Embed Size (px)
Citation preview
The Impact of Age of Onset and Effects of Antipsychotics on Executive Functions, Attention, and Reaction Time:
A Study of Cognitive Functions in First-Episode Psychotic Children and Schizophrenic Adults
Ph.D. Thesis Birgitte Fagerlund
Department of Psychology Faculty of Humanities
University of Copenhagen &
Copenhagen University Hospital Bispebjerg Department of Psychiatry E
København 2004


Acknowledgements I became part of the research group on biological psychiatry at Bispebjerg University Hospital in 1997, where two clinical studies concerning schizophrenia and psychosis were in the planning stages. Torben Mackeprang, M.D., and Katrine Pagsberg, M.D., became my closest collaborators as they conducted their PhD projects in the studies on adult onset schizophrenia, and adolescent onset schizophrenia and psychosis, respectively. The three of us became sparring partners in a process that for me has been both stimulating and rewarding professionally, and a great pleasure personally. I look forward to continued collaborations with Katrine, where Torben will be greatly missed. I am grateful to my principal supervisor Anders Gade, Ph.D., for the combination of always relevant, focused comments and unwavering support throughout the project, and for introducing me to neuropsychology in the first place. Many thanks to my co-supervisor Birte Glenthøj, D.M., for support and discussions, especially concerning theories on early information processing, and for introducing me to the field of psychopharmacology. Thanks to Professor Ralf Hemmingsen, D.M., for support and comments throughout the project. Thanks to Jens Richardt Jepsen, M.Sc., for clinical supervision in the adolescent project, and for continuing, fruitful discussions and collaboration. Thanks to Mai-Britt Hansen, M.D., William Baaré, Ph.D., and Klaus Tjelle Kristiansen, M.D., with whom it has been a pleasure to work. Psychologists and clinicians at the Child- and Adolescent Psychiatric Departments of Bispebjerg, Glostrup and Hillerød Hospitals are thanked for contributing test results and recruitment of patients to the project. Patients, controls, and their parents are thanked for their contribution of time and efforts, without whose co-operation, the project would not have been possible. The work was supported by grants from the following, who are all thanked for their help: The University of Copenhagen, Institute of Psychology at the Faculty of Humanities; The Danish Medical Research Council, H:S (Copenhagen Hospital Cooperation) Research Council; Janssen-Cilag A/S (unrestricted grant). Thanks to my parents, my brother Michael, and my friends for their patience and for providing welcome distractions from the work. Very special thanks to Dan for exceptional support and patience throughout.
Preface The thesis is based on two parallel clinical studies that were carried out at the Adult Psychiatric Department E in collaboration with the Child- and Adolescent Psychiatric Department F at Bispebjerg Hospital. Study I included adult first-episode, drug-naïve patients with schizophrenia and a healthy control group. Study II included children and adolescents with first-episode early onset schizophrenia or psychotic disorder and a healthy control group. The primary objectives of the thesis are to characterise the profile of cognitive deficits in the domains of executive, attentional, and reaction time functions in adult first-episode drug-naïve schizophrenic patients (Study I), and child and adolescent patients with early onset first-episode schizophrenia or psychotic disorder (Study II), as well as examine the effects of age of onset in a cross-sectional comparison between Study I and Study II. The secondary objectives are to examine the differential effects of typical and atypical antipsychotic medication on cognitive deficits in adult first-episode drug-naïve schizophrenic patients in a longitudinal design in Study I, and examine whether there are differences in the profile of deficits in early onset schizophrenia and early onset psychotic disorder in Study II. The thesis consists of an introduction to and brief overview of the relevant theoretical background concerning cognitive deficits in schizophrenia (Chapters 1 and 2). The methodology and empirical data concerning cognitive functions from the two clinical studies are presented and discussed separately: Study I involving first-episode drug-naïve schizophrenic adults in Chapter 3, and Study II involving children and adolescents with first-episode schizophrenia or non-schizophrenic psychotic disorders in Chapter 4. Chapter 5 is a discussion of the impact of age of onset on cognitive deficits, as a cross-sectional comparison of results from Study I and Study II. Chapter 6 is a conclusion of the thesis. As part of Study I, Chapter 3 includes a discussion of results concerning the effects of antipsychotics on cognitive deficits from the enclosed paper: Fagerlund, B., Mackeprang, T., Gade, A., Hemmingsen, R., Glenthøj, B. Effects of Low-Dose Risperidone and Low-Dose Zuclopenthixol on Cognitive Functions in First-Episode Drug-Naïve Schizophrenic Patients. Paper IN PRESS CNS Spectrums May 2004 (Appendix 1).
Contents
DANSK RESUMÉ............................................................... 4
ENGLISH SUMMARY....................................................... 4
LIST OF ABBREVIATIONS ............................................. 5
CHAPTER 1: INTRODUCTION ...................................... 6
CHAPTER 2: THEORETICAL BACKGROUND........... 6
2.1. GLOBAL AND SPECIFIC COGNITIVE DEFICITS IN SCHIZOPHRENIA ............................................................... 6
2.1.1. Relations of cognitive deficits with psychopathology ......................................................... 6 2.1.2. Relations of cognitive deficits with functional outcome....................................................................... 7
2.2. THE NEURODEVELOPMENTAL HYPOTHESIS OR PROGRESSIVE DETERIORATION ........................................ 7 2.3. THE RELEVANCE OF NORMAL COGNITIVE DEVELOPMENT FOR COGNITIVE DEFICITS IN SCHIZOPHRENIA ............................................................... 8
2.3.1. The development of cognitive functions in adolescence................................................................. 8 2.3.2. Deficits of cognitive functions that mature late in the developmental process .......................................... 8
2.4. INTELLIGENCE........................................................... 9 2.4.1. Deficits of premorbid and current intelligence in schizophrenia .............................................................. 9
2.5. EXECUTIVE FUNCTIONS ............................................. 9 2.5.1. Deficits of executive functions in schizophrenia 9 2.5.2. Progression of executive deficits in schizophrenia ............................................................ 10
2.6. ATTENTION.............................................................. 10 2.6.1. Attentional deficits of automatic, pre-cognitive functions in schizophrenia ........................................ 10 2.6.2. Cognitive attentional deficits in schizophrenia10 2.6.3. Attentional deficits are stable vulnerability indicators in schizophrenia....................................... 10
2.7. REACTION TIME ...................................................... 11 2.7.1. Reaction time deficits in schizophrenia........... 11
2.8. EFFECTS OF ANTIPSYCHOTIC MEDICATION ON COGNITIVE DEFICITS ...................................................... 11
CHAPTER 3: STUDY I: ADULTS WITH FIRST PRESENTATION SCHIZOPHRENIA........................... 11
3.1. STUDY OBJECTIVES AND HYPOTHESES ................... 12 3.2. METHODS ................................................................ 12
3.2.1. Subjects ........................................................... 12 3.2.2. Materials......................................................... 13
3.3 RESULTS ................................................................... 15 3.3.0. Demographics ................................................. 15 3.3.1. Psychopathology ............................................. 15 3.3.2. Cognitive deficits............................................. 15 3.3.4. Effects of antipsychotic medication on cognitive deficits....................................................................... 16
3.4. DISCUSSION ............................................................. 17
3.4.1. Demographics..................................................17 3.4.2. Cognitive deficits .............................................17 3.4.3. Effects of antipsychotic medication on cognitive deficits .......................................................................18
3.5 CONCLUSIONS ...........................................................19
CHAPTER 4: STUDY II: CHILDREN AND ADOLESCENTS WITH FIRST PRESENTATION SCHIZOPHRENIA OR NON-SCHIZOPHRENIC PSYCHOSIS.......................................................................19
4.0. THEORETICAL BACKGROUND: CHILDREN AND ADOLESCENTS WITH SCHIZOPHRENIA AND PSYCHOSIS ...19
4.0.1. Prevalence and diagnostic stability and validity of early onset schizophrenia ......................................19 4.0.2. Early onset schizophrenia: Increased vulnerability and worse outcome...............................20 4.0.3. Cognitive deficits in early onset schizophrenia20
4.1. STUDY OBJECTIVES AND HYPOTHESES....................21 4.2. METHODS.................................................................21
4.2.1. Subjects............................................................21 4.2.2. Materials .........................................................22
4.3. RESULTS...................................................................23 4.3.1. Psychopathology..............................................23 4.3.2. Cognitive deficits .............................................23
4.4. DISCUSSION ..............................................................25 4.4.1. Early onset schizophrenia vs non-schizophrenic psychosis....................................................................25 4.4.2. Demographics..................................................25 4.4.3. Cognitive deficits .............................................25
4.5. CONCLUSIONS ..........................................................26
CHAPTER 5. THE IMPACT OF AGE OF ONSET OF SCHIZOPHRENIA AND PSYCHOSIS ON COGNITIVE DEFICITS...........................................................................27
5.1. STUDY OBJECTIVES AND HYPOTHESES....................27 5.2. METHODS.................................................................27 5.3. RESULTS & DISCUSSION ...........................................27
5.3.0. Demographics..................................................27 5.3.1. Psychopathology..............................................27 5.3.2. Cognitive deficits .............................................27
5.4. STUDY LIMITATIONS ................................................28 5.5. CONCLUSIONS ..........................................................28
CHAPTER 6: CONCLUSIONS AND FUTURE DIRECTIONS:...................................................................29
REFERENCES...................................................................30
APPENDIX 1:.....................................................................37
FAGERLUND, B., MACKEPRANG, T., GADE, A., HEMMINGSEN, R., GLENTHØJ, B. EFFECTS OF LOW-DOSE RISPERIDONE AND LOW-DOSE ZUCLOPENTHIXOL ON COGNITIVE FUNCTIONS IN FIRST-EPISODE DRUG-NAÏVE SCHIZOPHRENIC PATIENTS. PAPER IN PRESS CNS SPECTRUMS MAY 2004. ..................................................37
Dansk Resumé Ph.d. projektet blev udført på Bispebjerg Hospitals Voksenpsykiatriske Afdeling E i samarbejde med Børne- og Ungdomspsykiatrisk Afdeling F og Institut for Psykologi på Københavns Universitet. Afhandlingen er baseret på data fra to parallelle kliniske studier med debuterende, antipsykotika-naive voksne skizofrene patienter og børn og unge med debuterende skizofreni eller anden ikke-organisk psykose. Teoretisk baggrund: Kognitive deficits er kernesymptomer ved skizofreni, der anses som sårbarhedsindikatorer overfor udviklingen af sygdommen og karakteriserer patienterne uanset klinisk tilstand. Forstyrrelserne er hverken forårsaget af psykopatologiske symptomer eller antipsykotisk medicin. De kognitive deficits er af stor betydning for patienternes sociale og arbejdsmæssige prognose og derfor er der betydeligt incitament for at udvikle behandlingsstrategier der kan bedre disse deficits. Profilen af forstyrrelser involverer både globale kognitive funktioner, men også med fremtrædende forstyrrelser i visse afgrænsede kognitive domæner. Karakterisering af udviklingen, stabiliteten og progressionen af de kognitive forstyrrelser er aktuelt relevante problemstillinger. Metoder: Studie I inkluderede debuterende, antipsykotika-naive voksne skizofrene patienter (N=25) og en rask kontrolgruppe matchet på alder og køn. Patienterne blev undersøgt mens umedicinerede og igen efter 13 ugers behandling med enten det atypiske antipsykotika risperidone eller det typiske antipsykotika zuclopenthixol (efter tilfældig allokation) for at undersøge effekten på kognitive forstyrrelser. Studie II inkluderede børn og unge med tidligt debuterende psykose (N=40), hvoraf 18 blev diagnosticerede med skizofreni og 22 med anden ikke-organisk psykose, samt en rask kontrolgruppe matchet på alder og køn. Kognitive forstyrrelser blev undersøgt i begge studier, med fokus på tests af eksekutive funktioner, opmærksomhed og reaktionstid. Formål: De primære formål var at karakterisere profilen af kognitive deficits hos voksne debuterende skizofrene og børn og unge med tidligt debuterende skizofreni eller anden ikke-organisk psykose hver for sig, samt at undersøge effekten af alder ved debut på kognitive forstyrrelser ved en direkte sammenligning mellem Studie I og Studie II. De sekundære formål var at undersøge effekten af antipsykotisk medicin på kognitive forstyrrelser i Studie I, samt at sammenligne profilen af forstyrrelser hos de tidligt debuterende patienter med skizofreni og anden psykose i Studie II. Resultater: Profilen og sværhedsgraden af psykopatologi og kognitive deficits var lignende hos patienterne med tidlig og voksen debut, hvilket støtter hypoteser om klinisk og kognitiv kontinuitet mellem tidlig og voksen debut af skizofreni. Imidlertid var profilen af kognitive deficits hos patienterne med tidlig debut primært karakteriseret af forstyrrelser af formodede frontallaps funktioner, mens patienterne med voksen debut derudover havde deficits der formodentlig yderligere implicerer forstyrrelser af fronto-striatale forbindelser. Resultaterne støttede en lignende profil og sværhedsgrad af kognitive forstyrrelser hos tidligt debuterende skizofrene sammenlignet med patienter med tidligt debuterende ikke-organisk psyksose. Mht. effekten af antipsykotisk medicin på kognitive deficits hos de voksne patienter, fandtes kun begrænset effekt og få forskelle mellem effekten af risperidone og zuclopenthixol mht. reaktionstid, og disse forskelle kunne ikke skelnes fra retest effekt, ekstrapyramidale bivirkninger, eller effekt af antikolinerg medicinsk behandling. Konklusion: Resultaterne støtter indirekte hypoteser om skizofreni som en udviklingsforstyrrelse, med et aspekt af progressiv forværring. En genundersøgelse af patienterne i både Studie I og Studie II kunne hjælpe til at afklare hypotesen at de tidligt debuterende patienter muligvis udgør en delgruppe af skizofrene patienter med progressiv forværring både klinisk og kognitivt.
English summary The ph.d. project was carried out at the Department of Psychiatry E in collaboration with the Department of Child and Adolescent Psychiatry F at Bispebjerg Hospital and the Department of Psychology, at the University of Copenhagen. The thesis is based on data collected from two parallel clinical studies including adult first-episode drug-naïve schizophrenic patients and children and adolescents with first-episode schizophrenia or other non-organic psychotic disorders. Theoretical background: Cognitive deficits have been established as core deficits of schizophrenia, and are considered vulnerability indicators of the illness that are present regardless of clinical state, and are caused neither by the symptoms of psychopathology nor antipsychotic medication. Cognitive deficits are important for the social and occupational prognosis of patients, and therefore the incentive for developing treatment strategies that target these deficits is significant. The profile of deficits involves global cognitive functions, with particularly prevalent deficits in certain cognitive domains. This implicates an underlying pathophysiology that is widely distributed, perhaps with more severe expression in certain brain areas or networks. However, issues regarding the development, stability, and progression of cognitive deficits are still equivocal. Methods: Study I included first-episode, drug-naive adult schizophrenic patients (N=25) and an age and gender matched healthy control group. Patients were tested both when drug-naïve, and again after 13 weeks of randomly allocated treatment with either an atypical antipsychotic medication (risperidone) or a typical antipsychotic compound (zuclopenthixol) to examine differential efficacy on cognitive deficits. Study II included first-episode children and adolescents with early onset psychosis (N=40), of whom 18 were diagnosed with schizophrenia, and 22 with non-organic psychosis, as well as an age and gender matched healthy control group. Neuropsychological cognitive deficits were examined in both studies, focusing on tests of executive functions, attention, and reaction time. Objectives: The primary objectives were to characterise the profile of cognitive deficits in adult onset schizophrenia, and early onset schizophrenia or psychosis separately, as well as examine the impact of age of onset on cognitive deficits in a direct comparison between Study I and Study II. Secondary objectives were to examine the efficacy of antipsychotic medication on cognitive deficits in Study I, and compare the profile of deficits in early onset schizophrenia with early onset psychosis in Study II. Results: The overall profile and severity of psychopathology and cognitive deficits was similar in the adult and early onset patients, which yields support for viewing adult and early onset schizophrenia as clinically and cognitively continuous. However, while the cognitive deficits of the early onset patients were primarily characteristic of putative frontal lobe involvement, the adult patients additionally showed deficits indicative of the implication of putative fronto-striatal pathways. The results did not support a different level of impairment of cognitive deficits in early onset schizophrenia compared to early onset non-organic psychosis. In terms of efficacy of antipsychotic medication on cognitive deficits in the adult patients, only few differential effects were found between risperidone and zuclopenthixol on measures of reaction time, and these were indistinguishable from retest effects, extrapyramidal side-effects, and effects of adjunctive anticholinergic medication. Conclusions: The results yield indirect support for viewing schizophrenia as a neurodevelopmental disorder with a progressively deteriorating aspect. A follow-up study of both Study I and Study II could help determine the further development of cognitive deficits in both adult onset and early onset schizophrenic patients, in order to examine the hypothesis that the early onset patients may represent a sub-group of schizophrenic patients that show progressive deterioration both clinically and in terms of cognitive deficits.
4

List of abbreviations AOS = Adult onset schizophrenia CANTAB = Cambridge Neuropsychological Test Automated Battery DART = Danish Adult Reading Test DUP = Duration of untreated psychosis EOS = Early onset schizophrenia EPS = Extrapyramidal symptoms ESRS = Extrapyramidal Symptom Rating Scale FIQ = Full Scale Intelligence Quotient ICD-10 = International Classification of Diseases (World Health Organization) IED = Intra- and extradimensional IQ = Intelligence Quotient MRI = Magnetic Resonance Imaging NART = New/National Adult Reading Test NSP = Non-Schizophrenic Psychosis PANSS = Positive and Negative Symptom Scale PFC = Prefrontal cortex PIQ = Performance Intelligence Quotient RIS = Risperidone/Risperdal RVP = Rapid Visual Information Processing SANS = Scale for the Assessment of Negative Symptoms SAPS = Scale for the Assessment of Positive Symptoms SCAN = Schedules for Clinical Assessment in Neuropsychiatry Version 2.1 SD = Standard Deviation SES = Socio-economic status SOC = Stockings of Cambridge SPECT = Single Photon Emitted Computed Tomography VEOS = Very early onset schizophrenia VIQ = Verbal Intelligence Quotient WAIS = Wechsler Adult Intelligence Scale WCST = Wisconsin Card Sorting Test WISC-III = Wechsler Intelligence Scale for Children-III WISC-R = Wechsler Intelligence Scale for Children-Revised ZUC = Zuclopenthixol/Cisordinol
5

Chapter 1: Introduction Since the 1980's, cognitive deficits have increasingly been seen as core deficits of schizophrenia 1-3. The increased focus on cognition in schizophrenia is part of the continued effort to characterise and delineate the distinctive aspects of the disease. Historically, the theoretical frame of reference for schizophrenia has undergone radical shifts between organic and functional etiological theories, as has often been the case in psychiatry. Many of the insights of the early theorists such as Kraepelin and Bleuler are still highly relevant for the theories and controversies that are presently at issue in schizophrenia research. Kraepelin's view of the illness as having an organic base is well-established and indisputable today, as is a chronic course of illness, while the assertion of a progressively deteriorating course is debatable. Kraepelin considered the cognitive deficits central in the disease process, and not secondary to the clinical state and psychotic symptoms 4. Bleuler's contribution 5 was a shift in focus to withdrawn and introverted negative symptoms as well as cognitive deficits, both of which are of topical relevance as being primary and central in the pathological etiological mechanisms. Whether cognitive deficits are central to the disease to the extent that they characterise all schizophrenic patients is unclear 6. Comparative studies between schizophrenic patients and healthy controls have found mild to moderate cognitive deficits in approximately 80 % of patients, with estimates ranging from 75-90 % of patients 7;8. However, it is unclear whether the remaining patients represent a subgroup of patients with intact cognitive functions, or whether these patients have experienced a decrease in cognitive functions compared to their potential level of function. Some studies have found lower levels of cognitive function in patients compared to their siblings 9, and others have found discrepancies between the current cognitive level and higher levels of estimated premorbid cognitive function, suggesting functions that are affected, but within normal limits 10. Other findings underscore the methodological problems involved in estimating potential levels of function and support the existence of a subgroup of schizophrenic patients without cognitive impairment 11-13. Nevertheless, for the majority of patients, cognitive deficits are core characteristics of the illness. The cognitive deficits reflect increased vulnerability towards developing the illness 14-16, are contributing factors to the development of certain clinical symptoms 17-20, and are of great importance for the prognosis of patients 21-26. However, a number of questions remain at issue regarding the extent and profile of cognitive deficits, the course and stability of deficits, as well as which neural substrates are primarily involved. The increased focus on cognitive deficits since the 1980's and 90's is partly due to the advances in neuroimaging technology that have allowed for studies to examine the neurobiological underpinnings of the disorder. The field of neuropsychology has become the connecting link between psychological processes and their neurobiological underpinnings, by providing an intermediary level of description. Theories regarding the neuropathological mechanisms involved in the cognitive deficits of schizophrenia converge on the central importance of prefrontal cortex and distributed networks, the support of which is drawn from several lines of evidence such as subtle structural and functional brain abnormalities, and neurotransmitter dysregulation 27;28. One of the problems in determining the specific neurobiological substrates of cognitive deficits in schizophrenia is that it is still unclear exactly what specific functions characterise the frontal lobes as opposed to distributed networks involving the frontal lobes and other brain areas 29. While prefrontal cortex is undoubtedly specialised in different functional domains 30, the nature of this specialisation is still equivocal, especially in terms of whether the specialisation is modality- or process specific 31-33. A diverse array of cognitive
tasks recruits similar areas of prefrontal cortex in imaging studies 34. Conversely, damage to frontal and subcortical areas can produce very similar cognitive deficits, as has been shown in both pre-clinical and clinical studies 35;36. In order to attempt to distinguish the possible neurobiological substrate of cognitive deficits in schizophrenia, a detailed level of analysis of cognitive components is necessary.
Chapter 2: Theoretical Background 2.1. Global and specific cognitive deficits in schizophrenia The heterogeneity of schizophrenia in terms of clinical symptomatology is similarly reflected in the profile of cognitive deficits, in which there is considerable variation between patients 37. Numerous studies have shown deficits in a wide variety of cognitive domains, encompassing early sensory and perceptual information processing, memory, attention, executive functions, and social cognition 17;18;38;39. Whether this wide array of deficits reflects a global reduction of cognition or specific domains that are selectively impaired beyond the general level of function continues to be at issue. Some studies have found evidence for global deficits, without support for differentially impaired deficits in specific cognitive domains 40-42. Other studies have found specific differential deficits beyond the global level of deficits particularly in the areas of memory 43-48, or executive functions. 49-53 The problem of concluding the profile and extent of deficits from previous studies is largely a methodological one, both in terms of the construct validity of tests used and because of the diversity of patient samples included in the various studies at different stages of the disease, with different clinical status and treatment history. A particular problem when comparing differential levels of deficit in specific cognitive domains is test batteries that are skewed in terms of including tests that are sensitive to deficits in one domain together with crude tests of deficits in other domains. Intrinsic differences between tests in terms of level of difficulty make the direct comparison of differential deficits between cognitive domains a challenge 54. The clinical and epidemiological heterogeneity of patients in terms of symptom profile, chronicity, age of illness onset, and medication status as well as methodological problems in cognitive tests used in the studies that have been done, hampers the conclusions that can presently be made concerning specific characterisation of profiles of cognitive deficits. However, the evidence suggesting a profile of generalised, global deficits with select functions that may be particularly impaired, supports an underlying pathophysiology that is widely distributed, perhaps with more severe expression in certain specific brain areas or networks 55. The profile of cognitive deficits is related to several factors such as the disease process, in which a less severe course of illness is correlated with specific cognitive impairments, and a more severe course with generalised, global cognitive deficits 56;57. However, there are numerous factors (such as clinical sub-types, age of onset, level of chronicity etc.) that are involved in determining the profile of cognitive deficits, but the nature of impact of these factors is still unclear.
2.1.1. Relations of cognitive deficits with psychopathology The cognitive deficits are central characteristics of the illness and not secondary phenomena that can be attributed to either the clinical symptoms or effects of medication. Intuitively, the argument that patients are cognitively reduced because of the presence of severe psychopathology is attractive, because it is easy to infer how the presence of hallucinations or delusions could impair e.g. memory or concentration. However, the empirical data indicate that the causal effects work in the
6

opposite direction, where primary deficits of attention, speed and capacity of information processing and memory are contributing factors to the development of clinical symptoms. The cognitive deficits are present before clinical onset 58 and do not disappear with the abatement of clinical symptoms 59. Numerous studies have shown that cognitive deficits are prevalent regardless of clinical state (whether patients are hospitalised, psychotic, or in remission) 60. In fact, cognitive deficits are surprisingly independent of clinical symptoms, with a lack of correlation with positive symptoms 22 and only a partial correlation with negative symptoms and disorganisation symptoms 61;62. However, at a more detailed level there are correlations between specific cognitive deficits and specific symptoms, e.g. between deficits in fluency tasks with negative symptoms 63, and between deficits in semantic memory and formal thought disorder 20;64-67. This is not surprising, since these are the same dysfunctions described at a cognitive componential level and how they are expressed at a psychopathological level. There are also less obvious correlations, between working memory deficits and thought disorder 19;68 and between metacognitive skills and paranoid delusions and hallucinations 18. These specific correlations are important because they help delineate the different symptoms of psychopathology and their cognitive background. One way of dividing the cognitive deficits is according to their relation with clinical state, as stable, potentially mediating, and episode vulnerability indicators 69. Stable vulnerability indicators are deficits that are present in patients independently of clinical state, from before clinical illness onset and during psychotic episodes as well as in periods of remission. These are chronic deficits that represent an increased vulnerability towards developing the illness. There is substantial evidence that the stable vulnerability indicators are partly genetically mediated, as these deficits are found (although to a lesser degree) in first-degree relatives of schizophrenic patients 70-72, and have predictive power of later schizophrenia in high-risk individuals 73-76. Potentially mediating indicators are deficits that are partly dependent on clinical status, as they are more pronounced during psychotic episodes, and are ameliorated but still present during periods of clinical remission. Episodic indicators are state dependent deficits that are present solely during psychotic episodes, and in all probability are general characteristics of psychosis, regardless of whether the psychosis is caused by e.g. schizophrenia, manio-depressive illness or is drug-induced 17;71;72. Nevertheless, the majority of cognitive deficits in schizophrenia are trait rather than state dependent 77 78. The validity and reliability of cognitive tests in schizophrenic patients have been substantiated in numerous studies 1;78-80. One study found high retest reliability in a large group of schizophrenic patients (N= 142), and that test-retest correlations were not different from that of controls 78. Heaton found that reliability of neuropsychological function is not affected by the presence or severity of psychotic symptoms in patients, because even large changes in clinical symptoms did not influence the neuropsychological performance of patients 77. This is naturally very important for the validity and reliability of cognitive tests in acutely psychotic patients. Heaton 78 also found no differences in test-retest reliability and practice effects between schizophrenic patients and healthy controls, regardless of whether patients had mild or severe psychopathology scores, or had mild or severe cognitive deficits.
2.1.2. Relations of cognitive deficits with functional outcome Cognitive deficits are important predictors of the functional prognosis of patients. Factor-analytic reviews of prognostic studies have shown that cognitive functions at first episode are predictive of later prognosis, especially in terms of social function (friendships, close relations) and ability to be integrated
in the work community 1;21;23-26;81;82. These recent studies have indicated that cognitive function has a greater impact on, and predictive strength for, the subsequent social function and ability to work of schizophrenic patients than does clinical state and the severity of psychotic symptoms 21;22;83;84. This is consistent with the fact that even with clear amelioration of psychotic symptoms with antipsychotic medication, the patients continue to have a poor prognosis. Of course, these results do not imply that other factors such as psychopathology are irrelevant for the prognosis of patients. Some studies show that only certain negative symptoms and formal thought disorder (characterised by faulty thinking) are strong predictors of outcome 85;86. However, in terms of social and work-related abilities, collectively there is a stronger correlation between cognitive deficits and prognosis than between symptom severity and prognosis. More specifically, executive functions have been correlated to global functioning and aspects of memory and attention to social-vocational outcome 1;22. There is also evidence that cognitive deficits at first episode are better indicators of subsequent clinical outcome than clinical symptoms 21;23, because symptoms at first episode fluctuate considerably and are not a good indication of later symptoms 1. Finally, cognitive deficits are (not surprisingly) also good indicators of the ability to benefit from social and cognitive training 87;88. This has implications for the type of training that would benefit different patients based on their cognitive profile; e.g. based on techniques that do not place large demands on secondary memory, but instead rely on procedural learning 7. 2.2. The neurodevelopmental hypothesis or progressive
deterioration Whether schizophrenia should be viewed as a developmental disorder or a progressively deteriorating disease (or a combination of both) is of topical concern. In schizophrenia, the illness onset most often occurs in early adulthood, with an average age of illness onset of 26 years for men and 29 for women 89. Kraepelin coined the term 'dementia praecox' to characterise what he considered a progressively deteriorating disease, with an onset in early adulthood. However, even Kraepelin acknowledged that some cases of schizophrenia had an earlier onset in childhood and probably occurred as a result of impaired prenatal development of the brain 90. The neurodevelopmental hypothesis of schizophrenia posits that early pre- and perinatal disturbances in the development of the brain interact with other factors occurring during childhood to jointly increase the vulnerability towards developing schizophrenia 90-92. The long delay from the early disturbances of brain development until the effects can be seen as illness onset in early adulthood, is explained by the completion of the normal maturational process of the brain, at which time the lack of integrity in brain function becomes apparent 93. There are several lines of evidence supporting the neurodevelopmental hypothesis: Various pre- and perinatal insults, such as maternal infections 94 and obstetric complications 95, are correlated with an increased risk of developing schizophrenia, and structural brain imaging studies have found subtle indications of aberrant brain development 93. Retrospective studies have found slight deficits or developmental delays of motor skills and language acquisition 96-99. An alternative theory is that early disturbances may be present, but certain maturational processes are also defective, resulting in excessive synaptic pruning 94;100. In terms of structural brain changes, recent longitudinal studies have found progressive loss of grey matter after illness onset, supporting theories of accelerated synaptic pruning in schizophrenia 100-102. However, according to the neurodevelopmental theories, these changes are not progressive after the onset of symptoms 91;93.
7

Most of the evidence for the neurodevelopmental and neurodegenerative hypotheses comes from neurobiological data. The evidence from neuropsychological studies is inconclusive. Even though several studies have found subtle structural brain changes over time, the results from the same studies are inconclusive regarding cognitive deficits, some studies finding deterioration in intellectual functions 103, while others have not 104-106. This discrepancy might reflect primarily stable deficits, or test methodologies that are too crude to assess changes in cognitive functions. Premorbid deficits are present, but slight, mostly within normal limits 98. There is consensus that there is undoubtedly a decrease in cognitive functions from premorbid levels around illness onset 40;107, but the question remains whether this onset of clinical symptoms is the "end-point" of the disease process from a developmental perspective, from which there is no further decline beyond that which is normal. It is, however, possible that there is a continued deterioration of function throughout the course of the illness, in which neurodegenerative processes are accelerated in schizophrenia 55. The issue of progressive deterioration of cognitive functions is controversial and findings from studies contradictory. Many studies do not support a degenerative course 78;108-110. Longitudinal studies have mainly found stability of cognitive deficits in schizophrenia 111, which does not support the neurodegenerative hypothesis 112. Some studies have even found slight improvements over time on certain tasks, which have been found to correlate with improvements in negative symptoms 45;113. A review from 1998 of 15 longitudinal studies with a follow-up period of at least one year concluded that overall, cognitive deficits were stable without either exacerbation or amelioration of deficits over time 112. A 2-year follow-up study of geriatric schizophrenic patients found that increased impairments were very slow, and not in line with a neurodegenerative process 77. However, some of the functions were less stable over time, with either improvements or declines, in the areas of executive functions and attention 114. Cross-sectional studies comparing patients at different stages of the disease yield conflicting results 115. Several studies have found that compared to patients earlier in the disease process, more severe deficits are present with increasing chronicity, or increasing age. Landrø et al. found more severe memory deficits in chronic patients, but it is unclear whether these deficits are related to normal age-related declines 116. In a cross-sectional study comparing schizophrenic patients with ages spanning from 20-75, Fucetola et al. 117 examined whether declines in cognitive functions exceeded the normal age-related declines. Schizophrenic patients showed normal, age-related declines in most cognitive domains, except for executive functions, in which the decline exceeded the normal age-related decline of the healthy control group. Similarly, cross-sectional studies have found different profiles of executive functions in first-episode and chronic patients 50;118-121. Therefore, most cognitive deficits appear to be stable in most patients after illness onset, and further declines generally do not seem to surpass normal age-related declines. An exception may be executive functions and speed of information processing that have been found to show declines from first-episode to chronic stages 122; and there is some evidence for a further decline of executive functions in elderly patients 117. Another possibility is that certain sub-groups of patients show declines in cognitive functions, of which early onset patients are a particularly interesting possibility. It remains unclear whether psychotic episodes have a toxic effect on the brain and therefore cognitive function. The hypotheses regarding relations between psychotic episodes and deteriorations in cognitive deficits focus either on the toxic effects of number of psychotic episodes, or the duration of untreated psychosis (DUP). While some studies support the impact of DUP 119, others have not found any correlation
between DUP and cognitive deficits in patients 118;123. That psychosis does deleteriously affect certain cognitive functions has been established, however, rather than DUP, this may be related to the number of psychotic episodes 124. 2.3. The relevance of normal cognitive development for
cognitive deficits in schizophrenia
2.3.1. The development of cognitive functions in adolescence Since the age of onset in schizophrenia is during adolescence or early adulthood and in view of the neurodevelopmental hypothesis, the time course of normal development of cognitive functions is important to consider when investigating the cognitive deficits in schizophrenia. This may yield important clues to the pathophysiological process involved in the illness. During normal brain development from early childhood through adolescence to early adulthood, the prefrontal cortex (PFC) continues to grow, and myelination of cells is increased and progresses until early adulthood 125. In addition, neural pathways between brain areas are further consolidated throughout adolescence 93;126-128. In cognitive neuropsychological terms, this has direct implications on which functions are considered fully developed at particular ages throughout adolescence. While some cognitive functions are fully developed when children reach school-age, others develop throughout adolescence into early adulthood. Some of the functions that are considered consolidated by the age of 7 are memory functions that do not place large demands on strategic recalling: such as passively holding information available for short periods of time in working memory, as well as recognition and recall from long term memory 129. While passive maintenance of information in working memory does not improve markedly after the age of 7, the active use and manipulation of information in working memory improves until early adulthood. This is exemplified in the digit-span testsi, in which the forward digit span improves by approximately 1.5 digits between the ages 7 to 13, while the backward digit span improves 3 digits in the same time frame – which is twice the improvement seen in the digit forward condition 129. Similarly, functions involved on tasks that demand either manipulation of information or inhibition of a pre-potent response or shifting of attentional resources continue to evolve throughout adolescence 126. Speed of cognitive processing is one of the psychological domains that develop markedly throughout early adolescence, and then more gradually during late adolescence. The improvement in speed of processing is strongly related to the improvement of complex operations in working memory. The reasons for this strongly age-related improvement in cognitive processing speed and its relation to complex cognitive operations is most likely due to the late maturation of the prefrontal cortex and its connections. Diamond (129s. 493) suggests that faster and more efficient information processing becomes possible only when "a more mature and better functioning dorsolateral prefrontal cortex is able to reduce signal-to-noise ratios in diverse neural regions" 129.
2.3.2. Deficits of cognitive functions that mature late in the developmental process Regardless of whether early insults or later defective developmental processes are primarily involved in the pathophysiology of schizophrenia, the timing of normal development of cognitive functions must be important determinants for the profile of cognitive deficits in patients after illness onset. A very recent theory posits that due to the normal age-related decrease in neural plasticity, one would expect that the pathological processes of schizophrenia have a greater impact on cognitive functions that mature later in the
i The digit-span test from Wechsler Intelligence Scale for Children (WISC) 290
8

developmental process, while functions that are fully developed early are relatively spared 130. This seems in accordance with data concerning premorbid deficits and developmental delays present early in life compared to later on. The cognitive functions that undergo the largest development and improvement throughout adolescence are speed of cognitive processing, the ability to make and use strategies in problem solving, and the ability to manipulate information while holding it active in working memory (while inhibiting irrelevant information). These are functions that are linked to the development of PFC as well as connections between PFC and other brain areas. And these are the functions that are of particular interest in patients with schizophrenia. Premorbid deficits in functions that are normally fully developed early in life (such as sensory and motor functions and basic mnemonic and basic language skills) in prospective schizophrenic patients show signs of impairment and developmental delay early in childhood, but are ameliorated and not particularly impaired later in adolescence 96;98;99;131. In contrast, functions that continue to develop throughout adolescence and early adulthood (such as speed of information processing, executive functions and focused attention) are impaired at the time of clinical illness onset 131. The main hypothesis of the present thesis is that executive functions, focused attention, and speed of processing are the cognitive functions that will be particularly sensitive to possible differences in pathological processes involved in determining the age of illness onset, and sensitive to the effects of a possibly progressive deteriorating disease process. 2.4. Intelligence
2.4.1. Deficits of premorbid and current intelligence in schizophrenia In group comparative studies, the global level of cognitive functions of schizophrenic patients is lower than that of healthy controls. In term of measures of intelligence this is reflected in a significantly lower intelligence quotient (IQ) in patients, both premorbidly and after illness onset 132-134. In most studies, premorbid intelligence is either examined or estimated to less than 1 standard deviation (SD) below the average of controls; which is still within the interval of normal function. The Israeli army studies in which all Israeli draftees (i.e. most all young Israeli men) are examined with cognitive tests have allowed for impressive prospective studies of people who later develop schizophrenia 57. Most other studies are retrospective and estimate intelligence using neuropsychological tests of functions that in neurological populations have been shown to be remarkably stable. These functions are usually verbal functions that are highly consolidated and resistant to change, such as reading and vocabulary tests 135;136. Low premorbid intelligence is a risk-factor for an early onset of schizophrenia and a severe course of illness. Similarly, a high premorbid IQ is considered a protective factor predictive of later onset and a milder illness profile 15;133;137. There is some evidence for a further reduction in intelligence around and immediately after illness onset of less than 1 SD 132;133;138;139. However, most results support that this reduction in IQ does not progress throughout the illness, but is stabilised at the new level within the first years of illness onset 140. Weickert et al. found a decline of 10 IQ points from estimated premorbid to current levels in approximately half of patients studied. One quarter of patients showed low but equivalent premorbid and current IQ levels, and the remaining quarter had well-preserved premorbid and current IQ 139. This supports intellectual decline to be present in some, but not all patients. Results from children and adolescents with early onset suggest stagnation in cognitive development, rather than loss of previously acquired functions 141. In fact, Bedwell et al. recently found that an age-related
decline in scaled IQ scores in patients with early onset schizophrenia was indicative of stable raw scores and a lack of age-related improvements, reflected as a decline in age-scaled scores 141. While intelligence is generally a good predictor of global function in terms of work function and social relations for healthy people, the same is not true of schizophrenic patients, who function at a level much lower than would be expected from their level of intelligence. Accordingly, correlations between intelligence and functional outcome of patients are weak. This lack of correlation between intelligence and outcome is reminiscent of other patient groups such as people with frontal lobe damage, who do relatively better on intelligence tests than would be expected from their everyday level of functioning. There are other cognitive functions (such as executive functions) that are more important predictors of outcome in schizophrenia than intelligence. 2.5. Executive functions Executive functions are comprehensive functions that are considered to be at a higher cognitive level, supervising other functions 142, and/or are considered central processes that integrate other functions 143. The top-down regulation from executive functions encompasses regulatory mechanisms of cognition, behaviour, emotion, motivation, and other "drives". The characteristics of executive functions are that they are involved in inhibition of prepotent responses, in prospective thinking, and in delay of responses. Executive functions are required for tasks that are neither well-learned nor automatic, but novel or complicated, or require the integration of many different functions. Executive functions and frontal lobe functions are terms that have often been used interchangeably even though this is unwarranted 144. Executive functions may reflect a common factor of "fluid intelligence" similarly to Spearman's g factor of crystallised intelligence 145. However, delineating the separate components of executive functions has relevancy for identifying the neural substrates involved in different executive deficits. There are several ways of separating executive functions into cognitive components, but both factor-analytic studies of healthy populations and several studies of neurological populations substantiate a distinction between spontaneous flexibility and reactive flexibility 36;146-148. Spontaneous flexibility refers to the ability to initiate a strategy and continuously evaluate whether the strategy is working 36. Reactive flexibility refers to the ability to change attentional focus and strategies according to outside requirements 36. It appears that the frontal lobes and basal ganglia contribute differentially to strategy initiation and strategy monitoring, illustrated in the distinction between spontaneous and reactive flexibility, where both fronto-striatal areas and pathways are implicated in reactive flexibility, while spontaneous flexibility appears to primarily be a putative frontal lobe function 36;149. This distinction between spontaneous and reactive flexibility along the fronto-striatal axis has been supported by clinical studies of frontal lobe patients and disorders of the basal ganglia, such as Parkinson's disease and Huntington's disease. While performance on executive tests is impaired in both groups, the pattern of deficits is different 150.
2.5.1. Deficits of executive functions in schizophrenia Executive deficits are unique compared to most other cognitive deficits in schizophrenia, because they have not been found in patients during the prodromal phase, but co-occur with the exacerbation of clinical symptoms and the clinical onset of illness, and may be the cognitive functions most likely to progressively deteriorate during the course of the disease 117;151. The deficits of executive functions appear to be the most ubiquitous of deficits because they are present in most patients,
9

regardless of the global level of cognitive function152 and independently of intelligence. In fact, Weickert et al found executive deficits in patients with otherwise intact cognitive functions as well as in patients both with and without reductions in current IQ compared to premorbid IQ 139. This is supported by a meta-analytic study, in which executive deficits were present regardless of IQ, and in which there was no systematic variance in executive scores that could be related to intelligence 153. A recent meta-analysis pooled data from various measures (based on 72 studies; N=4524) and found an effect size of d=-1.45 when schizophrenic patients were compared to healthy controls 153. Moderator variables that could potentially confound executive deficits, such as education, medication, and duration of illness were not correlated with executive deficits; however, both positive and negative symptoms correlated with severity of executive deficits, as did the number of hospitalisations and which specific tests of executive function were used 153. This suggests that executive deficits are related to the pathophysiological process involved in both negative and positive symptoms, may progress during the illness, and could represent differential patterns of deficits of executive components.
2.5.2. Progression of executive deficits in schizophrenia Most studies support equivalent deficits of most cognitive functions in first-episode patients compared to chronic patients. However, there are conflicting data concerning the level of executive deficits in first-episode patients compared to chronic patients. Several studies have found less severe or no deficits on Wisconsin Card Sorting Test (WCST) in first-episode patients compared to chronic patients and therefore concluded that executive deficits were not present in the early stage of the disease 1;50;154. As an example, Addington found that only 1/3 of first-episode patients had deficits on WCST155. However, lack of impairment on the WCST does not necessarily imply normal executive functions, and others support the presence of executive deficits in patients at first-episode 1;40;50;114;119;156. Hutton found that first-episode schizophrenic patients had a different profile of executive deficits than what has previously been found in chronic schizophrenic patients, with more deficits in planning (spontaneous flexibility) than attentional set shifting (reactive flexibility) in first episode patients; with the opposite pattern in chronic patients 50. Similarly, accelerated declines in executive functions have been found against a backdrop of normal age-related declines of other functions 117. This supports the notion that the profile of executive deficits changes over the course of the illness (maybe as one of the few cognitive domains for which this is the case) 119. 2.6. Attention
2.6.1. Attentional deficits of automatic, pre-cognitive functions in schizophrenia Attentional deficits are among those best established in schizophrenia research 74. Since theorists such as Kraepelin and Bleuler, attentional functions in schizophrenia have been described as unsteady and unfocused 17, and they are among the cognitive deficits that are most evident clinically. According to the early theories of attentional deficits in schizophrenia, only higher-level, conscious cognitive processes were impaired, while early sensory and perceptual processed were considered intact 157. However, several lines of evidence support a breakdown in processes both at cognitive and pre-cognitive levels of information processing 72. Deficits in early, pre-cognitive automatic levels of sensory information processing have been
found using various test paradigms (such as P50 gatingii, and Prepulse inhibitioniii). The different test paradigms have all found deficits in automatic functions of stimulus inhibition, which normally function as a buffer against information processing overload 17;18;158. The original and revised filter-hypotheses 158-160 assert that impairments in early, automatic selective processes in a bottom-up process lead to increased load on higher cognitive systems of information processing, causing deficits in higher cognitive functions such as attention and executive functions. These deficiencies in early information processing are hypothesised to be directly involved in the development of cognitive fragmentation and psychotic symptoms 17. The attentional deficits of early, automatic processing are already present at illness onset and appear unaffected by clinical state and antipsychotic medication 161;162.
2.6.2. Cognitive attentional deficits in schizophrenia Schizophrenic patients have deficits in focusing, maintaining, and shifting attention to relevant information. In terms of the profile of attentional deficits in schizophrenia, there is evidence for deficits of selective attention rather than sustained attentioniv at the level of cognitive attentional processing 74;163, while deficits of both selective and sustained attention may be present at earlier, pre-cognitive stages of information processing in schizophrenia 157. Patients do not make disproportionately more errors on late as opposed to early stages of attentional tasks (such as the Continuous Performance Test), and even though their slope of decline of signal detection is lower, it is parallel to that of healthy controls 74;157. This indicates that while patients have general deficits maintaining attentional focus on relevant targets, the profile of attentional deficits may not include particular deficits in sustaining the attentional focus over long periods of time. The theories explaining attentional deficits in schizophrenia are multiple. In addition to the bottom-up impact of early information processing deficits on cognition, most theories propose that the attentional deficits at a cognitive level may also involve deficits in the top-down regulation of attentional resources from supervisory processes 69;163. The allocation of attentional resources is managed by executive functions 164. The neural substrates of attentional control are hypothesised to involve widely distributed neural networks, with PFC playing an important role in the integration of attentional processes 165.
2.6.3. Attentional deficits are stable vulnerability indicators in schizophrenia Attentional deficits are considered stable vulnerability indicators of schizophrenia spectrum disorders. This is due to several lines of evidence that have found attentional deficits in subjects at high risk for developing schizophrenia, such as schizotypical patients, unaffected first-degree relatives of schizophrenic patients, and in children of schizophrenic patients, as predictors of later development of the illness 17;72;74;166-168. These deficits are thought to reflect a genetically transmitted increased vulnerability towards developing the illness 17. The presence of attentional deficits regardless of clinical state further establishes these deficits as stable vulnerability (or trait) indicators. Nevertheless, when specific attentional tasks are examined in detail, there is evidence for a progression of certain attentional deficits in schizophrenia from the first episode to chronic phases of the illness 169. This has been found in studies focusing on
ii P50 gating refers to automatic gating of the P50 event related potential (ERP) component when 2 stimuli are presented in close temporal proximity17 iii Prepulse Inhibition refers to automatic sensory gating of the startle response after a weak pre-stimulus17 iv Maintenance of attention can refer to short time intervals, while sustained attention is over longer time periods
10

shifts in covert spatial attention, supporting the presence of a progressively deteriorating course 170;171. 2.7. Reaction Time In spite of being called the "closest thing to a north star" in schizophrenia research (Cancro 1971, cited by Braff 17), few of the schizophrenia studies done in the 1990s include simple measures of reaction time. However, the focus on reaction time has been resumed very recently, as different theories of prefrontal lobe function converge on the central importance of temporal integration and efficient speed of information processing for optimal brain function 172;173. Studies correlating reaction time to neuropsychological tests suggest that reaction time tasks are sensitive to subtle changes in brain function 174, and different reaction time paradigms are indicative of different patterns of cognitive impairments 175.
2.7.1. Reaction time deficits in schizophrenia Reaction times have been found to be slower and more variable in schizophrenic patients 176;177. A recent meta-analysis of 40 reaction time studies found that a generalised slowing of information processing accounted for 87 % of the variance in reaction time, but that the extent and pattern of slowing was dependent on the type of task used, with particular deficits in tasks requiring response inhibition 178. This is a more specific profile than the generalised slowing related to e.g. ageing. Simple reaction time tasks reflect speed of information processing at the basic levels of attention and response initiation, and as such are specific and sensitive measures, not multimodal as most of the higher level cognitive tests. Therefore they may present a more unbiased reflection of the underlying neurobiological systems necessary for higher levels of attentional processes. Aspects of the reaction time deficits are considered trait-related, because they are present in patients both before illness onset, during psychotic episodes, and during remission 176. Other aspects are related to the clinical symptoms of schizophrenia 179;180. When patients with persistent illness are compared to patients with fluctuating illness, reaction time deficits have been correlated to different clinical symptoms. Simple reaction time deficits have been found correlated to negative symptoms only in patients with persistent illness, while choice reaction time deficits are correlated with disorganisation symptoms, both in patients with persistent and fluctuating illness 181. Whether the deficits are stable at the same level throughout the illness or progressively deteriorate is at issue, with some studies supporting a stable level of deficits, and others a deterioration that increases linearly with the number of psychotic episodes 21. In support of previous studies 124, Eberhard et al. found that most cognitive functions were impaired approximately 1 SD compared to previous levels, except for reaction times that were impaired at a level 3.5 SD below previous function. The decrease in reaction time was positively, linearly correlated with number of psychotic episodes, suggesting a detrimental effect on reaction time 122. Interestingly, duration of untreated psychosis was not indicative of an increase in reaction time deficits, which suggests that the detrimental effects are caused by the underlying pathophysiological process itself, which perhaps continues even when psychotic symptoms abate. The increased impairment of reaction time has also been found in studies in which other cognitive deficits were stable over time 21;182. 2.8. Effects of antipsychotic medication on cognitive deficits Since cognitive deficits are established as central characteristics of schizophrenia that are critical for the prognosis of patients
particularly in terms of social and occupational function, there is considerable incentive for finding effective pharmacological treatment strategies for cognitive deficits. It is clear that the cognitive deficits in schizophrenia are not caused by antipsychotic medication 3. However, whether different antipsychotic compounds have beneficial, detrimental or no effects on various cognitive functions, is still inconclusive 183;184. The typical (first generation) antipsychotic compounds have been found to ameliorate positive symptoms. They do, however, often result in extrapyramidal side effects (EPS) and therefore in adjunctive anticholinergic medication (which is known to have deleterious effects on cognition) 185;186. The effectiveness of typical compounds on negative symptoms and cognitive deficits is limited. Throughout the 1990's there has been a prevalent optimism regarding the potential effects of newer antipsychotics (the second generation atypical compounds) on cognitive deficits, as several studies have found better effect of atypicals over typicals on cognitive deficits 187. Furthermore, in contrast to first generation antipsychotics, these compounds have a better effect on negative symptoms 184;188-194 and cause fewer extrapyramidal side effects 195-197. There are theoretical reasons why differential efficacy would be expected from typical and atypical compounds due to their different receptor profiles. Both typical and atypical antipsychotics act as dopamine D2 receptor antagonists; however, while this is the primary mode of action of the typical compounds, the atypical compounds have a broader receptor profile affinity, particularly being more antagonistic to serotonin 5-HT2A receptors compared to dopamine D2-receptors. The preferential effect on serotonin 5-HT2A-receptor activity may help optimise the balance both within and between the dopaminergic and serotonergic receptor systems causing fewer EPS and improving information processing. In addition, some of the atypical compounds have a faster dissociation from the dopamine D2 receptor than the typical compounds and thus block the dopamine receptors for shorter periods of time 198. This may explain why these compounds generally do not cause as many EPS as typical compounds, because the time period of action is long enough to achieve the therapeutic antipsychotic effect, but not long enough to cause as many side-effects. However, the optimism regarding efficacy of atypicals on cognitive deficits has recently been dampened by meta-analyses and recent studies that have shown that the literature concerning efficacy of antipsychotics on cognitive deficits is confounded by methodological problems which limits the conclusions that can be drawn presently183;184;199;200 196. The most prominent of these problems is incomparable doses used in head-to-head compound comparisons, as well as a lack of control for the impact of indirect factors such as clinical improvements, retest effects, EPS, and adjunctive treatment with e.g. anticholinergic medication. (These issues are discussed in more detail in the enclosed paper in Appendix 1). Therefore, the characterisation of efficacy of different antipsychotic compounds on cognitive deficits has not been sufficiently substantiated.
Chapter 3: Study I: Adults with first presentation schizophrenia In this longitudinal study, cognitive functions of first-episode drug-naïve schizophrenic patients as well as a gender- and age matched control group were examined. Patients were randomly allocated to open-label treatment with a typical antipsychotic compound (zuclopenthixol) or an atypical compound (risperidone) and re-examined after 13 weeks of treatment in order to study effects of antipsychotic medication on cognition. Retest effects were studied by re-examining a portion of the healthy control group after 13 weeks. An extensive examination program of psychopathology and Extrapyramidal side-effects (EPS) ratings, sensory gating (prepulse inhibition), magnetic resonance imaging (MRI) and single photon emitted computed
11

tomography (SPECT 123I-epidepride) scans were carried out as part of a parallel Ph.D. project conducted by M.D. Torben Mackeprang, whose results are presented elsewhere. The present presentation includes the results of examination of cognitive functions and relations to psychopathology. 3.1. Study Objectives and Hypotheses Objectives: The primary objective was to characterise the profile of deficits in drug-naïve, first-episode adult schizophrenic patients in the cognitive domains of executive, attentional, and reaction time functions. The secondary objective was to examine the differential effects of a typical and an atypical antipsychotic medication on executive, attentional and reaction time functions. Hypotheses: 1. The patients have significant deficits in the cognitive domains of attention, executive functions and reaction time. 2. The patients have a profile of executive deficits in which spontaneous flexibility is more impaired than reactive flexibility. 3. There is a differential beneficial effect on cognitive deficits of the atypical compound risperidone over the typical compound zuclopenthixol, which is expected to have little effect (neither beneficial nor detrimental). 3.2. Methods
3.2.1. Subjects Patients: Patients were included from January 1998 to January 2002 from the psychiatric departments of 5 participating hospitals in the Copenhagen catchment area: Bispebjerg University Hospital (61.2 %); Kommunehospitalet (19.3 %); Rigshospitalet (6.5 %); County Hospital Gentofte (6.5 %); and Glostrup Hospital (6.5 %). The population in the catchment area is approximately 500.000 people. Inclusion and exclusion criteria: The inclusion criteria were: Patients between the ages 18 to 45, fulfilling the International Classification of Diseases (ICD-10)201 diagnostic criteria for schizophrenia. Only antipsychotic-naïve patients admitted to psychiatric care of schizophrenia were included. The exclusion criteria were: Patients who were compulsorily hospitalised or deemed in acute need of medication. Patients with somatic or neurological illnesses were excluded, as well as patients with known mental retardation (IQ<70). Psychopathology: Diagnostic evaluations were done by referring psychiatrists, and confirmed by M.D. Torben Mackeprang using the SCAN 2.1 interview (Schedules for Clinical Assessment in Neuropsychiatry Version 2.1202). Psychopathology ratings were carried out using PANSS203 (the Positive and Negative Syndrome Scale) as well as SANS204 and SAPS205 (The Scale for the Assessment of Negative symptoms and The Scale for the Assessment of Positive Symptoms). Global ratings from the SANS and SAPS were used to summarise severity of symptoms in 3 illness dimensionsv: Global Psychotic Dimension (global hallucinations and delusions), Global Negative Dimension (global affective flattening, alogia, avolition, and anhedonia), and Global Disorganisation Dimension (global bizarre behaviour and global positive formal thought disorder). Psychopathology ratings were done at baseline and at follow-up after 13 weeks of
v The 3 symptom dimensions were calculated in accordance with criteria defined by Andreasen 204;205, based on a tripartite illness partition suggested by Liddle 180.
treatment. EPS were rated using the Extrapyramidal Symptom Rating Scale (ESRS). Recruitment process: All patients were recruited by M.D. Torben Mackeprang. A total of 31 patients were included, of whom 25 completed the study. The reasons for drop-out of patients were: change to another antipsychotic compound (N=1); compulsory hospitalisation (N=1); acute medication at baseline (N=1), patient drop-out (N=1), and inability to participate in neuropsychological testing at baseline due to psychotic symptoms (N=2). The 2 patients who were unable to complete tests at baseline, had a non-significant tendency towards a higher positive PANSS score than the rest of the patients (p= 0.08 using the nonparametric Mann-Whitney significance test), but there were no other differences in terms of psychopathology. The diagnostic distribution of the 25 participating patients was: F 20.0 Paranoid schizophrenia (N=18), F 20.3 Undifferentiated schizophrenia (N=4), F 20.9 Unspecified schizophrenia (N=3). Random allocation to treatment: After baseline assessments, patients were randomly allocated (by blind drawing of treatment codes) to treatment with comparable, low flexible doses of either risperidone (from 2-26 mg) or zuclopenthixol (from 2-7 mg). Treatment responsibility remained localised to clinicians outside the project, who determined and adjusted drug doses according to clinical response. The average dose in the risperidone group was 3.6 mg (± 1.6 mg), and the average dose in the zuclopenthixol group was 9.6 mg (± 5.9 mg). After random allocation to treatment groups, 15 patients received risperidone, and 10 patients zuclopenthixol. (The fewer patients in the zuclopenthixol group was coincidental and not due to increased drop-out from this group after medication.) Benzodiazepines were allowed throughout the study, except on examination days. In the risperidone group, 60 % of patients received benzodiazepines at baseline and 33.3 % after 13 weeks of medication, which was not significantly different from 70 % at baseline and 40 % after 13 weeks in the zuclopenthixol group. Anticholinergics were allowed (except on examination days), but were kept to a minimum by lowering the dose of antipsychotics when EPS occurred. Eighty percent of patients in the zuclopenthixol group and 26.7 % of patients in the risperidone group received anticholinergics, a difference that was highly significant (p= 0.007). Healthy Controls: Healthy controls (N=25) were recruited among hospital staff unrelated to the project and university students from adverts in student and hospital magazines. Controls were matched to the patients 1:1 according to gender and age. Exclusion criteria for controls were the presence of a psychiatric diagnosis (assessed by TM using SCAN 2.1), somatic illness; psychiatric diagnoses in first-degree relatives, history of drug- or alcohol abuse, presence of mental retardation or any known learning disabilities. Healthy controls participated in all the same examinations as patients at baseline. In order to examine retest effects, 12 of the healthy controls were retested on the cognitive measures after 13 weeks. Background variables:The average age of patients was 27.4 (±6.4); ranging from 19 to 37 years, and the average age of controls was 28.4 (±5.2). The duration of untreated psychosis was highly variable, and ranged from 4 to 78 months (Median= 14 months). The gender distribution was 17 males (68 %) to 8 females (32 %). There were no differences between medication groups before
12

allocation to treatment in terms of age, gender, duration of untreated psychosis, psychopathology, or cognitive deficits. Socioeconomic status (SES): Socioeconomic status (SES) was calculated based on a combination of parental education/occupationvi (6 groups) and household income (3 groups) according to criteria from the Danish Institute of Clinical Epidemiology, and resulted in 3 socioeconomic groups (SES). Parental SES is considered a reliable indicator of potential SES of offspring and was used instead of patient SES, which would underestimate the potential socioeconomic level, since the illness has profound impact on education, vocation and income because of the common timing of illness onset during early adulthood. There were no significant differences between the parental education/occupation of patients and controls, but there was a significantly lower level of income in the patient group (χ2= 8.30; p= 0.02), and consequently a lower combined SES (χ2= 7.1; p= 0.03). The socio-demographic data (parental education/occupation, income, and SES) of patients and controls are shown in table 3.1. Table 3.1. Demographical data Study I: Parental education/occupation, income, and socioeconomic status.
N Parental Education/ Occupation Patients Controls Pearson's χ2 Df P
2-sided
Academic 6 9 3.16 5 0.676 Bachelor 10 8 Expert 2 4 Skilled 4 2 Non-skilled 2 2 Non-skilled, Unemployed 1 -
N Parental Income Patients Controls Pearson's χ2 Df P
2-sidedHigh 3 10 8.30 2 0.016 Middle 15 14 Low 7 1
N SES Patients Controls Pearson's χ2 Df P 2-sided
A (High) 3 9 7.12 2 0.028 B (Middle) 18 16 C (Low) 4 -
3.2.2. Materials Cognitive Test Battery: The test battery comprised tests from Cambridge Neuropsychological Test Automated Battery (CANTAB) 206;207 as well as paper-and-pencil cognitive tests. Executive functions and selective attention were examined using tests from CANTAB, Wisconsin Card Sorting Test (WCST) 208 as well as verbal fluency 209, figural fluency 210, and Trail Making tests A & B 211. Tests of reaction and movement time were assessed using CANTAB. Premorbid intelligence was estimated using the Danish Adult Reading Test (DART); the Danish version of the New/National Adult Reading Test (NART) 135. Cognitive functions were tested by the same examiner (BF) at baseline and retest. Furthermore, tests of episodic and semantic memory, facial affect recognition, and spatial working memory were carried out, but are not included in the thesis and will be presented elsewhere. Intelligence: DART Premorbid intelligence was estimated using the DART (Danish Adult Reading Test). DART is the Danish version of the NART (New/National Adult Reading Test 135). A list of 50 words with irregular pronunciation is presented, and subjects are asked to correctly read and pronounce each word. vi Education/occupation was recorded from the parent with the highest rating, either according to education or occupation.
WAIS Vocabulary The Vocabulary subtest from the Wechsler Adult Intelligence Scale (WAIS) 136 battery was administered. An abbreviated 20-word version was used 212. The test consists of a list of words that subjects are asked to define. Definitions are scored according to accuracy, and abstract- or concreteness of answers. The vocabulary subtest has been found to correlate well with total full-scale IQ (FIQ). The Vocabulary test is the subtest of the WAIS battery that is the most reliable indication of FIQ, and is also a good indication of premorbid IQ 136. Trail Making test A & B: Trail Making A assesses visuospatial scanning and psychomotor speed by combining ascending numbers. Trail Making B assesses psychomotor speed and set shifting by subjects combining circles containing numbers, and letters – continuously alternating between ascending numbers and letters in alphabetical order. Trail Making B requires focused attention and executive reactive flexibility in continuously alternating between two separately highly consolidated systems. As such, it is also a test of response inhibition and perseveration because the alternation between letters and numbers requires the inhibition of the pre-potent response to continue tracking alphabetically or numerically. The Trail Making A and B were administered according to Halstead-Reitan criteria, in which mistakes are continuously corrected and included in the total time score 211;213. The outcome measures are the time taken to complete Trail Making A and Trail Making B, respectively. In addition, the time difference between Trail Making B and Trail Making A is calculated, as an indication of the executive set shifting required in Trail Making B, controlled for the psychomotor speed requirements of Trail Making A 214. Verbal Fluency: Verbal phonological and semantic fluency were assessed. Phonological fluency was tested asking subjects to say as many different words as possible beginning with the letter "S" in 1 minute. Semantic fluency was tested by subjects saying as many different examples as possible from the category "animals" in 1 minute. Figural Fluency: Figural fluency was assessed using Regard's figural fluency task 210. Subjects are given 3 minutes to draw as many different figures as possible, combining two or more of 5 dots. The outcome measure is the number of different figures. Wisconsin Card Sorting Test: The 128 card version of the WCST was used 208. Subjects are asked to sort cards according to a rule, and are told that the rule is changed occasionally without warning. Subjects have to sort cards according to the correct rule (which is cards matching according to colour, shape, or number), and change their sorting strategy accordingly when the rules are changed. The WCST assesses the ability to make and maintain hypotheses, and utilise feedback to change strategies when relevant. The outcome measures were selected to examine attentional set shifting ability using: Total number of perseverative errorsvii, percentage perseverative errorsviii, and learning efficiency using: other errorsix, percentage other errorsx, and total number of cards used to complete the test. Exploratory analyses examined Nelson perseverative errorsxi and unique errorsxii.
vii Perseverative sorting errors to the previously correct sorting category208. viii Percentage perseverative errors from total errors. ix Errors that are neither perseverative nor unique, such as errors of distraction, where sorting changes from the correct rule. x Percentage other errors from total errors xi Perseverative sorting errors to immediately preceding wrong guess228. xii Errors when cards sorted do not correspond to any of the 3 sorting rules.
13

Cambridge Neuropsychological Test Automated Battery: The CANTAB test-battery 206;207 is a computerised test-battery in which responses are made using a touch-screen. The test-battery has been developed based on classic neuropsychological tasks as well as tests used in pre-clinical studies, with test designs that allow componential analysis of cognitive deficits. The test battery has been validated in several neurological populations 215-219, which yields the possibility, albeit indirectly, of addressing hypotheses regarding neurobiological processes involved in specific patterns of deficits. The CANTAB battery is also based on tests used in pre-clinical studies, in which e.g. lesion studies in monkeys have validated the differential components that comprise the test battery 220. As such, the test battery is suitable to examine theories regarding the neurobiological substrates of cognitive deficits; particularly deficits involving fronto-striatal pathways 49. Executive functions: IED Set Shifting task: The CANTAB Intra-Extradimensional Set Shifting (IED) task was developed as an analogue to the WCST. While testing similar attentional set shifting abilities, it avoids some of the methodological and theoretical problems involved in interpreting the WCST 221;222. The IED task consists of 9 different stages that have to be completed in order for subjects to pass the test. If a subject fails to complete a stage of the test, the test is terminated and later stages are not presented. The test is set up with several stages of simple discriminant learning and reversal, and the level of difficulty increases throughout the test, making it possible to identify the stages at which problems occur. This allows for a componential analysis of the basis of problems involved in solving the test. The IED tests the ability at increasing levels of difficulty to utilise feedback to discriminate between figures, as well as to make, maintain, and shift hypotheses within and between categories. The ability to shift hypotheses between categories is required at stage 8 (the extradimensional set shifting stage), which is theoretically akin to the shift between categories in the WCST. An alternative version of the test was administered at retest after 13 weeks. Outcome measures are number of subjects who complete all 9 stages of the test, total errors (adjusted for stages not completed)xiii, errors made at the extradimensional set shifting stage (EDS errors), percentage EDS errorsxiv, total number of trials (adjusted for stages not completed)xv, completed stage errors, and completed stage trialsxvi. Stockings of Cambridge The CANTAB Stockings of Cambridge (SOC) planning task is an analogue to the classic Tower of London test 223. While not as widely used as an executive task in schizophrenia research as the WCST (in spite of being perhaps a more specific executive task than the WCST 224), some recent studies have found deficits on the Tower of London in schizophrenic samples 120;146;225-227. The SOC tests planning ability with a task that demands identifying, planning, and carrying out the separate steps involved in completing the task. Two arrays of coloured balls are presented on the computer screen, and subjects are required to move the balls at the bottom of the screen to match to the array presented at the top of the screen. The test difficulty gradually increases throughout the test, where minimum moves required in solving the problem increases from 2 to 3, 4, and 5 moves. The number of problems solved "perfectly" with the minimum number of moves required, as well as the average number of moves used at each level, initial thinking latencies and subsequent thinking latencies are registered for each 2, 3, 4, and 5 move problems.
xiii The adjusted error score adds 25 errors for each stage not completed, since it takes 50 trials to fail a stage, and 25 of these could be correct by chance alone. xiv Percentage EDS errors from total errors. xv The adjusted trial score adds 50 trials for each stage not completed. xvi Errors and trials on the stages that were completed.
Initial thinking latency is the time from the test first appears on the computer until the subject first touches the screen. Subsequent thinking latency is the time from the subject first touches the screen until the problem is solved. The planning task is followed by a motor control task that repeats the moves made by the subject during the planning task, this time merely requiring the subject to repeat the moves made by the computer. The motor latencies are then subtracted from the subsequent latencies in the planning task, thereby approximating a measure of "pure" problem-solving time; i.e. the time taken to think while carrying out the planning task. Attention: Rapid Visual Information Processing The Rapid Visual Information Processing Test (RVP) from CANTAB is a continuous performance test, which consists of 3 numbers (3-5-7) that subjects have to attend and respond to continuously within a series of other numbers. The number of correct hits, misses, and signal detection sensitivity were recorded. Signal detection sensitivity (A') is a measure of the ability to distinguish signals (3-5-7 in sequence) from noise (all other numbers), and ranges from 0 to 1. At high A', information processing is effective, which means that signals are detected and noises ignored. At low A', information processing is less effective, and noise disturbs the detection of signals. The RVP assesses selective attention and vigilance with a small working memory component. Reaction and Movement time: In the Reaction and Movement Time task (RTI) from CANTAB, stimuli (yellow dots) are briefly presented on the computer screen. Subjects respond by releasing a press-pad and touching the dot on the screen as fast as possible. The test distinguishes between reaction and motor times, as well as between simple and choice latencies. Reaction times are the latencies from the stimulus is presented on the screen, until subjects release the press-pad. Motor times are the latencies from when the press-pad has been released, until the subject touches the stimulus on the screen. Simple reaction and motor latencies are when there is only one location on the screen in which the stimulus can appear. Choice reaction and movement latencies are when the stimulus can appear in any of 5 locations on the screen. Because these tasks involve an element of precision, they are dependent on a trade-off between speed and accuracy. Statistical Analyses: Data analysis was done using SPSS 11.0. (Statistical Package for Social Sciences). Two-tailed levels of significance were applied in all analyses. Results were standardised to z-scores, using the results of the healthy control group as reference point with an average of 0 and SD of 1. The assumption of normal distribution of data was examined using Q-Q plots because a Kolmogorov-Smirnow test of normality was deemed too conservative. Data that did not fit a normal distribution were log transformed to reduce skew, and parametric statistics were used for all analyses, except for analyses with small N, for which non-parametric analyses were used. In order to reduce Type I errors, the many cognitive measures were reduced by extracting 1 or 2 factors per test using principal component analysisxvii. Nominal and ordinal data were analysed using Pearson's χ2, or Fisher's exact test for analyses with small N. Bivariate correlations were examined using Pearson's correlation coefficient. Effects of medication and retest effects were examined using repeated measures ANCOVA, with the difference between baseline and retest scores as the dependent xvii In order to enable direct comparisons between groups, the principal components were based on all subjects (patients and controls) in Study I and Study II, including both baseline and retest results from subjects in Study I.
14
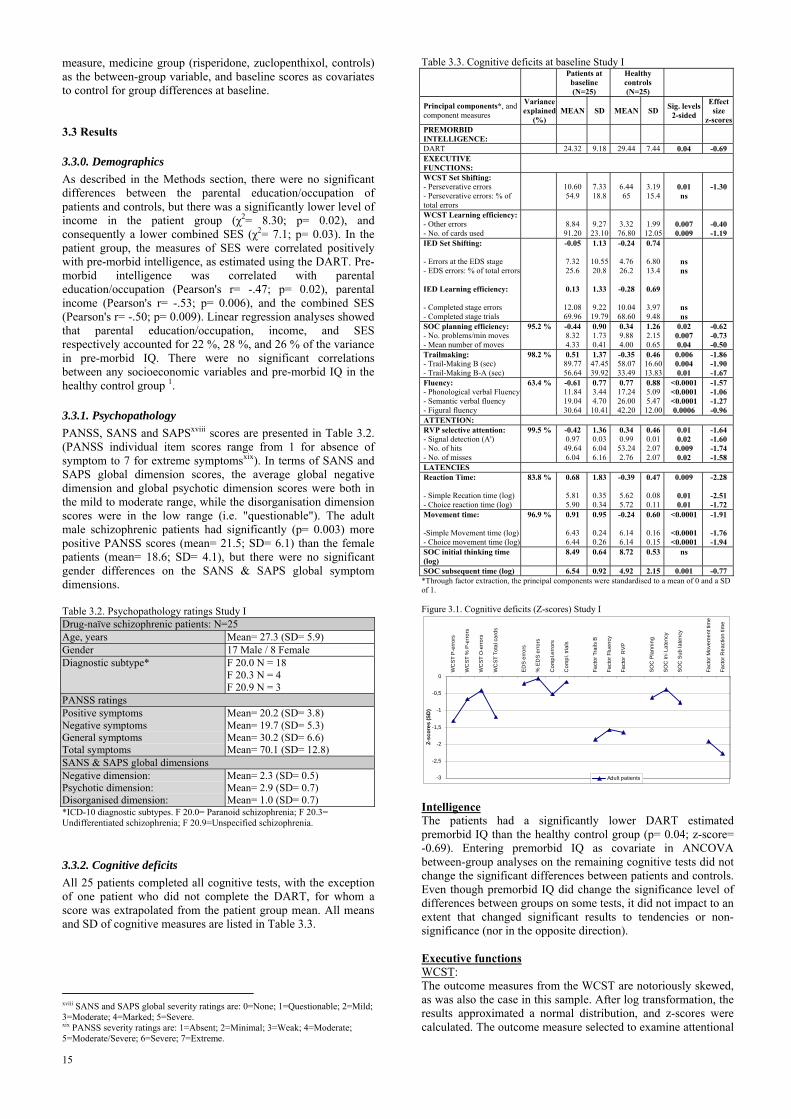
measure, medicine group (risperidone, zuclopenthixol, controls) as the between-group variable, and baseline scores as covariates to control for group differences at baseline. 3.3 Results
3.3.0. Demographics As described in the Methods section, there were no significant differences between the parental education/occupation of patients and controls, but there was a significantly lower level of income in the patient group (χ2= 8.30; p= 0.02), and consequently a lower combined SES (χ2= 7.1; p= 0.03). In the patient group, the measures of SES were correlated positively with pre-morbid intelligence, as estimated using the DART. Pre-morbid intelligence was correlated with parental education/occupation (Pearson's r= -.47; p= 0.02), parental income (Pearson's r= -.53; p= 0.006), and the combined SES (Pearson's r= -.50; p= 0.009). Linear regression analyses showed that parental education/occupation, income, and SES respectively accounted for 22 %, 28 %, and 26 % of the variance in pre-morbid IQ. There were no significant correlations between any socioeconomic variables and pre-morbid IQ in the healthy control group 1.
3.3.1. Psychopathology PANSS, SANS and SAPSxviii scores are presented in Table 3.2. (PANSS individual item scores range from 1 for absence of symptom to 7 for extreme symptomsxix). In terms of SANS and SAPS global dimension scores, the average global negative dimension and global psychotic dimension scores were both in the mild to moderate range, while the disorganisation dimension scores were in the low range (i.e. "questionable"). The adult male schizophrenic patients had significantly (p= 0.003) more positive PANSS scores (mean= 21.5; SD= 6.1) than the female patients (mean= 18.6; SD= 4.1), but there were no significant gender differences on the SANS & SAPS global symptom dimensions. Table 3.2. Psychopathology ratings Study I Drug-naïve schizophrenic patients: N=25 Age, years Mean= 27.3 (SD= 5.9) Gender 17 Male / 8 Female Diagnostic subtype* F 20.0 N = 18
F 20.3 N = 4 F 20.9 N = 3
PANSS ratings Positive symptoms Negative symptoms General symptoms Total symptoms
Mean= 20.2 (SD= 3.8) Mean= 19.7 (SD= 5.3) Mean= 30.2 (SD= 6.6) Mean= 70.1 (SD= 12.8)
SANS & SAPS global dimensions Negative dimension: Psychotic dimension: Disorganised dimension:
Mean= 2.3 (SD= 0.5) Mean= 2.9 (SD= 0.7) Mean= 1.0 (SD= 0.7)
*ICD-10 diagnostic subtypes. F 20.0= Paranoid schizophrenia; F 20.3= Undifferentiated schizophrenia; F 20.9=Unspecified schizophrenia.
3.3.2. Cognitive deficits All 25 patients completed all cognitive tests, with the exception of one patient who did not complete the DART, for whom a score was extrapolated from the patient group mean. All means and SD of cognitive measures are listed in Table 3.3.
xviii SANS and SAPS global severity ratings are: 0=None; 1=Questionable; 2=Mild; 3=Moderate; 4=Marked; 5=Severe. xix PANSS severity ratings are: 1=Absent; 2=Minimal; 3=Weak; 4=Moderate; 5=Moderate/Severe; 6=Severe; 7=Extreme.
Table 3.3. Cognitive deficits at baseline Study I
Patients at
baseline (N=25)
Healthy controls (N=25)
Principal components*, and component measures
Variance explained
(%) MEAN SD MEAN SD Sig. levels
2-sided
Effect size
z-scoresPREMORBID INTELLIGENCE:
DART 24.32 9.18 29.44 7.44 0.04 -0.69 EXECUTIVE FUNCTIONS:
WCST Set Shifting: - Perseverative errors - Perseverative errors: % of total errors
10.60 54.9
7.33 18.8
6.44 65
3.1915.4
0.01 ns
-1.30
WCST Learning efficiency:- Other errors - No. of cards used
8.84 91.20
9.27 23.10
3.32 76.80
1.9912.05
0.007 0.009
-0.40 -1.19
IED Set Shifting: - Errors at the EDS stage - EDS errors: % of total errors IED Learning efficiency: - Completed stage errors - Completed stage trials
-0.05
7.32 25.6
0.13
12.08 69.96
1.13
10.55 20.8
1.33
9.22 19.79
-0.24
4.76 26.2
-0.28
10.04 68.60
0.74
6.8013.4
0.69
3.979.48
ns ns
ns ns
SOC planning efficiency: - No. problems/min moves - Mean number of moves
95.2 % -0.44 8.32 4.33
0.90 1.73 0.41
0.34 9.88 4.00
1.262.150.65
0.02 0.007 0.04
-0.62 -0.73 -0.50
Trailmaking: - Trail-Making B (sec) - Trail-Making B-A (sec)
98.2 % 0.51 89.77 56.64
1.37 47.45 39.92
-0.35 58.07 33.49
0.4616.6013.83
0.006 0.004 0.01
-1.86 -1.90 -1.67
Fluency: - Phonological verbal Fluency- Semantic verbal fluency - Figural fluency
63.4 % -0.61 11.84 19.04 30.64
0.77 3.44 4.70 10.41
0.77 17.24 26.00 42.20
0.885.095.4712.00
<0.0001 <0.0001 <0.0001 0.0006
-1.57 -1.06 -1.27 -0.96
ATTENTION: RVP selective attention: - Signal detection (A') - No. of hits - No. of misses
99.5 %
-0.42 0.97 49.64 6.04
1.36 0.03 6.04 6.16
0.34 0.99 53.24 2.76
0.460.012.072.07
0.01 0.02 0.009 0.02
-1.64 -1.60 -1.74 -1.58
LATENCIES Reaction Time: - Simple Recation time (log) - Choice reaction time (log)
83.8 % 0.68
5.81 5.90
1.83
0.35 0.34
-0.39
5.62 5.72
0.47
0.080.11
0.009
0.01 0.01
-2.28
-2.51 -1.72
Movement time: -Simple Movement time (log)- Choice movement time (log)
96.9 %
0.91
6.43 6.44
0.95
0.24 0.26
-0.24
6.14 6.14
0.60
0.160.15
<0.0001
<0.0001 <0.0001
-1.91
-1.76 -1.94
SOC initial thinking time (log)
8.49 0.64 8.72 0.53 ns
SOC subsequent time (log) 6.54 0.92 4.92 2.15 0.001 -0.77 *Through factor extraction, the principal components were standardised to a mean of 0 and a SD of 1. Figure 3.1. Cognitive deficits (Z-scores) Study I
-3
-2,5
-2
-1,5
-1
-0,5
0
WC
ST P
-err
ors
WC
ST %
P-e
rrors
WC
ST O
-err
ors
WC
ST T
otal
car
ds
ED
S er
rors
% E
DS
erro
rs
Com
pl.e
rrors
Com
pl. t
rials
Fact
or T
rails
B
Fact
or F
luen
cy
Fact
or R
VP
SO
C P
lann
ing
SO
C In
i Lat
ency
SO
C S
ub la
tenc
y
Fact
or M
ovem
ent t
ime
Fact
or R
eact
ion
time
Z-sc
ores
(SD
)
Adult patients IntelligenceThe patients had a significantly lower DART estimated premorbid IQ than the healthy control group (p= 0.04; z-score= -0.69). Entering premorbid IQ as covariate in ANCOVA between-group analyses on the remaining cognitive tests did not change the significant differences between patients and controls. Even though premorbid IQ did change the significance level of differences between groups on some tests, it did not impact to an extent that changed significant results to tendencies or non-significance (nor in the opposite direction). Executive functions WCST: The outcome measures from the WCST are notoriously skewed, as was also the case in this sample. After log transformation, the results approximated a normal distribution, and z-scores were calculated. The outcome measure selected to examine attentional
15

set shifting ability (total number of perseverative errors) showed a significantly lower performance in patients than controls (p= 0.01; z-score= -1.3), but there was no difference between groups on percentage perseverative errors. In terms of learning efficiency, there was a significantly worse performance in patients than controls on other errors (p= 0.007; z-score= -0.4), and on total number of cards used (p= 0.009; z-score= 1.19). The percentage other errors was not different between groups. Nelson perseverative errors 228 and unique errors 208 were skewed even after log transformation, and results were instead compared using non-parametric analyses. Exploratory analyses revealed a significant difference between patients and controls on Nelson perseverative errors (p= 0.0002) and a tendency towards a difference on unique errors (p= 0.08). While 95 % of controls made 1 or less Nelson errors, 48 % of patients made more than 1 Nelson error, ranging from 0-21 errors, with an outlier making as many as 70 Nelson errors. Similarly, 95 % of controls made 1 or less unique errors, while 28 % of patients made more unique errors, ranging from 0-20 errors (again with an outlier, who made 50 unique errors). IED Set Shifting task: Similarly to the WCST, measures assessing attentional set shifting ability and learning efficiency from the IED were calculated. Errors made at the EDS stage were logged to fit a normal distribution, and the percentage of total errors made at the EDS stage was calculated, both as measures of set shifting ability. There were no differences between patients and controls on either measure of set shifting ability. Learning efficiency was assessed using the completed stage errors and completed stage trials, on which there were no differences between patients and controls. In the patient group, 76 % reached criterion and completed all 9 stages of the test, which was not significantly different from the control group, in which 88 % completed all 9 stages. Trail Making: Patients took significantly longer to complete both Trail Making tasks A and B, but with a level of deficit that was approximately 1 SD more impaired on the Trail Making B than version A (Trail Making A: p= 0.005; z-score= 0.98, and Trail Making B: p= 0.004; z-score= 1.90). The subtracted difference between Trail Making A and B was significantly impaired in the patient group compared to the healthy controls (p= 0.01; z-score= 1.67). Stockings of Cambridge: The efficiency of problem solving in the SOC was significantly worse in the patient group: Number of problems solved with the minimum number of moves (i.e. most efficiently) (p= 0.007; z-score= -0.73), and mean number of moves made with 2,3,4,5 moves combined (p= 0.04; z-score= 0.5). A similar level of impairment was seen when these two measures were combined in the planning efficiency factor (p= 0.02; z-score= -0.62). The initial and subsequent latencies were skewed and log transformed to approximate a normal distibution.There were no significant differences between patients and controls on the initial thinking latencies involved in solving the SOC. However, the subsequent thinking latencies were significantly slower in the patient group than the control group (p= 0.001; z-score= -0.77). Fluency: The differences between patients and controls on verbal and figural fluency tasks were all highly significant and all at a similar level of impairment in patients: Phonological verbal fluency (p= 0.00006; z-score= -1.06), semantic verbal fluency (p= 0.00001; z-score -1.27), and figural fluency (p= 0.00065; z-score= -0.96), and the combined fluency factor combining all 3 tasks (p<0.0000006; z-score= -1.57).
Selective Attention: Rapid Visual Information Processing: The combined factor of selective attention, calculated from the A', hits, and misses sub-scores from the RVP, was significantly impaired in patients (p= 0.013; z-score= -1.64), as was each component score= A' (p= 0.015; z-score= -1.6); Hits (p= 0.009; z-score= -1.74), and Misses (p= 0.02; z-score= 1-58). Reaction and Movement times: In the 5-Choice Reaction and Movement task, both reaction and movement times were skewed; therefore, latencies were log transformed. Both the simple and choice reaction and movement times were much slower in the patient group, with highly significant between-group differences. Simple movement time (p= 0.00001; z-score= -1.76), Choice movement time (p= 0.00001; z-score= -1.94); Simple reaction time (p= 0.01; z-score= -2.51), and Choice reaction time (p= 0.01; z-score= -1.72). Principal components were calculated, combining movement time and choice movement time into a movement time factor, and reaction time and choice reaction time into a reaction time factor, which were both impaired (Movement Time Factor p= 0.000005; z-score= -1.91; and Reaction Time Factor p= 0.009; z-score= -2.3).
3.3.4. Effects of antipsychotic medication on cognitive deficits The results are described in more detail in the enclosed paper in Appendix 1, but are summarised below. Psychopathology: There were significant improvements in both the risperidone group and zuclopenthixol group on PANSS positive, negative, general, and total scores, with no differential changes between groups. The patients in the zuclopenthixol group had a tendency towards more EPS after medication than the risperidone group (p=0.07), and consequently significantly more patients in the zuclopenthixol group received anticholinergic medication (Pearson's χ2 = 6.8; p= 0.009). Cognitive deficits: Using baseline scores as covariates for all analyses, only few differential changes in cognitive functions were seen between the risperidone and zuclopenthixol groups. There were no differential changes on measures of executive functions or attention. However, regarding latencies on the Movement time and Reaction time tasks, a significant differential change was found between the medication groups on the combined factor Movement time (p=0.004), and a tendency towards a difference was found on the combined factor Reaction time (p=0.08). When improvements in psychopathology (PANSS scores) were entered as covariates in the between-group analyses, the difference between groups on Movement time remained significant, while the tendency towards differential change on Reaction time remained at trend level after covarying for negative, general, and total PANSS scores, but disappeared when covarying for positive PANSS scores. Entering ESRS ratings and anticholinergic medication in separate analyses each covaried out differences on Reaction time. Changes in both medication groups were parallel to the changes (retest effects) in the healthy control group on most measures. However, the control group showed a significantly larger retest effect on Movement time than both the risperidone (p=0.007) and zuclopenthixol group (p=0.003), and a significantly larger improvement on SOC planning efficiency than the zuclopenthixol group (p=0.02).
16

3.4. Discussion
3.4.1. Demographics It was not possible to obtain a full match between patients and controls on SES, even though this was originally attempted. While there were no differences in terms of parental education/occupation, the level of income (and combined SES) was significantly lower in the patient group. This is a possible confounding factor in the interpretation of cognitive results, especially IQ results. While the relation between SES and estimated premorbid IQ (with parental combined SES accounting for 26 % of the variance in IQ scores) was similar to that previously found in patient samples 1, no significant correlation was found between any SES measures and estimated premorbid IQ in the control group. This was unexpected and may be due to a selection bias in the control group or a Type II error because of the small sample.
3.4.2. Cognitive deficits The advantage of examining first-episode (especially drug-naïve) patients is the opportunity to study patients without the presence of possibly confounding factors such as previous long-term medication, hospitalisation, the progression of the disease process itself or a combination of the above. The discrepancies of previous findings concerning the pattern and extent of cognitive deficits are possibly due to differences between the patients in terms of clinical status, stage of illness, treatment history, as well as the variability of the cognitive functions studied. The present sample was homogeneous to the extent that only patients who had never before received antipsychotic medication were included. The patients were not stabilised clinically during baseline assessment, but several studies have shown that the presence of psychosis does not affect the reliability of neuropsychological tasks 77;78. Intelligence: The estimation of premorbid intelligence was based solely on a measure of verbal intelligence. This is because certain verbal abilities are highly consolidated and have been shown to be remarkably stable and intact after various forms of cerebral insults 135. While there are tests of performance intelligence that correlate well with both Performance IQ and full-scale IQ (such as WAIS Block Design and Raven's Progressive Matrices 229), these tests are sensitive to many kinds of cognitive change, and thus are not good estimators of the potential premorbid level. The NART (respective DART) is often used as the single measure of pre-morbid intelligence, because it has been shown to be remarkably stable even after neurological insults and is a reliable measure of highly consolidated cognitive abilities and knowledge 135. Most studies have shown NART to be an accurate estimate of pre-morbid IQ in schizophrenia patients 230-
232, although a recent study cautions against an estimation of pre-morbid IQ based solely on the NART233. The patients had significantly lower estimates of premorbid IQ than controls, at the level of 0.69 SD, which is similar to the level found in previous studies 234. Controls were deliberately not matched to patients according to IQ, because several possible confounding factors are involved in matching according to IQ. Matching according to premorbid IQ systematically mismatches patients and controls by underestimating the potential IQ of patients, and creates non-representative groups of both patients and controls. In the patient group, there were highly significant correlations between the measures of premorbid intelligence and SES. The lack of such correlations in the control group does not support what has been found previously 1, but may be due to a Type II error due to the small sample size.
Executive functions WCST: While there are several potential outcome scores from the WCST, only specific outcome scores were selected in order to examine attentional set shifting ability (perseverative error scores and percentage perseverative errors) and learning efficiency (other errors and percentage other errors, as well as number of cards used to solve the test). Numerous studies have shown that schizophrenic patients make more perseverative errors than controls on the WCST, and this has been widely interpreted as a specific executive deficit of failure to shift attention (reviewed by Laws 221). However, the problem with this interpretation is that the perseverative errors are made in the context of an increased total number of errors, encompassing other, more non-specific types of errors. The measure of percentage perseverative errors is an indication of whether a disproportionate share of errors is perseverative in nature. This measure is a more valid indication of a specific executive deficit, and has been found to be the measure that best characterises the errors made by frontal lobe patients 221. The most widely used version of WCST in schizophrenia research is Heaton's version from 1981 235 and 1993 236, in which perseverative error scores are more broadly defined than according to Nelson's or Milner's original definitions 208;228, and are too non-specific to fulfil the cognitive definition of perseveration as "stuck in set" errors, and instead involve a more generalised pattern of errors. The non-specific nature of this broader definition of perseverative errors was illustrated in a study, in which a large proportion of healthy controls were characterised as having perseverative errors at a level of "possible frontal lobe dysfunction" as defined by the WCST norms 235;236. The present results support the presence of more perseverative errors in schizophrenic first-episode patients than in controls, at a level of impairment that is similar to what has previously been found 40;47. However, these errors were not disproportionate to the total number of errors made. As such, the perseverative errors can be interpreted as part of a generalised pattern of errors that encompasses problems with rule learning, distraction, or guessing. This is in accordance with a meta-analysis from 1999 including 29 studies, which found medium effect sizes when the number of perseverative errors was used as outcome measure, but only small effect sizes (d=0.18) when percentage perseverative errors was considered 221. The indication that deficits on the WCST in this study are dependent on generalised cognitive functions more than specific executive functions was supported by the deficits on the measures of other errors and number of cards used that in the present study was termed learning efficiency. The level of impairment on Other errors (z-score= -1.38) was equal to that of Perseverative errors (z-score= -1.34), and similarly, the Other errors were not disproportionately prevalent compared to the total number of errors in the patient group. In conclusion, the deficits on the WCST may represent a non-specific rather than purely executive deficit, but conversely, executive deficits may not be detected by the WCST because of the multimodal nature of the test. IED Set Shifting: The IED task was the only test on which patients were not impaired compared to controls. Neither of the measures of attentional set shifting or learning efficiency was significantly different from controls. In terms of ability to reach criterion at all 9 stages, 76 % of patients completed the whole test. The lack of set shifting deficits is very similar to what has previously been found in first-episode patients, where Hutton et al. found that 80 % of patients in their first-episode sample completed all stages
17

of the test 50. In comparison, chronic patients are considerably more impaired on the IED set shifting task, with the percentage of patients completing the task as low as 40 % 49. The chronic patients make more perseverative errors both at the EDS stage and earlier stages, supporting deficits of reactive flexibility. In fact, chronic schizophrenic patients have more severe deficits also at earlier stages of the IED Set Shifting task than frontal lobe patients, suggesting that deficits involve more than the frontal lobes. In a sample of severely disabled chronic patients hospitalised for approximately 18 years, Pantelis et al. found severe, more generalised deficits of both concept formation and set shifting 210. These results yield support for a progression of executive deficits from first-episode to chronic phase. However, follow-up studies of the patients included in this study will help substantiate this. Trail Making: Deficits on the Trail Making test were seen on both versions A and B, supporting deficits of visuomotor speed. The deficits on Trail Making B, and the subtracted difference between versions A and B were more impaired than performance on Trail Making A by approximately 1 SD. This indicates that the increased level of impairments on Trail Making B (in addition to visuomotor slowing) involves deficits due to the demands for continuous cognitive alternation between letters and numbers in version B, which requires focused attention and executive reactive flexibility. Stockings of Cambridge: The profile of impairment in the patient group of less efficient problem-solving and increased subsequent thinking latencies (but without major impairments on planning latencies) indicates that patients do not benefit from the time spent planning the task, and instead attempt to compensate from this inefficient planning by spending more time solving the task. The adult patients had longer subsequent thinking times than controls, mostly but not only, on the most difficult problems. They took significantly longer to solve problems involving 4 and 5 move solutions, but also showed a tendency towards longer latencies on problems involving only 2-move solutions. Overall, the patients did not have significantly shorter initial thinking times than controls, but patients had tendencies towards shorter latencies on some of the difficult problems. The combination of normal initial thinking latencies with inefficient problem solving could indicate that patients do not spend the initial thinking time on planning how to solve the task, but because of a more general slowing in reaction times, the initial thinking latencies are not faster than that of controls. In spite of spending longer time solving problems, patients solve fewer problems efficiently and make more errors, which suggest a problem in strategy monitoring. This is similar to what has previously been found in a study of first-episode patients, in which patients had faster planning times only on difficult problems, and longer subsequent latencies 50 (although another first episode study did not find longer subsequent latencies 119). In comparison, chronic patients do not have shorter planning times, but longer subsequent thinking times 49;51;120. In terms of underlying neurobiological processes, the longer subsequent thinking times are non-specific, and have been found in other patient groups involving basal ganglia impairments, such as Parkinson's disease, Huntington's disease, as well as in patients with temporal lobe excisions 50;237;238. Fluency: Patients were impaired on both the phonological and semantic verbal fluency tasks, with a similar level of impairment in both. Differential deficits on semantic verbal fluency tasks can be interpreted as abnormal organization of words and concepts in semantic memory, while similar impairment on phonological and semantic fluency tasks can be interpreted as deficits in initiating and executing relevant search strategies 63;239;240. Studies rarely include a measure of figural fluency, in spite of it
being perhaps a more pure test of fluency (being less dependent on learnt verbal abilities), which is supported by factor analytic studies that cluster figural fluency tasks among the more clean tests of putative frontal function 144;241. The impairment on figural fluency was similar to the impairments of verbal fluency, which suggests that the fluency deficits are not lateralised (as has previously been proposed) 153, but due to problems with the initiation of effective problem solving strategies regardless of whether verbal or nonverbal material is involved. This supports a problem with executive spontaneous flexibility. Selective attention: Rapid Visual Information Processing Test: The patients were significantly impaired on the RVP, both in terms of the number of hits and misses and on the ability to distinguish signals from noise (A'). The performance of patients did not deteriorate during the RVP test, and there are no significant differences over the 7 minutes of each version. This suggests that the impairment on the RVP does not involve problems with sustaining attention over time, but rather in focused, selective attention. This supports previous findings of a profile of higher level attentional deficits in schizophrenic patients of selective, but not sustained attention 157;242. Reaction and movement times: The patients showed extensive impairments with longer latencies than controls on both reaction and movement time tasks, in both the simple and choice conditions. The present results do not support a disproportionate level of impairments in the choice condition (in which the stimulus location is unpredictable) compared to the simple condition. This has important implications for the interpretation of reaction time deficits, because it shows that the increased latencies are present at the level of simple invariant response initiation (in the simple condition), and not only when response inhibition is also required (as in the choice condition) 175. Of particular interest is that the increased latencies are not only present in mental speed of processing, but also in motor movement time. The results also show that slow reaction and movement times are not caused by medication because the deficits are present in patients when drug-naïve. Eberhard et al. 122 stress the similarity between reaction time deficits in schizophrenia, and neurological illnesses involving the basal ganglia, and interpret both as involving a markedly reduced response readiness.
3.4.3. Effects of antipsychotic medication on cognitive deficits The results are discussed in more detail in the paper attached (Appendix 1), but the discussion is summarised below. Psychopathology: Both the risperidone and zuclopenthixol groups improved significantly on all global PANSS measures, without any differential changes between groups. However, even with comparable, low doses of both compounds, the typical compound zuclopenthixol causes more EPS and therefore more adjunctive anticholinergic medication than risperidone. Cognitive deficits: There were no differential changes between the risperidone and zuclopenthixol groups on most cognitive measures, except for reaction time and movement time. When only the two medicine groups are included in the analyses, there were differential changes (significant or at trend level) between groups on reaction time and movement time, reflecting significant within group changes in the risperidone group and a lack of change in the zuclopenthixol group. These differential changes were still present after controlling for improvements in psychopathology scores, except when differential changes in reaction time were covaried for improvements in positive symptom scores. This indicates that the tendency towards differential change in
18

reaction time (with within group improvements in the risperidone group) may be related to improvement in positive symptoms. In separate analyses, the differential changes between risperidone and zuclopenthixol on reaction time and movement time were no longer significant when covaried for EPS and adjunctive anticholinergic medication, both of which were more prevalent in the zuclopenthixol group. However, these secondary analyses should be interpreted with caution due to the small sample size. In summary, it appears that the risperidone group improves significantly on reaction time and movement time, and the zuclopenthixol group remains stable, possibly due to more EPS and anticholinergic medication. However, when compared to the healthy control group, neither the risperidone group nor the zuclopenthixol group showed improvement on reaction time and movement time that reached the extent of the retest effects in the healthy control group. Therefore, the within group changes in the risperidone group on reaction and movement time may be interpreted as retest effects (although not to the extent of the healthy control group) rather than improvements due to the medication. Similarly, the lack of change in the zuclopenthixol group on the same measures as well as SOC planning efficiency may be interpreted as actual detrimental effects of medication (possibly through more prevalent EPS and anticholinergic medication). The results contribute to the field particularly through the inclusion of only drug-naïve patients experiencing their first episode, which enables the assessment of impact of medication on cognitive functions at an early stage of the illness, where the confounding factors of previous medication and a long course of illness are not present. In addition, comparable, low doses of risperidone and zuclopenthixol were used. The results underscore the theoretical importance both of controlling for the impact of clinical improvement, side effects, and adjunctive medication when assessing effects of medication, and of examining retest effects in healthy controls as a necessary standard of reference before changes over time (or lack thereof) can be attributed to detrimental effects, no effects, or beneficial effects of medication. Regardless of the theoretical implications of efficacy of antipsychotics (which is the most important of the points presently at issue), the clinical implication is a tentative indication in favour of risperidone over zuclopenthixol, based on the more prevalent EPS, adjunctive anticholinergic medication, and lack of change on most measures in the zuclopenthixol group compared to the risperidone group. However, the conclusions that can be drawn from the results are limited by the small sample size, which increases the risk of both type I and type II errors. Also, the time period of 3 months from the unmedicated baseline test to retest after medication may be too short to detect both within and between group changes that may potentially occur later, after longer exposure 199. 3.5 Conclusions Hypotheses: The hypotheses of Study I were not all supported. Hypothesis 1 was supported: The patients had significant deficits in all cognitive domains of attention, executive functions, and reaction time. Hypothesis 2 was also supported: The profile of executive deficits found impairments in spontaneous flexibility, with a relative sparing of reactive flexibility, which is similar to what has previously been found in first-episode patients. Hypothesis 3 was not supported: There was little evidence for differential beneficial effects of risperidone over zuclopenthixol on cognitive deficits, except for on measures of reaction time and
movement time, which in turn could not be distinguished from retest effects. Conclusions: The adult schizophrenic patients show deficits of executive functions, selective attention, and reaction time at first episode, when drug-naïve, in domains that previous studies have found are also impaired in chronic schizophrenic patients. The profile of executive deficits, however, is different from the profile of chronic schizophrenic patients in past studies. The study supports that executive deficits in spontaneous flexibility are more prevalent during the early stages of the illness than deficits in reactive flexibility. The profile of lack of impairment on the IED set shifting task with impaired performance on the SOC is not merely due to differences in difficulty, as the tests are not inherently different in level of difficulty. This is supported by the fact that chronic schizophrenics as well as other patient-groups (e.g. frontal lobe patients, and Huntington's patients) are more impaired on the IED than the SOC. The theoretical implication may be that during the course of the illness, it appears that the pattern of executive deficits change and progressively deteriorate, such that the deficits in executive reactive flexibility surpass those of spontaneous flexibility later on in the disease process. This supports that subcortical areas and fronto-striatal pathways are increasingly more implicated in the cognitive deficits as the disease progresses after illness onset.
Chapter 4: Study II: Children and adolescents with first presentation schizophrenia or non-schizophrenic psychosis This was a cross-sectional study examining cognitive functions in first-episode children and adolescents with non-organic psychotic as well as an age- and gender matched control group. Psychopathology ratings, MRI scans, and neurological examinations were carried out as part of a parallel Ph.D. project conducted by M.D. Katrine Pagsberg, and those results are presented elsewhere. Results concerning cognition and relations to psychopathology are presented. 4.0. Theoretical background: Children and adolescents with
schizophrenia and psychosis
4.0.1. Prevalence and diagnostic stability and validity of early onset schizophrenia The prevalence of schizophrenia in childhood and adolescence is low compared to illness onset in adulthood. Some studies estimate the prevalence of schizophrenia in childhood before the age of 13 as low as 1:10 000 243, which is very rare compared to the adult onset schizophrenia rate of around 1:100. Very early onset schizophrenia (VEOS) before the age of 10 is exceedingly rare. After age 13, there is a remarkable increase in illness prevalence compared to younger children, although the precise estimates vary 128;244. Since Kraepelin 4 and Bleuler 5, early onset in childhood and adolescence has been seen as a rarely occurring subtype of schizophrenia, with similar clinical presentation. However, until the 1970's, other pervasive developmental disorders were considered as indicators of later schizophrenia, and included with schizophrenia in early onset studies 244. Therefore, there has been a dearth of studies of what is now specifically considered early onset schizophrenia. Since the 1970's, a clear distinction was made between childhood onset schizophrenia and autism, and from the diagnoses of DSM-III and ICD-9, the same criteria used to diagnose adult onset schizophrenia have been used for child and adolescent onset patients 244. While the diagnosis of
19

schizophrenia was previously only given to adult patients, according to present diagnostic systems, the diagnosis can be given to children as young as 7 years of age in accordance with the same criteria used for adults 245;246. The age limit of 7 years is due to the diagnostic dependence on subjective reporting of symptoms, which is considered unreliable below the age of 7 243. However, in Denmark, the diagnosis of childhood and adolescent onset schizophrenia was only introduced when the ICD-8 was replaced with the implementation of the ICD-10 in 1995 243; therefore, the use of the schizophrenia diagnosis in childhood and adolescence is recent in clinical practice. The reason for the renewed use of the schizophrenia diagnosis in children and adolescents is that the diagnosis is more stable than previously thought 244. However, most studies estimate that the diagnosis of schizophrenia is not as stable in early onset patients as in adult patients, even though the estimates vary considerably. While the stability of adult schizophrenic diagnoses in different studies has been found to be between 74-93 % 247-250, in EOS, between 20–35 % of patients with an initial diagnosis of schizophrenia change diagnoses to other non-schizophrenic psychotic diagnoses, schizoaffective or affective diagnosis at subsequent follow-up 243;251;252. A recent longitudinal study at Maudsley Institute of Psychiatry followed early onset patients over a period averaging 11.5 years after onset to determine diagnostic stability. The diagnosis of schizophrenia in childhood and adolescence was stable, with a positive predictive validity of 80 % 252, which is comparable to the stability of the diagnosis in adult samples. However, there is a larger proportion of patients that change diagnoses in the other direction, from different non-organic psychotic diagnoses in childhood and adolescence to schizophrenia at follow-up 251. In other words, a large proportion of early onset patients, who receive various diagnoses of non-organic psychosis at illness onset, are later diagnosed with schizophrenia, although the exact proportion is unclear 251.
4.0.2. Early onset schizophrenia: Increased vulnerability and worse outcome Recently, studies focusing on the group of early onset schizophrenia have increased for several reasons. The formulation of the neurodevelopmental hypothesis of schizophrenia 92;93 has provided a theoretical incentive for focusing research on the early onset patients because of the theoretical implications for schizophrenia, regardless of age of onset. Interest has converged on genetic, neurobiological, and neuropsychological aspects, because early onset schizophrenia is considered clinically and etiologically continuous with adult onset schizophrenia, but with more severe clinical symptoms, neurobiological and premorbid vulnerability indicators, and familial schizophrenia spectrum incidence in early than adult onset patients. As such, the early onset patients are considered a subgroup of patients with increased genetic and neurodevelopmental vulnerability towards developing schizophrenia. EOS is considered etiologically and clinically continuous with adult onset schizophrenia, but is characterised by a more insidious onset 97. The evidence of continuity stems from both from family studies and clinical follow-up studies. The UCLA family studies have found similar patterns of other psychiatric disorders in parents of EOS as has been found in parents of adult onset schizophrenia (AOS), supporting a similar etiological background 70. However, there is some evidence for a higher prevalence of familial schizophrenia spectrum incidence in EOS patients 253;254. The clinical symptomatology of EOS appears to be continuous with AOS 246, although studies support the presence of more negative and disorganisation symptoms in early onset patients 255.
According to the neurodevelopmental hypothesis, an early onset of illness is an indicator of an accelerated and thus more severe disease process, progression and outcome 92;93. This is supported by studies that have found more vulnerability indicators, such as obstetric complications and developmental delays in patients with an early onset. Early onset schizophrenia have a higher incidence of premorbid developmental delays of function; e.g. concerning acquisition of motor and language skills 99;256, which in some form is present in approximately 20 % of early onset patients, which compares to a prevalence of approximately 10 % in adult onset patients 98;244. The characterisation of neuropsychological deficits at various ages of onset and stages of the disease can help examine the neurodevelopmental hypothesis, and the hypothesis of progressively deteriorating functions. Early onset schizophrenia patients have a more severe course of illness and most of the evidence points towards a worse functional social and vocational outcome than schizophrenia with adult onset, and other psychotic disorders with onset in adolescence 257;258, although this is not unanimous 97. Patients with very early onset schizophrenia (VEOS) before the age of 13 have a very poor prognosis, as do the patients for whom the onset is insidious 128;259. Conversely, adult patients with a later onset (typically women) tend to have a milder course of illness 260. Patients for whom schizophrenia spectrum diagnoses are prevalent in close family members (and thus are considered to have increased familial load) have a worse prognosis 128, while good premorbid function socially and cognitively are indicators of a good prognosis 258.
4.0.3. Cognitive deficits in early onset schizophrenia Several studies have found cognitive deficits in childhood and adolescent onset patients, in the same cognitive domains as AOS 97;253. However, there is some evidence that early onset patients may have a more homogenous profile of deficits than AOS 131. The cognitive deficits that are best substantiated in EOS are in the domains of working memory, attention, and speed of information processing 131. Asarnow 96;131;261;262 hypothesised that the cognitive deficits in early onset patients are caused by a reduced working memory capacity (which implies that there is insufficient work space to process complex tasks), and/or deficits in the executive functions that do not sufficiently control the allocation of resources to relevant information needed in complex tasks. Deficits in the same domains are found in other developmental disorders (such as Attention Deficit Hyperactivity Disorder (ADHD)), although the specific profiles and extent of deficits differ 244. In contrast, functions that are normally considered "crystallised", such as basic rote memory and language, are spared. Retrospective studies have found that premorbidly, language acquisition is slow and both gross and fine motor functions are impaired. However, studies of language functions in EOS after illness onset have not found particular impairments in this area, suggesting a pre-morbid developmental delay in language acquisition, rather than a stable deficit 262. However, EOS patients have more extensive deficits on IQ measures than AOS. Most studies have found lower IQ levels in EOS patients, with averages generally ranging from 80-90 (approximately 1-1½ SD below the normative mean) 103;131;256;261;263. Approximately ⅓ of EOS patients have IQ levels lower than 70, which lies in the range of mild retardation 244. This average IQ level in early onset patients is approximately 10 IQ points (almost 1 SD) lower than that found in studies of patients with adult onset schizophrenia. According to the neurodevelopmental hypothesis, it is expected that EOS may be associated with more severe cognitive deficits than AOS. However, there have been very few studies done that have enabled direct comparisons of patterns and levels of
20

deficits in EOS and AOS, and the conclusions remain equivocal. An important factor in determining whether EOS represents a sub-group of schizophrenic patients with more severe cognitive deficits than AOS, is the stage of illness at which patients are studied. Retrospective studies of chronic patients show that patients who had an early onset of illness are more cognitively impaired than patients with later onset 264;265. However, studies of early onset patients examined recently after illness onset have failed to find evidence for more severe deficits in this group than in adult onset patients 266. These are particularly significant findings in terms of the implications for the neurodevelopmental and neurodegenerative hypotheses 267;268. The EOS patients may not initially have a worse cognitive profile than AOS at the first episode, but may represent a subgroup of patients with progressively deteriorating functions. An early onset study at Maudsley did not find a significant effect of duration of untreated psychosis (DUP) on cognitive deficits, which does not support a progressive deterioration 266. However, other factors such as the number of psychotic episodes may instead be involved in a possibly increased deterioration 122, and head-to-head comparisons of patients with EOS and AOS at different stages of the disease are warranted. Similarly, it is unclear whether cognitive deficits are more prevalent in early onset patients with schizophrenia compared to other early onset patients with non-organic psychotic disorders, because very few studies have directly compared early onset schizophrenic and other psychotic disorders and the conclusions are equivocal. In other words, whether the findings of increased premorbid indicators, and prevalent cognitive deficits is specific to early onset schizophrenia or more generally to early onset psychosis is unclear 251;256;269;270. 4.1. Study Objectives and Hypotheses Objectives: The primary objective was to characterise the profile of cognitive deficits in the domains of executive, attentional, and reaction time functions in early onset psychotic patients. The secondary objective was to examine whether there are differences between early onset schizophrenia (EOS) and non-schizophrenic psychosis (NSP) in terms of pattern and level of cognitive deficits. Hypotheses: 1. The patients have significantly lower IQ than controls 2. The patients have significant deficits in all cognitive domains of attention, executive functions and reaction time. 3. The patients with EOS and NSP have a similar profile and level of cognitive impairment. 4.2. Methods
4.2.1. Subjects Patients: Patients were included from February 1998 to February 2002 from child- and adolescent psychiatric departments in the Copenhagen and Northern Zealand catchment areas. (The population in the catchment area is 1.8 million people.) The participating referring hospitals were: Bispebjerg Hospital; Copenhagen County Hospital Glostrup; and Frederiksborg County Hospital Hillerød. Patient inclusion and exclusion criteria: The inclusion criteria were: Patients between the ages 10-18, referred for treatment to a psychiatric department for the first time. The diagnostic inclusion criterium was an ICD-10 (International Classification of Diseases; World Health Organization) diagnosis of non-organic psychosis. These diagnoses encompassed F.20 Schizophrenia, F. 21 Schizotypal
disorder, F. 22 Persistent delusional disorder, F 23 Acute and transient psychotic disorder, F. 25 Schizoaffective disorder, F. 28 Other non-organic disorder, F. 30.2 Mania with psychotic symptoms, F. 32.3 Severe depressive episode with psychotic symptoms. The exclusion criteria were: Any known or suspected mental retardation (IQ<70); the presence of any chronic somatic illness, neurological illness or severe head injury; and a history of alcohol or drug abuse, or antipsychotic treatment for more than 6 months. Psychopathology: Diagnoses were made using the Schedules for Clinical Assessment in Neuropsychiatry Version 2.1 (SCAN 2.1) interview, and psychopathology ratings were carried out using PANSS (Positive and Negative Syndrome Scale) SANS and SAPS (Scale for the Assessment of Negative Symptoms and Scale for the Assessment of Positive Symptoms) by the same psychiatrist (M.D. Katrine Pagsberg). Diagnostic interviews were videotaped and co-rated with other psychiatrists to ensure validity of ratings. SANS and SAPS scores were divided into 3 dimensions: psychotic symptoms, negative symptoms, and disorganised symptoms in accordance with recommendations from meta-analytic studies of the most valid distinction of symptom dimensions in schizophrenia180. Recruitment process: Recruitment and SCAN interviews of patients were done by M.D. Katrine Pagsberg. During the 4-year inclusion period, 191 patients were referred to the project with a possible diagnosis of non-organic psychosis. Of these, 167 completed the SCAN interview, 88 of whom fulfilled the study criteria for inclusion in the project. A total of 48 patients agreed to participate and were included in the project. Patient drop-out (from the N=48) occurred for the following reasons: Patient withdrawal (N=2); exclusion because of hydrocephalus discovered in the MR scan (N=1); inability to participate in neuropsychological tests due to psychotic or anxiety symptoms (N=5). Of the 5 patients who did not complete neuropsychological tests, 4 were diagnosed with schizophrenia (paranoid schizophrenia N=1; hebephrenic schizophrenia N=1; and undifferentiated schizophrenia N=2) and 1 was diagnosed with mania with episodic psychosis. These 5 patients as a group had significantly more negative (p= 0.009), general (p= 0.003) and consequently total symptoms (p= 0.001) on the PANSS scale than the patients who completed the tests. In terms of SANS and SAPS global ratings, these 5 patients had significantly (p= 0.004) more symptoms in the disorganised symptom dimension (average rating disorganised dimension: 3, i.e. moderate; SD= 0.7) than the rest of the patients. Consequently, a total of 40 patients completed the neuropsychological assessments and are included in the present analysis. Diagnostic distribution Eighteen patients (45 %) were diagnosed with schizophrenia: F 20.0 Paranoid schizophrenia (N=13; 32.5 %), F 20.1 Hebephrenic schizophrenia (N=2; 0.5 %), F 20.3 Undifferentiated schizophrenia (N=2; 0.5 %), F 20.9 Unspecified schizophrenia (N=1; 0.25 %). Twenty two patients (55 %) received a diagnosis of non-organic, non-schizophrenic psychosis (NSP): F 21 Schizotypal disorder (N=10; 25 %), F 22 Paranoid psychosis (N=1; 0.25 %), F 23.3 Acute paranoid psychosis (N=1; 0.25 %), F 23.91 Acute psychosis, unspecified (N=1; 0.25 %), F 28 Other non-organic psychosis (N=8; 20 %), F. 32.3 Severe depressive episode with psychotic symptoms (N=1; 0.25 %). Antipsychotic medication: Of the 40 patients, 13 (32.5 %) were antipsychotic naïve, and 27 (67.5 %) were receiving antipsychotic medication when the
21
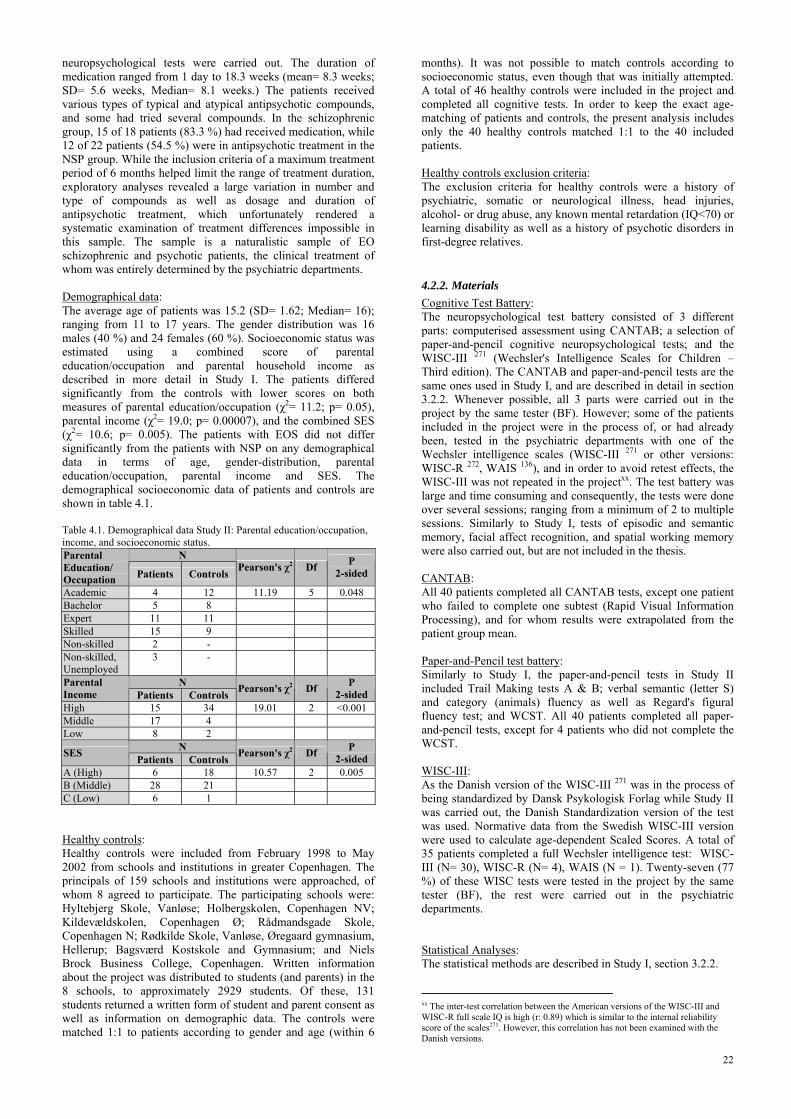
neuropsychological tests were carried out. The duration of medication ranged from 1 day to 18.3 weeks (mean= 8.3 weeks; SD= 5.6 weeks, Median= 8.1 weeks.) The patients received various types of typical and atypical antipsychotic compounds, and some had tried several compounds. In the schizophrenic group, 15 of 18 patients (83.3 %) had received medication, while 12 of 22 patients (54.5 %) were in antipsychotic treatment in the NSP group. While the inclusion criteria of a maximum treatment period of 6 months helped limit the range of treatment duration, exploratory analyses revealed a large variation in number and type of compounds as well as dosage and duration of antipsychotic treatment, which unfortunately rendered a systematic examination of treatment differences impossible in this sample. The sample is a naturalistic sample of EO schizophrenic and psychotic patients, the clinical treatment of whom was entirely determined by the psychiatric departments. Demographical data: The average age of patients was 15.2 (SD= 1.62; Median= 16); ranging from 11 to 17 years. The gender distribution was 16 males (40 %) and 24 females (60 %). Socioeconomic status was estimated using a combined score of parental education/occupation and parental household income as described in more detail in Study I. The patients differed significantly from the controls with lower scores on both measures of parental education/occupation (χ2= 11.2; p= 0.05), parental income (χ2= 19.0; p= 0.00007), and the combined SES (χ2= 10.6; p= 0.005). The patients with EOS did not differ significantly from the patients with NSP on any demographical data in terms of age, gender-distribution, parental education/occupation, parental income and SES. The demographical socioeconomic data of patients and controls are shown in table 4.1. Table 4.1. Demographical data Study II: Parental education/occupation, income, and socioeconomic status.
N Parental Education/ Occupation Patients Controls Pearson's χ2 Df P
2-sided
Academic 4 12 11.19 5 0.048 Bachelor 5 8 Expert 11 11 Skilled 15 9 Non-skilled 2 - Non-skilled, Unemployed
3 -
N Parental Income Patients Controls Pearson's χ2 Df P
2-sided High 15 34 19.01 2 <0.001 Middle 17 4 Low 8 2
N SES Patients Controls Pearson's χ2 Df P 2-sided
A (High) 6 18 10.57 2 0.005 B (Middle) 28 21 C (Low) 6 1 Healthy controls: Healthy controls were included from February 1998 to May 2002 from schools and institutions in greater Copenhagen. The principals of 159 schools and institutions were approached, of whom 8 agreed to participate. The participating schools were: Hyltebjerg Skole, Vanløse; Holbergskolen, Copenhagen NV; Kildevældskolen, Copenhagen Ø; Rådmandsgade Skole, Copenhagen N; Rødkilde Skole, Vanløse, Øregaard gymnasium, Hellerup; Bagsværd Kostskole and Gymnasium; and Niels Brock Business College, Copenhagen. Written information about the project was distributed to students (and parents) in the 8 schools, to approximately 2929 students. Of these, 131 students returned a written form of student and parent consent as well as information on demographic data. The controls were matched 1:1 to patients according to gender and age (within 6
months). It was not possible to match controls according to socioeconomic status, even though that was initially attempted. A total of 46 healthy controls were included in the project and completed all cognitive tests. In order to keep the exact age- matching of patients and controls, the present analysis includes only the 40 healthy controls matched 1:1 to the 40 included patients. Healthy controls exclusion criteria: The exclusion criteria for healthy controls were a history of psychiatric, somatic or neurological illness, head injuries, alcohol- or drug abuse, any known mental retardation (IQ<70) or learning disability as well as a history of psychotic disorders in first-degree relatives.
4.2.2. Materials Cognitive Test Battery: The neuropsychological test battery consisted of 3 different parts: computerised assessment using CANTAB; a selection of paper-and-pencil cognitive neuropsychological tests; and the WISC-III 271 (Wechsler's Intelligence Scales for Children – Third edition). The CANTAB and paper-and-pencil tests are the same ones used in Study I, and are described in detail in section 3.2.2. Whenever possible, all 3 parts were carried out in the project by the same tester (BF). However; some of the patients included in the project were in the process of, or had already been, tested in the psychiatric departments with one of the Wechsler intelligence scales (WISC-III 271 or other versions: WISC-R 272, WAIS 136), and in order to avoid retest effects, the WISC-III was not repeated in the projectxx. The test battery was large and time consuming and consequently, the tests were done over several sessions; ranging from a minimum of 2 to multiple sessions. Similarly to Study I, tests of episodic and semantic memory, facial affect recognition, and spatial working memory were also carried out, but are not included in the thesis. CANTAB: All 40 patients completed all CANTAB tests, except one patient who failed to complete one subtest (Rapid Visual Information Processing), and for whom results were extrapolated from the patient group mean. Paper-and-Pencil test battery: Similarly to Study I, the paper-and-pencil tests in Study II included Trail Making tests A & B; verbal semantic (letter S) and category (animals) fluency as well as Regard's figural fluency test; and WCST. All 40 patients completed all paper-and-pencil tests, except for 4 patients who did not complete the WCST. WISC-III: As the Danish version of the WISC-III 271 was in the process of being standardized by Dansk Psykologisk Forlag while Study II was carried out, the Danish Standardization version of the test was used. Normative data from the Swedish WISC-III version were used to calculate age-dependent Scaled Scores. A total of 35 patients completed a full Wechsler intelligence test: WISC-III (N= 30), WISC-R (N= 4), WAIS (N = 1). Twenty-seven (77 %) of these WISC tests were tested in the project by the same tester (BF), the rest were carried out in the psychiatric departments. Statistical Analyses: The statistical methods are described in Study I, section 3.2.2.
xx The inter-test correlation between the American versions of the WISC-III and WISC-R full scale IQ is high (r: 0.89) which is similar to the internal reliability score of the scales271. However, this correlation has not been examined with the Danish versions.
22

4.3. Results
4.3.1. Psychopathology The schizophrenic subgroup on average had a tendency towards higher Positive PANSS (p= 0.056) and Total PANSS (p= 0.053) scores than the NSP subgroup. On the SANS and SAPS global symptom dimensions, there were significantly more positive psychotic symptoms in the schizophrenic group than in the NSP group (p= 0.007). In both groups, the symptoms in the global negative dimension on average were mild to moderatexxi, and in the global disorganisation dimension questionable to mild. The symptoms in the global psychotic dimension were mild to moderate in the NSP group, while moderate to marked in the schizophrenic group. In the NSP group, males had significantly more Positive PANSS scores than females, but there were no gender differences on PANSS scores in the schizophrenic group. In terms of SANS and SAPS symptom dimensions, the boys in the NSP group had significantly (p= 0.0002) more disorganisation symptoms than girls, with no such difference in the schizophrenic group. In contrast, the girls in the schizophrenic group had significantly (p= 0.04) more psychotic symptoms than boys, a difference that was not present in the NSP group. The PANSS scores and SANS & SAPS symptom dimensions are listed in Table 4.2. Table 4.2. Diagnostic distribution and psychopathology ratings Study II
Diagnostic distribution Schizophrenia NSP
Total
N= 18 N= 22 N= 40 Age Mean= 15.2 (SD= 1.7) Mean= 15.2 (SD= 1.6) Mean= 15.2 (SD= 1.6)Gender 8 Male / 10 Female 8 Male / 14 Female 16 Male / 24 Female Diagnostic subtype* F 20.0: N= 13
F 20.1: N= 2 F 20.3: N= 2 F 20.9: N= 1
F 21: N=10 F 22: N=1 F 23.3: N=1 F 23.91: N=1 F 28: N= 8 F 32.3: N= 1
PANSS ratings Positive symptoms: Negative symptoms: General symptoms: Total symptoms:
Mean= 21.3 (SD= 4.7) Mean= 21.8 (SD= 6.7) Mean= 42.9 (SD= 7.5) Mean= 86.1 (SD= 14.6)
Mean= 18.2 (SD= 5.1) Mean= 18.2 (SD= 6.0) Mean= 40.0 (SD= 6.7) Mean=77.8 (SD= 11.5)
Mean= 19.6 (SD= 5.1)Mean= 20.4 (SD= 6.4)Mean= 41.3 (SD= 7.1)Mean=81.5 (SD= 13.4)
SANS & SAPS global Dimensions Negative dimension: Psychotic dimension: Disorganised dimension
Mean= 2.8 (SD= 0.8) Mean= 3.3 (SD= 1.2) Mean= 1.7 (SD= 1.2)
Mean= 2.5 (SD= 0.7) Mean= 2.3 (SD= 0.9) Mean= 1.3 (SD= 1.1)
Mean= 2.6 (SD= 0.8) Mean= 2.7 (SD= 1.2) Mean= 1.4 (SD= 1.2)
Medication status Unmedicated: Weeks medication:
N= 3 (16.7 %) Mean= 9.3 (SD= 5.5)
N= 10 (45.5 %) Mean= 7.0 (SD= 5.6)
N= 13 (32.5 %) Mean= 8.3 (SD= 5.6)
*ICD-10 diagnostic subtypes. F 20.0= Paranoid schizophrenia; F 20.1=Hebephrenic schizophrenia; F 20.3=Undifferentiated schizophrenia; F 20.9=Unspecified schizophrenia; F 21= Schizotypal disorder; F 22=Paranoid psychosis; F23.3=Acute paranoid psychosis; F 23.91=Actue Psychosis, unspecified; F 28=Other, non-organic psychosis; F32.3=Severe depressive episode with psychotic symptoms.
4.3.2. Cognitive deficits Overall, there were no significant differences between schizophrenic patients and patients with NSP on most cognitive measures, and the same significant deficits were present regardless of whether the groups were viewed combined or separately; therefore, for clarity combined results from both groups are presented. Separate results from EOS and NSP are presented for the few measures on which the groups differed. Intelligence: Compared to controls, the patients had significantly worse results on all subtests and summary scores of the WISC-III. Patients had a mean Full scale IQ (FIQ) of 89.4 (SD= 17.5; Range 46-126), which compared to the FIQ of 110.8 of controls (SD= 12.6; Range= 83-138) was a highly significant difference (p= 0.00000013). Similar impairments were found in Performance IQ (PIQ) and Verbal IQ (VIQ), in which the mean PIQ of patients of 91.6 (SD= 18; Range= 53-121) was
xxi SANS and SAPS global severity ratings are: 0=None; 1=Questionable; 2=Mild; 3=Moderate; 4=Marked; 5=Severe204;205.
significantly different (P= 0.000012) from that of the controls (PIQ= 109; SD= 13; range= 76-138), and the VIQ of patients (mean VIQ= 90; SD= 18.5; Range= 51-130) was significantly different (p= 0.0000013) from the VIQ of controls (mean VIQ= 110; SD= 12.9; Range= 81-134). There were no differences in level of impairment between the average PIQ and VIQ. However, the variability of scores within the WISC-III was much larger in the patient group than the control group (which is illustrated in Figure 4.1.) Figure 4.1. Verbal and Performance IQ variance in Study II.
Adolescent controls (N=40)150
140
130
120
110
100
90
80
70
60
50
40
Verbal IQ
Performance IQ
Early onset patients (N=35)150
140
130
120
110
100
90
80
70
60
50
40
Verbal IQ
Performance IQ
In the patient group, 15 of 35 subjects (42.9 %) had differences larger than 1 SD (15 IQ points) between VIQ and PIQ, 9 of whom with higher PIQ than VIQ (IQ points range= 19-48; mean difference= 27.11; SD= 9.1); and 6 with higher VIQ than PIQ (IQ points range= 15-35; mean difference= 23.5; SD= 9.16). In comparison, 9 of 40 healthy controls (22.5 %) had performance IQ-verbal IQ differences larger than 15 IQ points; only 3 of whom had higher PIQ than VIQ (IQ point range= 16-26; mean difference= 22.3; SD= 5.5), while 6 controls had higher VIQ than PIQ (IQ point range= 15-28; mean difference= 20.67; SD= 4.9). In addition to the verbal and performance IQ scores, results from the WISC III were calculated into 4 factor IQ scoresxxii= Verbal Comprehension, Perceptual Organisation, Attention, and Speed of processing271. The 4 factors were all highly significantly different between patients and controls, but without differential levels of deficits between factors. Figure 4.2. shows the z-scores of the WISC Full-scale-, Verbal- and Performance IQ as well as of the 4 factor scores of the patients and healthy controls based on normative data. Figure 4.2. WISC Z-scores based on normative data
-1,2
-1
-0,8
-0,6
-0,4
-0,2
0
0,2
0,4
0,6
0,8
1
FIQ VIQ PIQ Verbal Factor PerceptualFactor
AttentionFactor
Speed Factor
Z-sc
ores
(SD
)
EOS and NSP Controls
There were no significant gender differences on WISC verbal IQ, performance IQ, or full scale IQ scores in either patients or controls, but male patients had significantly better results on the Information subtest of the WISC, assessing general knowledge (p= 0.04) than female patients. There was a tendency for female patients to have better results than male patients on the digit span subtest of the WISC (p= 0.09).
xxii The 4 factor scores can only be calculated from full WISC-III results, and are based on 28 patients and 40 controls.
23
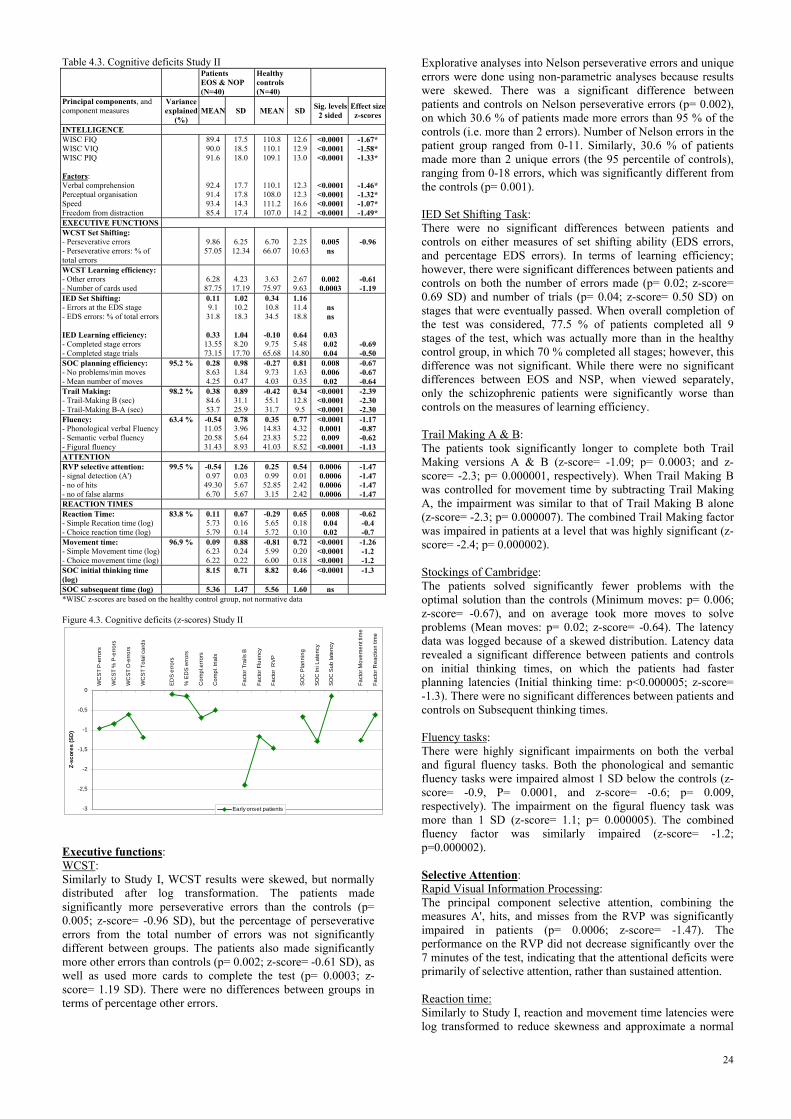
Table 4.3. Cognitive deficits Study II Patients
EOS & NOP (N=40)
Healthy controls (N=40)
Principal components, and component measures
Variance explained
(%) MEAN SD MEAN SD Sig. levels
2 sided Effect sizez-scores
INTELLIGENCE WISC FIQ WISC VIQ WISC PIQ Factors: Verbal comprehension Perceptual organisation Speed Freedom from distraction
89.4 90.0 91.6
92.4 91.4 93.4 85.4
17.5 18.5 18.0
17.7 17.8 14.3 17.4
110.8 110.1 109.1
110.1 108.0 111.2 107.0
12.6 12.9 13.0
12.3 12.3 16.6 14.2
<0.0001<0.0001<0.0001
<0.0001<0.0001<0.0001<0.0001
-1.67* -1.58* -1.33*
-1.46* -1.32* -1.07* -1.49*
EXECUTIVE FUNCTIONS WCST Set Shifting: - Perseverative errors - Perseverative errors: % of total errors
9.86 57.05
6.25 12.34
6.70 66.07
2.25 10.63
0.005
ns
-0.96
WCST Learning efficiency: - Other errors - Number of cards used
6.28 87.75
4.23 17.19
3.63 75.97
2.67 9.63
0.002 0.0003
-0.61 -1.19
IED Set Shifting: - Errors at the EDS stage - EDS errors: % of total errors IED Learning efficiency: - Completed stage errors - Completed stage trials
0.11 9.1 31.8
0.33 13.55 73.15
1.02 10.2 18.3
1.04 8.20 17.70
0.34 10.8 34.5
-0.10 9.75 65.68
1.16 11.4 18.8
0.64 5.48 14.80
ns ns
0.03 0.02 0.04
-0.69 -0.50
SOC planning efficiency: - No problems/min moves - Mean number of moves
95.2 % 0.28 8.63 4.25
0.98 1.84 0.47
-0.27 9.73 4.03
0.81 1.63 0.35
0.008 0.006 0.02
-0.67 -0.67 -0.64
Trail Making: - Trail-Making B (sec) - Trail-Making B-A (sec)
98.2 % 0.38 84.6 53.7
0.89 31.1 25.9
-0.42 55.1 31.7
0.34 12.8 9.5
<0.0001<0.0001<0.0001
-2.39 -2.30 -2.30
Fluency: - Phonological verbal Fluency - Semantic verbal fluency - Figural fluency
63.4 % -0.54 11.05 20.58 31.43
0.78 3.96 5.64 8.93
0.35 14.83 23.83 41.03
0.77 4.32 5.22 8.52
<0.00010.0001 0.009
<0.0001
-1.17 -0.87 -0.62 -1.13
ATTENTION RVP selective attention: - signal detection (A') - no of hits - no of false alarms
99.5 %
-0.54 0.97 49.30 6.70
1.26 0.03 5.67 5.67
0.25 0.99 52.85 3.15
0.54 0.01 2.42 2.42
0.0006 0.0006 0.0006 0.0006
-1.47 -1.47 -1.47 -1.47
REACTION TIMES Reaction Time: - Simple Recation time (log) - Choice reaction time (log)
83.8 % 0.11 5.73 5.79
0.67 0.16 0.14
-0.29 5.65 5.72
0.65 0.18 0.10
0.008 0.04 0.02
-0.62 -0.4 -0.7
Movement time: - Simple Movement time (log) - Choice movement time (log)
96.9 % 0.09 6.23 6.22
0.88 0.24 0.22
-0.81 5.99 6.00
0.72 0.20 0.18
<0.0001<0.0001<0.0001
-1.26 -1.2 -1.2
SOC initial thinking time (log)
8.15 0.71 8.82 0.46 <0.0001 -1.3
SOC subsequent time (log) 5.36 1.47 5.56 1.60 ns *WISC z-scores are based on the healthy control group, not normative data Figure 4.3. Cognitive deficits (z-scores) Study II
-3
-2,5
-2
-1,5
-1
-0,5
0
WC
ST P
-err
ors
WC
ST %
P-e
rror
s
WC
ST O
-erro
rs
WC
ST T
otal
car
ds
EDS
erro
rs
% E
DS
erro
rs
Com
pl.e
rrors
Com
pl. t
rials
Fact
or T
rails
B
Fact
or F
luen
cy
Fact
or R
VP
SOC
Pla
nnin
g
SOC
Ini L
aten
cy
SOC
Sub
late
ncy
Fact
or M
ovem
ent t
ime
Fact
or R
eact
ion
time
Z-sc
ores
(SD
)
Early onset patients
Executive functions: WCST: Similarly to Study I, WCST results were skewed, but normally distributed after log transformation. The patients made significantly more perseverative errors than the controls (p= 0.005; z-score= -0.96 SD), but the percentage of perseverative errors from the total number of errors was not significantly different between groups. The patients also made significantly more other errors than controls (p= 0.002; z-score= -0.61 SD), as well as used more cards to complete the test (p= 0.0003; z-score= 1.19 SD). There were no differences between groups in terms of percentage other errors.
Explorative analyses into Nelson perseverative errors and unique errors were done using non-parametric analyses because results were skewed. There was a significant difference between patients and controls on Nelson perseverative errors (p= 0.002), on which 30.6 % of patients made more errors than 95 % of the controls (i.e. more than 2 errors). Number of Nelson errors in the patient group ranged from 0-11. Similarly, 30.6 % of patients made more than 2 unique errors (the 95 percentile of controls), ranging from 0-18 errors, which was significantly different from the controls (p= 0.001). IED Set Shifting Task: There were no significant differences between patients and controls on either measures of set shifting ability (EDS errors, and percentage EDS errors). In terms of learning efficiency; however, there were significant differences between patients and controls on both the number of errors made (p= 0.02; z-score= 0.69 SD) and number of trials (p= 0.04; z-score= 0.50 SD) on stages that were eventually passed. When overall completion of the test was considered, 77.5 % of patients completed all 9 stages of the test, which was actually more than in the healthy control group, in which 70 % completed all stages; however, this difference was not significant. While there were no significant differences between EOS and NSP, when viewed separately, only the schizophrenic patients were significantly worse than controls on the measures of learning efficiency. Trail Making A & B: The patients took significantly longer to complete both Trail Making versions A & B (z-score= -1.09; p= 0.0003; and z-score= -2.3; p= 0.000001, respectively). When Trail Making B was controlled for movement time by subtracting Trail Making A, the impairment was similar to that of Trail Making B alone (z-score= -2.3; p= 0.000007). The combined Trail Making factor was impaired in patients at a level that was highly significant (z-score= -2.4; p= 0.000002). Stockings of Cambridge: The patients solved significantly fewer problems with the optimal solution than the controls (Minimum moves: p= 0.006; z-score= -0.67), and on average took more moves to solve problems (Mean moves: p= 0.02; z-score= -0.64). The latency data was logged because of a skewed distribution. Latency data revealed a significant difference between patients and controls on initial thinking times, on which the patients had faster planning latencies (Initial thinking time: p<0.000005; z-score= -1.3). There were no significant differences between patients and controls on Subsequent thinking times. Fluency tasks: There were highly significant impairments on both the verbal and figural fluency tasks. Both the phonological and semantic fluency tasks were impaired almost 1 SD below the controls (z-score= -0.9, P= 0.0001, and z-score= -0.6; p= 0.009, respectively). The impairment on the figural fluency task was more than 1 SD (z-score= 1.1; p= 0.000005). The combined fluency factor was similarly impaired (z-score= -1.2; p=0.000002). Selective Attention: Rapid Visual Information Processing: The principal component selective attention, combining the measures A', hits, and misses from the RVP was significantly impaired in patients (p= 0.0006; z-score= -1.47). The performance on the RVP did not decrease significantly over the 7 minutes of the test, indicating that the attentional deficits were primarily of selective attention, rather than sustained attention. Reaction time: Similarly to Study I, reaction and movement time latencies were log transformed to reduce skewness and approximate a normal
24

distribution. The patients had significantly longer reaction latencies than controls, both in the simple RT task (p= 0.04; z-score= -0.4) and in the 5-Choice RT task (p= 0.02; z-score= -0.7). Highly significant differences between patients and controls were seen on both the simple motor times (p< 0.000005; z-score= -1.2) and 5-Choice motor latencies (p<0.000004; z-score= -1.2). Principal components of movement time (combining simple and choice reaction time conditions) and reaction time (combining simple and choice movement time conditions) were both significantly impaired (p= 0.000003; z-score= 1.26; and p= 0.008; z-score= 0.62), respectively. 4.4. Discussion
4.4.1. Early onset schizophrenia vs non-schizophrenic psychosis The literature comparing schizophrenic with other diagnoses of non-organic psychosis is not very extensive and the findings are inconsistent. Compared to other psychotic disorders, early onset schizophrenia has a worse prognosis in terms of a more chronic course of illness with more severe symptomatic profile and worse social outcome 252. Some studies stress the similarities between e.g. schizoaffective disorder and schizophrenia in terms of genetic, epidemiological, and clinical characteristics 273-275. In terms of cognitive deficits in schizophrenic compared to non-schizophrenic psychotic patients, the data is inconclusive. Some studies support the presence of more extensive and prevalent cognitive deficits in schizophrenia compared to other schizophrenia spectrum disorders 153;276;277, while others do not. Addington et al. found no evidence for different cognitive deficits in first episode psychosis compared to first episode schizophrenia 155. In our study, the group diagnosed with non-organic, non-schizophrenic psychosis (NSP) encompassed a variety of diagnoses, most of which are considered part of the schizophrenia spectrum, but also including one patient with affective disorder (ICD 10: F. 32.3 Depressive with single episode psychosis, severe). Whether this patient should be included in the sample is debatable, based on theoretical considerations of the diagnostically predictive validity of distinguishing between schizophrenic and affective psychoses in early onset patients 270. However, based on the lower diagnostic stability of schizophrenia and other psychotic disorders in children and adolescents, we aimed at including as many "potential" schizophrenic patients as possible (this being the baseline investigation of a 5 year longitudinal follow-up study). Several of the patients with early onset non-schizophrenic psychosis are expected to receive a diagnosis of schizophrenia later in the disease process, although the exact estimates vary considerably 251.
4.4.2. Demographics Even though a full match between patients and controls on SES was attempted, it was not possible to achieve a match on SES, and therefore there are differences between patient groups and controls in terms of demographics. The patients had a significantly lower SES than controls, which may be a possible confounding factor when interpreting cognitive, and especially IQ results. However, the IQ levels of both the patient group and the control group are very similar to those in previous studies 137. Parental education/occupation was a better predictor of IQ for both the patients and controls than parental income (or combined SES), though a linear relation between education/occupation and IQ only accounted for approximately 19 % of the variance in IQ (Pearson's r= .44 in both groups). While parental income and total SES were significantly correlated with FIQ in the control
group (Pearson's r= .39, and r= .32, respectively), no significant correlations were seen in the patient group. This is similar to what has previously been found. Bilder et al. 1 have shown that intelligence in schizophrenic patients is rather independent of demographic factors, and predicting IQ from demographics such as age, gender and parental education only accounts for approximately 20 % of the variance in IQ scores. In addition, a swedish cohort study examining data from approximately 100 000 male conscripts found that low IQ was predictive of an early onset of psychotic disorder, a finding which was not confounded by socioeconomic factors such as parental education 278.
4.4.3. Cognitive deficits Intelligence: The low IQ in the patient group raises the question of test validity in this population during psychotic episodes. Known mental retardation (IQ<70) was an exclusion criteria for both patients and controls. Nonetheless, of 35 patients, 5 (14.3 %) received an IQ less than 70 (in ranges that in functional terms lies within the area of mild retardation). A superficial intuitively attractive interpretation is that the IQ results are state-, rather than trait-related deficits that are brought about by the presence of clinical symptoms (psychotic, negative, disorganised or anxiety symptoms), and as such are transient rather than stable impairments. Another interpretation is that the low IQ scores are stable, representing either the level of IQ function before illness onset or a decline from premorbid levels. While none of the patients had been assessed as mildly retarded prior to illness onset, some of the patients with IQ scores lower than 70, were described as having various learning problems, hyperactivity, and social problems at school. However, these issues were not characterised more explicitly. However, the level of IQ deficits in this sample is precisely similar to the findings from previous studies with a patient average approximately 1 SD below the normative average IQ 103;131;256;263, and a range spanning from moderate retardation to giftedness 103;256. The stability of cognitive tests in previous studies of similar patient samples has been found to be remarkable, regardless of clinical state 1;78. Bedwell et al. recently found that an age-related decline in scaled IQ scores in patients with early onset schizophrenia was indicative of stable raw scores and a lack of age-related improvements, reflected as a decline in age-scaled scores 141. This suggests a developmental stagnation in, rather than loss of, previously acquired functions.The average FIQ of 110.8 of the healthy control group, which is approximately ⅔ SD above the normative average, is also similar to the level found in previous studies 266, which is probably indicative of a selection bias that practically is difficult to avoid in research projects. Profile of IQ deficits: While patients have varying profiles of impairment on the WISC-III tests – some with high performance IQ and low verbal IQ, others with mostly normal results and a few severely impaired functions – the group average shows little differential deficits in intellectual impairment. However, the variability of scores within the WISC-III is much larger in the patient group than the control group. The significance of the differential IQ scores is that differences larger than 1 SD (15 IQ points) are considered clinically relevant and theoretically indicative of a discrepancy in intelligence profile that (regardless of level of IQ) is larger than expected and could be indicative of lateralised or diffuse cerebral dysfunction. While large discrepancies with higher Performance IQ could indicate lateralised left-hemisphere dysfunction, large discrepancies with higher Verbal IQ are considered indicative of either lateralised right-hemisphere dysfunction, or diffuse global cerebral dysfunction 279. Previous studies by Asarnow's group at UCLA have found particularly prevalent deficits in the attentional factor "freedom from
25

distraction" calculated from the WISC-Rxxiii, with a relative sparing of measures of perceptual organisation 131;262. This pattern of deficits was not supported by our findings, in which significant deficits were found in all measures of the WISC-R or WISC-III, without any indications of either selectively impaired or spared areas of function. Executive deficits: WCST: The patients made significantly more perseverative errors than the controls; however, the perseverative errors were not disproportionately prevalent compared to the total number of errors, which was reflected in the lack of difference between the groups on the measure of percentage perseverative errors. Similarly, the patients made more other errors than controls, but not in a pattern that was disproportionate to the overall number of errors made. This indicates that attentional set shifting may not be specifically impaired in early onset patients, and if they are, they are not easily distinguished from a generalised pattern of errors. The performance of healthy children reaches the level of adults on the WCST already at 10-11 years of age 129, in spite of the continued improvement of performance on other tests of attentional set shifting until early adulthood 129. This could be due to the multi-componential nature of the WCST, on which the primary demands may not be on shifting of hypotheses, but other functions such as concept formation. IED Set Shifting Task: The patients were not significantly impaired on the IED set shifting task, when attentional set shifting ability was considered. There were no significant differences between patients and controls in terms of how many patients completed the test, and patients did not make more errors at the ED shift stage. However, in terms of learning efficiency, patients made significantly more errors and took more trials to complete the test, which suggests that learning took longer and was more inefficient for patients than the control group. The increased trials and errors at the different stages suggest that the learning deficits involve both problems with concept formation and executive strategy monitoring, but also an inability to generalise what has already been learnt to new, even similar situations. This is similar to what Hemsley has termed the "primary cognitive deficit" in schizophrenia; i.e. an inability to use information that was previously learnt to guide current perception and behaviour 280. Support for deficits in generalising learnt information comes from studies in which patients are taught how to solve the WCST. The performance of patients improves when they are guided through the test on a card-to-card basis. But when instructions cease and patients have to use the previously learnt information to guide behaviour, they return to performing poorly on the test 281. Trail Making: The patients were significantly slower than controls on both versions A and B of the Trail Making test. However, the level of impairment on the Trail Making B (and the subtracted measure B-A, controlling for psychomotor speed) was more than 2 SD below the average of the controls group, and more than 1 SD below the impairment on Trail Making A. Trail Making B was the measure on which the adolescent patients were most impaired of all cognitive tasks. Trail Making B requires attentional set shifting, but is also very dependent on the speed at which attention can be shifted. Stockings of Cambridge: Patients were not as efficient in problem solving on the Stockings of Cambridge as controls, which was evident both in terms of solving fewer problems with the optimal solution (i.e. xxiii The WISC-R consists of 3 factors: freedom from distraction; verbal comprehension, and perceptual organisation that are very similar, but not identical, to the 4 factors from WISC-III.
with the minimum number of moves required), and using more moves on average to reach solutions. The latency data revealed an interesting distinction between initial thinking times and subsequent thinking times involved during problem solving. The initial thinking time is an indication of time spent planning ahead, before a solution is attempted. The patients had significantly shorter initial thinking latencies than controls, which shows that they did not plan ahead (as is prompted in the instructions to the test) but were uninhibited in their approach to solving the problems. However, the patients did not differ from controls in terms of subsequent thinking time, which is the time from the problem is presented on the screen until it is solved. The lack of increased subsequent thinking latencies indicate that the patients do not try to compensate from the lack of planning ahead by taking more time to solve problems, which in turn results in less efficient problem solving reflected in the more moves required. This suggests a profile of executive deficits, in which early onset patients are impulsive and uninhibited and have deficits in planning and monitoring problem solving strategies. This is similar to the profile of short initial planning latencies and inefficient problem solving found in patients with frontal lobe damage 121;237;282. This profile of reduced initial thinking times, without prolonged subsequent thinking times is the same as that found in a recent study from Maudsley's Early Onset Schizophrenia Study, using a similar computerised Tower of London task 266. Fluency: Patients were similarly impaired on all tasks of verbal or figural fluency, approximately 1 SD below the level of the controls. The similar level of impairment of the verbal and figural fluency tasks indicates that these deficits are not specific to either verbal or nonverbal material but dependent on problems in generating and carrying out a relevant problem solving strategy, i.e. executive spontaneous flexibility. Selective Attention: Rapid Visual Information Processing: The adolescent patients had significant impairments on hits, misses, and signal detection (A'), which indicates deficits in selective attention. Similarly to the adult patients, the adolescent patients did not show evidence of sustained attentional deficits, as deficits did not deteriorate over the 7 minutes of the test. Reaction and movement times: The patients had significantly longer latencies than controls on both simple and choice motor and reaction time tasks. This is in accordance with previous studies that have found reaction time deficits in early onset patients 177;283;284. Similarly to the adult sample, there were no differences in the level of impairment on the choice respectively simple reaction and motor time conditions. 4.5. Conclusions Hypotheses: All 3 hypotheses of Study II were supported. Hypothesis 1: The patients did have significantly lower IQ than controls, at a level of impairment that was similar to that found in previous studies. Hypothesis 2: The patients were significantly impaired in all cognitive domains of attention, executive functions and reaction time. Hypothesis 3: There were no significant differences between EOS and NSP in terms of profile and level of cognitive deficits. The results show a profile of executive deficits in early onset patients in spontaneous flexibility rather than reactive flexibility, characterised by a disinhibitive and impulsive approach to problem solving. While movement and reaction times are
26

reduced, the early onset patients do not show a generalised slowing of information processing.
Chapter 5. The impact of age of onset of schizophrenia and psychosis on cognitive deficits 5.1. Study Objectives and Hypotheses Objectives: The primary objective of combining results from Study I and Study II was to examine whether adolescent onset schizophrenia is continuous with adult onset schizophrenia in terms of clinical symptoms and cognitive deficits. The secondary objective was to examine whether there are differences between the adolescent and adult onset patients with more severe deficits in the former, which would indirectly support the neurodevelopmental hypothesis. Hypotheses: 1. There is a similar pattern and level of severity of clinical symptoms in adolescent and adult patients supporting clinical continuity, except for the presence of more marked negative symptoms in the adolescent sample. 2. The profile of cognitive deficits is similar in the adult and adolescent samples, supporting cognitive continuity between adolescent and adult onset schizophrenia. 3. The severity of deficits is worse in the adolescent patients compared to the adult patients, supporting the neurodevelopmental hypothesis. 5.2. Methods In order to enable a direct comparison of the results from Study I and II with the purpose of examining the effects of age of onset on cognitive deficits, the same tests were used in Study I and II (with the exception of intelligence tests). The tests were carried out by the same tester (BF) in both studies, eliminating potential systematic inter-tester differences between the studies. To summarise, the total combined patient sample from Study I and Study II is 65 patients; 43 of whom have a schizophrenia diagnosis, and the remaining 22 a diagnosis of NSP. For the purpose of clarity, the adolescent schizophrenic and NSP patients are combined, except when results differ between the groups. Results from patients in Study I and Study II are presented as z-scores based on their respective control groups. 5.3. Results & discussion
5.3.0. Demographics Table 5.1. shows a summary of the demographic and clinical data from subjects in Study I and Study II combined. The gender distribution in the entire adolescent sample including both patients with schizophrenia and NSP was significantly different from that of the schizophrenic adult group (p= 0.039), with significantly more females than males in the adolescent group. However, when the adolescent group was divided into diagnostic subgroups with schizophrenia and other psychoses, the gender distribution was no longer significantly different in the early onset schizophrenia vs. adult onset schizophrenia groups; but still significantly different between the early onset NSP patients compared to the adult onset schizophrenia group. The similar prevalence of males and females in the adolescent and adult schizophrenic groups is in accordance with previous findings 258;285.
Table 5.1. Gender distribution in Study I and Study II: differences according to diagnostic group.
N Gender Study I Study IIA Df Fisher's Exact Test (2-tailed)
Male 17 16 1 0.041 Female 8 24 Total 25 40
N Gender Study I Study IIB Df Fisher's Exact Test (2-tailed)
Male 17 8 1 0.21 Female 8 10 Total 25 18
N Gender Study I Study IIC Df Fisher's Exact Test (2-tailed)
Male 17 8 1 0.042 Female 8 14 Total 25 22 A: All patients with schizophrenia and other psychosis (N=40) B: Only patients with schizophrenia (N=18) C: Only patients with other psychosis (N=22)
5.3.1. Psychopathology In terms of psychopathology, the adolescent sample had significantly higher general and total PANSS scores than the adult sample. These differences were significant regardless of whether the comparison included the entire adolescent group (General PANSS p< 0.000; Total PANSS p=0.001), the schizophrenic group (General PANSS p< 0.000; Total PANSS p<0.000), or the NSP group (General PANSS p<0.000; Total PANSS p<0.035). There were no significant differences between the adult and adolescent patients on positive and negative symptoms on the PANSS scale. The SANS and SAPS scores were similar in both the adolescent and adult patient samples, with symptoms in the negative dimension mild to moderate; psychotic dimension mild to moderate; and the disorganised dimension questionable to mild. When only the schizophrenic adolescents are included in the analysis, significantly more severe negative symptoms (p= 0.03) and a tendency towards more severe disorganised symptoms (p= 0.051) are present in the adolescent patients compared to the adult schizophrenic patients. This is in accordance with what has previously been found 244;286.
5.3.2. Cognitive deficits Because separate results from Study I and Study II have been presented, only measures that differ between the groups or are otherwise relevant are described here. Intelligence: While the adolescent sample was tested with the whole WISC-III test battery, the adult patients did not complete a full WAIS IQ test. A full version of WAIS was not included primarily because of the time constraints involved in testing drug-naïve patients, but also in lieu of a Danish version of the WAIS-III 287. The adults instead completed the DART (Danish version of the NART), which provides a valid and reliable indication of premorbid verbal intelligence and is correlated with full scale IQ 135. However, a direct comparison between adult and adolescent patients on intelligence was not possible. In terms of comparisons of the severity of IQ deficits, the adolescent schizophrenic patients were approximately 1 SD below normative data. Compared to their matched control group, the impairment was 1.67 SD. The adult patients were 0.68 SD below their matched control group on DART. This is similar to the level of IQ in adolescent and adult onset patients found in previous studies. The expected profile of more severe cognitive deficits in the adolescent group compared to the adult group was not supported by our results. As is shown in Figure 5.1., the level of cognitive deficits in the adolescent and adult samples is strikingly similar.
27
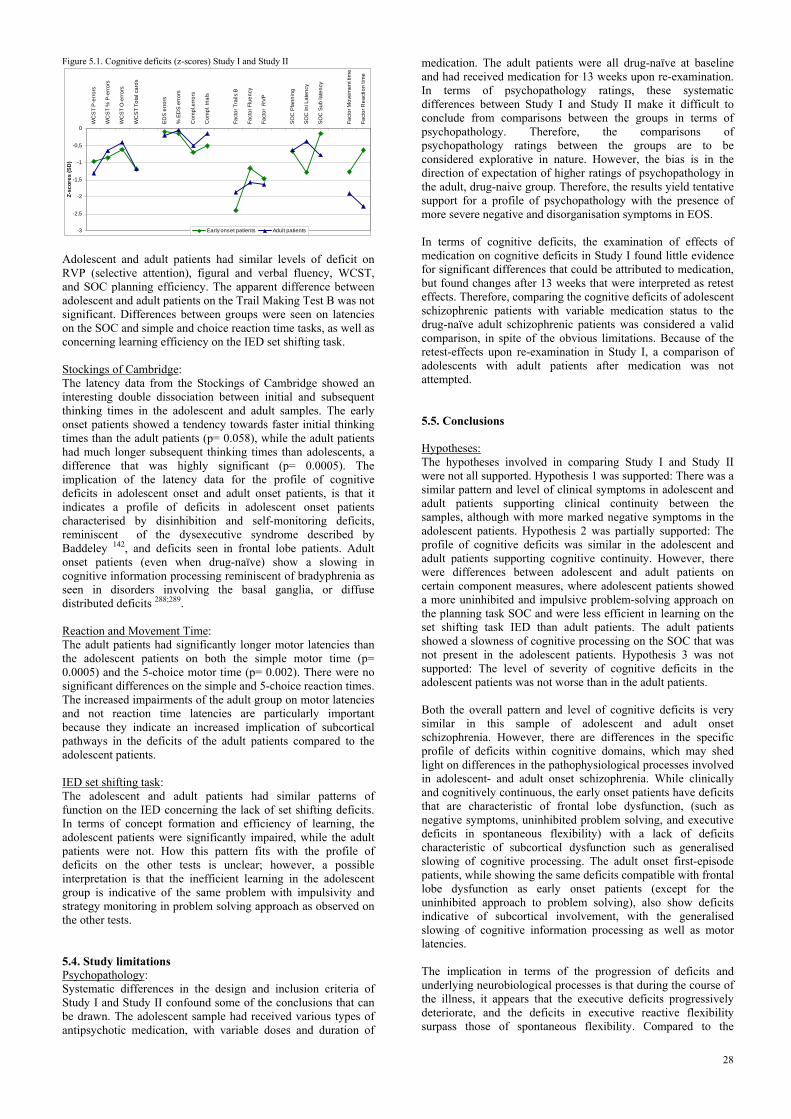
Figure 5.1. Cognitive deficits (z-scores) Study I and Study II
-3
-2,5
-2
-1,5
-1
-0,5
0
WC
ST
P-er
rors
WC
ST
% P
-erro
rs
WC
ST
O-e
rrors
WC
ST
Tota
l car
ds
ED
S e
rrors
% E
DS
erro
rs
Com
pl.e
rror
s
Com
pl. t
rials
Fact
or T
rails
B
Fact
or F
luen
cy
Fact
or R
VP
SO
C P
lann
ing
SO
C In
i Lat
ency
SO
C S
ub la
tenc
y
Fact
or M
ovem
ent t
ime
Fact
or R
eact
ion
time
Z-sc
ores
(SD
)
Early onset patients Adult patients Adolescent and adult patients had similar levels of deficit on RVP (selective attention), figural and verbal fluency, WCST, and SOC planning efficiency. The apparent difference between adolescent and adult patients on the Trail Making Test B was not significant. Differences between groups were seen on latencies on the SOC and simple and choice reaction time tasks, as well as concerning learning efficiency on the IED set shifting task. Stockings of Cambridge: The latency data from the Stockings of Cambridge showed an interesting double dissociation between initial and subsequent thinking times in the adolescent and adult samples. The early onset patients showed a tendency towards faster initial thinking times than the adult patients (p= 0.058), while the adult patients had much longer subsequent thinking times than adolescents, a difference that was highly significant (p= 0.0005). The implication of the latency data for the profile of cognitive deficits in adolescent onset and adult onset patients, is that it indicates a profile of deficits in adolescent onset patients characterised by disinhibition and self-monitoring deficits, reminiscent of the dysexecutive syndrome described by Baddeley 142, and deficits seen in frontal lobe patients. Adult onset patients (even when drug-naïve) show a slowing in cognitive information processing reminiscent of bradyphrenia as seen in disorders involving the basal ganglia, or diffuse distributed deficits 288;289. Reaction and Movement Time: The adult patients had significantly longer motor latencies than the adolescent patients on both the simple motor time (p= 0.0005) and the 5-choice motor time (p= 0.002). There were no significant differences on the simple and 5-choice reaction times. The increased impairments of the adult group on motor latencies and not reaction time latencies are particularly important because they indicate an increased implication of subcortical pathways in the deficits of the adult patients compared to the adolescent patients. IED set shifting task: The adolescent and adult patients had similar patterns of function on the IED concerning the lack of set shifting deficits. In terms of concept formation and efficiency of learning, the adolescent patients were significantly impaired, while the adult patients were not. How this pattern fits with the profile of deficits on the other tests is unclear; however, a possible interpretation is that the inefficient learning in the adolescent group is indicative of the same problem with impulsivity and strategy monitoring in problem solving approach as observed on the other tests. 5.4. Study limitations Psychopathology: Systematic differences in the design and inclusion criteria of Study I and Study II confound some of the conclusions that can be drawn. The adolescent sample had received various types of antipsychotic medication, with variable doses and duration of
medication. The adult patients were all drug-naïve at baseline and had received medication for 13 weeks upon re-examination. In terms of psychopathology ratings, these systematic differences between Study I and Study II make it difficult to conclude from comparisons between the groups in terms of psychopathology. Therefore, the comparisons of psychopathology ratings between the groups are to be considered explorative in nature. However, the bias is in the direction of expectation of higher ratings of psychopathology in the adult, drug-naive group. Therefore, the results yield tentative support for a profile of psychopathology with the presence of more severe negative and disorganisation symptoms in EOS. In terms of cognitive deficits, the examination of effects of medication on cognitive deficits in Study I found little evidence for significant differences that could be attributed to medication, but found changes after 13 weeks that were interpreted as retest effects. Therefore, comparing the cognitive deficits of adolescent schizophrenic patients with variable medication status to the drug-naïve adult schizophrenic patients was considered a valid comparison, in spite of the obvious limitations. Because of the retest-effects upon re-examination in Study I, a comparison of adolescents with adult patients after medication was not attempted. 5.5. Conclusions Hypotheses: The hypotheses involved in comparing Study I and Study II were not all supported. Hypothesis 1 was supported: There was a similar pattern and level of clinical symptoms in adolescent and adult patients supporting clinical continuity between the samples, although with more marked negative symptoms in the adolescent patients. Hypothesis 2 was partially supported: The profile of cognitive deficits was similar in the adolescent and adult patients supporting cognitive continuity. However, there were differences between adolescent and adult patients on certain component measures, where adolescent patients showed a more uninhibited and impulsive problem-solving approach on the planning task SOC and were less efficient in learning on the set shifting task IED than adult patients. The adult patients showed a slowness of cognitive processing on the SOC that was not present in the adolescent patients. Hypothesis 3 was not supported: The level of severity of cognitive deficits in the adolescent patients was not worse than in the adult patients. Both the overall pattern and level of cognitive deficits is very similar in this sample of adolescent and adult onset schizophrenia. However, there are differences in the specific profile of deficits within cognitive domains, which may shed light on differences in the pathophysiological processes involved in adolescent- and adult onset schizophrenia. While clinically and cognitively continuous, the early onset patients have deficits that are characteristic of frontal lobe dysfunction, (such as negative symptoms, uninhibited problem solving, and executive deficits in spontaneous flexibility) with a lack of deficits characteristic of subcortical dysfunction such as generalised slowing of cognitive processing. The adult onset first-episode patients, while showing the same deficits compatible with frontal lobe dysfunction as early onset patients (except for the uninhibited approach to problem solving), also show deficits indicative of subcortical involvement, with the generalised slowing of cognitive information processing as well as motor latencies. The implication in terms of the progression of deficits and underlying neurobiological processes is that during the course of the illness, it appears that the executive deficits progressively deteriorate, and the deficits in executive reactive flexibility surpass those of spontaneous flexibility. Compared to the
28

literature involving chronic patients, both the first episode adolescent and adult patients are less impaired on executive reactive flexibility than spontaneous flexibility, supporting the progression of deficits from functions primarily involving prefrontal areas to deficits implicating the pathways of frontal and sub-cortical areas. Aside from the different specific profiles described above, the early onset patients have a similar pattern and level of impairment compared to the adult onset patients. However, both are groups in which the illness onset is recent. The progression of deficits may be different as patients enter chronic phases of the illness, where the adolescent onset patients perhaps represent a sub-group of patients with a more aggressive, progressively deteriorating level of cognitive functions than the adult onset patients. The conclusions that can be drawn from this study tentatively yield indirect support for a neurodevelopmental disorder with a progressively deteriorating aspect, but further studies are needed to characterise and delineate the mechanisms involved.
Chapter 6: Conclusions and future directions: Age of onset and progression of cognitive deficits: The profiles of deficits in the adolescent and adult onset patients could be interpreted as indicative of a disease process that primarily affects cognitive functions of the prefrontal cortex and subsequently the distributed networks emanating from PFC, leading to deficits involving subcortical areas and fronto-striatal pathways. The early illness onset in adolescence could be caused by increased vulnerability requiring less environmental stress and less deficiencies in brain function before the threshold to illness onset is reached. In other words, the relatively circumscribed deficits of putative frontal lobe function may be enough to entail illness onset in adolescence if sufficient vulnerability indicators are present. The same cognitive deficits may merely present as prodromal deficits in patients without the presence of increased vulnerability, for whom the threshold to illness onset is reached only when the disease process has progressed, and the lack of functional integrity of distributed systems in the brain contribute to the clinical onset of illness in adulthood. According to the theories involving developmentally reduced synaptic connectivity, children and adolescents with early onset schizophrenia reach the threshold for illness onset earlier both because of increased vulnerability and an abnormally aggressive synaptic pruning process. However, as the maturational processes of the brain continue in adolescence after illness onset, the prediction from this model is that early onset patients will show further deterioration of clinical and cognitive functions, until the maturational processes are completed. This may explain why the early onset patients do not have more severe cognitive deficits than adult onset patients, when examined recently after onset, and may also predict that the cognitive deficits will progress after illness onset, at least until the maturational processes are largely complete. The early onset patients may represent a subgroup of patients with progressively deteriorating functions throughout the course of the illness. Methodological issues: When examining cognitive functions in schizophrenia research or clinical practice, the methodology of cognitive tests used is an important issue. Refined measures of cognitive function are needed for the characterisation of cognitive deficits and examination of hypotheses such as stability or deterioration of cognitive deficits. The present results further stress the importance of assessing cognitive function in schizophrenic patients at different stages of the disease process with test methods that have good construct validity and allow detailed
analyses of the components involved in cognitive dysfunction in schizophrenia. These methodological concerns should be prioritised when test batteries are selected for use in schizophrenia research and clinical practice, because they have direct impact on the conclusions that can be drawn from the tests. Effects of antipsychotic medication: The development of treatments that effectively target cognitive deficits is of pivotal importance for the prognosis of patients. However, the characterisation of profiles of efficacy of different antipsychotic compounds on cognitive deficits has not yet been sufficiently substantiated, as the literature is confounded by several methodological problems. The present results underscore the importance of addressing methodological issues such as comparable compound dosages, the influence of improvements in clinical state, side-effects and adjunctive medication as well as retest effects when assessing effects of medication on cognitive deficits in a longitudinal design. While there is reason to be optimistic, whether second- or third generation antipsychotics are the most promising possibility of effective treatment of cognitive deficits is debatable. There are other promising avenues of novel pharmacological treatment possibilities that target receptor systems other than dopamine and serotonin (e.g. the glutamatergic and cholinergic systems). A combination of different types of pharmacological compounds with non-pharmacological treatment (such as cognitive training) based on the cognitive profiles of individual patients may be a potentially advantageous treatment approach to ameliorate their cognitive deficits. The long term goal should be to target cognitive deficits on equal footing with clinical symptoms, which emphasizes the importance of characterising the profile of cognitive deficits in schizophrenic patients at different stages of the disease, in order to optimise the treatment strategies implemented.
29

References 1. Bilder RM, Goldman RS, Robinson D, Reiter G, Bell L, Bates
JA, Pappadopulos E, Willson DF, Alvir JM, Woerner MG, Geisler S, Kane JM, Lieberman JA. Neuropsychology of first-episode schizophrenia: initial characterization and clinical correlates. Am J Psychiatry. 2000;157:549-59.
2. Green MF, Nuechterlein KH. Should schizophrenia be treated as a neurocognitive disorder? Schizophr Bull. 1999;25:309-319.
3. Green MF, Braff DL. Translating the basic and clinical cognitive neuroscience of schizophrenia to drug development and clinical trials of antipsychotic medications. Biol Psychiatry. 2001;49:374-384.
4. Kraepelin E. Dementia Praecox and Paraphrenia. Huntington, New York.: Robert E. Krieger Publishing Co. Inc.; 1971.
5. Bleuler E. Dementia Praecox of the Group of Schizophrenias. New York: International Universities Press; 1950.
6. Kremen WR, Seidman LJ, Faraone SV, Toomey R, Tsuang MT. The question of neuropsychologically normal schizophrenia. Schizophr Res. 1999;36:140-141.
7. Green MF. Schizophrenia Revealed. From Neurons to Social Interactions. 1 ed. New York: Norton; 2001.
8. Meltzer HY, Park S, Kessler R. Cognition, schizophrenia, and the atypical antipsychotic drugs. Proc Natl Acad Sci U S A. 1999;96:13591-13593.
9. Goldberg TE, Torrey EF, Gold JM, Bigelow LB, Ragland RD, Taylor E, Weinberger DR. Genetic risk of neuropsychological impairment in schizophrenia: a study of monozygotic twins discordant and concordant for the disorder. Schizophr Res. 1995;17:77-84.
10. Kremen WS, Seidman LJ, Faraone SV, Toomey R, Tsuang MT. The paradox of normal neuropsychological function in schizophrenia. J Abnorm Psychol. 2000;109:743-752.
11. Allen DN, Goldstein G, Warnick E. A consideration of neuropsychologically normal schizophrenia. J Int Neuropsychol Soc. 2003;9:56-63.
12. Holthausen EAE, Wiersma D, Sitskoorn MM, Hijman R, Dingemans PM, Schene AH, van den Bosch RJ. Schizophrenic patients without neuropsychological deficits: subgroup, disease severity or cognitive compensation? Psychiatry Research. 2002;112:1-11.
13. Palmer BW, Heaton RK, Paulsen JS, Kuck J , Braff D, Harris MJ, Zisook S, Jeste DV. Is it possible to be schizophrenic yet neuropsychologically normal? Neuropsychology. 1997;11:437-446.
14. Cannon TD, Bearden CE, Hollister JM, Rosso IM, Sanchez LE, Hadley T. Childhood cognitive functioning in schizophrenia patients and their unaffected siblings: a prospective cohort study. Schizophr Bull. 2000;26:379-393.
15. David AS, Malmberg A, Brandt L, Allebeck P, Lewis G. IQ and risk for schizophrenia: a population-based cohort study. Psychol Med. 1997;27:1311-1323.
16. Green MF, Nuechterlein KH. Backward masking performance as an indicator of vulnerability to schizophrenia. Acta Psychiatr Scand Suppl. 1999;395:34-40.
17. Braff DL. Information processing and attention dysfunctions in schizophrenia. Schizophr Bull. 1993;19:233-259.
18. Frith CD. The cognitive neuropsychology of schizophrenia. Hove: Erlbaum.; 1992.
19. Goldman-Rakic PS. Working memory dysfunction in schizophrenia. J Neuropsychiatry Clin Neurosci. 1994;6:348-357.
20. McKenna PJ, Mortimer AM, Hodges JR. Semantic memory and schizophrenia. In: David AS, Cutting JC, eds. The neuropsychology of schizophrenia. Hove: Lawrence Erlbaum Associates; 1994:163-178.
21. Grawe RW, Levander S. Neuropsychological impairments in patients with schizophrenia: stability and prediction of outcome. Acta Psychiatr Scand Suppl. 2001;60-64.
22. Green MF. What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry. 1996;153:321-330.
23. Moritz S, Krausz M, Gottwalz E, Lambert M, Perro C, Ganzer S, Naber D. Cognitive dysfunction at baseline predicts symptomatic 1-year outcome in first-episode schizophrenics. Psychopathology. 2000;33:48-51.
24. Munro JC, Russell AJ, Murray RM, Kerwin RW, Jones PB. IQ in childhood psychiatric attendees predicts outcome of later schizophrenia at 21 year follow-up. Acta Psychiatr Scand. 2002;106:139-142.
25. Velligan DI, Miller AL. Cognitive dysfunction in schizophrenia and its importance to outcome: the place of atypical antipsychotics in treatment. J Clin Psychiatry. 1999;60 Suppl 23:25-8.
26. Weiss EM, Bilder RM, Fleischhacker WW. The effects of second-generation antipsychotics on cognitive functioning and psychosocial outcome in schizophrenia. Psychopharmacology (Berl). 2002;162:11-7.
27. Carlsson A. The current status of the dopamine hypothesis of schizophrenia. Neuropsychopharmacology. 1988;1:179-186.
28. Weinberger DR, Berman KF. Prefrontal function in schizophrenia: confounds and controversies. Philos Trans R Soc Lond B Biol Sci. 1996;351:1495-1503.
29. Saint-Cyr JA, Bronstein YL, Cummings JL. Neurobehavioral Consequences of neurosurgical Treatments and Focal Lesions of Frontal-Subcortical Circuits. In: Stuss DT, Knight RT, eds. Principles of Frontal Lobe Function. Oxford: Oxford University Press; 2002:408-427.
30. Fuster JM. Executive frontal functions. Exp Brain Res. 2000;133:66-70.
31. Owen AM. Tuning in to the temporal dynamics of brain activation using functional magnetic resonance imaging (fMRI). Trends in Cognitive Sciences . 1997;1:123-125.
32. Courtney SM, Ungeleider LG, Haxby JV. Response from Courtney, Ungeleider and Haxby. Trends in Cognitive Sciences. 1997;1:125-126.
33. Cohen JD, Smith EE. Response from Cohen and Smith. Trends in Cognitive Sciences. 1997;1:126-127.
34. Duncan J, Owen AM. Common regions of the human frontal lobe recruited by diverse cognitive demands. Trends Neurosci. 2000;23:475-483.
35. Divac I. Neostriatum and functions of prefrontal cortex. Acta Neurobiol Exp (Warsz ). 1972;32:461-477.
36. Eslinger PJ, Grattan LM. Frontal lobe and frontal-striatal substrates for different forms of human cognitive flexibility. Neuropsychologia. 1993;31:17-28.
37. Rund BR. A review of longitudinal studies of cognitive functions in schizophrenia patients. Schizophr Bull. 1998;24:425-435.
38. Gur RC, Ragland JD, Moberg PJ, Bilker WB , Kohler C, Siegel SJ, Gur RE. Computerized neurocognitive scanning: II. The profile of schizophrenia. Neuropsychopharmacology. 2001;25:777-88.
39. Heinrichs RW, Zakzanis KK. Neurocognitive deficit in schizophrenia: a quantitative review of the evidence. Neuropsychology. 1998;12:426-445.
40. Hoff AL, Riordan H, O'Donnell DW, Morris L, DeLisi LE. Neuropsychological functioning of first-episode schizophreniform patients. Am J Psychiatry. 1992;149:898-903.
41. Blanchard JJ, Neale JM. The Neuropsychological Signature of Schizophrenia: Generalized or Differential Deficit? Am J Psychiatry. 1994;151:40-48.
42. Mohamed S, Paulsen JS, O'Leary D, Arndt S, Andreasen N. Generalized cognitive deficits in schizophrenia: a study of first-episode patients. Arch Gen Psychiatry. 1999;56:749-54.
43. Albus M, Hubmann W, Mohr F, Scherer J, Sobizack N, Franz U, Hecht S, Borrmann M, Wahlheim C. Are there gender differences in neuropsychological performance in patients with first-episode schizophrenia? Schizophr Res. 1997;28:39-50.
44. Gold JM, Randolph C, Carpenter CJ, Goldberg TE, Weinberger DR. Forms of memory failure in schizophrenia. J Abnorm Psychol. 1992;101:487-494.
45. Censits DM, Ragland JD, Gur RC, Gur RE. Neuropsychological evidence supporting a neurodevelopmental model of schizophrenia: a longitudinal study. Schizophr Res. 1997;24:289-98.
46. Saykin AJ, Gur RC, Gur RE, Mozley PD, Mozley LH, Resnick SM, Kester DB, Stafiniak P. Neuropsychological function in schizophrenia. Selective impairment in memory and learning. Arch Gen Psychiatry. 1991;48:618-24.
47. Saykin AJ, Shtasel DL, Gur RE, Kester DB , Mozley LH, Stafiniak P, Gur RC. Neuropsychological deficits in neuroleptic naive patients with first-episode schizophrenia. Arch Gen Psychiatry. 1994;51:124-31.
48. Tamlyn D, McKenna PJ, Mortimer AM, Lund CE, Hammond S, Baddeley AD. Memory impairment in schizophrenia: its extent, affiliations and neuropsychological character. Psychol Med. 1992;22:101-115.
30

49. Elliott R, McKenna PJ, Robbins TW, Sahakian BJ. Neuropsychological evidence for frontostriatal dysfunction in schizophrenia. Psychol Med. 1995;25:619-30.
50. Hutton SB, Puri BK, Duncan LJ, Robbins TW, Barnes TR, Joyce EM. Executive function in first-episode schizophrenia. Psychol Med. 1998;28:463-473.
51. Elliott R, McKenna PJ, Robbins TW, Sahakian BI. Specific Neuropsychological Deficits in Schizophrenic Patients with Preserved Intellectual Function. Cognitive Neuropsychiatry. 1998;3:45-70.
52. Morrison-Stewart SL, Williamson PC, Corning WC, Kutcher SP, Snow WG, Merskey H. Frontal and non-frontal lobe neuropsychological test performance and clinical symptomatology in schizophrenia. Psychol Med. 1992;22:353-359.
53. Shallice T, Burgess PW, Frith CD. Can the neuropsychological case-study approach be applied to schizophrenia? Psychol Med. 1991;21:661-673.
54. Chapman LJ, Chapman JP. The measurement of differential deficit. Journal of Psychiatric Research. 1978;14:303-311.
55. Lieberman JA. Is schizophrenia a neurodegenerative disorder? A clinical and neurobiological perspective. Biol Psychiatry. 1999;46:729-739.
56. Rabinowitz J, Reichenberg A, Weiser M, Mark M, Kaplan Z, Davidson M. Cognitive and behavioural functioning in men with schizophrenia both before and shortly after first admission to hospital. Cross-sectional analysis. Br J Psychiatry. 2000;177:26-32.
57. Reichenberg A, Rabinowitz J, Weiser M, Mark M, Kaplan Z, Davidson M. Premorbid functioning in a national population of male twins discordant for psychoses. Am J Psychiatry. 2000;157:1514-6.
58. O'Carroll R. Cognitive impairment in schizophrenia. Adv Psychiatr Treat. 2000;6:161-168.
59. Cornblatt B, Obuchowski M, Schnur DB, O'Brien JD. Attention and clinical symptoms in schizophrenia. Psychiatr Q. 1997;68:343-359.
60. Nuechterlein KH, Dawson ME, Gitlin M, Ventura J, Goldstein MJ, Snyder KS, Yee CM, Mintz J. Developmental Processes in Schizophrenic Disorders: longitudinal studies of vulnerability and stress. Schizophr Bull. 1992;18:387-425.
61. Addington J, Addington D, Maticka-Tyndale E. Cognitive functioning and positive and negative symptoms in schizophrenia. Schizophr Res. 1991;5:123-134.
62. Berman I, Viegner B, Merson A, Allan E, Pappas D, Green AI. Differential relationships between positive and negative symptoms and neuropsychological deficits in schizophrenia. Schizophr Res. 1997;25:1-10.
63. Allen HA, Liddle PF, Frith CD. Negative features, retrieval processes and verbal fluency in schizophrenia. Br J Psychiatry. 1993;163:769-775.
64. Moritz S, Woodward TS, Kuppers D, Lausen A, Schickel M. Increased automatic spreading of activation in thought-disordered schizophrenic patients. Schizophr Res. 2003;59:181-186.
65. Spitzer M. A cognitive neuroscience view of schizophrenic thought disorder. Schizophr Bull. 1997;23:29-50.
66. Spitzer M, Braun U, Hermle L, Maier S. Associative semantic network dysfunction in thought-disordered schizophrenic patients: direct evidence from indirect semantic priming. Biol Psychiatry. 1993;34:864-877.
67. Nestor PG, Shenton ME, Wible C, Hokama H , O'Donnell BF, Law S, McCarley RW. A neuropsychological analysis of schizophrenic thought disorder. Schizophr Res. 1998;29:217-225.
68. Goldman-Rakic PS, Selemon LD. Functional and anatomical aspects of prefrontal pathology in schizophrenia. Schizophr Bull . 1997;23:437-458.
69. Nuechterlein KH, Dawson ME. Information processing and attentional functioning in the developmental course of schizophrenic disorders. Schizophr Bull. 1984;10:160-203.
70. Asarnow RF, Nuechterlein KH, Fogelson D, Subotnik KL, Payne DA, Russell AT, Asamen J, Kuppinger H, Kendler KS. Schizophrenia and schizophrenia-spectrum personality disorders in the first-degree relatives of children with schizophrenia: the UCLA family study. Arch Gen Psychiatry. 2001;58:581-588.
71. Asarnow RF, Nuechterlein KH, Subotnik KL, Fogelson DL, Torquato RD, Payne DL, Asamen J, Mintz J, Guthrie D. Neurocognitive impairments in nonpsychotic parents of children with schizophrenia and attention-deficit/hyperactivity disorder:
the University of California, Los Angeles Family Study. Arch Gen Psychiatry. 2002;59:1053-1060.
72. Nuechterlein KH, Dawson ME, Green MF. Information-processing abnormalities as neuropsychological vulnerability indicators for schizophrenia. Acta Psychiatr Scand Suppl. 1994;384:71-79.
73. Cornblatt B, Obuchowski M, Roberts S, Pollack S, Erlenmeyer-Kimling L. Cognitive and behavioral precursors of schizophrenia. Dev Psychopathol. 1999;11:487-508.
74. Cornblatt BA, Keilp JG. Impaired attention, genetics, and the pathophysiology of schizophrenia. Schizophr Bull. 1994;20:31-46.
75. Cornblatt BA. The New York high risk project to the Hillside recognition and prevention (RAP) program. Am J Med Genet. 2002;114:956-66.
76. Erlenmeyer-Kimling L. Neurobehavioral Deficits in Offspring of Schizophrenic Parents: Liability Indicators and Predictors of Illness. Am J Med Gen (SEMIN MED GENET ). 2000;97:65–71 (2000).
77. Harvey PD, White L, Parrella M, Putnam KM, Kincaid MM, Powchik P, Mohs RC, Davidson M. The longitudinal stability of cognitive impairment in schizophrenia. Mini-mental state scores at one- and two-year follow-ups in geriatric in-patients. Br J Psychiatry. 1995;166 :630-633.
78. Heaton RK, Gladsjo JA, Palmer BW, Kuck J , Marcotte TD, Jeste DV. Stability and course of neuropsychological deficits in schizophrenia. Arch Gen Psychiatry. 2001;58:24-32.
79. Wilk CM, Gold JM, Bartko JJ, Dickerson F, Fenton WS, Knable M, Randolph C, Buchanan RW. Test-retest stability of the Repeatable Battery for the Assessment of Neuropsychological Status in schizophrenia. Am J Psychiatry. 2002;159:838-844.
80. Rosmark B, Osby U, Engelbrektson K, Nyman H. Stability of performance on neuropsychological tests in patients with schizophrenia. Eur Arch Psychiatry Clin Neurosci. 1999;249:299-304.
81. Velligan DI, Mahurin RK, Diamond PL, Hazelton BC, Eckert SL, Miller AL. The functional significance of symtomatology and cognitive function in schizohrenia. Schizophrenia Research. 1997;25:21-31.
82. Green MF, Kern RS, Braff DL, Mintz J. Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the "right stuff"? Schizophr Bull. 2000;26:119-136.
83. Lysaker P, Bell M, Beam-Goulet J. Wisconsin card sorting test and work performance in schizophrenia. Psychiatry Res. 1995;56:45-51.
84. Nuechterlein KE, Subotnik KL, Gitlin M, Dawson ME, Ventura J, Snyder KS, Fogelson DL, Shaw S, Mintz J. Neurocognitive and environmental contributors to work recovery after initial onset of schizophrenia: Answers from path analysis. Schizophr Res. 1999.
85. Fenton WS, McGlashan TH. Antecedents, symptom progression, and long-term outcome of the deficit syndrome in schizophrenia. Am J Psychiatry. 1994;151:351-356.
86. Racenstein JM, Penn D, Harrow M, Schleser R. Thought disorder and psychosocial functioning in schizophrenia: the concurrent and predictive relationships. J Nerv Ment Dis. 1999;187:281-289.
87. Hoffmann H, Kupper Z, Zbinden M, Hirsbrunner HP. Predicting vocational functioning and outcome in schizophrenia outpatients attending a vocational rehabilitation program. Soc Psychiatry Psychiatr Epidemiol. 2003;38:76-82.
88. Mueser KT, Bellack AS, Douglas MS, Wade JH. Prediction of social skill acquisition in schizophrenic and major affective disorder patients from memory and symptomatology. Psychiatry Res. 1991;37:281-296.
89. Parnas J. Det skizofrene spektrum. In: Hemmingsen R, Parnas J, Sørensen T, Gjerris A, Bolwig TG, Reisby N, eds. Klinisk Psykiatri. København: Munksgaard; 1994.
90. Weinberger DR. Schizophrenia as a Neurodevelopmental Disorder. In: Hirsch SR, Weinberger DR, eds. Schizophrenia. Oxford: Blackwell Science; 1995:293-323.
91. Murray RM, Lewis SW. Is schizophrenia a neurodevelopmental disorder? Br Med J (Clin Res Ed). 1987;295:681-682.
92. Murray RM. Neurodevelopmental schizophrenia: The rediscovery of dementia praecox. Br J Psychiatry Suppl. 1994;165:6-12.
93. Weinberger DR. Implications of normal brain development for the pathogenesis of schizophrenia. Arch Gen Psychiatry. 1987;44:660-669.
31
94. McGlashan TH, Hoffman RE. Schizophrenia as a disorder of developmentally reduced synaptic connectivity. Arch Gen Psychiatry. 2000;57:637-648.
95. Parnas J, Schulsinger F, Teasdale TW, Schulsinger H, Feldman PM, Mednick SA. Perinatal complications and clinical outcome within the schizophrenia spectrum. The British Journal of Psychiatry. 1982;140:416.
96. Asarnow RF. Neurocognitive impairments in schizophrenia: a piece of the epigenetic puzzle. Eur Child Adolesc Psychiatry. 1999;8 Suppl 1:I5-I8.
97. Eggers C. Some remarks on etiological aspects of early-onset schizophrenia. Eur Child Adolesc Psychiatry. 1999;8 Suppl 1 :I1-I4.
98. Jones P, Rodgers B, Murray R, Marmot M. Child development risk factors for adult schizophrenia in the British 1946 birth cohort. Lancet. 1994;344:1398-1402.
99. Walker EF. Neurodevelopmental precursors of schizophrenia. In: David AS, Cutting J.C, eds. The Neuropsychology of Schizophrenia. Hove: Lawrence Erlbaum Associates; 1994:119-129.
100. Keshavan MS, Anderson S, Pettegrew JW. Is schizophrenia due to excessive synaptic pruning in the prefrontal cortex? the Feinberg hypthesis revisited. J Psychiatr Res. 1994;28:239-265.
101. Giedd JN, Jeffries NO, Blumenthal J, Castellanos FX, Vaituzis AC, Fernandez T, Hamburger SD, Liu H, Nelson J, Bedwell J, Tran L, Lenane M, Nicolson R, Rapoport JL. Childhood-onset schizophrenia: progressive brain changes during adolescence 9. Biol Psychiatry. 1999;46:892-898.
102. Thompson PM, Vidal C, Giedd JN, Gochman P, Blumenthal J, Nicolson R, Toga AW, Rapoport JL. Mapping adolescent brain change reveals dynamic wave of accelerated gray matter loss in very early-onset schizophrenia 3. Proc Natl Acad Sci U S A. 2001;98:11650-11655.
103. Jacobsen LK, Rapoport JL. Research update: childhood-onset schizophrenia: implications of clinical and neurobiological research 13. J Child Psychol Psychiatry. 1998;39 :101-113.
104. Madsen AL, Karle A, Rubin P, Cortsen M, Andersen HS, Hemmingsen R. Progressive atrophy of the frontal lobes in first-episode schizophrenia: interaction with clinical course and neuroleptic treatment. Acta Psychiatr Scand. 1999;100:367-374.
105. Madsen AL, Vorstrup S, Rubin P, Larsen JK, Hemmingsen R. Neurological abnormalities in schizophrenic patients: a prospective follow-up study 5 years after first admission. Acta Psychiatr Scand. 1999;100:119-125.
106. DeLisi LE, Tew W, Xie S, Hoff AL, Sakuma M, Kushner M, Lee G, Shedlack K, Smith AM, Grimson R. A prospective follow-up study of brain morphology and cognition in first-episode schizophrenic patients: preliminary findings. Biol Psychiatry. 1995;38:349-360.
107. Bilder RM, Lipschutz-Broch L, Reiter G, Geisler SH, Mayerhoff DI, Lieberman JA. Intellectual deficits in first-episode schizophrenia: evidence for progressive deterioration. Schizophr Bull. 1992;18:437-48.
108. Mockler D, Riordan J, Sharma T. Memory and intellectual deficits do not decline with age in schizophrenia. Schizophr Res. 1997;26:1-7.
109. Rund BR, Landrø NI, Ørbeck AL. Stability of cognitive dysfunctions in schizophrenic patients. Psychiatry Research. 1997;69:131-141.
110. Rosmark B, Osby U, Engelbrektson K, Nyman H. Stability of performance on neuropsychological tests in patients with schizophrenia. Eur Arch Psychiatry Clin Neurosci. 1999;249:299-304.
111. Albus M, Hubmann W, Scherer J, Dreikorn B, Hecht S, Sobizack N, Mohr F. A prospective 2-year follow-up study of neurocognitive functioning in patients with first-episode schizophrenia. Eur Arch Psychiatry Clin Neurosci. 2002;252:262-7.
112. Rund BR. A review of longitudinal studies of cognitive functions in schizophrenia patients. Schizophr Bull. 1998;24:425-435.
113. Gold S, Arndt S, Nopoulos P, O'Leary DS, Andreasen NC. Longitudinal study of cognitive function in first-episode and recent-onset schizophrenia. Am J Psychiatry. 1999;156:1342-8.
114. Bilder RM, Lipschutz-Broch L, Reiter G, Geisler S, Mayerhoff D, Lieberman JA. Neuropsychological deficits in the early course of first episode schizophrenia. Schizophr Res. 1991;5:198-9.
115. Moritz S, Andresen B, Perro C, Schickel M, Krausz M, Naber D. Neurocognitive performance in first-episode and chronic schizophrenic patients. Eur Arch Psychiatry Clin Neurosci. 2002;252:33-7.
116. Landrø NI, Ørbeck AL, Rund BR. Memory functioning in chronic and non-chronic schizophrenics, affectively disturbed patients and normal controls. Schizophr Res. 1993;10:85-92.
117. Fucetola R, Seidman LJ, Kremen WS, Faraone SV, Goldstein JM, Tsuang MT. Age and neuropsychologic function in schizophrenia: a decline in executive abilities beyond that observed in healthy volunteers. Biol Psychiatry. 2000;48:137-46.
118. Barnes TR, Hutton SB, Chapman MJ, Mutsatsa S, Puri BK, Joyce EM. West London first-episode study of schizophrenia. Clinical correlates of duration of untreated psychosis. Br J Psychiatry. 2000;177:207-211.
119. Joyce E, Hutton S, Mutsatsa S, Gibbins H, Webb E, Paul S, Robbins T, Barnes T. Executive dysfunction in first-episode schizophrenia and relationship to duration of untreated psychosis: the West London Study. Br J Psychiatry Suppl. 2002;43:s38-s44.
120. Pantelis C, Barnes TR, Nelson HE, Tanner S, Weatherley L, Owen AM, Robbins TW. Frontal-striatal cognitive deficits in patients with chronic schizophrenia. Brain. 1997;120 ( Pt 10):1823-1843.
121. Pantelis C, Barber FZ, Barnes TR, Nelson HE, Owen AM, Robbins TW. Comparison of set-shifting ability in patients with chronic schizophrenia and frontal lobe damage. Schizophr Res. 1999;37:251-270.
122. Eberhard J, Riley F, Levander S. Premorbid IQ and schizophrenia Increasing cognitive reduction by episodes. Eur Arch Psychiatry Clin Neurosci. 2003;253:84-88.
123. Norman RMG, Townsend L, Malla AK. Duration of untreated psychosis and cognitive functioning in first-episode patients. Br J Psychiatry. 2001;179:340-345.
124. Levander S, Jensen J, Grawe R, Tuninger E. Schizophrenia--progressive and massive decline in response readiness by episodes. Acta Psychiatr Scand Suppl. 2001;65-74.
125. Keshavan MS, Hogarty GE. Brain maturational processes and delayed onset in schizophrenia. Dev Psychopathol. 1999;11:525-543.
126. Luna B, Thulborn KR, Munoz DP, Merriam EP, Garver KE, Minshew NJ, Keshavan MS, Genovese CR, Eddy WF, Sweeney JA. Maturation of widely distributed brain function subserves cognitive development. Neuroimage. 2001;13:786-793.
127. Fuster JM. Frontal lobe and cognitive development. J Neurocytol . 2002;31:373-385.
128. Remschmidt H. Early-onset schizophrenia as a progressive-deteriorating developmental disorder: evidence from child psychiatry 2. J Neural Transm. 2002;109:101-117.
129. Diamond A. Normal Development of Prefrontal Cortex from Birth to Young Adulthood: Cognitive Fuctions, Anatomy, and Biochemistry. In: Stuss DT, Knight RT, eds. Principles of Frontal Lobe Function. Oxford: Oxford University Press; 2002:466-503.
130. Pantelis C, Yucel M, Wood SJ, McGorry PD, Velakoulis D. Early and late neurodevelopmental disturbances in schizophrenia and their functional consequences. Aust N Z J Psychiatry. 2003;37:399-406.
131. Asarnow RF, Asamen J, Granholm E, Sherman T, Watkins JM, Williams ME. Cognitive/neuropsychological studies of children with a schizophrenic disorder. Schizophr Bull. 1994;20:647-669.
132. Goldberg TE, Gold JM, Greenberg R, Griffin S, Schulz SC, Pickar D, Kleinman JE, Weinberger DR. Contrasts between patients with affective disorders and patients with schizophrenia on a neuropsychological test battery. Am J Psychiatry. 1993;150:1355-1362.
133. Kremen WS, Seidman LJ, Faraone SV, Tsuang MT. Intelligence quotient and neuropsychological profiles in patients with schizophrenia and in normal volunteers. Biol Psychiatry. 2001;50:453-462.
134. Nelson HE, Pantelis C, Carruthers K, Speller J, Baxendale S, Barnes TR. Cognitive functioning and symptomatology in chronic schizophrenia. Psychol Med. 1990;20:357-365.
135. Nelson HE, O'Connell A. Dementia: the estimation of premorbid intelligence levels using the New Adult Reading Test 1. Cortex. 1978;14:234-244.
32

136. Wechsler D. Manual for the Wechsler Adult Intelligence Scale (WAIS). San Antonio, Texas: The Psychological Corporation; 1955.
137. Gilvarry C, Takei N, Russell A, Rushe T , Hemsley D, Murray RM. Premorbid IQ in patients with functional psychosis and their first-degree relatives. Schizophr Res. 2000;41:417-29.
138. Kremen WS, Buka SL, Seidman LJ, Goldstein JM, Koren D, Tsuang MT. IQ decline during childhood and adult psychotic symptoms in a community sample: a 19-year longitudinal study. Am J Psychiatry. 1998;155:672-677.
139. Weickert TW, Goldberg TE, Gold JM, Bigelow LB, Egan MF, Weinberger DR. Cognitive impairments in patients with schizophrenia displaying preserved and compromised intellect. Arch Gen Psychiatry. 2000;57:907-913.
140. Frith C. Functional imaging and cognitive abnormalities. Lancet 1995;346:615-620.
141. Bedwell JS, Keller B, Smith AK, Hamburger S, Kumra S, Rapoport JL. Why does postpsychotic IQ decline in childhood-onset schizophrenia? Am J Psychiatry. 1999;156:1996-1997.
142. Baddeley A. Working Memory. Oxford: Oxford University Press; 1986.
143. Denckla MB. A Theory and Model of Executive Function: A Neuropsychological Perspective. In: Lyon GR, Krasnegor NA, eds. Attention, Memory, and Executive Function. Baltimore, ML.: Paul Brookes Publishing Co.; 1996:263-278.
144. Phillips LH. Do "Frontal Tests" Measure Executive Function?: Issues of Assessment and Evidence from Fluency Tests. In: Rabbitt P, ed. Methodology of Frontal and Executive Function. Hove, U.K.: Psychology Press; 1997:191-213.
145. Duncan J, Burgess P, Emslie H. Fluid intelligence after frontal lobe lesions. Neuropsychologia. 1995;33:261-268.
146. Morice R, Delahunty A. Frontal/executive impairments in schizophrenia. Schizophr Bull. 1996;22:125-137.
147. Robbins TW. Dissociating executive functions of the prefrontal cortex. Philos Trans R Soc Lond B Biol Sci. 1996;351:1463-1470.
148. Robbins TW, James M, Owen AM, Sahakian BJ, Lawrence AD, McInnes L, Rabbitt PM. A study of performance on tests from the CANTAB battery sensitive to frontal lobe dysfunction in a large sample of normal volunteers: implications for theories of executive functioning and cognitive aging.Cambridge Neuropsychological Test Automated Battery. J Int Neuropsychol Soc. 1998;4:474-490.
149. Pantelis C, Brewer W. Neurocognitive and Neurobehavioral Patterns and the Syndromes of Schizophrenia: Role of Frontal-Subcortical Networks. In: Pantelis C, Nelson HE, Barnes TRE, eds. Schizophrenia: A Neuropsychological Perspective. Chichester: John Wiley & Sons Ltd.; 1996:317-343.
150. Zalla T, Posada A, Franck N, Georgieff N, Sirigu A. A component analysis of action planning processes in schizophrenia: A comparison with patients with frontal lobe damage. Cognitive Neuropsychiatry. 2001;6:271-296.
151. Seidman LJ. Schizophrenia and brain dysfunction: an integration of recent neurodiagnostic findings. Psychol Bull. 1983;94:195-238.
152. Bryson G, Whelahan HA, Bell M. Memory and executive function impairments in deficit syndrome schizophrenia. Psychiatry Res. 2001;102:29-37.
153. Johnson-Selfridge M, Zalewski C. Moderator variables of executive functioning in schizophrenia: meta-analytic findings. Schizophr Bull. 2001;27:305-316.
154. Addington J, Addington D. Cognitive functioning in first-episode schizophrenia. J Psychiatry Neurosci. 2002;27:188-92.
155. Addington J, Brooks BL, Addington D. Cognitive functioning in first episode psychosis: initial presentation. Schizophrenia Research. 2003;62:59-64.
156. Rubin P, Holm A, Møller-Madsen S, Videbech P, Hertel C, Povlsen UJ, Hemmingsen R. Neuropsychological deficits in newly diagnosed patients with schizophrenia or schizophreniform disorder. Acta Psychiatr Scand. 1995;92:35-43.
157. Nestor PG, O'Donnell BF. The Mind Adrift: Attentional Dysregulation in Schizophrenia. In: Parasuraman R, ed. The Attentive Brain. Cambridge: The MIT Press; 2000.
158. McGhie A, Chapman J. Disorders of attention and perception in early schizophrenia. Br J Med Psychol. 1961;34:103-116.
159. Carlsson A. Speculations on the control of mental and motor functions by dopamine-modulated cortico-striato-thalamo-cortical feedback loops. Mt Sinai J Med. 1988;55:6-10.
160. Glenthoj BY, Hemmingsen R. Transmitter dysfunction during the process of schizophrenia. Acta Psychiatr Scand Suppl. 1999;395:105-112.
161. Hong KS, Kim JG, Koh HJ, Koo MS, Kim JH, Lee D, Kim E. Effects of risperidone on information processing and attention in first-episode schizophrenia. Schizophr Res. 2002;53:7-16.
162. Mackeprang T, Kristiansen KT, Glenthoj BY. Effects of antipsychotics on prepulse inhibition of the startle response in drug-naive schizophrenic patients. Biol Psychiatry. 2002;52:863-873.
163. van den Bosch RJ, Rombouts RP, van Asma MJ. What determines continuous performance task performance? Schizophr Bull. 1996;22:643-651.
164. LaBerge D. Thalamic and Cortical Mechanisms of Attention Suggested by Recent Positron Emission Tomographic Experiments. J Cogn Neurosci. 1990;2:358-372.
165. Mesulam MM. From sensation to cognition. Brain. 1998;121 ( Pt 6):1013-1052.
166. Cannon TD, Zorrilla LE, Shtasel D, Gur RE, Gur RC, Marco EJ, Moberg P, Price RA. Neuropsychological functioning in siblings discordant for schizophrenia and healthy volunteers. Arch Gen Psychiatry. 1994;51:651-661.
167. Franke P, Maier W, Hardt J, Hain C, Cornblatt BA. Attentional abilities and measures of schizotypy: their variation and covariation in schizophrenic patients, their siblings, and normal control subjects. Psychiatry Res. 1994;54:259-272.
168. Erlenmeyer-Kimling L, Rock D, Roberts SA, Janal M, Kestenbaum C, Cornblatt B, Adamo UH, Gottesman II. Attention, memory, and motor skills as childhood predictors of schizophrenia-related psychoses: the New York High-Risk Project. Am J Psychiatry. 2000;157:1416-1422.
169. DiGirolamo GJ, Posner MI. Attention and Schizophrenia: A View from Cognitive Neuroscience. Cognitive Neuropsychiatry. 1996;1:95-102.
170. Maruff P, Hay D, Malone V, Currie J. Asymmetries in the covert orienting of visual spatial attention in schizophrenia. Neuropsychologia. 1995;33:1205-1223.
171. Maruff P, Pantelis C, Danckert J, Smith D, Currie J. Deficits in the endogenous redirection of covert visual attention in chronic schizophrenia. Neuropsychologia. 1996;34:1079-1084.
172. Fuster JM. Physiology of Executive Functions: The Perception-Action Cycle. In: Stuss DT, Knight RT, eds. Principles of frontal lobe function. Oxford: Oxford University Press; 2002:96-108.
173. Tulving E. Chronesthesia: Conscious Awareness of Subjective Time. In: Stuss DT, Knight RT, eds. Principles of frontal lobe function. Oxford: Oxford University Press; 2002:311-325.
174. MacFlynn G, Montgomery EA, Fenton GW, Rutherford W. Measurement of reaction time following minor head injury. J Neurol Neurosurg Psychiatry. 1984;47:1326-1331.
175. Western SL, Long CJ. Relationship between reaction time and neuropsychological test performance. Archives of Clinical Neuropsychology. 1996;11:557-571.
176. Gale HJ, Holzman PS. A new look at reaction time in schizophrenia. Schizophrenia Research. 2000;46:149-165.
177. Zahn TP, Jacobsen LK, Gordon CT, McKenna K, Frazier JA, Rapoport JL. Attention deficits in childhood-onset schizophrenia: reaction time studies. J Abnorm Psychol. 1998;107:97-108.
178. Schatz J. Cognitive processing efficiency in schizophrenia: generalized vs domain specific deficits. Schizophr Res. 1998;30:41-49.
179. Maier W, Franke P, Kopp B, Hardt J, Hain C, Rist F. Reaction time paradigms in subjects at risk for schizophrenia. Schizophr Res. 1994;13:35-43.
180. Liddle PF, Barnes TR, Morris D, Haque S . Three syndromes in chronic schizophrenia review. Br J Psychiatry. 1989;Suppl. 7:119-122.
181. Ngan ET, Liddle PF. Reaction time, symptom profiles and course of illness in schizophrenia. Schizophr Res. 2000;46:195-201.
182. Tuninger E, Levander S. Neuropsychological impairment in patients treated with depot neuroleptics: a longitudinal study. Acta Psychiatr Scand Suppl. 2001;75-80.
183. Carpenter WT, Gold JM. Another view of therapy for cognition in schizophrenia. Biol Psychiatry. 2002;51:969-71.
184. Harvey PD, Keefe RS. Studies of cognitive change in patients with schizophrenia following novel antipsychotic treatment. Am J Psychiatry. 2001;158:176-184.
33
185. Spohn HE, Strauss ME. Relation of neuroleptic and anticholinergic medication to cognitive functions in schizophrenia. J Abnorm Psychol. 1989;98:367-80.
186. Sweeney JA, Keilp JG, Haas GL, Hill J, Weiden PJ. Relationships between medication treatments and neuropsychological test performance in schizophrenia. Psychiatry Res. 1991;37:297-308.
187. Kern RS, Green MF, Marshall BD, Jr., Wirshing WC, Wirshing D, McGurk S, Marder SR, Mintz J. Risperidone vs. haloperidol on reaction time, manual dexterity, and motor learning in treatment-resistant schizophrenia patients. Biol Psychiatry. 1998;44:726-732.
188. Meltzer HY, McGurk SR. The effects of clozapine, risperidone, and olanzapine on cognitive function in schizophrenia. Schizophr Bull. 1999;25:233-255.
189. Kern RS, Green MF, Marshall BD, Jr., Wirshing WC, Wirshing D, McGurk SR , Marder SR, Mintz J. Risperidone versus haloperidol on secondary memory: can newer medications aid learning? Schizophr Bull. 1999;25:223-232.
190. Bilder RM, Goldman RS, Volavka J, Czobor P, Hoptman M, Sheitman B, Lindenmayer JP, Citrome L, McEvoy J, Kunz M, Chakos M, Cooper TB, Horowitz TL, Lieberman JA. Neurocognitive effects of clozapine, olanzapine, risperidone, and haloperidol in patients with chronic schizophrenia or schizoaffective disorder. Am J Psychiatry. 2002;159:1018-1028.
191. Purdon SE. Cognitive improvement in schizophrenia with novel antipsychotic medications. Schizophr Res. 1999;35 Suppl:S51-S60.
192. Purdon SE, Jones BD, Stip E, Labelle A, Addington D, David SR, Breier A, Tollefson GD. Neuropsychological change in early phase schizophrenia during 12 months of treatment with olanzapine, risperidone, or haloperidol. The Canadian Collaborative Group for research in schizophrenia. Arch Gen Psychiatry. 2000;57:249-258.
193. Keefe RS, Silva SG, Perkins DO, Lieberman JA. The effects of atypical antipsychotic drugs on neurocognitive impairment in schizophrenia: a review and meta-analysis. Schizophr Bull. 1999;25:201-22.
194. Velligan DI, Newcomer J, Pultz J, Csernansky J, Hoff AL, Mahurin R, Miller AL. Does cognitive function improve with quetiapine in comparison to haloperidol? Schizophr Res. 2002;53:239-48.
195. Bollini P, Pampallona S, Orza MJ, Adams ME, Chalmers TC. Antipsychotic drugs: is more worse? A meta-analysis of the published randomized control trials. Psychol Med. 1994;24:307-16.
196. Geddes J, Freemantle N, Harrison P, Bebbington P. Atypical antipsychotics in the treatment of schizophrenia: systematic overview and meta-regression analysis. Bmj. 2000;321:1371-6.
197. Leucht S, Pitschel-Walz G, Abraham D, Kissling W. Efficacy and extrapyramidal side-effects of the new antipsychotics olanzapine, quetiapine, risperidone, and sertindole compared to conventional antipsychotics and placebo. A meta-analysis of randomized controlled trials. Schizophr Res. 1999;35:51-68.
198. Kapur S, Seeman P. Does fast dissociation from the dopamine d(2) receptor explain the action of atypical antipsychotics?: A new hypothesis. Am J Psychiatry. 2001;158:360-9.
199. Green MF, Marder SR, Glynn SM, McGurk SR, Wirshing WC, Wirshing DA, Liberman RP, Mintz J. The neurocognitive effects of low-dose haloperidol: a two-year comparison with risperidone. Biol Psychiatry. 2002;51:972-978.
200. Harvey PD, Green MF, McGurk SR, Meltzer HY. Changes in cognitive functioning with risperidone and olanzapine treatment: a large-scale, double-blind, randomized study. Psychopharmacology (Berl). 2003.
201. The ICD-10 classification of mental and behavioral disorders. Diagnostic criteria for research. World Health Organization; 1993.
202. Schedules for clinical assessment in neuropsychiatry. World Health Organization; 1994.
203. Kay SR. Positive and Negative Syndromes in Schizophrenia. New York: Brunner/Mazel; 1991.
204. Andreasen NC. The Scale for the Assessment of Negative Symptoms (SANS). Iowa City: Department of Psychiatry, The University of Iowa College of Medicine; 1984.
205. Andreasen NC. The Scale for the Assessment of Positive Symptoms (SAPS). Iowa City: Department of Psychiatry, The University of Iowa College of Medicine; 1984.
206. Fray PJ, Robbins TW. CANTAB battery: proposed utility in neurotoxicology. Neurotoxicol Teratol. 1996;18:499-504.
207. Sahakian BJ, Owen AM. Computerized assessment in neuropsychiatry using CANTAB: discussion paper. J R Soc Med. 1992;85:399-402.
208. Milner B. Effects of different brain lesions on card sorting. Archives of neurology. 1963;9:90-100.
209. Spreen O, Strauss E. A compendium of neuropsychological tests . New York: Oxford University Press; 1991.
210. Regard M, Strauss E, Knapp P. Children's production on verbal and non-verbal fluency tasks. Percept Mot Skills. 1982;55:839-844.
211. Reitan RM, Wolfson D. The Halstead-Reitan Neuropsychological Test Battery: Theory and Clinical Interpretation. Tucson, AZ.: Neuropsychology Press; 1993.
212. Hess, G. WAIS anvendt på 698 50-årige. 1974. University of Copenhagen. Ref Type: Thesis/Dissertation
213. Lezak MD. Neuropsychological Assessment. 3 ed. New York: Oxford University Press; 1995.
214. Buchanan RW, Strauss ME, Kirkpatrick B, Holstein C, Breier A, Carpenter WT, Jr. Neuropsychological impairments in deficit vs nondeficit forms of schizophrenia. Arch Gen Psychiatry. 1994;51:804-11.
215. Rahman S, Sahakian BJ, Hodges JR, Rogers RD, Robbins TW. Specific cognitive deficits in mild frontal variant frontotemporal dementia. Brain. 1999;122 ( Pt 8):1469-1493.
216. Lawrence AD, Weeks RA, Brooks DJ, Andrews TC, Watkins LH, Harding AE, Robbins TW, Sahakian BJ. The relationship between striatal dopamine receptor binding and cognitive performance in Huntington's disease. Brain. 1998;121 ( Pt 7):1343-1355.
217. Owen AM, Morris RG, Sahakian BJ, Polkey CE, Robbins TW. Double dissociations of memory and executive functions in working memory tasks following frontal lobe excisions, temporal lobe excisions or amygdalo-hippocampectomy in man. Brain. 1996;119 ( Pt 5):1597-1615.
218. Sahakian BJ, Morris RG, Evenden JL, Heald A, Levy R, Philpot M, Robbins TW. A comparative study of visuospatial memory and learning in Alzheimer-type dementia and Parkinson's disease. Brain. 1988;111 ( Pt 3):695-718.
219. Joyce EM, Robbins TW. Frontal lobe function in Korsakoff and non-Korsakoff alcoholics: planning and spatial working memory. Neuropsychologia. 1991;29:709-723.
220. Weed MR, Taffe MA, Polis I, Roberts AC, Robbins TW, Koob GF, Bloom FE, Gold LH. Performance norms for a rhesus monkey neuropsychological testing battery: acquisition and long-term performance. Brain Res Cogn Brain Res. 1999;8:185-201.
221. Laws KR. A Meta-analytic Review of Wisconsin Card Sorting Studies in Schizophrenia: General Intellectual Deficit in Disguise? Cognitive Neuropsychiatry. 1999;4:1-35.
222. Owen AM, Roberts AC, Polkey CE, Sahakian BJ, Robbins TW. Extra-dimensional versus intra-dimensional set shifting performance following frontal lobe excisions, temporal lobe excisions or amygdalo-hippocampectomy in man. Neuropsychologia. 1991;29:993-1006.
223. Shallice T. Specific impairments in planning. Philos Trans R Soc Lond. 1982;298:199-209.
224. Heinrichs RW. In Search of Madness. Schizophrenia and Neuroscience. Oxford: Oxford University Press; 2001.
225. Andreasen NC, Rezai K, Alliger R, Swayze VW, Flaum M, Kirchner P, Cohen G, O'Leary DS. Hypofrontality in neuroleptic-naive patients and in patients with chronic schizophrenia. Assessment with xenon 133 single-photon emission computed tomography and the Tower of London. Arch Gen Psychiatry. 1992;49:943-958.
226. Goldberg TE, Saint-Cyr JA, Weinberger DR. Assessment of procedural learning and problem solving in schizophrenic patients by Tower of Hanoi type tasks. J Neuropsychiatry Clin Neurosci. 1990;2:165-173.
227. Morris RG, Rushe T, Woodruffe PW, Murray RM. Problem solving in schizophrenia: a specific deficit in planing ability. Schizophr Res. 1995; 14:246.
228. Nelson HE. A modified card sorting test sensitive to frontal lobe defects. Cortex. 1976;12:313-24.
229. Raven JC, Court JH, Raven J. Manual for Raven's Progressive Matrices. London: H.K. Lewis; 1976.
230. Crawford JR, Besson JA, Bremner M, Ebmeier KP, Cochrane RH, Kirkwood K. Estimation of premorbid intelligence in schizophrenia. Br J Psychiatry. 1992;161 :69-74.
34

231. O'Carroll R, Walker M, Dunan J, Murray C, Blackwood D, Ebmeier KP, Goodwin GM. Selecting controls for schizophrenia research studies: the use of the National Adult Reading Test (NART) is a measure of premorbid ability. Schizophr Res. 1992;8:137-41.
232. Smith D, Roberts S, Brewer W, Pantelis C. Test-retest Reliability of the National Adult Reading Test (NART) as an Estimate of Premorbid IQ in Patients with Schizophrenia. Cognitive Neuropsychiatry. 1998;3:71-80.
233. Russell AJ, Munro J, Jones PB, Hayward P, Hemsley DR, Murray RM. The National Adult Reading Test as a measure of premorbid IQ in schizophrenia. Br J Clin Psychol. 2000;39 ( Pt 3):297-305.
234. Weickert TW, Goldberg TE. The course of cognitive impairment in patients with schizophrenia. In: Sharma T, Harvey PD, eds. Cognition in schizophrenia. Impairments, Importance and Treatment Strategies. Oxford: Oxford University Press; 2000:3-15.
235. Heaton RK. Wisconsin Card Sorting Test Manual. Odessa, Florida.: Psychological Assessment Resources.; 1981.
236. Heaton RK, Chelune GJ, Talley JL, Kay GG, Curtiss G. Wisconsin Card Sorting Test Manual: Revised and Expanded. Odessa, FL.: Psychological Assessment Resources Inc.; 1993.
237. Owen AM, Morris RG, Sahakian BJ, Polkey CE, Robbins TW. Double dissociations of memory and executive functions in working memory tasks following frontal lobe excisions, temporal lobe excisions or amygdalo-hippocampectomy in man. Brain. 1996;119 ( Pt 5):1597-1615.
238. Owen AM, James M, Leigh PN, Summers BA, Marsden CD, Quinn NP, Lange KW, Robbins TW. Fronto-striatal cognitive deficits at different stages of Parkinson's disease. Brain. 1992;115 ( Pt 6):1727-1751.
239. Kremen WS, Seidman LJ, Faraone SV, Tsuang MT. Is there disproportionate impairment in semantic or phonemic fluency in schizophrenia? J Int Neuropsychol Soc. 2003;9:79-88.
240. Giovannetti T, Goldstein RZ, Schullery M, Barr WB, Bilder RM. Category fluency in first-episode schizophrenia. J Int Neuropsychol Soc. 2003;9:384-393.
241. Robbins TW. Dissociating executive functions of the prefrontal cortex. In: Roberts AC, Robbins TW, Weiskrantz L, eds. The Prefrontal Cortex. Executive and Cognitive Functions. Oxford: Oxford University Press; 1998:117-130.
242. Riley EM, McGovern D, Mockler D, Doku VC, S OC, Fannon DG, Tennakoon L, Santamaria M, Soni W, Morris RG, Sharma T. Neuropsychological functioning in first-episode psychosis--evidence of specific deficits. Schizophr Res. 2000;43:47-55.
243. Thomsen PH. Schizophrenia with childhood and adolescent onset--a nationwide register-based study. Acta Psychiatr Scand. 1996;94:187-193.
244. Hollis C. Adolescent schizophrenia. Adv Psychiatr Treat. 2000;6:83-92.
245. Green WH, Padron-Gayol M, Hardesty AS, Bassiri M. Schizophrenia with childhood onset: a phenomenological study of 38 cases 1. J Am Acad Child Adolesc Psychiatry. 1992;31:968-976.
246. Russell AT. The clinical presentation of childhood-onset schizophrenia 1. Schizophr Bull. 1994;20:631-646.
247. Daradkeh TK. Stability of psychiatric diagnoses in clinical practice. Int J Soc Psychiatry. 1996;42:207-212.
248. Tsuang MT, Woolson RF, Winokur G, Crowe RR. Stability of psychiatric diagnosis. Schizophrenia and affective disorders followed up over a 30- to 40-year period. Arch Gen Psychiatry. 1981;38:535-539.
249. Mason P, Harrison G, Croudace T, Glazebrook C, Medley I. The predictive validity of a diagnosis of schizophrenia. A report from the International Study of Schizophrenia (ISoS) coordinated by the World Health Organization and the Department of Psychiatry, University of Nottingham. The British Journal of Psychiatry. 1997;170:321.
250. Chen YR, Swann AC, Burt DB. Stability of diagnosis in schizophrenia. American Journal of Psychiatry. 1996;153:682.
251. Kumra S, Jacobsen LK, Lenane M, Zahn TP , Wiggs E, Alaghband-Rad J, Castellanos FX, Frazier JA, McKenna K, Gordon CT, Smith A, Hamburger S, Rapoport JL. "Multidimensionally impaired disorder": is it a variant of very early-onset schizophrenia? J Am Acad Child Adolesc Psychiatry. 1998;37:91-9.
252. Hollis C. Adult Outcomes of Child- and Adolescent-Onset Schizophrenia: Diagnostic Stability and Predictive Validity. Am J Psychiatry. 2000;157:1652-1659.
253. Asarnow RF, Brown W, Strandburg R. Children with a schizophrenic disorder: neurobehavioral studies. Eur Arch Psychiatry Clin Neurosci. 1995;245:70-79.
254. Nicolson R, Brookner FB, Lenane M, Gochman P, Ingraham LJ, Egan MF, Kendler KS, Pickar D, Weinberger DR, Rapoport JL. Parental schizophrenia spectrum disorders in childhood-onset and adult-onset schizophrenia. Am J Psychiatry. 2003;160:490-495.
255. Maziade M, Bouchard S, Gingras N, Charron L, Cardinal A, Roy MA, Gauthier B, Tremblay G, Cote S, Fournier C, Boutin P, Hamel M, Merette C, Martinez M. Long-term stability of diagnosis and symptom dimensions in a systematic sample of patients with onset of schizophrenia in childhood and early adolescence. II: Postnegative distinction and childhood predictors of adult outcome. The British Journal of Psychiatry. 1996;169:371-378.
256. Hollis C. Developmental precursors of child- and adolescent-onset schizophrenia and affective psychoses: diagnostic specificity and continuity with symptom dimensions. Br J Psychiatry. 2003;182:37-44.
257. Eggers C, Bunk D. The long-term course of childhood-onset schizophrenia: a 42-year followup. Schizophr Bull. 1997;23:105-117.
258. Werry JS, McClellan JM, Andrews LK, Ham M. Clinical features and outcome of child and adolescent schizophrenia. Schizophr Bull. 1994;20:619-630.
259. Asarnow JR, Tompson MC, Goldstein MJ. Childhood-onset schizophrenia: a followup study. Schizophr Bull. 1994;20:599-617.
260. Hafner H. Gender differences in schizophrenia. Psychoneuroendocrinology. 2003;28 Suppl 2:17-54.
261. Asarnow RF, Tanguay PE, Bott L, Freeman BJ. Patterns of intellectual functioning in non-retarded autistic and schizophrenic children. J Child Psychol Psychiatry. 1987;28:273-280.
262. Asarnow RF, Caplan R, Asarnow JR. Neurobehavioral Studies of Schizophrenic Children: A Developmental Perspective on Schizophrenic Disorders. In: Häfner H, Gattaz WF, eds. Search for the Causes of Schizophrenia, Vol. III. Berlin Heidelberg: Springer-Verlag; 1995:87-113.
263. Banaschewski T, Schulz E, Martin M, Remschmidt H. Cognitive functions and psychopathological symptoms in early-onset schizophrenia. Eur Child Adolesc Psychiatry. 2000;9:11-20.
264. Basso MR, Nasrallah HA, Olson SC, Bornstein RA. Cognitive deficits distinguish patients with adolescent- and adult-onset schizophrenia. Neuropsychiatry Neuropsychol Behav Neurol. 1997;10:107-112.
265. Hoff AL, Harris D, Faustman WO, Beal M, DeVilliers D, Mone RD, Moses JA, Csernansky JG. A neuropsychological study of early onset schizophrenia. Schizophr Res. 1996;20:21-28.
266. Kravariti E, Morris RG, Rabe-Hesketh S, Murray RM, Frangou S. The Maudsley early onset schizophrenia study: cognitive function in adolescents with recent onset schizophrenia. Schizophr Res. 2003; 61:137-148.
267. Oie M, Rund BR, Sundet K, Bryhn G. Auditory laterality and selective attention: normal performance in patients with early-onset schizophrenia. Schizophr Bull. 1998;24:643-652.
268. Rund BR, Zeiner P, Sundet K, Oie M, Bryhn G. No vigilance deficit found in either young schizophrenic or ADHD subjects. Scand J Psychol. 1998;39:101-107.
269. Kumra S, Wiggs E, Bedwell J, Smith AK, Arling E, Albus K, Hamburger SD, McKenna K, Jacobsen LK, Rapoport JL, Asarnow RF. Neuropsychological deficits in pediatric patients with childhood-onset schizophrenia and psychotic disorder not otherwise specified. Schizophr Res. 2000;42:135-44.
270. Werry JS, McClellan JM, Chard L. Childhood and adolescent schizophrenic, bipolar, and schizoaffective disorders: a clinical and outcome study. J Am Acad Child Adolesc Psychiatry. 1991;30:457-65.
271. Wechsler D. Manual for the Wechsler Intelligence Scale for Children - Third Edition (WISC-III). San Antonio, Texas: The Psychological Corporation; 1991.
272. Wechsler D. Manual for the Wechsler Intelligence Scale for Children - Revised (WISC-R). San Antonio, Texas: The Psychological Corporation; 1974.
35
273. Albus M, Hubmann W, Wahlheim C, Sobizack N, Franz U, Mohr F. Contrasts in neuropsychological test profile between patients with first-episode schizophrenia and first-episode affective disorders. Acta Psychiatr Scand. 1996;94:87-93.
274. Jeste DV, Heaton SC, Paulsen JS, Ercoli L, Harris J, Heaton RK. Clinical and neuropsychological comparison of psychotic depression with nonpsychotic depression and schizophrenia. Am J Psychiatry. 1996;153:490-6.
275. Evans JD, Heaton RK, Paulsen JS, McAdams LA, Heaton SC, Jeste DV. Schizoaffective disorder: a form of schizophrenia or affective disorder? 2. J Clin Psychiatry. 1999;60:874-882.
276. Salisbury DF, Shenton ME, Sherwood AR, Fischer IA, Yurgelun-Todd DA, Tohen M, McCarley RW. First-episode schizophrenic psychosis differs from first-episode affective psychosis and controls in P300 amplitude over left temporal lobe. Arch Gen Psychiatry. 1998;55:173-80.
277. Poulton R, Caspi A, Moffitt TE, Cannon M, Murray R, Harrington H. Children's self-reported psychotic symptoms and adult schizophreniform disorder: a 15-year longitudinal study. Arch Gen Psychiatry. 2000;57:1053-1058.
278. Gunnell D, Harrison G, Rasmussen F, Fouskakis D, Tynelius P. Associations between premorbid intellectual performance, early-life exposures and early-onset schizophrenia: Cohort study. Br J Psychiatry. 2002;181:298-305.
279. Purcell DW, Lewine RR, Caudle J, Price LR. Sex differences in verbal IQ-performance IQ discrepancies among patients with schizophrenia and normal volunteers. J Abnorm Psychol. 1998;107:161-165.
280. Hemsley DR. Perceptual and Cognitive Abnormalities as the Bases for Schizophrenic Symptoms. In: David AS, Cutting J.C , eds. The Neuropsychology of Schizophrenia. Hove, UK: Lawrence Erlbaum Associates, Publishers; 1994:97-116.
281. Weinberger DR. Schizophrenia and the frontal lobe. Trends Neurosci. 1988;11:367-370.
282. Owen AM, Downes JJ, Sahakian BJ, Polkey CE, Robbins TW. Planning and spatial working memory following frontal lobe lesions in man. Neuropsychologia. 1990;28:1021-1034.
283. Asarnow RF, Sherman T. Studies of visual information processing in schizophrenic children. Child Dev. 1984; 55:249-261.
284. Bellgrove MA, Vance A, Bradshaw JL. Local-global processing in early-onset schizophrenia: evidence for an impairment in shifting the spatial scale of attention. Brain Cogn. 2003;51:48-65.
285. Galdos PM, van Os JJ, Murray RM. Puberty and the onset of psychosis. Schizophr Res. 1993;10:7-14.
286. Maziade M, Gingras N, Rodrigue C, Bouchard S, Cardinal A, Gauthier B, Tremblay G, Cote S, Fournier C, Boutin P, Hamel M, Roy MA, Martinez M, Merette C. Long-term stability of diagnosis and symptom dimensions in a systematic sample of patients with onset of schizophrenia in childhood and early adolescence. I: nosology, sex and age of onset. Br J Psychiatry. 1996;169:361-370.
287. Wechsler D. Manual for the Wechsler Adult Intelligence Scale - Third Edition (WAIS-III). San Antonio, Texas.: The Psychological Corporation.; 1997.
288. Cummings JL, Benson DF. Psychological dysfunction accompanying subcortical dementias. Annu Rev Med. 1988;39:53-61.
289. Cummings JL. Subcortical dementia. Neuropsychology, neuropsychiatry, and pathophysiology. Br J Psychiatry. 1986;149 :682-697.
290. Wechsler D. Manual for the Wechsler Intelligence Scale for Children (WISC). San Antonio, Texas: The Psychological Corporation; 1949.
36

Appendix 1: Fagerlund, B., Mackeprang, T., Gade, A., Hemmingsen, R.,
Glenthøj, B. Effects of Low-Dose Risperidone and Low-Dose Zuclopenthixol on Cognitive Functions in First-Episode Drug-Naïve Schizophrenic Patients. Paper IN PRESS CNS Spectrums May 2004.
Article Type: Original Research Title: Effects of Low-Dose Risperidone and Low-Dose Zuclopenthixol on Cognitive Functions in First-Episode Drug-Naïve Schizophrenic Patients. Byline: Birgitte Fagerlund, M.Sc.*ab; Torben Mackeprang†, M.D.a; Anders Gade Ph.D.b; Ralf Hemmingsen, D.M.Sca; Birte Y. Glenthøj, D.M.Sc.a. Location of work: a: Department of Psychiatry, Copenhagen University Hospital Bispebjerg, Copenhagen, Denmark; b: Department of Psychology, University of Copenhagen, Copenhagen, Denmark. Corresponding author: Birgitte Fagerlund. Department of Psychiatry E, Copenhagen University Hospital Bispebjerg. Bispebjerg Bakke 23. Copenhagen DK-2400 NV. Telephone: +45 35 31 24 93. Fax: +45 35 31 39 53. Email: [email protected]. Disclosure of Commercial and Non-Commercial Interests: The study was sponsored by The Danish Medical Research Council, H:S (Copenhagen Hospital Cooperation) Research Council, The University of Copenhagen Faculty of Humanities; Copenhagen University Hospital Bispebjerg, and an unrestricted grant from Janssen-Cilag A/S, and the NOVO Nordic Foundation. Acknowledgements: We thank the following for sponsoring the study: The Danish Medical Research Council, H:S (Copenhagen Hospital Cooperation) Research Council, The University of Copenhagen Faculty of Humanities; Copenhagen University Hospital Bispebjerg, and an unrestricted grant from Janssen-Cilag A/S, and the NOVO Nordic Foundation. Abstract: Studies on the effects of antipsychotics on cognitive deficits in schizophrenia mostly suggest a superior effect of atypical over typical compounds, although findings are inconsistent and effect sizes small. Several methodological issues such as heterogenous patient samples, incomparable drug doses, effects of prior medication, construct validity and retest effects on neuropsychological tasks confound most results and the comparability between studies. Consequently, the conclusion concerning effects of antipsychotics on cognition is still equivocal. Objective: The present randomised clinical trial examined the effects on cognition of comparatively low doses of a typical antipsychotic (zuclopenthixol) and an atypical antipsychotic (risperidone) in a homogenous group of drug-naïve first episode schizophrenic patients in a longitudinal setting. Methods: First-episode schizophrenic patients who had never previously been exposed to antipsychotic treatment (N=25) were randomly allocated to treatment with flexible doses of zuclopenthixol or risperidone in an open label design. Cognitive functions were examined both when patients were drug-naive, and after 13 weeks of treatment. A comprehensive neuropsychological battery was used in order to optimise construct validity, and principal components of cognitive functions were extrapolated in order to reduce Type I errors. A healthy control group was tested at baseline and after 13 weeks,
in order to examine retest effects. The cognitive domains studied were executive functions, selective attention, and reaction time. Results: The patients showed considerable cognitive deficits when drug-naïve. There were few differential effects of risperidone and zuclopenthixol on cognitive deficits, except for a differential significance respectively tendency towards improved reaction and movement times in the risperidone group, and a lack of such in the zuclopenthixol group. These differences were no longer significant after covarying for EPS and anticholinergic medication that were more prevalent in the zuclopenthixol group, and the increases after medication were comparable to retest effects in controls. Conclusion: The study underscores the importance of examining impact of factors such as clinical improvement, EPS, anticholinergic medication and retest effects in longitudinal efficacy studies. This study does not support efficacy of either risperidone or zuclopenthixol on cognitive functions in drug-naïve schizophrenic patients after 3 months of medication, because neither could be distinguished from retest effects of the healthy control group. KEY words: schizophrenia, drug-naive, first-episode, antipsychotics, cognition Introduction: The focus on cognitive deficits as targets for pharmacological intervention in the treatment of schizophrenia has increased in recent years. This is due to overwhelming evidence from numerous studies that place cognitive deficits as core deficits of the illness, independent of clinical symptoms 1-3. Furthermore, the impact of cognitive deficits on the functional outcome of patients is striking 1;2;4-6. The prognosis of patients concerning social and occupational function is poor in spite of treatments effectively controlling clinical symptoms. While difficult to quantify in general terms, several researchers suggest that even small improvements in cognitive deficits (i.e. increases of 1/2 SD) are clinically relevant 7;8, and that differences of this magnitude could have significant impact on relevant outcome measures 9. Therefore, the incentive for finding effective treatments that can improve cognitive deficits in schizophrenia is considerable. Studies 10 comparing typical and atypical antipsychotics have shown similar effectiveness on positive symptoms, differential effects favouring atypical over typical compounds regarding negative symptoms, and fewer extrapyramidal side effects (EPS) with atypical compounds11;12. Most studies and meta-analyses also favour atypical over typical compounds regarding effects on cognitive deficits 7;13-20; however, the conclusions that can be drawn from these studies are confounded by several methodological issues, the most important of which concerns incomparable doses of medications. A recent meta-analysis concluded that differential effects on cognition were only present when low dose atypicals were compared to high dose typicals, and that this superior effect of atypicals disappeared when compared to low dose typical compounds 11. In support of this, a recent study 21 using comparatively low doses of typical and atypical compounds failed to show differential effects on cognitive deficits, and several authors stress the importance of using similar, low doses in comparative studies 13;22. Besides dosage, several other methodological issues limit the conclusions that can be drawn concerning the effects of different antipsychotic compounds on cognition, such as heterogeneous patient samples, effects of prior medication, lack of control for retest-effects on cognitive measures, inadequate correlations of cognitive changes to clinical symptoms, EPS, and adjunctive anticholinergic medication. Therefore, the interpretation of findings from studies showing changes in cognitive deficits over
37

time is at issue presently, and it is unclear whether changes reflect direct drug-related improvements, clinical improvement, or effects due to repeated testing 23;24. Similarly, a lack of change over time (e.g. in patient groups treated with high doses of typical compounds) could reflect stability of cognitive deficits, or actual detrimental effects of the medication resulting in lack of a normal retest effect. This detrimental effect could be directly related to the drug or indirectly through more EPS and consequently more adjunctive anticholinergic medication, which is known to have deleterious effects on some cognitive functions 25;26. The conclusion concerning effects of antipsychotics (typical and atypical) on cognition is still equivocal 13;22. The present randomised clinical trial examined the effects of comparable, low doses of a typical compound (zuclopenthixol) or an atypical compound (risperidone) on executive functions, selective attention and reaction time in a homogenous group of drug-naïve, first-episode schizophrenic patients in a 13-week longitudinal setting. Retest effects on cognitive measures were examined in a gender- and age matched healthy control group. Methods: Patients: Patients were included from the psychiatric wards of 5 participating hospitals in the Copenhagen catchment area (background population of approximately 500,000 inhabitants). All patients fulfilled the ICD-10 F.20 criteria for schizophrenia 27. Diagnoses were made by referring psychiatrists and confirmed by the same experienced psychiatrist (Staff Specialist TM) who was traind in using SCAN-2.1 (Schedules for Clinical Assessment in Neuropsychiatry Version 2.1.; World Health Organization 1994) 28. Psychopathology ratings were likewise carried out by TM at baseline and at follow-up after 13 weeks of treatment, using the Positive and Negative Syndrome Scale (PANSS). Only antipsychotic-naïve patients admitted for treatment for the first time were included. Patients with known retardation were excluded, as were patients who were deemed in acute need of medication, or were compulsorily hospitalised. Extrapyramidal side-effects (EPS) were rated using the Extrapyramidal Symptom Rating Scale (ESRS). A total of 31 patients were included. Of these, 25 completed the study. The reasons for drop-out of patients were: change to another antipsychotic compound (n=1); compulsory hospitalisation (n=1); acute medication at baseline (n=1), patient withdrawal (n=1), and inability to participate in neuropsychological testing at baseline due to psychotic symptoms (n=2). The average age of patients was 27.3 (±5.9), ranging from 19 to 37 years. The duration of untreated psychosis ranged from 4 to 78 months (median = 14 months). The duration of untreated psychosis was very short in some instances; however, ICD-10 schizophrenia diagnoses can be made after 1 month (compared with 6 months according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) 29, with similar diagnostic validity 30), and diagnoses were all validated at the follow-up examination after 3 months. Patients were randomly allocated to treatment with comparable low flexible doses of either risperidone 2-7 mg (median = 3 mg) or zuclopenthixol 6-26 mg (median = 8 mg) in an open-label design. Zuclopenthixol is an intermediate-potency conventional antipsychopic compound with preferential affinity for dopamine D2-receptors, and a modest affinity for D1-receptors. In Europe, it is commonly used for management of acute and chronic psychotic states. Treatment responsibility remained localised to clinicians outside the project, who determined and adjusted drug doses according to clinical response. The average dose in the risperidone group was 3.6 mg (± 1.6 mg), and the average dose in the zuclopenthixol group was 9.6 mg (± 5.9 mg), which is equivalent to approximately 3-4 mg haloperidol 31. After random
allocation to treatment groups, 15 patients received risperidone, and 10 patients zuclopenthixol. (The fewer patients in the zuclopenthixol group was coincidental and not due to increased drop-out from this group after medication.) Benzodiazepines were allowed throughout the study, except on examination days. In the risperidone group, 60 % of patients received benzodiazepines at baseline and 33.3 % after 13 weeks of medication, which was not significantly different from 70 % at baseline and 40 % after 13 weeks in the zuclopenthixol group. Anticholinergics were allowed (except on examination days), but were kept to a minimum by lowering the dose of antipsychotics when EPS occurred. Eighty percent of patients in the zuclopenthixol group and 26.7 % of patients in the risperidone group received anticholinergics, a difference that was highly significant (Pearson's χ2 = 6.8; df = 1; p= 0.009). There were no differences between medication groups before allocation to treatment in terms of demographic measures (age, gender, socioeconomic status), duration of untreated psychosis, psychopathology, or cognitive deficits. Healthy Controls: Healthy controls (N=25) were recruited among hospital staff and university students, and were matched to the patients 1:1 according to gender, age, and parental education/occupationxxiv. Exclusion criteria for controls were the presence of a psychiatric diagnosis (assessed by TM using SCAN 2.0), somatic illness, psychiatric diagnoses in first-degree relatives, history of drug or alcohol abuse, presence of mental retardation or any known learning disabilities. Healthy controls participated in all the same examinations as patients at baseline. In order to examine retest effects, 12 of the healthy controls were retested on the cognitive measures after 13 weeks. The present study encompassed an extensive examination program of psychopathology and EPS ratings, cognitive tests, sensory gating (using prepulse inhibition), as well as functional magnetic resonance imaging and single photon emission computed tomography (123I-epidepride) scans. The effects of risperidone and zuclopethixol on prepulse inhibition have been presented 32, and the remaining data will be presented elsewhere. Written informed consent was obtained from all subjects prior to inclusion into the study. The study was approved by the scientific ethics committee for Copenhagen and Frederiksberg. Cognitive functions: Executive functions and selective attention were examined using tests from the computerised Cambridge Neuropsychological Test Automated Battery (CANTAB) 33;34., Wisconsin Card Sorting Test (WCST) 35 as well as verbal fluency, figural fluency, and Trail Making tests A & B 36. Tests of reaction and movement time were assessed using CANTAB. Premorbid intelligence was estimated using the Danish Adult Reading Test (DART); the Danish version of the New Adult Reading Test (NART) 37. Cognitive functions were tested by the same examiner (BF) at baseline and retest. The comprehensive neuropsychological test battery was used in order to optimise construct validity 38, and principal components of cognitive functions were extrapolated in order to minimize Type I errors. Cognitive tests: The original 128 card version of the Wisconsin Card Sorting Test (WCST) was used 35. The WCST assesses the ability to make and maintain hypotheses by sorting cards according to the categories colour, shape, or number, and assesses attentional set shifting ability by requiring subjects to use feedback to shift hypotheses when relevant (i.e. when the correct sorting category changes). Outcome measures are number of categories achieved
xxiv Education/occupation was recorded from the parent with the highest rating, either according to education or occupation.
38

(maximum score: 6); total number of errors; perseverative errors; unique errors; other errors; total number of cards used. The CANTAB Intra-Extra Dimensional set shifting task (IED) consists of 9 different stages of increasing difficulty that test the ability to utilise feedback to discriminate between figures, as well as to make, maintain, and shift hypotheses within and between categories. The IED assesses attentional set shifting similarly to the WCST. Outcome measures: number of stages completed; total errors (adjusted for stages not completed); errors made at the extradimensional set shifting stage; number of trials (adjusted for stages not completed). The CANTAB Stockings of Cambridge (SOC) presents two arrays of coloured balls, where subjects are required to move the balls at the bottom of the screen to match the array presented at the top of the screen. The SOC assesses planning ability, strategy formation and execution similarly to the Tower of London. Outcome measures are: number of problems solved with minimum number of moves (i.e. most efficiently); mean number of moves used to solve problems (averaged from 2, 3, 4, and 5 move-problems); initial thinking times (i.e. planning time, from the problem is presented on the screen until the subject touches the screen); subsequent thinking times (i.e. time from first touching the screen until the problem is solved; controlled for motor times). The Trail Making test A assesses visuospatial scanning and psychomotor speed by subjects combining circles with ascending numbers. In addition to these functions, the Trail Making test B also assesses attentional set shifting ability by subjects combining circles, continuously alternating between ascending numbers and letters in alphabetical order. Outcome measures are: time to complete Trail Making A; time to complete Trail Making B; as well as Trail Making B minus Trail Making A. Verbal phonological fluency was assessed by subjects generating as many words as possible in 60 seconds beginning with the letter “S”. Verbal semantic fluency was assessed by subjects generating words from the category “animals” in 60 seconds. Figural fluency was assessed using Regard’s Figural Fluency Task 39, in which subjects draw as many figures as possible in 3 minutes, by combining two or more of 5 dots in different combinations. Outcome measures are number of words with the letter S; number of animals; and number of figures. The CANTAB Rapid Visual Information Processing Test (RVP) is a continuous performance test, in which different numbers are continuously presented in random order on a computer screen, for 7 minutes. The target consists of three numbers (3-5-7) that subjects have to continuously attend and respond to within a series of other numbers. The RVP assesses selective attention and vigilance with a small working memory component. The outcome measures are signal detection; number of hits; and number of misses. The CANTAB Reaction and Movement Time Test presents yellow dots on a touchscreen, to which subjects respond by releasing a press pad and touching the dot on the screen as fast as possible. The reaction time is the time taken to release the press pad in response to the stimulus, while the movement time is the time taken to touch the stimulus on the screen after the press pad has been released. Simple Reaction Time and Simple Movement Time is when there is only one location on the screen, in which the stimulus can appear, while Choice Reaction Time and Choice Movement Time is when the stimulus can appear in any of 5 locations.
Statistical Analysis: Data were analysed using Statistical Package for the Social Sciences (SPSS), version 11.0. All analyses used two-tailed levels of significance. Missing data was extrapolated (using substitution of group mean) for one patient on DART. Results from the reaction time and movement time tasks did not fit a normal distribution and data were log transformed to reduce skew. Parametric statistics were used for all analyses. Results were standardised to z-scores, using the healthy control group as reference point with an average of 0 and a SD of 1. The numerous neuropsychological measures were reduced using principal component analysis as extraction method into 1 or 2 factors per testxxv. Nominal data were analysed using Pearson's χ2. Effects of medication were examined using a repeated-measures ANCOVA, with the subtracted difference between the baseline score and retest score as the dependent measure. The between-subject variable was medicine group (risperidone, zuclopenthixol, none (healthy controls)). Baseline scores were included as covariates, in order to control for group differences at baseline. In secondary post-hoc analyses, changes in psychopathology (PANSS ratings), side effects (ESRS ratings), and anticholinergic medication were separately assessed as covariates. Results: Socioeconomic status (SES): Socioeconomic status (SES) was calculated based on a combination of parental education/occupation (6 groups) and household income (3 groups) according to criteria from the Danish Institute of Clinical Epidemiology, and resulted in 3 socioeconomic groups (SES). Parental SES is considered a reliable indicator of potential SES of offspring and was used instead of patient SES, which would underestimate the potential socioeconomic level, since the illness has profound impact on education, vocation and income because of the common timing of illness onset during early adulthood. There were no significant differences between the parental education/occupation of patients and controls, but there was a significantly lower level of income in the patient group (χ2= 8.30; df=2; p= 0.02), and consequently a lower combined SES (χ2= 7.1; df=2; p= 0.03). The socio-demographic data (parental education/occupation, income, and SES) of patients and controls are shown in Table 1. Table 1: Demographical data: Parental education/occupation, income, and socio-economic status
N Parental Education/ Occupation
Patients Controls Pearson's χ2 Df P (2-sided)
Academic 6 9 3.16 5 0.676 Bachelor 10 8 Expert 2 4 Skilled 4 2 Non-skilled 2 2 Non-skilled, Unemployed 1 -
N Parental Income Patients Controls Pearson's χ2 Df P (2-sided)
High 3 10 8.30 2 0.016 Middle 15 14 Low 7 1
N SES Patients Controls Pearson's χ2 Df P (2-sided)
A (High) 3 9 7.12 2 0.028 B (Middle) 18 16 C (Low) 4 -
xxv Principal component analysis was carried out on all subjects participating in a larger study which, in addition to these 25 adult schizophrenic patients and 25 healthy controls, included 40 schizophrenic and/or psychotic adolescents and 40 age-matched controls (Total subject N=130).
39
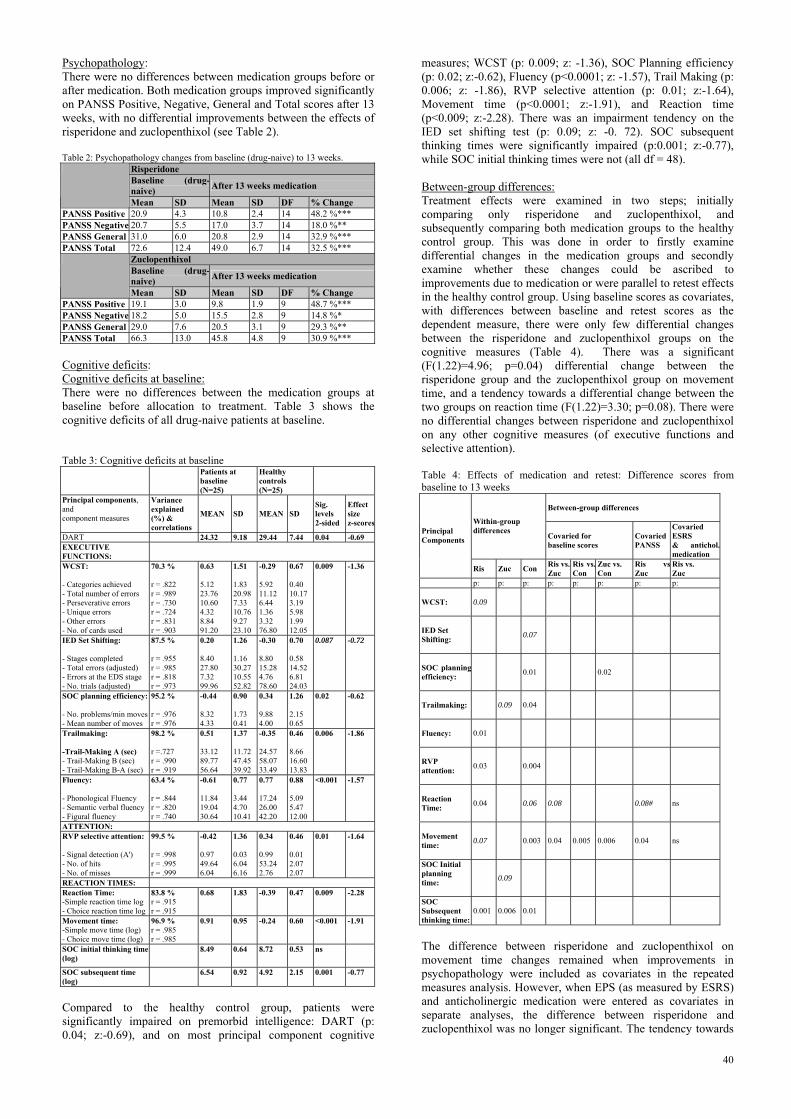
Psychopathology: There were no differences between medication groups before or after medication. Both medication groups improved significantly on PANSS Positive, Negative, General and Total scores after 13 weeks, with no differential improvements between the effects of risperidone and zuclopenthixol (see Table 2). Table 2: Psychopathology changes from baseline (drug-naive) to 13 weeks.
Risperidone Baseline (drug-naive) After 13 weeks medication
Mean SD Mean SD DF % Change PANSS Positive 20.9 4.3 10.8 2.4 14 48.2 %*** PANSS Negative 20.7 5.5 17.0 3.7 14 18.0 %** PANSS General 31.0 6.0 20.8 2.9 14 32.9 %*** PANSS Total 72.6 12.4 49.0 6.7 14 32.5 %***
Zuclopenthixol Baseline (drug-naive) After 13 weeks medication
Mean SD Mean SD DF % Change PANSS Positive 19.1 3.0 9.8 1.9 9 48.7 %*** PANSS Negative 18.2 5.0 15.5 2.8 9 14.8 %* PANSS General 29.0 7.6 20.5 3.1 9 29.3 %** PANSS Total 66.3 13.0 45.8 4.8 9 30.9 %*** Cognitive deficits: Cognitive deficits at baseline: There were no differences between the medication groups at baseline before allocation to treatment. Table 3 shows the cognitive deficits of all drug-naive patients at baseline. Table 3: Cognitive deficits at baseline Patients at
baseline (N=25)
Healthy controls (N=25)
Principal components, and component measures
Variance explained (%) & correlations
MEAN SD MEAN SD Sig. levels 2-sided
Effect size z-scores
DART 24.32 9.18 29.44 7.44 0.04 -0.69 EXECUTIVE FUNCTIONS:
WCST: - Categories achieved - Total number of errors - Perseverative errors - Unique errors - Other errors - No. of cards used
70.3 % r = .822 r = .989 r = .730 r = .724 r = .831 r = .903
0.63 5.12 23.76 10.60 4.32 8.84 91.20
1.51 1.83 20.98 7.33 10.76 9.27 23.10
-0.29 5.92 11.12 6.44 1.36 3.32 76.80
0.67 0.40 10.17 3.19 5.98 1.99 12.05
0.009
-1.36
IED Set Shifting: - Stages completed - Total errors (adjusted) - Errors at the EDS stage - No. trials (adjusted)
87.5 % r = .955 r = .985 r = .818 r = .973
0.20 8.40 27.80 7.32 99.96
1.26 1.16 30.27 10.55 52.82
-0.30 8.80 15.28 4.76 78.60
0.70 0.58 14.52 6.81 24.03
0.087
-0.72
SOC planning efficiency: - No. problems/min moves - Mean number of moves
95.2 % r = .976 r = .976
-0.44 8.32 4.33
0.90 1.73 0.41
0.34 9.88 4.00
1.26 2.15 0.65
0.02
-0.62
Trailmaking: -Trail-Making A (sec) - Trail-Making B (sec) - Trail-Making B-A (sec)
98.2 % r =.727 r = .990 r = .919
0.51 33.12 89.77 56.64
1.37 11.72 47.45 39.92
-0.35 24.57 58.07 33.49
0.46 8.66 16.60 13.83
0.006
-1.86
Fluency: - Phonological Fluency - Semantic verbal fluency - Figural fluency
63.4 % r = .844 r = .820 r = .740
-0.61 11.84 19.04 30.64
0.77 3.44 4.70 10.41
0.77 17.24 26.00 42.20
0.88 5.09 5.47 12.00
<0.001
-1.57
ATTENTION: RVP selective attention: - Signal detection (A') - No. of hits - No. of misses
99.5 % r = .998 r = .995 r = .999
-0.42 0.97 49.64 6.04
1.36 0.03 6.04 6.16
0.34 0.99 53.24 2.76
0.46 0.01 2.07 2.07
0.01
-1.64
REACTION TIMES: Reaction Time: -Simple reaction time log - Choice reaction time log
83.8 % r = .915 r = .915
0.68
1.83
-0.39
0.47
0.009
-2.28
Movement time: -Simple move time (log) - Choice move time (log)
96.9 % r = .985 r = .985
0.91
0.95
-0.24
0.60
<0.001
-1.91
SOC initial thinking time (log)
8.49 0.64 8.72 0.53 ns
SOC subsequent time (log)
6.54 0.92 4.92 2.15 0.001 -0.77
Compared to the healthy control group, patients were significantly impaired on premorbid intelligence: DART (p: 0.04; z:-0.69), and on most principal component cognitive
measures; WCST (p: 0.009; z: -1.36), SOC Planning efficiency (p: 0.02; z:-0.62), Fluency (p<0.0001; z: -1.57), Trail Making (p: 0.006; z: -1.86), RVP selective attention (p: 0.01; z:-1.64), Movement time (p<0.0001; z:-1.91), and Reaction time (p<0.009; z:-2.28). There was an impairment tendency on the IED set shifting test (p: 0.09; z: -0. 72). SOC subsequent thinking times were significantly impaired (p:0.001; z:-0.77), while SOC initial thinking times were not (all df = 48). Between-group differences: Treatment effects were examined in two steps; initially comparing only risperidone and zuclopenthixol, and subsequently comparing both medication groups to the healthy control group. This was done in order to firstly examine differential changes in the medication groups and secondly examine whether these changes could be ascribed to improvements due to medication or were parallel to retest effects in the healthy control group. Using baseline scores as covariates, with differences between baseline and retest scores as the dependent measure, there were only few differential changes between the risperidone and zuclopenthixol groups on the cognitive measures (Table 4). There was a significant (F(1.22)=4.96; p=0.04) differential change between the risperidone group and the zuclopenthixol group on movement time, and a tendency towards a differential change between the two groups on reaction time (F(1.22)=3.30; p=0.08). There were no differential changes between risperidone and zuclopenthixol on any other cognitive measures (of executive functions and selective attention). Table 4: Effects of medication and retest: Difference scores from baseline to 13 weeks
Between-group differences Within-group
differences Covaried for baseline scores
Covaried PANSS
Covaried ESRS & antichol.medication
Principal Components
Ris Zuc Con Ris vs. Zuc
Ris vs.Con
Zuc vs. Con
Ris vsZuc
Ris vs. Zuc
p: p: p: p: p: p: p: p: WCST:
0.09
IED Set Shifting:
0.07
SOC planningefficiency:
0.01 0.02
Trailmaking:
0.09 0.04
Fluency:
0.01
RVP attention:
0.03 0.004
Reaction Time:
0.04 0.06 0.08 0.08# ns
Movement time:
0.07 0.003 0.04 0.005 0.006 0.04 ns
SOC Initial planning time:
0.09
SOC Subsequent thinking time:
0.001 0.006 0.01
The difference between risperidone and zuclopenthixol on movement time changes remained when improvements in psychopathology were included as covariates in the repeated measures analysis. However, when EPS (as measured by ESRS) and anticholinergic medication were entered as covariates in separate analyses, the difference between risperidone and zuclopenthixol was no longer significant. The tendency towards
40

differential changes in reaction times between the medication groups remained when covaried for improvements in psychopathology scores regarding negative, general and total PANSS scores, but disappeared when covaried for improvements in positive PANSS scores (Table 4). In separate analyses, ESRS ratings and anticholinergic medication each covaried out the tendency towards differential changes between risperidone and zuclopenthixol on meaction times. Within-group differences: The risperidone group showed significant within-group changes on Reaction times (p=0.04), Fluency (p: 0.01), RVP selective attention (p: 0.03), and SOC subsequent thinking latencies (p: 0.001), and tendencies to changes on WCST (p: 0.09), and Movement times (p: 0.07) (all df = 14). The zuclopenthixol group showed significant within-group changes on one measure only: SOC subsequent thinking latencies (p: 0.006), and a tendency towards improvement on initial thinking times (p=0.09) and Trail Making (p: 0.09) (all df = 9). Retest-effects: The healthy control group showed significant retest-effects on several measures. Significant within-group changes were seen on Trail Making (p: 0.04), RVP selective attention (p: 0.004), Movement times (p: 0.003), SOC planning efficiency (p: 0.01), and SOC subsequent thinking latencies (p: 0.01), and tendencies towards improvements on Reaction times (p: 0.06) and IED set shifting (p: 0.07) (all df = 11). In most cases the changes in both medication groups were parallel to the retest-effects in the healthy control. However, the healthy control group showed a significant (p: 0.004) improvement on Movement times that was significantly different from the changes in both the risperidone group (p: 0.005) and the zuclopenthixol group (p: 0.006). While the risperidone group showed a tendency towards improvement on Movement times, the change was not as large as the retest effect in the healthy control group. Similarly, the zuclopenthixol group showed a lack of retest effect on the Movement times. In addition, the significant retest effect of the healthy control group on SOC planning efficiency was significantly different (F(1.19)=6.42; p: 0.02) from the lack of change in the zuclopenthixol group, which can be interpreted as a lack of retest effect in the zuclopenthixol group. Discussion: Effects of medication: The risperidone and zuclopenthixol treated patients showed few differential changes after medication, with no differences on changes in psychopathology or most cognitive measures. The exceptions were Movement times and Reaction times, on which the zuclopenthixol group showed a lack of change over time on both measures. This was significantly different from the tendency of the risperidone group to improve over time on Movement time, and was different at trend level from the significant within group improvement of the risperidone group on Reaction time. The differential improvement tendency in Reaction times in the risperidone group disappeared when covaried for improvements in positive PANSS scores which suggests that the improved reaction times in this group may be related to clinical improvement of positive symptoms. Covarying for improvements in psychopathology did not affect the differential change of risperidone on Movement times. However, when EPS were entered as covariate in separate analyses, the differential change of risperidone over zuclopenthixol on both Reaction times and Movement times disappeared. This indicates that the lack of improvement in Reaction times and Movement times in the zuclopenthixol group may be related to the significantly (p:
0.02) more prevalent EPS in this group. However, these secondary post-hoc analyses should be interpreted with caution, because the risk of type 2 errors is high due to the small sample size. Retest Effects: The changes in both medication groups were parallel to the changes in the healthy control group on most measures. Both the risperidone group and zuclopenthixol group showed significantly less retest effects than the healthy control group on Movement times. While the risperidone group had a tendency towards improvement that was significantly different from the lack of change in the zuclopenthixol group, this change did not reach the retest effect of the healthy control group. In other words, the healthy control group showed larger improvements in Movement time than either of the medication groups, but the risperidone group showed an improvement in Movement time which was different from the lack of change in the zuclopenthixol group. The healthy control group showed only a tendency towards improvements on Reaction times, while the risperidone group improved significantly on Reaction times, however, after covarying for the large differences in baseline scores, there were no differential changes between any of the groups. The zuclopenthixol group showed a lack of retest effect on SOC planning efficiency compared to the improvement in the healthy control group. The zuclopenthixol group showed within-group changes on only few measures. While the risperidone group showed significant or tendencies towards within-group changes on several measures, these changes were not significantly different from the changes in the zuclopenthixol group or the changes in the healthy control group. This raises the question whether within-group changes in medication groups should be interpreted as effects of medication or mere retest effects. Whether retest effects in schizophrenia patients are similar to that of healthy controls is unclear. While few studies have found less retest effects in patients than controls 40, most have found similar retest effects over both short and long time intervals 38;41;42. In a longitudinal design, Heaton et al. 38 found similar retest effects in schizophrenic patients as healthy controls, interestingly regardless of level of psychopathological symptoms and clinical state. Covert, procedural learning seems to be one of the few neuropsychological domains in which schizophrenic patients are not particularly impaired 43. Conversely, the interpretation of a lack of effect over time as stability of deficits or detrimental effects reflected in a lack of normal retest effect is dependent on the examination of retest effects. Whether changes in patient groups (e.g. on an executive task) represent practice effects (intact learning), or improved executive functions (and impaired learning) cannot be distinguished in lieu of a placebo-controlled patient group. The inclusion of unmedicated patient groups in longitudinal studies of medication effects on cognition would be theoretically preferable, but ethically problematic. Therefore, examining retest-effects in a matched, healthy control group as a minimum is necessary as standard of reference in studies using repeated cognitive testing. However, in the present study, both medication groups showed less retest effects than controls on certain measures. This indicated that schizophrenic patients may show less retest effects than healthy controls, or that antipsychotic medication (perhaps typical compounds in particular) may interfere with learning and retest effects. Theoretical Implications: The conclusions concerning the efficacy of antipsychotics on cognitive deficits are still at issue 23;24. That low doses of atypicals are superior to high doses of typicals has been well established in several studies and reviews 7;13-16;18-20;44. Recent studies have found similar effects of typicals and atypicals, when comparably low doses are used 21. Because of different receptor profiles and methods of action of various atypical compounds, it
41

is possible that different compounds have differential effects on cognitive measures. Few comparative studies have been done, and they yield conflicting results. Some studies support differential effects of different atypicals 17;19 while another tentatively supports slight differential effects 7. However; for the time being, there is insufficient evidence to substantiate different profiles of effect. Findings from a recent large-scale study including almost 400 patients did not support differential effects of low doses of risperidone and olanzapine on cognitive functions 8.The impact of retest effects on these changes over time has not been addressed in most studies. The inconclusive data on the efficacy of antipsychotics on cognitive deficits appears to encompass at least some areas of early information processing as well. The superior efficacy of atypicals over typicals on deficits of prepulse inhibition of the gating response has recently been challenged by negative findings in longitudinal studies from Duncan 45 and our own group 32. Whether these deficits should be considered as stable vulnerability indicators is unclear, since other treatment strategies may impact on these functions. Clinical implications: In terms of the clinical relevance of the present results, the zuclopenthixol group showed a lack of change over time on most measures, and had more EPS and needed more adjunctive anticholinergic medication than the risperidone group. Strengths of the study: The inclusion of only first-episode drug-naïve patients in the study makes it possible to delineate the profile of cognitive deficits early in the disease process, and assess the impact of medication, where the possibly confounding factor of previous medication is not present. Only few previous studies have examined effects of medication in drug-naïve patients 46. The study was a randomised clinical trial, where medication effects were tested in a longitudinal setting that was naturalistic. After allocation to treatment groups, any treatment changes were decided by psychiatrists outside of the project, based on clinical response. The doses used were comparable, low doses in both medication groups. Retest-effects were examined in an age- and gender matched, healthy control group. Limitations of the study: The 25 patients included in this study constitute a small sample size, which increases the risk of both type 1 and type 2 errors. Especially the inability to reject the null-hypothesis in this sample may be compounded by the small sample size, and therefore the low power. Subsequent studies with more patients will help strengthen the results. Furthermore, 13 weeks may not be sufficient time to observe differential improvements between the compounds that may potentially occur later. In a 2-year longitudinal design, Green et al. 21 found that the effects of Haloperidol were observed more quickly than the effects of risperidone, but that the beneficial effects of risperidone gained momentum and surpassed Haloperidol after 12 months. The present study was open-label because a double-blind design was not a practically viable option, and investigators were not blind to subject assignment. The examination of retest effects using a healthy control group is necessary to establish the expected level of retest effects in patients; however, the conclusions that can be drawn are limited in lieu of an unmedicated schizophrenic control group. A final note on the results is that there may be a selection bias in the patients included in this study. The examination program was very comprehensive, and besides participating in psychopathology ratings and neuropsychological tests, patients were tested with PPI and scanned with SPECT and fMRI both before and after medication. Therefore, the patients included were relatively motivated and could manage to participate in all parts of the study, and were neither deemed in need of acute medication nor compulsorily hospitalised. However, the patients included fulfilled the study criteria for ICD-10 F.20 schizophrenia diagnosis and had considerable cognitive deficits,
and as such were not necessarily a biased representation of drug-naïve, first episode patients. Conclusion: The results from the present study do not support the effectiveness of antipsychotics (neither typical nor atypical) on cognitive deficits, but suggest that while the risperidone group shows mainly normal retest effects, the zuclopenthixol group may show a lack of retest effects on certain measures, perhaps due to more prevalent EPS, effects of adjunctive anticholinergic medication, or deficits in learning. The results indicate that retest effects on cognitive tests is an important issue to consider in studies examining the effects of medication on cognition in a longitudinal setting. Distinguishing cognitive changes (improvements, no change or deleterious effects) from retest effects is not a trivial issue, but a methodological necessity in clinical trials using repeated testing. The results support careful consideration of whether changes over time are due to direct effects of the antipsychotic compounds or indirect effects of e.g. clinical improvements, EPS, or anticholinergic medication. However, the conclusions that can be drawn are limited by the small sample size and the time interval of 3 months, which may be too short to detect potential differential effects of different antipsychotic compounds. Reference List: 1. Bilder RM, Goldman RS, Robinson D, Reiter G, Bell L, Bates
JA, Pappadopulos E, Willson DF, Alvir JM, Woerner MG, Geisler S, Kane JM, Lieberman JA. Neuropsychology of first-episode schizophrenia: initial characterization and clinical correlates. Am J Psychiatry. 2000;157:549-59.
2. Green MF, Nuechterlein KH. Should schizophrenia be treated as a neurocognitive disorder? Schizophr Bull. 1999;25:309-319.
3. Green MF, Braff DL. Translating the basic and clinical cognitive neuroscience of schizophrenia to drug development and clinical trials of antipsychotic medications. Biol Psychiatry. 2001;49:374-384.
4. Green MF, Kern RS, Braff DL, Mintz J. Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the "right stuff"? Schizophr Bull. 2000;26:119-136.
5. Velligan DI, Mahurin RK, Diamond PL, Hazelton BC, Eckert SL, Miller AL. The functional significance of symtomatology and cognitive function in schizohrenia. Schizophrenia Research. 1997;25:21-31.
6. Velligan DI, Miller AL. Cognitive dysfunction in schizophrenia and its importance to outcome: the place of atypical antipsychotics in treatment. J Clin Psychiatry. 1999;60 Suppl 23:25-8.
7. Bilder RM, Goldman RS, Volavka J, Czobor P, Hoptman M, Sheitman B, Lindenmayer JP, Citrome L, McEvoy J, Kunz M, Chakos M, Cooper TB, Horowitz TL, Lieberman JA. Neurocognitive effects of clozapine, olanzapine, risperidone, and haloperidol in patients with chronic schizophrenia or schizoaffective disorder. Am J Psychiatry. 2002;159:1018-1028.
8. Harvey PD, Green MF, McGurk SR, Meltzer HY. Changes in cognitive functioning with risperidone and olanzapine treatment: a large-scale, double-blind, randomized study. Psychopharmacology (Berl). 2003;169:404-411.
9. Lysaker P, Bell M, Beam-Goulet J. Wisconsin card sorting test and work performance in schizophrenia. Psychiatry Res. 1995;56:45-51.
10. Bollini P, Pampallona S, Orza MJ, Adams ME, Chalmers TC. Antipsychotic drugs: is more worse? A meta-analysis of the published randomized control trials. Psychol Med. 1994;24:307-16.
11. Geddes J, Freemantle N, Harrison P, Bebbington P. Atypical antipsychotics in the treatment of schizophrenia: systematic overview and meta-regression analysis. Bmj. 2000;321:1371-6.
12. Leucht S, Pitschel-Walz G, Abraham D, Kissling W. Efficacy and extrapyramidal side-effects of the new antipsychotics olanzapine, quetiapine, risperidone, and sertindole compared to conventional antipsychotics and placebo. A meta-analysis of randomized controlled trials. Schizophr Res. 1999;35:51-68.
13. Harvey PD, Keefe RS. Studies of cognitive change in patients with schizophrenia following novel antipsychotic treatment. Am J Psychiatry. 2001;158:176-184.
42
14. Keefe RS, Silva SG, Perkins DO, Lieberman JA. The effects of atypical antipsychotic drugs on neurocognitive impairment in schizophrenia: a review and meta-analysis. Schizophr Bull. 1999;25:201-22.
15. Kern RS, Green MF, Marshall BD, Jr., Wirshing WC, Wirshing D, McGurk S, Marder SR, Mintz J. Risperidone vs. haloperidol on reaction time, manual dexterity, and motor learning in treatment-resistant schizophrenia patients. Biol Psychiatry. 1998;44:726-732.
16. Kern RS, Green MF, Marshall BD, Jr., Wirshing WC, Wirshing D, McGurk SR, Marder SR, Mintz J. Risperidone versus haloperidol on secondary memory: can newer medications aid learning? Schizophr Bull. 1999;25:223-232.
17. Meltzer HY, McGurk SR. The effects of clozapine, risperidone, and olanzapine on cognitive function in schizophrenia. Schizophr Bull. 1999;25:233-255.
18. Purdon SE. Cognitive improvement in schizophrenia with novel antipsychotic medications. Schizophr Res. 1999;35 Suppl:S51-S60.
19. Purdon SE, Jones BD, Stip E, Labelle A, Addington D, David SR, Breier A, Tollefson GD. Neuropsychological change in early phase schizophrenia during 12 months of treatment with olanzapine, risperidone, or haloperidol. The Canadian Collaborative Group for research in schizophrenia. Arch Gen Psychiatry. 2000;57:249-258.
20. Velligan DI, Newcomer J, Pultz J, Csernansky J, Hoff AL, Mahurin R, Miller AL. Does cognitive function improve with quetiapine in comparison to haloperidol? Schizophr Res. 2002;53:239-48.
21. Green MF, Marder SR, Glynn SM, McGurk SR, Wirshing WC, Wirshing DA, Liberman RP, Mintz J. The neurocognitive effects of low-dose haloperidol: a two-year comparison with risperidone. Biol Psychiatry. 2002;51:972-978.
22. Carpenter WT, Gold JM. Another view of therapy for cognition in schizophrenia. Biol Psychiatry. 2002;51:969-71.
23. Carpenter WT, Gold JM. Reply. Biol Psychiatry. 2003;53:267-8.
24. Meltzer HY, Sumiyoshi T. Atypical antipsychotic drugs improve cognition in schizophrenia. Biol Psychiatry. 2003;53:265-7.
25. Spohn HE, Strauss ME. Relation of neuroleptic and anticholinergic medication to cognitive functions in schizophrenia. J Abnorm Psychol. 1989;98:367-80.
26. Sweeney JA, Keilp JG, Haas GL, Hill J, Weiden PJ. Relationships between medication treatments and neuropsychological test performance in schizophrenia. Psychiatry Res. 1991;37:297-308.
27. The ICD-10 classification of mental and behavioral disorders. Diagnostic criteria for research. World Health Organization; 1993.
28. Schedules for clinical assessment in neuropsychiatry. World Health Organization; 1994.
29. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). 4 ed. Washington, DC: American Psychiatric Association; 1994.
30. Amin S, Singh SP, Brewin J, Jones PB, Medley I, Harrison G. Diagnostic stability of first-episode psychosis. Comparison of ICD-10 and DSM-III-R systems. Br J Psychiatry. 1999;175:537-543.
31. Glenthoj BY, Gerlach J, Licht R, Gulmann N, Jorgensen OS. Guidelines for treatment with antipsychotics. (Danish Psychiatric Association. The Committee on Biological Treatments in Psychiatry) (in danish). Journal of the Danish Medical Association. 1998;Klaringsrapport nr. 5..
32. Mackeprang T, Kristiansen KT, Glenthoj BY. Effects of antipsychotics on prepulse inhibition of the startle response in drug-naive schizophrenic patients. Biol Psychiatry. 2002;52:863-873.
33. Lowe C, Rabbitt P. Test/re-test reliability of the CANTAB and ISPOCD neuropsychological batteries: theoretical and practical issues. Cambridge Neuropsychological Test Automated Battery. International Study of Post-Operative Cognitive Dysfunction. Neuropsychologia. 1998;36:915-23.
34. Sahakian BJ, Owen AM. Computerized assessment in neuropsychiatry using CANTAB: discussion paper. J R Soc Med. 1992;85:399-402.
35. Milner B. Effects of different brain lesions on card sorting. Archives of neurology. 1963;9:90-100.
36. Reitan RM, Wolfson D. The Halstead-Reitan Neuropsychological Test Battery: Theory and Clinical Interpretation. Tucson, AZ.: Neuropsychology Press; 1993.
37. Nelson HE, O'Connell A. Dementia: the estimation of premorbid intelligence levels using the New Adult Reading Test 1. Cortex. 1978;14:234-244.
38. Heaton RK, Gladsjo JA, Palmer BW, Kuck J, Marcotte TD, Jeste DV. Stability and course of neuropsychological deficits in schizophrenia. Arch Gen Psychiatry. 2001;58:24-32.
39. Regard M, Strauss E, Knapp P. Children's production on verbal and non-verbal fluency tasks. Percept Mot Skills. 1982;55:839-844.
40. Goldstein G, Watson JR. Test-retest reliabiilty of the Halstead-Reitan battery and the WAIS in a neuropsychiatric population. Clinical Neuropsychologist. 1989;3:265-272.
41. Boone DE. Reliability of the WAIS-R with psychiatric inpatients. J Clin Psychol. 1992;48:72-6.
42. Weber B. RBANS has reasonable test-retest reliability in schizophrenia. Evid Based Ment Health. 2003;6:22.
43. Danion JM, Meulemans T, Kauffmann-Muller F, Vermaat H. Intact implicit learning in schizophrenia. Am J Psychiatry. 2001;158:944-8.
44. Meltzer HY, Park S, Kessler R. Cognition, schizophrenia, and the atypical antipsychotic drugs. Proc Natl Acad Sci U S A. 1999;96:13591-13593.
45. Duncan EJ, Szilagyi S, Efferen TR, Schwartz MP, Parwani A, Chakravorty S, Madonick SH, Kunzova A, Harmon JW, Angrist B, Gonzenbach S, Rotrosen JP. Effect of treatment status on prepulse inhibition of acoustic startle in schizophrenia. Psychopharmacology (Berl). 2003;167:63-71.
46. Hong KS, Kim JG, Koh HJ, Koo MS, Kim JH, Lee D, Kim E. Effects of risperidone on information processing and attention in first-episode schizophrenia. Schizophr Res. 2002;53:7-16.
43



























![[Birgitte Rahbaek] Democratisation in the Middle E(Bokos-Z1)](https://img.pdfslide.us/doc/110x75/563db831550346aa9a91654b/birgitte-rahbaek-democratisation-in-the-middle-ebokos-z1.jpg)
