Embed Size (px)
Citation preview
THE FUTURE OF PM&R
From a PGY-46
Randall L. Braddom, M.D., M.S.
Clinical Professor Rutgers NJ Medical School
Rutgers Robert Wood Johnson Medical School
WORD TO THE WISE
FREE PREDICTIONS
Are worth what you pay for them!
I might be less accurate than a $5 Psychic
CURRENT STATUS OF PM&R
High Satisfaction Among Physiatrists
As measured by
Direct contacts with practitioners
Questionnaires
Double-Boarded Usually Practice PMR
Wide Spectrum of Practice Options
Settings (inpatient/outpatient)
Patient categories (msk/neuro)
*Courtesy JW Melvin
Some of my predictions have been horribly wrong! (1969) I said:
EDX is Late 20th
Century Test
Won’t be around after the year 2000
Some new imaging test will replace it
HOW TO DETERMINE THE FUTURE ?
1. Project current trends
2. Analyze new events that threaten current trends
1. Political changes
2. Technological changes
3. Unexpected major events
4. Economic cycles
3. Ask the “wizards”
PM&R: Where do we stand?
6 decades of growth
Rising incomes
Rising numbers of physiatrists/residents
Rising prestige, visibility
Better residents

2011 Physiatrist Gross Income
Full-time Physiatrists
Mean $271,000
90th Percentile $461, 000
Mean Pay by subspecialty
Lowest: Hospice/Palliative Medicine
$217,000
Highest: Interventional Spine Medicine
$335,000
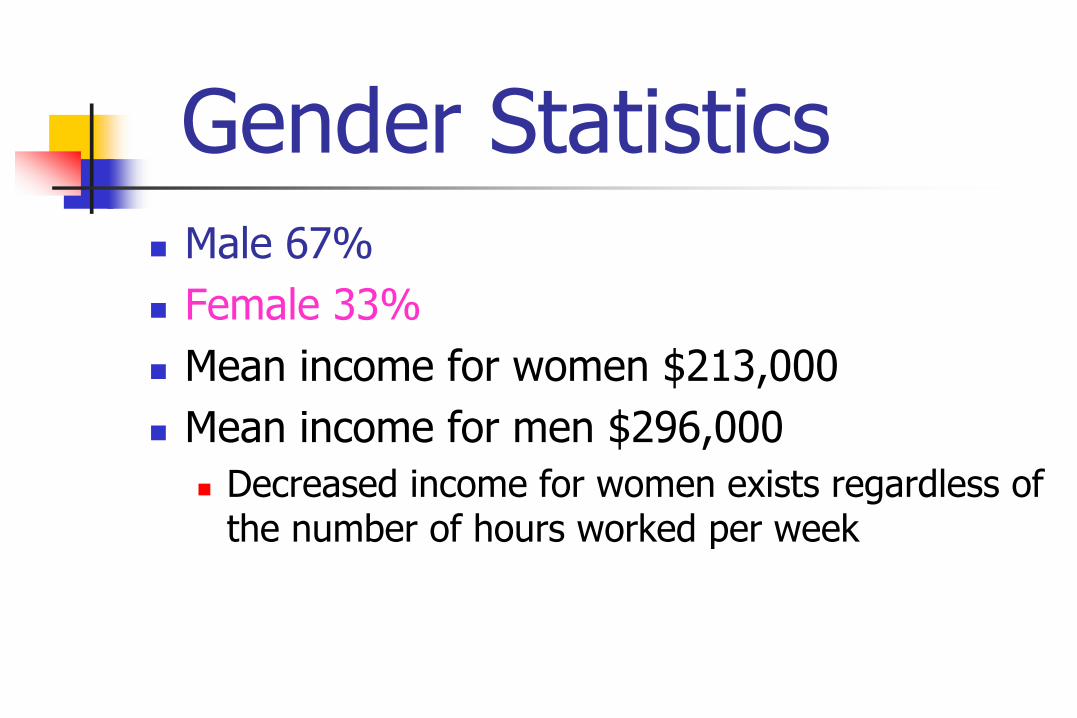
Gender Statistics Male 67%
Female 33%
Mean income for women $213,000
Mean income for men $296,000
Decreased income for women exists regardless of the number of hours worked per week
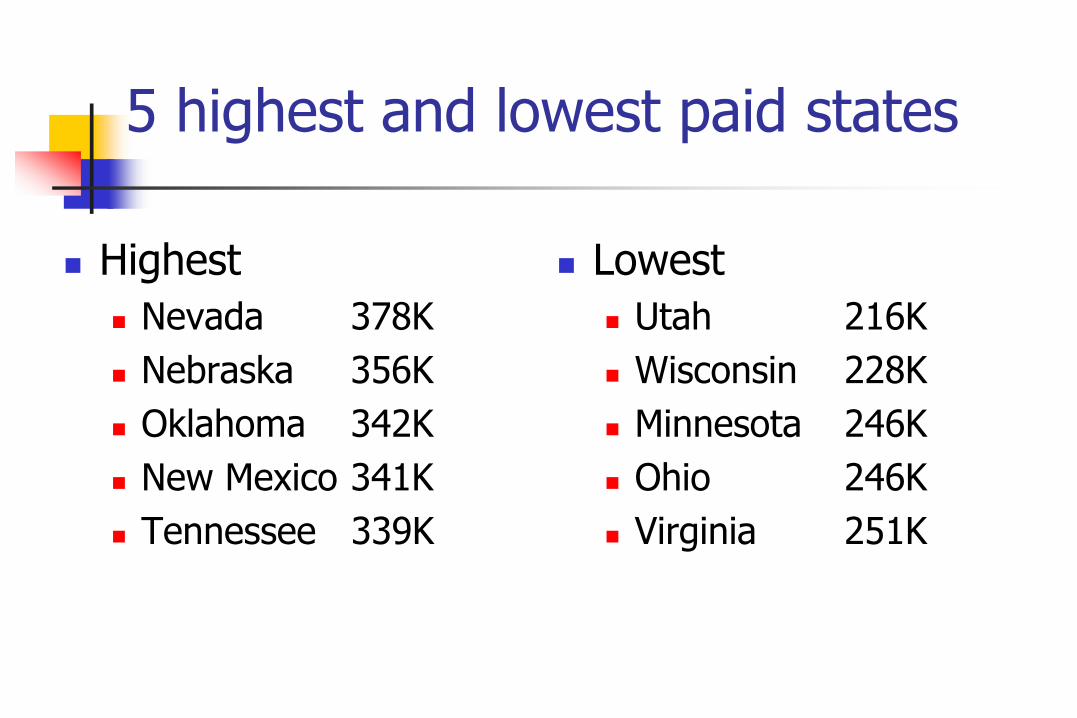
5 highest and lowest paid states
Highest
Nevada 378K
Nebraska 356K
Oklahoma 342K
New Mexico 341K
Tennessee 339K
Lowest
Utah 216K
Wisconsin 228K
Minnesota 246K
Ohio 246K
Virginia 251K
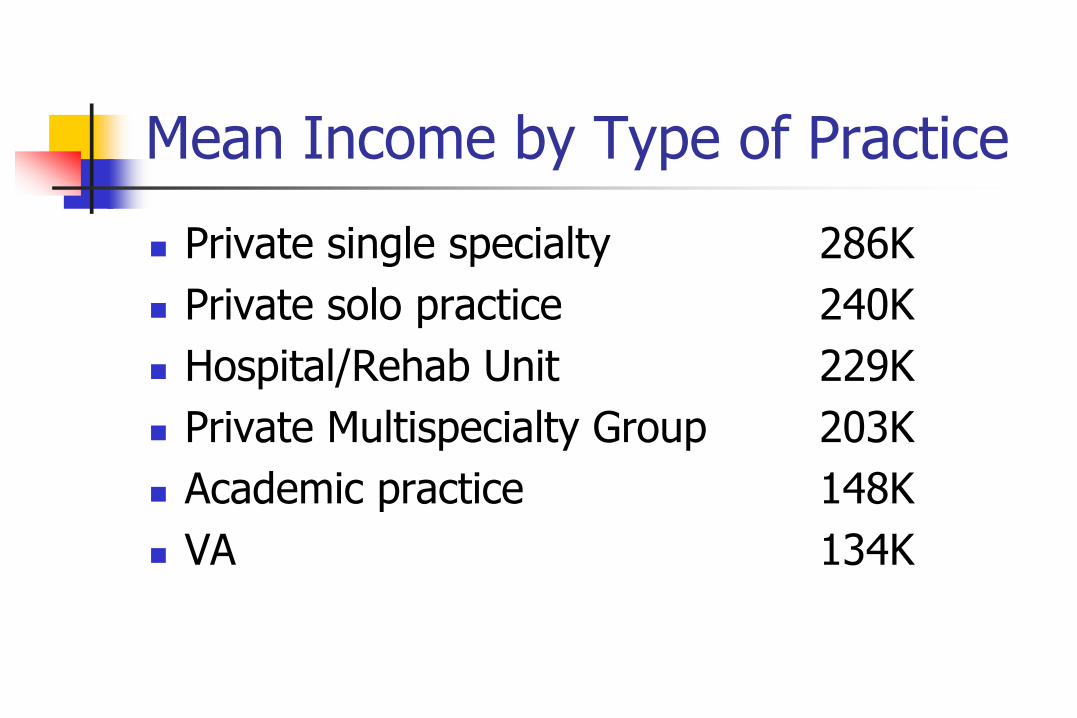
Mean Income by Type of Practice
Private single specialty 286K
Private solo practice 240K
Hospital/Rehab Unit 229K
Private Multispecialty Group 203K
Academic practice 148K
VA 134K
Trend to Evidence Based Medicine
Problem:
Evidence Basis of PM&R is Significantly limited
Due to variability/complexity
Due to limited research
Distant from molecular biology
Clinical studies lack analytical rigor Courtesy JW Melvin
Research is critical for PM&R
Survival of the Field
Survival of Academic Programs
Improving our Practice
EBM Linked to Payment
Research is critical for Academic PM&R Survival
Deans want funded research Prestige
Overhead dollars
Deans don’t take us seriously unless we produce research
Hobby research versus funded research
A field has to buy its way into medical schools
Money talks: Research dollars are part of the “coin of the realm”
Research is critical for PM&R Residency Program Survival
Residency Programs are Required to have Scholarly Activity by the ACGME and the PM&R RRC
No Research = No Residency Program
Research is critical for PM&R Practice
Outcome Studies are key to practice survival
Randomized controlled trials (RCT’s) Almost no other kind of research is taken seriously
Uncontrolled research is only a pilot study, at best
Laboratory moving closer to the bedside
New emphasis on Evidence Based Medicine in Health Care Reform
Research is critical for PM&R Field Survival
Research is our “R&D”
Most of the treatments you learn to do in the residency will be out of date in 10 years or less (I am a PGY-43)
Without research, we can’t be part of a medical school and have residencies
Without residencies…we will cease to exist in a few years
Few Physiatrists Have Become High Quality Researchers
WHY?
Length of training required
Debt level problem
Perceived decrease in research funding
Instability in research funding
Monetary rewards of clinical practice
Physiatric personality
PM&R and Research: Problems
We began and continue as a clinical field Lots of art; but less science and research
Shortage of physiatrists We have spent most of our time on clinical
practice: meeting the demand
Physiatric personality People oriented rather than rat oriented
Lieberman, 1993
It has also been generally agreed that Rehabilitation research has not done well in fulfilling its objective of providing a foundation of knowledge for rehabilitation practice. K-12 Application, Association of Academic
Physiatrists, 1993
Few Physiatrists Become High Quality Researchers
Actually, this is a trend in all fields, beginning in the 1960’s
From 1968-1980, the number of physician post-doctoral research fellows at the NIH fell from 4100 to 1700
Decrease in physicians getting grants from the NIH has been paralleled by an increase in PhD grantees

Few Physiatrists Have Become High Quality Researchers
Why? Academic departments failed to provide
nurturing environment for researchers
Pressure in academic departments to provide clinical revenue
Difficulty obtaining protected research time
Mentors aren’t funded researchers
Only 1.3% of PM&R academicians have had an NIH grant
SPECIAL PROBLEMS FOR US
Lack of recruitment and retention of Physiatrists into academic careers
Insufficient time spent by academic physiatrists on research
Low levels of grant applications and external funding
Lack of research training
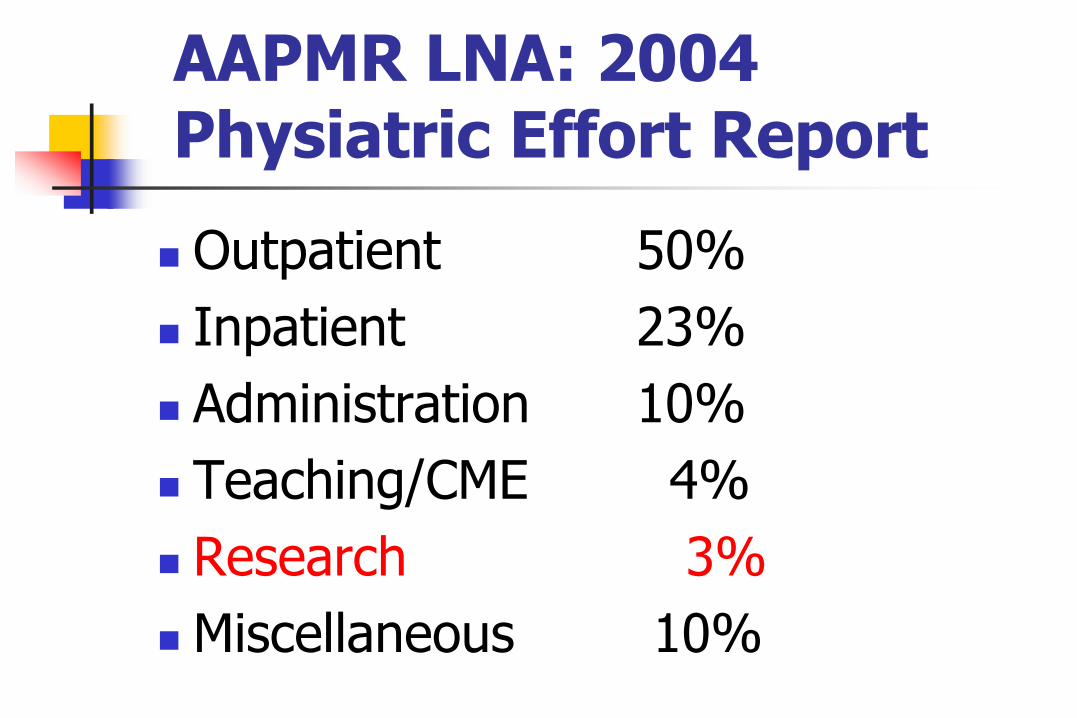
AAPMR LNA: 2004 Physiatric Effort Report
Outpatient 50%
Inpatient 23%
Administration 10%
Teaching/CME 4%
Research 3%
Miscellaneous 10%
EBM and Spinal Injections
EBM will ultimately determine billing for spinal injections
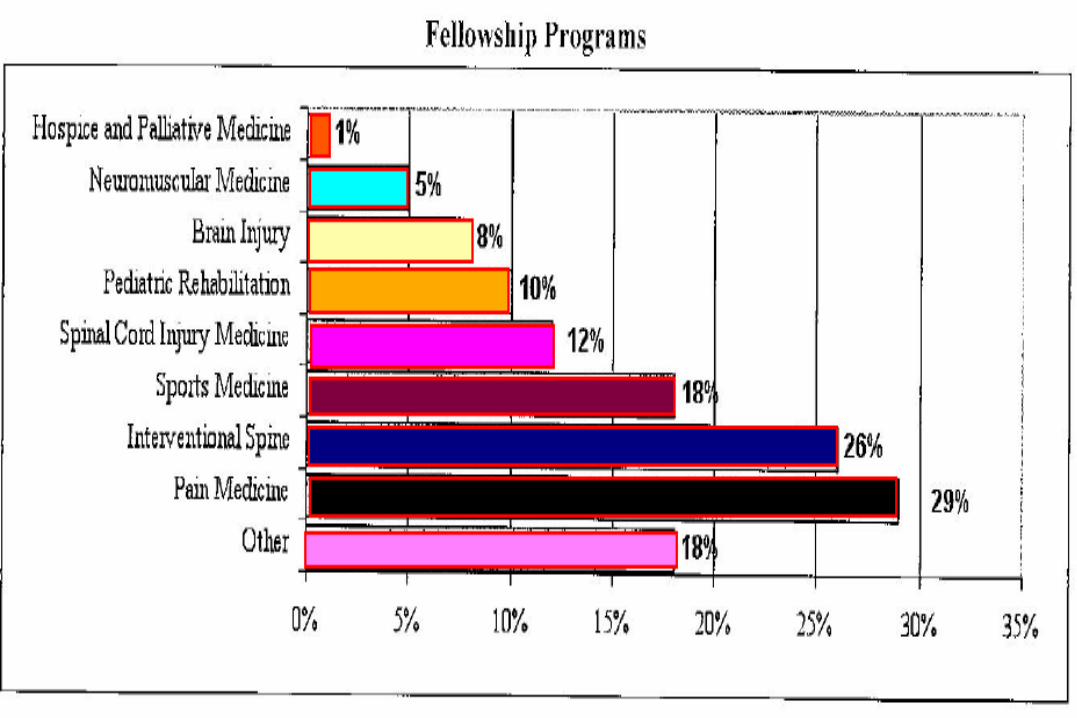
Currently a massive trend toward physiatrists taking fellowships in Pain Medicine/Spinal Injections
Physiatrists As Spinal Interventionalists
CMS says that physiatrists had an 838% increase in epidural, Z-joint and SI joint injections in last 8 years
Anesthesiologists had an even higher percentage increase in injections
Medicare interventional spinal procedures increased by 169%
CMS recently slashed payments for spine injections

Trend: More Capitated Care
Capitated care will grow But grow more slowly
Change due to market forces Example: Many policies requiring a referral
are not competitive now
Fail to take over all Medicare patients
Why won’t private Medicare plans take over Medicare?
They are too expensive. (Forbes April 21, 2008)
Private Medicare Plans Too Expensive
Supposed to save 5%; but cost 12% more
They are a pain to doctors and hospitals
Physiatric Compensation will vary by region
% of patients insured by MCOs
Limits on worker’s comp payments
Limits on auto insurance patients
INCOME ENHANCING ACTIVITIES
Electrodiagnostic Procedures
Spinal Injections
Facility Ownership
Management Roles
Niche programs MVA’s
WC
Medicolegal Adapted from John Melvin
FUTURE CONPENSATION TREND PREDICTIONS (by John Melvin)
Increase in Relative Payment for E&M Codes
Procedures
Limits on use
Reduced Payment
Result: More Focus on Patient Management, Less Emphasis on Procedures
Prediction: Physiatric Income Will Continue to Grow
Due to shift to techniques and away from E&M
Aging population

WHAT WILL OUR PRACTICE ACTIVITY BE IN THE FUTURE?
What Will Our Practices Look Like in the Future?
More musculoskeletal/outpatient?
More procedures?
More rehab/inpatient?
YES

Let’s Look At the Current Physiatric
TRENDS
ABPMR CERTIFICANTS
About 10,000 certified
Adding about 400 per year

The Trend is Clear PM&R is becoming
Less Inpatient Rehab
More Outpatient Musculoskeletal
Field Creep
Into Anesthesiology
My Survey: INJECTIONS DURING RESIDENCY?
Question: Should we teach injections in residency rather than in a fellowship?
YES 5
NO 6
JOBS IN THE FUTURE ?
Survey: DO YOUR RESIDENTS NOW JOIN ORTHO GROUPS?
Question: What percentage of your residents now join orthopedic groups?
22%Range from 10-40%
Survey: SENTIMENT FROM ONE CHAIR
On residents joining Orthopedic groups:
“This is a sin against humanity!!”
Survey Responses: RESIDENTS FINDING JOBS?
QUESTION: Are your residents finding jobs now as easily as they were a decade ago?
YES 9
NO 1
PREDICTION
Physiatrists will practice in larger groups Working for HMO’s
Working for Physician Multi-specialty Practices
Employed by Hospital Networks
Fewer will be in private practice
PredictionThe trend to large groups will continue because of
Economies of scale/Market Power
Life style issues
Referral patterns
But “pioneer personalities” or “entrepreneur personalities” will attempt solo practice
Especially the “injectionists”
Prediction about Jobs
Jobs will be plentiful in the next decade
Fellowship trained will have an advantage
Toughest markets will be around training centers
Because of Newton’s Law of Inertia
Smaller towns and suburbs will have the most openings
Future # of Residents ?
How many residency positions will we have in the future?
Will there be PM&R residency positions in the future?
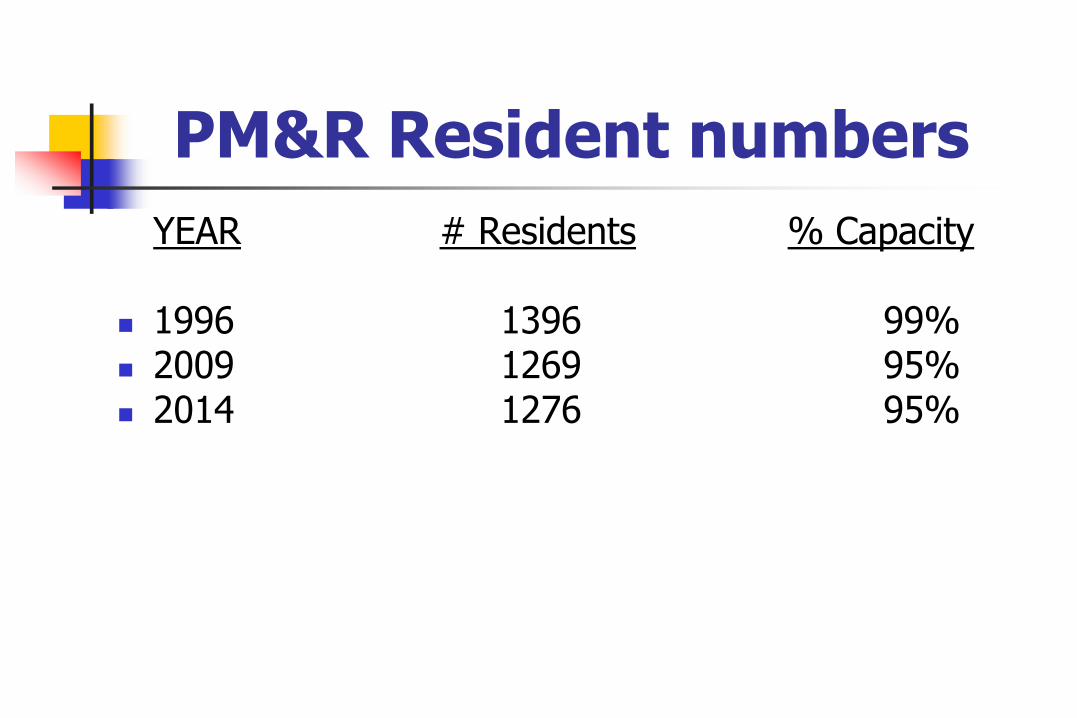
PM&R Resident numbers
YEAR # Residents % Capacity
1996 1396 99% 2009 1269 95% 2014 1276 95%
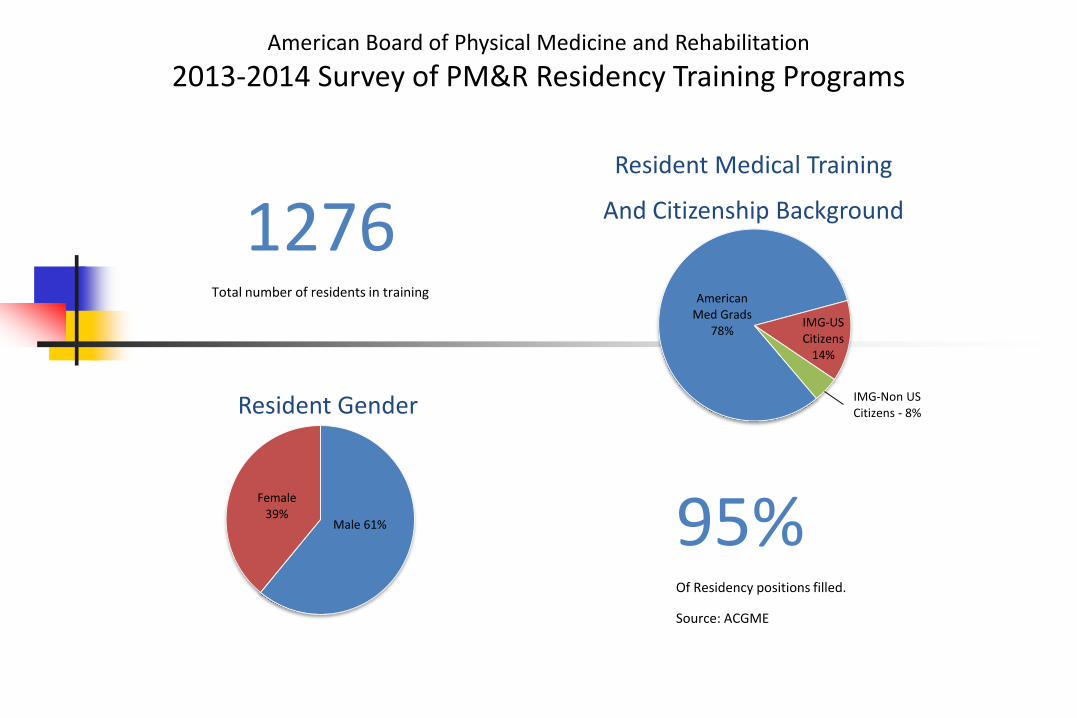
American Board of Physical Medicine and Rehabilitation
2013-2014 Survey of PM&R Residency Training Programs
1276Total number of residents in training
Male 61%
Female 39%
Resident Gender
95%Of Residency positions filled.
Source: ACGME
IMG-US Citizens
14%
IMG-Non US Citizens - 8%
American Med Grads
78%
Resident Medical Training
And Citizenship Background
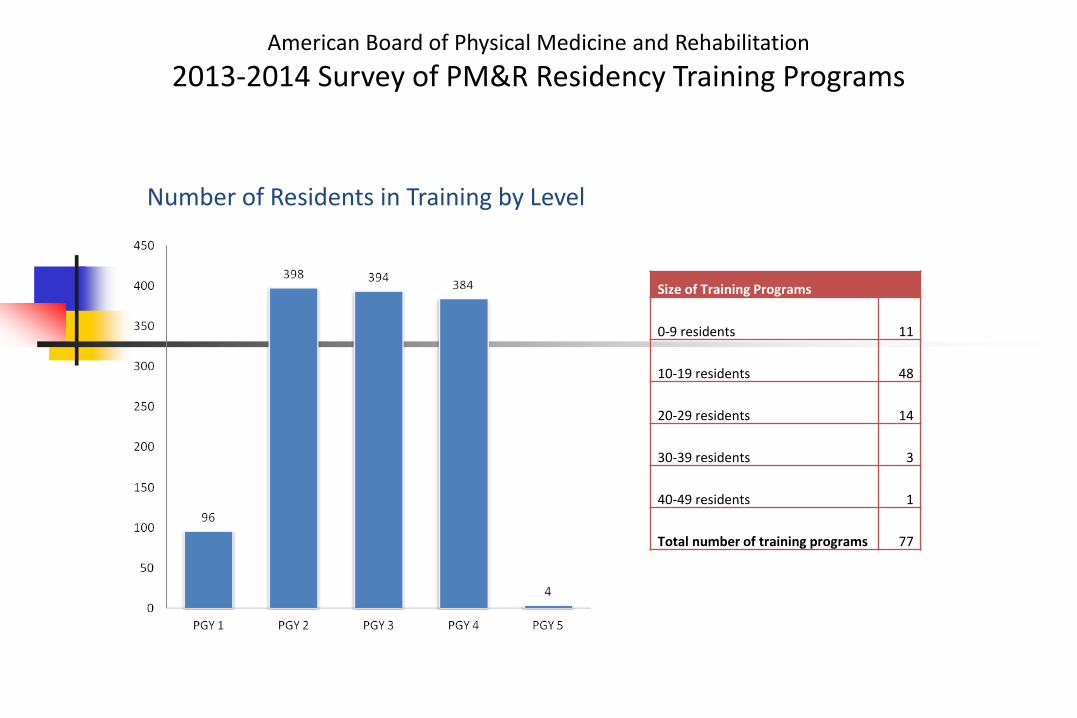
American Board of Physical Medicine and Rehabilitation
2013-2014 Survey of PM&R Residency Training Programs
Number of Residents in Training by Level
Size of Training Programs
0-9 residents 11
10-19 residents 48
20-29 residents 14
30-39 residents 3
40-49 residents 1
Total number of training programs 77
Predictions about PM&R Residents in Next Decade
More GME funding
More Restrictions on Recruiting IMG’s
Tougher RRC rules for having a program
More Residents More women residents
Fewer IMG residents
Predictions on Residency Programs
CMS will eventually increase GME funding to allow more residency positions
# of PM&R departments will increase by 5-10 in the next decade
Physician Workforce in USA Not Increasing Yet
Physicians are getting older
Only 16,000 medical students/year
With retirements the # of physicians might drop by 2020
US Health and Resources Administration says we will be 155,000 doctors short in 2020
Doctors not working as many hours now
One-fourth of US doctors in practice are IMGs
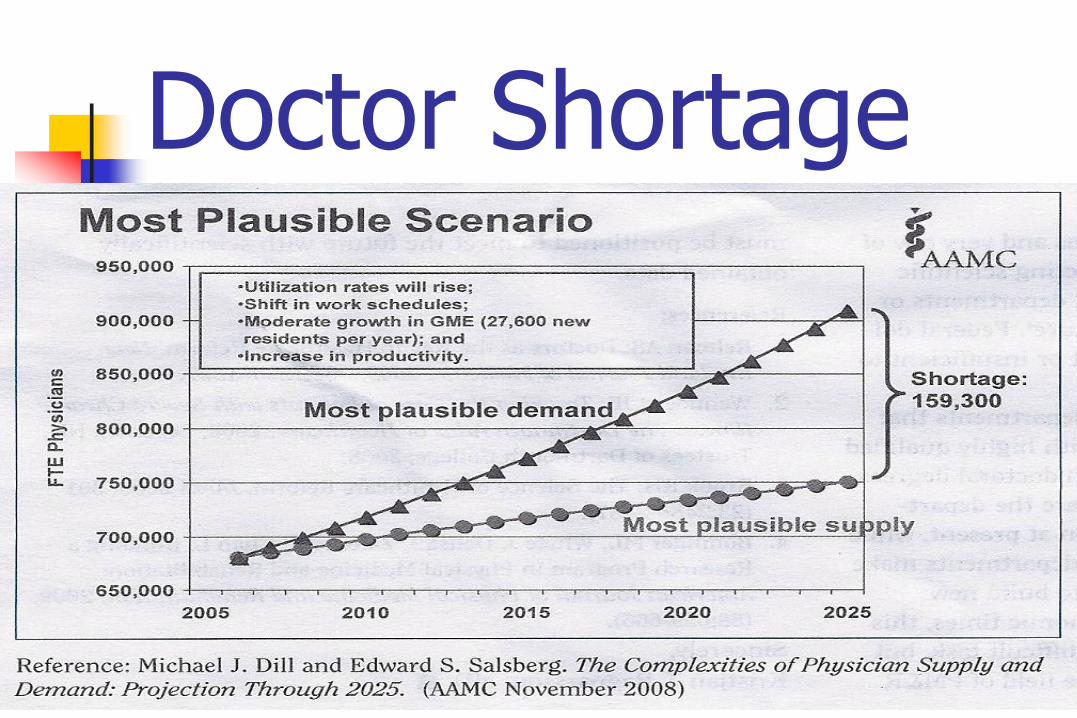
Doctor Shortage
Prediction on Medical Students
More medical students in the next decade
AAMC has changed its stance on physician workforce
We have 680,000 FTE of physicians in USA
AAMC says that by 2025 we will be short 159,000 to 300,000 FTEs
Physiatric Workforce
AAP asked the AAMC’s Center for Workforce Studies to examine trends impacting PM&R in the future
Salsberg E, Erikson C. Am J Phys Med Rehabil 2007; 86:838-844.
Physiatric Workforce We are a young field and our mean age
is younger than other fields
Only 22% of physiatrists are over 55
7700 practicing physiatrist now
Growing by about 400/year
Saturation ranges from 1/100,000 in Mississippi to 5/100,000 in NY
Demand for Care Rising
US population growing 25 million/decade
Over 65 group will double 2000-2030
Elderly use twice the physician services
Doctor visit rates for elderly increasing
Medicine can do more for them now
Elderly have high expectations of what we can do for them
Living longer
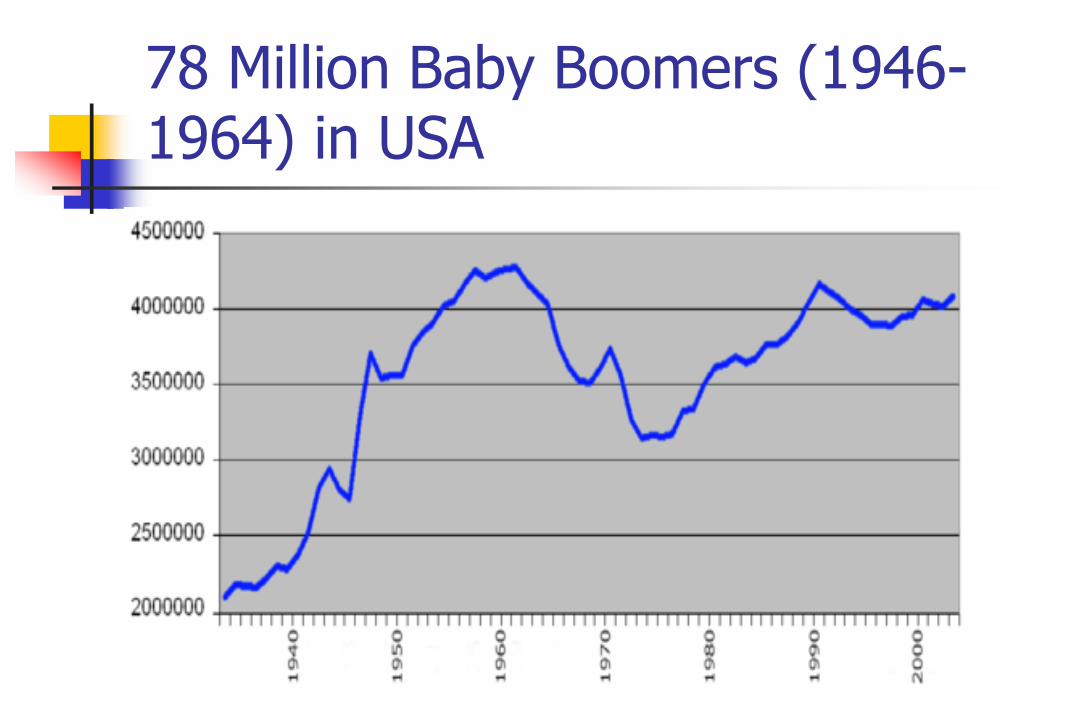
78 Million Baby Boomers (1946-1964) in USA
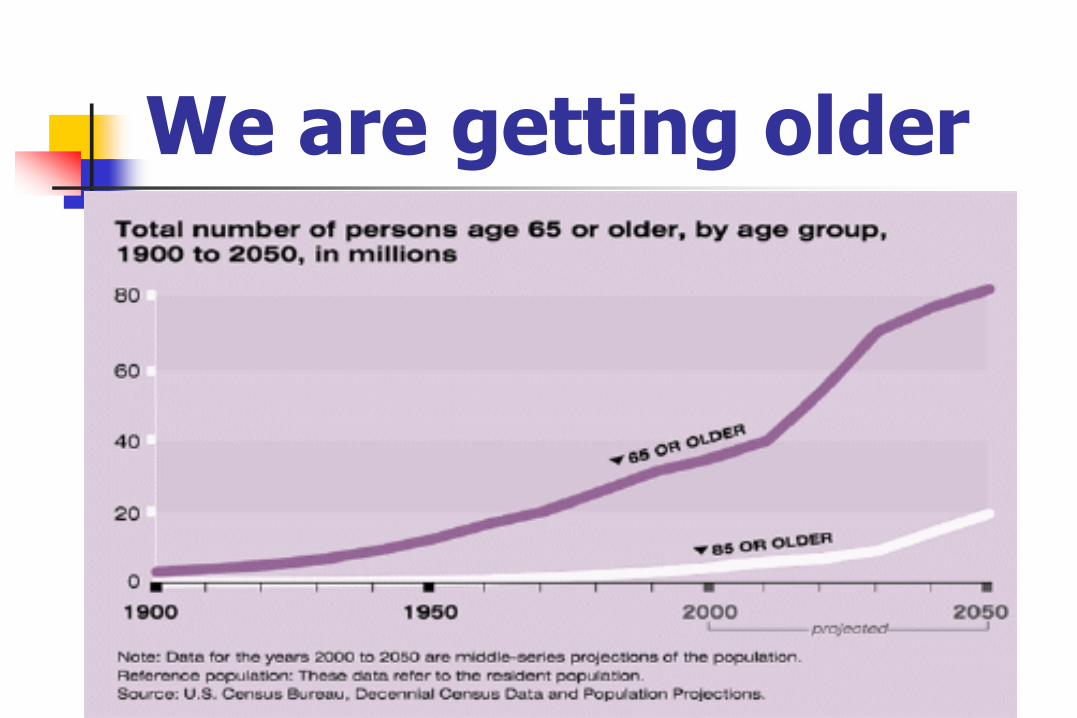
We are getting older
Social Security & Medicare on course to run out of money
The good news:
Medicare and Medicaid costs decreasing
Medicare Trust Fund will be solvent until 2026
This has improved lately from 2024
Social Security solvent until 2033
Treasury Secretary Jacob Lew says both are on “unstainable paths”
2014 ABPMR Subspecialty Exams for Physiatrists
Sports Medicine
Neuromuscular Medicine
Pain Medicine
Hospice and Palliative Medicine
Pediatric Rehabilitation Medicine
Spinal Cord Injury Medicine
Brain Injury Medicine
Randy’s Fellowship Prediction
The number of fellowships will grow dramatically in the next decade
Eventually we will look like the Internal Medicine model for fellowships
What Will We Call Ourselves in the Future?
Our Name Has Changed Before
Krusen initially originally called himself a “physical therapy physician.” Krusen coined “Physiatrist” when physical
therapists took our name
We became PM&R in 1947
PASSOR wanted name changed when they first formed
Younger physiatrists not happy with “PM&R”
Internationally we are PRM
The International Society when formed a few years ago went with:
ISPRM
International Society of Physical and Rehabilitation Medicine
Prediction on Name
Name of the field will change to Musculoskeletal & Rehabilitative Medicine in the next decade
The term “Physical Medicine” will have only historic interest
The terms “Physiatry/Physiatrist” will continue in use
Maybe we should be called
PM&R
Pain Medicine & Rehabilitation

New Wrinkle in our Future
Health Care Reform
OBAMACARE
Patient Protection and Affordable Care Act
Reform Provisions 2010-2011
Pre-existing Condition Insurance Plan
Adult Dependent Coverage to Age 26
Consumer Protections in Insurance No lifetime limits on dollar value of coverage
Rescinding coverage except in case of fraud
Denying children with pre-existing conditions
Reform Provisions 2010-2011
Medicare Independent Payment Advisory Board 15 members appointed by President and
approved by the Senate
They design a plan to reduce per capita growth in Medicare spending if spending exceeds targeted growth rate (Begins Oct. 1st)
HHS has to abide by this plan unless Congress passes its own plan that has equal savings
Reform Provisions 2010-2011
Medicaid Long-Term Care Services
Fed matching payments to increase services including attendant support services to people with disabilities

Health Reform for 2012
Reduced Medicare Payments for Hospital Readmissions
Health Reform for 2013
Medicare Bundled Payment Pilot Program
National Medicare Pilot Program making bundled payment for acute to post-acute services for an episode of care
Medicaid Payments for Primary Care
Increased Medicaid payment for primary care by primary care doctors to 100% of Medicare rate for 2013 and 2014
Health Reform for 2013
Itemized Deductions for Medical Expenses Increases from 7.5% of AGI to 10% threshold to
claim medical deductions for those <65 years
Medicare Tax Increase 0.9% to 2.35% for earnings over $200,000 and
3.8% on unearned income for high income taxpayers
Tax on Medical Devices Fed. Excise Tax of 2.3% on sale of device
Health Reform for 2013
CO-OP Health Insurance Plans
Encourages development of non-profit member-run health insurance companies
Extension of CHIP to 2015
Health Reform for 2014
Individual Requirement to Have Insurance
All US citizens and legal residents must have qualifying health coverage. (January 1, 2014)
There is a phased in tax penalty for those without coverage, with certain exceptions
Who Doesn’t Have to Have Insurance?
Non-documented aliens
Incarcerated
Members of Indian Tribes
No access to affordable health plan
If it costs 8% or more of income
Religious objection to health insurance
Income low enough that no tax filing required
Hardship exemption: Can apply for this
Paying if You Don’t Have Insurance (starts 2014)
Health insurance providers have to provide proof of coverage to file with your income taxes
If no proof of coverage, penalty will be assessed on taxes
Penalty will gradually increase from 1% of income in 2014 to 2.5% in 2016
Health Reform for 2014
Health Insurance Exchanges
Exchanges administered by government agency or non-profit organization
Individuals and small businesses up to 100 employees can purchase coverage
Health Reform for 2014
Expanded Medicaid Coverage
Any US citizen or legal resident not on Medicare under age 65 with income below 133% of FPL is eligible for Medicaid
Presumptive Eligibility for Medicaid
All hospitals to make presumptive eligibility determinations for Medicaid
Health Reform for 2014
Health Insurance Premium and Cost Sharing Subsidies
Those 133-400% of FPL can purchase insurance through the exchanges with premium subsidies and tax refunds and tax credits
2% of income limit for 133% of FPL and 9.5% for 300-400% FPL
Guaranteed Availability of Insurance
Insurance regardless of health status
Rating: Cost variation can be based only on age, geographic area, family composition, and tobacco use
Ratings have proportion limits
Health Reform for 2014
No Annual Limits on Coverage
Essential Health Benefits
Creates 4 categories of plans to be offered through the exchanges
Temporary Reinsurance Program
Collects payments from health insurers to provide payments to plans that cover high-risk individuals
Health Reform for 2014
Employer Requirements
>50 employees: $2000 fee per full time employee not offering health plan coverage
Medicare and Medicaid Disproportional Share Hospital Payments
Reduces this by 75% for Medicare and increases payments based on % uninsured and amount of uncompensated care
Medicare Payments for Hosp.-Acquired Inf.
Reduces Medicare payment by 1%
Health Reform for 2015
Increase Federal Match for CHIP

Health Reform for 2016
Health Care Choice Compacts States can form health care choice compacts and
insurers can sell policies in any state participating in the compact
Health Reform for 2017
No changes
Health Reform for 2018
Tax on “Cadillac” Insurance
Puts excise tax on insurers of employer-sponsored health plans with aggregate expenses that exceed $10,200 per person and $27,500 per family.
2019: The End Result of HR
2019: 32 million more with have health insurance
CBO: Estimates $938 Billion cost from 2010-2019
Illegal Aliens and International Tourists still not covered
How Will It Be Paid For? Fee on health insurance companies
Fee on pharmaceutical industry
Sales tax on medical devices
Increase in Medicare tax on high earned or unearned income individuals
Tax on Cadillac health plans
Penalties on employers who do not provide
Penalties on individuals who do not purchase
Will Health Reform Increase the Deficit?
CBO says it will save 124 Billion dollars over 10 years.
Different Types of Plans
Employee-provided
Other Private
Public Exchange Plan
Medicare
Medicaid
CHIP
On Balance HCR will (in my opinion)
Get us paid by more of our patients
Increase the # of our patients
Force us to be more competitive in our rates
Make it more difficult to be in solo practice
Force us to prove that our treatments actually work
Will have a net neutral effect on our institutions (rehab centers in particular)
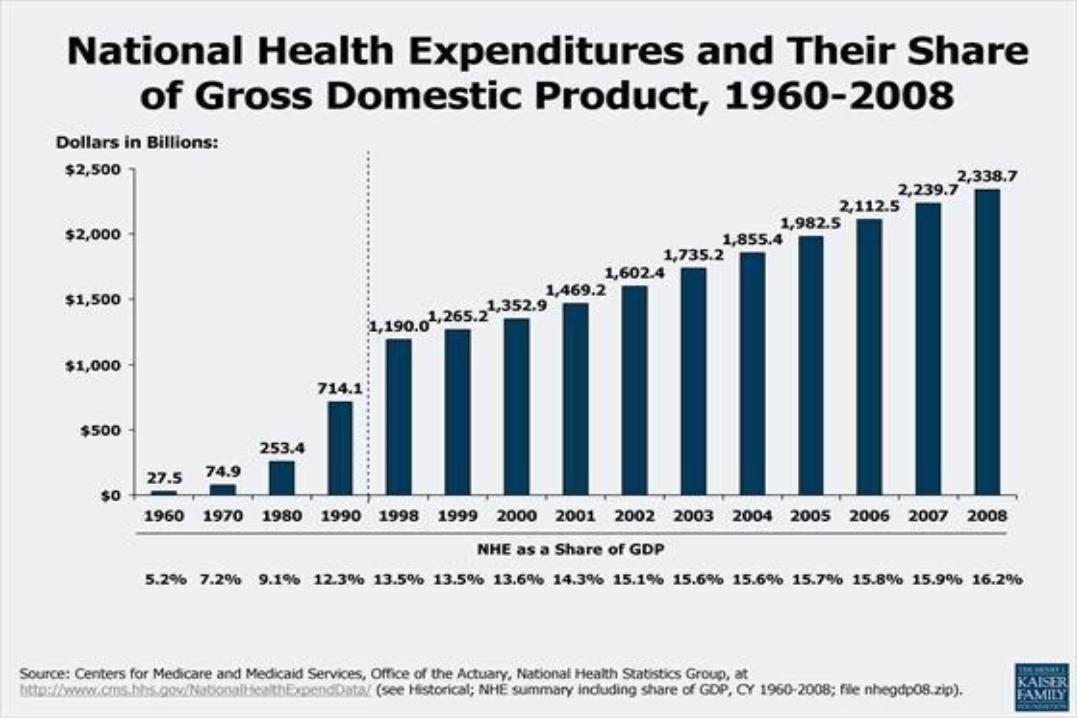
Rise in Health Costs Now Slowing
***USATODAY.com Breaking News***
Health care costs rose by only 1.3% a year between 2010 and 2013, a new report from the White House Council on Economic Advisersshows. That's the lowest increase in a three-year period on record. White House officials cite the 2010 Affordable Care Act as a main factor in lowering costs.
The Changing Reality of Medicine
Specialties continue to take a hit in billing.
Bundling of charges is continuing
CMS reductions
Radiology codes slashed 12 times in six years
Cardiology procedures cut by 25%
Opthalmology cut by 20%
CMS cuts in EMG and NCS have affected us the most
2011: RANDY’S PREDICTION
Like our physiatric predecessors, we will successfully adapt PM&R to new impairments and legislation
Major Problems we have already overcome Polio decline Loss of Long Length of Inpatient Stays TEFRA Caps on Inpatient Stays Advent of DRG exemption Increased Orthopedic Implant surgery
PACE OF CHANGE WILL CONTINUE TO ACCELERATE
You’ll have more of that “just hanging by a limb feeling”
Predictions of the future will be useful for shorter and shorter periods
The Future: Don’t let it get you down!
Remain upbeat
Remain flexible
Learn more about medical business
Stay up with the trends in the field
Keep up your competence
RANDY’S MOOD IS UPBEAT
No field is more interesting than medicine
PM&R has great flexibility...it will bend rather than break
In a democracy, people eventually get what they want, and they want better medical care
The managed care era will evolve into a better form of medical care over the next decade
PM&R IS A GREAT FIELD!
Small (10,000) Not limited by an organ Jobs of all types available Population demographics favor us High income/life style ratio Good balance of procedure/E&M Many academic opportunities Good physiatric profile/nice people Patients appreciate what we do
RANDY’S CONCLUSION
The future belongs not to those who try to predict it, but to those who make it.
What future do you want for yourself, your family, your field?
How do you plan to achieve it?





























