Embed Size (px)
Citation preview

Waldenstrom’s Macroglobulinemia and Amyloidosis
Steve Treon MD, PhD, FRCP, FACPProfessor of Medicine, Harvard Medical School
Dana Farber Cancer Institute

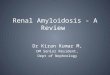
Manifestations of WM Disease
≤20% at diagnosis;50-60% at relapse.
↓Hb>>> ↓PLT> ↓WBC
Hyperviscosity Syndrome:Epistaxis, Headaches
Impaired vision>6,000 mg/dL or >4.0 CP
Treon S., Hematol Oncol. 2013; 31:76-80.
Cold Agglutinemia (5%)Cryoglobulinemia (10%)IgM Neuropathy (22%)Amyloidosis (10-15%)
Hepcidin ↓Fe Anemia
Bone Marrow
Bing NeelSyndrome

Primary Therapy of WM with RituximabRegimen ORR CR TTP (mo)
Rituximab x 4 25-30% 0-5% 13 Rituximab x 8 40-45% 0-5% 16-22Rituximab/thalidomide 70% 5% 30Rituximab/cyclophosphamidei.e. CHOP-R, CVP-R, CPR, CDR
70-80% 5-15% 30-36
Rituximab/nucleoside analoguesi.e. FR, FCR, CDA-R
70-90% 5-15% 36-62
Rituximab/Proteasome Inhibitori.e. BDR, VR, CaRD
70-90% 5-15% 42-66
Rituximab/bendamustine 90% 15-20% 69
Reviewed in Dimopoulos et al, Blood 2014; 124(9):1404-11; Treon et al, Blood 2015; How I Treat WM

Agent WM Toxicities
Rituximab • IgM flare (40-60%)-> Hyperviscosity crisis, Aggravation of IgM related PN, CAGG, Cryos.
• Hypogammaglobulinemia-> infections, IVIG • Intolerance (10-15%)
Fludarabine • Hypogammaglobulinemia-> infections, IVIG• Transformation, AML/MDS (15%)
Bendamustine • Prolonged neutropenia, thrombocytopenia(especially after fludarabine)
• AML/MDS (5-8%)
Bortezomib • Grade 2+3 Peripheral neuropathy (60-70%); High discontinuation (20-60%)
WM–centric toxicities with commonly used therapies

Mutated MYD88 Pro-Survival Signaling in WMMYD88 mutated in 93-97% of WM patients
Treon et al, NEJM 2012Yang et al, Blood 2013Yang et al, Blood 2016
Degradation
TLRs IL-6
IL-6
IL-6
IL-6R
gp-130
growth survival
IL-6
mTOR
ERK1/2
HCK
NFKB
MYD88
BTKIRAK1/4
AKT
ibrutinib

Drug resistance
Bone Marrow Stroma
CXCR4 mutations permit ongoing pro-survival signaling by CXCL12, the ligand for CXCR4 receptor
CXCR4 is mutated in 30-40% of WM patients
CXCR4
WM Cell
CXCL12
Hunter et al, Blood 2013; Cao et al, Leukemia 2014; Roccaro et al, Blood 2014.
CXCR4 receptor remainsup with mutation

Multicenter study of Ibrutinib in Relapsed/Refractory WM (>1 prior therapy)
✔ MYD88, CXCR4 Mutation Status
Treon et al, NEJM 2015NCT01614821
R Advani L PalombaS. Treon PI

ALL MYD88Mut
CXCR4WTMYD88Mut
CXCR4MutMYD88WT
CXCR4WTP-value
N= 63 36 21 5*
ORR 90% 100% 86% 50% <0.001
Major (>PR) 78% 97% 64% 0% <0.001
VGPR 29% 44% 9% 0% <0.001
Time to Minor Response (mos.)
1.0 1.0 1.0 1.0 0.10
Time to Major response (mos.)
2.0 2.0 6.0 N/A 0.05
Responses to ibrutinib are impacted by MYD88 (L265P and non-L265P) and CXCR4 mutations.
One patient had MYD88 mutation, but no CXCR4 determination and had SD.
Treon et al, ICML 2019Median follow-up: 47.1 months

OIbrutinib in Previously Treated WM: Updated PFS
5 year PFS: 54%5 year OS: 87%
All patients MYD88 and CXCR4 Status
MYD88 MUTATED ONLY
MYD88 AND CXCR4 MUTATED
NO MYD88 OR CXCR4 MUTATIONS
Treon et al, ICML 2019
5 yr 34%
5 yr 71%

★
Adverse Events related to ibrutinib monotherapy
Number of Subjects with Toxicity
• No impact on IGA and IGG immunoglobulins
Update on Adverse Events (Grade >2) in >5% of patients: Neutropenia (22%);Thrombocytopenia (14%), Pneumonia (9%); GERD (8%); Hypertension (8%); anemia (6%); andskin infection (5%). Seven patients (11%) had atrial arrhythmia [Grade 1 (n=1); Grade 2 (n=5);Grade 3 (n=1)], and 6 continued ibrutinib following medical management.
5% to 11% with longer follow-up
22% (No change)
14% (No change)
2% to 8% with longer follow-up
Minimal changes in serum IGG, IGA during course of treatment.

R
Ibrutinib Monotherapy in Symptomatic Treatment Naive WM
✔ MYD88, CXCR4 Mutation Status
Treon et al, JCO 2018NCT02604511

Time to and depth of response to ibrutinib are impacted by CXCR4 mutations.
All Patients MYD88MUT
CXCR4WTMYD88MUT
CXCR4MUT P-value
N= 30 16 14 N/AOverall Response Rate-no. (%)
30 (100%) 16 (100%) 14 (100%) 1.00Major Response Rate-no. (%)
25 (83%) 15 (94%) 10 (71%) 0.16
Categorical responsesMinor responses-no. (%)
5 (17%) 1 (6%) 4 (29%) 0.16Partial responses-no. (%)
19 (63%) 10 (63%) 9 (64%) 1.00Very good partial responses-no. (%)
6 (20%) 5 (31%) 1 (7%) 0.18
Median time to response (months)Minor response (≥Minor response)
1.0 0.9 1.7 0.07Major response (≥Partial response)
1.9 1.8 7.3 0.01
Median f/u: 14.6 months 18 mo. PFS: 92% Treon et al, JCO 2018

Frontline Ibrutinib: Adverse Events (>5%)
Event or Abnormality Grade 2 Grade 3 Grade 4 Total
Grades 2-4Arthralgia 2 (7%) 0 (0%) 0 (0%) 2 (7%)
Atrial fibrillation 3 (10%) 0 (0%) 0 (0%) 3 (10%)
Bruising 2 (7%) 0 (0%) 0 (0%) 2 (7%)
Hypertension 2 (7%) 2 (7%) 0 (0%) 4 (13%)
Neutropenia 2 (7%) 0 (0%) 0 (0%) 2 (7%)
Upper respiratory infection
2 (7%) 0 (0%) 0 (0%) 2 (7%)
Urinary tract infection
2 (7%) 0 (0%) 0 (0%) 2 (7%)
• Minimal hematological toxicity• Median serum IgA levels decreased from 62 to 39 mg/dL; p=0.04• Median serum IgG levels declined from 563 to 462; p=0.003• Afib medically managed in 2 patients who continue on treatment; cardiac
ablation for one patient with left atrial enlargement off treatment.

Mason et al. Br J Haematol 2016
Ibrutinib penetrates the CNS and produces response in Bing Neel Syndrome

Phase III Study of Zanubrutinib vs. Ibrutinib in WM

Strategies to Enhance BTK Inhibitors in WM

ARM B: Placebo+ Rituximab 375mg/m2 x 8 infusions (weeks 1,2,3,4,17,18,19, and 20)
ARM A: ibrutinib 420mg+ Rituximab 375mg/m2 x 8 infusions (weeks 1,2,3,4,17,18,19, and 20)
1:1 Randomization
N = 150
ARM C: ibrutinib 420mgSubjects considered
refractory to prior rituximab
N=31
iNNOVATE Study in WMTreatment Naïve + Previously Treated
45 centers in 9 countries
ABC patients genotyped for MYD88 and CXCR4
Dimopoulos et al, Lancet Oncol 2017; NEJM 2018

16 15 6 17 239
27 22
5329 56
23
58
44
3633
25
3
38
6
1527
14
0102030405060708090
100
Ibrutinib-RTX
Placebo-RTX
Ibrutinib-RTX
Placebo-RTX
Ibrutinib-RTX
Placebo-RTX
Ibrutinib-RTX
Placebo-RTX
Innovate: Impact of CXCR4 on WM responseB
est
Res
pons
e (%
) ORR 95%
ORR 48%
aFollowing modified 6th IWWM Response Criteria (NCCN 2014); required two consecutive assessments.
MYD88L265P/CXCR4WT MYD88L265P/CXCR4WHIM MYD88WT/CXCR4WT
ORR 100%
ORR 46%
ORR 96%
ORR 57%
ORR 91%
ORR 56%
CRVGPRPRMR
Median time to ≥PR, months (range) 2
(1–28)6
(2–26)2
(1–28)5
(2–17)3
(1–19)11
(4–18)6
(1–17)6
(5–26)
Median time to ≥MR, months (range) 1
(1–18)3
(1–24)1
(1–18)3
(1–24)1
(1–11)3
(1–8)2
(1-17)3
(2–17)
Overall
Major33%
Major79%
Major29%
Major94%
Major48%
Major73%
Major33%
Major64%
??
Dimopoulos et al, NEJM 2018; Updated by Buske et al, ASH 2018

Importance of CXCR4 in PFS
• Improved PFS with ibrutinib
• 36-month PFS rates MYD88L265P/CXCR4WT: 84%
vs 29%
MYD88L265P/CXCR4WHIM: 64% vs 26%
MYD88WT/CXCR4WT: 82% vs 44%
MYD88L265P/CXCR4WT
Prog
ress
ion-
Free
Sur
viva
l (%
)
Months
MYD88WT/CXCR4WT
MYD88L265P/CXCR4WHIM
MYD88L265P/CXCR4WHIM
MYD88WT/CXCR4WT
MYD88L265P/CXCR4WT
Ibrutinib-RTX
RTX
Dimopoulos et al, NEJM 2018; Updated by Buske et al, ASH 2018

Phase I/II Trial of Ulocuplumab and Ibrutinib in CXCR4 mutated patients with symptomatic WM
Ibrutinib Until PD or Intolerance
Weekly Ulo
4 weeks
Biweekly Ulo
20 weeks
ClinicalTrials.gov Identifier: NCT03225716
STOP
Dose Level Ibrutinib Ulocuplumab Cycle 1 Ulocuplumab Cycles 2-6
Level 1 –Starting dose 420mg PO DQ 400 mg weekly 800 mg every other week
Level 2 420mg PO DQ 800 mg weekly 1200 mg every other week
Level 3 420mg PO DQ 800 mg weekly 1600 mg every other week
Schema

Phase II Study of Venetoclaxin Previously Treated WM
ResponseNo prior ibrutinib
(n=15)Prior ibrutinib
(n=15)
Overall 14 (93%) 12 (80%)
Major 13 (87%) 9 (60%)
Very good 4 (27%) 1 (7%)
Partial 9 (60%) 8 (53%)
Minor 1 (7%) 3 (20%)
Stable 1 (7%) 3 (20%)
CXCR4 WT(n=14)
CXCR4 MUT(n=16)
12 (86%) 14 (87%)
9 (86%) 13 (63%)
4 (29%) 1 (7%)
8 (57%) 9 (56%)
0 (0%) 4 (25%)
2 (14%) 2 (13%)
1 patient had progressive disease at 9 months (MYD88, CXCR4, TP53)
Castillo et al. EHA 2018
Median follow-up: 11 months

The role of BCL2 in WM
Cao et al, BJH 2015
Higher BCL2 levels in MYD88 mutated WM

Ibrutinib and Venetoclax in Treatment Naïve WM
Ibrutinib 420 mg/day
x 4 weeks
Ibrutinib 420 mg/day
Add Venetoclax100 mg/day week 5 200 mg/day week 6
400 mg/day weeks 7,8
Ibrutinib 420 mg/day
And
Venetoclax400 mg/day
Observation
4 weeks 4 weeks 22 months Follow to PDor off study
24 months
Jorge Castillo, PI (DFCI)

BTK Cys481 Mutations accompany CXCR4 in WM Patients on Ibrutinib.
Patient*
L265P positive cells
with BTK C481RT>C
L265P positive cells
with BTK C481ST>A
L265P positive cells
with BTK C481SG>C
L265P positive cells
with BTK C481YG>A
L265P positive cells with PLCG2
Y495HT>C
L265P positive cells
with CARD11 L878FC>T
P1 None None None None None None
P2 32.4% 6.6% 5.8% 1.0% None None
P3 0.3% 34.4% 6.5% 0.3% None 0.2%
P4 None None None None None None
P5 None None None None None None
P6 None None 10.3% None 11.9% None
Targeted next-generation sequencing for MYD88, CXCR4, BTK, PLCG2, CARD11, LYN.All patients are MYD88 Mutated.
P2, P3, P6 are CXCR4 WHIM Mutated. Xu et al, BLOOD 2017

BTK C481S cells show uniform ERK 1/2 activation in the presence of ibrutinib.
Chen et al, Blood 2018

Ibrutinib
+ ERK-inhibitor
DFCI/ELI LILLY COLLABORATIONPhase I/II Clinical Trial of the oral ERK inhibitor LY3214996 in
BTK Cys 481 and PLCG2 mutated CLL, WM, MZL, MCL

Frontline Therapy of Symptomatic WM
Hyperviscosity, Severe Cryos, CAGG, PN Plasmapheresis
MYD88 Mutated/No CXCR4 mutationNo bulky disease, no contraindications IbrutinibBulky disease Benda-RAmyloidosis Bortezomib/Dex/Rituximab (BDR)IgM Peripheral Neuropathy Rituximab + Alkylator or Ibrutinib
MYD88 Mutated/CXCR4 mutationSame caveats as aboveIf immediate response needed, either BDR or Benda-R
MYD88 Wild-Type✓non-L265P MYD88 mutations BDR > Benda-R
• Hold Rituximab until IgM <4000 mg/dLor empiric pheresis is performed.
• Consider Maintenance Rituximab• Consider Ofatumumab if R intolerant.
Hunter et al, JCO 2017; LeBlond IWWM10
+Ibrutinib and Rituximab

Salvage Therapy of Symptomatic WMConsider repeat primary therapy if response >2 years
MYD88 Mutated/No CXCR4 mutationSame caveats as primary therapy
MYD88 Mutated/CXCR4 mutationSame caveats as primary therapyIf immediate response needed, either BDR or Benda-R
MYD88 Wild-TypeSame caveats as primary therapy ✓non-L265P MYD88 mutations
• Everolimus >2 prior therapies• Nucleoside analogues (non-ASCT candidates)• ASCT in multiple relapses,
chemosensitive disease
Hunter et al, JCO 2017
+Venetoclax for ptspreviously exposed to IB

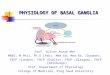
Merlini et al, Nat Rev Dis Primers. 2018
Amyloidosis
Courtesy of G. Merlini

Diagnostic approach to systemic amyloidosis
2. Muchtar et al, Ann Med. 2017 – 3. Fernandez de Larrea et al, Blood 2015 – 4. Quarta et al, Eur Heart J 2017 – 5. Vrana et al, Blood 2009; 6. Lavatelli et al, Mol Cell Proteom. 2008; 7. Arbustini et al, Amyloid 2002; 8. Schonland et al, Blood 2012
Abdominal fat aspirate: (underutilised):2 sensitivity 81-84%3,4
Possible lip/minor salivary gland biopsy for Congo red
PositiveNegative
Cardiac MRI
Organ biopsy
Type amyloid deposits- Proteomics-MS5,6
- Immuno-EM7
- Immunohistochemistry8
CR
FSBCR
Courtesy of G. Merlini

Patients with organ response (%)CR, VGPR, and PR data from 1065 patients at Pavia ARTC
MRD data by NGF on 69 patients at Pavia ARTC
Organ response strictly depends on the quality of hematologic response
Courtesy of G. Merlini

• 1,536 patients at 134 centers from1995 to 2012• HR/CR 61/33%, TRM 4% (2007-2012)• Renal response 30%
D’Souza et al, J Clin Oncol 2015
Fit patients: ~20%age < 70 years, ECOG PS≤2, BP >90 mmHg, cTnT < 0.06 ng/mL, Creatinine clear. >30 mL/min, NYHA I or II, ≤ 2 organs involved
Treatment of Fit Amyloid Patients
1. Tandon et al, BMT 2017 - 2. Sidiqi et al, JCO 2018
• CyBorD induction3,4,5
• Consolidation with BDex if < CR6
ASCT with MEL 2001,2
CRPR
VGPR
NR
NA
3. Hwa et al, Am J Hematol, 2016 - 4. Scharman et al, ASH 2017 Abstr .4552 – 5. Afrough, et al. Biol Blood Marrow Transplant 2018 - 6. Landau et al, Leukemia 2017
1,2
Courtesy of G. Merlini

Choice of upfront treatment in transplant ineligible patients
• CyBorD – stem cell sparing, is preferred in patients with renal failure, in patients with t(11;14)(~50% of patients) is associated with lower response rate
• BMDex – overcomes the effects of both gain 1q21 and t(11;14)
• MDex – preferred in patients with neuropathy or fibrotic lung disease
High risk patients (stage IIIb, NYHA class III or IV) – Low dose combinationregimens or standard regimens with intensive care support
Merlini, et al. Nat Rev Dis Primers. 2018
Courtesy of G. Merlini

Stage IIIb: NT-proBNP> 8500 ng/L (~20%)
Bortezomib-based regimensPalladini et al, Blood 2015 – Le Bras et al, Eur J Cancer 2017
Heart transplantation • age < 65 yrs, • no significant extra-cardiac amyloidosis • ASCT after HTx very effective1-4
• outcomes comparable to non-amyloid5
1. Lacy et al, J Heart Lung Transplant. 2008 – 2. Dey et al, Transplantation 2010 –3. Sattianayagam et al, Am J Transplant. 2010 - 4. Gray Gilstrap, et al, J Heart Lung Transpl 2014 – 5. Kristen et al, J Heart Lung Transplant. 2018
Rapid and deep responses improve outcome of patients with advanced heart involvement
Manwani et al, Haematologica 2018
Courtesy of G. Merlini

Treatment of relapsing/refractory patients
HR 68%, ≥VGPR 29% Responders 36 mos
NR 19 mos
P=0.001
IMiDs are effective rescue agents (increase in NT-proBNP, Len potentialnephrotoxicity)Pomalidomide produces rapid and profound responses(Dispenzieri et al, Blood 2012, Sanchorawala et al., Blood 2016 – Palladini et al, Blood 2017)

Daratumumab in AL amyloidosis
Phase III international study of CyBorD vs CyBorD+Dara upfront (ANDROMEDA) - Safety run-in results: Merlini et al, EHA23 PS1318
Kaufman et al, Blood 2017 & Kaufman et al, EHA23 PS1305Jaccard et al, EHA23 S851
No 44Prior lines of therapy, n (range) 3 (1–8)ORR n (%) 25 (83)CR n (%) 5 (17)VGPR n (%) 19 (63)PR n (%) 1 (3)Time to 1st/ best response, 2.2 months
Abeykoon et al, Leukemia 2018Sanchorawala et al, ASH 2018See also: Lee et al, ASH 2018 - Rahman et al, ASH 2018 - Milani et al, ASH 2018 – Kastritis et al ASH 2018