Embed Size (px)
Citation preview

519Immunotherapy (2014) 6(5), 519–531 ISSN 1750-743X
part of
Drug Evaluation
10.2217/IMT.14.22
HER2 peptide nelipepimut-S (E75) vaccine (NeuVax™) in breast cancer patients at risk for
Nelipepimut-S (formerly known as E75) is an immunogenic peptide from the HER2 protein that is highly expressed in breast cancer. The NeuVax™ (Galena, OR, USA) vaccine, nelipepimut-S plus granulocyte–macrophage colony-stimulating factor, is designed for the prevention of clinical recurrences in high risk, disease-free breast cancer patients. Although cancer vaccines such as NeuVax represent promising approaches to cancer immunotherapy, much remains to be elucidated regarding their mechanisms of action: particularly given that multiple cancer vaccine trials have failed to demonstrate a correlation between immunologic data and clinical outcome. Here, we briefly discuss our clinical trial experience with NeuVax focusing on immunologic response data and its implication on how the immune system may be affected by this peptide vaccine. Most importantly, we demonstrate the potential capability of certain immunologic assays to predict clinical benefit in our trials.
Keywords:
BackgroundThe HER2/neu proto-oncogene, a member of the EGF receptor family, is expressed in a variety of malignancies including breast cancer. Historically, HER2 overexpression (immunohistochemistry [IHC] 3+ and/or FISH >2.2]) has been associated with a poor prognosis. Given that the overexpression of HER2 is associated with more aggressive subtypes of breast cancer and other adeno-carcinomas, HER2 is an attractive immuno-logic target for both cell-mediated immunity, including cytotoxic T cells, and antibody-mediated immunotherapy approaches [1,2]. Currently, in addition to traditional thera-pies of surgery, chemotherapy, radiation and endocrine therapy, a small percentage of breast cancer patients benefit from trastu-zumab and other HER2-targeted therapies including pertuzumab [3,4] and trastuzumab emtasine [5]. Trastuzumab, a mono clonal antibody targeting the highest level of HER2-overexpressing tumor cells, provides a proven disease-free survival (DFS) benefit to high-risk node- negative and node-positive
breast cancer patients decreasing recurrence rates by approximately 50% [6–8].
Recent data show that patients with a HER2-overexpressing tumor treated with trastuzumab have a much better prognosis than HER2 low-to-intermediate (IHC 1–2+) patients not treated with trastuzumab [9]. How-ever, trastuzumab is limited in that it has only been shown to be efficacious in the 20–30% of patients with tumors of the highest level of HER2 expression (IHC 3+) [10]. HER2 low-to-intermediate patients represent over 50% of breast cancer patients [10,11]. Thus, there exists a need to develop other adjuvant approaches to treat this HER2 low-to- intermediate-expressing population while avoiding the tox-icities associated with trastuzumab and other HER2-targeted therapies.
An ideal immunologic therapy would induce immunologic memory, making clinical response long-acting and sustainable. Trastu-zumab and other monoclonal antibodies are limited by passive mechanism of actions such as ADCC. Without full activation of the immune system, there is little to no immunologic
Erika J Schneble1, John S Berry1, Francois A Trappey1, Guy T Clifton1, Sathibalan Ponniah2, Elizabeth Mittendorf3 & George E Peoples*,1
1
3
The HER2 peptide nelipepimut-S (E75) vaccine (NeuVax™) in breast cancer patients at risk for recurrence: correlation of immunologic data with clinical response
For reprint orders, please contact: [email protected]

520 Immunotherapy (2014) 6(5) future science group
Drug Evaluation Schneble, Berry, Trappey et al.
Table 1. Selected preclinical studies of the ability for nelipepimut-S to stimulate cytotoxic T lymphocytes to lyse HER2-expressing targets.
Study (year) Study design Immunologic response/study conclusion Ref.
Fisk et al. (1995) Fresh cell lines from ovarian cancer pts
First described nelipepimut-S (KIFGSLAFL, HER2/neu, p369-377)Identified common immunogenic epitopes of HER2 that were recognized by isolated CD3+CD4+CD8+ ovarian-specific CTL linesNelipepimut-S epitope from tumor-associated lymphocytes from HLA-A2+ tumor-associated lymphocytes dominantly recognized by all CTL lines tested
[13]
Lustgarten et al. (1997)
In vitro/in vivo animal model Nelipepimut-S capable of stimulating potent CTL response that lysed tumor cells in vivoNelipepimut-S dose-dependent HER2 tumor-killing effect by nelipepimut-S-specific CTL in this mouse model
[28]
Disis et al. (1998) In vitro/in vivo animal model; nelipeminut-S-containing HER2-derived peptides plus GM-CSF or IFA
No dose-limiting toxicity on necropsyNo evidence of autoimmunitySignificant T-cell response detected
[29]
Anderson et al. (2000)
Ten healthy human donors Nelipepimut-S-specific cytolytic activity in healthy donors when presented on autologous DCs elicited in 50% of healthy donors
[30]
memory. Cancer vaccines are a form of active immu-notherapy where the body’s own immune system is uti-lized to target and kill tumor cells. The appeal of this active immunotherapeutic strategy includes the ability to generate a sustained T-cell response and immunologic memory with minimal toxicity. More specifically, vac-cines target tumor-associated antigens (TAAs) that are recognized by human cytotoxic T lymphocytes (CTLs), which are critical for the removal of tumor cells in vivo. HER2, the most studied TAA in breast cancer, has been shown to elicit a specific immune response. Identification of HLA-A2 as a restriction element in HER2-expressing cancers [12] led to the discovery of CTL-eliciting epi-topes, nelipepimut-S and GP2 [13,14]. Nelipepimut-S, a nine-amino-acid peptide derived from the extracellular HER2 protein (KIFGSLAFL, HER2 p369-377) [13], is the most studied HER2-derived peptide to date [15].
Introduction to NeuVax™ (Galena, OR, USA)NeuVax™ (Galena, OR, USA), a vaccine comprised of nelipiminut-S and the hematopoietic growth factor, gran-ulocyte–macrophage colony-stimulating factor (GM-CSF), holds promise as an effective adjuvant therapy for women with low-to-intermediate HER2 expression. GM-CSF is known to induce proliferation, maturation and migration of dendritic cells [16,17], and it is intended to enhance nelipepimut-S-specific immunity through augmentation of antigen presentation to CTLs [1,16,17]. Nelipepimut-S binds HLA-A2 and HLA-A3 [18,19] mol-ecules (expressed in ∼60–75% of the general population) on antigen presenting cells that then stimulate CTLs to recognize and lyse HER2-expressing tumor cells.
Laboratory & clinical studiesNelipepimut-S has been studied in multiple labora-tory and clinical studies [13,14,20–27]. The ability for nelipepimut -S to stimulate CTL to lyse HER2- expressing targets in the preclinical setting was established in both ex vivo/in vitro studies of ovarian and breast tumor cells lines [13,27] and animal models (Table 1) [28,29]. Pharmoki-netic studies within animal models were not performed given the small peptide dose used and rapid peptide clearance. As such, typical pharmokinetic parameters (e.g., absorption, plasma protein binding, distribution, metabolism and excretion) were not established.
In addition to administering nelipepimut-S with GM-CSF, other vaccine formulations utilizing the peptide have included: loading the peptide onto autologous dendritic cells [20,24], inclusion into longer peptides to elicit both CTL and CD4+ helper T-cell response [21,22], and use of a single peptide with different immuno adjuvants [23,25,26]. All Phase I clinical trials utilizing GM-CSF as an immu-noadjuvant revealed nelipepimut-S-specific CTL expan-sion [23,25,31]. However, despite the effective stimulation of a nelipepimut-S-specific T-cell response, little was known from the initial trials regarding antitumor activ-ity secondary to the fact that these trials enrolled patients with advanced disease (Table 2) [23,25,26].
Our group has extensively studied the nelipepimut-S peptide as a vaccine but with a shift of focus from the treatment of late-stage disease to the prevention of disease recurrence in high-risk patients after standard-of-care therapy. In our Phase I/II clinical trials, we enrolled both node-positive and high-risk node-negative breast cancer patients who have been rendered clinically free of disease

www.futuremedicine.com 521future science group
HER2 peptide nelipepimut-S (E75) vaccine (NeuVax™) in breast cancer patients at risk for recurrence Drug Evaluation
Table 2. Selected clinical studies examining the ability of nelipepimut-S to stimulate cytotoxic T lymphocytes.
Study (year), phase, design
Patient sample size
Clinical response Toxicity/immunogenic response Ref.
Zaks and Rosenberg (1998), nelipepimut-S plus IFA
Four pts (breast, ovarian and colorectal cancer)
Not disclosed Peptide-specific CTLs detected in post- but not pre-immunization bloodCTLs failed to react with HER2+ tumor cells
[26]
Disis et al. (1999) and Disis et al. (2002), subdominant HER2-derived epitope plus GM-CSF
64 pts (breast, ovarian and NSCLC)
Not disclosed 92% of patients develop T-cell immunity to HER2 peptide and 68% to HER2 protein domainEpitope spreading in 84% of patients38% of patients maintained immunity to HER2 protein at 1 year
[21,22]
Brossart et al. (2000), pilot, peptide loaded onto autologous DCs
Ten pts (advanced breast and ovarian cancer)
Not disclosed No side effects notedMajor CTL response in vivo was induced with the HER2-derived nelipepimut-S and the MUC1-derived M1.2 peptide, which lasted >6 monthsPatient immunized with the HER2-derived peptides, MUC1-specific T lymphocytes were induced after seven immunizations, suggesting that antigen spreading in vivo may occur after successful immunization with a single tumor antigen
[32]
Knutson et al. (2002), Phase I, nelipepimut-S peptide plus GM-CSF
Six pts; stage III/IV breast (4)/ovarian (2) cancer
Not disclosed Minimal toxicityNelipepimut-S-specific precursors developed in two out of four evaluable patients and the responses were short-lived and not detectable at 5 months after the final vaccination
[23]
Murray et al. (2002), Phase I, nelipepimut-S plus GM-CSF
14 pts; stage IV breast (13) and ovarian (1) cancer pts
Not disclosed Vaccine found to be safe, no grade 3/4 toxicitiesFour out of the eight patients showed CTL-mediated lytic activity
[25]
Kono et al. (2002), Phase I, peptide loaded onto autologous DCs
Nine pts (gastric cancer)
One out of nine pts with decreased tumor marker; one out of nine with stabilization of disease status ×3 months
No serious adverse side effectsHER2 peptide-specific recognition demonstrated in six out of nine patients after immunization, whereas no HER2 peptide-specific recognition was present prior to immunizationPeptide-specific delayed-type hypersensitivity response occurred in three out of nine patients
[24]
Peoples et al. (2005), Phase I, nelipepimut-S plus GM-CSF
53 pts; early-stage NP breast cancer post-standard-of-care therapy
DFS VG versus CG: 85.7 versus 59.8% at 22 months (p < 0.19)
Minor toxicity only (one grade 3–4%)Nelipepimut-S-specific CTL expansion exhibited in all ptsDTH VG versus CG (33 vs 7 mm; p < 0.01)
[31]
Peoples et al. (2008), Phase I/II, nelipepimut-S plus GM-CSF
186 pts: early-stage breast cancer post-standard-of-care therapy (NP = 95; NN = 91) VG = 101, CG = 85
VG versus CG recurrence (5.6 vs 14.2%, p = 0.04) at 20 months; (8.3 vs 14.8%) at 26 months; VG with increased time to recurrence (11 vs 8 months)
Mild local/systemic toxicities74% positive postvaccine DTH with an average induration of VG versus CG (14.0 ± 1.4 mm vs 2.1 ± 0.5 mm, p < 0.0001)Nelipepimut-S-specific CTL proliferation peak levels after the third or fourth dose in 65% of patientsStatistically significant increase in median percentage nelipepimut-S-CTLs pre- to post-vaccination43% pts maintained significant residual immunity (dimer > 0.5) 6 months postvaccination
[34]

522 Immunotherapy (2014) 6(5) future science group
Drug Evaluation Schneble, Berry, Trappey et al.
Study (year), phase, design
Patient sample size
Clinical response Toxicity/immunogenic response Ref.
Mittendorf et al. (2012), Phase I/II, nelipepimut-S plus GM-CSF
182 pts: 106 (VG), 76 (CG)
VG versus CG 24-month DFS 94.3 versus 86.8% (p = 0.08)
DFS subset analyses (VG vs CG):Lymph node-positive (90.2 vs 79.1%; p = 0.13)HER2 IHC 1+−2+ (94.0 vs 79.4%; p = 0.04)Grade 1 or 2 tumors (98.4 vs 86.0%; p = 0.01)Optimally dosed (97.3 vs 86.8%; p = 0.08)
[33]
Table 2. Selected clinical studies examining the ability of nelipepimut-S to stimulate cytotoxic T lymphocytes (cont.).
after surgery, chemotherapy and radiation as indicated (Table 2) [31,33,34]. In the Phase I/II trials, HLA-A2/A3+ breast cancer patients with any level of HER2 expression were enrolled into the vaccine group while HLA-A2/A3- patients were followed prospectively as a control group. HLA-A2/3 has never been reported as an independent prognostic factor in breast cancer. Furthermore, a com-parison of control patients from a separate randomized trial of adjuvant vaccines found no difference in survival between HLA-A2-positive and -negative patients [35]. The vaccine group received 4–6 monthly inoculations of NeuVax during the primary vaccine series. A voluntary booster program was initiated, and patients electing to participate were administered booster inoculations every 6 months out to 5 years post-primary vaccination series. These Phase I/II NeuVax clinical trials demonstrated that the vaccine has minimal toxicity and is capable of stimu-lating peptide-specific T-cell expansion, even within the context of low-level antigen expression [31,33,34,36] and after multiple booster doses [37]. Perhaps most impor-tantly, dose-responsive clinical benefit was shown. In the combined trials of node-positive and node-negative patients, 60-month DFS was 89.7% in the vaccine group versus 80.2% in the control group (p = 0.08), although only 35% of patients were optimally dosed secondary to trial design. The 5-year DFS approached significance with 94.7% surviving disease free in the optimally dosed patients in comparison to 80.2% in the control group (p = 0.05) [38]. Interestingly, superior clinical benefit was also shown in HER2 low-to-intermediate-expressing patients versus controls (88.1 vs 77.5%, p = 0.16) [38]. Patients with low-to-intermediate HER2 expression will thus serve as the vaccination population for the ongoing Phase III clinical trial.
Correlating immune & clinical responsesAn integral component of cancer vaccine trials is in vivo and ex vivo immune response monitoring as a means to predict reaction to vaccination and potential clinical ben-efit [39]. Current assays are designed to assess the type and magnitude of T-cell response over multiple time points throughout the trial. Theoretically, immune-monitoring
modalities could provide insight into a vaccine’s specific immunologic mechanisms of action as well as early infor-mation regarding clinical efficacy. However, the optimal method to monitor activity of these peptide vaccines is not clear.
Multiple failed cancer vaccine trials (e.g., Theratope, Stimuvax and Canvaxin) [40–42] have supplied infor-mation regarding the endogenous immune response to malignancy. Particularly within the context of mela-noma research, past cancer vaccine trials have assessed efficacy with immune surrogate end points but have rarely been able to correlate this data to clinical benefit or prevention of tumor progression [43]. In 2013, Hail-emichael et al. specifically addressed clinical trials where CTL proliferation occurs without an associated benefi-cial tumor response [44]. Here, incomplete Freund’s adju-vant (IFA), the most commonly used peptide vaccine adjuvant to date, was assessed. IFA, a water-in-oil emul-sion, acts slowly to release antigen to the immune system to enhance immunogenicity of vaccines. In a series of experiments using a gp100 peptide plus IFA vaccine in a mouse model, the authors observed a T-cell trap with sequestration of CTL at the vaccination site. The seques-tered T cells underwent deletion without evidence of immunologic memory and subsequent hyporesponsive-ness. This diminished response occurred even in vacci-nation of B cell-deficient and CD4 knockout mice, thus eliminating B cells and Tregs as causative sources [44]. Interestingly, vaccine trials utilizing IFA have failed to reveal objective clinical benefit [43], which, based on the work by Hailemichael et al., one may hypothesize is due to IFA-associated CTL sequestration, dysfunction and deletion [44].
CTL degradation within a T-cell trap provides some explanation as to the lack of observed clinical response despite the demonstration of CTL proliferation in response to vaccines. The Phase I clinical trials of neli-pepimut-S plus adjuvant [23,25,26,31] revealed E75-specific CTL proliferation with associated antitumor activity in all but the trial utilizing IFA [26]. As discussed above, our Phase I/II trials [31,33,34,36] evaluating nelipepimut-S have utilized GM-CSF (as opposed to IFA) as the

www.futuremedicine.com 523future science group
HER2 peptide nelipepimut-S (E75) vaccine (NeuVax™) in breast cancer patients at risk for recurrence Drug Evaluation
immunoadjuvant. As will be discussed below, we have been able to correlate nelipepimut-S-specific immune response and increased DFS. Such ability to correlate immune response with clinical benefit has alluded past cancer vaccine trials set in the metastatic setting or in patients with residual tumor burden. However, our trial design differs from previous studies in that we have administered the vaccine as an adjuvant therapy to high-risk, disease-free patients. Just as vaccination site T-cell trap is attributed to long-lasting adjuvants such as IFA, T cells may also be sequestered at the site of extensive tumor burden with its hostile microenvironment. Utiliz-ing a vaccine in the setting of minimal to no residual disease and with a rapidly degrading adjuvant such as GM-CSF, such as in our Phase I/II trials, avoids these limitations.
Immunogenic testingOur group has performed extensive immunologic stud-ies to elucidate the specific immunologic mechanisms by which NeuVax confers clinical benefit. Again, as opposed to clinical trials intended to treat later-stage patients, our group has been able to correlate magnitude of peptide-specific immune response with clinical benefit [33]. We have previously outlined the immunologic monitoring methods used in these trials including delayed-type hypersensitivity (DTH) reaction, dimer assay, ELISPOT assay, assessment of regulatory T cells, cytokine evalua-tion, epitope spreading and circulating tumor cell (CTC) quantification as surrogates for immunologic response to NeuVax [15].
Phase I/II NeuVax clinical trials assessed ex vivo and in vivo response by evaluating nelipepimut-S-specific CTL expansion and DTH, respectively. Peptide-specific CTL expansion was measured by the dimer assay. Briefly, nelipepimut-S peptide-loaded dimers are mixed with the patient’s peripheral blood sample. This sample is ana-lyzed by flow cytometry to quantify the number of CD8+ T cells specifically bound to the peptide dimer molecules [45]. The assay is run on blood without any ex vivo manip-ulation and/or stimulation. Of note, vaccinated HER2 low-to-intermediate-expressing patients have displayed larger maximum immunologic responses compared with overexpressed patients (p = 0.04), an intriguing finding given the reduced mortality of low-expressor patients compared with controls (p = 0.08) [36]. DTH is assessed by injecting 100 μg of nelipepimut-S in 0.5 ml of normal saline (without GM-CSF) 1 month after completion of the vaccine series. Normal saline is injected as a paral-lel volume control. 48–72 h later, the area of erythema and/or induration that develops in response to this injec-tion is measured in two dimensions and recorded as the orthogonal mean. In both of our node-positive and node-negative early-phase trials, a postvaccination DTH
response was assessed. In the node-negative trial, a pre-vaccination DTH was measured as well and compared with the postvaccination DTH [34].
Using the Luminex® assay (Luminex Molecular Diagnostics Inc., ON, Canada) to delineate cytokine profiles in our vaccinated patients, significant differ-ences were elucidated between vaccinated and unvac-cinated patients. Specifically, monocyte chemotactic protein-1 (MCP-1), a chemokine associated with stimu-lating tumor-associated macrophages, angiogenesis and metastasis [46], showed the most significant elevation postvaccination (p = 0.003) [47]. However, as opposed to the metastatic setting where increased MCP-1 levels are implicated in tumor progression, high MCP-1 levels act as favorable prognostic indicators within the context of an adjuvant cancer vaccine. An association between MCP-1 and pre-existing HER2 immunity has also been demonstrated [48–50]. NeuVax vaccination correlated with the largest MCP-1 increase in higher-risk patients with lower initial serum MCP-1 levels. This suggests that the larger the MCP-1 response, the greater the vaccine-induced, peptide-specific immunity [51]. Thus, cytokine profiling may identify patients with low initial serum MCP-1 levels who are most likely to benefit from vaccination.
Despite the presence of an immune response to Neu-Vax, the interplay between malignancy and the immune system is a complex process where tumors are able to escape immune recognition. The fact that most TAAs are also self-antigens tolerated by the immune system is a major obstacle in cancer immunotherapy. A subpopu-lation of regulatory CD4+ T cells, Tregs, are implicated in the process of immune response downregulation and escape from immune recognition [52]. Identification of the regulatory CD4+CD25+ T-cell population, appreci-ated for prevention of autoimmunity and regulation of inflammatory reactions, as well as implicated in sup-pressing immune response against certain malignancies, enhanced the understanding of CD4+ T cells’ impor-tance in immune response regulation [53,54]. Our group analyzed Treg levels in a subset of vaccinated patients. Here, postvaccination Treg levels significantly decreased despite an overall increase in levels of circulating CD4+ T cells [55].
Having shown that vaccination with nelipepimut-S plus GM-CSF can elicit clonal expansion of nelipepimut-S-specific CTL by dimer assay, we next sought to deter-mine whether vaccination with this single peptide was capable of inducing epitope spreading [56]. Although the mechanism of epitope spreading is not fully understood, this phenomenon refers to the natural spread of immu-nity from one portion of an immunogenic protein to other areas within the same antigen (intra-antigenic) or to other antigens (interantigenic) [22]. We examined this

524 Immunotherapy (2014) 6(5) future science group
Drug Evaluation Schneble, Berry, Trappey et al.
phenomenon in 44 patients enrolled in the early stage NeuVax clinical trials. Intra-antigenic epitope spreading to GP2, a second MHC class I epitope derived from the HER2 protein, was observed in 100% of node-positive and 85% of node-negative patients [56]. Of note, inter-antigenic spreading to E41, an epitope from the folate binding protein antigen, was also shown in 63% of tested
patients. All patients with node-positive and 95% of the node-negative patients showed nelipeminut-S- specific clonal expansion, although node-negative patients showed only moderate expansion to this subdominant epitope. This high percentage of epitope spreading in clinically disease-free patients suggests the presence of occult disease [56].
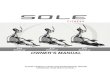
Figure 1. Post-vaccination (R6) dimer levels in vaccinated patients and disease-free survival benefit of vaccine patients with a R6 dimer above the mean. (A) R6 dimer levels in vaccinated patients. Recurrences are shown in red. The mean R6 dimer in the vaccine group is 0.63 mdi ± 0.08. Of the 30 patients with an R6 dimer above the mean, only one recurred, compared with eight of the 56 below the mean (p = 0.09). (B) Disease-free survival benefit of vaccine patients with a R6 dimer above the mean (p = 0.12), a 76.9% relative risk reduction. f/u: Follow-up; mdi: Mean dimer index.
4.00
3.50
3.00
2.50
2.00
1.50
1.00
0.50 p = 0.09
Recurrence above the mean 1/30 (3%)
Patient
R6
dim
er (m
di)
Recurrence below the mean 8/56 (14%)
0.00
Mean R6 dimer = 0.63 mdi
1.0
0.6
0.7
76.9%
96.7%
85.7%
0.8
0.9
Time (months)
Frac
tion
surv
ivin
g di
seas
e fr
ee
Log rankp = 0.12
0.00 10.00 20.00 30.00
Median f/u:60 months
R6 above the meann = 30R6 below the meann = 26
40.00 50.00 60.00

www.futuremedicine.com 525future science group
HER2 peptide nelipepimut-S (E75) vaccine (NeuVax™) in breast cancer patients at risk for recurrence Drug Evaluation
In order to further investigate the presence of occult disease, we have used the CellSearch® system (Veri-dex, NJ, USA) to quantify and phenotype CTCs [57]. Whereas ex vivo phenotypic (dimer/multimer) and functional (ELISPOT, cytokine flow cytometry) T-cell assays are limited by lower sensitivity given the potential for interfering background cytokines and
inconsistent assay conditions, CTC hold potential as an extremely sensitive, clinically relevant surrogate to monitor vaccine response in clinically disease-free patients. In the metastatic setting, substantial numbers of CTC have been identified in up to 70% of patients [58]. Here, CTC burden is shown to predict treatment efficacy, progression-free and overall survival prior to
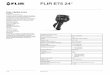
Figure 2. Mean dimer change in vaccinated patients and disease-free survival benefit of vaccine patients with a maximum dimer change above the mean. (A) Mean dimer change in vaccinated patients. The difference between baseline and max. mdi was available in 56 HER2 underexpressing, vaccine group patients. Of the 26 patients above the mean difference (1.08 mdi ± 0.17), one recurred, compared with six clinical recurrences in the 30 patients below the mean (p = 0.06). (B) Disease-free survival benefit of vaccine patients with a maximum dimer change above the mean (p = 0.07), a 80.4% relative risk reduction. f/u: Follow-up; Max.: Maximum; mdi: Mean dimer index.
p = 0.06
Recurrence above the mean 1/26 (4%)
Recurrence below the mean 6/30 (20%)
4.00
5.00
6.00
3.00
2.00
-2.00
1.00
-1.00
Patient
Del
ta m
ax. d
imer
(mdi
)
0.00
Mean max. dimer change = 1.08 mdi
1.0
0.6
0.7
96.2%
80.4%
80.6%0.8
0.9
Time (months)
Frac
tion
surv
ivin
g di
seas
e fr
ee
Log rankp = 0.07
0.00 10.00 20.00 30.00
Median f/u:60 months
Delta max. dimer abovethe mean, n = 26Delta max. dimer belowthe mean, n = 30
40.00 50.00 60.00

526 Immunotherapy (2014) 6(5) future science group
Drug Evaluation Schneble, Berry, Trappey et al.
Table 3. Logistic regression model associating the immunologic variables R0, RC6 and delayed-type hypersensitivity with increased recurrence.
Sample (n) Variables in the optimal model R0 odds ratio (p-value) Sensitivity, specificity AUC
Vaccine group (n = 93) R0, RC6 2.36 (0.09) 75%, 73% 0.71
HER2 low-to-intermediate expression (IHC 1 or 2+, FISH <2.2; n = 58)
R0 1.90 (0.19) 80%, 83% (R0 < 1.19) 0.72
Unboosted (n = 52) R0, post-PVS DTH 3.37 (0.12) 85%, 70% 0.76
and at any point after initiation of systemic therapy [59–61]. Data from our pilot study evaluating CTC revealed quantifiable levels of CTC in peripheral blood samples both pre- and post-vaccination [62]. Expand-ing this pilot study, data was collected in 25 patients within the NeuVax trial. CTC were present in 76% of patients (mean: 4.8 ± 1.0 CTC/20 ml of blood) with 68% of patients exhibiting at least two CTCs. CTC appeared to decrease from pre- to post- vaccination. Six months after the primary vaccination series, nine out of ten patients exhibited stable or decreasing CTC levels. Following NeuVax booster administration, there was a >50% reduction in CTC/20 ml (pre- 1.1 ± 0.5 vs post- 0.4 ± 0.2, p = 0.14) in a matched cohort [63]. Although initial data is promising, correlating CTC with traits to include HLA expression levels, immunologic response and DFS remains challenging secondary to low CTC detection levels. The specific clinical significance has yet to be determined and will require larger studies to make meaningful correlations. However, recent studies suggest that even a single CTC detected by the Cell-Search system in the adjuvant setting has prognostic significance [64,65].
Biomarkers associated with NeuVax responseAs discussed above, multiple modalities are available for immunologic monitoring in cancer vaccine trials. Impor-tantly, our group has been able to associate immune response magnitude with the clinical benefit of Neu-Vax™ [66]. We examined the relationship between ex vivo immunologic response and clinical recurrence after 5-year follow-up of the prospective, completed Phase I/II NeuVax clinical trials [34,38]. Ex vivo immune response was assessed for E75-specific CTL clonal expansion by the dimer assay prevaccination (R0), after the primary vaccination series (R6) and 6 months after completing the primary vaccination series (RC6). In vivo immune response was assessed by DTH reactions to nelipepimut-S at baseline and post-primary vaccine series. Of the 195 patients enrolled, 187 evaluable patients were available for analysis; 108 in the vaccine group and 79 in the con-trol group. R6 dimer assays were available for 86 patients in the vaccine group. R6 dimer levels of individual patients were compared with the mean R6 dimer level
for the entire vaccine group. At 60 months, 3% of the patients above the mean recurred, while 14% recurred below the mean (p = 0.09), a 76.9% relative risk reduc-tion (Figure 1A & 1B). No clinical recurrence occurred in patients with HER2 low-to-intermediate expression with a mean difference in dimer levels ranked in the top third. Examining the mean dimer change from R0 to R6, the mean dimer level was also compared. Here, the greatest dimer change also demonstrated a potential DFS advan-tage and 80.4% relative risk reduction (Figure 2A & 2B). Together, these analyses suggest that patients exhibiting robust ex vivo immune responses have lower recurrence rates suggesting E75-specific CTL clonal expansion as a valid biomarker predicting response in patients treated with NeuVax [66].
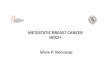
From this initial analysis, our group advanced to a logistical regression model to determine the best immune response parameters for predicting disease recurrence after completion of the primary vaccina-tion series [67]. Here, the immunologic data from all vaccinated patients were examined. Subgroup analysis was performed to include HER2 low-to-intermedi-ate-expressing and nonboosted patients as well. The logistical regression model was performed with back-wards elimination of ex vivo/in vivo tests to predict the chance of recurrence (Table 3). The odds ratio and the area under the curve from the receiver operating characteristic curves was reported for statistical analy-sis (Figure 3). Results revealed that patients lacking pre-existing immunity, or a low R0 dimer level, have improved DFS after NeuVax.
Immunologic response of HER2 low-to-interme-diate expressing patients is of importance based on the DFS benefit shown in the Phase I/II trials. Those patients with minimal pre-existing HER2-specific immunity who experience a robust T-cell response after vaccination are less likely to recur than those who have pre-existing immunity to HER2 or have a small T-cell response. In HER low-to-intermediate-expressing patients, a single variable, R0 dimer, tended to predict recurrence with an odds ratio of 1.9; meaning patients with an R0 level of nelipepimut-S specific CTL greater than 1.19 were nearly twice as likely to recur. Here, the initial dimer value at R0 had a negative predictive

www.futuremedicine.com 527future science group
HER2 peptide nelipepimut-S (E75) vaccine (NeuVax™) in breast cancer patients at risk for recurrence Drug Evaluation
value of 97% and the sensitivity and specificity were 80 and 83%, respectively. Interestingly, the R0 dimer was the dominant variable in multiple modeling groups demonstrating that a low pre-existing immunity is the most important factor in predicting clinical benefit. This analysis may explain why Neuvax works best in HER2 low-to-intermediate-expressing patient with less HER2 antigen exposure.
ConclusionIn the context of clinical trials, the immune monitoring of a vaccine administered in the adjuvant setting differs than that in metastatic setting. In past trials conducted within the metastatic setting, CTL proliferation in response to vaccination failed to show a correlation with clinical response. An explanation may be the sequester-ing of CTL away from a patient’s peripheral circulation towards the hostile environment of an existing tumor burden. Within the context of adjuvant therapies, sam-pling peripheral blood mononuclear cells brings new significance to real-time immune monitoring. As a short-lived vaccination delivered to patients without significant disease burden, NeuVax may avoid trafficking of T cells either to an existing tumor burden or sequestration at the vaccination sites where antigen-driven T-cell dysfunction and deletion ensues.
The promise of NeuVax exists in the prevention of breast cancer recurrence by stimulation of the active immune system. Extensive immunologic monitoring of the NeuVax clinical trials has revealed a correlation of clinical outcome with the magnitude of immune response measured across multiple modalities. Spe-cifically, R0 dimer holds potential as a predictive bio-marker. Exhibition of a low R0 dimer indicates a lack of pre-existing immunity. Data suggest that patients with a low R0 dimer have improved DFS with those demonstrating a more robust response recurring less often. This suggests that induction, rather than ampli-fication, of an anti-HER2 immune response confers a survival advantage. The clinical utility lies in the ability of an initial R0 dimer assessment to identify patients who will benefit from the vaccine prior to inoculation. This holds important implications in future trial design.
Confirmation of NeuVax’s clinical utility will require a large, multicenter, randomized, double-blind trial. Mov-ing forward, the Phase III adjuvant trial (Clinicaltrials.gov identifier: NCT01479244) entitled ‘PRESENT: Prevention of Recurrence in Early-Stage, Node-Positive Breast Cancer with Low-to- Intermediate HER2 Expres-sion with NeuVax Treatment’ is currently enrolling high-risk, node-positive patients with HER2 1+ and 2+
Figure 3. Forest plot depiction of the logistic regression model analysis. Both pre- and post-vaccination dimer, R0 and RC6, are included in the optimal regression model in vaccinated patients. A single variable, the prevaccination dimer (R0), predicted increased chance of recurrence among multiple modeling groups. (A) Vaccinated patients, (B) HER2 low-expressor patients and (C) unboosted patients. DTH: Delayed-type hypersensitivity; PVS: Primary vaccine series.
Vaccinated patients
HER2 low-expressor patients Unboosted patients
Odds ratio
Odds ratio Odds ratio
RC6 dimer
R0 dimer
R0 dimer
0.25 0.5 1 2 4 8
0.25 0.5 1 2 4 8
+
+ +
+
+
+
R0 dimer
Post-PVS DTH
0.25 0.5 1 2 4 8 16 32
+
+ +
+
A
B C

528 Immunotherapy (2014) 6(5) future science group
Drug Evaluation Schneble, Berry, Trappey et al.
Executive summary
BackgroundCancer vaccines are a promising immunotherapeutic strategy given minimal toxicity and the ability to generate a sustained immunologic response with immunologic memory.Vaccines work by targeting tumor-associated antigens that can be recognized by cytotoxic T lymphocytes (CTLs), critical for the removal of tumor cells in vivo.
Introduction to NeuVax™ (Galena, OR, USA)NeuVax™ (Galena, OR, USA) utilizes E75 or nelipepimut-S, a nine-amino-acid peptide derived from the HER2 protein (KIFGLSAFL, HER2 p369-377) as its immunologic focus.NeuVax is administered to disease-free patients in the adjuvant setting after completion of standard-of-care therapy with concurrent endocrine therapy as indicated.The vaccine administers nelipepimut-S in 6-monthly intradermal inoculations with granulocyte–macrophage colony-stimulating factor (GM-CSF) as an immunoadjuvant with booster inoculations every 6 months after the primary vaccine series.
Laboratory & clinical studiesNeuVax shows promise in Phase I/II clinical trials although the mechanism of action, whether by inducing an immune response versus augmenting a pre-existing immune response, has been unknown.
Correlating immune & clinical responseAn integral component of clinical trials for cancer vaccines is in vivo and ex vivo immune response monitoring with multiple cancer vaccine studies failing to correlate peptide-specific CTL expansion with clinical benefit.T-cell trafficking at vaccination and tumor sites may account for T-cell degradation and deletion leading to absence of immunologic memory and subsequent hyporesponsivness.Vaccination models utilizing rapidly degrading adjuvant (GM-CSF) within the adjuvant setting may avoid the pitfalls of CTL sequestration.
Immunologic testingNeuVax immunogenicity has been assessed by multiple immunologic parameters to include delayed-type hypersensitivity, dimer assay, ELISPOT assay, Treg population assessment, cytokine evaluation, epitope spreading and CTC quantification.
Biomarkers associated with NeuVax responseRecent correlation of immunogenic variables with DFS supports nelipepimut-S-specific CTL clonal expansion as a valid biomarker for predicting clinical recurrence after NeuVax administration.Examination of nelipepimut-S-specific CTL clonal expansion data with clinical benefit suggests induction, rather than amplification, of an anti-HER2 immune response correlates with NeuVax’s efficacy.Whereas a large tumor burden may sequester CTLs, in vitro immune monitoring may be more accurate within the adjuvant setting.
Future perspective & conclusionConfirmation of NeuVax’s clinical utility will require a large, multicenter, randomized trial.The Phase III adjuvant trial (NCT01479244) titled ‘PRESENT: Prevention of Recurrence in Early-Stage, Node-Positive Breast Cancer with Low to Intermediate HER2 Expression with NeuVax Treatment’ is currently enrolling HLA-A2+ and/or HLA-A3+ node-positive patients with HER2 1+ and 2+ tumors. Enrollment will be complete in 2014.The vaccine may also be clinically synergistic in combination with Herceptin®. A Phase II trial examining the clinical efficacy of trastuzumab plus NeuVax versus trastuzumab plus GM-CSF alone is currently enrolling.
tumors. Due to a potential relationship between HLA type and prognostic factors, the Phase III study is only enrolling HLA-A2+ and HLA-A3+ patients to be ran-domized to nelipepimut-S plus GM-CSF or GM-CSF alone as the control group. The primary end point is 36 month DFS [68].
Ultimately, combination, both active and passive, immunotherapy may portend the most significant con-tribution to the treatment of HER2-expressing breast cancer patients. The synergistic mechanism of action between trastuzumab and nelipepimut-S was exam-ined in a preclinical study of trastuzumab- pretreated breast cancer cells, which were lysed more efficiently by E75-primed CTL compared with untreated breast
cancer cells. This enhanced CTL-mediated lysis occurred regardless of the level of HER2 expression [69]. Subsequently, a pilot clinical study revealed lower recurrence rates in breast cancer patients receiving adjuvant trastuzumab followed by vaccination with a CD8-eliciting peptide vaccine compared with adju-vant trastuzumab alone [70]. These findings prompted the initiation of an ongoing Phase II clinical trial, Combination Immunotherapy with Herceptin and the HER2 Vaccine NeuVax (Clinicaltrials.gov identi-fier: NCT01570036). This trial hopes to demonstrate the clinical efficacy of combining the known benefits of proven passive immunotherapy with the promise of active specific immunotherapy.

www.futuremedicine.com 529future science group
HER2 peptide nelipepimut-S (E75) vaccine (NeuVax™) in breast cancer patients at risk for recurrence Drug Evaluation
Financial & competing interests disclosure
References1 Disis ML, Smith JW, Murphy AE, Chen W, Cheever MA.
In vitro generation of human cytolytic T-cells specific for peptides derived from the HER-2/neu protooncogene protein. Cancer Res. 54(4), 1071–1076 (1994).
2 Ioannides CG, Fisk B, Fan D, Biddison WE, Wharton JT, O’Brian CA. Cytotoxic T cells isolated from ovarian malignant ascites recognize a peptide derived from the HER-2/neu proto-oncogene. Cell. Immunol. 151(1), 225–234 (1993).
3 Baselga J, Cortes J, Kim SB et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. N. Engl. J. Med. 366(2), 109–119 (2012).
4 Gianni L, Pienkowski T, Im YH et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, Phase II trial. Lancet Oncol. 13(1), 25–32 (2012).
5 Verma S, Miles D, Gianni L et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N. Engl. J. Med. 367(19), 1783–1791 (2012).
6 Piccart-Gebhart MJ, Procter M, Leyland-Jones B et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N. Engl. J. Med. 353(16), 1659–1672 (2005).
7 Romond EH, Perez EA, Bryant J et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J.Med. 353(16), 1673–1684 (2005).
8 Perez EA, Romond EH, Suman VJ et al. Four-year follow-up of trastuzumab plus adjuvant chemotherapy for operable human epidermal growth factor receptor 2-positive breast cancer: joint analysis of data from NCCTG N9831 and NSABP B-31. J. Clin. Oncol. 29(25), 3366–3373 (2011).
9 Vreeland T, Trappey AF, Berry JS et al. Breast cancer patients with HER2 low-expression: an under-recognized group at significant risk for recurrence (abstract). Presented at: San Antonio Breast Cancer Symposium. San Antonio, TX, USA, 3–6 December 2013.
10 Slamon DJ, Godolphin W, Jones LA et al. Studies of the HER-2/neu proto-oncogene in human breast and ovarian cancer. Science 244(4905), 707–712 (1989).
11 Serrano-Olvera A, Duenas-Gonzalez A, Gallardo-Rincon D, Candelaria M, De La Garza-Salazar J. Prognostic, predictive and therapeutic implications of HER2 in invasive epithelial ovarian cancer. Cancer Treat. Rev. 32(3), 180–190 (2006).
12 Peoples GE, Goedegebuure PS, Andrews JV, Schoof DD, Eberlein TJ. HLA-A2 presents shared tumor-associated antigens derived from endogenous proteins in ovarian cancer. J. Immunol. 151(10), 5481–5491 (1993).
13 Fisk B, Blevins TL, Wharton JT, Ioannides CG. Identification of an immunodominant peptide of HER-2/
neu protooncogene recognized by ovarian tumor-specific cytotoxic T lymphocyte lines. J. Exp. Med. 181(6), 2109–2117 (1995).
14 Peoples GE, Goedegebuure PS, Smith R, Linehan DC, Yoshino I, Eberlein TJ. Breast and ovarian cancer-specific cytotoxic T lymphocytes recognize the same HER2/neu-derived peptide. Proc. Natl Acad. Sci. USA 92(2), 432–436 (1995).
15 Mittendorf EA, Holmes JP, Ponniah S, Peoples GE. The E75 HER2/neu peptide vaccine. Cancer Immunol. Immunother. 57(10), 1511–1521 (2008).
16 Disis ML, Bernhard H, Shiota FM et al. Granulocyte-macrophage colony-stimulating factor: an effective adjuvant for protein and peptide-based vaccines. Blood 88(1), 202–210 (1996).
17 Armitage JO. Emerging applications of recombinant human granulocyte-macrophage colony-stimulating factor. Blood 92(12), 4491–4508 (1998).
18 Patil R, Clifton GT, Holmes JP et al. Clinical and immunologic responses of HLA-A3+ breast cancer patients vaccinated with the HER2/neu-derived peptide vaccine, E75, in a Phase I/II clinical trial. J. Am. Coll. Surg. 210(2), 140–147 (2010).
19 Sotiropoulou PA, Perez SA, Iliopoulou EG et al. Cytotoxic T-cell precursor frequencies to HER-2 (369–377) in patients with HER-2/neu-positive epithelial tumours. Br. J. Cancer 89(6), 1055–1061 (2003).
20 Brossart P, Wirths S, Stuhler G, Reichardt VL, Kanz L, Brugger W. Induction of cytotoxic T-lymphocyte responses in vivo after vaccinations with peptide-pulsed dendritic cells. Blood 96(9), 3102–3108 (2000).
21 Disis ML, Gooley TA, Rinn K et al. Generation of T-cell immunity to the HER-2/neu protein after active immunization with HER-2/neu peptide-based vaccines. J. Clin. Oncol. 20(11), 2624–2632 (2002).
22 Disis ML, Grabstein KH, Sleath PR, Cheever MA. Generation of immunity to the HER-2/neu oncogenic protein in patients with breast and ovarian cancer using a peptide-based vaccine. Clin. Cancer Res. 5(6), 1289–1297 (1999).
23 Knutson KL, Schiffman K, Cheever MA, Disis ML. Immunization of cancer patients with a HER-2/neu, HLA-A2 peptide, p369–377, results in short-lived peptide-specific immunity. Clin. Cancer Res. 8(5), 1014–1018 (2002).
24 Kono K, Takahashi A, Sugai H et al. Dendritic cells pulsed with HER-2/neu-derived peptides can induce specific T-cell responses in patients with gastric cancer. Clin. Cancer Res. 8(11), 3394–3400 (2002).

530 Immunotherapy (2014) 6(5) future science group
Drug Evaluation Schneble, Berry, Trappey et al.
25 Murray JL, Gillogly ME, Przepiorka D et al. Toxicity, immunogenicity, and induction of E75-specific tumor-lytic CTLs by HER-2 peptide E75 (369–377) combined with granulocyte macrophage colony-stimulating factor in HLA-A2+ patients with metastatic breast and ovarian cancer. Clin. Cancer Res. 8(11), 3407–3418 (2002).
26 Zaks TZ, Rosenberg SA. Immunization with a peptide epitope (p369–377) from HER-2/neu leads to peptide-specific cytotoxic T lymphocytes that fail to recognize HER-2/neu+ tumors. Cancer Res. 58(21), 4902–4908 (1998).
27 Fisk B, Chesak B, Pollack MS, Wharton JT, Ioannides CG. Oligopeptide induction of a cytotoxic T lymphocyte response to HER-2/neu proto-oncogene in vitro. Cell. Immunol. 157(2), 415–427 (1994).
28 Lustgarten J, Theobald M, Labadie C et al. Identification of Her-2/Neu CTL epitopes using double transgenic mice expressing HLA-A2.1 and human CD.8. Hum. Immunol. 52(2), 109–118 (1997).
29 Disis ML, Shiota FM, Cheever MA. Human HER-2/neu protein immunization circumvents tolerance to rat neu: a vaccine strategy for ‘self ’ tumour antigens. Immunology 93(2), 192–199 (1998).
30 Anderson BW, Peoples GE, Murray JL, Gillogly MA, Gershenson DM, Ioannides CG. Peptide priming of cytolytic activity to HER-2 epitope 369–377 in healthy individuals. Clin. Cancer Res. 6(11), 4192–4200 (2000).
31 Peoples GE, Gurney JM, Hueman MT et al. Clinical trial results of a HER2/neu (E75) vaccine to prevent recurrence in high-risk breast cancer patients. J. Clin. Oncol. 23(30), 7536–7545 (2005).
32 Brossart P, Zobywalski A, Grunebach F et al. Tumor necrosis factor alpha and CD40 ligand antagonize the inhibitory effects of interleukin 10 on T-cell stimulatory capacity of dendritic cells. Cancer Res. 60(16), 4485–4492 (2000).
33 Mittendorf EA, Clifton GT, Holmes JP et al. Clinical trial results of the HER-2/neu (E75) vaccine to prevent breast cancer recurrence in high-risk patients: from US Military Cancer Institute Clinical Trials Group Study I-01 and I-02. Cancer 118(10), 2594–2602 (2012).
34 Peoples GE, Holmes JP, Hueman MT et al. Combined clinical trial results of a HER2/neu (E75) vaccine for the prevention of recurrence in high-risk breast cancer patients: US Military Cancer Institute Clinical Trials Group Study I-01 and I-02. Clin. Cancer Res. 14(3), 797–803 (2008).
35 Trappey ABJ, Vreeland T, Clifton G et al. HLA-A2 Is not a prognostic indicator in breast cancer: implications for cancer vaccine trials (abstract). Presented at: San Antonio Breast Cancer Symposium. San Antonio, TX, USA, 3–6 December 2013.
36 Benavides LC, Gates JD, Carmichael MG et al. The impact of HER2/neu expression level on response to the E75 vaccine: from US Military Cancer Institute Clinical Trials Group Study I-01 and I-02. Clin. Cancer Res. 15(8), 2895–2904 (2009).
37 Holmes JP, Clifton GT, Patil R et al. Use of booster inoculations to sustain the clinical effect of an adjuvant breast cancer vaccine: from US Military Cancer Institute Clinical Trials Group Study I-01 and I-02. Cancer 117(3), 463–471 (2011).
38 Vreeland TJ, Clifton GT, Hale DF et al. Final results of the Phase I/II trials of the E75 adjuvant breast cancer vaccine. Cancer Res. 72(24 Suppl.), P5-16-02 (2012).
39 Walker EB, Disis ML. Monitoring immune responses in cancer patients receiving tumor vaccines. Int. Rev. Immunol. 22(3–4), 283–319 (2003).
40 Miles D, Roche H, Martin M et al. Phase III multicenter clinical trial of the sialyl-TN (STn)-keyhole limpet hemocyanin (KLH) vaccine for metastatic breast cancer. Oncologist 16(8), 1092–1100 (2011).
41 Kroemer G, Zitvogel L, Galluzzi L. Victories and deceptions in tumor immunology: Stimuvax. Oncoimmunology 2(1), e23687 (2013).
42 Cancervax. CancerVax announces results of Phase 3 clinical trials of Canvaxin™ in patients with stage III and stage IV melanoma. www.sec.gov/Archives/edgar/containers/fix060/1131907/000093639206000264/a18983e425.htm
43 Rosenberg SA, Yang JC, Restifo NP. Cancer immunotherapy: moving beyond current vaccines. Nat. Med. 10(9), 909–915 (2004).
44 Hailemichael Y, Dai Z, Jaffarzad N et al. Persistent antigen at vaccination sites induces tumor-specific CD8(+) T cell sequestration, dysfunction and deletion. Nat. Med. 19(4), 465–472 (2013).
45 Woll MM, Fisher CM, Ryan GB et al. Direct measurement of peptide-specific CD8+ T cells using HLA-A2:Ig dimer for monitoring the in vivo immune response to a HER2/neu vaccine in breast and prostate cancer patients. J. Clin. Immunol. 24(4), 449–461 (2004).
46 Salcedo R, Resau JH, Halverson D et al. Differential expression and responsiveness of chemokine receptors (CXCR1–3) by human microvascular endothelial cells and umbilical vein endothelial cells. FASEB J. 14(13), 2055–2064 (2000).
47 Dehqanzada ZA, Storrer CE, Hueman MT et al. Assessing serum cytokine profiles in breast cancer patients receiving a HER2/neu vaccine using Luminex technology. Oncol. Rep. 17(3), 687–694 (2007).
48 Neumark E, Sagi-Assif O, Shalmon B, Ben-Baruch A, Witz IP. Progression of mouse mammary tumors: MCP-1-TNFalpha cross-regulatory pathway and clonal expression of promalignancy and antimalignancy factors. Int. J. Cancer 106(6), 879–886 (2003).
49 Saji H, Koike M, Yamori T et al. Significant correlation of monocyte chemoattractant protein-1 expression with neovascularization and progression of breast carcinoma. Cancer 92(5), 1085–1091 (2001).
50 Salcedo R, Ponce ML, Young HA et al. Human endothelial cells express CCR2 and respond to MCP-1: direct role of MCP-1 in angiogenesis and tumor progression. Blood 96(1), 34–40 (2000).
51 Dehqanzada ZA, Storrer CE, Hueman MT et al. Correlations between serum monocyte chemotactic protein-1 levels, clinical prognostic factors, and HER-2/neu vaccine-related immunity in breast cancer patients. Clin. Cancer Res. 12(2), 478–486 (2006).

www.futuremedicine.com 531future science group
HER2 peptide nelipepimut-S (E75) vaccine (NeuVax™) in breast cancer patients at risk for recurrence Drug Evaluation
52 Gershon RK, Kondo K. Cell interactions in the induction of tolerance: the role of thymic lymphocytes. Immunology 18(5), 723–737 (1970).
53 Shimizu J, Yamazaki S, Sakaguchi S. Induction of tumor immunity by removing CD25+CD4+ T cells: a common basis between tumor immunity and autoimmunity. J. Immunol. 163(10), 5211–5218 (1999).
54 Coutinho A, Hori S, Carvalho T, Caramalho I, Demengeot J. Regulatory T cells: the physiology of autoreactivity in dominant tolerance and ‘quality control’ of immune responses. Immunol. Rev. 182, 89–98 (2001).
55 Hueman MT, Stojadinovic A, Storrer CE et al. Analysis of naive and memory CD4 and CD8 T cell populations in breast cancer patients receiving a HER2/neu peptide (E75) and GM-CSF vaccine. Cancer Immunol. Immunother. 56(2), 135–146 (2007).
56 Mittendorf EA, Gurney JM, Storrer CE, Shriver CD, Ponniah S, Peoples GE. Vaccination with a HER2/neu peptide induces intra- and inter-antigenic epitope spreading in patients with early stage breast cancer. Surgery 139(3), 407–418 (2006).
57 Stojadinovic A, Moskovitz O, Gallimidi Z et al. Prospective study of electrical impedance scanning for identifying young women at risk for breast cancer. Breast Cancer Res. Treat. 97(2), 179–189 (2006).
58 Riethdorf S, Fritsche H, Muller V et al. Detection of circulating tumor cells in peripheral blood of patients with metastatic breast cancer: a validation study of the CellSearch system. Clin. Cancer Res. 13(3), 920–928 (2007).
59 Cristofanilli M, Budd GT, Ellis MJ et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N. Engl. J. Med. 351(8), 781–791 (2004).
60 Cristofanilli M, Hayes DF, Budd GT et al. Circulating tumor cells: a novel prognostic factor for newly diagnosed metastatic breast cancer. J. Clin. Oncol. 23(7), 1420–1430 (2005).
61 Hayes DF, Cristofanilli M, Budd GT et al. Circulating tumor cells at each follow-up time point during therapy of metastatic breast cancer patients predict progression-free and overall survival. Clin. Cancer Res. 12(14 Pt 1), 4218–4224 (2006).
62 Stojadinovic A, Mittendorf EA, Holmes JP et al. Quantification and phenotypic characterization of
circulating tumor cells for monitoring response to a preventive HER2/neu vaccine-based immunotherapy for breast cancer: a pilot study. Ann. Surg. Oncol. 14(12), 3359–3368 (2007).
63 Gates J, Stojadinovic A, Benavides L. Abstract 2833: Assessment of circulating tumor cells (CTCs) for monitoring immediate and long-term response to primary and booster innoculations with a preventative HER2/neu vaccine in breast cancer patients. Presented at: American Association Cancer Research 2008 Annual Meeting. San Diego, CA, USA, 12–16 April 2008.
64 Bidard FC, Mathiot C, Delaloge S et al. Single circulating tumor cell detection and overall survival in nonmetastatic breast cancer. Ann. Oncol. 21(4), 729–733 (2010).
65 Rack BK, Schindlbeck C, Andergassen U et al. Use of circulating tumor cells (CTC) in peripheral blood of breast cancer patients before and after adjuvant chemotherapy to predict risk for relapse: the SUCCESS trial. J. Clin. Oncol. 28(15 Suppl.), 1003 (2010).
66 Berry JS, Trappey AF, Vreeland TJ et al. Biomarker correlation to clinical response in Phase I/II Trials of the Adjuvant Breast Cancer Vaccine, NeuVax (nelipepimut-S or E75) (abstract). Presented at: American Society of Clinical Oncologists Annual Meeting. Chicago, IL, USA, 31 May–4 June 2013.
67 Berry J, Trappey A, Aden J et al. Predicting Clinical Benefit after Completion of Treatment with the Adjuvant Breast Cancer (BCa) Vaccine, NeuVax (nelipepimut-S or E75) (abstract). Presented at: American College of Surgeons 99th Annual Congress. Washington, DC, USA. 6–10 October 2013.
68 Efficacy and safety study of NeuVax(TM)(nelipepimut-S or E75) vaccine to prevent breast cancer recurrence. http://clinicaltrials.gov/show/NCT01479244
69 Mittendorf EA, Storrer CE, Shriver CD, Ponniah S, Peoples GE. Investigating the combination of trastuzumab and HER2/neu peptide vaccines for the treatment of breast cancer. Ann. Surg. Oncol. 13(8), 1085–1098 (2006).
70 Sears AK, Clifton GT, Patil R et al. Sequential administration of trastuzumab and a CD8 T-cell-eliciting HER2/neu peptide vaccine in patients with breast cancer compared with trastuzumab alone (abstract). Presented at: ASCO Annual Meeting. Chicago, IL, USA, 3–7 June, 2011.