Embed Size (px)
Citation preview

The Evolution of Innovation

Current Status
Welcome The Innovations Exchange helps you solve problems, improve health care quality, and reduce disparities.Find evidence-based innovations and Quality Tools. View new innovations and tools published biweekly. Learn from experts through events and articles.
Read about our Experts.

Past and Current Status: Ahead of the Curve
INNOVATION Aqui Para Ti HCMC
Family and Patient Centeredness
2001 2010
Health Care Home 2007 (before MN adopted the model)
2010
Health Care Neighborhood
2010 ……
Working on Social Determinants of Health
2001- 2010 2o10
EHR as a patient Centered Tool for teens
2008 ……..

Family and Patient Centeredness:2001-current
Funded by MDH through EHDIEliminating
Health Disparities Initiatives
Designed as Family and Patient Center approach for Latino
Youth and their families
Parallel Family Care
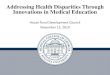
Figure 1: APT Conceptual Model
Improved Family Functioning
Connection Expectations Participation Communication
Youth Assets Pos. ethnic identity Empathy Problem solving Self-awareness Goal orientation School orientation
Parents Parenting self-efficacy
Parenting Knowledge/skills Monitoring Discipline
Cognitive Participation
Youth/Family Connection to
Resources
Coaching modules Case Management
Youth Knowledge and
skills
Maintenance of Positive Youth
Behavior or Decreased Risk:
Depression Substance use Sexual
behaviors School
engagement
Cultural literacy/ Youth friendliness /Parallel family care
Collective Action
Cultural literacy/ Youth friendliness /Parallel family care Coherence
Reflexive Monitoring
Patient – provider factors
Youth Behavioral self-efficacy
Emotional self-regulation

Core intervention components
1) Presence of a trained adolescent care team (provider, health educator, care manager).
2) Family parallel care (needs of both parents and youth are addressed in a parallel fashion).
3) Structured approach to screening, utilizing nationally established clinical practice guidelines.
4) Case management.5) Delivery of coaching modules.

The team (from left to right)
Monica Hurtado Program Developer
Laura Trebs Community Health worker
Dora Palma Family Case Manager
Amelia Yaurincela Community Health Worker
In the picture:Bibiana Garzon , our late Program Coordinator
Veronica Svetaz Medical Director/Provider
Ursula Reynoso Program Coordinator
Maria Isabel Graybow College Connector

Our Dedicated Staff:
Is bicultural and bilingual in English and Spanish.Collaborates with other community organizations
and sustains long-term partnerships.Has experience and interest in working and serving
young Latino immigrants in Minnesota. Has successfully secured a diverse funding
structure to ensure the continuity of our program.Is compassionate and understanding of the needs
and assets of the Latino community.

IN PROGRAMDEVELOPMENT:
Managing budgets
Managing reports
Writing grants
Doing presentations
Teaching medical workforce and the giving back to the community
Doing advocacy in Health Disparities, etc
Working in system change, etc
1) Program Coordinator
2) Program Developer
TEENSBoys/girls11-24 yo
PARENTS
CommunityHealth Workers (2)Main Tasks:EDUCATECOORDINATE
FamilyEducator (1)Main tasks: EDUCATECOORDINATEHOME VISITS
Parallel Family Care
Physician
College Connector (1)
IN ACTION IN THE CLINIC
TEEN ADVISORY BOARD
PARENT ADVISORY BOARD
WEEKLY Case Management (all the team plus residents plus medical students)

TEENSBoys/girls11-24 yo
PARENTS
Care Coordinators(2)Main Tasks:EDUCATECOORDINATE
FamilyEducator (1)Main tasks: EDUCATECOORDINATEHOME VISITS
Parallel Family Care
Physician
College Connector (1)
IN ACTION IN THE CLINIC
TEEN ADVISORY BOARD PARENT ADVISORY BOARD
WEEKLY Case
Management (all the
team plus residents
plus medical
students)

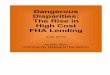
Health Care Home 2007current: AROUND 230 pts. enrolled
Around 2006 the team noted a change in our population (those patients that we were receiving).
We had become a Referral Center.
On a EHDI presentation on 2007, we concluded that we have become a Health Care Home, due to the type of complex patients followed and the system of care we used.
0%
10%
20%
30%
40%
50%
60%
70%
80%
2002 2003 2004 2005 2006 2007
Low
Medium
High
APT Patients’ Risk/Needs Level:From Prevention to Crisis Intervention

APT-HCMC HCH as a State Model

APT-HCMC HCH as a National Model

National Model Adolescent Care Program

The National Endorsement

The National Webinar
Aqui Para Ti/ Here for you was showcased as an example of Cultural Inclusivity in second National Webinar of the new Educational initiative launched by the Society of Adolescent Health and Medicine (SAHM).

SAHM Webinar Cultural Inclusivity:
The Practice
MARIA VERONICA SVETAZ MD, MPH

APT’s awards and recognitions
The U.S. Agency for Healthcare Research and Quality's Health Care Innovations Exchange Program identified APT as an innovative approach to accelerate the development and adoption of innovations in health care delivery, with special emphasis on reducing disparities among racial, ethnic, and socioeconomic groups.
The National Alliance to Advance Adolescent Care has highlighted APT as a model program for teens and is featured on its website (http://thenationalalliance.org/programs/program.cfm?programID=3).
APT received the Partners in Prevention Award in 2003 from the Centers for Disease Control and Prevention (CDC) National Teen Pregnancy Prevention Research Center at the University of Minnesota.
Teenwise Minnesota (formerly the Minnesota Organization on Adolescent Pregnancy, Prevention and Parenting, or MOAPPP) presented APT with the Community Partner of the Year Award in 2009 for contributing to public understanding and dialogue of adolescent sexual health, pregnancy prevention and parent support.
Leading Light Award 2010, together with “People Magazine”, per the National Multicultural Institute, in Washington D.C.

Community Clinic Integration.Health Care Neighborhood.2010-current
Centro is more than a multi-social service agency...
Centro is a partnership with Latino and Chicano families. Centro is a place where we offer respite from troubles, understanding to solve crises, education and encouragement to make change, nurturing and healing to strengthen families, art and culture to reaffirm our identity and value, and resources to build a better future.

Community Clinic Integration

Our Neighborhood
Centro – Centro is a social services agency, serving Latino families. Centro and APT collaborate on multiple projects seeking to integrate clinical and community services.
La Conexion de las Americas – La Conexion joined APT and Centro to integrate clinical and community services, using leadership and community ownership to improve the physical, emotional, and social health of Latino youth (This collaboration ended in May 2012, given that this agency closed it services).
Family Partnership, Inc. – Family Partnership joined APT and Centro to integrate clinical and community services, using leadership and community ownership to improve the physical, emotional, and social health of Latino youth.
NAVIGATE. A volunteer organization was created to address the growing need for resources that help immigrant students in Minnesota to pursue higher education, regardless of immigration status. APT has been working with Navigate to connect APT patients and their families with higher education and to better understand the U.S. education system.
Hennepin East Lake Clinic (HCE) – Hennepin East Lake Clinic and Family Medical Center have been implementing the model of Centering Pregnancy and Parenting. APT staff has been instrumental in developing this project, which entails offering health assessment, education, and support within a group setting.
Minnesota Visiting Nurse Agency (MVNA) – MVNA has been a partner to APT for five years providing home visits to APT pregnant teens and teens with new babies, as well as providing education on healthy pregnancy, breastfeeding, practical tips on baby care, and parenting tips.
El Colegio: El Colegio Charter School is a small public high school in Minneapolis that has been serving students in English and Spanish since 2000. Its mission is to graduate creative, culturally-grounded students who excel in bilingual and bicultural environments, prepare them for college, employment and community leadership.
Hiawatha Academies is a network of high-performing college preparatory charter schools located in South Minneapolis. Our mission is to empower all Hiawatha scholars with the knowledge, character and leadership skills to graduate from college and serve the common good.

Those who support us in Our Neighborhood
University of Minnesota Program in Health Disparities Research – Since 2007, this department and APT had been developing a culturally-appropriate curriculum for Latino parents of adolescents under the community based participatory research framework.
University of Minnesota Extension –This department has advised APT in its evaluation efforts and partnered with APT and others for the development of a curriculum for Latino Parents.
Prevention Research Center, PRC, of the Pediatrics and Adolescent Health Division of University of Minnesota. Since 2008, APT staff has been part of Encuentro, a Community Based Participatory Research project lead by the PRC to explore the meaning and consequences of teen pregnancy in the Latino community
Alliance for Racial and Cultural Health Equity (ARCHe) – In 2009, APT was one of 67 community organizations interviewed by the Center for Cross Cultural Health (CCCH) to explore and better understand the situation of health disparities in Minnesota.
HCMC Volunteer Services – APT, in collaboration with HCMC Volunteer Services, continues to provide valuable experience to volunteers from different colleges and academic programs who are interested in learning about the APT program, the Latino culture and practicing Spanish.

Social Determinants of Health as a major reason not to be healthy2001- currently
Working on Social Determinants of Health from a clinic based program, by identifying leverage points.
Leverage points:Health and Education inequities coexist in the same population
They need to be addressed together.
APT, through a very competitive family planning grant from City of MPLS, in 2011 hired a college connector, now
sustained by our EHDI grant

2012 CHIP Forum: Working with Leverage Points
Local community Health systems
(from our 2012-2013 Health Services Plan)

Teen Centered EMR APT: Henne-Teen 2008 (piloting at East)
Improving Electronic Medical Records (EMR) so that they are a tool for truly patient centered care
EMR-Confidentiality and Teens

Henne-Teen

Outcomes
The IHI Triple Aim is a framework developed by the Institute for Healthcare Improvement that describes an approach to optimizing health system performance.
It is IHI’s belief that new designs must be developed to simultaneously pursue three dimensions, which we call the “Triple Aim”:
• Improving the patient experience of care (including quality and satisfaction);
•Improving the health of populations; and•Reducing the per capita cost of health care.

The Tripe Aim: Improve Health
AHRQ report (charts in this and several other slides about this)
APT flyerBrown Bag Presentation
1. Sexual Health2. Mental Health: both teens and parents3. Overall Health

Table 4. Birth Control Types Classes (n=141) n=(%)
Before Health Educator After Health Educator
High Efficiency Birth Control 10 (7) 70 (50)Low Efficiency Birth Control 31 (22) 19 (13)No Birth Control 66 (47) 19 (13)Abstinent/Not active/Pregnant
34 (21) 30 (21)
Table 4. Birth control shift. Divideds BCM into high and low efficiency and describes patient trends between BCM classes. Indicates 7% of patients used a High-Efficiency BCM upon arrival, and 50% of patients shifted to a High-Efficiency BCM after discussing with Health Educator.
Table 5. Pregnancy Prevention At Risk Secondary Pregnancy Total in Group Predicted
Pregnancies Total at risk (Without APT) 70 15 With APT (n=70) No birth control 11 2 Low efficiency BCM 9 1 High Efficiency BCM 50 0Total Predicted with APT 3
At Risk Primary Pregnancy Total at risk (Without APT) 67* 7With APT (n=67) No birth control 8 1 Low efficiency BCM 11 1 High Efficiency BCM 19 0 Abstinence 29 0Total Predicted With APT 2
Table 5. Pregnancy Prevention. Secondary pregnancy care Table denotes the chosen BCM of teens in 2 separate at risk groups. Demonstrates the APT model effectiveness in preventing pregnancies in Latina teens. Of 137* eligible teens APT reduced the amount of predicted pregnancies from 22 to 5 through placing teens on high and low efficiency BCMs. *4 teens were pregnant at the time of survey and inelegible for data inclusion.
1-Sexual Health

Table 6. Saved Costs to Society through Pregnancy Prevention Prenatal to
Birth CostYear 1 Year 2 Year 3 Year 4 Total
Average Costs $10,682 $5,506 $5,506 $5,506 $5,506 $32,706 Without APT (176 pregnancies)
$1,880,032 $969,056 $969,056 $969,056 $969,056 $5,756,256
With APT (38 pregnancies)
$405,916 $209,228 $209,228 $209,228 $209,228 $1,242,828
Total Savings over 5 years
$4,513,428
Table 6. APT savings over 5 year period. Demonstrates amount of money the APT model saved over a 5 year period of time.
1-Sexual Health

2-Mental Health: Teens
Mental Health – Beck Depression Inventory
Overall, patients exhibited significantly fewer depressive symptoms at their final assessment (M = 11.09), compared to their first assessment (M = 14.07) (paired t-test = 2.20, p = .03).
For those whose depressive symptoms were above the clinical cut-off (higher than 17) (n=20), there was a clinically significant decrease in symptoms over the time period from a mean of 25 to a mean of 15 , that was also statistically significant (p = .003).

2-Mental Health : Parents
Parents’ depressive symptoms were also assessed:78 parents completed one or more Beck Depression
Inventories. At the time of the first assessment, total scores ranged from 0-43 (M = 13.58, SD = 11.50) and 19 parents (24.1%) had depression scores that exceeded the clinical cut-off (>17).
This highlights the appropriateness of the program's model, providing parallel care during adolescents years
to the Latino families is critical.
Parents’ Experiences – Beck Depression Inventory, and Parenting Styles and Efficacy

Findings: Quantitative: Overall Health
Table 2: Youth Self Report of Health Issues Worked on with APT Team
Health Issue
Reporting working on
issue with APT team: n (%)
Those reporting having worked on issue who felt the treatments or
solutions proposed by APT made sense: n (%)
Those reporting having worked on the issue
who felt that the issue has improved since first being seen at APT for
it: n (%)Emotional issues, like feeling upset, depressed, etc. 26 (86.7%) 26 (100%) 24 (92.3%)
Issues related to sexual behaviors, such as pregnancy prevention, sexually transmitted diseases, etc.
26 (86.7%) 25 (96.2%) 22 (84.6%)
Issues related to relationships with your parents and other family members
24 (80%) 23 (95.8%) 18 (75%)

The Tripe Aim: Improve the Patient Experience
An 8-item follow-up survey was conducted to assess the teen-provider trust and delivery of more appropriate service plans:
Nearly all (97%) reported that clinic staff supported them and their needs.
Most (71%) patients reported that it was important to them that APT staff spoke Spanish
Most (71%) reported that it was important to them that APT staff be Latino and a majority (84%) reported that it was important to them that APT take into account their culture, language, and values


Outcomes: Improve Costs
Challenges to measure this: Innovative Parallel Care: both ends of the family Multilevel approach:
screening and intervening: finding the “unmet needs” strengthening and preventing: coaching leveling the strength of the intervention in mental health, physical
health, social health, with emphasis in education, as a leverage point of future health among our population.
coordination of care. system of care.
Proxies: all of our approaches are evidence based nationally embraced Prime Time Patient Delivery care approaches.

Patients served
Over ten years, APT has seen 1,015 patients.
From July 2010 through March 2012, APT had 769 encounters with 266 distinct patients (for an average of 3 visits per patient with a range of 1-25).
Of these, 108 were new to the clinic (70% girls, 30% boys).
We are a referral center for Pregnant Latino Teens, and recently started Centering Pregnancy Teen, for our patients, a conjoined effort among APT, MVNA, HCMC Doulas and Midwifes Delivery Services.

Patients served-IMPROVING ACCESS
Since June 2012: we change our recruitment strategy and increased to three clinics per week.
We started using Advanced Access, reserving some overbook appointments for those patients with urgent needs.
We started recruiting the children of our teen parents , most of them lost to other system of care for lack of access, and increase the number of patients seen per session to an average of 9 visits per day.
Started 24/7 coverage via providers at East Lake Clinic

Patients served
APT/Svetaz/ELC Centering Teen Visit totals by month
(from Mediware) Month Visit Totals New Jun-12 67 7 pts. Jul-12 49 3 pts. Aug-12 85 13 pts. Sep-12 68 15 pts. Oct-12 114 11 pts.
Nov-12 66 9 pts.

Funding: a Hybrid
HCH: sustainable core, certified by MDH.Grants: main (for the past 10 years):
Eliminating Health Disparities Initiative (EHDI)Office of Minority and Multicultural Health(OMMH) Minnesota Department of Health (MDH)
More coming: HHF report

Current State
We are a certified Adolescent Health Care Home at HCMC
We are a Referral Center in the Twin Cities.
We are a “clinic within a clinic”.
We are a pioneer of Family and Patient Care Model (2001).
We are part of a Health Care Neighborhood (2010).
We are a model for Primary Care of Adolescents endorsed by the National Alliance to Advance Adolescent Health (2010-2012).

Current State
We use an innovative approach to improving health care delivery and reducing disparities among racial, ethnic, and socioeconomic groups, as identified by AHRQ (Agency for Healthcare Research and Quality)'s Health Care Innovations Exchange Program.
The Public Health Institute in California recognized APT as one of the 4 HCMC examples of Community Benefit Programs, where these programs provide Emphasis on Disproportionate Unmet Health Needs, Emphasis on Primary Prevention, Building a Seamless Continuum of Care, Building Community Capacity, and Collaborative Governance.

Current State
(from our 2012-2013 Health Services Plan)

In Summary
Our team and program is ready to move to a new level of system change at HCMC, as already is at that level at state and national arena.
We need a firm structure that assure that the clinical model is secure.

System Changes Initiative
Aqui Para Ti launched two HCMC system changes Initiatives: Henne-Teen (already presented)
Center for Health Equity Leadership (CHEL)Aqui Para Ti supports system change Initiatives:
ARCHE (Alliance for Racial and Cultural Health Equity)
Advocacy: members seat in a myriad of Boards.

Healthy Minnesota 2020

Center for Health Equity Leadership (CHEL) Rationale
THE CENTER WILL BE A CONJOINT EFFORT AMONG AQUI PARA TI , THE DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE , AND THE FAMILY MEDICINE RESIDENCY PROGRAM.
THE CENTER, WHICH RESIDES IN THE DEPARTMENT OF FAMILY MEDICINE AT HENNEPIN COUNTY MEDICAL CENTER, HAS AS ITS CORE THE ACHIEVEMENT OF THE AQUI PARA TI (“HERE FOR YOU”) PROGRAM, A MODEL PROGRAM OF INTEGRATIVE CARE THAT HAS BEEN NATIONALLY-RECOGNIZED BY ITS INNOVATION BY AHRQ.

CHEL: Main Mission
Highlights Leadership of:
………….Communities defining their own priorities to achieve health
………………Primary Care as a leverage point for those activities to take place
…………………..Safety Net as the natural trust center where that care is already happening

Where we should be