Embed Size (px)
Citation preview
ORIGINAL RESEARCH
The Impact of Capsaicin Intake on Risk of Developing GastricCancers: A Meta-Analysis
Noel Pabalan & Hamdi Jarjanazi & Hilmi Ozcelik
# Springer Science+Business Media New York 2014
AbstractBackground Reported associations of capsaicin with gastriccancer development have been conflicting. Here, we examine10 published articles that explore these associations using2,452 cases and 3,996 controls.Methods We used multiple search strategies in MEDLINEthrough PubMed to seek for suitable articles that had case-control design with gastric cancer as outcome.Results The outcomes of our study shows protection (oddsratio [OR] 0.55, P=0.003) and susceptibility (OR 1.94, P=0.0004), both significant with low and medium-high intake ofcapsaicin, respectively, although under relatively heteroge-neous conditions (Pheterogeneity=<0.0001). Outlier analysis re-sulted in loss of overall heterogeneity (P=0.14) without af-fecting the pooled ORs. Among the subgroups, low intakeelicited protection in both Korean (OR 0.37) and Mexican(OR 0.63) populations while high intake rendered these sub-groups susceptible (OR 2.96 and OR 1.57, respectively).These subgroup values were highly significant (P=0.0001–0.01) obtained in heterogeneous conditions (Pheterogeneity<0.0001–0.04). The homogeneous (Pheterogeneity=0.27–0.37)H. pylori (OR 0.60 and 1.69) effects were highly significant
(P<0.001) in the low and medium-high intake analyses, re-spectively. Given outcomes from the tests of interaction, highcapsaicin intake is significantly different from the protectionthat low consumption offers.Conclusions This meta-analysis implies moderation in capsa-icin consumption in order to derive its protective benefits.
Keywords Gastric cancer . Capsaicin intake . Case-control .
H. pylori
Introduction
Gastric cancer incidence rates vary by more than 20-foldaround the world, and the differences in dietary patterns mayexplain much of the variation in rates across countries [1, 2].Dietary habits characterized with high intake of salty, smoked,pickled, preserved foods and nitrites, and higher intake ofcooked rather than fresh vegetables have been implicated toimpact upon susceptibility to gastric cancers [3]. High intakeof fresh fruits, vegetables, and antioxidants has, in contrast,provided a beneficial effect for reducing risk of gastric cancers[4]. Hot red chili peppers, which belong to the plant genusCapsicum, are among the most heavily and frequently con-sumed spices throughout the world. The principal pungentingredient of the red-hot chili peppers is the phenolic sub-stance capsaicin (8-methyl-N-vanillyl-6-nonenamide), the ef-fect of which appears to result from the activation of sensoryafferent neurons in the stomach, and is mediated by variousphysiological functions, such as mucosal blood flow [5, 6],mucus secretion [7], and bicarbonate secretions [8].
The role of capsaicin in carcinogenic processes is quitecontroversial. While it has been suspected to be a carcinogen,cocarcinogen, or tumor promoter [9, 10], others have reportedit to be chemopreventive and chemotherapeutic [11, 12].Although the action of capsaicin may still be unclear, one
Hilmi Ozcelik Deceased, (May, 2013)
N. PabalanSchool of Natural Sciences and Nursing, Saint Louis University,2600 Baguio City, Philippines
H. Jarjanazi (*)Environmental Monitoring and Reporting Branch, Ontario Ministryof the Environment, 125 Resources Road, Toronto, ON, CanadaM9P 3V6e-mail: [email protected]
H. OzcelikFred A. Litwin Centre for Cancer Genetics, Samuel LunenfeldResearch Institute, Mount Sinai Hospital, 60 Murray St. RoomL6-303, Box 29, Toronto, ON M5T 3L9, Canada
J Gastrointest CancDOI 10.1007/s12029-014-9610-2

possible mechanism is the interaction of this compound withHelicobacter pylori (H. pylori), the bacteria that colonize thestomach adjacent to gastric epithelial cells [13] and are con-sidered a human carcinogen [14].
Capsaicin has been shown to alter expression of tumorforming genes by mediating overexpression of p53 and/or c-myc in a stomach cancer cell line [15]. Furthermore, thevanilloid receptor subtype 1 responsible for capsaicin actionwas found expressed peripherally in gastric mucosal epithelialcells, therefore playing a role in cell protection [16]. It hasbeen demonstrated that capsaicin inhibits mutagenicity andDNA binding of some chemical carcinogens, possibly bysuppressing their metabolic activation [17, 18]. Its antiprolif-erative activity has been ascribed to its ability to induceapoptosis [15, 19]. Capsaicin-induced apoptosis has beendemonstrated in various cultured cells (squamous cell carci-noma and T cells) where it inhibited mitochondrial respiration[20] and increased reactive oxygen species [21]. In addition,capsaicin has been found to preferentially repress the growthof some transformed mouse and human cells including HeLa,ovarian carcinoma, and mammary adenocarcinoma [22, 23].
Studies of gastric cancers investigating the intake of cap-saicin have generated a spectrum of differing outcomes. Cap-saicin containing kimchi [24] has been reported as risk con-ferring for [25] and protective against [26] gastric cancer. Astudy has shown visible gastric bleeding and mucosalmicrobleeding after intake of red and black pepper [27]. Onthe other hand, another study showed no mucosal erosions orother abnormalities after consumption of ground jalapeñopeppers, even when placed directly in the stomach [28]. Otherstudies have also shown that capsaicin protects the gastricmucosa of animals and humans against various kinds ofdamage [29–31].
To date, evidence accumulating from a number ofstudies suggests association of capsaicin with gastriccancers although discrepancies among the findings exist.Such discrepancies prompted us to carry the meta-analysis of capsaicin to understand its role in the devel-opment of gastric cancers.
Materials and Methods
Selection of Studies and Data Extraction
We searched MEDLINE using PubMed employing threestrategies with the following search terms: (1) “diet” and“stomach cancer”, (2) “lifestyle” and “stomach cancer”, and(3) “chili” and “gastric cancer”, which yielded 321, 83, andnine articles, respectively. The electronic search was supple-mented with checking of reference lists from the identifiedarticles. All studies must meet the following criteria: (1) case-control design, (2) outcome is gastric cancer, and (3) at least
two comparison groups. The exclusion criteria were the fol-lowing: (1) duplicate data; (2) reviews, reports, clinical trials,and genetic and cell studies; and (3) insufficient data. Twoinvestigators independently extracted data and reached con-sensus on all the items. The following information was ob-tained from each publication: first author’s name, publishedyear, country of origin, study design, matching criteria, andnumber of cases and controls as well as degree of capsaicinintake. Studies are included if they have data on low, medium,and high intake of capsaicin (chili) from which odds ratios(OR) and 95 % confidence intervals can be calculated. Nu-merical data were extracted from the studies that categorizedconsumption in terms of frequency or intensity of capsaicineffects.
Quality Assessment of the Studies
Quality of the studies was evaluated with use of theNewcastle-Ottawa Scale (NOS) [32]. Each study was assessedbased on three broad perspectives: selection, comparability,and exposure with a score ranging from 0 to 9. Studies with ascore ≥7 were considered to be of high quality.
Meta-Analysis
We estimated OR and 95 % confidence intervals of gastriccancer associated with intake of capsaicin. Raw data,without adjustment, were used to calculate study-specificestimates of the OR. Pooled ORs were obtained usingeither the fixed (used in the absence of heterogeneity[33]) or random (used in its presence [34]) effects models.We also examined effect of capsaicin in the milieu of Hpylori infection given provision of independent data fromfour studies [35–38]. We performed subgroup analysisusing geography as variable. Heterogeneity between stud-ies was estimated using the χ2-based Q test [39], signif-icance of which was set at P<0.10 [40] and its sourcesidentified using the Galbraith plot [41, 42].
Publication bias was statistically evaluated with Egger’sregression asymmetry test which detects whether the inter-cept deviates significantly from zero in a regression of thestandardized effect estimates against their precision [43].The Begg-Mazumdar diagnostic (nonparametric τ correla-tion coefficient) was also applied to evaluate whether themagnitude of observed association was related to the var-iance of each study [44]. Data were analyzed using ReviewManager 5.1 (Copenhagen: The Nordic Cochrane Centre,The Cochrane Collaboration, 2011), SigmaStat 2.03, andSigmaPlot 11.0. Significance was set at a P value of <0.05throughout except in heterogeneity estimation. All Pvalues were two-tailed.
J Gastrointest Canc
Results
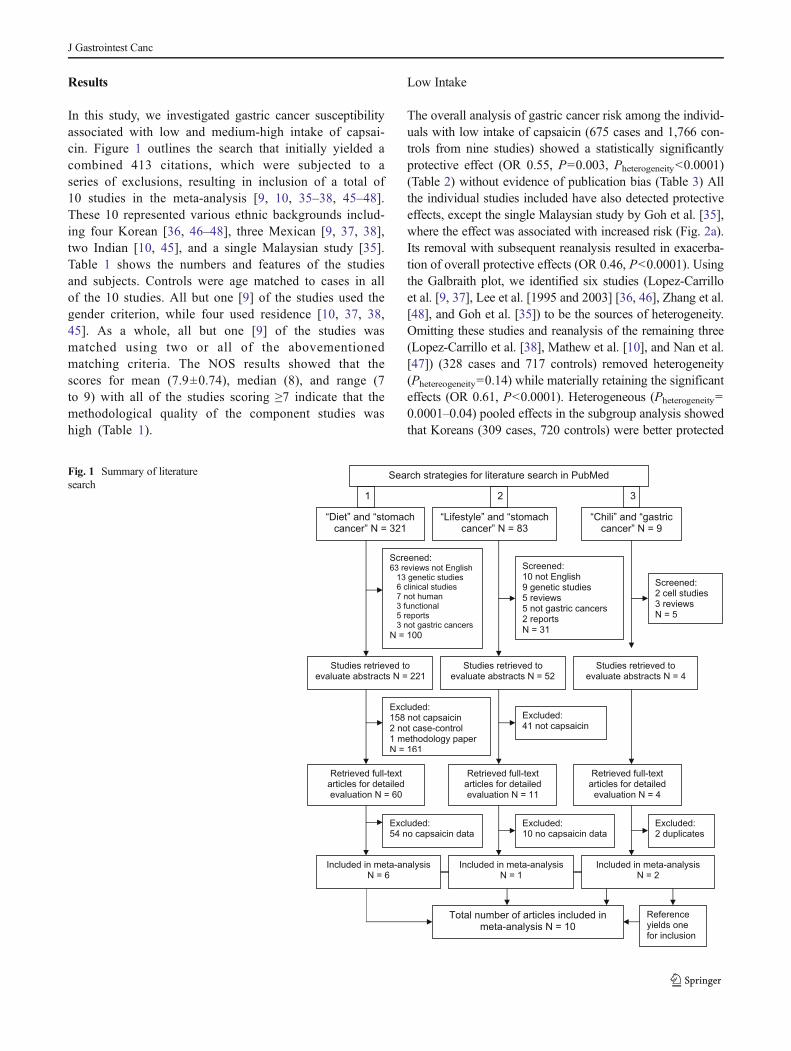
In this study, we investigated gastric cancer susceptibilityassociated with low and medium-high intake of capsai-cin. Figure 1 outlines the search that initially yielded acombined 413 citations, which were subjected to aseries of exclusions, resulting in inclusion of a total of10 studies in the meta-analysis [9, 10, 35–38, 45–48].These 10 represented various ethnic backgrounds includ-ing four Korean [36, 46–48], three Mexican [9, 37, 38],two Indian [10, 45], and a single Malaysian study [35].Table 1 shows the numbers and features of the studiesand subjects. Controls were age matched to cases in allof the 10 studies. All but one [9] of the studies used thegender criterion, while four used residence [10, 37, 38,45]. As a whole, all but one [9] of the studies wasmatched using two or all of the abovementionedmatching criteria. The NOS results showed that thescores for mean (7.9±0.74), median (8), and range (7to 9) with all of the studies scoring ≥7 indicate that themethodological quality of the component studies washigh (Table 1).
Low Intake
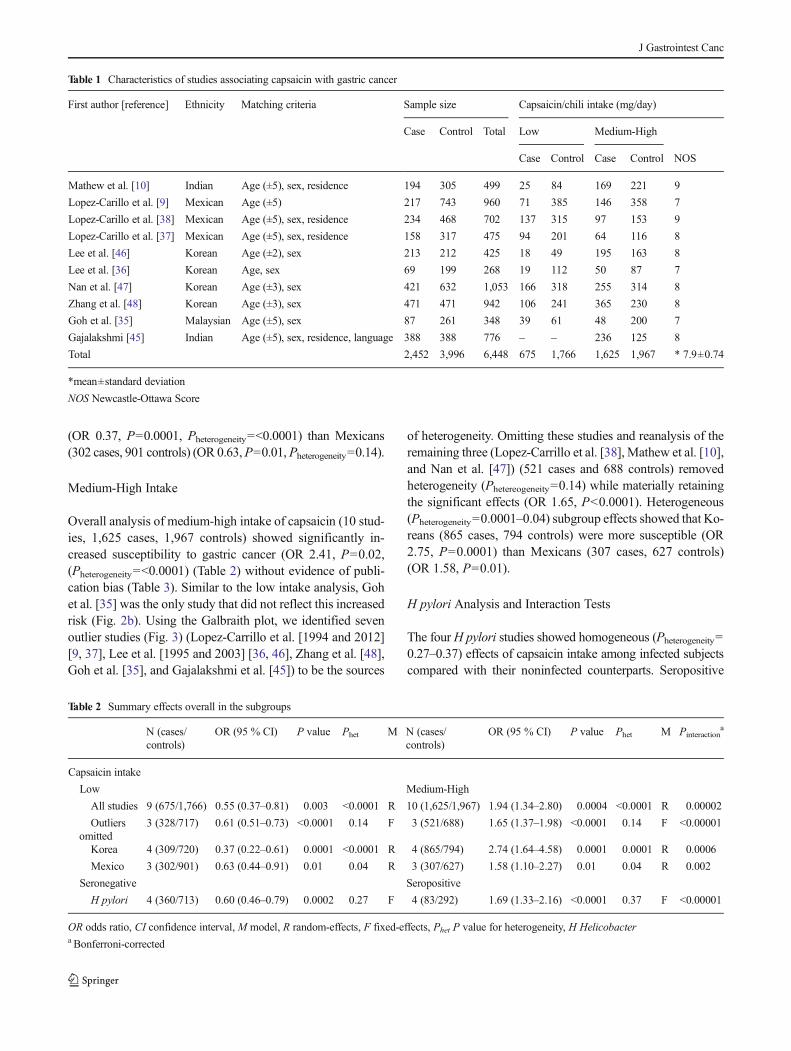
The overall analysis of gastric cancer risk among the individ-uals with low intake of capsaicin (675 cases and 1,766 con-trols from nine studies) showed a statistically significantlyprotective effect (OR 0.55, P=0.003, Pheterogeneity<0.0001)(Table 2) without evidence of publication bias (Table 3) Allthe individual studies included have also detected protectiveeffects, except the single Malaysian study by Goh et al. [35],where the effect was associated with increased risk (Fig. 2a).Its removal with subsequent reanalysis resulted in exacerba-tion of overall protective effects (OR 0.46, P<0.0001). Usingthe Galbraith plot, we identified six studies (Lopez-Carrilloet al. [9, 37], Lee et al. [1995 and 2003] [36, 46], Zhang et al.[48], and Goh et al. [35]) to be the sources of heterogeneity.Omitting these studies and reanalysis of the remaining three(Lopez-Carrillo et al. [38], Mathew et al. [10], and Nan et al.[47]) (328 cases and 717 controls) removed heterogeneity(Phetereogeneity=0.14) while materially retaining the significanteffects (OR 0.61, P<0.0001). Heterogeneous (Pheterogeneity=0.0001–0.04) pooled effects in the subgroup analysis showedthat Koreans (309 cases, 720 controls) were better protected
Fig. 1 Summary of literaturesearch
J Gastrointest Canc
(OR 0.37, P=0.0001, Pheterogeneity=<0.0001) than Mexicans(302 cases, 901 controls) (OR 0.63,P=0.01,Pheterogeneity=0.14).
Medium-High Intake
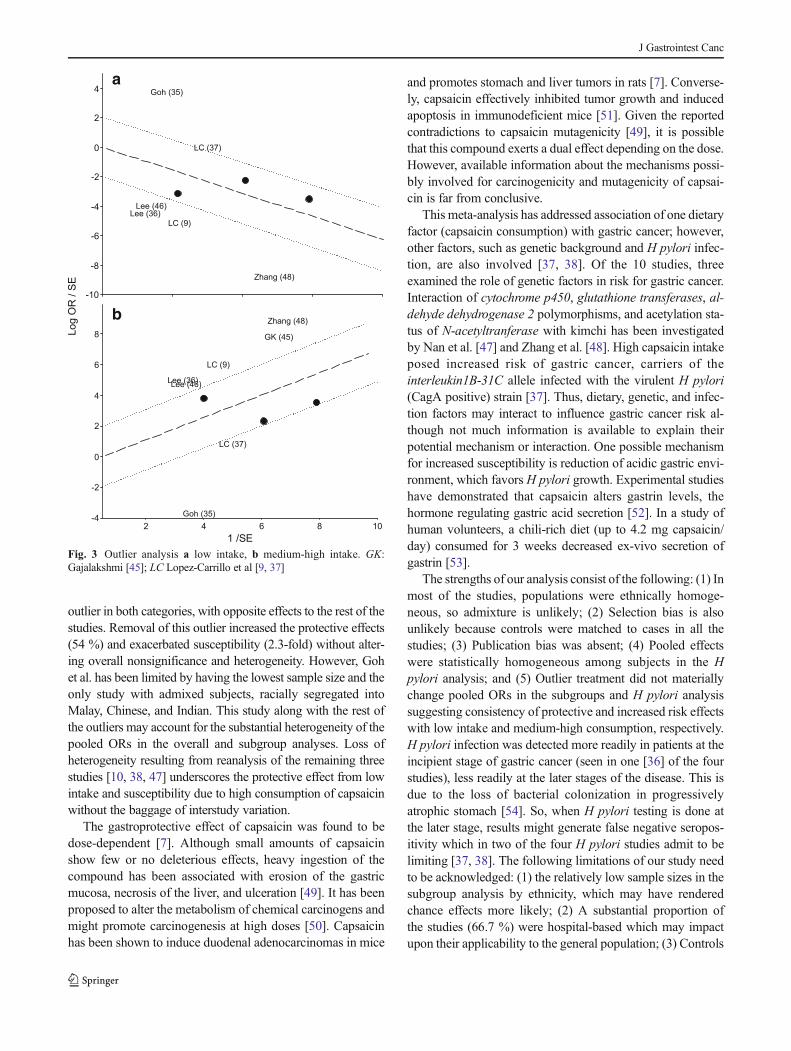
Overall analysis of medium-high intake of capsaicin (10 stud-ies, 1,625 cases, 1,967 controls) showed significantly in-creased susceptibility to gastric cancer (OR 2.41, P=0.02,(Pheterogeneity=<0.0001) (Table 2) without evidence of publi-cation bias (Table 3). Similar to the low intake analysis, Gohet al. [35] was the only study that did not reflect this increasedrisk (Fig. 2b). Using the Galbraith plot, we identified sevenoutlier studies (Fig. 3) (Lopez-Carrillo et al. [1994 and 2012][9, 37], Lee et al. [1995 and 2003] [36, 46], Zhang et al. [48],Goh et al. [35], and Gajalakshmi et al. [45]) to be the sources
of heterogeneity. Omitting these studies and reanalysis of theremaining three (Lopez-Carrillo et al. [38], Mathew et al. [10],and Nan et al. [47]) (521 cases and 688 controls) removedheterogeneity (Phetereogeneity=0.14) while materially retainingthe significant effects (OR 1.65, P<0.0001). Heterogeneous(Pheterogeneity=0.0001–0.04) subgroup effects showed that Ko-reans (865 cases, 794 controls) were more susceptible (OR2.75, P=0.0001) than Mexicans (307 cases, 627 controls)(OR 1.58, P=0.01).
H pylori Analysis and Interaction Tests
The fourH pylori studies showed homogeneous (Pheterogeneity=0.27–0.37) effects of capsaicin intake among infected subjectscompared with their noninfected counterparts. Seropositive
Table 1 Characteristics of studies associating capsaicin with gastric cancer
First author [reference] Ethnicity Matching criteria Sample size Capsaicin/chili intake (mg/day)
Case Control Total Low Medium-High
Case Control Case Control NOS
Mathew et al. [10] Indian Age (±5), sex, residence 194 305 499 25 84 169 221 9
Lopez-Carillo et al. [9] Mexican Age (±5) 217 743 960 71 385 146 358 7
Lopez-Carillo et al. [38] Mexican Age (±5), sex, residence 234 468 702 137 315 97 153 9
Lopez-Carillo et al. [37] Mexican Age (±5), sex, residence 158 317 475 94 201 64 116 8
Lee et al. [46] Korean Age (±2), sex 213 212 425 18 49 195 163 8
Lee et al. [36] Korean Age, sex 69 199 268 19 112 50 87 7
Nan et al. [47] Korean Age (±3), sex 421 632 1,053 166 318 255 314 8
Zhang et al. [48] Korean Age (±3), sex 471 471 942 106 241 365 230 8
Goh et al. [35] Malaysian Age (±5), sex 87 261 348 39 61 48 200 7
Gajalakshmi [45] Indian Age (±5), sex, residence, language 388 388 776 – – 236 125 8
Total 2,452 3,996 6,448 675 1,766 1,625 1,967 * 7.9±0.74
*mean±standard deviation
NOS Newcastle-Ottawa Score
Table 2 Summary effects overall in the subgroups
N (cases/controls)
OR (95 % CI) P value Phet M N (cases/controls)
OR (95 % CI) P value Phet M Pinteractiona
Capsaicin intake
Low Medium-High
All studies 9 (675/1,766) 0.55 (0.37–0.81) 0.003 <0.0001 R 10 (1,625/1,967) 1.94 (1.34–2.80) 0.0004 <0.0001 R 0.00002
Outliersomitted
3 (328/717) 0.61 (0.51–0.73) <0.0001 0.14 F 3 (521/688) 1.65 (1.37–1.98) <0.0001 0.14 F <0.00001
Korea 4 (309/720) 0.37 (0.22–0.61) 0.0001 <0.0001 R 4 (865/794) 2.74 (1.64–4.58) 0.0001 0.0001 R 0.0006
Mexico 3 (302/901) 0.63 (0.44–0.91) 0.01 0.04 R 3 (307/627) 1.58 (1.10–2.27) 0.01 0.04 R 0.002
Seronegative Seropositive
H pylori 4 (360/713) 0.60 (0.46–0.79) 0.0002 0.27 F 4 (83/292) 1.69 (1.33–2.16) <0.0001 0.37 F <0.00001
OR odds ratio, CI confidence interval, M model, R random-effects, F fixed-effects, Phet P value for heterogeneity, H Helicobactera Bonferroni-corrected
J Gastrointest Canc
patients (83 cases, 292 controls) were highly susceptible (OR1.69, P<0.0001) while seronegative subjects (360 cases, 713controls) were significantly protected (OR 0.60, P=0.0002).All tests of interaction between low and high consumption ofcapsaicin, overall and in the subgroups remained significantafter Bonferroni correction treatment (Table 2).
Discussion
With a sample size of over 6,400 from 10 published case-control studies, this meta-analysis demonstrates significant as-sociations between capsaicin intake and gastric cancer with a
45% protective and 1.9-fold increased risk effects with low andhigh consumption, respectively. The gastric cancer risk effectsassociated with low and medium-high intake were exacerbatedamong Koreans (63 % protection and 2.7-fold susceptibility)and modulated in theMexican population (37% protection and1.6-fold increased risk). In the medium-high intake category,the Korean studies all point to increased risk that ranged from1.6-fold to 3.8-fold with high consumption [36, 47, 48]. Sim-ilarly, the Mexican study, Lopez-Carrillo et al. [9] (17-fold) andthe Indian, Mathew et al. [10] (7.4-fold) studies showed thehighest study-specific increased risks incriminating capsaicinas a susceptibility factor for gastric cancer. Given outcomesfrom the tests of interaction, high capsaicin intake is signifi-cantly different from the protection that low consumptionoffers. To the best of our knowledge, this is the first study thatexamines association of capsaicin with gastric cancer using themeta-analysis approach.
Using various methodologies, we have identified outliers inboth low and medium-high categories, the removal of whichgreatly improved the heterogeneity, where outcomes remainedconsistent (39 % protection and 1.7-fold increased risk).Among all the studies, Goh et al. [35] represented the major
Table 3 Tests for publication bias
Egger regression Begg-Mazumdar
Intercept P value Kendall’s τ P value
Low intake 1.08 0.79 −0.06 0.84
Medium-High intake 1.72 0.66 −0.07 0.79
Fig. 2 Effects of low-medium (a) and medium-high (b) intake of capsaicin on gastric cancer; OR odds ratio, CI confidence interval
J Gastrointest Canc
outlier in both categories, with opposite effects to the rest of thestudies. Removal of this outlier increased the protective effects(54 %) and exacerbated susceptibility (2.3-fold) without alter-ing overall nonsignificance and heterogeneity. However, Gohet al. has been limited by having the lowest sample size and theonly study with admixed subjects, racially segregated intoMalay, Chinese, and Indian. This study along with the rest ofthe outliers may account for the substantial heterogeneity of thepooled ORs in the overall and subgroup analyses. Loss ofheterogeneity resulting from reanalysis of the remaining threestudies [10, 38, 47] underscores the protective effect from lowintake and susceptibility due to high consumption of capsaicinwithout the baggage of interstudy variation.
The gastroprotective effect of capsaicin was found to bedose-dependent [7]. Although small amounts of capsaicinshow few or no deleterious effects, heavy ingestion of thecompound has been associated with erosion of the gastricmucosa, necrosis of the liver, and ulceration [49]. It has beenproposed to alter the metabolism of chemical carcinogens andmight promote carcinogenesis at high doses [50]. Capsaicinhas been shown to induce duodenal adenocarcinomas in mice
and promotes stomach and liver tumors in rats [7]. Converse-ly, capsaicin effectively inhibited tumor growth and inducedapoptosis in immunodeficient mice [51]. Given the reportedcontradictions to capsaicin mutagenicity [49], it is possiblethat this compound exerts a dual effect depending on the dose.However, available information about the mechanisms possi-bly involved for carcinogenicity and mutagenicity of capsai-cin is far from conclusive.
This meta-analysis has addressed association of one dietaryfactor (capsaicin consumption) with gastric cancer; however,other factors, such as genetic background and H pylori infec-tion, are also involved [37, 38]. Of the 10 studies, threeexamined the role of genetic factors in risk for gastric cancer.Interaction of cytochrome p450, glutathione transferases, al-dehyde dehydrogenase 2 polymorphisms, and acetylation sta-tus of N-acetyltranferase with kimchi has been investigatedby Nan et al. [47] and Zhang et al. [48]. High capsaicin intakeposed increased risk of gastric cancer, carriers of theinterleukin1B-31C allele infected with the virulent H pylori(CagA positive) strain [37]. Thus, dietary, genetic, and infec-tion factors may interact to influence gastric cancer risk al-though not much information is available to explain theirpotential mechanism or interaction. One possible mechanismfor increased susceptibility is reduction of acidic gastric envi-ronment, which favors H pylori growth. Experimental studieshave demonstrated that capsaicin alters gastrin levels, thehormone regulating gastric acid secretion [52]. In a study ofhuman volunteers, a chili-rich diet (up to 4.2 mg capsaicin/day) consumed for 3 weeks decreased ex-vivo secretion ofgastrin [53].
The strengths of our analysis consist of the following: (1) Inmost of the studies, populations were ethnically homoge-neous, so admixture is unlikely; (2) Selection bias is alsounlikely because controls were matched to cases in all thestudies; (3) Publication bias was absent; (4) Pooled effectswere statistically homogeneous among subjects in the Hpylori analysis; and (5) Outlier treatment did not materiallychange pooled ORs in the subgroups and H pylori analysissuggesting consistency of protective and increased risk effectswith low intake and medium-high consumption, respectively.H pylori infection was detected more readily in patients at theincipient stage of gastric cancer (seen in one [36] of the fourstudies), less readily at the later stages of the disease. This isdue to the loss of bacterial colonization in progressivelyatrophic stomach [54]. So, when H pylori testing is done atthe later stage, results might generate false negative seropos-itivity which in two of the four H pylori studies admit to belimiting [37, 38]. The following limitations of our study needto be acknowledged: (1) the relatively low sample sizes in thesubgroup analysis by ethnicity, which may have renderedchance effects more likely; (2) A substantial proportion ofthe studies (66.7 %) were hospital-based which may impactupon their applicability to the general population; (3) Controls
a
b
Fig. 3 Outlier analysis a low intake, b medium-high intake. GK:Gajalakshmi [45]; LC Lopez-Carrillo et al [9, 37]
J Gastrointest Canc

in most of the studies were not healthy individuals but patientsalthough their ailments were unrelated to gastric cancer. Stillthis does not disregard for the possibility of nondifferentialmisclassification bias owing to the inclusion of control groupswith different risks of developing gastric cancer; and (4) Ittook removal of seven outlying studies to erase overall het-erogeneity sacrificing reduced sample size in the process.
Conclusion
Results of this meta-analysis underscore that the dual-roles ofcapsaicin are dose-dependent. These roles have been demon-strated to be tenable with subgroup, outlier, and H pylorianalyses. Future investigations of the association of capsaicinintake with gastric cancer warrant close attention to design,methodological features, and expansion into other less studiedpopulation groups. Well-designed and controlled epidemio-logical studies based on sample sizes would help illuminatethe complex interplay of factors that may be associated withgastric cancer risk.
Acknowledgments This project has been funded by the Saint LouisUniversity multigrant awarded to Dr. Noel Pabalan. The Canadian BreastCancer Foundation (CBCF) and Canadian Institute of Health Research(CIHR) grants support Dr. Hilmi Ozcelik. We thank Ofelia Francisco.This paper is dedicated to the memory of Dr. Hilmi Ozcelik, a longtimefriend, colleague, and mentor.
Conflict of Interest The authors declare that they have no conflict ofinterest.
References
1. Parkin DM. Epidemiology of cancer: global patterns and trends.Toxicol Lett. 1998;102–103:227–34.
2. Howson CP, Hiyama T, Wynder EL. The decline in gastric cancer:epidemiology of an unplanned triumph. Epidemiol Rev. 1986;8:1–27.
3. Hyun Ja Kim WKC, Mi Kyung KIM, Sang Sun LEE, Bo YoulCHOI. Dietary factors and gastric cancer in Korea: a case-controlstudy. Int J Cancer. 2002;97:531–5.
4. Palli D. Epidemiology of gastric cancer: an evaluation of availableevidence. J Gastroenterol. 2000;35 Suppl 12:84–9.
5. Holzer P, Pabst MA, Lippe IT, Peskar BM, Peskar BA, LivingstonEH, et al. Afferent nerve-mediated protection against deep mucosaldamage in the rat stomach. Gastroenterology. 1990;98(4):838–48.
6. Matsumoto J, Takeuchi K, Okabe S. Characterization of gastricmucosal blood flow response induced by intragastric capsaicin inrats. Jpn J Pharmacol. 1991;57(2):205–13.
7. Kang JY, TengCH,Wee A, Chen FC. Effect of capsaicin and chilli onethanol induced gastric mucosal injury in the rat. Gut. 1995;36(5):664–9.
8. Takeuchi K, Ueshima K, Matsumoto J, Okabe S. Role of capsaicin-sensitive sensory nerves in acid-induced bicarbonate secretion in ratstomach. Dig Dis Sci. 1992;37(5):737–43.
9. Lopez-Carrillo L, Hernandez Avila M, Dubrow R. Chili pepperconsumption and gastric cancer in Mexico: a case-control study.Am J Epidemiol. 1994;139(3):263–71.
10. Mathew A, Gangadharan P, Varghese C, Nair MK. Diet and stomachcancer: a case-control study in South India. Eur J Cancer Prev.2000;9(2):89–97.
11. Surh YJ, Lee SS. Capsaicin, a double-edged sword: toxicity,metabolism, and chemopreventive potential. Life Sci. 1995;56(22):1845–55.
12. Buiatti E, Palli D, Decarli A, Amadori D, Avellini C, Bianchi S, et al.A case-control study of gastric cancer and diet in Italy. Int J Cancer.1989;44(4):611–6.
13. Huang JQ, Sridhar S, Chen Y, Hunt RH. Meta-analysis of therelationship between Helicobacter pylori seropositivity and gastriccancer. Gastroenterology. 1998;114(6):1169–79.
14. IARC. Monograph on the evaluation of carcinogenic risk to humans,vol. 61. Lyon: IARC; 1994.
15. Kim JD, Kim JM, Pyo JO, Kim SY, Kim BS, Yu R, et al. Capsaicincan alter the expression of tumor forming-related genes which mightbe followed by induction of apoptosis of a Korean stomach cancercell line, SNU-1. Cancer Lett. 1997;120(2):235–41.
16. Kato S, Aihara E, Nakamura A, Xin H, Matsui H, Kohama K,et al. Expression of vanilloid receptors in rat gastric epithelialcells: role in cellular protection. Biochem Pharmacol.2003;66(6):1115–21.
17. Teel RW. Effects of capsaicin on rat liver S9-mediated metabolismand DNA binding of aflatoxin. Nutr Cancer. 1991;15(1):27–32.
18. Teel RW. Effects of different inducers of cytochrome P450 on themutagenes i s of the tobacco-spec i f i c n i t rosamine 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK) inSalmonella typhimurium TA1535. Anticancer Res. 1992;12(4):1287–90.
19. Lee YS, Kwon EJ, Jin DQ, Park SH, Kang YS, Huh K, et al. Redoxstatus-dependent regulation of cyclooxygenases mediates thecapsaicin-induced apoptosis in human neuroblastoma cells. JEnviron Pathol Toxicol Oncol. 2002;21(2):113–20.
20. Hail Jr N, Lotan R. Examining the role ofmitochondrial respiration invanilloid-induced apoptosis. J Natl Cancer Inst. 2002;94(17):1281–92.
21. Macho A, Blazquez MV, Navas P, Munoz E. Induction of apoptosisby vanilloid compounds does not require de novo gene transcriptionand activator protein 1 activity. Cell Growth Differ. 1998;9(3):277–86.
22. Morre DJ, Chueh PJ, Morre DM. Capsaicin inhibits preferentially theNADH oxidase and growth of transformed cells in culture. Proc NatlAcad Sci U S A. 1995;92(6):1831–5.
23. Morre DJ, Sun E, Geilen C, Wu LY, de Cabo R, Krasagakis K, et al.Capsaicin inhibits plasma membrane NADH oxidase and growth ofhuman and mouse melanoma lines. Eur J Cancer. 1996;32A(11):1995–2003.
24. Jeong E-J, Bang B-H, Kim K-P. The characteristics of kimchi by thedegree of hotness of powdered red pepper. Korean J Food Nutr.2005;18(1):88–93.
25. Crane PS, Rhee SU, Seel DJ. Experience with 1,079 cases of cancerof the stomach seen in Korea from 1962 to 1968. Am J Surg.1970;120(6):747–51.
26. KimHJ, ChangWK, KimMK, Lee SS, Choi BY. Dietary factors andgastric cancer in Korea: a case-control study. Int J Cancer.2002;97(4):531–5.
27. Myers BM, Smith JL, Graham DY. Effect of red pepper and blackpepper on the stomach. Am J Gastroenterol. 1987;82(3):211–4.
28. Graham DY, Smith JL, Opekun AR. Spicy food and the stomach.Evaluation by videoendoscopy. JAMA. 1988;260(23):3473–5.
29. Holzer P, Lippe IT. Stimulation of afferent nerve endings byintragastric capsaicin protects against ethanol-induced damage ofgastric mucosa. Neuroscience. 1988;27(3):981–7.
J Gastrointest Canc
30. Holzer P, Sametz W. Gastric mucosal protection against ulcerogenicfactors in the rat mediated by capsaicin-sensitive afferent neurons.Gastroenterology. 1986;91(4):975–81.
31. Yeoh KG, Kang JY, Yap I, Guan R, Tan CC, Wee A, et al. Chiliprotects against aspirin-induced gastroduodenal mucosal injury inhumans. Dig Dis Sci. 1995;40(3):580–3.
32. Stang A. Critical evaluation of the Newcastle-Ottawa scale for theassessment of the quality of nonrandomized studies in meta-analyses.Eur J Epidemiology. 2010;25(9):603–5
33. Mantel N, Haenszel W. Statistical aspects of the analysis of data fromretrospective studies of disease. J Natl Cancer Inst. 1959;22(4):719–48.
34. DerSimonian R, Laird N.Meta-analysis in clinical trials. Control ClinTrials. 1986;7(3):177–88.
35. Goh KL, Cheah PL, Md N, Quek KF, Parasakthi N. Ethnicity and H.pylori as risk factors for gastric cancer inMalaysia: a prospective casecontrol study. Am J Gastroenterol. 2007;102(1):40–5.
36. Lee SA, Kang D, Shim KN, Choe JW, Hong WS, Choi H. Effect ofdiet and Helicobacter pylori infection to the risk of early gastriccancer. J Epidemiol. 2003;13(3):162–8.
37. Lopez-Carrillo L, Camargo MC, Schneider BG, Sicinschi LA,Hernandez-Ramirez RU, Correa P, Cebrian ME (2012) Capsaicinconsumption, Helicobacter pylori CagA status and IL1B-31C>Tgenotypes: A host and environment interaction in gastric cancer.Food Chem Toxicol
38. Lopez-Carrillo L, Lopez-Cervantes M, Robles-Diaz G, Ramirez-Espitia A, Mohar-Betancourt A, Meneses-Garcia A, et al. Capsaicinconsumption, Helicobacter pylori positivity and gastric cancer inMexico. Int J Cancer. 2003;106(2):277–82.
39. Lau J, Ioannidis JP, Schmid CH. Quantitative synthesis in systematicreviews. Ann Intern Med. 1997;127(9):820–6.
40. Berman NG, Parker RA.Meta-analysis: neither quick nor easy. BMCMed Res Methodol. 2002;2:10.
41. Galbraith RF. A note on graphical presentation of estimated oddsratios from several clinical trials. Stat Med. 1988;7(8):889–94.
42. Pabalan N, Bapat B, Sung L, Jarjanazi H, Francisco-Pabalan O,Ozcelik H. Cyclin D1 Pro241Pro (CCND1-G870A) polymorphismis associated with increased cancer risk in human populations: a
meta-analysis. Cancer Epidemiol Biomarkers Prev. 2008;17(10):2773–81.
43. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ Clin Res Ed.1997;315(7109):629–34.
44. Begg CB, Mazumdar M. Operating characteristics of a rank correla-tion test for publication bias. Biometrics. 1994;50(4):1088–101.
45. Gajalakshmi CK, Shanta V. Lifestyle and risk of stomach cancer: ahospital-based case-control study. Int J Epidemiol. 1996;25(6):1146–53.
46. Lee JK, Park BJ, Yoo KY, Ahn YO. Dietary factors and stomachcancer: a case-control study in Korea. Int J Epidemiol. 1995;24(1):33–41.
47. Nan HM, Park JW, Song YJ, Yun HY, Park JS, Hyun T, et al. Kimchiand soybean pastes are risk factors of gastric cancer. World JGastroenterol. 2005;11(21):3175–81.
48. Zhang YW, Eom SY, Kim YD, Song YJ, Yun HY, Park JS, et al.Effects of dietary factors and the NAT2 acetylator status on gastriccancer in Koreans. Int J Cancer. 2009;125(1):139–45.
49. Monsereenusorn Y, Kongsamut S, Pezalla PD. Capsaicin—a litera-ture survey. Crit Rev Toxicol. 1982;10(4):321–39.
50. Lee BM, Park KK. Beneficial and adverse effects of chemopreven-tive agents. Mutat Res. 2003;523–524:265–78.
51. Ito K, Nakazato T, Yamato K, Miyakawa Y, Yamada T, Hozumi N,et al. Induction of apoptosis in leukemic cells by homovanillic acidderivative, capsaicin, through oxidative stress: implication of phos-phorylation of p53 at Ser-15 residue by reactive oxygen species.Cancer Res. 2004;64(3):1071–8.
52. Imatake K, Matsui T, Moriyama M. The effect and mechanism ofaction of capsaicin on gastric acid output. J Gastroenterol.2009;44(5):396–404.
53. Ericson A, Nur EM, Petersson F, Kechagias S. The effects ofcapsaicin on gastrin secretion in isolated human antral glands:before and after ingestion of red chilli. Dig Dis Sci. 2009;54(3):491–8.
54. Forman D, Webb P, Parsonnet J. H pylori and gastric cancer. Lancet.1994;343(8891):243–4.
J Gastrointest Canc









![Approach to Gastric Cancers - Sci Forschen · Gastric carcinoma is the second most prevalent cancer in men, and fourth most prevalent cancer in women worldwide [27]. The incidence](https://img.pdfslide.us/doc/110x75/5fc7a6c4a5f82734a930563a/approach-to-gastric-cancers-sci-forschen-gastric-carcinoma-is-the-second-most.jpg)



















