Embed Size (px)
DESCRIPTION
Arthritis of the Upper Limb To be added to the invitation list please email [email protected]
Citation preview

IN THIS ISSUE...
GENERAL CONCEPTS – Professor Cathy Speed see page 4
ARTHRITIS OF THE SHOULDER – Mr Andy Richards see page 8
ARTHRITIS IN THE ELBOW, HAND, WRIST – Mr David Hargreaves see page 12
The Fortius Clinic Lecture Series - October Issue
ARTHRITIS OF THE UPPER LIMB
IN THIS ISSUE...
GENERAL CONCEPTSProfessor Cathy Speed - see page 4
ARTHRITIS OF THE SHOULDERMr Andy Richards - see page 8
ARTHRITIS IN THE ELBOW, HAND & WRISTMr David Hargreaves - see page 12
“DOES ARTHRITIS HAVE AN OCCUPATIONAL LINK?”See page 13 to read more

32
Hi everyone, and welcome to our new look digital edition. It can be accessed online and also downloaded as a PDF. As ever, we’d love to hear your views.October was the first month of our new series of lectures and we have had had really positive feedback from all of you, which is great to hear! We welcomed Mr David Hargreaves, Mr Andy Richards and Professor Cathy Speed to the front, who talked on the broad topic of ‘arthritis in the upper limb’.
Professor Speed opened the evening, speaking about non surgical treatments, and giving a holistic view of Arthritis. As she made clear in her lecture, Arthritis is not just a disease of old age and there are more than 200 forms. The development of arthritis is influenced by 4 principal factors: genetics, mechanical influences, metabolic factors, and in some cases, immune function.
Mr Andy Richard’s lecture covered Glenohumeral joint arthritis, and joint replacement which is less common than hip and knee replacements. He picked up where Professor Speed’s finished
and looked at some of the secondary causes, including Atraumatic osteonecrosis, post inflammatory, post surgical and post-traumatic causes. He included a brief history of shoulder joint replacement and changing approaches.
In the final lecture Mr David Hargreaves talked about ‘the rest’ – elbow, hand, wrist and thumb, managing to throw in a few double entendres and raise some laughs, despite the unlikely subject matter! He covered the conditions, presentation and treatment both conservative and surgical. Along the way we learnt why the OK procedure was shortened...‘Outerbridge Kashiwagi procedure’ is a bit of a mouthful.
We enjoyed a very stimulating and engaging discussion between the speakers after they had presented, with great contribution from the floor. The MDT team were as enthusiastic as the audience about the opportunity to learn from each other.
The Fortius Lecture EveningEvery month the Fortius Clinic hosts a lecture evening for physiotherapists, Sports and Exercise Medicine professionals, led by a different team of specialists. The evening event is held in central London. If you would like to be added to our invitation list, please email RSVP@ fortiusclinic.com.
Mary Jones MSc MCSP Director of Research and Outcomes
Arthritis ClinicIf you have a patient that you think would benefit from a specialised arthritis consultation, contact us for more information on The Arthritis Clinic, which is led by Professor Cathy Speed. Her philosophy is to provide a holistic approach to managing arthritis, to ensure the best outcome for you, whether there is one joint affected or many areas. For more information on this service please contact us on 0203 195 2442 or [email protected].

54
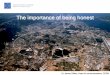
FEATURE | UPPER LIMB ARTHRITIS SESSION – GENERAL CONCEPTSArthritis is conventionally been classified as either ‘non-inflammatory’ osteoarthritis or ‘inflammatory’ (the rest, such as RA, gout, psoriatic arthritis, ankylosing spondylitis, infections, reactive). This definition is not accurate, as we now recognise that inflammation plays a role in osteoarthritis too.Different forms of arthritis are characterised by the pattern and symmetry of joints affected, the primary sites of the pathology in articular structures, and extra articular & systemic manifestations. WHICH FORM OF ARTHRITIS?The development of arthritis is influenced by 4 principal factors: genetics, mechanical influences, metabolic factors, and in some immune function. [see fig 1]
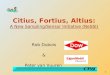
Once an individual has developed arthritis, it is vital to optimise mechanical influences across the joints, and metabolic health. The latter is important since anything that increases systemic inflammation – such as diabetes, high
lipids, other medical conditions – can influence the progression of ANY form of arthritis. [see fig 2]
Diagnosis of arthritis depends on careful clinical evaluation including a history (pain, swelling, stiffness, extra-articular symptoms), family history, and past medical history. Examination aims to identify the joints, pattern and symmetry of the disease, synovitis, skin and other changes, and level of function. Blood tests can often be helpful. Plain x-rays show changes only relatively late in the disease process. MRI can be a very useful tool. An early diagnosis is important to prevent progression of the disease. Education, exercise, biomechanical changes and pain management are all important. Inflammatory arthritides are treated with specific disease modifying agents.
Lecture by Professor Cathy Speed, Consultant in Rheumatology, Sports & Exercise Medicine
THERE ARE MORE THAN 200 FORMS OF ARTHRITIS AND ALL AGES
CAN BE AFFECTED
OBESITYANATOMIC ABNORMALITIESMICROFRACTURES & BONY
REMODELLINGLOSS OF JOINT STABILITY
TRAUMA
AGINGGENETIC & METABOLIC DISEASEINFLAMMATIONIMMUNE SYSTEM ACTIVITY
CARTILAGE BREAKDOWN
COMPROMISED CARTILAGE
BIOPHYSICAL CHANGESCollagen network fracture Proteoglycan unraveling
BIOCHEMICAL CHANGESInhibitors reduced
Proteolytic enzymes increased
ABNORMAL STRESSES
ABNORMAL CARTILAGE
Adapted from Mandelbaum B. Orthopedics. 2005
Fig 2: pathogenic Factors in Osteoarthritis
Fig 1: Which form of Arthritis?
RHEUMATOID PSORIATIC ANKYLOSINGSPONDYLITIS
OSTEOARTHRITIS

76
AN EARLY DIAGNOSIS IS IMPORTANT TO PREVENT PROGRESSION OF THE DISEASE Osteoarthritis is a heterogenous disease and patients differ in their likelihood of response to interventions, because pain may be driven by inflammation, subchondral bone oedema lesions, mechanical nociception, neural ingrowth and neuropeptides and the development of peripheral and central sensitisation. These characteristics can
be identified through careful evaluation and treatments are targeted appropriately.Supplements can be helpful: antioxidants in the form of omega 3 / fish oil to reduce systemic inflammation; vitamin D may influence pain and function; and there is some evidence that glucosamine/chondroitin may benefit symptoms in generalized OA of the hands. Thumb splints may help OA of the thumb.
Source Thompson (2002)
Professor Cathy Speed BMedSci BMBS MA Dip Sports Med PhD FRCP FFSEM (UK) Consultant in Rheumatology, Sport and Exercise Medicine.Professor Speed specialises in the management of elite athletes and patients of all ages with arthritis and complex pain, bone and soft tissue conditions.
In a recent 24-week randomized controlled trial, the effects of a traditional Chinese herbal remedy called TWHF (20mg three times daily) have been compared to methotrexate (MTX) alone (12.5 mg weekly), and combined TwHF + MTX combined in a sample of 207 patients with rheumatoid arthritis. A significant improvement was seen in all 3 groups, with the TwHF being effective in more patients. The combined group was statistically more effective than MTX alone This is a short study and often MTX is used in higher doses, but nevertheless is an interesting finding an no doubt should be researched further. The effects of TwHF in other autoimmune diseases and cancer are also being evaluated.
MUSCULOSKELETAL MATTERSARTHRITIS - HERBAL REMEDY FOR RHEUMATOID ARTHRITIS?
SOUR CHERRIES FOR JOINT INFLAMMATIONIn a small study of patients with inflammatory osteoarthritis, participants drank tart cherry juice twice a day for three weeks, and significant reductions in levels of inflammatory markers were noted. It is thought that tart cherries’ effects on inflammation may be due to their antioxidant compounds, called anthocyanins. Previous small studies have also shown these effects; further research is still needed.

98
Glenohumeral joint arthritis is not uncommon, but is less common than hip and knee replacements, as you can see from the list of operative treatments below.
OPERATIVE TREATMENTS HIPS 112,000 /YRKNEES 96,000/YRSHOULDERS 4,500/YRELBOWS 930/YR
Of the 4,500 shoulder replacements last year, Mr Richards and Mr Corbett did 50.The primary causes of shoulder arthritis are well explained by Professor Cathy Speed’s article. This article will pick up where Professor Speed’s finished and will look at some of the secondary causes.SECONDARY CAUSES• Atraumatic osteonecrosis - Alcohol induced - Corticosteroid therapy - Cytotoxic drugs - Radiation - Sickle cell disease
• Post inflammatory - Crystal/ post infection/ rheumatoid
arthritis• Post surgical - Capsulorrhaphy arthropathy – surgeons
used to burn the capsule to make it stiffen up. This may have been popular at one stage, but now we realise that there was a lot of arthritis secondary to the heat damage. You don’t see this anymore.
- Intra-articular hardware (e.g., screws, staples)
- Overtightened anterior joint capsule (prior Putti-Platt repair) – surgeons used to over-sew the suscapularis very tightly at the front to stop the shoulder coming out. This used to tighten the shoulder so much that it would cause arthritis. Again we have learnt not to do this anymore.
• Post-traumatic - Dislocation - Malunion of the proximal humerus
HOW DO WE DIAGNOSE IT? How does it present?Pain – patients present with a global pain, a deep aching sensation with a bit of a posterior focus. They will get pain at waist height, which differentiates them from the cuff tears and impinges. They get stiffness and a catching sensation, crepitus, and the pain tends to be progressive.
“BEWARE THE YOUNG MALE WITH PAIN THAT DOESN’T GO AWAY”
A group that don’t present like that are the early arthritics – beware the young male with pain that doesn’t go away, that have played rugby as teens. The pain doesn’t ever completely go away, they have a normal x-ray. The MRI scan shows more.
FEATURE | ARTHRITIS OF THE SHOULDER
EXAMINATIONPatients with arthritis of the shoulder will have a global restriction in movement . In contrast to those with the frozen shoulder who lose external rotation, the arthritics lose all rotation. They tend to have negative impingement signs. Always test for integrity of rotator cuff, get three views on the xray, and compare active with passive range.
“ALWAYS TEST FOR INTEGRITY OF ROTATOR CUFF, GET THREE VIEWS ON THE XRAY, AND COMPARE ACTIVE
WITH PASSIVE RANGE”
INVESTIGATIONSCT scans don’t help with diagnosis but they do help with surgical planning, as they indicate whether there is enough bone stock to do a replacement.MRI scan and Ultrasound will occasionally be useful – showing if there is a cuff tear or not, which is also helpful for surgical planning. There is no cure for arthritis so all the surgeon can do is reduce their symptoms, and pain. Range of movement (ROM) and function may be increased through reducing pain.
“THERE IS NO CURE FOR ARTHRITIS SO ALL THE SURGEON CAN DO IS
REDUCE SYMPTOMS - PAIN”
You may have heard of a new approach from the US, “Comprehensive arthroscopic management of glenohumeral joint arthritis” or CAM.It is a very precise combination of surgical procedures that is aimed at treating all of the
major pain generators in the shoulder region. Recommended for younger, active patients with arthritis, as it’s better if patients have some cartilage left. The procedure consists of a combination of:• Capsular release• Chondral abrasion and clean up• Labral debridement• LHB tenotomy• Excision of bone spurs• Arthoscopic release of axillary nerves• Subacromial decompression• Excision ACJEssentially you’re going in there and doing absolutely everything you can to the shoulder joint, without replacing it. His outcome is successful – results are good (ish), but very short-term follow up, this is the only paper on it, (http://www.ncbi.nlm.nih.gov/pubmed/23544687) and there is only one surgeon doing it. In my view it is ok- it does no harm.
REPLACEMENT SURGERY – A BRIEF HISTORYThere are 4,500 replacements for arthritis a year, of various sorts.The first arthroplasty was performed in 1894 by Jean Pean – using a platinum and rubber arthroplasty.The next arthroplasty to take off was by Charles Neer in the 1950s – spawned over 70 different designs.
The next big step forward was taken by Steve Copeland who decided that stems were problematic and that large amounts of perfectly decent bone was being removed.
In the 90s and following decade, resurfacing was the thing to do, involving minimal bone resection. The broken humeral head was replaced with an artificial joint, without replacement of the glenoid, and the fractured bone reconstructed around the artificial joint. This avoided glenoid issues.Then 5-10 years ago, the research showed that total shoulder replacements were better than hemi-arthroplasties, displaying better function and better pain relief.But it is difficult to do a shoulder replacement when doing a resurfacing as you don’t take the head off, so it is difficult to access the glenoid. We needed to resect the head, so we needed new kit.
There is still a role for hemiarthroplasty. Artificial components are not designed to withstand some of the demands that active individuals expect to place on them once comfort and function have been restored. This is particularly true for the glenoid that is prone to wear out loosen or even break in very active individuals.
Lecture by Mr Andy Richards, Consultant Shoulder Surgeon

1110
Patients who intend to return to activities that place physical demands on the shoulder replacement (such as golf tennis skiing weightlifting etc.) may therefore be at risk for eventual failure of the artificial shoulder socket. In these patients an alternative biological resurfacing that removes the destroyed cartilage and provides a smooth and stable surface without insertion of the plastic socket may be more sensible. Alternatively, it is sometime the case that there is insufficient bone stock for a glenoid replacement. These decisions need to be made on a case by case basis.
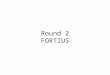
REVERSE GEOMETRY ARTHROPLASTY The rocking horse glenoid: If a total shoulder replacement is attempted when the cuff is deficient, the humeral head will not centre. The head will rock around and the humeral replacement will rock on the glenoid and it will loosen it. So we don’t do it.This is when we may consider the reverse geometry arthroplasty, for cuff tear arthropathy. Cuff tear arthropathy is arthritis of the shoulder that develops when the rotator cuff is damaged and patients get a painful pseudoparalytic shoulder, due to the loss of their fulcrum. For these patients, conventional total shoulder replacement may result in pain and limited motion, and reverse total shoulder replacement may be an option.A conventional shoulder replacement device mimics the normal anatomy of the shoulder, but in a reverse total shoulder replacement, the socket and metal ball swap places. The metal ball is fixed to the socket and the plastic cup is fixed to the upper end of the humerus.The reverse total shoulder replacement relies on the deltoid muscle, instead of the rotator cuff, to power and position the arm. The centre of rotation is lowered and medialised, improving arm movement and giving a better glenoid fix.
AND IT WORKS.There was a huge increase in this procedure in the 90’s and noughties, but also a huge increase in complications, with a rate of 50-60%, due to infection, nerve damage, dislocation and notching.The complication rate is now down to 20%, of which most is the notching. Now the reverse geometry has a widespread use for the correct indication such as in cuff arthropathy and revision procedures when the cuff is no longer working.
Mr Andy Richards MB BS FRCS (Orth) FFSEM (UK) Consultant Orthopaedic Shoulder and Elbow SurgeonMr Richards’ clinical interests are arthroscopic shoulder and elbow surgery particularly in treating sports injuries.
The first Fortius international sports injury conference is taking place next year on October 13th-14th, at the Queen Elizabeth II
Conference Centre, in central London.
For more information on the event please contact us, or visit the website www.fisic.co.uk.

1312
FEATURE | OSTEOARTHRITIS OF THE ELBOW, HAND AND WRISTLecture by David Hargreaves, Orthopaedic Hand, Wrist and Elbow Surgeon
ELBOW ARTHRITISAnyone can develop the arthritis of the elbow: whether post traumatic, following a fracture, or Idiopathic, which is the most common, but some people are more likely to develop arthritis because of their lifestyle, occupation, or habits. Any job that requires you to make the same motions day after day, year after year, puts you at increased risk for arthritis. Studies have shown a higher incidence of osteoarthritis of the elbow in steelworkers, blacksmiths, stonemasons and miners.And sports such as boxing or activities like press ups can increase incidence - I’m seeing quite a few former weightlifters, cage fighter and boxers who are now in their 30’s and 40’s with significant degenerative change.The radio-capatellar articulation (radial head) is the first area of the joint to be affected, The ulno –humeral articulation is often well preserved till late in the processThe first thing that happens inside the joint is the formation of the osteophytes. Marginal osteophytes don’t usually cause a problem in other joints, but in the elbow they cause impingement at the extremes of flexion and extension and thus reduce the arc of motion.Osteophytes will often form around the medial side of the joint line, and 20% patients with OA elbow have osteophytes adjacent to the ulnar nerve, which subsequently can causes ulnar nerve compression.
HOW DO THEY PRESENT?
Initial symptoms include pain and stiffness around the elbow. Patients find that it becomes increasingly difficult to bend or straighten the elbow as well as pain with forearm rotation. Initially, most patients have pain with lifting or with extremes of motion. In advanced stages, pain can be severe at night or at rest during the daytime. There may be synovitis in the joint causing swelling and inflammation.In some cases, patients can also have feelings of instability and weakness in t he elbow.Other symptoms include locking of the elbow or catching sensation from loose bodies in the elbow. Osteophytes may break off and start to cause an intermittent mechanical obstruction to the elbow movement (locking). Patients may also get locking because of soft tissue interposition –thickening of the synovial plica, which is located on the posterior radio-capitellar joint line. This is slightly different from tennis elbow, which has pain over the lateral epicondyle.
HOW CAN WE TREAT THEM? ARTHROSCOPYIn the earlier stages of OA, surgeons can arthroscopy remove loose bodies, tidy up the synovitis and remove the impinging osteophytes. This will all help with movement and function, and therefore reduced pain. The removal of the osteophytes doesn’t give back normal movement. The removal of loose bodies resolves the locking , but also often improves the range of
motion as well.Sometimes, when the radial head degeneration is the cause of pain arthroscopic radial head resection can be useful. BUT care must be taken as resecting the radial head can lead to increased instability.We can also do open surgery
to remove the fragments – the OK procedure – shorthand for the proper name, the Outerbridge Kashiwagi procedure… Fusion of the elbow is also a theoretical option, but there is no single position that offers a good functional position for the elbow to be fused in … so we try to avoid elbow fusions.
ELBOW REPLACEMENTS Elbow replacements can offer an excellent improvement in function , but because of the risk of loosening we try to avoid this in patients under 60years old.The results are slightly less good than in Hip and knee surgery:– 80-85% good or excellent results at 10 years.
THE WRIST NOT ONE JOINT BUT THREE. The anatomy of the wrist joint is probably the most complex of all the joints in the body. A collection of many bones and joints let us use our hands in lots of different ways.
The midcarpal joint allows movement in the “dart throwing” axis, the Radio-Carpal joint provides most of flexion and extension, and the Distal radio-Ulnar provides rotation.

1514
Arthritis of the wrist does happen but usually as a consequence of SNAC (scaphoid non-union advanced collapse – arthritis after an untreated scaphoid fracture), a SLAC (scapholunate advanced collapse) or a SMAC (scaphoid malunion advanced collapse).
PRESENTATIONPatients present with wrist pain, which settles, then will hurt again after activity. This discomfort starts with the arthritis of the impingement of the distal scaphoid against the radial styloid – that’s where the patients start getting their pain. Then it progresses to the whole of the scaphoid and then between capitate and scaphoid. The last place is the radio lunate articulation – that is almost always preserved. Idiopathic arthritis of the wrist only ever occurs in the STT joint – not on the ulnar side.
TREATMENTIn some cases, fusing the bones of the wrist together will reduce or eliminate pain and improve grip strength. However, wrist fusion substantially diminishes function and is usually avoidable. We want to keep function and movement so instead of doing full fusions we do a partial wrist fusion. Arthritis rarely affects all the joints of the wrist and there are now several movement–sparing procedures which can give predictably good outcomes.There are many different types of partial wrist fusions, which is not surprising when you consider the large number of bones involved
in the wrist joint.Radiolunate fusion can be a good solution and is most commonly performed for rheumatoid arthritis.Other types of fusion are Scaphocapitate fusion; Radioscapholunate fusion; Lunotriquetral fusion; STT fusion (scaphotrapeziotrapezoidal fusion); Four corner fusion (fusion of the capitate, lunate, hamate and trapezium with scaphoid excision);We can remove the arthritic joint with open surgery or arthroscopic surgery. The problem is that this can destabilise the wrist – which then causes a collapse of carpal bones.PRC or proximal row carpectomy is a radical excision, to remove the proximal row and bring the capitate down and articulate it into the lunate fossa, thus effectively changing a complex joint in the wrist to a simple yet workable hinge.
The procedure preserves a satisfying ROM and pain relief, and is recommended when
the head of the capitate and the lunate fossa are not affected by arthrosis.Wrist replacement is considered a last option as long term results are inconsistent.
THUMB ARTHRITISOsteoarthritis in the thumb is the most common form of arthritis in the hands. It can affect the basal joint or thumb CMC ( carpometacarpal)basal joint. It is slightly more common in non dominant hands as patients tend to hold things with the ‘non dom hand’. The basal joint normally allows you to pinch, pivot, and swivel your thumb for hundreds of tasks every day. Arthritis of the base of the thumb is more common in women than in men, (up to six times) and usually occurs after the age of 40. Previous fractures or other injuries to the joint such as Bennett’s fracture also increase the likelihood of developing osteoarthritis.
The cushioning cartilage wears away from the adjoining ends of the bones that form the carpometacarpal joint, so bone is rubbing against bone.
SYMPTOMS Thumb arthritis leads to pain in the basal joint on use of the thumb. Decreased grip strength, decreased range of motion, and swelling and pain throughout the hand make it difficult to do
simple household tasks, such as turning doorknobs, or opening jars.
Over time, swelling can result in an enlarged or out-of-joint appearance of the joint at the base of the thumb, A bony protuberance or bump can develop over the joint as well. The damage to the joint may result in growth of new bone along the sides of the existing bone (bone spurs), which can produce noticeable lumps on your thumb joint.
TREATMENTConservative treatment options include Splints, use of NSAIDs, activity modification and Steroid Injection.Treatment options include nonsteroidal anti-inflammatory drugs (NSAIDs), for pain relief and for decreasing inflammation and swelling. After a trial of bracing, activity modification, and use of NSAIDs is no longer effective and the pain becomes disabling, an injection of a long-acting corticosteroid into the thumb basilar joint may provide pain relief for a few months. However, the relief is usually only temporary and the arthritis in the joint will continue to progress.
SURGERYIf conservative management is no longer effective and the patient has persistent severe pain and weakness, there are a number of surgical options that would provide pain relief and improved function:Osteotomy: cutting the thumb metacarpal and repositioning the bone to take pressure off the joint. Can be useful in youngpatients , with early disease. Thumb arthrodesis (fusion): removing the diseased cartilage and fusing the bones in the affected joint. This provides stability and decreases pain. Although the patient may have improved strength with grip and lifting using the thumb without pain, there is some loss of flexibility.Thumb arthroplasty (replacement): Although there are joint replacements in the thumb, the long term results are quite poor –and they tend to loosen at an early stage.Trapeziumectomy (excision): Take
out the trapezium and try to stabilise base of metacarpal. The results are generally very good with much improved function because of the reduced pain. And it never wears out.
Mr David Hargreaves MBBS FRCS (Orth)Consultant Hand, Wrist and Elbow SurgeonMr Hargreaves treats a wide range of degenerative and traumatic conditions in adults and children. He specialises in minimal access surgery.

1716
FEATURE | OSTEOARTHRITIS IN PRIMARY CARE: EARLY DIAGNOSIS AND MANAGEMENTExtracts from an article by Professor Cathy Speed, published in GP Magazine on the 11th April 2014
Weight loss results in improvements in pain, function and progression of the arthritis. Every pound of weight lost will result in a fourfold reduction in the load exerted on the knee per step taken.6 Diet and exercise combined is the most effective behavioural method of weight loss; pain reduction in knee OA correlates with the amount of weight lost. [7]Strengthening exercise is important to reduce pain and improve function. Aerobic activities and those promoting proprioception are also encouraged.An initially supervised programme is more likely to be effective long-term and follow-up promotes adherence and better outcomes. Orthotics may help some with joint deformity.Patients should be advised to eat a Mediterranean diet. Cod liver oil is rich in omega-3 and vitamin D; vitamin D deficiencies should be corrected if necessary.NICE is reviewing its pharmacological recommendations for OA.[8] Analgesics to allow therapeutic exercise should be selected on the lowest risk/benefit ratio. Topical NSAIDs for superficial focal pain may be effective, as may capsaicin cream.
Some patients respond to paracetamol but this should not be continued if ineffective. Those with more inflammatory symptoms should be prescribed an NSAID/COX-2 inhibitor at the lowest dose for the shortest time, with PPI cover. A trial of up to three agents may be necessary.Low-dose colchicine may help those with inflammatory symptoms. Opiates should be used short-term and sparingly in recalcitrant pain. Aspiration of swollen joints can improve pain and function. Injection therapies are used sparingly. Steroid injections are used only in severe inflammation and pain in the absence of sepsis. Viscosupplement injections, although not recommended by NICE, may offer longer duration of relief than steroids.Hydroxychloroquine and/or low-dose colchicine may help some patients with hand OA. Agents under trial include biologics and those with effects on bone turnover. The latter may be particularly effective in those with bone lesions on MRI, which correlate with pain.Surgical referral should be considered for patients who continue to have symptoms and for whom OA has a significant effect on quality of life.
REFERENCES
1. Arthritis Research UK, 2008.
2. National Joint Registry for England and Wales, 9th Annual Report - 2012.
3. Lementowski PW, Zelicof SB. Obesity and osteoarthritis. Am J Orthop 2008; 37(3): 148-51.
4. Sellam J, Berenbaum F. Is osteoarthritis a metabolic disease? J Bone Spine 2013; 80: 568-73.
5. Hart DJ, Doyle DV, Spector TD. Association between metabolic factors and knee osteoarthritis in women: the Chingford Study. J Rheumatol 1995; 22: 1118-23.
6. Messier SP, Gutekunst DJ, Davis C et al. Weight loss reduces knee-joint loads in overweight and obese older adults with knee osteoarthritis. Arthritis Rheum 2005; 52: 2026-32.
7. Messier SP, Loeser RF, Miller GD et al. Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: the Arthritis, Diet, and Activity Promotion Trial. Arthritis Rheum 2004; 50: 1501-10.
8. NICE. Osteoarthritis: care and management in adults. CG177. London, NICE, 2014.
Osteoarthritis (OA), the most common musculoskeletal condition to affect synovial joints, causes significant pain and disability because of numerous effects on the whole joint. Approximately 1m primary care consultations for OA [1] and about 135,000 hip and knee replacements take place in the UK every year. [2] OA is a metabolically active process involving cartilage thinning and bone remodelling, the release of intra-articular cartilage debris, inflammatory cytokines and neuropeptides, and synovitis. Pain, swelling and disuse lead to muscle weakness, which, with other changes to joint biomechanics, leads to further pain through soft tissue strains.Hence inflammation, neuropeptides, bone remodelling, weakness and biomechanical changes are all targets for therapy.The principle risk factors for primary OA are genetics, body weight, biomechanical abnormalities and associated diseases.OA is closely linked to obesity. For every 5kg of weight gain, there is a commensurate
36% increased risk of developing OA.3 The link to obesity is not only mechanical, but also through systemic inflammatory effects on the joint, mediated by adipokines, and OA may simply be seen as a manifestation of metabolic disease. [4] Metabolic factors, such as hypertension, hypercholesterolaemia and blood glucose level, are all also associated with OA, independent of obesity. [5] The specific mechanisms involved are unclear.EARLY DIAGNOSISEarly osteoarthritis is often a clinical diagnosis. Patients typically present with activity-related joint pain, often localised. With time, swelling and limited early morning stiffness (30 minutes)In the early stages of the disease, X-rays are frequently normal. As the disease progresses, loss of joint space, subchondral sclerosis and osteophyte formation are seen. But ‘mild OA’ radiologically represents relatively advanced disease.Blood tests, including inflammatory markers, rheumatoid factor and uric acid, are normal,
although some patients may have a slightly elevated CRP. Vitamin D levels should be checked; low levels can contribute to muscle weakness and pain.[6]MRI scans show cartilage thinning and underlying bone lesions and can demonstrate low-grade synovitis and soft tissue changes.MANAGEMENTOA is an important diagnosis to make early, to allow for lifestyle changes that can help to influence prognosis. Subsequent follow-up is important to assess progress and reinforce lifestyle messages.Patient education is paramount. Ensuring the patient understands risk factors for the condition, the importance of weight management, metabolic disease control, therapeutic exercise, biomechanical alterations and approaches to sound pain management are the foundations of good treatment.Prognosis is strongly influenced by self-efficacy and the patient’s locus of control.
EARLY DIAGNOSIS AND MANAGEMENT OF PATIENTS WITH OSTEOARTHRITIS IS THE KEY TO EFFECTIVE CARE.

1918
NOVEMBER- Next month’s lecture
Mr Giles Heilpern MA (Cantab) MB BS FRCSEd (Tr & Orth) Consultant Orthopaedic Knee SurgeonMr Heilpern’s surgical practice encompasses all aspects of knee surgery but with a particular interest in meniscal injuries, ligament reconstruction and partial and total knee replacement.
Mr Peter Rosenfeld MB BS FRCS FRCS (Tr & Orth) Consultant Orthopaedic Foot and Ankle SurgeonMr Rosenfeld is the regional speciality trainer in foot and ankle orthopaedics and sports medicine and has particular fields of research in ankle replacement and cartilage reconstruction.
Dr Glyn Towlerton BSc MBBS(hons) MRCP FRCA FIPP FFMRCA Consultant in Spinal and Pain MedicineDr Towlerton has treated many elite athletes from a wide range of sports for over a decade. His special interests include spinal interventional procedures and injections and spinal cord stimulation.
Contact the Fortius Clinic If you would like to refer a patient to one of our consultants, please get in touch:
17 Fitzhardinge Street, London, W1H 6EQ
Tel: 0203 195 2442 Fax: 0203 070 0106
Email: [email protected] Web: www.fortiusclinic.com
Delete Arthritis as used elsewhereDelete Fisic, as used elsewhereWhole page article on imaging with big photo – Hattie can insert on Monday Delete Tendon with photo Delete French speakersDelete new joiner
We have X-ray, MRI, Ultrasound and Interventional Radiography scanning facilities at Fortius. Most scans can be performed on the same day and a patient will never have to wait more than 24 hours. We offer immediate reporting by our consultant radiologists.To refer a patient please call 0203 195 2446 or email [email protected]
IMAGING DEPARTMENT• Same day appointments • Reporting within two hours
UPDATE ON KNEE AND ANKLE REPLACEMENTS

Don’t forget to follow us on Twitter @FortiusClinicUK
You will also find us on Facebook and LinkedIn
t: +44 (0) 203 195 2442 or 0845 853 1000
f: 0203 070 0106
w: www.fortiusclinic.com
Fortius Clinic is situated in Central London, close to Selfridges, and just off Manchester Square.
17 Fitzhardinge Street London W1H 6EQ
For further information or to book an appointment, please contact us:
How to find us: