Embed Size (px)
Citation preview

CM
The Journal of Hand Surgery will contain at least 2 clinically relevanteditor to be offered for CME in each issue. For CME credit, the paarticles in print or online and correctly answer all related questexamination. The questions on the test are designed to make thoccasionally require the reader to go back and scrutinize the artic
The JHS CME Activity fee of $15.00 includes the exam questions/ansinclude access to the JHS articles referenced.
Statement of Need: This CME activity was developed by the JHSeducation tool to help increase or affirm reader’s knowledge. The ovis for participants to evaluate the appropriateness of clinical datapractice and the provision of patient care.
Accreditation: The ASSH is accredited by the Accreditation CounciEducation to provide continuing medical education for physicians.
AMA PRA Credit Designation: The American Society for Surgerythis Journal-Based CME activity for a maximum of 1.00 “AMA PRAPhysicians should claim only the credit commensurate with the extein the activity.
ASSH Disclaimer: The material presented in this CME activity isASSH for educational purposes only. This material is not intendedmethods or the best procedures appropriate for the medical siturather it is intended to present an approach, view, statement, orthat may be helpful, or of interest, to other practitioners. Examinein this medical education activity, sponsored by the ASSH, witawareness that they waive any claim they may have against the Ainformation presented. The approval of the US Food and Drug Adfor procedures and drugs that are considered experimental. Indiscussed or reviewed during this educational activity may notapproval.
From the *Department of Orthopaedic Surgery, Mayo Clinic, RochesteInstitute, Barcelona, Spain.
Received for publication November 16, 2015; accepted in revised
No benefits in any form have been received or will be received relato the subject of this article.
CURRENT CONCEPTS
The “Four-Leaf Clover” Treatment Algorithm:
A Practical Approach to Manage Disorders of the
Distal Radioulnar Joint
Sanjeev Kakar, MD,* Marc Garcia-Elias, MD, PhD*†
E INFORMATION AND DISCLOSURES
articles selected by therticipant must read theions through an onlinee reader think and willle for details.
wers only and does not
editors as a convenienterall goal of the activityand apply it to their
l for Continuing Medical
of the Hand designatesCategory 1 Credits�”.nt of their participation
made available by theto represent the onlyation(s) discussed, butopinion of the authorses agree to participateh full knowledge andSSH for reliance on anyministration is requiredstrumentation systemsyet have received FDA
Provider Information can be found at http://www.assh.org/Pages/ContactUs.aspx.
Technical Requirements for the Online Examination can be found at http://jhandsurg.org/cme/home.
Privacy Policy can be found at http://www.assh.org/pages/ASSHPrivacyPolicy.aspx.
ASSH Disclosure Policy: As a provider accredited by the ACCME, the ASSH must ensurebalance, independence, objectivity, and scientific rigor in all its activities.
Disclosures for this Article
EditorsDavid T. Netscher, MD, has no relevant conflicts of interest to disclose.
AuthorsAll authors of this journal-based CME activity have no relevant conflicts of interest todisclose. In the printed or PDF version of this article, author affiliations can be found at thebottom of the first page.
PlannersDavid T. Netscher, MD, has no relevant conflicts of interest to disclose. The editorial andeducation staff involved with this journal-based CME activity has no relevant conflicts ofinterest to disclose.
Learning Objectives
Upon completion of this CME activity, the learner should achieve an understanding of:
� Osseous constraints of the distal radio-ulnar joint (DRUJ)� Soft tissue restraints of the DRUJ� Interrelated multiple causes of disorders of the DRUJ� Treatment algorithm for disorders of the DRUJ
Deadline: Each examination purchased in 2016 must be completed by January 31, 2017, tobe eligible for CME. A certificate will be issued upon completion of the activity. Estimatedtime to complete each JHS CME activity is up to one hour.
Copyright ª 2016 by the American Society for Surgery of the Hand. All rights reserved.
Most symptomatic distal radioulnar joint (DRUJ) conditions result from derangements toseveral structures that may include the length, shape, and/or orientation of the articulatingsurfaces; the cartilage of the DRUJ and/or ulnocarpal joint; the DRUJ and/or ulnocarpal jointligaments; and the extensor carpi ulnaris and/or pronator quadratus muscle. Once a completediagnosis is made, often only one of these components is addressed, which results in suboptimalclinical outcomes. In this article, we present a treatment algorithm (the Four-Leaf Clover
r, MN; and the †Kaplan
form January 17, 2016.
ted directly or indirectly
Corresponding author: Sanjeev Kakar, MD, Department of Orthopaedic Surgery, MayoClinic, 200 First Street SW, Rochester, MN 55905; e-mail: [email protected].
0363-5023/16/4104-0008$36.00/0http://dx.doi.org/10.1016/j.jhsa.2016.01.005
� 2016 ASSH r Published by Elsevier, Inc. All rights reserved. r 551

552 FOUR-LEAF CLOVER TREATMENT ALGORITHM
algorithm) to guide treatment of DRUJ pathology. The Four-Leaf Clover principle is a guidingalgorithm, not a document forcing the surgeon to adopt one particular treatment. Its purpose is toprovide treating physicians with a checklist that helps ensure that they do not miss any of thedifferent components that need to be addressed for a complete treatment. Using the treatmentalgorithm, we should achieve satisfactory resolution of patients’ symptoms after addressing theparticular components in a stepwise approach. (J Hand Surg Am. 2016;41(4):551e564.Copyright � 2016 by the American Society for Surgery of the Hand. All rights reserved.)Key words Distal radioulnar joint, treatment, distal radioulnar joint pathology.
T HE DISTAL RADIOULNAR JOINT (DRUJ) IS of vital im-portance for optimal functioning of the wristand forearm during pronosupination.1e5 Its
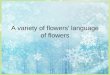
articulating surfaces comprise the ulnar head and sig-moid notch. There are 4 main types of sigmoid notch(Fig. 1),6 most of which are flat-faced. Because of this,an osteocartilaginous volar lip deepens the concavity ofthe notch to increase stability.AfEkenstamandHagert7
and others8,9 noted that the radius of curvature of thesigmoid notch was approximately 50% greater thanthe ulna head, permitting rotation and sliding duringpronation and supination. In maximal supination, thearticular contact area consists of only 2 to 3 mm at thepalmar lip.
Because of the lack of osseous constraint (it ac-counts for 20%), stability of the DRUJ is primarilyafforded by the soft tissues. Static stabilizers provideprimary stability and include the palmar and dorsalradioulnar ligaments. Originating from the palmar anddorsal regions of the DRUJ, respectively, the radio-ulnar ligaments converge into a superficial attachmentto the ulnar styloid and deep foveal attachment limb.These ligaments tighten up during pronosupination toprevent instability at the extremes of motion.10e12
The DRUJ capsule, ulnotriquetral ligament (UTL)and ulnolunate ligament, interosseous membrane, andtriangular fibrocartilage complex (TFCC) provideadditional static stabilization of the DRUJ. Dynamicstabilizers include the pronator quadratus and extensorcarpi ulnaris (ECU) tendon (Fig. 2).13,a
Disorders of the DRUJ are common and yet arepoorly understood. Often referred to low back painof the wrist, there is a wide spectrum of conditionsranging from joint stiffness to gross DRUJ instabilitythat poses many challenges to the treating physician.DRUJ instability can be hard to diagnose because itssigns and symptoms can be nonspecific. Patients maydescribe a history of a fall with the wrist in the extendedand pronated position that resulted in symptoms of apainful click with wrist motion, especially pronosupina-tion. Chronic overuse and degenerative conditions mayhave a history of trauma or a change in recent activities.
J Hand Surg Am. r V
Examination should start on the uninjured wrist,which can act as a control to determine what is thenormal range of motion and laxity of the DRUJ,because this can vary among individuals. Patientsoften have pain with pronation and supination of thewrist. With dorsal instability, they may have a protu-berant ulnar head at terminal pronation. In patientswithpalmar instability, a slight fullness may be seenwithin the volar DRUJ, with a depression noted on thedorsal wrist. Passive laxity should be assessed with theforearm in neutral, pronation, and supination andcomparedwith the uninjured side. Compression acrossthe DRUJ may cause pain or accentuate a clunk as theulna head dislocates and reduces within the notch. Apositive piano-key test may be noted with pain whenthe ulna head is reduced within the sigmoid notch withdorsal to palmar force and then released.14 Painmay berelieved by depressing the ulna head with the thumbwhile simultaneously elevating the pisiform bone inpatients with carpal supination and dorsal subluxationof the ulna head.15 Adams and Berger16 described themodified press test to detect DRUJ instability. Withforerarms pronated, patients press both hands on a flatsurface. In those with DRUJ instability, the ulnar headis proud dorsally and seems to subluxate volar withpressure, creating a dorsal hollow. Foveal tenderness, aregion located between the flexor carpi ulnaris tendonand ulnar styloid, may indicate disruption of the deepfibers of the radioulnar ligament.17
The ECU should be examined for signs of tender-ness and instability during pronosupination. The use ofselective local anesthetic injections can aid in diag-nosing ulnarwrist pain, given themyriad of differentialdiagnoses. These include TFCC tears, ECU tenosyn-ovitis, ECU instability, DRUJ instability, DRUJarthritis, ulnar impaction, ulnar styloid nonunions,lunotriquetral ligament insufficiency, and neuromas ofthe dorsal sensory branch of the ulnar nerve.
Standard neutral rotation posteroanterior (ECUgroove lies radial to ulnar styloid),18 oblique, and lateralplain wrist x-rays should be examined for fractures,carpal malalignment, ulnar variance, and inflammatory
ol. 41, April 2016
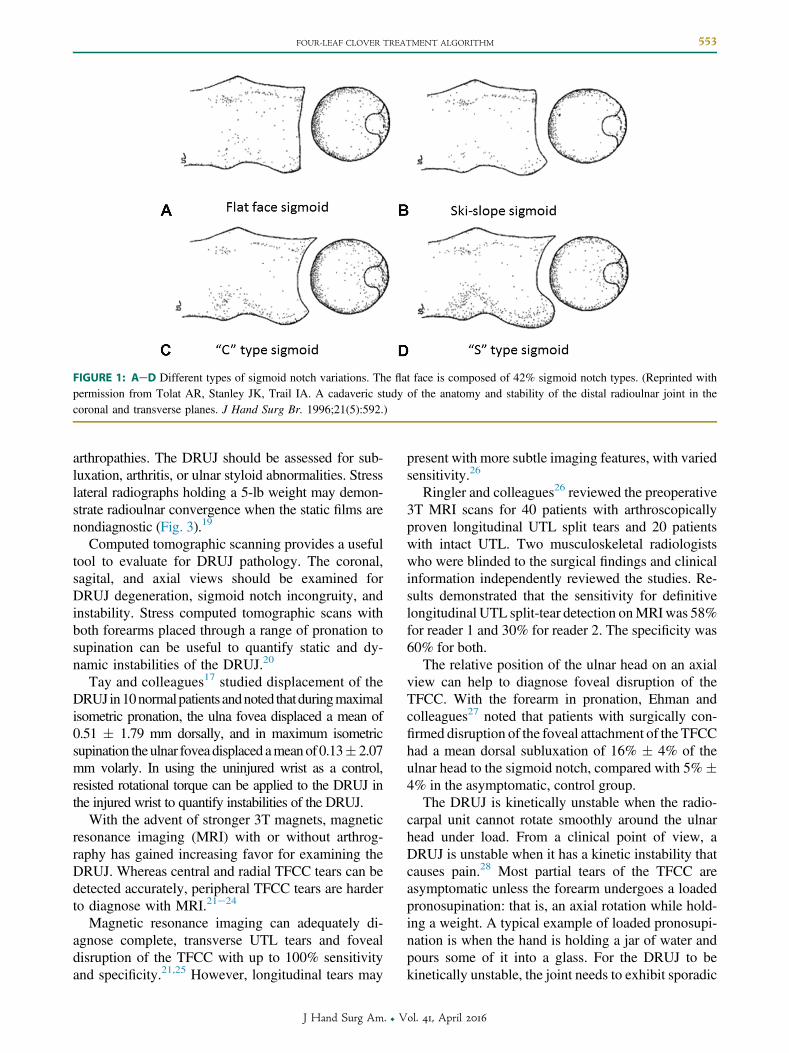
FIGURE 1: AeD Different types of sigmoid notch variations. The flat face is composed of 42% sigmoid notch types. (Reprinted withpermission from Tolat AR, Stanley JK, Trail IA. A cadaveric study of the anatomy and stability of the distal radioulnar joint in thecoronal and transverse planes. J Hand Surg Br. 1996;21(5):592.)
FOUR-LEAF CLOVER TREATMENT ALGORITHM 553
arthropathies. The DRUJ should be assessed for sub-luxation, arthritis, or ulnar styloid abnormalities. Stresslateral radiographs holding a 5-lb weight may demon-strate radioulnar convergence when the static films arenondiagnostic (Fig. 3).19
Computed tomographic scanning provides a usefultool to evaluate for DRUJ pathology. The coronal,sagital, and axial views should be examined forDRUJ degeneration, sigmoid notch incongruity, andinstability. Stress computed tomographic scans withboth forearms placed through a range of pronation tosupination can be useful to quantify static and dy-namic instabilities of the DRUJ.20
Tay and colleagues17 studied displacement of theDRUJ in10normalpatients andnoted thatduringmaximalisometric pronation, the ulna fovea displaced a mean of0.51 � 1.79 mm dorsally, and in maximum isometricsupination theulnar foveadisplaced ameanof 0.13� 2.07mm volarly. In using the uninjured wrist as a control,resisted rotational torque can be applied to the DRUJ inthe injured wrist to quantify instabilities of the DRUJ.
With the advent of stronger 3T magnets, magneticresonance imaging (MRI) with or without arthrog-raphy has gained increasing favor for examining theDRUJ. Whereas central and radial TFCC tears can bedetected accurately, peripheral TFCC tears are harderto diagnose with MRI.21e24
Magnetic resonance imaging can adequately di-agnose complete, transverse UTL tears and fovealdisruption of the TFCC with up to 100% sensitivityand specificity.21,25 However, longitudinal tears may
J Hand Surg Am. r V
present with more subtle imaging features, with variedsensitivity.26
Ringler and colleagues26 reviewed the preoperative3T MRI scans for 40 patients with arthroscopicallyproven longitudinal UTL split tears and 20 patientswith intact UTL. Two musculoskeletal radiologistswho were blinded to the surgical findings and clinicalinformation independently reviewed the studies. Re-sults demonstrated that the sensitivity for definitivelongitudinal UTL split-tear detection onMRIwas 58%for reader 1 and 30% for reader 2. The specificity was60% for both.
The relative position of the ulnar head on an axialview can help to diagnose foveal disruption of theTFCC. With the forearm in pronation, Ehman andcolleagues27 noted that patients with surgically con-firmed disruption of the foveal attachment of the TFCChad a mean dorsal subluxation of 16% � 4% of theulnar head to the sigmoid notch, compared with 5%�4% in the asymptomatic, control group.
The DRUJ is kinetically unstable when the radio-carpal unit cannot rotate smoothly around the ulnarhead under load. From a clinical point of view, aDRUJ is unstable when it has a kinetic instability thatcauses pain.28 Most partial tears of the TFCC areasymptomatic unless the forearm undergoes a loadedpronosupination: that is, an axial rotation while hold-ing a weight. A typical example of loaded pronosupi-nation is when the hand is holding a jar of water andpours some of it into a glass. For the DRUJ to bekinetically unstable, the joint needs to exhibit sporadic
ol. 41, April 2016
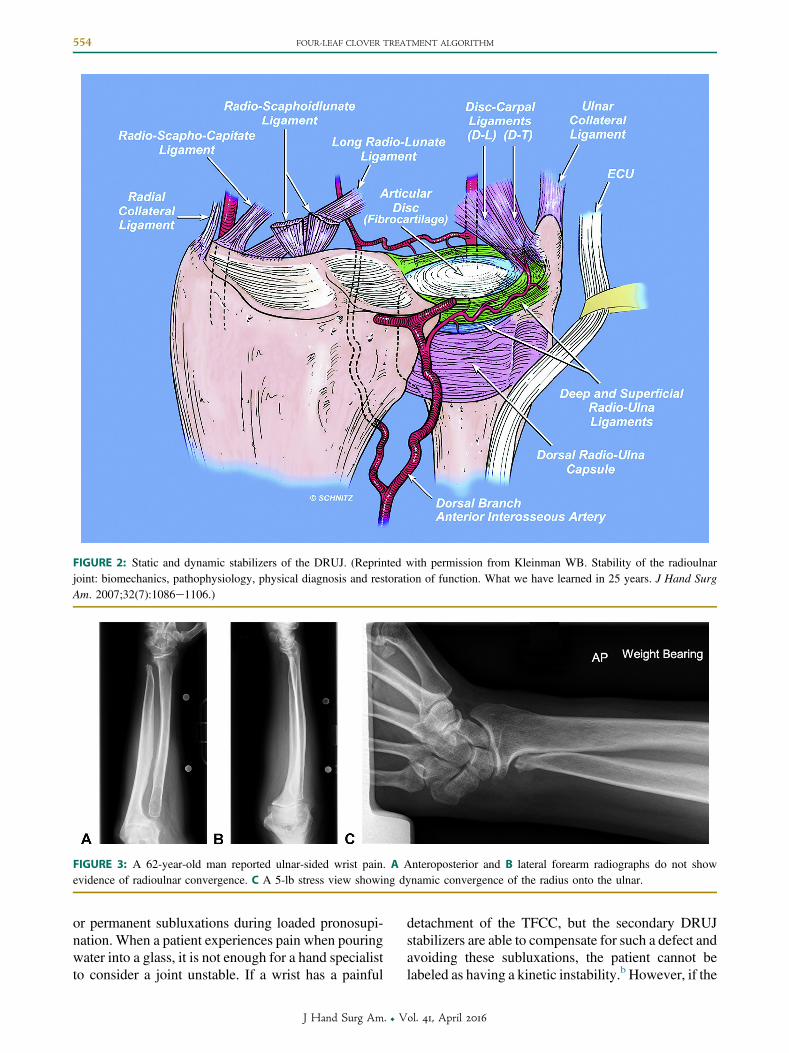
FIGURE 3: A 62-year-old man reported ulnar-sided wrist pain. A Anteroposterior and B lateral forearm radiographs do not showevidence of radioulnar convergence. C A 5-lb stress view showing dynamic convergence of the radius onto the ulnar.
FIGURE 2: Static and dynamic stabilizers of the DRUJ. (Reprinted with permission from Kleinman WB. Stability of the radioulnarjoint: biomechanics, pathophysiology, physical diagnosis and restoration of function. What we have learned in 25 years. J Hand SurgAm. 2007;32(7):1086e1106.)
554 FOUR-LEAF CLOVER TREATMENT ALGORITHM
or permanent subluxations during loaded pronosupi-nation. When a patient experiences pain when pouringwater into a glass, it is not enough for a hand specialistto consider a joint unstable. If a wrist has a painful
J Hand Surg Am. r V
detachment of the TFCC, but the secondary DRUJstabilizers are able to compensate for such a defect andavoiding these subluxations, the patient cannot belabeled as having a kinetic instability.b However, if the
ol. 41, April 2016
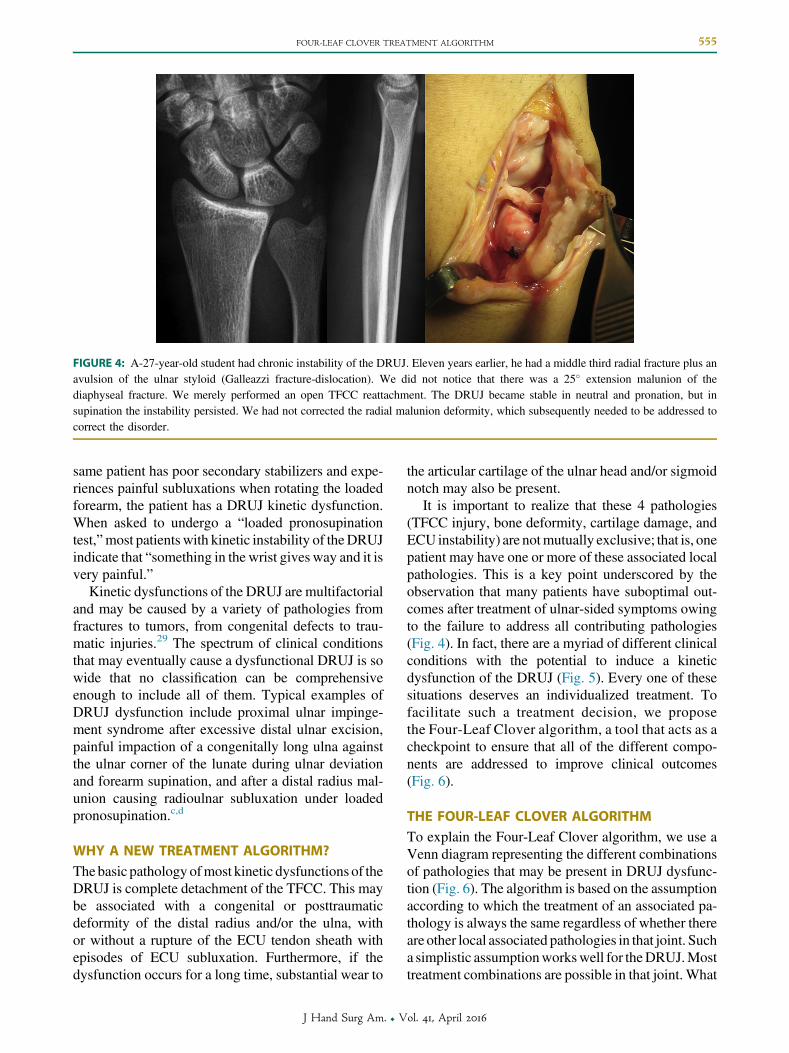
FIGURE 4: A-27-year-old student had chronic instability of the DRUJ. Eleven years earlier, he had a middle third radial fracture plus anavulsion of the ulnar styloid (Galleazzi fracture-dislocation). We did not notice that there was a 25� extension malunion of thediaphyseal fracture. We merely performed an open TFCC reattachment. The DRUJ became stable in neutral and pronation, but insupination the instability persisted. We had not corrected the radial malunion deformity, which subsequently needed to be addressed tocorrect the disorder.
FOUR-LEAF CLOVER TREATMENT ALGORITHM 555
same patient has poor secondary stabilizers and expe-riences painful subluxations when rotating the loadedforearm, the patient has a DRUJ kinetic dysfunction.When asked to undergo a “loaded pronosupinationtest,”most patients with kinetic instability of theDRUJindicate that “something in the wrist gives way and it isvery painful.”
Kinetic dysfunctions of the DRUJ are multifactorialand may be caused by a variety of pathologies fromfractures to tumors, from congenital defects to trau-matic injuries.29 The spectrum of clinical conditionsthat may eventually cause a dysfunctional DRUJ is sowide that no classification can be comprehensiveenough to include all of them. Typical examples ofDRUJ dysfunction include proximal ulnar impinge-ment syndrome after excessive distal ulnar excision,painful impaction of a congenitally long ulna againstthe ulnar corner of the lunate during ulnar deviationand forearm supination, and after a distal radius mal-union causing radioulnar subluxation under loadedpronosupination.c,d
WHY A NEW TREATMENT ALGORITHM?The basic pathology ofmost kinetic dysfunctions of theDRUJ is complete detachment of the TFCC. This maybe associated with a congenital or posttraumaticdeformity of the distal radius and/or the ulna, withor without a rupture of the ECU tendon sheath withepisodes of ECU subluxation. Furthermore, if thedysfunction occurs for a long time, substantial wear to
J Hand Surg Am. r V
the articular cartilage of the ulnar head and/or sigmoidnotch may also be present.
It is important to realize that these 4 pathologies(TFCC injury, bone deformity, cartilage damage, andECU instability) are notmutually exclusive; that is, onepatient may have one or more of these associated localpathologies. This is a key point underscored by theobservation that many patients have suboptimal out-comes after treatment of ulnar-sided symptoms owingto the failure to address all contributing pathologies(Fig. 4). In fact, there are a myriad of different clinicalconditions with the potential to induce a kineticdysfunction of the DRUJ (Fig. 5). Every one of thesesituations deserves an individualized treatment. Tofacilitate such a treatment decision, we proposethe Four-Leaf Clover algorithm, a tool that acts as acheckpoint to ensure that all of the different compo-nents are addressed to improve clinical outcomes(Fig. 6).
THE FOUR-LEAF CLOVER ALGORITHMTo explain the Four-Leaf Clover algorithm, we use aVenn diagram representing the different combinationsof pathologies that may be present in DRUJ dysfunc-tion (Fig. 6). The algorithm is based on the assumptionaccording to which the treatment of an associated pa-thology is always the same regardless of whether thereare other local associated pathologies in that joint. Sucha simplistic assumptionworkswell for theDRUJ.Mosttreatment combinations are possible in that joint. What
ol. 41, April 2016
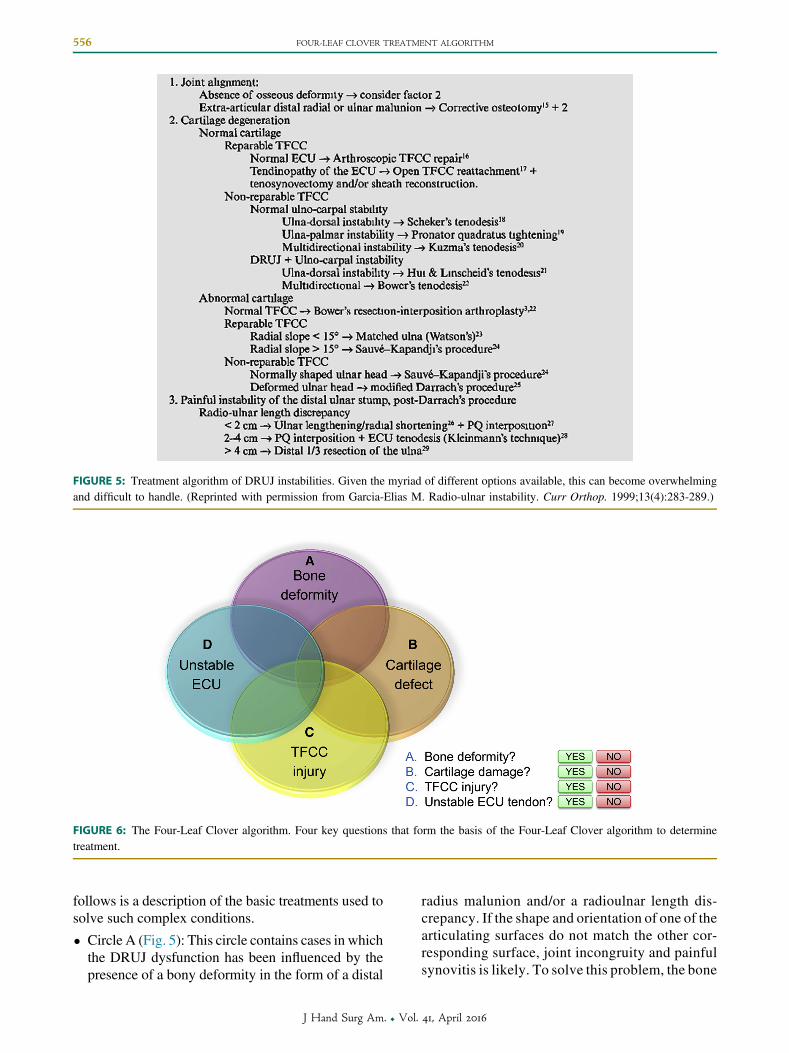
FIGURE 5: Treatment algorithm of DRUJ instabilities. Given the myriad of different options available, this can become overwhelmingand difficult to handle. (Reprinted with permission from Garcia-Elias M. Radio-ulnar instability. Curr Orthop. 1999;13(4):283-289.)
FIGURE 6: The Four-Leaf Clover algorithm. Four key questions that form the basis of the Four-Leaf Clover algorithm to determinetreatment.
556 FOUR-LEAF CLOVER TREATMENT ALGORITHM
follows is a description of the basic treatments used tosolve such complex conditions.
� Circle A (Fig. 5): This circle contains cases in whichthe DRUJ dysfunction has been influenced by thepresence of a bony deformity in the form of a distal
J Hand Surg Am. r V
radius malunion and/or a radioulnar length dis-crepancy. If the shape and orientation of one of thearticulating surfaces do not match the other cor-responding surface, joint incongruity and painfulsynovitis is likely. To solve this problem, the bone
ol. 41, April 2016
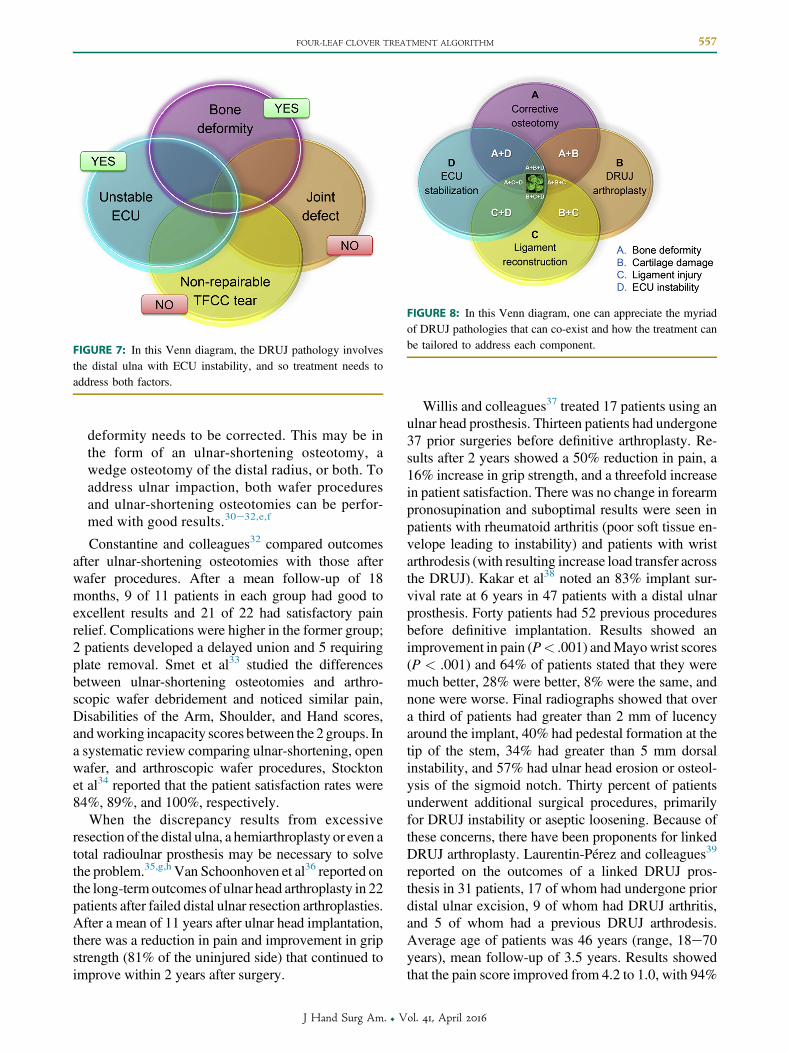
FIGURE 7: In this Venn diagram, the DRUJ pathology involvesthe distal ulna with ECU instability, and so treatment needs toaddress both factors.
FIGURE 8: In this Venn diagram, one can appreciate the myriadof DRUJ pathologies that can co-exist and how the treatment canbe tailored to address each component.
FOUR-LEAF CLOVER TREATMENT ALGORITHM 557
deformity needs to be corrected. This may be inthe form of an ulnar-shortening osteotomy, awedge osteotomy of the distal radius, or both. Toaddress ulnar impaction, both wafer proceduresand ulnar-shortening osteotomies can be perfor-med with good results.30e32,e,f
Constantine and colleagues32 compared outcomesafter ulnar-shortening osteotomies with those afterwafer procedures. After a mean follow-up of 18months, 9 of 11 patients in each group had good toexcellent results and 21 of 22 had satisfactory painrelief. Complications were higher in the former group;2 patients developed a delayed union and 5 requiringplate removal. Smet et al33 studied the differencesbetween ulnar-shortening osteotomies and arthro-scopic wafer debridement and noticed similar pain,Disabilities of the Arm, Shoulder, and Hand scores,andworking incapacity scores between the 2 groups. Ina systematic review comparing ulnar-shortening, openwafer, and arthroscopic wafer procedures, Stocktonet al34 reported that the patient satisfaction rates were84%, 89%, and 100%, respectively.
When the discrepancy results from excessiveresection of the distal ulna, a hemiarthroplasty or even atotal radioulnar prosthesis may be necessary to solvethe problem.35,g,h Van Schoonhoven et al36 reported onthe long-termoutcomes of ulnar head arthroplasty in 22patients after failed distal ulnar resection arthroplasties.After a mean of 11 years after ulnar head implantation,there was a reduction in pain and improvement in gripstrength (81% of the uninjured side) that continued toimprove within 2 years after surgery.
J Hand Surg Am. r V
Willis and colleagues37 treated 17 patients using anulnar head prosthesis. Thirteen patients had undergone37 prior surgeries before definitive arthroplasty. Re-sults after 2 years showed a 50% reduction in pain, a16% increase in grip strength, and a threefold increasein patient satisfaction. There was no change in forearmpronosupination and suboptimal results were seen inpatients with rheumatoid arthritis (poor soft tissue en-velope leading to instability) and patients with wristarthrodesis (with resulting increase load transfer acrossthe DRUJ). Kakar et al38 noted an 83% implant sur-vival rate at 6 years in 47 patients with a distal ulnarprosthesis. Forty patients had 52 previous proceduresbefore definitive implantation. Results showed animprovement in pain (P< .001) andMayowrist scores(P < .001) and 64% of patients stated that they weremuch better, 28% were better, 8% were the same, andnone were worse. Final radiographs showed that overa third of patients had greater than 2 mm of lucencyaround the implant, 40% had pedestal formation at thetip of the stem, 34% had greater than 5 mm dorsalinstability, and 57% had ulnar head erosion or osteol-ysis of the sigmoid notch. Thirty percent of patientsunderwent additional surgical procedures, primarilyfor DRUJ instability or aseptic loosening. Because ofthese concerns, there have been proponents for linkedDRUJ arthroplasty. Laurentin-Pérez and colleagues39
reported on the outcomes of a linked DRUJ pros-thesis in 31 patients, 17 of whom had undergone priordistal ulnar excision, 9 of whom had DRUJ arthritis,and 5 of whom had a previous DRUJ arthrodesis.Average age of patients was 46 years (range, 18e70years), mean follow-up of 3.5 years. Results showedthat the pain score improved from 4.2 to 1.0, with 94%
ol. 41, April 2016
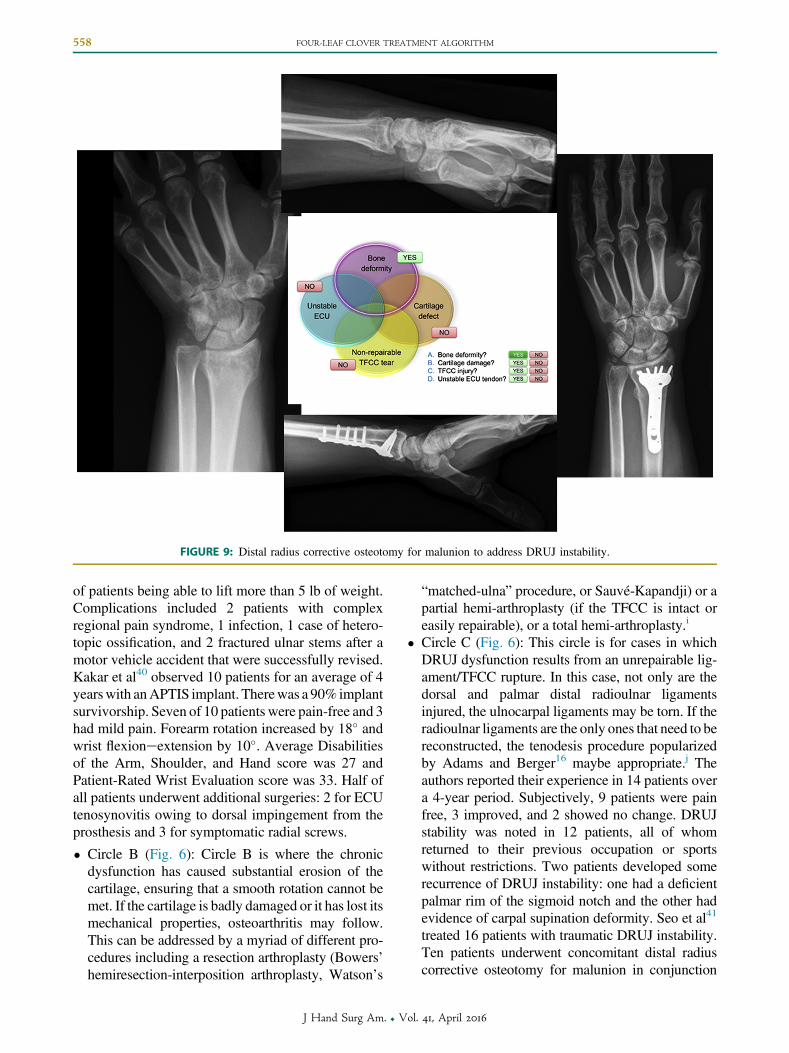
FIGURE 9: Distal radius corrective osteotomy for malunion to address DRUJ instability.
558 FOUR-LEAF CLOVER TREATMENT ALGORITHM
of patients being able to lift more than 5 lb of weight.Complications included 2 patients with complexregional pain syndrome, 1 infection, 1 case of hetero-topic ossification, and 2 fractured ulnar stems after amotor vehicle accident that were successfully revised.Kakar et al40 observed 10 patients for an average of 4yearswith anAPTIS implant. Therewas a 90% implantsurvivorship. Seven of 10 patients were pain-free and 3had mild pain. Forearm rotation increased by 18� andwrist flexioneextension by 10�. Average Disabilitiesof the Arm, Shoulder, and Hand score was 27 andPatient-Rated Wrist Evaluation score was 33. Half ofall patients underwent additional surgeries: 2 for ECUtenosynovitis owing to dorsal impingement from theprosthesis and 3 for symptomatic radial screws.
� Circle B (Fig. 6): Circle B is where the chronicdysfunction has caused substantial erosion of thecartilage, ensuring that a smooth rotation cannot bemet. If the cartilage is badly damaged or it has lost itsmechanical properties, osteoarthritis may follow.This can be addressed by a myriad of different pro-cedures including a resection arthroplasty (Bowers’hemiresection-interposition arthroplasty, Watson’s
J Hand Surg Am. r V
“matched-ulna” procedure, or Sauvé-Kapandji) or apartial hemi-arthroplasty (if the TFCC is intact oreasily repairable), or a total hemi-arthroplasty.i
� Circle C (Fig. 6): This circle is for cases in whichDRUJ dysfunction results from an unrepairable lig-ament/TFCC rupture. In this case, not only are thedorsal and palmar distal radioulnar ligamentsinjured, the ulnocarpal ligaments may be torn. If theradioulnar ligaments are the only ones that need to bereconstructed, the tenodesis procedure popularizedby Adams and Berger16 maybe appropriate.j Theauthors reported their experience in 14 patients overa 4-year period. Subjectively, 9 patients were painfree, 3 improved, and 2 showed no change. DRUJstability was noted in 12 patients, all of whomreturned to their previous occupation or sportswithout restrictions. Two patients developed somerecurrence of DRUJ instability: one had a deficientpalmar rim of the sigmoid notch and the other hadevidence of carpal supination deformity. Seo et al41
treated 16 patients with traumatic DRUJ instability.Ten patients underwent concomitant distal radiuscorrective osteotomy for malunion in conjunction
ol. 41, April 2016
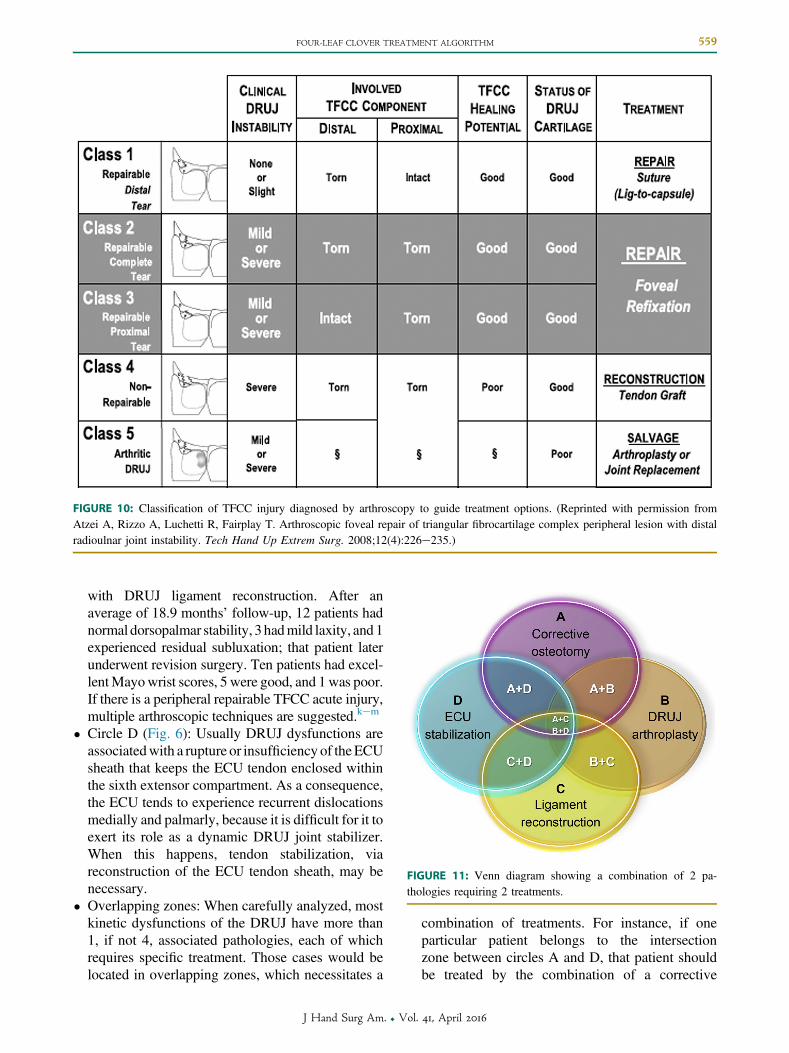
FIGURE 11: Venn diagram showing a combination of 2 pa-thologies requiring 2 treatments.
FIGURE 10: Classification of TFCC injury diagnosed by arthroscopy to guide treatment options. (Reprinted with permission fromAtzei A, Rizzo A, Luchetti R, Fairplay T. Arthroscopic foveal repair of triangular fibrocartilage complex peripheral lesion with distalradioulnar joint instability. Tech Hand Up Extrem Surg. 2008;12(4):226e235.)
FOUR-LEAF CLOVER TREATMENT ALGORITHM 559
with DRUJ ligament reconstruction. After anaverage of 18.9 months’ follow-up, 12 patients hadnormal dorsopalmar stability, 3 hadmild laxity, and 1experienced residual subluxation; that patient laterunderwent revision surgery. Ten patients had excel-lentMayowrist scores, 5 were good, and 1was poor.If there is a peripheral repairable TFCC acute injury,multiple arthroscopic techniques are suggested.kem
� Circle D (Fig. 6): Usually DRUJ dysfunctions areassociatedwith a rupture or insufficiency of theECUsheath that keeps the ECU tendon enclosed withinthe sixth extensor compartment. As a consequence,the ECU tends to experience recurrent dislocationsmedially and palmarly, because it is difficult for it toexert its role as a dynamic DRUJ joint stabilizer.When this happens, tendon stabilization, viareconstruction of the ECU tendon sheath, may benecessary.
� Overlapping zones: When carefully analyzed, mostkinetic dysfunctions of the DRUJ have more than1, if not 4, associated pathologies, each of whichrequires specific treatment. Those cases would belocated in overlapping zones, which necessitates a
J Hand Surg Am. r V
combination of treatments. For instance, if oneparticular patient belongs to the intersectionzone between circles A and D, that patient shouldbe treated by the combination of a corrective
ol. 41, April 2016
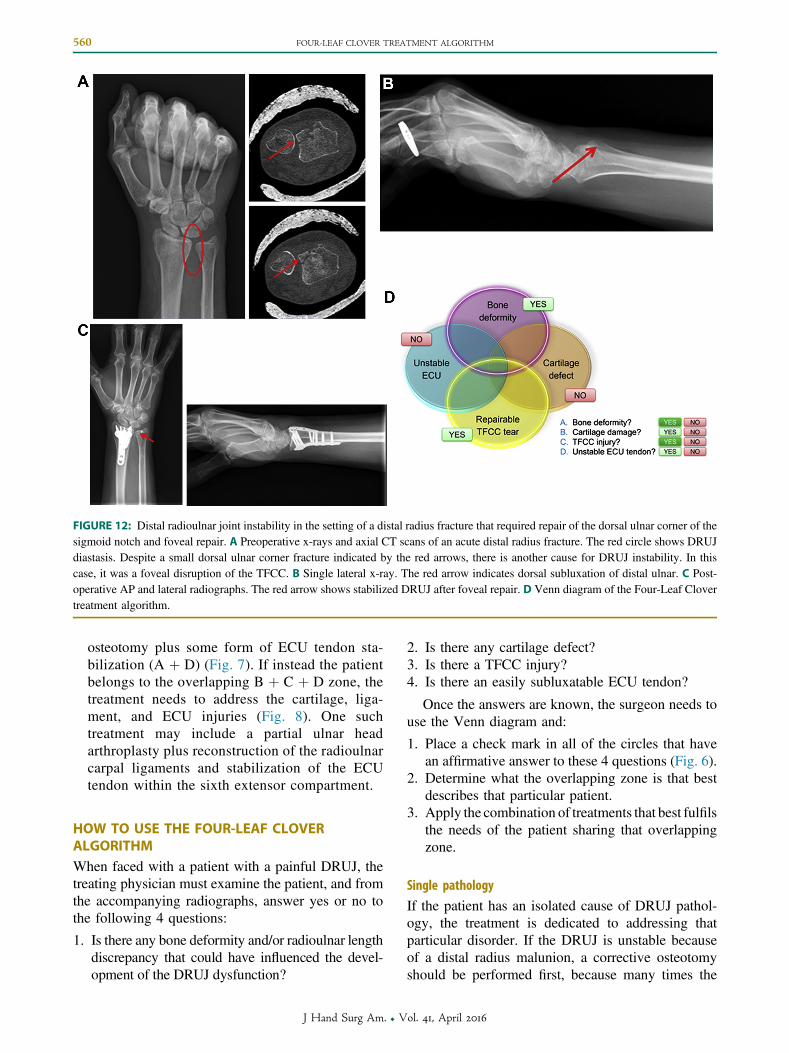
FIGURE 12: Distal radioulnar joint instability in the setting of a distal radius fracture that required repair of the dorsal ulnar corner of thesigmoid notch and foveal repair. A Preoperative x-rays and axial CT scans of an acute distal radius fracture. The red circle shows DRUJdiastasis. Despite a small dorsal ulnar corner fracture indicated by the red arrows, there is another cause for DRUJ instability. In thiscase, it was a foveal disruption of the TFCC. B Single lateral x-ray. The red arrow indicates dorsal subluxation of distal ulnar. C Post-operative AP and lateral radiographs. The red arrow shows stabilized DRUJ after foveal repair. D Venn diagram of the Four-Leaf Clovertreatment algorithm.
560 FOUR-LEAF CLOVER TREATMENT ALGORITHM
osteotomy plus some form of ECU tendon sta-bilization (A þ D) (Fig. 7). If instead the patientbelongs to the overlapping B þ C þ D zone, thetreatment needs to address the cartilage, liga-ment, and ECU injuries (Fig. 8). One suchtreatment may include a partial ulnar headarthroplasty plus reconstruction of the radioulnarcarpal ligaments and stabilization of the ECUtendon within the sixth extensor compartment.
HOW TO USE THE FOUR-LEAF CLOVERALGORITHMWhen faced with a patient with a painful DRUJ, thetreating physician must examine the patient, and fromthe accompanying radiographs, answer yes or no tothe following 4 questions:
1. Is there any bone deformity and/or radioulnar lengthdiscrepancy that could have influenced the devel-opment of the DRUJ dysfunction?
J Hand Surg Am. r V
2. Is there any cartilage defect?3. Is there a TFCC injury?4. Is there an easily subluxatable ECU tendon?
Once the answers are known, the surgeon needs touse the Venn diagram and:
1. Place a check mark in all of the circles that havean affirmative answer to these 4 questions (Fig. 6).
2. Determine what the overlapping zone is that bestdescribes that particular patient.
3. Apply the combination of treatments that best fulfilsthe needs of the patient sharing that overlappingzone.
Single pathology
If the patient has an isolated cause of DRUJ pathol-ogy, the treatment is dedicated to addressing thatparticular disorder. If the DRUJ is unstable becauseof a distal radius malunion, a corrective osteotomyshould be performed first, because many times the
ol. 41, April 2016
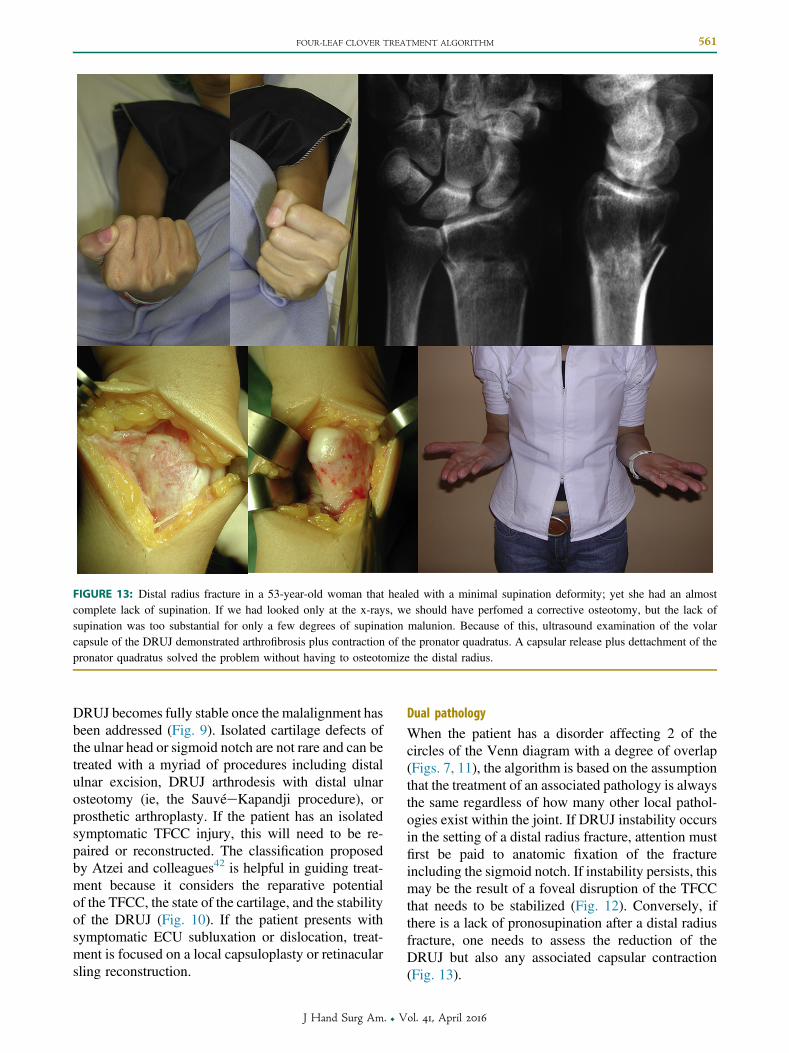
FIGURE 13: Distal radius fracture in a 53-year-old woman that healed with a minimal supination deformity; yet she had an almostcomplete lack of supination. If we had looked only at the x-rays, we should have perfomed a corrective osteotomy, but the lack ofsupination was too substantial for only a few degrees of supination malunion. Because of this, ultrasound examination of the volarcapsule of the DRUJ demonstrated arthrofibrosis plus contraction of the pronator quadratus. A capsular release plus dettachment of thepronator quadratus solved the problem without having to osteotomize the distal radius.
FOUR-LEAF CLOVER TREATMENT ALGORITHM 561
DRUJ becomes fully stable once the malalignment hasbeen addressed (Fig. 9). Isolated cartilage defects ofthe ulnar head or sigmoid notch are not rare and can betreated with a myriad of procedures including distalulnar excision, DRUJ arthrodesis with distal ulnarosteotomy (ie, the SauvéeKapandji procedure), orprosthetic arthroplasty. If the patient has an isolatedsymptomatic TFCC injury, this will need to be re-paired or reconstructed. The classification proposedby Atzei and colleagues42 is helpful in guiding treat-ment because it considers the reparative potentialof the TFCC, the state of the cartilage, and the stabilityof the DRUJ (Fig. 10). If the patient presents withsymptomatic ECU subluxation or dislocation, treat-ment is focused on a local capsuloplasty or retinacularsling reconstruction.
J Hand Surg Am. r V
Dual pathology
When the patient has a disorder affecting 2 of thecircles of the Venn diagram with a degree of overlap(Figs. 7, 11), the algorithm is based on the assumptionthat the treatment of an associated pathology is alwaysthe same regardless of how many other local pathol-ogies exist within the joint. If DRUJ instability occursin the setting of a distal radius fracture, attention mustfirst be paid to anatomic fixation of the fractureincluding the sigmoid notch. If instability persists, thismay be the result of a foveal disruption of the TFCCthat needs to be stabilized (Fig. 12). Conversely, ifthere is a lack of pronosupination after a distal radiusfracture, one needs to assess the reduction of theDRUJ but also any associated capsular contraction(Fig. 13).
ol. 41, April 2016
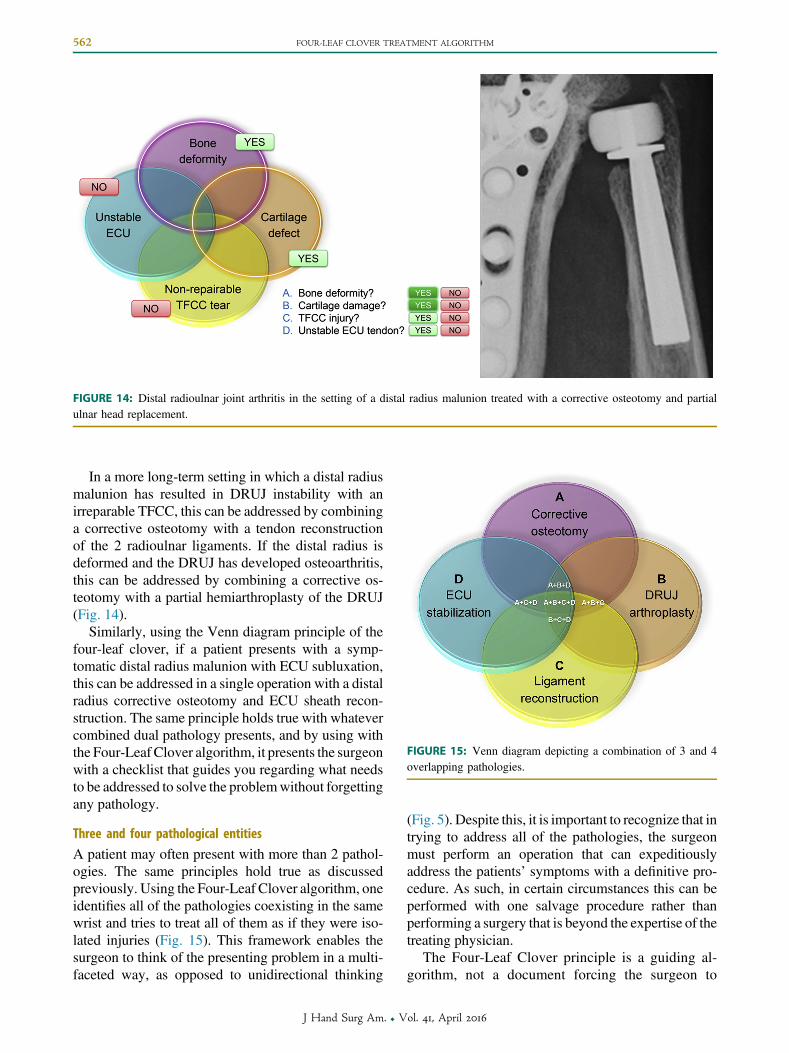
FIGURE 14: Distal radioulnar joint arthritis in the setting of a distal radius malunion treated with a corrective osteotomy and partialulnar head replacement.
FIGURE 15: Venn diagram depicting a combination of 3 and 4overlapping pathologies.
562 FOUR-LEAF CLOVER TREATMENT ALGORITHM
In a more long-term setting in which a distal radiusmalunion has resulted in DRUJ instability with anirreparable TFCC, this can be addressed by combininga corrective osteotomy with a tendon reconstructionof the 2 radioulnar ligaments. If the distal radius isdeformed and the DRUJ has developed osteoarthritis,this can be addressed by combining a corrective os-teotomy with a partial hemiarthroplasty of the DRUJ(Fig. 14).
Similarly, using the Venn diagram principle of thefour-leaf clover, if a patient presents with a symp-tomatic distal radius malunion with ECU subluxation,this can be addressed in a single operation with a distalradius corrective osteotomy and ECU sheath recon-struction. The same principle holds true with whatevercombined dual pathology presents, and by using withthe Four-Leaf Clover algorithm, it presents the surgeonwith a checklist that guides you regarding what needsto be addressed to solve the problemwithout forgettingany pathology.
Three and four pathological entities
A patient may often present with more than 2 pathol-ogies. The same principles hold true as discussedpreviously. Using the Four-Leaf Clover algorithm, oneidentifies all of the pathologies coexisting in the samewrist and tries to treat all of them as if they were iso-lated injuries (Fig. 15). This framework enables thesurgeon to think of the presenting problem in a multi-faceted way, as opposed to unidirectional thinking
J Hand Surg Am. r V
(Fig. 5). Despite this, it is important to recognize that intrying to address all of the pathologies, the surgeonmust perform an operation that can expeditiouslyaddress the patients’ symptoms with a definitive pro-cedure. As such, in certain circumstances this can beperformed with one salvage procedure rather thanperforming a surgery that is beyond the expertise of thetreating physician.
The Four-Leaf Clover principle is a guiding al-gorithm, not a document forcing the surgeon to
ol. 41, April 2016
FOUR-LEAF CLOVER TREATMENT ALGORITHM 563
adopt one particular treatment. Its purpose is toprovide the treating physician with a checklistthat helps to ensure that one does not miss any ofthe different components that need to be addressedfor a complete treatment. Once a full diagnosishas been made, the treatment algorithm that fol-lows may be straightforward because it is then amatter of addressing every component as if itwere an isolated injury. The Four-Leaf Clover al-gorithm helps one to achieve this and will informabout what needs to be done to solve all of thecomponents.
REFERENCES
1. Kauer JM. The distal radioulnar joint: anatomic and functional con-siderations. Clin Orthop Relat Res. 1992;275:37e45.
2. Shaaban H, Giakas G, Bolton M, et al. The load-bearing characteristicsof the forearm: pattern of axial and bending force transmitted throughulna and radius. J Hand Surg Br. 2006;31(3):274e279.
3. Linscheid RL. Biomechanics of the distal radioulnar joint. Clin OrthopRelat Res. 1992;275:46e55.
4. Palmer AK, Werner FW. Biomechanics of the distal radioulnar joint.Clin Orthop Relat Res. 1984;187:26e35.
5. Stuart PR, Berger RA, Linscheid RL, An KN. The dorsopalmar sta-bility of the distal radioulnar joint. J Hand Surg Am. 2000;25(4):689e699.
6. Tolat AR, Stanley JK, Trail IA. Different types of sigmoid notchvariations: the flat face comprises 42% of sigmoid notch types. Acadaveric study of the anatomy and stability of the distal radioulnarjoint in the coronal and transverse planes. J Hand Surg Br. 1996;21(5):592.
7. af Ekenstam F, Hagert CG. Anatomical studies on the geometry andstability of the distal radio ulnar joint. Scand J Plast Reconstr Surg.1985;19(1):17e25.
8. Johnston K, Durand D, Hildebrand KA. Chronic volar distal radio-ulnar joint instability: joint capsular plication to restore function. Can JSurg. 2009;52(2):112e118.
9. Ray RD, Johnson RJ, Jameson RM. Rotation of the forearm; anexperimental study of pronation and supination. J Bone Joint Surg Am.1951;33(4):993e996.
10. Kihara H, Short WH, Werner FW, Fortino MD, Palmer AK. Thestabilizing mechanism of the distal radioulnar joint during pronationand supination. J Hand Surg Am. 1995;20(6):930e936.
11. Schuind F, An KN, Berglund L, et al. The distal radio-ulnar liga-ments: a biomechanical study. J Hand Surg Am. 1991;16(6).1106e1014.
12. Ward LD, Ambrose CG, Masson MV, Levaro F. The role of thedistal radioulnar ligaments, interosseous membrane, and joint capsulein distal radioulnar joint stability. J Hand Surg Am. 2000;25(2):341e351.
13. Kleinman WB. Stability of the radioulnar joint. Biomechanics,pathophysiology, physical diagnosis and restoration of functionwhatwe have learned in 25 years. J Hand Surg Am. 2007;32(7):1086e1106.
14. Glowacki KA, Shin LA. Stabilization of the unstable distal ulna: theLinscheid-Hui procedure. Tech Hand Up Extrem Surg. 1999;3(4):229e236.
15. Hui FC, Linscheid RL. Ulnotriquetral augmentation tenodesis: areconstructive procedure for dorsal subluxation of the distal radio-ulnar joint. J Hand Surg Am. 1982;7(3):230e236.
16. Adams BD, Berger RA. An anatomic reconstruction of the distalradioulnar ligaments for posttraumatic distal radioulnar joint insta-bility. J Hand Surg Am. 2002;27(2):243e251.
J Hand Surg Am. r V
17. Tay SC, Tomita K, Berger RA. The “ulnar fovea sign” for definingulnar wrist pain: an analysis of sensitivity and specificity. J HandSurg Am. 2007;32(4):438e444.
18. Levis CM, Yang Z, Gilula LA. Validation of the extensor carpi ulnarisgroove as a predictor for recognition of standard posteroanterior ra-diographs of the wrist. J Hand Surg Am. 2002;27(2):252e257.
19. Lees VC, Sheker LR. The radiological demonstration of dynamiculnar impingement. J Hand Surg Br. 1997;22:448e450.
20. Tay SC, Berger RA, Tomita K, et al. In vivo three- dimensionaldisplacement of the distal radioulnar joint during resisted forearmrotation. J Hand Surg Am. 2007;32(4):450e458.
21. Anderson ML, Skinner JA, Felmlee JP, Berger RA, Amrami KK.Diagnostic comparison of 1.5 Tesla and 3.0 Tesla preoperative MRIof the wrist in patients with ulnar-sided wrist pain. J Hand Surg Am.2008;33(7):1153e1159.
22. Hobby JL, Tom BD, Bearcroft PW, Dixon AK. Magnetic resonanceimaging of the wrist: diagnostic performance statistics. Clin Radiol.2001;56(1):50e57.
23. Haims AH, Schweitzer ME, Morrison WB, et al. Limitations of MRimaging in the diagnosis of peripheral tears of the triangularfibrocartilage of the wrist. AJR Am J Roentgenol. 2002;178(2):419e422.
24. Zanetti M, Linkous MD, Gilula LA, Hodler J. Characteristics oftriangular fibrocartilage defects in symptomatic and contralateralasymptomatic wrists. Radiology. 2000;216(3):840e845.
25. Totterman SM, Miller RJ, McCance SE, Meyers SP. Lesions of thetriangular fibrocartilage complex:MR findingswith a three-dimensionalgradient-recalled-echo sequence. Radiology. 1996;199(1):227e232.
26. RinglerMD,HoweBM,AmramiKK,HagenCE,BergerRA.Utility ofmagnetic resonance imaging for detection of longitudinal split tear ofthe ulnotriquetral ligament. J Hand Surg Am. 2013;38(9):1723e1727.
27. Ehman EC, Hayes ML, Berger RA, Felmlee JP, Amrami KK. Sublux-ation of the distal radioulnar joint as a predictor of foveal triangularfibrocartilage complex tears. JHandSurgAm. 2011;36(11):1780e1784.
28. Garcia-Elias M, Lluch AL, Ferreres A, Lluch A, Lhamby F. Trans-verse loaded pronosupination test. J Hand Surg Eur Vol. 2008;33:765e767.
29. Ishikawa J, Iwasaki N, Minami A. Influence of distal radioulnar jointsubluxation on restricted forearm rotation after distal radius fracture.J Hand Surg Am. 2005;30(6):1178e1184.
30. Baek GH, Ghung MS, Lee YH, Gong HS, Lee S, Kim HH. Ulnarshortening osteotomy in idiopathic ulnar impaction syndrome.J Hand Surg Am. 2005;87(12):2649e2654.
31. Iwasaki N, Ishikawa J, Kato H, Minami M, Minami A. Factorsaffecting results of ulnar shortening for ulnar impaction syndrome.Clin Orthop Relat Res. 2007;465:215e219.
32. Constantine KJ, Tomaino MM, Herndon JH, Sotereanos DG. Com-parison of ulnar shortening osteotomy and the wafer resection pro-cedure as treatment for ulnar impaction syndrome. J Hand Surg Am.2000;25(1):55e60.
33. Smet LD, Vandenberghe L, Degreef I. Ulnar impaction syndrome:ulnar shortening vs arthroscopic wafer procedure. J Wrist Surg.2014;3(2):98e100.
34. Stockton DJ, Pelletier ME, Pike JM. Operative treatment of ulnarimpaction síndrome: a systematic review. J Hand Surg Eur Vol.2015;40(5):470e476.
35. Kim JP, ParkMJ. Assessment of distal radioulnar joint instability afterdistal radius fracture: comparison of computed tomography and clin-ical examination results. J Hand Surg Am. 2008;33(9):1486e1492.
36. van Schoonhoven J, Mühldorfer-Fodor M, Fernandez DL,Herbert TJ. Salvage of failed resection arthroplasties of the distalradioulnar joint using an ulnar head prosthesis: long-term results.J Hand Surg Am. 2012;37(7):1372e1380.
37. Willis AA, Berger RA, Cooney WP III. Arthroplasty of the distalradioulnar joint using a new head endoprosthesis: preliminary report.J Hand Surg Am. 2007;32(2):177e189.
38. Kakar S, Swann RP, Perry KI, Wood-Wentz CM, Shin AY,Moran SL. Functional and radiographic outcomes following
ol. 41, April 2016

c. Sachar K. Ulnar-sided wrist pain: evaluation and treatment of trian-gular fibrocartilage complex tears, ulnocarpal impaction syndrome andlunotriquetral ligament tears. J Hand Surg Am. 2008;33(9):1669e1679.
d. Greenberg JA. Reconstruction of the distal ulna: instability, impaction,impingement and arthrosis. J Hand Surg Am. 2009;34(2):351e356.
e. Bickel KD. Arthroscopic treatment of ulnar impaction syndrome.J Hand Surg Am. 2008;33(8):1420e1423.
f. Griska A, Feldon P. Wafer resection of the distal ulna. J Hand SurgAm. 2015;40(11):2283e2288.
g. Scheker LR. Implant arthroplasty for the distal radioulnar joint.J Hand Surg Am. 2008;33(9):1639e1644.
h. Jupiter JB. Tendon stabilization of the distal ulna. J Hand Surg Am.2008;33(7):1196e1200.
i. Slater RR. The Sauve-Kapandji procedure. J Hand Surg Am.
564 FOUR-LEAF CLOVER TREATMENT ALGORITHM
distal ulna implant arthroplasty. J Hand Surg Am. 2012;37(7):1364e1371.
39. Laurentin-Pérez LA, Goodwin AN, Babb BA, Scheker LR. A studyof functional outcomes following implantation of a total distal radi-oulnar joint prosthesis. J Hand Surg Eur Vol. 2008;33(1):18e28.
40. Kakar S, Fox T, Wagner E, Berger R. Linked distal radioulnar jointarthroplasty: an analysis of the APTIS prosthesis. J Hand Surg EurVol. 2014;39(7):739e744.
41. Seo KN, Park MJ, Kang HJ. Anatomic reconstruction of the distalradioulnar ligament for posttraumatic distal radioulnar joint insta-bility. Clin Orthop Surg. 2009;1(3):138e145.
42. Atzei A, Rizzo A, Luchetti R, Fairplay T. Arthroscopic foveal repairof triangular fibrocartilage complex peripheral lesion with distalradioulnar joint instability. Tech Hand Up Extrem Surg. 2008;12(4):226e235.
EDITOR’S SUGGESTIONS FOR MOREINFORMATION
a. Kleinman WB. Stability of the radioulnar joint: biomechanics,pathophysiology, physical diagnosis and restoration of function,what we have learned in 25 years. J Hand Surg Am. 2007;32(7):1086e1106.
b. Roenbeck K, Imbriglia JE. Peripheral triangular fibrocartilage complextears. J Hand Surg Am. 2011;36(10):1687e1690.
2008;33(9):1632e1638.j. Adams BD, Berger RA. An anatomic reconstruction of the distal
radioulnar ligaments for posttraumatic distal radioulnar joint instability.J Hand Surg Am. 2002;27(2):243e251.
k. Iwasaki N, Minami A. Arthroscopically assisted reattachment ofavulsed triangular fibrocartilage complex to the fovea of the ulnarhead. J Hand Surg Am. 2009;34(7):1323e1326.
l. Tang CY, Fung B, Rebecca C, Lung CP. Another light in the dark:review of a new method for the arthroscopic repair of triangularfibrocartilage complex. J Hand Surg Am. 2012;37(6):1263e1268.
m. Geissler WB. Arthroscopic knotless peripheral triangular cartilagerepair. J Hand Surg Am. 2012;37(2):350e355.
JOURNAL CME QUESTIONS
The “Four-Leaf Clover” Treatment Algorithm:A Practical Approach to Manage Disorders ofthe Distal Radioulnar Joint
In contrast to the soft tissue restraints of the distalradioulnar joint, the osseous constraints accountfor the following percentage of the stability of thatjoint:
a. 10%
b. 20%
c. 30%
d. 40%
e. 50%
Which radiographic view of the forearm and wristis most suited to demonstrate distal radioulnarconvergence?
a. Lateral, 20� tilt
b. Antero-posterior clenched fist
c. Oblique
d. Lateral, 5 lb weight
e. Anteroposterior, radial deviated
J Hand Surg Am. r V
With regard to the osseous distal radioulnar joint,by what percentage is the radius of curvature ofthe sigmoid notch greater than that of the ulnahead?
a. 10%
b. 20%
c. 30%
d. 40%
e. 50%
In the normal distal radioulnar joint, the meandorsal displacement of the ulna fovea duringmaximum isometric pronation is:
a. 0.2 mm
b. 0.5 mm
c. 0.8 mm
d. 1.1 mm
To take the online test and receive CME credit, go to http://www.jhandsurg.org/CME/home.
ol. 41, April 2016