Embed Size (px)
Citation preview

Gastroenterologia Japonica Vol. 8, No. 4 1973--
339
- - O r i g i n a l A r t i c l e - -
THE FATE OF THE P A T I E N T S S U R V I V I N G A C U T E P A N C R E A T I T I S
- - W I T H SPECIAL R E F E R E N C E TO C H R O N I C I T Y OF A C U T E P A N C R E A T I T I S - -
Toshio Sato, M.D. and Yoichi Saitoh, M.D. Department of Surgery
Tohoku University School of Medicine 1-1, Seiryo-machi, Sendai, Japan
Summary In order to clarify the fate of patients who had survived acute pancreatitis, follow-up studies
were performed. The results were as follows: (1) the cases progressed from acute pancreatitis to chronic one were considered to be 37 (18%) out of 206 cases, if chronic pancreatitis is diagnosed on the basis of frequent seizures of abdominal pain; (2) of the 50 patients who studied various ex- aminations, 13 (26%) were considered to be chronic pancreatitis if the criteria for diagnoses were based on the seizures of pain and on the disturbance of the pancreatic endocrine and exocrine functions; (3) the patients who showed final clinical picture, such as pancreatic lithiasis, severe diabetes mellitus, and steatorrhea were observed in four (7%) out of 62 cass: (4) those who could be diagnosed as chronic pancreatitis on the basis of overall test amounted to I 1 (18~ out of all the 62 cases who underwent our examinations.
I n the discussion of the et iology and pathogenesis o f c h e ronic pancreat i t i s , a pro- b l em has to be clarified to w h a t extent acute pancrea t i t i s progresses to the chronic fo rm o f this disease. For this prupose, it is d e e m e d m a n d a t o r y to follow up the pa t ien ts who had survived acute at tacks of pancrea t i t i s in m a n y pa t ien ts with this desease. Par t icu lar ly to be ment ioned is tha t it should be by all means clarified in w h a t fate the pat ients wi th acute pancrea t i t i s in J a p a n e s e people are destined, because the etiology and pathogenesis o f pancrea t i t i s repor ted ly v a r y with the races and nations to a considerable extent. T h e purpose of this s tudy is to follow up the pat ients who had survived at tacks of acute pancreat i t i s and to clarify the fate of the survivors.
I. Subjec t s
T h e subjects we selected for this s tudy were the cases with acute pancrea t i t i s exper ienced in the pas t 10 years at m a n y hospitals in nor th-eas te rn disrtict of J a p a n . I n order to exclude the cases resembl ing acute pancreat i t is , 364 cases
Key word: Chronic pancreatitis, Glucose tolerance test, Secretin test, Provocative pancreozymin-serum secretin serum enzyme test, Diabetes mellitus.

340 r . SA TO and Y. S A I T O H
were selected for various observations, including 344 cases definitely diagnosed as acute pancreatitis through laparotomy and 20 cases who underwent laparotomy in our clinic.
The subjects included 57 cases (30 males and 27 females) in the third decade, 83 (57 males and 26 females) in the fourth, 72 (46 males and 26 females) in the fifth, 86 (49 males and 37 females) in the sixth, 50 (30 males and 20 females) in the seventh, and 16 (6 males and 10 females) in the eighth. Hence, males totalled 218 and females 146 in a ratio of 1.5 : 1. Those with identified causative factors of their illness totalled 135 cases, which included heavy alcohol ingestion in 56 cases, gallstone in 41, overeating in 26, ascariasis in seven, and excessive fatigue in five. Of 41 cases associated with cholelithiasis, 25 had stones in the gallbladder, while 16 had stones in the common bile duct. The findings of the pancreas at laparotomy can be classified into three types of edematous, hemorrhagic, and necrotic type. The edematous type included 169 cases (46.4%) and the hemor- rhagic type 90 cases (24.7%), while the necrotic type included 105 cases (28.8%). The surgery subjected to all the 364 cases can be classified into 278 with drainage, 27 with cholecystectomy and biliary drainage, 18 with cholecystectomy alone, 12 with biliary drainage. The classical drainage with incision of pancreatic capsule was applied to 12 cases. Deaths directly attributable to the operations were 68 out of 364 cases (18.6%), including 22.9% for males and 12.3% for females. The mortalities by the findings of the pancreas at laparotomy were 1.8% in the edematous, 23.3% in the hemorrhagic, and 32.3% in the necrotic type.
II. Results of Follow-up Studies
1. Late Deaths in Follow-up Period The prognoses of 296 cases who could tolerate the operation were subsequently
studied by questionnaires, obtaining 223 replies (75.3%). The reply percentage by the type ofpancreatitis included 62.1% in the edematous, 91.3% in the hemor- rhagic, and 88.1% in the necrotic type. Of all the 223 answered, 17 deaths were subsequently identified by follow-up study. The causes of deaths were pancreatic cancer in four, apoplexy in three, and hepatic cancer, gastric cancer, and reticu- losacroma, ileus, uremia, trauma, and dotage in one each. All the cases with pancreatic cancer were operated due to acute attacks of pancreatitis, and they died nine months, one year, thirteen months, and nine years after laparotomy, respectively. 2. Post-operative Complicat ions
Post-operative complications related to acute pancreatitis or operations of panc- reatitis included six cases with pancreatic cyst, five with recurrences ofpancreatitis, four with pancreatic abscess, three each with ileus, abdominal hernia, and diabetes mellitus, two with pancreatic fistula, and one each with cholelithiasis and hepatitis. 3. Post-operative Complaints
Complaints listed in the questionnaires were abdominal pain, back pain, diar- rhea, thirst and others. Abdominal pain was complained of by 97 (47%) out of 206 cases and back pain by 67 (33%), while diarrhea was complained of by 24 (12%) and thirst was by 41 (20%) (Table 1). Of the 97 cases with abdominal pain, 37 (38%) complained of pain so frequently as several times monthly, 56 (58%) complained of back pain. However, no significant correlation could be. found between the frequency of post-operative complaints and the type of pan- creatitis (Table 2).

The Fate of the Patients Surviving Acute Pancreatitis
Table 1. Post-operative Complaints Studied by Questionnaires
341
Type of Pancreatitis No. of Abdominal Back Pain Diarrhea Thirst Patients Pain
Edematous Type 92 39 34 6 11 (42.3) (36.9) (6.5) (11.9)
Hemorrhagic Type 61 31 19 10 19 (50.8) (31.1) (16.3) (31.1)
Necrotic Type 53 27 14 8 11 (50.9) (26.4) (15.0) (20.7)
Total 206 97 67 24 41 (47.1) (32.5) (11.6) (19.9)
Figures in parentheses show percentages.
Table 2. Abdominal Pain Studied by Questionnaires
No. of Abdominal Pain Type of Pancreatitis Patients Several times Several times Occaisionally With
with Pain per month per year complained Back Pain
Edematous Type 39 12 19 8 25 (30.7) (48.7) (20.5) (64.1)
Hemorrhagic Type 31 14 13 4 18 (45.1) (41.9) (12.9) (58.0)
Necrotic Type 27 11 11 5 13 (40.7) (40.7) (18.5) (48.1)
Total 97 37 43 17 56 (38.1) (44.3) (17.5) (57.7)
4. R e s u l t s o f E x a m i n a t i o n s at the T i m e o f F o l l o w - u p Various studies were performed mainly for cases who had post-operative com-
plaints and were available to examinations at our clinic. 1) Secretin test The secretin test was used for examining the pancreat ic exocrine function, and
the volume of duodenal aspirate, its bicarbonate concentrat ion and amylase out- pu t were assessed. The result was classified into mild disturbance when only one of the three values was low, moderate dis turbance when two of the three values were low, and marked disturbance when all of the three values were low.
O f all the cases available as above, 50 cases underwent the secretin test. In the edematous type, eight out of 19 cases showed disturbance in th secretin test, while eight out of 16 in the hemorrhagic type and 14 out of 15 in the necrotic type showed disturbance. In total, 30 cases (60%) showed disturbance of the pancreat ic exocrine function. Those with moderate and marked disturbance amoun ted to three (16%) in the edematous type, three (19%) in the hemorrhagic type and ten (67%) in the necrotic type, 32 as a whole (Tab le 3). No significant relationship could be seen between these results and the lapse of post-operative years. Furthermore, 20 out of 29 cases with abdominal pain and nine out of 12 with back pain showed disturbance in the secretin test (Tab le 4). I n the cases with disturbance in the secretin test, a decrease in the volume of duodenal aspirate and m a x i m u m bicarbonate concentrat ion was observed. An abnormal i ty in amylase value was infrequently observed compared with those in other factors.

342 T. SA TO and Y. SAITOH
Table 3. Secret in Test in Follow-Up Period Viewed f rom Type of Pancreat i t is
Result of Secretin Test
Type of Pancreatitis No. of Normal Mild Moderate Marked Patients Disturbance Disturbance Disturbance
Edematous Type 19 11 5 0 3 Hemorrhagic Type 16 8 5 1 2 Necrotic Type 15 1 4 6 4
Total 50 20 14 7 9
Table 4. Relationship between Postoperat ive Compla in t s and Result of Secretin Test in Follow-Up Period
Grade of Abdominal Pain Back Pain Disturbance With Pain No Pain With Pain No Pain
Marked Disturbance 6 3 2 7 Moderate Disturbance 5 2 2 5 Mild Disturbance 9 5 5 9 Without Disturbance 9 11 3 17
Total 29 21 12 38
2) Glucose tolerance test Glucose tolerance test was per formed in 62 cases. Its j udgemen t was done in
accordance with the standards proposed by the Commit tee of J a p a n Diabetes Society. 1~ Abnormali t ies were detected in 44 (70~o) out of 62 cases, including 18 with normal glucose tolerance curve, 20 with decreased glucose tolerance curve, and 24 with diabetic curve. While abnormali t ies of glucose tolerance test were seen in 17 (65%) out of 26 cases in the edematous pancreati t is , 27 (75%) out of 36 showed abnormali t ies in the hemorrhag ic and necrotic pancreati t is ( T a b l e 5). No significant relationship was seen between the results of this test and post-op- rative complaints.
Table 5. Re la t ionship between Type of Pancreat i t is and Result of Glucose Tolerance Test in Follow-Up Period
Result of Glucose Tolerance Test Type of Pancreatitis No. of Normal Decreased Diabetic
Patients Glucose Tolerance Curve Curve
Edematous Type 26 9 10 7 Hemorrhagic Type 16 4 5 7 Necrotic Type 20 5 5 10
Total 62 18 20 24
3) Provocat ive pancreozymin-secre t in serum enzyme test This test was performed in 52 cases, resulting in abnormali t ies in 16 cases (31%).
More abnormali t ies were seen in those with hemorrhagic and necrotic pancreati t is

The Fate of the Patients Surviving Acute Pancreatitis 343
than in those with edematous pancreatitis. Eleven out of 27 cases with post-op- erative complaints showed abnormalities in the results of this test, whereas only five showed abnormalities out of 25 without post-operative complaints.
4) Pancreatic scintigram Pancreatic scintigram was performed using Se-methionin. Normal scintigrams
were seen in 15, abnormal ones were seen in 11, which included three with scatter- ed pattern, one with pat tern of circumscribed defect, four with visualization of the head and body of the pancreas alone, two with visualization of the head of the pancreas alone, and one with no feasible visualization. The relationship between the results of this study and the type of pancreatitis were also examined to find that two cases with abnormalities were experienced against four normal cases in the edematous group and three cases with abnormalities were found out against seven normal cases in the hemorrhagic group, while six cases with abnormalities were detected against five normal cases in the necrotic group, showing that more cases with abnormalities were experienced as the pathological changes in the pan- creas advanced. 5. Relationship between Acute Pancreatit is and Chronic Pancreatit is
On the basis of the results thus obtained, further evaluation was done on the problem of progress from acute pancreatitis to chronic one.
1) Evaluation from clinical picture and the result of examination According to the criteria for diagnosis of chronic panereatitis so far proposed
by many authors, the results of our present study can be summarized as follows. On the basis of above mentioned results, chronic pancreatitis could be seen
in 97 (47%) out of 206 cases if viewed only from the attack of pain, while it could be seen in 37 (18%) out of 206 cases if viewed from the abdominal pain so frequent as several times per month. From the results of pancreatic function test, chronic pancreatitis could be found in 30 (60~o) out of 50 cases in terms of disturbance of the secretin test and 16 (32%) out of 50 cases if the cases with disturbance in more than two factors are regarded as abnormal. Furthermore, from the results of the glucose tolerance test, chronic pancreatitis could be seen in 44 (71%) out of 62 cases. I f chronic pancreatitis is defined to be those with the attack of pain and disturbance in the endocrine and exocrine functions of the pancreas, thirteen (26%) out of 50 cases could be considered to be chronic pancreatitis. However, since the pancreatic acinar structure is replaced by fattly tissue in some cases as described in the following chapter, if chronic pancreatitis may be claimed to fall under those with higher values of provocative pancreozymin-secretin serum en- zyme test (that is, those with remaining pancreatic functions), chronic pancrea- titis was seen in seven (19~o) out of 37 cases. In other words, those who still have pancreatic parenchyma despite the disturbance in the endocrine and exocrine functions of the pancreas and the attack of pain may be considered to be about 20% of all the cases we studied. I f chronic pancreatitis is defined from the criteria including pancreatic calcification, severe diabetes mellitus, or steatorrhea, four (7%) out of 62 can be considered to be chronic pancreatitis.
2) Evaluation from histology of the pancreas O f all the cases examined in our present study, four cases could be evaluated
from histology of the pancreas. Case 1 A male patient, aged 38. He had been affected by acute pancreatitis
and had undergone laparotomy about 6 years ago. The pancreas at laparotomy had been found diffusely necrotic. He had been treated successfully by abdominal drainage, but he did not quit drinking even after that and had seizures of pain as

344
Fig. 1.
T. SA TO and Y. S A I T O H
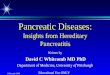
Case 1. Plain f i lm of the a b d o m e n d e m o n s t r a t - ing calc i f icat ions (arrows) in the region of the pancreas .
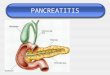
Fig. 2. Case 1. Hi s to logy of the pancreas s h o w i n g highly advanced f ibros i s wi th atrophic g landular cel ls and di latat ion o f the ductule.
often as more than 50 times. In our study six years and three months after lap- arotomy, marked disturbance was seen in the result of the secretin test and diabetic curve was found out in the glucose tolerance test. In addition, an abnormality was observed in the provocative pancreozymin-secretin serum enzyme test, and visualization of the head of the pancreas alone was seen in the pancreatic scint- tigram, while calcification in the region of the pancreas was observed in plain film of the abdomen (Fig. 1). This patient was, therefore, diagnosed as chronic pancreatitis associated with pancreatic calculi and was subjected to side-to-side pancreatico-jejunostomy. The histology of the pancreas showed highly advanced fibrosis and dilatation of the pancreatic duct (Fig. 2).

The Fate of the Patients Surviving Acute Pancreatitis 345
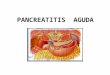
Fig. 3. Case 2. His to logy of the pancreas showing re- p lacement of acinar s tructure by fatty t i s sue and scattered atrophic is lets .
Fig. 4. Case 3. His to logy o f the pancreas showing m i l d f ibrosis around the ductule , wi thout intraac inar and interacinar f ibrosis .
Case 2 : A male patient, aged 43. He had undergone laparotomy due to acute pancreatitis two years ago. Hemorrhagia and enlargement were observed in the entire pancreas at that time, an abdominal drainage was then performed. He quitted drinking thereafter and has been exclusively engaged in the medical treat- ment such as limitation of fatty diets, and has been fairly improved in recent days to an extent that he complained of mild abdominal pain only occasionally after overeating. The glucose tolerance test showed a diabetic curve. No abnormality was seen in the secretin test or provocative pancreozymin-secretin serum enzyme test. However, the pancreatic scintigram visualized only the head of the pancreas. Gastric cancer was detected through the gastro-intestinal series at the time of our investigation, and total gastrectomy was performed. Upon laparotomy, normal consistency and size were observed in the head of the pancreas, but striking atrophy

346 T. SA TO and Y. S A I T O H
was observed at the tail of the pancreas. Total gastrectomy with resection of the tail of the pancreas was performed. Histologically, pancreatic acinar cells were totally replaced by fatty tissue. In the biopsy obtained at the same time from the head of the pancreas, nearly normal pancreatic histology could be ob- tained (Fig. 3).
Case 3: A male patient, aged 49. He had undergone laparotomy two years ago under the diagnosis of acute pancreatitis, and the pancreas allegedly had shown overall swelling. Thereafter, he had been occasionally complained of abdominal pain. Since he had undergone gastrectomy before our investigation, the secretin test was not applicable in our study. The values of urine and serum amylase were normal and the result of provocative pancreozymin secretin serum enzyme test was also normal, but the pancreatic scintigram indicated a scattered pattern. This patient was complicated by acute cholecystitis six months after our examination and had to be subjected to cholecystectomy. The biopsy of the pancreas hardly showed the traces of pancreatitis as shown in Fig. 4.
Case 4: A male patient, aged 39. He had undergone an abdominal drainage due to acute pancreatitis 13 years and seven months ago. The finding of the pancreas at that time had allegedly indicated hemorrhagia and swelling in the entire pancreas. The patient had continued to drink alcohol and had repeated attacks of pain, and he had been treated as diabetes mellitus since several years ago. According to our present study, marked disturbance was observed in the secretin test and diabetic curve was found out in the glucose tolerance test. An abnormality was observed in the provocative pancreozymin-secretin serum en- zyme test, while the pancreatic scintigram could not be visualized. This patient died eight months after our study due to uremia. The histology of the pancreas upon autopsy showed highly advanced fibrosis and atrophy of pancreatic acinar cells as well as calculi in the dilated fine pancreatic duct were observed (Fig. 5).
Fig. 5. Case 4. His to logy o f the pancreas showing intraacinar and interacinar f ibrosis in wh ich atrophic g landular cel ls are scattered, and dila- tat ion of the ductule wl th calculi ( inset at left).

The Fate of the Patients Surviving Acute Panceatitis 347
e o d
N
m ~.~ ' ~ 0 " ~ td ~
8 ~ . �9 ~ . ~
,.O ~ <
r ,.O ,.O ,.~
"6 "-8 -6 -8 ,.~ ,-el ~ 4zi
8 8 8 8 < < < <
& ~ ~ o ~
o ~ o o ~ o ~ '~
.-a ;6 ~ "5 8
~o~ o-~ ~ ~
"a
~.~ ~
�9 ~
~ ~ . , ~ . ~
~'~ 8 ~
"-a "a "-a ~
0 0 r , .a ,.~ 0 , .a r ~ < < < ~ < <
o
+ ~_ ~_ ~ +
i~ ~ ~
8 8 8 > ~ < < < 0 < @
0~
,-a
4
,-a
o
~F
,-a

348 T. SA TO and Y. S AI T OH
3) Cases progressed from acute pancreatitis to chronic pancreatitis Of all the 62 cases who responded to our request to visit our clinic, seven cases
indicated clinical symptoms such as painful seizures and disturbance in the en- docrine and exocrine function tests of the pancreas and provocative pancreozymin- secretin serum enzyme test. I t may be assumed that, of these seven cases, five may be considered to be the cases with chronic pancreatitis in a stricter sense, if the results of pancreatic scintigram are taken into consideration. Including these cases, 11 may be considered to be with chronic pancreatitis because they showed abnormalities in most of our tests as shown in Table 6. All of these 11 were males and eight had alcohol ingestion as the direct causative factor. In the Cases 1 and 4 in the table with no quitting of drinking even after the initial seizures, pan- creatic calculi was found and one of them repeated the painful seizures so frequent- ly as to qualify the side-to-side pancreatico-jejunostomy. The pancreas of these cases upon laparotomy indicated the finding of necrotic or hemorrhagic pan- creatitis in nine cases.
From the above-mentioned results, we studied the frequency of progress from acute pancreatitis to chronic one. Of the 50 cases who underwent the secretin test, 29 complained of abdominal pain. On the other hand, 20 out of 50 cases were identified to have been with disturbance in the secretin test and abdominal pain. 97 (47%) out of 206 cases who responded to our questionnaires complain- ed of abdominal pain. From the ratios as above, it may be concluded that 37 out of 206 cases had been affected by chronic pancreatitis. In other words, the frequency of progress from acute pancreatitis to chronic one amounts to about 18~ . Of all the cases who studied the secretin test, two out of I9 cases with ede- matous type, two out of 15 with hemorrhagic type and seven out of 16 with necrotic type were assumed to have been affected by chronic pancreatitis. Since the percentage of the cases with edematous type in all the patients amounted to 46.4%, while those with hemorrhagic type and necrotic type were 24.7% and 28.8%, respectively, the frequency of chronicity of acute pancreatitis were 4.8% for the edematous, 3.3% for the hemorrhagic and 12.6% for the necrotic type, respec- tively, totalling 20.7% in the patients who studied the secretin test. Deaths due to cancer during a short period after acute pancreatitis amounted to four cases.
III. D i s c u s s i o n
Dreiling & Janowitz ~ reported on the disturbance of pancreatic exocrine func- tion in acute pancreatitis, stating that volume of duodenal aspirate, maximum bicarbonate concentration and amylase output were within normal range in 76%, 67% and 58% of 113 patients studied the secretin test, respectively, and that even the patients who had shown abnormal function at the time of onset could be relieved in about a week to nearly normal function. Thus, the disturbance in pancreatic exocrine functin in patients who survived acute pancreatitis are deemed to be rapidly normalized. However, of the 50 cases on which we per- formed the secretin test in follow-up study after acute pancreatitis, the highest frequency of disturbance was seen, as a matter of course, in the pancreatic ex- ocrine function in the patients who had survived acute necrotizing pancreatitis, but the disturbance in the pancreatic exocrine function was observed in even eight out of 19 with edematous type and in 30 (60%) in total of three types. In regard to three factors of the secretin test, a decrease in the volume of duodenal aspirate and maximum bicarbonate concentration was observed more evidently than in

The Fate of the Patients Surviving Acute Pancratitis 349
the amylase value. Sebening 3~ reported, on the other hand, that the disturbance in glucose tolerance test could be normalized nearly completely in six months and completely in 12 months. Hence, it appears that the disturbance in pancrea- tic endocrine function tends to show the delay of recovery to normal conditions than the disturbance in pancreatic exocrine functon. In our series, of all the 62 cases who studied the glucose tolerance test, 20 were those with decreased glucose tolerance curve and 24 wee those with diabetic curve, while those with normal curve amounted only to 18. Those showing abnormalities of the glucose tolerance test in follow-up period were more frequent in those with hemorrhagic and necrotic pancreatitis, but it should be attended to that even those with ed- ematous pancreatitis showed abnormalities in seven out of 26. From our present study, we could not always draw a conclusion that the disturbance in the pan- creatic endocrine function can be normalized sooner than those in the exocrine functoin. In any event, it should be heeded to that such a high percentage of disturbance in the pancreatic exocrine and endocrine functions will remain after acute pancreatitis and that proper guidances should be given to the patients in their post-treatment regimens and lives with careful observations by the physi- cians.
The provocative pancreozymin-secretin serum enzyme test is presently re- commended as a testing method for prediction of abnormalities still actively remaining or persisting in the pancreas; it is regarded as a clue for diagnosis of persisting acute pancreatitis and detection of chronic relapsing pancreatitis. Abnormalities in the provocative pancreozymin-secretin serum enzyme test were seen in those who had highly advanced findings of pancreatitis upon laparotomy or who had post-operative complaints.
How many cases of acute pancreatitis do progress to the chronic form? Apart from some suggestions, there was no clear answer given to this question in the literature. In recent years, Trapnell 4~ reported that 20 (20%) out of 99 cases who survived idiopathic acute pancreatitis had recurrent attacks and that 59 out of 82 for whom gallstones were not extirpated and three out of 55 whose gall- stones were extirpated showed such recurrent attacks. Hence, it was shown that the recurrence of pancreatitis was experienced in 62 (45%) out of 137 cases with gallstones. However, he also stated in his report that, despite the high percen- tage of recurrences, the cases with acutal progress to chronic pancreatitis were so few as only one who had pancreatic dysfunction, four who had chronic relaps- ing pancreatitis and six who had pancreatic calculi. On the other hand, Edlund et al?' studied their patients on follow-up basis for two to seven years and reported that recurrent pancreatitis could be seen in all 14 severe alcoholics who had not changed their drinking habits.
According to our study, the frequency of chronicity of acute pancreatitis was 47% on the basis of the seizures of pain alone and 18% on the basis of seizures of highly frequent pain, taking into account the diagnostic criteria so far pro- posed by many authors. I f chronic pancreatitis is defined as those with abdo- minal pain and disturbance in the pancreatic endocrine and exocrine functions, the frequency of chronicity was 26O/o . However, it may also have to be pointed out that the cases with final patterns of chronic pancreatitis such as pancreatic calculi, severe diabetes mellitus, and steatorrhea were seen in only 7%. Tra- pnell 4~ reported that they could detect in 11 out of 236 cases these patterns similar to the above-mentioned final pattern. Their results were quite similar to those of our present study.

350 T. SA TO and Y. SAITOH
It is of great interest to study what tissue patterns the pancreas will show in patients who survived acute pancreatitis. We experienced three cases who underwent relaparotomy after the course of acute pancreatitis and one with aut- opsy. Histologically, two cases indicated typical patterns of chronic pancreatitis such as highly advanced fibrosis, atrophy of acinar cells and calculi, while one each showed either replacement of acinar structure by fatty tissue or absence of any trace of pancreatitis. Thus, the three patients for whom we could per- form relaparotomy after the course of acute pancreatitis had tissue patterns dif- ferent from each other. I f the presence of abdominal pain is regarded as the criterion of chronicity, the patients like Cases 2 and 3 may be eligible to be includ- ed in the category of chronic pancreatitis. In conjunction with patient like Case 2 whose pancreatic glandular tissue was totally replaced by fatty tissue, we earlier experienced that similar tissue pattern could be experienced in the tail of the pancreas of patient with pancreatic cyst at the body of the pancreas. It may have yet to be further argued to diagnose the above-mentioned tissue pattern as chronic pancreatitis. Therefore, unless histologically examined, it may be likely that not a few cases with what may be called the sequela of acute pancreatitis may occasionally be included in those patients who are diagnosed as chronic pancreatitis after the course of acute pancreatitis.
In 11 out of the 62 patients who underwent various test, it was considered likely that their symptoms had progressed to chronic pancreatitis if every possible judge- ment is directed to these cases ; the two cases out of them, who did not quit drink- ing alcohols despite the seizures, showed pancreatic calculi. These may be com- parable to the cases reported by Edlund et al. s~, in whom recurrence of pancrea- titis could be detected very frequently unless the drinking habit was not abolished even after the course of pancreatitis. However, except these cases, there was none who complained of severe pain, probably because they were spending their daily lives very carefully after the seizures. This is a considerable difference from the cases with chronic ancreatitis associated with pancreatic lithiasis we usually experience; it seems to be considered that clinical pictures of the patients who progressed from acute pancreatitis to chronic one are usually mild.
There were four deaths due to pancreatic cancer within a short period after operation of acute pancreatitis. Sterling 7~ proposed 66 possible factors for in- ducing acute pancreatitis, one of which he claimed to be pancreatic tumor. Howard and Jo rdan 8~ also quoted ampullary carcinoma as one of the factors of the disease. Miller et al. 9~ also reported that 20% of the cases with pancreatic cancer were associated with pancreatitis. Hence, attention should be paid to the likelihood that pancreatic cancer may be masked and overlooked by the clini- cal feature of acute pancreatitis and by the finding of the pancreas upon laparo- tomy.
R e f e r e n c e s
1) Committee of Japan Diabetes Society: Diagnostic criteria for diabetes mellitus by glucose tolerance test. J. Japan Diabetes Society, 13:1, 1970.
2) Dreiling, D.A. & Janowitz, H.D.: The measurement of pancreatic secretory function. Ciba foundation symposium on the exocrine pancreas, normal and abnormal functions. J. and A. Churchill Ltd., London, 1962.
3) Sebening, W.: Folgezustande nach akuter Pankreasnekrose. Med. Klin., 23:551, 1927. 4) Trapnell, J.E.: The natural history and prognosis of acute pancreatitis, Hunterian Lecture,
Royal College of Surgeons. Ann. Roy. Coll. Surg., 38:265, 1966.

The Fate of the Patients Surviving Acute Pancreatitis 351
5) Edlund, Y., Norback, B. & Risholm, L.: Acute pancreatitis, etiology and prevention of re- currence. Follow-up study of 118 patients. Rev. Surg. (Phila.), 25:153, 1968.
6) Maki, T., Sato, T., Saitoh, Y. & Koyama, K.: Clinical study of pancreatic cyst, with special reference to its pathogenesis. Geka (Jap.), 28:112, 1966.
7) Sterling, J.A. : The biliary tract. William & Wilkins Co., Baltimore, 1955. 8) Howard, J.M. & Jordan, G.L.: Surgical diseases of the pancreas. J.B. Lipponcott, Co.,
Philadelphia, 1960. 9) Miller, J.R., Baggenstoss, A. & Comfort, M.W. : Carcinoma of the pancreas, effect of histolo-
gical type and grade of malignancy on its behavior. Cancer, 4:233, 1951.
Received 13th July 1973 Accepted 23rd July 1973