Embed Size (px)
DESCRIPTION
An antenatal interventionto prevent or reduce maternal distress in pregnancy
Citation preview

ORIGINAL ARTICLE
The effect of Wazzup Mama?! An antenatal interventionto prevent or reduce maternal distress in pregnancy
Yvonne J. Fontein-Kuipers1 & Marlein Ausems1 & Raymond de Vries1,2,3 &
Marianne J. Nieuwenhuijze1
Received: 4 November 2015 /Accepted: 29 February 2016# Springer-Verlag Wien 2016
Abstract We evaluated the effect of the interventionWazzUpMama?! on antenatal maternal distress in a non-randomizedpre-post study including healthy women in 17Dutch midwife-ry practices. The control group (n=215) received antenatalcare-as-usual. The experimental group (n=218) received theintervention. Data were collected at the first and third trimesterof pregnancy. Maternal distress (MD) was measuredwith the Edinburgh Depression Scale (EDS), State-TraitAnxiety Inventory (STAI), and Pregnancy-Related AnxietyQuestionnaire (PRAQ). We used multivariate repeated-measure analysis to examine the across time changes andANCOVA was used to examine the differences between thetwo groups. In the control group, mean EDS, STAI, and MDscores significantly increased from first to third trimester ofpregnancy, mean PRAQ scores increased, but not significant-ly, the proportion of scores above cut-off level of EDS, STAI,and PRAQ significantly increased from first to third trimester,and the proportion ofMD scores above cut-off level increased,but not significantly. Within the experimental group, the meanSTAI, PRAQ, and MD scores significantly decreased fromfirst to third trimester, the EDS mean scores decreased but
not significantly, proportions of scores above cut-off levelfor PRAQ and MD significantly decreased from first to thirdtrimester of pregnancy, the proportions of EDS and STAIscores above cut-off level decreased but not significantly.There was a moderate significant positive effect of WazzUPMama?! on the MD scores (F(1.43) = 27.05, p < 0.001,d=0.5). The results provide support for the effectiveness ofthe intervention WazzUp Mama?!
Keywords Antenatal intervention .Maternal distress .
Depression . Anxiety . Pregnancy-related anxiety
Introduction
Maternal distress refers to different psychological constructsoccurring during pregnancy, most commonly identified as de-pression and anxiety in general or specifically related to preg-nancy that are significantly correlated (Heron et al. 2004;Fontein-Kuipers et al. 2015b). Maternal distress has adversehealth consequences. Maternal distress is associated with ma-ternal short and long-term (chronic) postnatal mental healthproblems, including post partum depression. Maternal distressis also associated with the physical, neurobehavioral, and cog-nitive development of the child (Brouwers et al. 2001; Mulderet al. 2002; Heron et al. 2004; Mennes et al. 2006; Van denBergh et al. 2008; Loomans et al. 2012).
It is difficult to report exact prevalence rates of maternaldistress because it is a compilation of different psycho-logical constructs with no validated psychometric toolfor measurement (Nast et al. 2013). Using a maternaldistress score compiled from different one-dimensional psy-chological constructs, we found a prevalence rate of 22 % in aDutch population of women with healthy pregnancies(Fontein-Kuipers et al. 2015b).
* Yvonne J. [email protected]; [email protected]
1 Midwifery Education & Studies Maastricht-ZUYD, Research Centrefor Midwifery Science, PO Box 1256,6201 Maastricht, The Netherlands
2 Maastricht University Medical Centre/CAPHRI, PO Box 6202AZMaastricht, The Netherlands
3 Center for Bioethics and Social Sciences in Medicine, University ofMichigan Medical School, 300 North Ingalis Street, Rm 7C27, AnnArbor, MI 48109-5429, USA
Arch Womens Ment HealthDOI 10.1007/s00737-016-0614-8

Despite the development of various interventions to reducematernal distress (Matthey et al. 2004; Beddoe and Lee 2008;Cupples et al. 2011; Svensson et al. 2009; Ickovics et al.2011), the weight of current evidence suggests that antenatalprograms have limited success in preventing or reducing ma-ternal distress.
Maternal distress is a complex concept (Fontein-Kuiperset al., submitted) requiring an intervention based on a system-atic and evidence-based understanding of the underlying prob-lem, its context, and the processes used to intervene (MRC2006; Campbell et al. 2007). In the Netherlands, there is nostandard care-routine for maternal distress (Fontein-Kuiperset al. 2014; Pop et al. 1992). We developed WazzUp Mama?!,an intervention offered during midwife-led care to prevent orreduce maternal distress among healthy pregnant women. Weused Intervention Mapping as the framework for interventiondevelopment and implementation, and drew on theoreticalmodels to identify strategies to address the behavior of boththe women receiving, and themidwives delivering the interven-tion (Bartholomew et al. 2011). The systematic process of theintervention development and production of WazzUp Mama?!has been described elsewhere (Fontein-Kuipers et al. 2015a).
In this paper, we evaluate the effect of the interventionWazzUp Mama?! on antenatal maternal distress by examiningthe changes across time inmaternal distress among healthy preg-nant women who received the antenatal intervention WazzUpMama?! and healthy pregnant women who received antenatalcare-as-usual, and the differences between these groups.
Methods
Design and sample procedure
When we drew the project plan, we considered conducting arandomized trial to test the effect of the intervention. Powercalculation showed that a minimum of 46 midwifery practiceswould be necessary to conduct the study. We decided that iswas more feasible to conduct a non-randomized pre-post in-tervention study with a sequential control and experimentalgroup. Using the design, we needed a more manageable num-ber of midwifery practices, 16, to detect a small effect.
In our study, we included two cohorts of healthy Dutch-speaking women in midwifery-led care. Women with (pre-)existing medical conditions at the point of registration, requir-ing medical and/ or obstetric care were excluded. Pregnantwomen from 17 midwifery practices, situated in theSouthern, Mid-Eastern, and Northern regions of theNetherlands were recruited for the study. Midwifery practiceswere recruited using convenience sampling.
Recruitment of the participants and data collection for thecontrol and experimental group were carried out in two se-quential time periods in the participating practices, between 24
April 2013 and 7 March 2014 for the control group, and be-tween 14 April 2014 and 9 March 2015 for the experimentalgroup (Fig. 1). The control group received antenatal care-as-usual, provided by the midwifery practices. The data for bothcohorts were collected during the first trimester of pregnancy(T1) and during the third trimester (T2). T1 was at 7 (SD±2.2,range 4–14) weeks gestation, before women had their firstphysical appointment (a booking appointment and/ or scan)with their midwife. T2 took place at 37 (SD±1.53, range 35–42) weeks gestation. Each questionnaire was followed up bytwo reminders with 1 week interval for each reminder.
Midwives or practice assistants approached women aboutthe study during women’s registration telephone call. Womenwere verbally informed about the topic of the study and weretold that their involvement would consist of filling out twoquestionnaires at two time points during pregnancy. If womenwere willing to participate, their email addresses wereforwarded to the researcher (Y.F.). Additional informationabout the study and an invitation to participate in the first
Control group
295 invita ons andques onnaires sent (24April to 22 August 2013)
T1 215 completedques onnaires returned
(response 72.8%)
25 pregnany losses
190 ques onnaires sent(20 October 2013 to 7
March 2014)
T2 165 completedques onnaires returned
(response 55.9%).Reasons for a ri on:immature birth (2);
intra uterine death (1);premature birth (3);
maternal illness (8); toobusy (7); no specific
reason (4)
Observed cases, n = 165ITT analysis, n = 215
Experimental group
272 invita ons andques onnaires sent (14April to 22 August 2014 )
T1 218 completedques onnaires returned
(response 80.1%)
32 pregnancy losses
186 ques onnaires sent(17 October 2014 to 9
March 2015)
T2 178 completedques onnaires returned(65.4%). Reasons for
a ri on: immature birth(1); premature birth (1);transfer to other prac cenot par cipa ng in thestudy (3); incorrectemailaddress (1): nospecific reason (2)
Observed cases, n = 178ITT analysis, n = 218
Fig. 1 Flowchart study population
Y.J. Fontein-Kuipers et al.

questionnaire were then digitally distributed to the women.Participants digitally consented to participate before they wereable to fill out the first questionnaire. The researcherapproached midwifery practices, either midwives or practiceassistants, prior to sending out the second questionnaires toinquire about women who had experienced pregnancy losses.Those women were not approached for the second question-naire (n=26 in control group; n=32 in experimental group).Women who did not respond to the second questionnaire wereapproached by email to ask their reason for non-responding.
Ethical approval was obtained by the Medical EthicalCommittee Atrium-Orbis Medical Centre Zuyd (registrationno. 13-N-45 (11-N-101)/11-4-2013). The study was registeredwith the Dutch Trial Registration (TC 4688).
WazzUp Mama?!
The program has two parts: one for pregnant women and onefor midwives. The program part for women aims to identifythe vulnerability of, or the presence and severity of maternaldistress during pregnancy. When maternal distress is absent orvulnerability is identified, the program is designed to preventit from developing. When maternal distress is present, theprogram aims to reduce it. The program included a web-based tailored program, consisting of (i) a homepage, (ii) aprocess for collecting personal information including firstname, residence, midwifery practice, and results of screeningtests addressing personal circumstances and history, emotionalwell-being, emotional stamina or perceived burden, maternaldistress and coping mechanisms, and (iii) personalized feed-back based on the data collection in (ii). The screening testsused three self-directed pathways. The first pathway focusedon the signs and symptoms of maternal distress and the iden-tification of whether the respondent’s mood state belongs tothe physiological process of pregnancy or deviates from thatprocess. The second pathway focused on identifying(potential) stress factors, problems or difficult situations inthe past or present that may lead to, or contribute to, the de-velopment of maternal distress. The third pathway focused onthe measurement of maternal distress, operationalized usingthe Edinburgh Depression Scale. Scores above defined cut-offpoints identified the level of severity of maternal distress andthe consequent advice on self-management and support.When women identified stress factors or the presence of prob-lems or difficulties, they were asked to score their perceivedburden or emotional stamina on a scale from 0 to 10. Cut-offpoints indicated women’s need for self-management or foradditional (professional) support.
The personalized feedback from the screening tests included(i) advice for everyday life in order to provide respondents witha variety of practical tools to choose from, including relaxation,(ii) advice about positive ways of coping and offering alterna-tive approaches to effective coping, and (iii) resources for self-
management, and information about local lay workers, supportgroups and individual regular and alternative (local) healthcarefor psychological help and support. Finally, a synopsis of all theadvice given was presented to the woman, who was encour-aged to print it out and discuss it with her midwife.
The program part for midwives provided a format to sup-port pregnant women’s self-disclosure and self-managementwith regard to maternal distress and for the implementationand coordination of care for maternal distress. The programincluded an educational part and a toolkit. The toolkitcontained (i) a guideline including a clinical pathway for con-sultation and referral, (ii) a regional healthcare map includingall relevant caregivers aiming at emotional well-being in themidwives’ local area of practice, (iii) a format for teammeetings/client discussion, consultation, and referral. Theguideline used case-finding questions consistently askedthroughout antenatal care and the clinical pathways used thescoring system of perceived burden or emotional stamina withthe same cut-off points as the web-based program for women.Midwives were trained how to use the tools. Development andimplementation of the program is described extensively else-where (Fontein-Kuipers et al 2015a).
Measures
Our data were collected using a self-reported questionnaire.We collected socio-demographic information and personal de-tails and we used Dutch versions of the Edinburgh DepressionScale (EDS) (Pop et al. 1992), State-Trait Anxiety Inventory(STAI) (van der Ploeg et al. 1980), and the Pregnancy RelatedAnxiety Questionnaire (PRAQ) (van der Ploeg et al. 1980). Toour knowledge, there is no existing psychometric measure-ment tool to measure maternal distress as a multidimensionalconcept of different pregnancy specific mood states and moodstates that are not pregnancy or birth-related (Nast et al. 2013).Therefore, we chose to simultaneously measure depression,anxiety, and pregnancy-related anxiety as we did in a previousstudy (Fontein-Kuipers et al. 2015b).
Edinburgh Depression Scale (EDS)
We used the EDS, a 10-item questionnaire developed toscreen for the likelihood of antenatal depression (Murrayand Cox 1990). Cronbach’s alphas at T1 in the control andexperimental group were α 0.83, 0.84 and at T2 α 0.94, 0.88.The EDS shows high reliability and validity in pregnant pop-ulations (Nast et al. 2013). Responses are scored 0, 1, 2, or 3 inseriousness of symptoms. The total score ranges from 0 to 30.In this study, we used a cut-off score of 11 or more for womenin the first trimester and 10 or more for women in the secondand third trimester to measure depression. These cut-off scoresappear adequate and balance sensitivity, specificity, and posi-tive predictive value per trimester (Bergink et al. 2011).
Antenatal intervention to prevent or reduce maternal distress

State-Trait Anxiety Inventory (STAI)
To identify feelings of anxiety we employed the Trait scale ofthe STAI (Spielberger et al. 1970). Trait anxiety is viewed asanxiety proneness, a relatively stable personality characteris-tic. The Trait scale shows high concurrent validity in the preg-nant validation sample (Nast et al. 2013). Cronbach’s alphas atT1 in the control and experimental group were α 0.93, 0.92and at T2 α 0.96, 0.98. The Trait scale contains 20 items anduses a 4-point rating scale to measure anxiety (1 ‘not at all’; 4‘very’). Scores vary between 20 and 80.Womenwith scores of41 and higher are perceived to have high levels of anxiety.This cut-off point has been validated in pregnant Dutch wom-en (van der Ploeg et al. 1980).
Pregnancy-Related Anxiety Questionnaire (PRAQ)
We measured pregnancy-related anxiety with the 10-itemPRAQ (Van den Bergh 1990). Cronbach’s alphas at T1 inthe control and experimental group were α 0.82, 0.85 and atT2 α 0.88 for both groups. The questionnaire consists of threesubscales measuring: fear of giving birth, fear of bearing aphysically or mentally handicapped child, and concern aboutown appearance. The PRAQ uses a 5-point rating scale tomeasure fear and worries (1 ‘not at all’; 5 ‘very’). Scores varybetween 10 and 50. Based on an earlier Dutch study(Loomans et al. 2012), we used the 90th percentile of the T1PRAQ total scores to identify women scoring high onpregnancy-related anxiety at T1 and T2. The PRAQ scoreshave shown predictive validity (Huizink et al. 2004).
Maternal Distress (MD)
Compiling scores of different constructs measured at the sametime provides a more complete and clear picture of maternaldistress and provides more stable data (Lynn et al. 2011). Wechose to define the measure of maternal distress (MD) as thesum of the different individual measures of the EDS, STAI, andPRAQ. When participants scored above the cut-off level onone or more of the respective individual measures, participantswere rated as having heightened levels of maternal distress.
Data analysis
Power calculation was based on a 1:1 ratio between control andexperimental group, a hypothesized 10 % decrease of height-ened scores of maternal distress, 80 % power, and α level of<0.05. To achieve this, 149 women were required in each arm.Data from all participants were evaluated for completeness.Normality of distribution was visually interpreted with thegraphical tests—histograms and Q–Q plots—and deemed tobe satisfactory. Mean sum scores were calculated for depres-sion (EDS), anxiety (STAI), pregnancy-related anxiety
(PRAQ), and maternal distress (MD). To justify our multidi-mensional approach, we measured the degree of relationshipbetween the EDS, STAI, and PRAQ scores with Pearson’scorrelation coefficient (one-tailed), which showed significantmoderate to very strong positive correlations (Table 1). Wecalculated descriptive statistics for the socio-demographic fac-tors and personal characteristics. We compared socio-demo-graphic, personal characteristics, and the baseline maternal dis-tress scores between the two groups, using chi-square tests andanalysis of variance. We conducted logistic regression to eval-uate the factors that are related to responding and non-responding participants in both groups. We used the observeddata for the comparison of baseline characteristics and for com-parison of responders and non-responders.
To handle the at random missing values in the responseprocess of our study, we imputed missing values using max-imum likelihood methods (expectation maximization) (Field2009). In addition, we performed a multivariate repeated-measures design to examine the within-group changes of ma-ternal distress among pregnant women who received antenatalcare-as-usual (control group) and women who received theinterventionWazzUp Mama?! (experimental group). The con-junction of these methods is fully consistent with intention-to-treat (ITT) (Molenberghs et al. 2004).
Our effect analyses focused on the within-group andbetween-group differences ofMD scores in change from base-line (T1) to post-intervention (T2), to describe and comparethe change of direction in both groups and to assess thebetween-group difference. We examined the within-groupchanges by comparing baseline (T1) and post-test (T2) meansfor EDS, STAI, PRAQ, andMD scores within both the controland experimental group with multivariate repeated-measureanalysis. We compared the proportion of women with scoresabove the cut-off levels of the respective measures using chi-square tests (Field 2009) in both the control and experimentalgroup at T1 and T2.
To select the dependent variable to determine the effect ofthe intervention without losing statistical power, we checkedthe assumptions for multicollinearity with Pearson’s correla-tion coefficient (two-tailed) between MD and EDS, STAI, andPRAQ (Field 2009). As expected, there were very strong pos-itive Pearson’s correlations between MD and the respectivemeasures depression (r = 0.802, p < 0.001), anxiety(r = 0.925, p < 0.001), and pregnancy-related anxiety(r=0.718, p<0.001). We therefore chose MD as our depen-dent variable and performed analysis of covariance(ANCOVA) to determine the effect of the intervention andsignificance of differences between the control and experi-mental group for the post-test MD scores. We entered thebaseline MD scores and parity, planned pregnancies, life-events 1 year prior to pregnancy, history of miscarriage, in-come, use of medication, and history of psychological/psychiatric problems as covariates to control for initial
Y.J. Fontein-Kuipers et al.

between-group differences. Covariates were chosen based onthe findings of earlier studies (Fontein-Kuipers et al. 2015b;Fontein-Kuipers et al., submitted) and expert judgment. Effectsizes were calculated using Cohen’s d. Avalue of p<0.05 wasconsidered statistically significant. Data entry and analysiswere performed using the Statistical Package for the SocialSciences (SPSS) version 22.0.
Results
Participants
Figure 1 shows the flowchart of the participants in both con-trol and experimental group. Baseline characteristics of theparticipants from both control and experimental group arepresented in Table 2. There were no significant differencesbetween the participants in the control and experimentalgroup. Reasons for non-responses are presented in Fig. 1.Logistic regression was conducted to evaluate which indepen-dent baseline variables were predictors for responding to bothquestionnaires at T1 and T2 (see a in Table 2). Analysisshowed that the having a planned pregnancy significantly pre-dicted responding at T1 and T2. Having an unplanned preg-nancy showed decreased likelihood to responding at T2 (OR0.26, 95 % CI 0.12–0.55, p<0.001).
Changes in maternal distress scores within controland experimental groups
The within-group changes are reported in Table 3. In the con-trol group, the mean EDS, STAI, and MD scores significantlyincreased from baseline (T1) to post-intervention (T2)(p < 0.001, p < 0.001, p< 0.001). Mean PRAQ scores in-creased but did not reach statistical significance (p=0.12).The proportion of EDS, STAI, and PRAQ scores above cut-off level significantly increased from baseline (T1) to post-intervention (T2) (p<0.001, p=0.045, p=0.03). The MDscores above cut-off level increased but not significantly(p= 0.13). There was 5.6 % increase in the proportion ofMD scores above cut-off level from T1 to T2.
In the experimental group, the mean EDS scores decreasedat T2 compared to T1 but did not reach statistical significance(p=0.13). The mean STAI, PRAQ, and MD scores in theexperimental group were significantly lower at T2 compared
to T1 (p= 0.001, p< 0.001, p< 0.001). The proportion ofPRAQ and MD scores above cut-off level were significantlylower at T2 compared to T1 (p=0.002, p=0.009). The EDSand STAI scores above cut-off level decreased, but this did notreach statistical significance (p= 0.4, p= 0.4). There was9.2 % decrease in the proportion of MD scores above cut-offlevel from T1 to T2.
Effect of the intervention WazzUp Mama?!
The proportion ofMD scores above cut-off level in the controlgroup significantly increased with 5.6 % from first to thirdtrimester while these significantly decreased with 9.2 % inthe experimental group. The total difference of the proportionsof scores above cut-off levels between the control and exper-imental group was 13.2 %, taking the difference at baselinebetween the two groups into account.
ANCOVA was conducted to evaluate the effectiveness ofthe intervention WazzUp Mama?! after controlling for base-lineMD scores, parity, planned pregnancies, life-events 1 yearprior to pregnancy, history of miscarriage, income, use ofmedication, and history of psychological/psychiatric prob-lems. There were no covariate outliers and relationships be-tween maternal distress and the respective covariates werelinear, increasing explanatory power of the model (Field2009). Significant between-groupMD changes were observedbetween the control and the experimental group. There was amoderate significant main effect of WazzUP Mama?! on theMD scores (F(1.43)=27.05, p<0.001, d=0.5). The covari-ates showed no impact on the post-test MD scores. There wasno interaction between MD and the covariates hence the as-sumption of homogeneity of regression slopes was not violat-ed, which means that the model was accurate (Field 2009).
Discussion
Main findings
We evaluated the effect of the intervention WazzUp Mama?!on antenatal maternal distress by examining the changes inmaternal distress among pregnant women after receiving theantenatal intervention WazzUp Mama?! compared to womenreceiving antenatal care-as-usual. Levels of maternal distressof the participants in the control group significantly increased
Table 1 Pearson’s correlationcoefficient (one-tailed) for EDS,STAI, and PRAQ scores
EDS and STAI EDS and PRAQ STAI and PRAQ
Control T1 r= 0.75 p =<0.001 r= 0.32 p=<0.001 r= 0.36 p=<0.001
Control T2 r= 0.89 p =<0.001 r= 0.65 p=<0.001 r= 0.68 p=<0.001
Experimental T1 r= 0.79 p =<0.001 r= 0.42 p=<0.001 r= 0.49 p=<0.001
Experimental T2 r= 0.86 p =<0.001 r= 0.6 p=<0.001 r= 0.66 p=<0.001
Antenatal intervention to prevent or reduce maternal distress
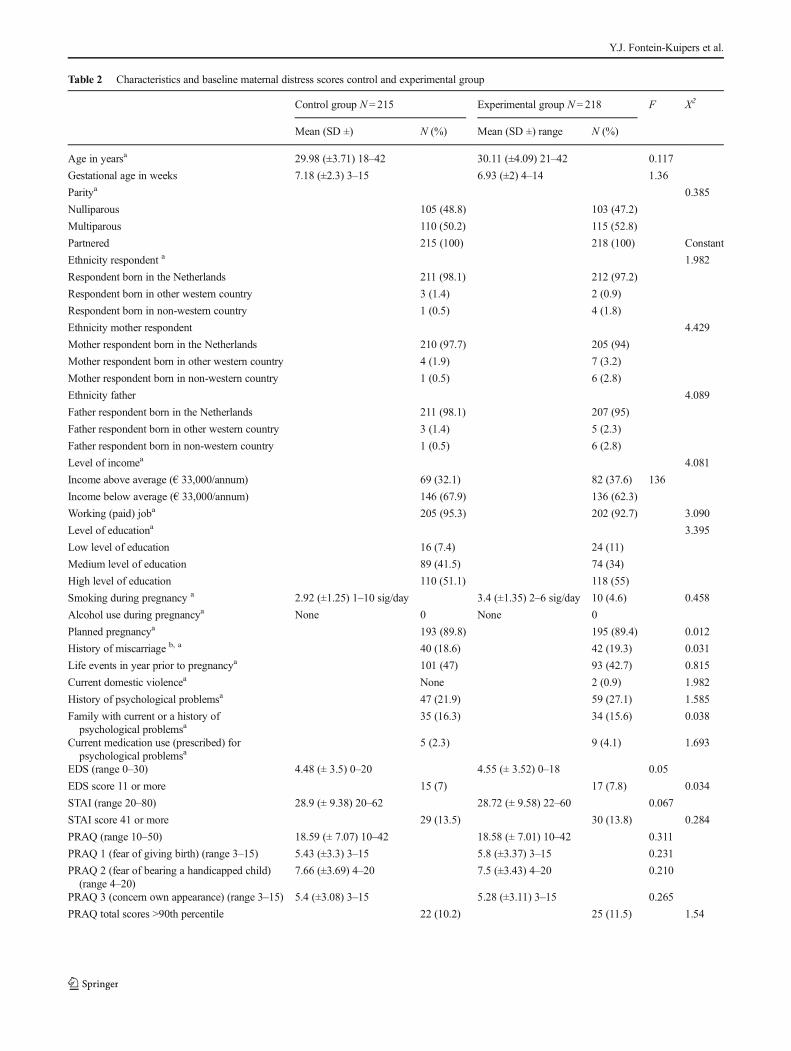
Table 2 Characteristics and baseline maternal distress scores control and experimental group
Control group N= 215 Experimental group N= 218 F X2
Mean (SD ±) N (%) Mean (SD ±) range N (%)
Age in yearsa 29.98 (±3.71) 18–42 30.11 (±4.09) 21–42 0.117
Gestational age in weeks 7.18 (±2.3) 3–15 6.93 (±2) 4–14 1.36
Paritya 0.385
Nulliparous 105 (48.8) 103 (47.2)
Multiparous 110 (50.2) 115 (52.8)
Partnered 215 (100) 218 (100) Constant
Ethnicity respondent a 1.982
Respondent born in the Netherlands 211 (98.1) 212 (97.2)
Respondent born in other western country 3 (1.4) 2 (0.9)
Respondent born in non-western country 1 (0.5) 4 (1.8)
Ethnicity mother respondent 4.429
Mother respondent born in the Netherlands 210 (97.7) 205 (94)
Mother respondent born in other western country 4 (1.9) 7 (3.2)
Mother respondent born in non-western country 1 (0.5) 6 (2.8)
Ethnicity father 4.089
Father respondent born in the Netherlands 211 (98.1) 207 (95)
Father respondent born in other western country 3 (1.4) 5 (2.3)
Father respondent born in non-western country 1 (0.5) 6 (2.8)
Level of incomea 4.081
Income above average (€ 33,000/annum) 69 (32.1) 82 (37.6) 136
Income below average (€ 33,000/annum) 146 (67.9) 136 (62.3)
Working (paid) joba 205 (95.3) 202 (92.7) 3.090
Level of educationa 3.395
Low level of education 16 (7.4) 24 (11)
Medium level of education 89 (41.5) 74 (34)
High level of education 110 (51.1) 118 (55)
Smoking during pregnancy a 2.92 (±1.25) 1–10 sig/day 3.4 (±1.35) 2–6 sig/day 10 (4.6) 0.458
Alcohol use during pregnancya None 0 None 0
Planned pregnancya 193 (89.8) 195 (89.4) 0.012
History of miscarriage b, a 40 (18.6) 42 (19.3) 0.031
Life events in year prior to pregnancya 101 (47) 93 (42.7) 0.815
Current domestic violencea None 2 (0.9) 1.982
History of psychological problemsa 47 (21.9) 59 (27.1) 1.585
Family with current or a history ofpsychological problemsa
35 (16.3) 34 (15.6) 0.038
Current medication use (prescribed) forpsychological problemsa
5 (2.3) 9 (4.1) 1.693
EDS (range 0–30) 4.48 (± 3.5) 0–20 4.55 (± 3.52) 0–18 0.05
EDS score 11 or more 15 (7) 17 (7.8) 0.034
STAI (range 20–80) 28.9 (± 9.38) 20–62 28.72 (± 9.58) 22–60 0.067
STAI score 41 or more 29 (13.5) 30 (13.8) 0.284
PRAQ (range 10–50) 18.59 (± 7.07) 10–42 18.58 (± 7.01) 10–42 0.311
PRAQ 1 (fear of giving birth) (range 3–15) 5.43 (±3.3) 3–15 5.8 (±3.37) 3–15 0.231
PRAQ 2 (fear of bearing a handicapped child)(range 4–20)
7.66 (±3.69) 4–20 7.5 (±3.43) 4–20 0.210
PRAQ 3 (concern own appearance) (range 3–15) 5.4 (±3.08) 3–15 5.28 (±3.11) 3–15 0.265
PRAQ total scores >90th percentile 22 (10.2) 25 (11.5) 1.54
Y.J. Fontein-Kuipers et al.

from first trimester to the third trimester of pregnancy. Thiswas in contrast with the decrease in maternal distress scoresfrom first to third trimester for women in the experimentalgroup. We reached the hypothesized 10 % decrease of
heightened levels of maternal distress after receiving the inter-vention. Receiving the intervention had a significant moderatepositive effect on maternal distress when compared to thosenot receiving the intervention.
Table 2 (continued)
Control group N= 215 Experimental group N= 218 F X2
Mean (SD ±) N (%) Mean (SD ±) range N (%)
MDa 17.32 (±6.65) 0–62 17.28 (±6.64) 0–60 0.001
Heightened levels of MDc 45 (20.9) 49 (22.5) 0.477
a Entered in logistic regressionb Previous miscarriage, ectopic pregnancy, surgical/pharmaceutical abortionc Heightened scores on one of more levels of EDS ≥11, STAI ≥41 and/or PRAQ >90th percentile
Table 3 Changes within experimental and control group from first trimester (T1) to third trimester (T2)
Measure Control group (n = 215) F (4.21) X2 pT1 (baseline) T2 (post)
Mean SD (±) N (%) Mean SD (±) N (%)
Depression (EDS) (0–30) 4.48 ± 3.5, 0–20 7.21 ± 4.69, 1–26 70.23 <0.001
Above cut-off level EDS 15 (7) 42 (19.5) 14.74 <0.001
Anxiety (STAI) (20–80) 28.9 ± 9.38, 20–62 31.6 ± 10.17, 20–72 16.6 <0.001
Above cut-off level STAI 29 (13.5) 43 (20) 3.27 0.045
Pregnancy-related anxiety (PRAQ) (10–50) 18.59 ± 7.07, 10–42 19.43 ± 7.17, 10–42 1.47 0.12
PRAQ 1 (3–15)a 5.43 ± 3.3, 3–15 6.1 ± 2.67, 3–14
PRAQ 2 (4–20)a 7.66 ± 3.69, 4–20 7.68 ± 3.54, 3–18
PRAQ3 (3–15)a 5.4 ± 3.08, 3–15 5.65 ± 2.85, 3–15
Above cut-off level PRAQ 22 (10.2) 37 (17.2) 4.42 0.03
Maternal Distress (MD) (0–80) 17.32 ± 6.65, 0–62 19.41 ± 7.34, 1–72 11.94 <0.001
Above cut-off level MDb 45 (20.9) 57 (26.5) 1.55 0.13
Experimental group (n= 218) F (4.21) X2 pT1 (baseline) T2 (post)
Mean SD (±), range N (%) Mean SD (±), range N (%)
Depression (EDS) (0–30) 4.55 ± 3.52, 0–18 4 ± 3.4, 0–24 0.13
Above cut-off level EDS 17 (7.8) 14 (6.4) 0.313 0.4
Anxiety (STAI) (20–80) 28.72 ± 9.58, 22–60 26.93 ± 9.85, 20–63 11.1 0.001
Above cut-off level STAI 30 (13.8) 27 (12.4) 0.182 0.4
Pregnancy-related anxiety (PRAQ) (10–50) 18.58 ± 7.01, 10–42 15.04 ± 6.42, 10–41 47.4 <0.001
PRAQ 1 (3–15)a 5.8 ± 3.37, 3–15 4.68 ± 2.83, 3–15
PRAQ 2 (4–20)a 7.5 ± 3.43, 4–20 6.05 ± 3.19, 3–17
PRAQ 3 (3–15)a 5.28 ± 3.11, 3–15 4.31 ± 2.52, 3–15
Above cut-off level PRAQ 25 (11.5) 8 (3.7) 9.48 0.002
Maternal distress (MD) (0–80) 17.28 ± 6.64, 0–60 15.32 ± 6.55, 0–63 28.69 <0.001
Above cut-off level MDb 49 (22.5) 29 (13.3) 6.25 0.009
aNot included in multivariate repeated measure analysisb Heightened scores on one of more levels of EDS ≥11 (T1)/ ≥10 (T2), STAI ≥41 and/or PRAQ >90th percentile
Antenatal intervention to prevent or reduce maternal distress

Strengths and limitations
Our antenatal intervention used the systematic interventionmap-ping approach in its development and implementation, which islikely to have contributed to the effectiveness of WazzUpMama?! (Campbell et al. 2007; Bartholomew et al. 2011). Ourresults are sufficiently promising to warrant a definitive evalua-tion of the effect of the interventionWazzUp Mama?! for futureimplementation on a larger scale (Campbell et al. 2007).
Midwifery practices were recruited by means of conve-nience sampling, which may have led to participating mid-wives having affinity with maternal distress. It is known thatthe more interested midwives are in maternal distress or themore they believe that an intervention will be beneficial, themore they engage with maternal distress (Harris et al. 2006;Fontein-Kuipers et al. 2014), resulting in selection bias.However, midwives participated in both control and experi-mental conditions, diminishing possible selection bias.Women were approached for participation by midwifery prac-tices. It is unknown if midwives and practice assistants con-sciously and selectively approached certain women to partic-ipate creating the possibility of selection bias and threateninginternal validity. Women’s decision to participate could havebeen influenced by self-recognition of maternal distress andconsequently have led to self-selection. Self-selection couldhave led to a higher prevalence of maternal distress.
We have studied the effect of WazzUp Mama?! in an onaverage healthy population of pregnant women receivingmidwife-led care. The results are therefore not generalizableto pregnant women in other clinical settings, as it has beensuggested that high-risk women have other emotional healthneeds (Poel et al. 2009).
We used lower cut-off points for EDS compared to inter-national studies (Matthey et al. 2006). Our cut-off levels werebased on populations with similar culture and ethnic back-ground (Matthey et al. 2006; Bergink et al. 2011) as our studypopulation. This might have led to (over)pathologising mater-nal distress (Matthey 2010). Finally, we lack a standard to testthe validity of the maternal distress measure.
Interpretation
Maternal distress as used in our study is a composite score of theone-dimensional constructs depression, anxiety, and pregnancy-related anxiety. The three components depression, anxiety, andpregnancy-related anxiety have been measured with analogouspsychometric metrics. Interrelations between depression, anxi-ety and pregnancy-related anxiety have been documented(DiPietro et al. 2008; Fontein-Kuipers et al. 2015b). In thisstudy, we measured moderate to very strong positive relation-ships between the scores of the EDS, STAI, and PRAQmetrics,which indicate that the metrics are measuring common aspectsof maternal distress (Crawford and Garthwaite 2002).
The STAI and PRAQ scores in our study showed largerstandard deviations than the EDS scores, which suggests thatthese mean scores are likely to be weighted more in our com-piled score maternal distress (Ackerman and Cianciolo 2000).This could have been adjusted by compositing a unit-weightedscore (Ackerman and Cianciolo 2000). By standardizing themetrics scores would be averaged and would affect the distri-bution of differences of the scores above cut-off levels that weused to assess the presence of heightened levels of maternaldistress (Crawford and Garthwaite 2002; Sauro and Kindlund2005). We also would have lost the meaningfulness of thescores of the different psychometric measures (Wiesen 2006).
The characteristics of our sample are fairly representativefor the average healthy Dutch pregnant population, apart fromlevel of income and ethnicity (PRN 2013; RIVM 2013; CBS2014), thus our findings are generalizable to similar popula-tions of pregnant women. There were no systematic differ-ences between the characteristics of participants of the controland experimental group. Although we did not randomize ourparticipants, the similarities in characteristics indicate that it isunlikely that selection bias has occurred (Harris et al. 2006).We have also run both ANOVA of change and ANCOVAanalyses resulting in consistent findings between both analy-ses, indicating that we have taken appropriate measures toreduce bias (van Breukelen 2006). Non-responders were morelikely to have an unplanned pregnancy. Having a history ofpsychological problems, inadequate finances, and a low levelof education are known reasons that women drop out of stud-ies during pregnancy that focus on affected moods in preg-nancy (Morse and Durkin 2004). This is however not consis-tent with the characteristics of the non-responders in our study.
Recommendations for research
In our study there was no random assignment to the interventionbut we used a pre-test and comparison group. If wider implemen-tation of the intervention is to be considered, it would be advis-able to repeat the study with random assignment of the interven-tion to avoid threats to internal validity, preferably with largersample sizes to take account of extra variability (MRC 2006;Campbell et al. 2007). Future research should also build on ourwork, examining and constructing the measure maternal distress.
It would be of great interest to public health to consider thesustainability of the positive outcomes in the first year afterbirth and thereafter. Long-term follow-up may be needed todetermine whether the changes that occurred during pregnan-cy persist or have post partum effects (Reay et al. 2011).Additionally, a process evaluation will provide valuable infor-mation to understand the causal mechanism of the interven-tion and the contribution of the separate components of theintervention, both of which will optimize the intervention forfuture implementation (Campbell et al. 2007).
Y.J. Fontein-Kuipers et al.

Recommendations for practice
Given the positive effect ofWazzUpMama?!we advise use ofthe intervention in midwifery practice. It is advisable to im-plement the interventions as a whole, containing both the partsfor women and for midwives. Because the interventioncontained several interacting components, it is possiblethat separate components variably contributed to theoverall effect of WazzUp Mama?!. The structure andcontent of the two parts enhance each other and thevarious features of the two program parts are likely tohave an interchangeable intervention effect. Individualwomen might respond or benefit differently to separateintervention parts or components. Because of the tailoring andself-management aspects of the intervention, women are ableto choose what suits them best.
Conclusion
Our non-randomized pre-post intervention study showedthat the intervention WazzUp Mama?! had a significanteffect on maternal distress. In the control group, mea-suring depression, anxiety, and pregnancy-related anxi-ety moved in the negative direction while in the exper-imental group these scores moved in the positive direc-tion. WazzUp Mama?! has a promising effect on maternaldistress when carried out by midwives among healthypregnant women.
Acknowledgments The authors would like to thank all the participat-ing midwives, practice assistants, and women who made this study pos-sible and we would like to thank the Promoting Healthy Pregnancy con-sortium members for their support.
This study is part of the research project ‘Promoting HealthyPregnancy’, funded by the Regional Attention and Action forKnowledge (RAAK PRO, ref. 2–014). RAAK is managed by theFoundation Innovation Alliance (SIA) with funding from the Ministryof Education, Culture and Science (OCW).
Contribution to authorship MN and MA designed the study and YFcollected and analysed the data. YF drafted the first manuscript. All au-thors interpreted the data, contributed to discussion and reviewed oredited the manuscript. All authors take responsibility for the integrity ofthe data and the accuracy of the data analysis. RdV supervised the studyand is the guarantor.
Compliance with ethical standards Ethical approval was obtained bythe Medical Ethical Committee Atrium-Orbis Medical Centre Zuyd (reg-istration no. 13-N-45 (11-N-101)/11-4-2013). The study was registeredwith the Dutch Trial Registration (TC 4688).
Conflict of interest BAll authors declare that: no support from anyorganisation for the submitted work; no financial relationships with anyorganisations that might have an interest in the submitted work in theprevious 3 years, no other relationships or activities that could appear tohave influenced the submitted work.^
References
Ackerman PL, Cianciolo AT (2000) Cognitive, perceptual-speeds, andpsychomotor determinants of individual differences during skill ac-quisition. J Exp Psychol Appl 6(4):259–290
Bartholomew L, Parcel G, Kok G, Gottlieb N, Fernàndez M (2011)Planning health promotion programs. An intervention mapping ap-proach, 3rd edition. Jossey-Bass, San Francisco
Beddoe AE, Lee KA (2008) Mind-body interventions during pregnancy.J Obstetric, Gynecologic Neonatal Nursing 37:165–175
Bergink V, Kooistra M, van den Berg M, Wijnen H, Bunevicius R, vanBaar A et al (2011) Validation of the Edinburgh depression scaleduring gestation. J Psychosom Res 70:385–389
Brouwers E, van Baar A, Pop V (2001) Maternal anxiety during preg-nancy and subsequent infant development. Infant BehavDev 24:95–106
Campbell NC, Murray E, Darbyshire J, Emery J, Farmer A, Griffiths F,Guthrie et al (2007) Designing and evaluating complex interven-tions to improve healthcare. BMJ 334:455–459
CBS. [Average income: households according to diverse characteristics].2014 Available at http://statline.cbs.nl/StatWeb/publication/?DM=SLNL&PA=80048NED&D1=a&D2=a&D3=0&D4=(l-1)-l&VW=T[Accessed April, 2015]
Crawford JR, Garthwaite PH (2002) Investigation of the single case inneuropsychology: confidence limits on the abnormality of testscores and test scores differences. Neuropsychologia 40:1196–1208
CupplesM, Stewart M, Percy A, Hepper P, Murphy C, Halliday H (2011)A RCT of peer-mentoring for first-time mothers in sociallydisadvantaged areas (The MOMENTS-study). Arch Dis Child96:252–258
DiPietro J, Costigan K, Sipsma H (2008) Continuity in self-report mea-sures of maternal anxiety, stress, and depressive symptoms frompregnancy through two years postpartum. J PsychosomaticObstetrics Gynecology 1:1–10
Field A (2009) Discovering statistics using SPSS, 3rd edn. SAGEPublications Ltd, London
Fontein-Kuipers Y, Budé L, Ausems M, de Vries R, Nieuwenhuijze M(2014) Midwives’ behavioural intentions of antenatal managementof maternal distress and factors influencing these intentions: an ex-ploratory survey. Midwifery 30:234–241
Fontein-Kuipers Y, van Limbeek E, Ausems M, de Vries R,Nieuwenhuijze M (2015a) Using Intervention Mapping forSystematic Development of a Midwife-Delivered Intervention forPrevention and Reduction of Maternal Distress during Pregnancy.Int J Womens Health Wellness 1:008
Fontein-Kuipers Y, Ausems M, Budé L, van Limbeek E, de Vries R,Nieuwenhuijze M (2015b) Factors influencing maternal distressamong Dutch women with a healthy pregnancy. Women Birth28(30):e36–e43
Harris A, McGregor J, Perencevich E, Furuno J, Zhu J, Peterson D et al(2006) The use of interpretation of quasi-experimental studies inmedical informatics. J Am Med Inform Assoc 13(1):16–23
Heron J, O’Connor T, Evans J, Golding J, Glover V (2004) The course ofanxiety and depression through pregnancy and the partum in a com-munity sample. J Affect Disord 80:65–73
Huizink AC, Mulder EJ, de Medina PG R, Visser GH, Buitelaar JK(2004) Is pregnancy anxiety a distinctive syndrome? Early HumDev 79:81–91
Ickovics J, Reed E, Magriples U, Westdahk C, Schindler Rising S,Kershaw T (2011) Effects of group prenatal care on psychosocialrisk in pregnancy: results from a randomised controlled trial.Psychol Health 26:235–250
Loomans E, van Dijk A, Vrijkotte T, van Eijsden M, Stronks K, GemkeR, et al. Psychosocial stress during pregnancy is related to adverse
Antenatal intervention to prevent or reduce maternal distress

outcomes: results from a large multi-ethnic community-based birthcohort. The European Journal of Public Health. 2012;1–6
Lynn F, Alderdice F, Crealey G, McElnay J (2011) Associations betweenmaternal characteristics and pregnancy-related stress among low-risk mothers: an observational cross-sectional study. Int J NursStud 48:620–627
Matthey S (2010) Are we overpathologising motherhood? J AffectDisord 120:263–266
Matthey S, Phillips J, White T, Glossop P, Hopper U, Panasetis P et al(2004) Routine psychosocial assessment in the antenatal period:frequency of risk factors and implications for clinical service.Archives Womens Mental Health 7:223–229
Matthey S, Henshaw C, Elliot S, Barnett B (2006) Variability in use ofcut-off scores and formats on the Edinburgh Postnatal DepressionScale—implications for clinical and research practice. ArchivesWomens Mental health 9:309–315
Mennes M, Stiers P, Lagae L, Van den Bergh B (2006) Long-term cog-nitive sequelae of antenatal maternal anxiety: involvement of theorbitofrontal cortex. Neurosci Biobehav Rev 30:1078–1086
Molenberghs G, Thijs H, Jansen I, Beunckens C, Kenward M,Mallinckrodt C et al (2004) Analyzing incomplete longitudinal clin-ical trial data. Biostatics 5(3):445–464
Morse C, Durkin S (2004) ‘Staying the distance’: characteristics of wom-en who do not continue in a longitudinal study of pregnancy-relatedmoods. Psychology, Health Med 9(3):293–305
MRC (2006) A framework for development and evaluation of RCTs forcomplex interventions to improve health. Medical ResearchCouncil, London
Mulder E, Robles deMedina P, Huizink A, Van den Bergh B, Buitelaar J,Visser G (2002) Prenatal maternal stress: effects on pregnancy andthe (unborn) child. Early Human Development 70:3–14
Murray D, Cox J (1990) Screening for depression during pregnancy withthe Edinburgh depression scale (EPDS). J Reproductive InfantPsychology 8:99–107
Nast I, BoltenM,Meinlschmidt G, HelhammerD (2013) How tomeasureprenatal stress? A systematic review of psychometric instruments toassess psychosocial stress during pregnancy. Paediatr PerinatEpidemiol 27:313–322
Poel Y, Swinkels P, de Vries J (2009) Psychological treatment of womenwith psychological complaints after pre-eclampsia. J PsychosomObstet Gynecol 30(10):65–72
Pop V, Komproe I, van Son M (1992) Characteristics of the Edinburghpost-natal depression scale in the Netherlands. J Affect Disord 26:105–110
PRN (2013) The Netherlands perinatal registry trends 1999–2012.Stichting Perinatale Registratie, Utrecht
Reay R, Matthey S, Ellwood D, Scott M (2011) Long-term outcomes ofparticipants in a perinatal depression early detection program. JAffect Disord 129:94–103
RIVM (2013) [Ethnicity: definitions and details] In: VolksgezondheidToekomst Verkenning, Nationaal Kompas Volksgezondheid versie4.14. RIVM, Bilthoven
Sauro J, Kindlund E. A method to standardize usability metrics into asingle score. CHI. 2005;April 2–7:401–409
Spielberger CD, Gorsuch RL, Lushene RE (1970) Manual for the statetrait anxiety inventory. Consulting Psychologists Press, Palo Alto
Svensson J, Barclay L, Cooke M (2009) Randomised-controlled trial oftwo antenatal education programmes. Midwifery 24:114–125
van Breukelen GJP (2006) ANCOVA versus change from baseline hadmore power in randomized studies and more bias in nonrandomizedstudies. J Clin Epidemiol 59:920–925
Van den Bergh B (1990) The influence of maternal emotions duringpregnancy on fetal and neonatal behavior. J Prenatal PerinatalPsychology Health 5:119–130
Van den Bergh B, Calster B, Smits T, Van Huffel S, Lagae, L (2008)Antenatal maternal anxiety is related to HPA-axis dysregulationand self-reported depressive symptoms in adolescence: A prospec-t ive s tudy on the fe ta l o r ig ins of depressed mood.Neuropsychopharmacology 33:536–545
van der Ploeg H, Defares P, Spielberger C (1980) Manual of self-reportedquestionnaire. A Dutch translation of the Spielberger State-TraitAnxiety Inventory. Swets and Zeitlinger BV, Lisse
Wiesen JP. Benefits, drawbacks, and pitfalls of z-score weighting. LasVegas: 30th Annual IPMAAC Conference; 2006
Y.J. Fontein-Kuipers et al.