Embed Size (px)
Citation preview

The Future of Health Care
Matthew Morgan MD, MSc, FRCP(C), FACPVice President, Patient Experience and Outcomes,
Mount Sinai Hospital, Toronto, Canada

A significant health system challenge
50% of adults live with chronic illness 80% of adults over age 65 have a chronic
disease 60% of hospitalizations are due to chronic
disease 2/3 of medical admissions via emergency
are due to exacerbation of a chronic disease
80% of family doctor visits are chronic disease-related
60 to 80% medical costs are related to chronic disease
Chronic diseases constitute a significant burden and are not being managed well.
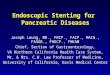
… and the quality of care varies substantially
11
68
73
76
65
58
49
45
0 25 50 75 100
AlcoholDependence
Diabetes Mellitus
Hyperlipidemia
COPD
Hypertension
Coronary ArteryDisease
Prenatal Care
Breast Cancer
Percentage of recommended care received (US data)
Source: McGlynn et al. NEJM 2003
The Health Care Gap: Evidence reveals a significant gap between recommended care and care actually delivered.

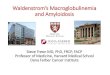
Diabetes care in six countries
Patients with chronic diseases do not receive recommended health care.
Indicator
CAN
%
AUS
%
NZ
%
UK
%
US
%
GER
%
A1C in last 6 mos. 90 86 79 85 90 91Feet exam in last year 52 57 66 75 70 65Eye exam in last year 73 73 66 83 69 85Cholesterol checked in last year 91 93 87 92 92 95
All 4 services received In last year 38 41 40 58 56 55
3
Source: Schoen et al. (2005) “Taking the pulse of health care systems: experiences of patients with health problems in six countries.” Health Affairs.

4
The Chronic Care Model requires system transformation, physician leadership and high performance team work.
Source: www.improvingchroniccare.org

5
Physicians, Health Care Organizations and Patient Populations must be effectively organized to deliver integrated health care.
Health Care Trends• Shift in focus from acute care to community
– Acute care facilities no longer sole decision-makers
• Single accountability for the well-being of a region’s population health
– Improved integration of health services between provider organizations
– Significant consolidation of services, resulting in increased purchasing power
– Further consolidation to continue within/between health regions
• Increased need for an EHR to support integration across the continuum of care
Health Care Organizations
Health Care Providers
The future of health care requires integration and coordination of general community, health care organizations and health care providers
Implications
• Need population-based health regions with the integrated leadership, structure and authority to drive large-scale health care improvements
• Need to enable primary care reform to support population-based health care delivery
• Need a smart informatics approach with a longitudinal EHR
• Need to incent high performance teams to deliver high quality, safe, efficient care
• Need to engage patients in the design, delivery and improvement of health care delivery
Community

6
Successful physician engagement is an art, science and essential skill for health care managers and leaders.
www.ihi.org

To establish a successful performance improvement program, three elements are required.
7
Data Skills
Planning & Incentives
Analytical capabilities to interpret and use data for
identifying, prioritizing and implementing operational
improvement interventions
Access to timely, high quality data that can be
analyzed and interpreted
Integration of performance improvement targets and accountabilities into operational plans, performance objectives and incentive programs
Using data to inform and monitor performance improvement activities must be embedded in management structures and processes
Performance Improvement Methodology

There are some common pitfalls that inhibit leaders from effectively using information to drive performance improvement.
8
Improvement efforts run in parallel to line management structures responsible for operations
• Improving performance is seen as additional work, above and beyond standard management responsibilities
• Line managers are not held accountable for performance improvement in their departments
• Individual incentives are not aligned with ability to improve performance
The content of reports is based on what data is available, not what actions need to be informed
• Many reports are generated, but few are regularly used to drive decision making and management action
• The indicators reported are not linked to performance improvement objectives
• Poor data quality renders some reports unusable
Reports are generated, but data is not thoroughly analyzed and interpreted
• Point-in-time graphs and charts are created, but few actually present data that enables managers to draw conclusions and plan and implement interventions to improve performance
• Content of the reports is useful, but there is a lack of skill in interpreting and using the data to prioritize and implement interventions to improve performance
Finger pointing ensues when performance is poor
• Focus is on blame for poor performance, rather than on identifying opportunities to improve
• Accountability for moving the performance of an indicator is not assigned to any one individual
• Accountability for performance is assigned to individuals that do not have the authority/capability to affect an indicator

Diabetes Patient RegistryA Case Study in Physician Leadership
(people, processes and technology)
9

Context
• A large New York public healthcare system, consisting of 11 acute care hospitals and providing services to nearly 1.3 million people, established as a priority, the provision of better care to chronic disease patients
• Develop a chronic diseases patient registry and manage its implementation through stakeholder engagement, workflow assessments and software development
• In partnership with management, IT, physicians and the clinical teams developed a system:
– Generates call lists for providers to contact high-risk patients who are not receiving care based on clinical best practices
– Issues reminders to patients by automatically generating letters
– Provider reports that support improved management of chronic diseases
– Facility and system-level reports to support population-based planning for services, care models and resource allocation
10
The objective was to identify and remove care gaps in the management of chronic diseases and issue reminders to patients and providers.

Performance indicators were established for each chronic disease by a consortium of clinicians, led by physicians.
11

12
Benchmarking data are provided to physicians and care teams as well as care gap reminders.
• Care teams are provided with peer benchmarking data to ensure consistency of care
• The comparative data must be presented in a manner that’s easy to understand
• Each care team manages the list of their patients with chronic diseases
• Reminders are provided to care teams and automatically mailed to patients to support management of their care

13
Indicators are summarized at a facility and system-level to monitor performance and support target setting and accountability agreements.
Care Team-Level Indicators
Facility-Level Indicators
Network-Level Indicators

20
30
40
50
60
70
80
90
100
150
200
250
300
350
Dec-05 J an-06 Feb-06 Mar-06 Apr-06 May-06 J un-06 J ul-06 Aug-06 Sep-06 Oct-06 Nov-06
User Enrollment
Use
r Enr
ollm
ent
Uni
que
Use
r Log
ons
per m
onth
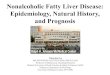
Patient Registry User Enrollment and Utilization
• In the first six months• User enrolment increased by 33%
• 10% month over month average increase in unique user logons
Reporting physician engagement over time helps ensures adoption.
14

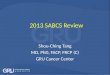
• The ten care teams who used the diabetes patient registry most frequently had a higher percentage of their diabetic patients receiving care according to clinical best practices
Comparison of Average Diabetes Indicators for Top Ten Physicians’ Care Teams versus All Care Teams
Increased use of the diabetes registry correlates to improved patient care.
HbA1c LDL BP0%
10%
20%
30%
40%
50%
60%
30%
57%
30%23%
43%
22%
Top 10 Users Care Teams All Care Teams
Diabetes indicators
Perc
ent d
iabe
tic p
atien
ts m
eetin
g cr
iteri
a


A Physician’s Perspective: To improve quality and decrease cost, the four roles of the doctor must be separated and disrupted by innovation.
Diabetes / Depression / Obesity
Level 1 Quality: Reliable performance Level 2 Quality: Convenient, affordable and responsive
Innovator’s Prescription, A Disruptive Solution for Health Care, Christensen 2009, Figure 4.1, p. 113
› Skill and judgment (specialist)› Scientific advancement› Disrupt with centres of excellence› eHealth enabled with e-referral,
synoptic data analysis, data mining, networks, tele-consult
› Reimburse with fee for service
Osteosarcoma / Epilepsy / Rare diseases
› Disrupt with onsite technology› Disrupt with solution shops and value
add processes› eHealth enabled by CRM, population-
based registries› Reimburse with fee for membership /
service as well as pay for outcomes
Immunizations / Cancer Screening
› Disrupt with retail clinics and solution shops
› Disrupt with application of E.B.M.› eHealth enabled by AI (protocols,
pathways, CDS), telemedicine› Reimburse with fee for service + / -
pay for outcomes
Cataract Surgery / Inguinal Hernia / M.I.
Rules-based precision medicine
Wellness and
preventive health
Doctor
Intuitive medicine
Oversight of chronic disease
› Disrupt with network facilitated business models
› eHealth enabled by CDS, registries, tele-health, PHRs
› Reimburse with fee for membership / service as well as pay for outcomes

Engage patients and families as partners in the design, delivery and improvement of patient care
Create and sustain a culture in which all express ownership and responsibility for the experience
Understand Deliver
Deliver a patientexperience that exceeds expectations
Understand the patient experience through meaningful engagement
Patient-Family Experience
Measure the patient experience and recognize value and achievement
Enhance thepatient experience through best practices and innovation
Enhance
Measure
Patient and Family Centered Care