Embed Size (px)
Citation preview

The health burden of diabetes in Latin America and the Caribbean: estimates of diabetes-free life expectancy and the effects of diabetes on healthy life expectancy
Flavia Andrade
Center for Demography and Ecology

Demographic context
Life expectancy at birth in Latin America has increased from 52 years to near 72 years in the last fifty years and further increases are expected in the next decades (CELADE 2004);Percentage of those aged 65 and over is expected to rise from the current 5.5% to 10% in 2025 (CELADE 2004).

Do increases in life expectancy imply better health for this larger surviving aging population?

Context: epidemiological and nutritional transitions are in progress
In the last decades, a considerable part of Latin American and Caribbean population has changed diet and lifestyles (mainly through lack of exercise) and those changes have influenced the prevalence of diabetes.
Diabetes prevalence is on rise - in 1995, the prevalence rate was estimated to be 5.7% and it is expected to reach 8.1% in 2025 – a 42% increase (King et al. 1998).
There is some evidence that obesity is also on the rise in Latin America and the Caribbean.

Diabetes prevalence among elders in Latin America and the Caribbean
Diabetes prevalence in Latin America and the Caribbean is relatively high.Most of the cases are of type 2 diabetes (~90 to 95%).

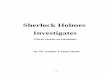
Prevalence of self-reported diabetes among elders (60+) in Latin America and the Caribbean
12.7
22.3
17.9
13.615.2
22.0
13.0
17.6
19.8
13.714.7
0.0
5.0
10.0
15.0
20.0
25.0
Buen
os A
ires
Bridg
etown
São P
aulo
Santi
ago
Havan
aMex
ico C
ityMon
tevide
o
Mexico
Mex
ico (u
rban)
Mexico
(rura
l)US
(BRFS
S 20
00)
Note: Estimates are not age standardized.
US data from Mokdad et al 2001

Diabetes and disability
Diabetes has been shown to be strongly associated with physical limitation and functional disability. In general, individuals with diabetes are about two to three times more likely to have disability than those without (Gregg et al. 2000, Valderrama-Gama et al. 2002, Bruce et al. 2003, Ryerson et al. 2003, Maty et al. 2004).

Diabetes and disabilityThose with diabetes are also more likely to become functionally disabled (Gregg et al. 2002). Gregg et al. (2002) report a yearly incidence of 9.8% among women with diabetes and 4.8% among non-diabetics. After controlling for comorbidities and potential confounders, diabetes was still associated with an increase of 42% in the risk of any incident disability in elderly women (Gregg et al. 2002).

The effects of diabetes on life expectancy and healthy life expectancy
Bélanger et al. (2002) find that disability-free life expectancy at age 45 is 14.1 years lower for women with diabetes than for those without the disease. Among men, diabetes reduces disability-free life expectancy in 10.7 years. Diabetes also had a strong effect reducing total life expectancy of women in Canada – total life expectancy at age 45 is reduced in 13 years among women. However, the effects are much smaller among men. The authors conclude that diabetes imposes a bigger burden on total life expectancy among women, but diabetes-related disabilities are probably similar among both sexes.

The effects of diabetes on life expectancy and healthy life expectancy
Jagger et al. (2003) show diabetics in U.K. have lower total life expectancy than those without diabetes – life expectancy at age 75 reaches 10.3 among non-diabetics and 7.2 among diabetics. Results also show that active life expectancy of diabetics is reduced in 2.4 years – active life expectancy of diabetics aged 75 is 4.7 years, while non-diabetics are expected to live, on average, 7.1 years without any losses on autonomy.

The effects of diabetes on life expectancy and healthy life expectancy
Laditka and Laditka (2005) show that individuals with diabetes live shorter lives with more disability. Diabetes reduces the total life expectancy by 4.1 years among white, highly educated women aged 70. These white highly educated women are expected to live almost 40% of their remaining lives with some sort of impairment if they are diabetic at age 70, compared with 28% among their non-diabetic counterparts.Among white highly educated men, life expectancy is reduced in 2.8 years for those with diabetes. They are also expected to live a larger percentage of their lives with some impairment compared with non-diabetics, 26.5% and 19.1%, respectively.

The effects of diabetes on life expectancy and healthy life expectancy
Laditka and Laditka (2005) conclude that diabetic toll in terms of total life expectancy and unimpaired life expectancy is higher for women. Also, as expected, having lower education and/or being non-white reduce the total life expectancy and increases the number (and percentage) of years expected to be lived with impairment for both diabetics and non-diabetics.

Hypothesis and goalsThe main hypothesis of this paper is that diabetes is likely to impose an important burden on those with the condition. More specifically, this paper aims to:1) estimate the diabetes-free life expectancy using
data from seven regions in Latin America and the Caribbean based on the Sullivan method and,2) estimate the total, active and inactive life expectancies for individuals with and without diabetes based data from a nationally representative panel data from Mexico conducted in 2001 and 2003.

Data
• Salud, Bienestar y Envejecimiento en América Latina y el Caribe Proyecto (SABE)
• Mexican Health and Aging Study (MHAS)• Life tables by 5-year age groups, sex and
country

Data - SABESABE is a multicenter survey that investigates the health and well being of older people (aged 60 and over) and, in some cases, of their surviving spouse in seven capital/major cities in countries of Latin America and the Caribbean. The cities investigated were: Buenos Aires (Argentina); Bridgetown (Barbados); São Paulo (Brazil); Santiago (Chile); Havana (Cuba); Mexico City (Mexico); Montevideo (Uruguay).
The final sample is composed by 10,902 individuals aged 60 and over.

Data - MHAS
MHAS is a prospective two-wave panel study of a nationally representative cohort of Mexicans born prior to 1951 (50 and older). The survey has national and urban/rural representation. Surviving spouses regardless of their age were also interviewed. The baseline interview was conducted in 2001 and the second wave during 2003.

Data - MHASFirst wave: A total of 15,186 complete interviews were obtained (response rate reached 90.1%)
In the first wave, the final sample is composed by 13,055 individuals aged 50 and over with complete information on age, sex and diabetic status. There are 7,150 individuals aged 60 and over.
Mortality information was obtained in the next-of-kin questionnaires.

Disability measures – SABE and MHAS
Activities of daily living (ADL): dressing, bathing, eating, getting in and out of a bed (transferring), toileting, and getting across the room Instrumental activities of daily living (IADL):preparing a hot meal, money management, shopping, and taking medication.Nagi (Nagi, 1976) - physical performance measure: lifting or carrying objects weighted 5 Kg or over; lifting up a coin (using fingers to grasp or handle); pulling or pushing a large object such as a living room chair; stooping, kneeling or crouching; and, reaching or extending arms above shoulder level.

ADL, IADL and NAGIADL, IADL and Nagi scale were measured in two different ways:Binary - scoring ‘0’ indicates no limitation and scoring ‘1’ indicates having difficulty performing at least one activity;Binary with severity - scoring ‘0’ indicates having difficulty performing none or less than 3 activities, score ‘1’ indicates having difficulties performing 3 or more activities.

ADL and IADL help
Two measures capture the need for help in basic life activities (ADL and IADL limitations). Individuals were asked in MHAS whether a spouse or another person assisted them on basic and instrumental daily activities. Help on ADL activities and on IADL activities are in the binary form, in which those scoring ‘0’ indicate that they do not have require assistance on ADL or IADL activities, while score ‘1’ was assigned for those who have reported requiring human assistance in least one activity of each scale.

Life tablesBuenos Aires – INDECBridgetown – data from Barbados – WHOSão Paulo – SEADESantiago – INEHavana - Esther María León DíazMexico - Roberto Ham-ChandeMexico City – CONAPOMontevideo – INE ((http://www.ine.gub.uy)

Methods
Sullivan method will be used to estimate the diabetes-free life expectancy based on prevalence data from SABE and MHAS 2001
Multistate life table method (MSLT) will be used to estimate active (disability-free) and disabled life expectancy by sex and diabetic status - IMach 0.98g version (stepm=1 and estepm=1).

Descriptive data – SABE and MHASVariables SABE MHAS 2001 Percentages and means Non-diabetics Diabetics p-value Non-diabetics Diabetics p-value Age (mean) 71.8 71.6 0.221 69.6 68.9 0.002 Female 61.0 66.5 0.000 52.4 60.3 0.000 ADL 19.0 25.3 0.000 13.9 21.1 0.000 IADL 15.2 22.5 0.000 11.4 17.7 0.000 Nagi 59.2 69.9 0.000 52.2 65.6 0.000 Severe ADL 6.2 8.9 0.000 4.5 8.9 0.000 Severe IADL 4.0 6.6 0.000 3.1 5.6 0.000 Severe Nagi 20.5 29.8 0.000 21.3 31.0 0.000 BMI (mean) * 26.6 27.7 0.000 26.8 27.9 0.003 Obesity 23.8 28.4 0.000 22.0 28.5 0.053 Cancer 3.9 3.8 0.855 1.9 2.3 0.311 Heart disease 19.8 26.4 0.000 3.9 7.8 0.000 Stroke 6.2 9.3 0.000 3.5 5.3 0.003 Arthritis 42.0 45.0 0.017 24.7 27.2 0.074
Note: * BMI in SABE does not include Argentina. Only 20% of the MHAS sample has anthropometric measures.

Prevalence of ADL among elderly people (60+) in Latin America and the Caribbean by diabetic status, SABE and MHAS
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
BuenosAires
Bridgetown São Paulo Santiago Havana Mexico City Montevideo Mexico
Non-diabetics Diabetics

Prevalence of Nagi limitations among elderly people (60+) by diabetic status, SABE and MHAS
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
BuenosAires
Bridgetown São Paulo Santiago Havana Mexico City Montevideo Mexico
Non-diabetics Diabetics

Results: diabetes-free life expectancy using data from SABE and MHAS

Males: total life expectancy and diabetes-free life expectancy (self-reports)
Sex and region
Total life expectancy at age 60 (e 60)
Diabetes life expectancy (DLE 60)
Diabetes-free life expectancy
(DFLE 60) s.e.
(DFLE) Males Buenos Aires (Argentina) 17.4 2.4 15.0 0.01 Bridgetown (Barbados) 17.6 3.4 14.2 0.29 São Paulo (Brazil) 17.2 2.9 14.3 0.01 Santiago (Chile) 19.9 2.3 17.6 0.22 Havana (Cuba) 18.4 1.3 17.1 0.01 Mexico City (Mexico) 20.3 4.5 15.8 0.01 Montevideo (Uruguay) 17.6 2.1 15.5 0.01 Mexico 21.6 3.1 18.5 0.13

Females: total life expectancy and diabetes-free life expectancy (self-reports)
Sex and region
Total life expectancy at age 60 (e 60)
Diabetes life expectancy (DLE 60)
Diabetes-free life expectancy
(DFLE 60) s.e.
(DFLE) Females Buenos Aires (Argentina) 22.1 2.5 19.6 0.01 Bridgetown (Barbados) 22.8 5.4 17.4 0.32 São Paulo (Brazil) 21.9 4.0 17.9 0.01 Santiago (Chile) 24.0 3.3 20.7 0.23 Havana (Cuba) 22.0 4.5 17.6 0.02 Mexico City (Mexico) 22.1 4.6 17.5 0.01 Montevideo (Uruguay) 22.9 3.1 19.9 0.01 Mexico 23.1 4.2 18.9 0.01

0.0
5.0
10.0
15.0
20.0
25.0
BuenosAires
Bridgetown São Paulo Santiago Havana Mexico City Montevideo Mexico
Without diabetes With diabetes
Males: total life expectancy and diabetes-free life expectancy

Females: total life expectancy and diabetes-free life expectancy
0.0
5.0
10.0
15.0
20.0
25.0
BuenosAires
Bridgetown São Paulo Santiago Havana Mexico City Montevideo Mexico
Without diabetes With diabetes

Results: active and inactive life expectancy by diabetes status using data from Mexico (MHAS)

Incidence: Conditional probabilities to be observed in the Nagi state in wave 2 being active in wave 1 by sex and diabetic status, Mexico, MHAS
0.00
0.02
0.04
0.06
0.08
50 55 60 65 70 75 80 85 90Age
Male non-diabetic Female non-diabetic Male diabetic Female diabetic
Diabetics

Recovery: Conditional probabilities of recovering from IADL limitation, by sex and diabetic status, Mexico, MHAS
0.00
0.02
0.04
0.06
0.08
50 55 60 65 70 75 80 85 90Age
Male non-diabetic Female non-diabetic Male diabetic Female diabetic
Diabetics

Males: Probabilities of dying by IADL and diabetes status, Mexico, MHAS
0.00
0.01
0.02
0.03
0.04
50 55 60 65 70 75 80 85 90Age
Non-diabetic, active Diabetic, active Non-diabetic, inactive Diabetic, inactive
Diabetics

Effects of diabetes on healthy life expectancy, Mexico
Impairment Age and sample size 50 (s.d) 60 (s.d) 70 (s.d) 80 (s.d) ADL (N=12,050) Non-diabetics TLE 32.8 (0.606) 24.2 (0.585) 16.6 (0.567) 10.4 (0.531) ALE 28.8 (0.520) 20.5 (0.498) 13.4 (0.478) 7.8 (0.437) ILE 3.9 (0.224) 3.7 (0.230) 3.2 (0.239) 2.6 (0.247) Diabetics TLE 24.7 (0.927) 17.2 (0.782) 11.1 (0.656) 6.6 (0.537) ALE 20.5 (0.739) 13.4 (0.599) 7.9 (0.470) 4.0 (0.345) ILE 4.2 (0.381) 3.8 (0.360) 3.3 (0.345) 2.6 (0.336)
Note: TLE (Total Life Expectancy), ALE (Active Life Expectancy) and ILE (Inactive Life Expectancy)Source: MHAS

Effects of diabetes on active and inactive life expectancies at age 50
0
5
10
15
20
25
30
35
Non-diabetics
Diabetics Non-diabetics
Diabetics Non-diabetics
Diabetics
Life
exp
ecta
ncy
(yea
rs)
ALEILE
ADL IADL Nagi

Effects of diabetes on active and inactive life expectancies at age 50
0
5
10
15
20
25
30
35
Non-diabetics
Diabetics Non-diabetics
Diabetics Non-diabetics
Diabetics Non-diabetics
Diabetics
Life
exp
ecta
ncy
(yea
rs)
ALEILE
ADL Severe ADL Nagi Severe Nagi

Effects of diabetes on total, active and inactive life expectancies by age and sexImpairment Age 50 Age 60 Age 70 and sample size Males Females Males Females Males Females IADL (N=12,065) Non-diabetics TLE 31.1 34.2 22.8 25.4 15.5 17.4ALE 29.0 29.0 20.7 20.3 13.5 12.6ILE 2.1 5.2 2.1 5.1 2.0 4.8ILE/TLE (%) 6.8% 15.2% 9.2% 20.0% 13.1% 27.5%Diabetics TLE 22.6 26.4 15.6 18.6 9.9 12.0ALE 20.8 21.5 13.8 13.9 8.1 7.7ILE 1.8 4.9 1.8 4.7 1.8 4.4ILE/TLE (%) 8.1% 18.4% 11.7% 25.4% 17.8% 36.2%
Note: TLE (Total Life Expectancy), ALE (Active Life Expectancy) and ILE (Inactive Life Expectancy)Source: MHAS

0
5
10
15
20
25
30
50 55 60 65 70 75 80 85 90
Age
Year
s
Males, non-diabetics Males, diabetics Females, non-diabetics Females, diabetics
Active life expectancy (ADL) by diabetic status and sex
Diabetics

Inactive life expectancy (ADL) by diabetic status and sex
0
1
2
3
4
5
6
50 55 60 65 70 75 80 85 90
Age
Inac
tive
life
expe
ctan
cy
Males, non-diabetics Males, diabetics Females, non-diabetics Females, diabetics

0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
Males Females Males Females
Year
s
ALEILE
Non-diabetics Diabetics
Active and inactive life expectancy (ADL) at age 50, by sex – Mexico

0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
Males Females Males Females
Year
s
ALEILE
Non-diabetics Diabetics
Active and inactive life expectancy (Nagi) at age 70, by sex – Mexico

Assistance on daily activitiesDiabetes status, health status AGE and sample size 50 (s.d) 80 (s.d) ADL assistance (N=12,050) Non-diabetics Total life expectancy 32.4 (0.594) 10.2 (0.516) Without help 30.4 (0.543) 8.5 (0.456) With help 2.0 (0.165) 1.7 (0.202) Diabetics Total life expectancy 24.6 (0.903) 6.4 (0.517) Without help 22.2 (0.785) 4.5 (0.381) With help 2.4 (0.289) 2.0 (0.318) IADL assistance (N=12,065) Non-diabetics Total life expectancy 32.4 (0.588) 10.1 (0.513) Without help 29.1 (0.484) 7.2 (0.379) With help 3.3 (0.228) 2.8 (0.278) Diabetics Total life expectancy 24.7 (0.885) 6.3 (0.525) Without help 21.5 (0.727) 3.7 (0.319) With help 3.3 (0.338) 2.6 (0.356)

Assistance on daily activities, by sexImpairment Age 50 Age 70 and sample size Males Females Males Females ADL assistance (N=12,050) Non-diabetics Life expectancy 31.0 33.8 15.3 17.3 Without help 29.5 31.2 13.9 14.8 With help 1.5 2.6 1.4 2.4With help (%) 4.8% 7.7% 9.0% 13.9% Diabetics Life expectancy 22.7 26.0 9.8 11.9 Without help 21.1 23.0 8.3 9.1With help 1.6 3.0 1.5 2.8With help (%) 7.1% 11.6% 15.5% 23.3% IADL assistance (N=12,065) Non-diabetics Life expectancy 30.9 33.9 15.3 17.2 Without help 29.0 29.1 13.5 12.7 With help 1.9 4.8 1.8 4.5With help (%) 6.1% 14.1% 12.0% 26.0% Diabetics Life expectancy 22.8 26.2 9.9 11.8 Without help 21.1 21.6 8.2 7.7With help 1.7 4.6 1.6 4.1With help (%) 7.5% 17.4% 16.6% 34.9%

What does this paper add to the literature?
To my knowledge this is the first study using panel data from a developing country in Latin America that analyzes the effects of diabetes on total and active life expectancy. The paper shows that, in Mexico, diabetes reduces both the total and active life expectancy at age 50 in about 8.7 years for men and 8 years among women. This contrasts with findings from Canada (Bélangeret al. 2002) and United States (Laditka and Laditka2005) that show a heavier toll for women than for men in terms of total life expectancy.

Other remarksPrevalence data from SABE and MHAS indicate that a large proportion of the remaining lives of those aged 60 are expected to be lived with diabetes. However, there are important differences across settings. Men aged 60 in Havana are expected to live 9.3% of their remaining years with diabetes, while this percentage reaches 21.7% in Mexico City. Among older women, residents in Buenos Aires are expected to live 13.2% of their remaining life with diabetes, but this percentage reaches 22.7% in Bridgetown.

Final remarksFindings from MHAS confirm the previous results in the literature (Bélanger et al. 2002, Jagger et al. 2003, Laditka and Laditka 2005) that diabetes imposes losses of autonomy and reduces active life expectancy.
Results from MHAS show that diabetes reduces the total life expectancy (at age 50) by about eight years and this reduction is basically in the form of reduction in active life expectancy.

Final remarksAs shown in the literature, women in Mexico face higher disability burden than men. Women with diabetes at age 50 is expected to live 20% of their remaining lives with limitations on at least one ADL, but their male counterparts will live 12.7% of their remaining years with disability. For non-diabetic women and men the percentages reach 14.8 and 9.3%, respectively.

Thank you

Diabetes: very brief overviewDiabetes is a metabolic disease characterized by high blood sugar levels.Diabetes results from defects in insulin secretion, or action, or both.Diabetes mellitus is generally recognized to be a result of genetic susceptibility and environmental factors. Type 1 diabetes: the body failures to produce insulin;Type 2: results from insulin resistance combined with relative insulin deficiency.Pre-diabetes: higher levels of blood glucose, but not as high for the diagnosis of type 2 diabetes.

Diabetes and obesity

Aging, chronic diseases and disabilityAging is associated with a natural decline in bodily systems. At the same time, it is usually associated with the onset and progression of chronic diseases. Chronic diseases and associated co-morbidities often lead to the impairments, functional limitations and difficulties performing activities of daily life. This progression is well described in the ‘disablement process’ (Verbrugge and Jette1994).

0.0 5.0 10.0 15.0 20.0 25.0 30.0 35.0 40.0 45.0 50.0
Buenos Aires (s)Buenos Aires (p)
Bridgetown (s)Bridgetown (p)
São Paulo (s)São Paulo (p)
Santiago (s)Santiago (p)
Havana (s)Havana (p)
Mexico City (s)Mexico City (p)Montevideo (s)Montevideo (p)
Mexico (s)Mexico (p)
Self-reported and predicted diabetes prevalence rates, and 95% confidence intervals, SABE and MHAS

Differences in diabetes-free life expectancy –self-reports and predicted values
Total life expectancy
Diabetes life expectancy (self-
reports)
Diabetes life expectancy (predicted)
Relative difference
(%)MalesBuenos Aires (Argentina) 17.4 2.4 2.5 5.3Bridgetown (Barbados) 17.6 3.4 3.5 1.4São Paulo (Brazil) 17.2 2.9 3.0 4.9Santiago (Chile) 19.9 2.3 2.7 18.8Havana (Cuba) 18.2 1.3 1.7 30.5Mexico City (Mexico) 20.3 4.5 4.4 -2.2Montevideo (Uruguay) 17.6 2.1 2.4 13.0Mexico 21.6 3.1 3.4 8.9FemalesBuenos Aires (Argentina) 22.1 2.5 2.9 18.0Bridgetown (Barbados) 22.8 5.4 5.2 -3.6São Paulo (Brazil) 21.9 4.0 4.2 5.5Santiago (Chile) 24.0 3.3 3.8 17.1Havana (Cuba) 21.5 4.4 4.5 3.5Mexico City (Mexico) 22.1 4.6 4.7 1.8Montevideo (Uruguay) 22.9 3.1 3.5 14.9Mexico 23.1 4.2 4.6 9.4

Predicted probabilities of truly having diabetes for an average person based by sex and diabetic status, ENSA 2000
0.035
0.857
0.0770.042
0.879
0.092
0.0
0.2
0.4
0.6
0.8
1.0
Self-reported no diabetes Self-reported having diabetes Total
Male Female

-
5.00
10.00
15.00
20.00
25.00
30.00
35.00
50 55 60 65 70 75 80 85 90 95 100
Age
Life
exp
ecta
ncy
Vital statistics IMach
Differences in life expectancy: IMach versus vital statistics, males, Mexico

Differences in life expectancy: IMach versus vital statistics, females, Mexico
-
5.00
10.00
15.00
20.00
25.00
30.00
35.00
50 55 60 65 70 75 80 85 90 95 100
Age
Life
exp
ecta
ncy
Vital statistics IMach

Diabetes and comorbidities
From: Diabetes Atlas, 2003.
Usually, functional disability among diabetics is thought to be a consequence of these medical conditions (Gregg et al. 2000, Gregg et al. 2002, Volpato et al. 2002, Egede 2004, Matyet al. 2004).

Diabetes costsA recent study conducted by Barceló and colleagues (2003) showed that the total annual cost associated with diabetes was estimated in more than US$65 billion. Indirect costs contributed to 82% of the overall costs. Indirect costs are due over 330,000 deaths occurring in year 2000 (over 757,000 years of productive life lost) and to approximately 178,000 individuals with permanent disability (over 136,000 years of productive life lost). Direct costs (drugs, consultations and hospitalizations) represented 18% of the overall costs and are estimated at US$703 per capita annually.

0.0
5.0
10.0
15.0
20.0
25.0
Bueno
s Aire
sBrid
getow
nSão
Pau
lo
Santia
go
Havan
aMex
ico C
ityMon
tevide
o
Mexico
US (B
RFSS 2000
)
CrudeSEGIWHO
Prevalence of diagnosed diabetes among elders (60+) in Latin America and the Caribbean – crude and age standardized rates

ADL measures
SABE: “Here are a few everyday activities. Please tell me if you have any difficulty with these because OF A HEALTH PROBLEM. Exclude any difficulties you expect to last less than three months.”ADL: Do you have difficulty with…?ADL: Yes, no, does not know, NR.

ADL measuresMHAS: Only for those with NAGI, except dressingMHAS: “Please tell me if you have any difficulty with each of the activities I mention. If you do not do any of the following activities, simply tell me. Do not include difficulties that you believe will last less than three months.”Because of a health problem, do you have any difficulty...?Yes, no, can’t do, doesn’t do, DK, RF.

IADL measuresSABE: “Here are a few everyday activities. Please tell me if you have any difficulty with these because OF A HEALTH PROBLEM. Exclude any difficulties you expect to last less than three months.”IADL: Do you have difficulty with…?IADL: Yes, no, cannot do it, does not do it, does not know, NR.

IADL measuresMHAS: “Now I am going to mention other activities. Please tell me if you have any difficulty with the activities that I mention to you. If you do not do any of the following activities, simply tell me. Do not include difficulties that you believe will last less than three months.”Because of a health problem, do you have any difficulty...Yes, no, can’t do, doesn’t do, DK, RF.Is this because of a health problem?

Nagi measures - wordingSABE: “We need to know about problems that people may have doing certain activities that are important to daily living BECAUSE OF A HEALTH OR PHYSICAL PROBLEM. Please tell me whether you have (at this time) any difficulty doing any of the activities that I am going to mention. EXCLUDE ANY DIFFICULTIES THAT YOU EXPECT TO LAST LESS THAN THREE MONTHS.”Do you have any difficulty….?Yes, no, cannot do it, DK, NR.

Nagi measures - wordingMHAS: “Please tell me if you have any difficulty in doing each of the daily activities that I am going to read. Don’t include difficulties that you believe will last less than three months.”Because of a health problem, do you have difficulty with….?Yes, no, cannot do it, does not do it, DK, RF.