or fewer studies were available for analysis at the timeof review.7–10 To better quantify the effectiveness of palliative carein the heart failure population across a range of patient-centredoutcomes, we conducted an updated systematic review of pub-lished RCTs.11 The primary objective of this review was todetermine the effect of interdisciplinary palliative care serviceson four outcomes: symptom burden, QOL, hospitalizations, andmortality.12
MethodsStudy designWe conducted a systematic review and meta-analysis of RCTs compar-ing palliative care interventions to usual care in patients with advancedheart failure.11 The study was registered with PROSPERO prior to itsinitiation (PROSPERO ID: CRD42017069685).
Study selectionThe following databases were originally searched from their inceptionuntil July 2017, and then updated until June 2019: the Cochrane CentralRegister of Controlled Trials (CENTRAL), CINAHL, EMBASE, andMEDLINE (see online supplementary Appendix S1 for description of thesearch strategy). In addition, we searched reference lists of identi!edarticles and systematic reviews that had been screened for full textreview.
Selection criteriaStudies were selected for inclusion in our review based on the followingcriteria: (i) published RCTs, (ii) adult patients >18 years of age, (iii)included participants with advanced heart failure (studies of mixedchronic disease populations were included if >50% of the studypopulation was comprised of heart failure participants), (iv) tested aninterdisciplinary palliative care intervention (utilizing multiple types ofhealthcare providers that targeted multiple domains of palliative care)compared to a usual care group, and (v) examined at least one of thefollowing: death, hospitalization, QOL, or symptom burden. Studieswere excluded if they were not published in the English language, orthe intervention was not primarily focused on the heart failure patient(e.g. caregiver targeted interventions).
Data extractionTwo reviewers (N.S. and P.J.) independently evaluated the titles andabstracts of all articles identi!ed by the initial search and selected arti-cles for further full text review. Disagreements between the reviewerswere resolved through common consensus. ..
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
.. Risk of biasStudies were evaluated for risks of biases using a modi!ed versionof the Cochrane Risk of Bias Tool for Randomized Controlled Trials.Two reviewers (P.J. and C.L.) independently evaluated each study anddiscrepancies were resolved through common consensus (see onlinesupplementary Appendix S1 for further details).
Study outcomesWe studied four main patient-centred outcomes in our systematicreview: QOL, symptom burden, hospitalizations, and death. Sincedifferent QOL measurement tools used in different studies could varyin terms of their directionality, we adjusted scores so that higherscores consistently indicated better QOL in all studies. Similarly, weadjusted symptom burden scores so that higher scores indicatedgreater symptom burden. If the published data were incomplete orfurther clari!cations were needed, we attempted to contact theauthors to provide additional information.
Statistical analysisFor the meta-analysis of each outcome of interest, the DerSimonian–Laird random-effects model was used to calculate the inversevariance-based weighted, pooled treatment effect across studies. Forbinary outcomes (e.g. hospitalization and mortality) we generatedodds ratios (OR) and 95% con!dence intervals (CI). Since symptomsand QOL were reported using different scores across studies, we usedthe standardized mean difference (SMD) of each score at follow-up asthe measure of comparison. Based on prior literature, we used thefollowing thresholds to interpret effect sizes based on the SMD: 0.2was considered to be small, 0.5 considered moderate, and 0.8 con-sidered large.13 Heterogeneity between studies was measured usingthe methods described by Deeks and Higgins.14 If the I2 statistic valuedemonstrated signi!cant heterogeneity (de!ned as a value >50%),we planned to explore for potential causes of heterogeneity usingsubgroup analyses based on differences in study methodology (e.g.study size, inclusion of other conditions, and studies with a high riskof bias) and intervention type (e.g. setting of treatment). All analyseswere performed using the Cochrane Collaboration Review Manager(version 5.3, Cochrane Collaboration, Copenhagen, Denmark), andP< 0.05 was considered the threshold for statistical signi!cance.
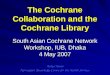
ResultsStudy selection and characteristicsAfter removing duplicate articles, our search identi!ed 2701 arti-cles (Figure 1). After the title and abstract review, 39 articles wereidenti!ed for full text review, and 10 independent RCTs meetingour criteria were ultimately selected, representing a total of 1050participants [921 (87.7%) with heart failure].15–26
Study selectionThe design, methods, and details for all included studies aresummarized in online supplementary Table S1. Seven trials wereconducted in North America, two in Europe, and one in Asia.Three studies were multicentre studies. We assessed how each
© 2020 European Society of Cardiology

Impact of palliative care in patients with heart failure 3
Figure 1 Study selection. RCT, randomized controlled trial.
intervention addressed each of the eight domains of palliativecare (although not explicitly stated in the studies, we assumedall addressed care of the immediately dying given the nature ofthe intervention). In all 10 studies, palliative care interventionsaddressed at least six of eight key palliative care domains, and ninestudies addressed at least seven domains. All studies utilized aninterdisciplinary approach that included at least a physician as wellas a nurse. Interventions primarily occurred in the hospital settingin three studies, in the outpatient setting in two studies, and in bothsettings in !ve studies (online supplementary Table S1).
With regard to the characteristics of the populations includedin each study, seven studies only included participants with heartfailure (with three studies including a majority with heart failure).Mean age of participants for each study ranged from between65.4 years to 81.9 years, and 545 (51.9%) of included participantswere male. In studies that provided data on New York HeartAssociation (NYHA) functional class, 452 of 513 (88%) partici-pants were in NYHA class III or IV. In nine studies, the durationof follow-up was between 3–6 months, and in one study it was2 weeks.
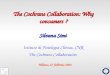
Risk of biasA summary of the risks of methodological biases for eachstudy is provided in Figure 2. All studies were at high risk forperformance-related bias due to the inability to blind participants ..
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
.. or personnel to the intervention groups (which was not feasibledue to the nature of palliative care interventions). All studies werealso at high risk of detection bias for subjective outcomes (i.e. QOLand symptom burden) because blinding participants was not possi-ble. Most studies had an unclear risk of selection-related bias dueto inadequate descriptions of allocation concealment. Funnel plotswere not reported because outcomes were reported on less than10 studies.
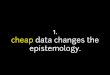
HospitalizationsThe proportion of participants who required at least one hospi-talization was available in four studies (356 patients). Across thesestudies, 159 of 356 (45%) participants required at least one hospi-talization during follow-up (68 in palliative care vs. 91 in usual care).Palliative care interventions reduced hospitalizations (OR 0.56,95% CI 0.33–0.94; I2 = 27%) compared to usual care (Figure 3).
MortalityMortality data were available in nine studies (954 patients)(Figure 4). A total of 159 (17%) participants died during follow-up.There was no clear impact on mortality with palliative care inter-ventions compared to usual care (OR 1.30, 95% CI 0.80–2.09;I2 = 33%).
© 2020 European Society of Cardiology

4 N. Sahlollbey et al.
Figure 2 Risk of bias among included randomized controlledtrials. QOL, quality of life.
Quality of lifeSeven studies reported follow-up mean QOL scores using avalidated questionnaire and were included in our meta-analysis(Figure 5 and online supplementary Table S2). In these studies, pal-liative care was associated with a modest improvement in QOL(SMD 0.25, 95% CI 0.06–0.45; I2 = 15%) compared to usual care. Inthree studies, an alternative questionnaire was also used to assessQOL, and substituting the alternative questionnaire scores yieldedsimilar results (online supplementary Figure S1).
Symptom burdenThree studies reported mean total symptom burden scores infollow-up using a validated questionnaire and were included in ourmeta-analysis (Figure 6 and online supplementary Table S3). In these ..
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
.. studies, palliative care was associated with a small reduction insymptom burden (SMD !0.29, 95% CI !0.54–0.03; I2 = 15%). Forindividual symptoms, there was no clear impact of palliative care onanxiety, dyspnoea, or pain, although few studies were available formeta-analysis of individual outcomes (online supplementary FiguresS2–S5). Palliative care appeared to be associated with a lower riskof depression based on a limited number of studies (SMD !0.28,95% CI !0.54–0.02; I2 = 0%).
DiscussionIn this systematic review, we examined the impact of palliative careon a range of clinical and patient-centred outcomes. The advancedheart failure population studied in our systematic review was athigh risk for adverse outcomes. Among studies that reportedclinical outcomes, 45% of participants required an acute carehospitalization, and 17% died in studies mostly conducted for6 months or less. In this context, palliative care was very effectiveat reducing acute care hospitalizations in the advanced heart failurepopulation. Determining whether palliative care has an adverseimpact on mortality is also necessary as this may in"uence decisionsby healthcare providers to introduce it, or by patients to acceptit. Importantly, we did not observe any clear adverse impact onmortality with the initiation of palliative care.
Palliative care interventions also improved two key subjectivepatient-centred outcomes: QOL and symptom burden. However,our !ndings also suggest that the impact of palliative care onthese outcomes was relatively modest. This may re"ect the highburden of persistent symptoms that advanced heart failure patientsexperience despite available therapies. Alternatively, the palliativecare interventions studied may not have completely addressedthe complex needs of the advanced heart failure population.For example, studies suggest that pain is a common but poorlymanaged symptom of advanced heart failure.27–29 In keeping, wefound that palliative interventions had no appreciable impact onpain symptoms, albeit few studies reported this symptom as anoutcome. Furthermore, while heart failure patients report a highburden of symptoms and functional disability with heart failure,they do not necessarily equate heart failure with a chronic andlife-limiting disease.30 In this context, key domains in palliative care,such as patient beliefs, goals of care, psychosocial and spiritualneeds, may differ in the advanced heart failure population whencompared with other chronic diseases that portend a similarsymptom burden (e.g. cancer), but there is little data to informhow to best address these factors in patients with advanced heartfailure.
Several methodological limitations in these studies also need tobe considered. First, the number of palliative care studies con-ducted in the heart failure population remains few, and manywere small in size (i.e. less than 100 participants), both of whichcould result in an overestimation of treatment effects. Second,studies were of a short duration, and it is unclear whether theeffects of palliative care on both subjective (i.e. QOL, symptomburden) and objective outcomes (i.e., hospitalizations, mortality)would be sustained over a longer duration of time. Although mor-tality was high in this population, most heart failure participants
© 2020 European Society of Cardiology

Impact of palliative care in patients with heart failure 5
Figure 3 Risk of at least one hospitalization during follow-up with palliative care vs. usual care. CI, con!dence interval.
Figure 4 Risk of death with palliative care vs. usual care. CI, con!dence interval.
were still alive upon study completion, signalling the need for addi-tional RCTs in the advanced heart failure population to ensure thatthe effects of palliative care remain consistent over time, espe-cially if it is now being considered earlier in advanced heart fail-ure management. Third, many subjective patient-centred outcomes(i.e. pain, dyspnoea, depression, anxiety, spiritual needs) werenot consistently examined across studies, but are necessary to ..
....
....
....
....
. better tailor interventions to the speci!c needs of the heart failurepopulation.
Some limitations of our review also need to be considered. Werestricted our search to published studies, which could result inbias reporting of favourable results. However, among the publishedstudies, pre-speci!ed outcomes were mostly reported. Althoughwe did not see a signi!cant effect of palliative care on symptoms of
Figure 5 Quality of life with palliative care vs. usual care. Quality of life was measured by the EuroQol-5D (Brannstrom 2014; Denvir 2016),Kansas City Cardiomyopathy Questionnaire (O’Donnell 2018, Rogers 2017), Minnesota Living with Heart Failure Questionnaire (O’Riordan2019, Sidebottom 2015), and the McGill Quality of Life Questionnaire for Hong Kong (MQOL-HK) (Wong 2015). If necessary, studies correctedfor directionality to allow higher scores to represent better quality of life. CI, con!dence interval; SD, standard deviation.
© 2020 European Society of Cardiology

6 N. Sahlollbey et al.
Figure 6 Total symptom burden with palliative care vs. usual care. Total symptom burden was measured by the Edmonton SymptomAssessment Scale in all studies. Sidebottom (2015) reported the mean change from baseline to 3 months, which was subtracted from eachbaseline score; standard deviations (SD) were not reported for 3-month scores and were imputed from Denvir (2016) as both studies usedthe same measurement scale and had the same time periods between baseline and !nal value measurement. CI, con!dence interval.
dyspnoea, pain and anxiety, these observations are limited by thesmall number of studies that were suitable for meta-analysis. Somestudies reported data on subjective outcomes, but without meanvalues, and thus could not be included in our quantitative analysesto characterize effect sizes.
There are several important implications of our !ndings froma clinical perspective and for future research. First, palliative careappears to be relatively safe to implement in advanced heart failurepatients, and it is effective at transitioning heart failure care fromacute management to a greater focus on QOL. However, as therole of palliative care grows in heart failure management, thereis also a need for more clinical trials to determine how it canbest be utilized to address the complex needs of heart failurepatients. From the patient perspective, these include the mostappropriate time to initiate palliative care; how to further improvepatient-centred outcomes such as QOL and symptom burden;how best to address psychosocial factors as patients progressalong the heart failure continuum; and the role of more complexpalliative interventions (such as inotropic support) as part of end-oflife care. At the system level, the optimal methods of deliveringpalliative care services to the advanced heart failure population (e.g.specialist-based vs. primary care models, the incremental value ofdigital or e-Health technologies) need to be better understood.
ConclusionsData from a small number of clinical trials suggest that pallia-tive care is very effective at reducing acute care hospitalizationsin patients with advanced heart failure, but current interven-tions appear only modestly effective at improving other importantpatient-centred outcomes. More high-quality studies are needed tounderstand how best to apply palliative care in the advanced heartfailure population.Con!ict of interest: none declared.
Supplementary InformationAdditional supporting information may be found online in theSupporting Information section at the end of the article.Appendix S1: Supporting Information ..
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
. Table S1. Characteristics of included studies – design, interven-tions, and population.Table S2. Summary of quality of life in included studies.Table S3. Summary of symptom burden in included studies.Figure S1. Alternative summary of quality of life in includedstudies.Figure S2. Summary of dyspnea in included studies.Figure S3. Summary of pain in included studies.Figure S4. Summary of anxiety in included studies.Figure S5. Summary of depression in included studies.
References1. Roger VL, Weston SA, Red!eld MM, Hellermann-Homan JP, Killian J, Yawn BP,
Jacobsen SJ. Trends in heart failure incidence and survival in a community-basedpopulation. JAMA 2004;292:344–350.
2. Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, DasSR, de Ferranti S, Després JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR,Jiménez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH,Magid DJ, McGuire DK, Mohler ER, Moy CS, Muntner P, Mussolino ME, Nasir K,Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ,Rosamond W, Sorlie PD, Stein J, Tow!ghi A, Turan TN, Virani SS, Woo D,Yeh RW, Turner MB; Writing Group Members, American Heart AssociationStatistics Committee, Stroke Statistics Subcommittee. Executive summary: heartdisease and stroke statistics—2016 update: a report from the American HeartAssociation. Circulation 2016;133:447–454.
3. Goodlin SJ. Palliative care in congestive heart failure. J Am Coll Cardiol2009;54:386–396.
4. Ferrell BR, Twaddle ML, Melnick A, Meier DE. National Consensus ProjectClinical Practice Guidelines for Quality Palliative Care Guidelines, 4th edition.J Palliat Med 2018;21:1684–1689.
5. Bakitas M, Lyons KD, Hegel MT, Balan S, Brokaw FC, Seville J, Hull JG, Li Z,Tosteson TD, Byock IR, Ahles TA. Effects of a palliative care intervention onclinical outcomes in patients with advanced cancer: the Project ENABLE IIrandomized controlled trial. JAMA 2009;302:741–749.
6. Kavalieratos D, Corbelli J, Zhang D, Dionne-Odom JN, Ernecoff NC, Hanmer J,Hoydich ZP, Ikejiani DZ, Klein-Fedyshin M, Zimmermann C, Morton SC, ArnoldRM, Heller L, Schenker Y. Association between palliative care and patient andcaregiver outcomes. JAMA 2016;316:2104–2114.
7. Diop MS, Rudolph JL, Zimmerman KM, Richter MA, Skarf LM. Palliative care inter-ventions for patients with heart failure: a systematic review and meta-analysis.J Palliat Med 2016;20:84–92.
8. Zhou K, Mao Y. Palliative care in heart failure: a meta-analysis of randomizedcontrolled trials. Herz 2019;44:440–444.
9. Xu Z, Chen L, Jin S, Yang B, Chen X, Wu Z. Effect of palliative care for patientswith heart failure. Int Heart J 2018;59:503–509.
10. Datla S, Verberkt CA, Hoye A, Janssen DJ, Johnson MJ. Multi-disciplinary palliativecare is effective in people with symptomatic heart failure: a systematic review andnarrative synthesis. Palliat Med 2019;33:1003–1016.
© 2020 European Society of Cardiology

Impact of palliative care in patients with heart failure 7
11. Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions, ver-sion 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Availablefrom www.handbook.cochrane.org.
12. Stygles N, Klein-Fedyshin M, Kavalieratos D. Response to the article “Palliativecare interventions for patients with heart failure: a systematic review andmeta-analysis”. J Palliat Med 2017;20:582–583.
13. Cohen J. Statistical power analysis for the behavioral sciences. New York: Routledge;2013. p. 579.
14. Deeks J, Higgins JP. Statistical algorithms in Review Manager 5. 2007.15. Aiken LS, Butner J, Lockhart CA, Volk-Craft BE, Hamilton G, Williams FG.
Outcome evaluation of a randomized trial of the PhoenixCare intervention:program of case management and coordinated care for the seriously chronicallyill. J Palliat Med 2006;9:111–126.
16. Brännström M, Boman K. Effects of person-centred and integrated chronic heartfailure and palliative home care. PREFER: a randomized controlled study. EurJ Heart Fail 2014;16:1142–1151.
17. Denvir MA, Cudmore S, Highet G, Robertson S, Donald L, Stephen J, Haga K,Hogg K, Weir CJ, Murray SA, Boyd K. Phase 2 randomised controlled trial andfeasibility study of future care planning in patients with advanced heart disease.Sci Rep 2016;6:24619.
18. Hopp FP, Zalenski RJ, Waselewsky D, Burn J, Camp J, Welch RD, Levy P.Results of a hospital-based palliative care intervention for patients with an acuteexacerbation of chronic heart failure. J Card Fail 2016;22:1033–1036.
19. O’Donnell AE, Schaefer KG, Stevenson LW, DeVoe K, Walsh K, Mehra MR,Desai AS. Social worker-aided palliative care intervention in high-risk patientswith heart failure (SWAP-HF): a pilot randomized clinical trial. JAMA Cardiol2018;3:516–519.
20. O’Riordan DL, Rathfon MA, Joseph DM, Hawgood J, Rabow MW, Dracup KA, DeMarco T, Pantilat SZ. Feasibility of implementing a palliative care intervention forpeople with heart failure: learnings from a pilot randomized clinical trial. J PalliatMed 2019;22:1583–1588. ..
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
... 21. Pantilat SZ. Hospital-based palliative medicine consultation: a randomized con-
trolled trial. Arch Intern Med 2010;170:2038–2040.22. Sidebottom AC, Jorgenson A, Richards H, Kirven J, Sillah A. Inpatient palliative
care for patients with acute heart failure: outcomes from a randomized trial.J Palliat Med 2015;18:134–142.
23. Rogers JG, Patel CB, Mentz RJ, Granger BB, Steinhauser KE, Fiuzat M, AdamsPA, Speck A, Johnson KS, Krishnamoorthy A, Yang H, Anstrom KJ, Dodson GC,Taylor DH, Kirchner JL, Mark DB, O’Connor CM, Tulsky JA. Palliative care inheart failure. J Am Coll Cardiol 2017;70:331–341.
24. Mentz RJ, O’Connor CM, Granger BB, Yang H, Patel CB, Steinhauser KE, FiuzatM, Johnson KS, Anstrom KJ, Dodson GC, Taylor DH Jr, Mark DB, Tulsky JA,Rogers JG. Palliative care and hospital readmissions in patients with advancedheart failure: insights from the PAL-HF trial. Am Heart J 2018;204:202-204.
25. Wong FK, Ng AY, Lee PH, Lam PT, Ng JS, Ng NH, Sham MM. Effects of atransitional palliative care model on patients with end-stage heart failure: arandomised controlled trial. Heart 2016;102:1100–1108.
26. Wong FK, So C, Ng AY, Lam PT, Ng JS, Ng NH, Chau J, Sham MM.Cost-effectiveness of a transitional home-based palliative care program forpatients with end-stage heart failure. Palliat Med 2018;32:476–484.
27. Kavalieratos D, Gelfman LP, Tycon LE, Riegel B, Bekelman DB, Ikejiani DZ,Goldstein N, Kimmel SE, Bakitas MA, Arnold RM. Palliative care in heartfailure: rationale, evidence, and future priorities. J Am Coll Cardiol 2017;70:1919–1930.
28. Goebel JR, Doering LV, Shugarman LR, Asch SM, Sherbourne CD, Lanto AB,Evangelista LS, Nyamathi AM, Maliski SL, Lorenz KA. Heart failure: the hiddenproblem of pain. J Pain Symptom Manage 2009;38:698–707.
29. Evangelista LS, Sackett E, Dracup K. Pain and heart failure: unrecognized anduntreated. Eur J Cardiovasc Nurs 2009;8:169–173.
30. Klindtworth K, Oster P, Hager K, Krause O, Bleidorn J, Schneider N. Living withand dying from advanced heart failure: understanding the needs of older patientsat the end of life. BMC Geriatr 2015;15:1–11.
© 2020 European Society of Cardiology