Embed Size (px)
Citation preview

THE EFFECT OF TREATMENT COUCHES ON DELIVERED DOSE
DURING RADIOTHERAPY TREATMENTS
_______________
A Thesis
Presented to the
Faculty of
San Diego State University
_______________
In Partial Fulfillment
of the Requirements for the Degree
Master of Science
in
Radiological Health Physics
_______________
by
Brittany Elizabeth Cochran
Spring 2012


iii
Copyright © 2012
by
Brittany Elizabeth Cochran
All Rights Reserved

iv
ABSTRACT OF THE THESIS
The Effect of Treatment Couches on Delivered Dose During Radiotherapy Treatments
by Brittany Elizabeth Cochran
Master of Science in Radiological Health Physics San Diego State University, 2012
This study measured the photon beam attenuation characteristics of the Varian
EXACT, Varian IGRT treatment couches and two CIVCO Universal extensions used during external beam radiotherapy; and assessed the accuracy of Varian’s Eclipse treatment planning system in modeling the beam attenuation of each couch. Dose Measurements were taken using a Farmer ion chamber inside a cylindrical acrylic phantom. They were taken for two photon energies (6MV and 15MV), at three different field sizes, for various gantry angles through the couch. The EXACT couch was tested both with the adjustable rails pushed to the outside of the couch, and pushed to the center of the couch. The IGRT couch was divided by thickness into three sections for more accurate representation of attenuation along the length of the couch. Effects on surface dose are measured using a Tissue Maximum Ratio for the Varian EXACT couch, and Percent Depth Dose curves for the Varian IGRT and CIVCO extensions. Both CIVCO extensions were introduced into the Eclipse planning system by tracing the couch structures as in viewed in Ct images. All measurements were modeled in the Eclipse treatment planning system for comparison. Maximum attenuation was measured at 6MV with the smallest field for all couch setups. The EXACT couch produced a maximum attenuation of 19.2% and a surface dose increase of 47% of Dmax through the couch. Maximum attenuation for the IGRT couch and both CIVCO extensions were between 6-8%. Through the couch, the IGRT couch showed a surface dose increase of 29% of Dmax,; the CIVCO extensions produced a surface dose increase of 33% and 7% of Dmax. Maximum difference between measured and planned dose was 7%, for the EXACT couch, 1.9% for the IGRT couch and 2.4% for both CIVCO extensions. These treatment couches were shown to affect delivered and surface dose. Including the couch structure during treatment planning can account for the couch attenuation in most cases, but some attenuation values are underestimated in the planning software. Largest effects are for oblique treatment angles using low energy and small field sizes.

v
TABLE OF CONTENTS
PAGE
ABSTRACT ............................................................................................................................. iv
LIST OF TABLES .................................................................................................................. vii
LIST OF FIGURES ............................................................................................................... viii
CHAPTER
1 TREATMENT OVERVIEW .........................................................................................1
1.1 Basics of Photon Radiotherapy ..........................................................................2
1.2 Treatment Beam Characteristics ........................................................................6
1.3 Dose Distribution ...............................................................................................7
1.4 Current Treatment Modalities ............................................................................9
1.5 Composition and Design of Typical Treatment Couch ...................................10
1.6 Previous Studies Concerning Couch Attenuation ............................................11
2 OVERVIEW OF STUDY ............................................................................................13
2.1 Materials and Methods .....................................................................................14
2.1.1 Direct Attenuation Measurements: General Setup .................................14
2.1.2 Varian EXACT Couch ............................................................................16
2.1.3 Varian IGRT Couch ................................................................................16
2.1.4 CIVCO Couch Extensions ......................................................................16
2.1.5 Tennis Racket Support ............................................................................17
2.1.6 Tissue Maximum Ratio Measurement of EXACT Couch with Rails Out ..........................................................................................................17
2.1.7 Percent Depth Dose Measurements of IGRT and CIVCO couches .............................................................................................................17
2.2 Eclipse Modeling .............................................................................................18
2.3 Error Considerations ........................................................................................19
2.4 Results ..............................................................................................................21
2.4.1 Varian Tennis Racket Insert....................................................................22
2.4.2 Varian EXACT Couch Attenuation ........................................................22
2.4.3 IGRT Couch Attenuation ........................................................................27
vi
2.4.4 CIVCO Couch Attenuation .....................................................................29
3 DISCUSSION ..............................................................................................................33
3.1 Conclusion .......................................................................................................35
REFERENCES ........................................................................................................................36

vii
LIST OF TABLES
PAGE
Table 2.1. Attenuation Measurements for the Varian Tennis Racket, when Beam is Passing Straight Through the Grid Surface .................................................................22
Table 2.2. Attenuation Measurements for 6MV Photon Beam Passing Intersecting the Varian EXACT Couch then the Adjustable Rails are Pushed Under the Center of the Treatment Couch (Rails-In Position) .................................................................23
Table 2.3. Percent Attenuation Measurements for 15MV Photon Beam Passing Intersecting the Varian EXACT Couch when the Adjustable Rails are Pushed Under the Center of the Treatment Couch (Rails-In Position) ....................................24
Table 2.4. Surface Dose Measurements for the Varian EXACT Couch, Taken from the TMR Curve Produced Using the Solid Water Phantom ........................................24
Table 2.5. Attenuation Measurements for a 6MV Photon Beam Passing Intersecting the Varian EXACT Couch when the Adjustable Rails are Pushed Under the Center of the Treatment Couch (Rails-Out Position) ..................................................25
Table 2.6. Attenuation Measurements for a 15MV Photon Beam Passing Intersecting the Varian EXACT Couch when the Adjustable Rails are Pushed Under the Center of the Treatment Couch (Rails-Out Position) ..................................................26
Table 2.7. Attenuation Measurements for a 6MV Photon Beam Passing Intersecting the Varian IGRT Couch for Thickness Divisions ........................................................27
Table 2.8. Attenuation Measurements for a 15MV Photon Beam Passing Intersecting the Varian IGRT Couch for Thickness Divisions ........................................................28

viii
LIST OF FIGURES
PAGE
Figure 1.1. Schematic of a linear accelerator.. ...........................................................................3
Figure 2.1. Gantry Rotation around isocenter. .........................................................................14
Figure 2.2. Experimental set-up for direct attenuation measurements. ...................................15
Figure 2.3. Measurement set-up for TMR measurement on EXACT couch. ..........................18
Figure 2.4. (a) CT scan slice of the CIVCO Universal couch extension, (b) Contour traced couch structures from CT scan slice, (c) Resultant couch structure set produced in the Eclipse treatment planning system, after couch contouring and Hounsfield unit assignment of each couch structure. ..................................................20
Figure 2.5. Attenuation measurements for a 10x10cm2 field, 6MV beam passing through the Varian EXACT couch with the adjustable rails pushed to the center of the couch. ......................................................................................................23
Figure 2.6. Attenuation measurements for a 10x10cm2 field, 6MV beam passing through the Varian EXACT couch with the adjustable rails pushed to the sides of the couch. .................................................................................................................25
Figure 2.7. Tissue maximum ratio curve produced for the Varian EXACT couch using a 6MV, 10x10cm2 treatment beam. ....................................................................26
Figure 2.8. Measured Attenuation values for the thickest section of the Varian IGRT couch for a 6MV treatment beam, using a 10x10cm2 field size. .................................28
Figure 2.9. Percent depth dose measurements for a 6MV beam, 10x10cm2 field, using the thickest section of the Varian IGRT couch. ...........................................................29
Figure 2.10. Attenuation measurements for the CIVCO universal extension using a 6MV treatment beam, with a 10x10cm2 field size. ......................................................30
Figure 2.11. Attenuation measurements for the CIVCO sample extension using a 6MV treatment beam, with a 10x10cm2 field size. ......................................................31
Figure 2.12. Comparison for attenuation measurements between the CIVCO universal and CIVCO sample extensions for a 6MV beam, 10x10cm2 field. .............................31
Figure 2.13. Eclipse modeled percent depth dose curves for the CIVCO universal and CIVCO sample extensions. ..........................................................................................32

1
CHAPTER 1
TREATMENT OVERVIEW
A neoplasm, also known as a tumor, is the result of abnormal tissue cells whose
reproductive cycles are malfunctioning, causing overactive reproduction and division.1 A
tumor is both benign and self-contained, or malignant (cancerous) with rapidly dividing cells
that kill surrounding tissue cells and metastasis throughout the body using the blood system.1
Removal of tumors can be difficult depending on the location and size of the tumor, and is
performed using either surgery, chemotherapy or radiation techniques.1
Radiation is defined as the emission and propagation of energy through space or a
material medium.2 Similarly, dose is defined as the amount of energy deposited in a medium
per unit mass. This transfer of energy is the basis for External Photon Beam Radiotherapy,
which is used in the treatment of both benign and malignant tumors. External Photon Beam
radiotherapy is performed using an x-ray beam from a source located outside the patient to
irradiate a target volume inside the patient.2 Through this targeting, energy is transferred to
particles inside tissue cells with the purpose of stopping cell reproduction attributed to tumor
growth.
Radiation exposure is closely monitored and regulated by federal organizations for
occupational, public, and medical exposure. The United States Nuclear Regulatory
Commission has published radiation exposure limits for non-medical exposures in Title 10,
Chapter 20 of the Code of Federal Regulations.3 Medical exposure limits are more complex,
the International Commission on Radiation Units and Measurements (ICRU) presents
recommended tolerance levels for calculation accuracy of treatment planning systems with
regards to delivered dose in Report 42. This report suggests that the calculated dose
distribution across high gradient distributions should be within 2% of the relative dose or
within 0.2cm of the isodose curve position in the target volume.4 Over the total planning
target volume, the ICRU recommends the delivered dose be within 5% of the actual
prescribed dose. Although the tolerances put forth by the ICRU are suggested tolerances

2
rather than required tolerance limits, these limits contribute to the principle of ALARA (As
Low As Reasonably Achievable) treatment doses.
Over the past 50 years or so, the use of linear accelerators has improved to allow for
more control over definition of treatment areas and required treatment beam characteristics,
resulting in improved control over dose delivery within patients. Furthermore, the use of
external photon beam radiotherapy has undergone several changes in radiation delivery
techniques and modalities. Over time the method of radiation treatment has switched from
the use of a single treatment beam to the utilization of multiple beams and field sizes,
although the basic principles of external beam radiation therapy still remains the same; to use
radiation to destroy tumor cells without damaging any surrounding normal tissue beyond
their ability to repair themselves.5 However with the advent of new treatment techniques, the
requirement for vigilant quality control requires the re-evaluation of elements that previously
may have been considered of no importance during early treatment techniques.
1.1 BASICS OF PHOTON RADIOTHERAPY External Photon Beam Therapy utilizes a linear accelerator to produce a focused,
beam of x-rays that can be used for patient exposure. A linear accelerator produces this x-ray
beam by first producing a beam of high-energy electrons and aiming the electron beam at a
target made of material with a high atomic number. The interactions of these electrons with
the target result in Bremsstrahlung x-ray emissions that form a resultant treatment x-ray
beam. This x-ray beam is shaped first by a primary set of collimators, found directly behind
the x-ray target. Because the x-ray beam is heterogeneous a flattening filter is used to
influence the energy uniformity of the beam before it passes through a second set of
moveable collimators. The primary collimators are stationary, but the secondary collimators
are made of lead or tungsten pieces, which allow for treatment field size variation through
adjustment of each piece.2
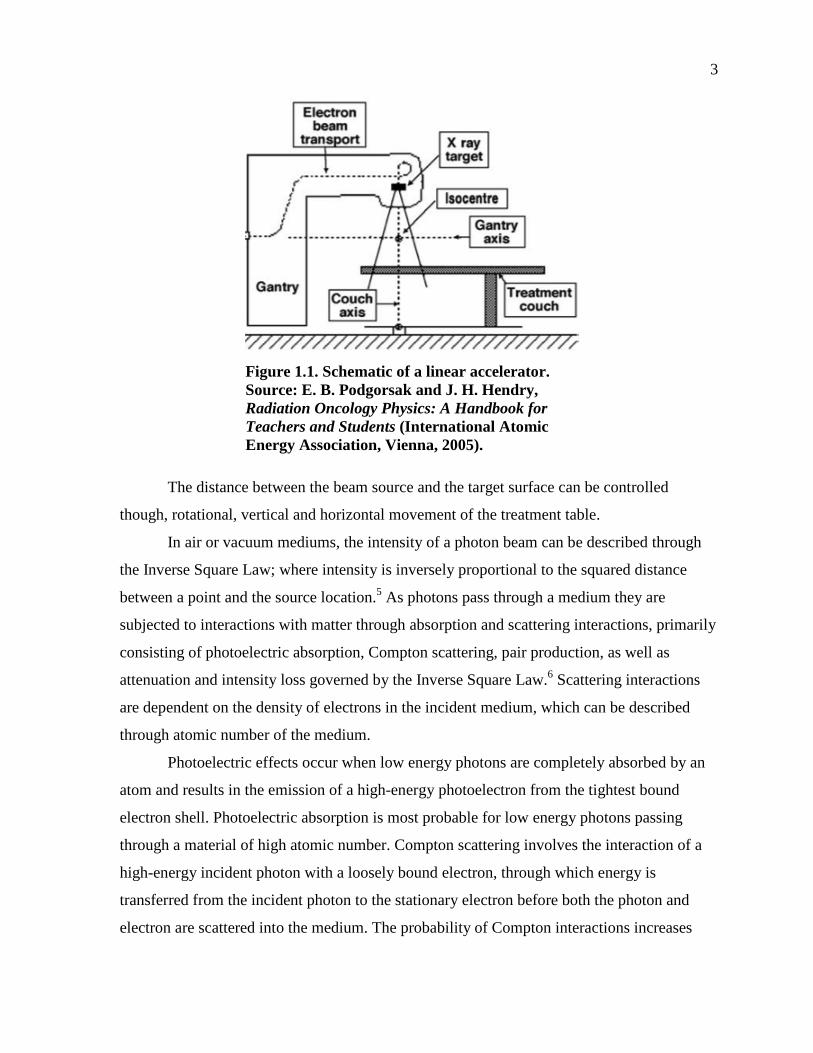
Linear accelerators used for isocentric treatments have a Gantry that allows for a full
360° rotation around the system’s isocenter, the point where the axis of rotation of the
secondary collimator perpendicularly intersects the gantry’s rotational axis (Figure 1.1).5
This rotation allows the treatment beam to enter the target medium at a designated angle of
incidence. While the gantry can move rotationally, the radius of rotation cannot be altered.
3
Figure 1.1. Schematic of a linear accelerator. Source: E. B. Podgorsak and J. H. Hendry, Radiation Oncology Physics: A Handbook for Teachers and Students (International Atomic Energy Association, Vienna, 2005).
The distance between the beam source and the target surface can be controlled
though, rotational, vertical and horizontal movement of the treatment table.
In air or vacuum mediums, the intensity of a photon beam can be described through
the Inverse Square Law; where intensity is inversely proportional to the squared distance
between a point and the source location.5 As photons pass through a medium they are
subjected to interactions with matter through absorption and scattering interactions, primarily
consisting of photoelectric absorption, Compton scattering, pair production, as well as
attenuation and intensity loss governed by the Inverse Square Law.6 Scattering interactions
are dependent on the density of electrons in the incident medium, which can be described
through atomic number of the medium.
Photoelectric effects occur when low energy photons are completely absorbed by an
atom and results in the emission of a high-energy photoelectron from the tightest bound
electron shell. Photoelectric absorption is most probable for low energy photons passing
through a material of high atomic number. Compton scattering involves the interaction of a
high-energy incident photon with a loosely bound electron, through which energy is
transferred from the incident photon to the stationary electron before both the photon and
electron are scattered into the medium. The probability of Compton interactions increases

4
linearly with the atomic number of a material. Pair production is strongly dependent on the
energy of the incident photon. For photons with energy greater than 1.02MeV, it is possible
for the photon to interact with the electromagnetic field of an atom’s nucleus, producing an
electron and positron pair. The probability of this interaction increases with the square of a
material’s atomic number.2,5,6
All of the primary interactions photons with matter cause secondary charged particles
to be released in the medium. Photons are thus considered to be indirectly ionizing radiation,
such that as high-energy photons pass into a medium they cause the medium to release
ionizing particles, electrons, which subsequently interact with and transfer energy to
surrounding particles.2 In the case of megavoltage external photon beam radiotherapy, the
energy of incident photons on the patient’s surface is on the order of 4 to 25MV.5 When the
relatively low effective atomic number of tissue ~7.5, is also taken into consideration, the
most probable interaction of incident photons is Compton scattering.6 As such, the transfer of
energy through the medium follows the following steps after the photon is incident on the
patient surface. For external photon beams on tissue, the megavoltage photon enters the skin
and continues to travel through the tissue until it strikes a stationary, loosely bound electron
in a tissue cell. The photon transfers a portion of its energy to the electron and is then
scattered at an angle relative to the photon’s original direction. At megavoltage energies this
scattering angle is relatively small and the photon still moves in a forward direction.7 At the
same time the electron is released to move through surrounding tissue.
Tissue cells are made primarily of water molecules, H2O. As electrons are freed
through Compton scattering, free radicals (molecules with an unpaired electron) are produced
in the tissue cell, which can damage DNA structure. In tissue, the produced Hydroxyl radical
(OH) can be highly damaging to DNA structure.8 The unpaired valence electron of the free
radical makes it highly reactive resulting in a short lifetime and an inability to travel far in
the tissue before reacting with another molecule. Still free radicals in tissue cells break apart
chemical bonds that alter DNA and cause biological effects.5 Unfortunately, this procedure is
not unique to target cells.
According to the Law of Bergonié and Tribondeau, cells that are more rapidly
reproducing and dividing are more sensitive to ionizing radiation than cells that reproduce at
slower rates.5 External Photon Beam Radiotherapy is generally used for deep tumors;

5
consequently the treatment beam passes through several layers of normal tissue cells before
reaching the target volume of tissues below the skin’s surface. Of the normal cells exposed to
radiation, by the definition of the law of Bergonié and Tribondeau, some of the most
radiosensitive cells include germinal epithelium, sebaceous glands and hair follicles. These
cells are all held within the epidermis skin layer, which undergoes a complete renewal and
replacement every 2 weeks.9
Radiation effects are classified in two types, stochastic and deterministic effects. A
stochastic effect is an effect that is dependent on a probability of occurrence, which is
increases with dose, but the effect does not always appear at a certain exposure, and there is
no minimum exposure needed for manifestation. The probability of a stochastic reaction is
expressed by organ weighting factors, given in the ICRP publication 60. Skin, for example,
has a weighting factor of 0.01 relative to the probability of stochastic effects being produced
with during total body irradiation.9 This corresponds to a low probability of ionizing
radiation causing any stochastic effects in skin, rather than another organ of the body.
On the other hand, deterministic effects have a high threshold dose, which must be
reached before they appear. Instead of the probability of deterministic effects increasing with
dose, the severity of the deterministic effect increases with dose beyond the threshold value.
The high threshold dose of deterministic effects results in cell death in exposed tissue
through interruptions of cell function and in structure.2
The surface skin layer is one of the first places to exhibit deterministic signs of
radiation exposure or damage. Before the Roentgen was instituted as the standard unit of
measure for Exposure, therapists used to use a unit called the Skin Erythema Dose.2 This unit
was defined as the amount of radiation exposure required to induce a reddening of the skin’s
surface within a given time period. This unit, however, was dropped due to the fact that
reactions of cells to radiation exposure are dependent on several different factors. Cell
response to radiation exposure is dependent on the amount of radiation, rate of exposure,
extent of exposure, and the quality of the beam used for exposure.9
Skin reactions were discovered through the first reported adverse skin radiation effect
in 1901, when Henri Becquerel suffered a skin burn after holding vial of radium in his
pocket.5 With the advent of radiation safety and protection, the threshold dose levels for
different skin reactions have been studied for various severities of skin reaction. The

6
minimum exposure for a reddening of the skin surface, erythema, is around 1Gy within a
relatively short time.9 For short exposures between 2 and 6 Gy, erythema can appear on
exposed skin within 1 to 2 days of exposure. If the exposure is over 3 Gy the erythema can be
accompanied by a temporary loss of hair over the small exposed area. These symptoms will
generally heal within about 4 to 8 weeks, during which the Erythema reappears for several
weeks, with the worst manifestation occurring the 3rd week after exposure.
Higher exposures result in a faster and more severe manifestation of erythema on the
exposed area. If the exposure over an approximate 4 week period, reaches a high enough
total dose between 20 to 50Gy, the skin reactions can include, but are not limited to,
permanent hair loss, acute radiation dermatitis with moist desquamation (peeling), vascular
damage, permanent darkening of the skin, and extreme erythema over the treatment area.
This amount of exposure produces permanent changes in skin tone and hair growth, however
the other symptoms can heal within 2 to 3 months of the first exposure. Depending on the
extent of the tissue damage caused by these large exposures, the skin can also become
atrophic, highly susceptible to damage and develop lesions or infections at the exposure site.9
1.2 TREATMENT BEAM CHARACTERISTICS Tumors can develop in any location and at any size within the body, which means
some tumors cannot be accessed or treated without passing radiation through surrounding
normal tissues. Because normal tissue cells, including those located in the skin surface, are
radiosensitive, effort has to be made to spare normal tissue as much as possible to reduce the
occurrence of skin reactions. The field of photon radiotherapy has changed to reflect this
need since the first introduction of linear accelerators as clinical delivery systems for external
photon beams in 1956.10
The earliest clinical linear accelerators were only capable of generating single photon
beam energies, with limited range of rotation (approximately 120°) of the source point
around the system’s isocenter.10 Modern linear accelerators are capable of producing multiple
photon beams of different beam energy, in addition to several electron beams with full gantry
rotation across 360 degrees. Beam field shaping methods have developed since the first
installation of a primary collimator in the 1960s, to the use of hand-positioned blocks and
wedges for normal tissue sparing in the 1970s, to the development and implementation of

7
multi-leaf collimators in the 1990s.10 Currently, external photon beams produced with
modern linear accelerators can be shaped and controlled for case-by-case treatment planning.
Some of the controllable aspects of treatment beams include beam energy, beam field size
and the angle of incidence between the treatment beam and target surface.
One of the most important factors in external photon beam radiotherapy is the energy
of the treatment beam used. As the energy of the incident photon increases the depth at which
maximum dose is delivered also increases. Consequently megavoltage beams provide an
advantage over lower energy beams such as orthovoltage (150-500kV), and supervoltage
(500-1000kV) beams, because they produce a lower deposited dose in surface and superficial
tissues.2 This is called skin sparing and is important when treating deep-seated tumors, such
as those found in the abdomen because the target volume may be defined several centimeters
below the skin surface and a lower deposited dose reduces the risk of deterministic effects in
normal tissue.
1.3 DOSE DISTRIBUTION Recall that dose is defined by the amount of energy deposited per unit mass. For
photon beams, the distribution of dose changes between the target surface, within the buildup
region, and declines after the depth of maximum dose deliver, dmax. As previously described,
surface dose is inversely related to the energy of incident photons on the medium. Because
photon beams are indirectly ionizing, surface dose is actually delivered due to contamination
of the incident photon beam by secondary electrons.2 These secondary electrons are produced
by backscatter in the target medium and interactions between the photon beam with
collimators, air, and any other material in the beam path.5 The surface dose therefore
increases with field size and source to skin distance, because the treatment beam has more
opportunities to interact before reaching the target surface. The higher the contamination of
the beam, the more electrons are present to transfer energy to surface cells, increasing the
delivered surface dose.
As previously discussed, as photon beams travel through a medium it causes the
release of ionizing particles. For megavoltage beams in a clinical setting, these ionizing
particles are recoil electrons produced by Compton interactions. As the beam passes through
the medium, the intensity of the beam decreases due to the scattering of photons and lost

8
energy given to released recoil electrons.5 Fewer high-energy photons at deeper depths
means the number of electrons released in the medium decreases with increasing depth. Since
dose is delivered by the electrons depositing energy at the end of their range in a medium, the
dose delivered through the medium reaches a maximum value at a depth dmax.2 This depth is
determined by the range of the electrons released near the surface and superficial layers of
the medium, since the highest numbers of electrons released are from interactions close to the
target surface.
The distance between the target surface and the depth at which maximum dose is
delivered is known as the build up region. Within this region the delivered dose increases
until reaching the maximum delivered dose at dmax.5 Beyond the build up region the delivered
dose decreases as depth increases. The distribution of dose through a medium can be
qualified using a Percent Depth Dose (PDD) curve or a Tissue Maximum Ratio (TMR). PDD
is defined as the ratio of delivered dose at a depth to the delivered dose at a reference depth.
Similarly the TMR is defined as the ratio of dose delivered at a given point in a phantom to
the dose at the same point for the reference depth of maximum delivered dose.5 As depth
increases both PDD and TMR values increase before reaching a maximum value at the given
reference depth, then decrease beyond the build up region. As beam energy increases both
PDD and TMR increase comparatively for depths beyond dmax, between energies due to
increased penetration of higher energy photon beams. The PDD and TMR values also
increase with an increased field size due to increased electron contamination in the beam
caused by scatter and interactions before intersecting the target.5 The difference between
these quantities lies in the method by which measurements are made.
Both PDD and TMR measurements can be made using an ionization chamber inside a
water phantom, and are mainly taken using small field sizes to reduce the effects of electron
contamination of the photon beam. PDD measurements are made using the same source to
surface distance for each depth measurement, that is the distance between the source and the
surface of the phantom remains constant while the detector moves within the phantom. TMR
measurements are made by placing the detector at isocenter, using a constant source to axis
of gantry rotation distance, but the source to surface distance decreases as depth increases.5
Through inverse square law, PDD values are dependent on the source to surface distance,

9
while source to surface distance has very little influence on TMR measurements because the
distance between the radiation source and the detector is unchanged.
1.4 CURRENT TREATMENT MODALITIES The development of linear accelerators with more control over the use of multiple
beams, field sizes, beam energies and gantry rotation, has led to the development of
rotational radiation therapy techniques using optimized treatment plans. The optimal
treatment plan for a treatment would deliver a lethal amount of dose to all the abnormal,
tumor cells without delivering any dose to normal tissues. While such a plan is not possible,
treatment plans can be ‘optimized’ in part through the use of multiple fields, beam modifiers
and proper beam angles, determined using 3D images of the patient.2 Taking advantage of
plan optimization through the use of multiple treatment beams has allowed therapists to use
radiation as a non-invasive treatment method for tumors that are in difficult locations in the
body, as defined by the depth of the tumor, or the radio-sensitivity of surrounding organs and
tissues.11
This can be performed through modalities such as Intensity Modulated Radiation
Therapy (IMRT) and Intensity Modulated Arc Therapy (IMAT). Both of these treatment
modalities use dynamic multi-leaf collimators to shape the treatment field specifically to the
desired treatment area for multiple treatment fields, while allowing for gantry rotation during
patient treatment. X-ray beams produced by linear accelerators are not necessarily of uniform
fluence without the use of a flattening filter. The basic principle of intensity-modulated
therapy is that multiple non-uniform treatment fields can be combined together to produce a
uniform fluence and subsequent absorbed dose across the target volume.12 Simultaneously,
the combination of non-uniform fluence fields can allow for greater sparing of surrounding
normal tissue, reducing damage done to surrounding tissue. The stricter definition of the
irradiated volume, allows for the use of higher radiation doses for treatment, with less
opportunity for adverse side effects in normal tissues. This is a benefit in tumor treatment
because higher radiation doses are more effective in damaging cells and thus are more
effective as treatment beams.11
In some IMRT treatments multiple fields can be utilized through a stop and shoot
method; the gantry moves to a certain angle position, the multi-leaf collimator shapes the

10
field for the given angle and the beam is initiated for a given exposure. The gantry then
moves to the next prescribed angle and the process repeats until all the prescribed fields have
been treated. IMAT treatments differ in that it stays in constant motion rotating a single, full
360° rotation arc around the patient, with varying rotation speed and exposure rate. During
this arc, the multi-leaf collimator constantly changes the shape of the source aperture in order
to shape the treatment volume to the tumor volume.13,11 Both IMRT and IMAT techniques
share the benefit of reduced treatment time, which limits the opportunity for patient or tumor
movement during treatment. Reduced treatment time also allows for more patients to under
go treatment on the same day.14
Although advances in radiation treatment techniques and technology have been
effective in the treatment of tumors, the advent of new treatment techniques brings new
challenges and at times a need for reevaluation of pre-existing treatment components. One
such evaluation has arisen concerning the treatment couches used for external photon beam
radiation treatments on linear accelerators. As the logistics of radiation delivery have shifted
towards the use of more fields, treatment beams start to pass through the treatment couches.
Up until the use of multiple treatment fields and beams, the treatment couches may have been
considered negligible in treatment planning, as they previously had little interference with the
delivered radiation beam.
1.5 COMPOSITION AND DESIGN OF TYPICAL TREATMENT COUCH
The interaction of a photon beam with a treatment couch is dependent on the same
variables prevalent during the photon beam’s interaction with skin tissue; field size, beam
energy, source to surface distance, and beam angle. The penetration of the beam depends on
the energy of the incident photons and the atomic number of the material being traversed
influences the attenuation of coefficient if the absorbing material.6 This is due to the idea that
the attenuation coefficient represents the likelihood of the photon beam running into a
particle with which it will interact. Typical treatment couches installed on clinically used
linear accelerators are composed of multiple layers. One of the most common combinations
of couch materials is the use of carbon fiber layers around an inner foam section. Carbon has
an atomic number of 6, which reduces the probability of pair production and photoelectric

11
absorption interactions occurring with megavoltage treatment photon beams. This reduces
the amount of attenuation of the treatment beams before target medium interactions.7
Under current federal regulations, treatment couches and linear accelerators used for
therapeutic radiation exposure fall under the classification of Class II devices and are subject
to regulation by the Center for Devices and Radiological Health (CDRH), held within the
United States Food &Drug Administration.7 Under this designation, treatment couches are
evaluated for motion and weight support characteristics. For example, during couch rotation,
the location of the system isocenter on the couch surface must be within 2mm for any degree
of rotation.2 As of yet regulations have not been published for attenuation limits of treatment
couches used in multi-beam treatments. This presents a possible problem if the attenuation
characteristics of a treatment couch are not accurately modeled in the treatment planning
system, the effect of the couch on delivered dose could exceed the ICRU suggested 5%
margin for prescribed to delivered dose.
1.6 PREVIOUS STUDIES CONCERNING COUCH ATTENUATION
As the number of fields used for patient treatment increases, the effect of treatment
couches becomes more significant.15 The investigation of the impact of treatment couches on
radiation delivery has been conducted from a vast array of perspectives and with focus on
several different treatment couches. The effect of treatment couches on skin sparing effects is
one of the most studied characteristics. An investigation of 8 different couch and insert
models, Seppala et al. found that megavoltage skin sparing benefits were reduced.16 A
photon treatment beam intersecting a iBEAM evo carbon fiber couch (Medical Intelligence,
Schwabmunchen, Germany) experienced an increased skin dose percentage of Dmax, from
17.9% to 92% of Dmax, using a 10x10cm, 6MV beam. A skin dose percentage of 92% of
maximum dose is almost a complete removal of any skin sparing characteristics of the
beam.17 This change in measured surface dose is tied to decreases in the depth at which
maximum dose is delivered. Gerig, et al. proposed that the shift in depth of maximum dose
delivery can be treated as a ‘radiological thickness’ for the treatment couch.18
Mihaylov, et al. evaluated a method for adding treatment couch structures into
treatment planning systems by importing CT scans of treatment couch and tracing contours
of each couch component. These traced contours can then be assigned densities or

12
Hounsfield units based on composition materials and added to patient images used for
planning.19 Using this method, Mihaylov, et al. added an ExacTrac couch into the Pinnacle
treatment planning system (Phillips Medical Systems, Fitchburg, WI) with resultant dose
calculations within 2% of delivered values.19
Similar couch tracing techniques have been used by Munjal, et al. for a Med-tec
carbon fiber couch during IMRT planning and Zhihui, et al. for accurate modeling of a
Siemens ZXT couch using the Pinnacle3 8.0 treatment planning system.20,21 Also, Wagner
and Vorwerk performed a study on the accuracy of the assigned Hounsfield unit values
present in the Varian Eclipse treatment planning system for the Varian EXACT couch. This
study showed that while the Eclipse software uses default Hounsfield numbers as -300HU for
the carbon layers, -1000HU for the internal foam, and 200 HU for the rails, better dose
predictions can be made by adjusting these values.22
The Varian EXACT couch is a frequently used treatment couch that has been
investigated for attenuation by several researchers. In 2003, Veira et al. found attenuation of
up to 15% for oblique beams passing through the EXACT couch.23 Furthermore according to
research done by Li, Lee, Johnson, Zhu and Kudchadker, this attenuation value can be as
high as 26.8% during multi-field treatments using 5x5cm2, 6MV beams passing through the
support rails and couch top.24 Similarly, Proojen, et al. published an article stating the
EXACT couch produced a 3% lower delivered dose through the planning target volume.
Their study also used Mihaylov-like techniques to predict dose within 2% accuracy. The
study generated a maximum attenuation of ~17.5%, for a 6MV beam passing through with
rails pushed to the side for an n approximate 237°±1° gantry angle.25
Measurements made on the Varian IGRT couch by Munjal, et al. showed a maximum
attenuation of 4.8% through the thickest section of the IGRT couch.21 The surface dose using
a 6MV beam for an IGRT couch was estimated to change from ~16% to ~90% of the
maximum delivered dose.26 The interference of treatment couches has been to shown to alter
delivered dose in clinical settings. As such, the four couch inserts investigated in this study
are expected to show attenuation of the treatment beam prior to entering the phantom.
13
CHAPTER 2
OVERVIEW OF STUDY
This study took place at University of California, San Diego Moores Cancer Center
facilities in La Jolla and Encinitas, California. Data was collected using three linear
accelerators, a Varian Truebeam 23iX Clinac accelerator and two Varian Trilogy medical
accelerators. In this investigation we evaluated the attenuation characteristics of 4 different
treatment couches used in multi-field dose treatments. These treatment couches are the
Varian EXACT couch, the Varian IGRT couch, the Varian tennis racket insert, the CIVCO
Universal treatment couch extension and a CIVCO Sample treatment couch extension for a
new construction of the original universal model. This evaluation was performed through
observation of direct attenuation measurements made using a tissue equivalent phantom, and
through determination of the effect of beam-couch interference on the surface dose of the
target medium. Direct attenuation measurements were made for two different beam energies,
using three field sizes in order to observe how energy and field size affect the severity of
couch attenuation effects. The accuracy of inclusion of treatment couches during treatment
planning will be evaluated through comparison of directly measured values with those
predicted by the treatment planning system.
Based on past research and studies, the attenuation of treatment couches is expected
to be most significant under relatively low treatment beam energies, using a small field sizes,
at oblique beam angles. One of the differences in this investigation is that although the
Varian tennis racket insert is considered, and modeled to be free of attenuation properties, the
tennis racket is expected to actually contribute to beam attenuation. Furthermore the study of
the CIVCO Sample extension has not been completed before, and it is expected that the
thinner overall design of the new construction, compared to the original Universal extension,
will allow for less beam attenuation.

14
2.1 MATERIALS AND METHODS This study consisted of two types of measurements, direct attenuation measurements
and percent depth dose measurements.
2.1.1 Direct Attenuation Measurements: General Setup
Direct measurements of couch attenuation were made using a 0.66c farmer-type ion
chamber isocentrically placed in the center of a homogeneous cylindrical acrylic CT dose
phantom (Fluke Biomedical, USA). The positioning of the ionization chamber at the
system’s isocenter results is a constant source to detector distance as the gantry is rotated
around the phantom (see Figure 2.1). Conveniently, the cylindrical phantom resulted in a
constant detector depth in the phantom across all gantry angles. The phantom was positioned
using triangular cushions along the central axis of the gantry as defined by system laser
guides (see Figure 2.2). This set up was used to make initial dose measurements at the
machine’s isocenter given an angle of incidence of 0 degrees. This measurement corresponds
to the dose collected at the isocenter by a beam not passing through a treatment couch.
Measurements were also taken from an angle of 180 degrees such that the beam passes
perpendicular through the treatment couch before reaching the system’s isocenter.
Figure 2.1. Gantry Rotation around isocenter.

15
Further measurements were taken at varying degree intervals between the 180
incident beam to beams reaching one side of the couch, for the purpose of monitoring the
Figure 2.2. Experimental set-up for direct attenuation measurements.
change in attenuation for given beam paths through the treatment couch. These
measurements represent the attenuation distributions across the couch from the center to one
side of the treatment couch during isocentric treatments. Comparing these measurements
with the dose collected without passing through the treatment couch produced the percentage
by which the beam was attenuated by the treatment couch using the equation:
%Attenuation =100 * (1 −Dtc
Dnc
)
Where Dtc represents the dose measured with the beam passing through the treatment
couch and Dnc represents the dose measured while the beam did not intersect the treatment
couch, and was always treated as the dose measured with the machine set for a 0 degree
angle of incidence. Each of these measurements were made at two different beam energies
of 6MV and 15MV, and for 3 different field sizes; 5x5cm2, 10x10cm2 and 20x20cm2.

16
2.1.2 Varian EXACT Couch Two different EXACT treatment couches were employed during the attenuation
measurements, both in use on Varian Trilogy treatment delivery systems. Initially attenuation
measurements were taken with regards to measurements made using a tennis racket support,
however it was later found that the tennis racket itself provided a small amount of attenuation
and in some cases increased scatter, and therefore dose. The EXACT couch measurements
were later corrected by subtracting direct attenuation measurements taken implementing the
tennis racket support from the attenuation measurements taken using the EXACT couch.
The EXACT couch is designed using a 2.5cm couch top, with two 8.5cm moveable
rails on the underside of the couch. The couch top is divided into three layers, a 1mm carbon
top carbon layer, a 2.5mm carbon bottom layer and an internal foam layer. The support
system is designed such that the rails can be positioned on the exterior sides or together in the
center of the couch.22 This rail movement reduces the necessity for patient repositioning
during treatment, but it makes it necessary to measure the attenuation of the couch in both
rails position setup cases for each energy and all three different field sizes within each
energy.27
2.1.3 Varian IGRT Couch The IGRT couch was installed on a Varian Truebeam treatment system and is
composed mostly of carbon fibers, and no metal components allowing for its use in
imaging.28 The IGRT couch increases in thickness moving longitudinally from the section of
the couch used for head treatments towards the section used for abdomen treatments. As such
the couch was subdivided such that three sections of the couch were subjected to attenuation
measurements at the region of average thickness, resulting in average attenuation
measurements for each of the three thickness sections. Direct attenuation measurements were
taken for each region of thickness for each energy and field size combination using the
general attenuation measurement set up discussed previously.
2.1.4 CIVCO Couch Extensions The CIVCO couch consists of a series of inserts, which can be changed depending on
the needs of each treatment. In this study two of the inserts were measured for attenuation
characteristics. The first of these inserts is a current model known as the CIVCO Universal

17
treatment extension that employs a thick couch top, about 5cm, with approximately 1cm
thick side wings, but has no supporting rails. The second insert is a new construction given to
the University of California, San Diego Moores Cancer Center as a beta sample. This insert,
called the CIVCO Sample extension from this point forward, employs a small, stationary
support rail, but the table thickness is much thinner that that of the currently used Universal
insert. Each construction was installed on a Varian Trilogy treatment system for
measurements, once again using the general attenuation measurement setup.
2.1.5 Tennis Racket Support A Tennis Racket insert consists of a thin carbon fiber grid that is considered air
equivalent during dose delivery.16 However it was noticed during measurements of the
EXACT couch that the Tennis Racket had an impact, although small, on the measured dose
of the system. As such, the attenuation of the tennis racket was directly measured using the
same general attenuation measurement setup as the other couch sets.
2.1.6 Tissue Maximum Ratio Measurement of EXACT Couch with Rails Out
For the EXACT couch, a TMR curve was created using measurements taken directly
through the use of a solid water phantom and the farmer-type ion chamber. This was done by
placing solid water directly onto the tennis racket insert, with the farmer chamber placed
inside the solid water phantom at isocenter and the EXACT couch insert, with rails out,
placed on top of the solid water phantom (Figure 2.3). Solid water was added to the top of the
phantom and the couch replaced on top of the phantom such that the farmer chamber
remained at isocenter but was submerged at increasing depths of solid water. These
measurements were compared to the measured dose at the depth of maximum dose for the
given beam energy. These measurements were repeated for both a 6MV and 15MV beam,
under the same three different field size scenarios used for the attenuation measurements and
without the EXACT couch insert between the phantom and the beam for comparison.
2.1.7 Percent Depth Dose Measurements of IGRT and CIVCO couches
EBT2 Gafchromic film (International Specialty Products, NJ) was used to produce a
Percent Depth Dose for the largest thickness of the IGRT couch using a 10x10 field size, at

18
Figure 2.3. Measurement set-up for TMR measurement on EXACT couch.
beam energy of 6MV. Of the energies and field sizes being investigated in this study, this
combination was determined to exhibit the highest percentage of attenuation. Placing the
Gafchromic film between slabs of solid water and placing the solid water such that the edge
of the film was against the couch surface produced the Percent Depth Dose curve after the
film was exposed using a beam from directly below the table. A second percent depth curve
was created for treatments not through the treatment couch by placing a piece of film
between slabs of solid water such that the top edge of the film was even with the central axis
of the treatment delivery system. This film was then exposed using the same 10x10cm2 field
size and 6MV photon beam, from above such that the beam did not pass through the
treatment couch.
Both constructions of the CIVCO couch were not directly measured to produce a
percent depth dose curve, but instead were modeled in the Eclipse planning software.
2.2 ECLIPSE MODELING The Moores Cancer Center utilizes Varian Eclipse treatment planning software
(Varian Medical Systems, Palo Alto, CA) for patient treatment and research. As such, the
accuracy of the Eclipse planning software was evaluated by modeling all of the direct
measurements made in this investigation for comparison, including the attenuation

19
measurements and TMR/PDD measurements. Both the Varian EXACT couch and Varian
IGRT couch have model structures that already exist in the Varian treatment planning
software. As such, the couches were included in the treatment planning by simply including
the structures in the initial plan and evaluating the Eclipse Software in its accuracy in
compensating for the added structures.
The CIVCO couch inserts were not as easily introduced in the treatment planning
software because they are not a Varian product and thus do not have pre-existing models in
the Eclipse software. In order to include the CIVCO couches in the planning system, each
insert was CT scanned and the images uploaded into the Eclipse program. From these CT
images each structure of the couch was traced and assigned a Hounsfield number based on
the value measured during the CT scan. The structure set was then copied into a treatment
plan including a model of the acrylic phantom, and dose calculations were made using the
new plan including the copied couch structure set (Figure 2.4).
Although the Eclipse software has a pre-existing structure set for the use of a tennis
racket, the pre-existing model is based on the idea that the tennis racket should have no
affect, be it attenuation or scatter contribution for the dose measurement. Therefore the tennis
racket insert was also CT scanned, uploaded to the Eclipse system, and was traced and
modeled for comparison with the pre-existing model and the direct attenuation measurements
made on the Trilogy treatment delivery system.
2.3 ERROR CONSIDERATIONS Uncertainty in the dose measurements within a phantom is dependent on the accuracy
of the ionization measurement and the positioning of the chamber inside the phantom. It was
difficult to judge the center of the ion chamber once placed inside the acrylic phantom. If our
setup was not accurately centered on the gantry’s isocenter our measurements may have been
lower than a clinical situation because as gantry angle increased the distance form the source
to the detector would increase, causing the intensity to decrease by the inverse square law. Or
if off center in the direction of gantry angle rotation, the dose measurements would be higher
based on the distance between the source and detector decreasing, causing the intensity to
increase. This would cause the intensity at the detector under an oblique angle setup to be

20
Figure 2.4. (a) CT scan slice of the CIVCO Universal couch extension, (b) Contour traced couch structures from CT scan slice, (c) Resultant couch structure set produced in the Eclipse treatment planning system, after couch contouring and Hounsfield unit assignment of each couch structure.
a
b
c
21
higher than at the comparison measurement, which would result in a lower calculated
attenuation. Subsequently if the chamber was off set away from the direction of rotation, the
intensity at the chamber would be lower at the oblique angle than at the degree comparison
measurement resulting in a higher calculation for attenuation.
Inherent in the measurement set up of the acrylic phantom and the Farmer type ion
chamber there is a small gap of air between the acrylic and the ion chamber. The radius of
the detector chamber was slightly smaller than the radius of the hole at the center of the
acrylic phantom. Medical tape had to be wrapped around the arm of the ionization chamber
to secure the chamber in the center of the phantom. Air increases scatter, so our
measurements may be higher than what may actually occur in a patient. However, since this
gap was present across all the measurements taken for each field size and energy pairing, we
can ignore this increase for evaluation of attenuation. That is, the scatter added by the air
surrounding the chamber for a measurement using the 6MV beam in a 5x5 field size should
be independent of the gantry angle and thus be negligible in comparison of two
measurements made using the same energy and field size.
Similarly if during the direct attenuation measurements, the acrylic was sitting up off
of the table through the use of the triangle cushions used to secure the cylindrical phantom,
then an air gap between the phantom and couch surface will result in increased scatter
contributions to dose. Still when measurements are taken under the same energy and field
size, scatter should be the same and negligible during attenuation calculations. According to
the measurements of Wagner and Vorwerk, calculated doses in the Eclipse planning system
have an uncertainty if 1% and measured values positioned using laser guides can be
estimated to have an uncertainty of 2.2% of the measured dose.22
2.4 RESULTS For all of the couches tested in this study, maximum attenuation was observed under
the smallest field size tested (5x5), using the lower energy of 6MV. Also for each couch and
across all three field sizes, the higher energy treatment beam of 15MV, was affected less by
the introduction of the treatment couch into the beam path, than the lower energy beam.
These measurements were all taken across half of the treatment couch; therefore any graphs
only represent the attenuation spectrum from the lengthwise central axis of the couch to one

22
side of the couch surface. However due to the symmetry present in all the couches studied in
this investigation the attenuation spectrums produced here should be representative of the
spectrum for each side of the couch.
2.4.1 Varian Tennis Racket Insert The straight measurement of the attenuation across the Varian Tennis Racket
produced attenuation values ranging from 0.06% to 0.39%, found in Table 2.1, depending on
beam energy and field size.
Table 2.1. Attenuation Measurements for the Varian Tennis Racket, when Beam is Passing Straight Through the Grid Surface
%Attenuation 6MV
beam
15MV
beam
5x5 field 0.39 0.33
10x10 field 0.19 0.06
20x20 field 0.18 0.22
The structure set corresponding to the use of a tennis racket in the treatment beam
produced no attenuation, and thus no effect on the calculated dose delivered through the
racket.
2.4.2 Varian EXACT Couch Attenuation The EXACT couch was measured to have a maximum attenuation of 19.2% when the
adjustable rails were pushed under the center of the couch. When the rails were in the outer
position, the EXACT couch measured a maximum attenuation of 5.98%. This value was
attained using an oblique treatment beam intersecting the side rail and couch surface. When
the rails were pushed to the center of the treatment couch, the distribution of attenuation
values across the couch surface produced a ‘M’ shaped curve (Figure 2.5), with two peaks of
maximum attenuation across gantry angles at which the beam intersected part of an
adjustable rail and the treatment couch. As energy of the treatment beam was increased, the
attenuation of the beam decreased relative to measurements made at the same gantry angle.
Both energies showed that an increased field size, decreased the effect of beam attenuation
despite gantry angle. Of further note is for situations where the rails are pushed under the

23
Figure 2.5. Attenuation measurements for a 10x10cm2 field, 6MV beam passing through the Varian EXACT couch with the adjustable rails pushed to the center of the couch.
center of the treatment couch, the angle of maximum attenuation differed from the angle of
maximum attenuation predicted by the Eclipse Treatment planning system. Values for the
attenuation measurements can be found in Table 2.2 and Table 2.3. The surface dose
measurements can be found in Table 2.4.
Table 2.2. Attenuation Measurements for 6MV Photon Beam Passing Intersecting the Varian EXACT Couch then the Adjustable Rails are Pushed Under the Center of the Treatment Couch (Rails-In Position) 6MV beam 5x5cm field 10x10cm field 20x20cm field
Gantry
Angle
Measured
%Attenuation
Calculated
%Attenuation
Measured
%Attenuation
Calculated
%Attenuation
Measured
%Attenuation
Calculated
%Attenuation
180 2.35 2.80 2.59 1.45 0.86 0.00
190 19.23 12.52 13.78 10.74 12.02 9.14
195 15.06 11.45 14.01 9.65 12.63 8.69
200 11.86 10.65 11.04 8.69 9.86 7.67
205 12.29 10.52 11.41 9.29 10.29 7.68
210 14.96 10.25 12.38 8.81 11.15 7.45
220 2.41 4.39 4.04 3.02 1.36 2.37
230 2.90 5.19 4.77 3.98 1.99 3.05
Average
Attenuation 10.13 8.47 9.25 6.95 7.52 5.76

24
Table 2.3. Percent Attenuation Measurements for 15MV Photon Beam Passing Intersecting the Varian EXACT Couch when the Adjustable Rails are Pushed Under the Center of the Treatment Couch (Rails-In Position)
15MV beam 5x5cm field 10x10cm field 20x20cm field
Gantry Angle
Measured
%Attenuation
Calculated
%Attenuation
Measured
%Attenuation
Calculated
%Attenuation
Measured
%Attenuation
Calculated
%Attenuation
180 1.24 2.22 0.28 2.27 -0.73 2.56
190 10.16 9.00 9.00 7.94 8.04 7.44
195 8.75 11.19 7.62 9.58 6.78 8.37
200 8.28 7.71 7.15 4.79 6.41 4.62
205 9.03 10.65 7.96 8.97 7.16 8.14
210 8.22 7.36 7.11 6.05 6.34 4.87
220 2.38 3.27 1.47 1.64 0.87 1.28
230 2.90 3.86 2.18 1.51 1.50 0.77
Average
Attenuation: 6.37 6.91 5.34 5.34 4.55 4.76
Table 2.4. Surface Dose Measurements for the Varian EXACT Couch, Taken from the TMR Curve Produced Using the Solid Water Phantom
6MV Beam No Couch in Beam Couch in Beam Difference
5x5 field 44.8 91.6 46.8
10x10 field 49.5 91.8 42.3
20x20 field 58.2 94.5 36.3
15MV
Beam No Couch in Beam Couch in Beam Difference
5x5 field 24.4 70.5 46.1
10x10 field 31 71.4 40.4
20x20 field 42.8 79.8 37
Positioning the rails to the outside of the treatment couch, the attenuation of the couch
insert itself was determined to be 1.64% in a 6MV beam and 1.27% for a 15MV beam. As
the gantry angle increased the attenuation also increased as seen in Figure 2.6. As with the
rails in set up, the maximum attenuation measurement was taken with the beam passing
directly

25
Figure 2.6. Attenuation measurements for a 10x10cm2 field, 6MV beam passing through the Varian EXACT couch with the adjustable rails pushed to the sides of the couch.
through one of the support rails at an oblique angle. For both energies and all three field sizes
the maximum attenuation occurred a gantry angle of 225°. All the measurement values for
the rails out set up can be found in Table 2.5 and Table 2.6.
Table 2.5. Attenuation Measurements for a 6MV Photon Beam Passing Intersecting the Varian EXACT Couch when the Adjustable Rails are Pushed Under the Center of the Treatment Couch (Rails-Out Position)
6MV beam 5x5cm field 10x10cm field 20x20cm field
Gantry Angle
Measured
Attenuation
Calculated
Attenuation
Measured
Attenuation
Calculated
Attenuation
Measured
Attenuation
Calculated
Attenuation
180 1.64 2.40 0.81 2.29 3.21 1.81
190 2.11 2.80 1.61 2.65 3.58 2.37
200 2.85 3.06 2.34 3.26 3.70 2.60
210 3.75 4.26 3.14 3.62 3.83 3.05
220 4.28 4.53 3.88 3.98 3.77 2.94
225 5.59 5.33 4.37 4.22 4.14 3.50
Average Attenuation: 3.37 3.73 2.69 3.34 3.70 2.71

26
Table 2.6. Attenuation Measurements for a 15MV Photon Beam Passing Intersecting the Varian EXACT Couch when the Adjustable Rails are Pushed Under the Center of the Treatment Couch (Rails-Out Position)
15MV beam 5x5cm field 10x10cm field 20x20cm field
Gantry Angle
Measured
Attenuation
Calculated
Attenuation
Measured
Attenuation
Calculated
Attenuation
Measured
Attenuation
Calculated
Attenuation
180 1.28 1.75 0.24 1.53 3.02 1.25
190 1.73 2.22 0.14 1.85 3.02 1.88
200 2.37 2.34 1.24 2.40 3.19 1.98
210 3.02 3.15 1.82 2.62 3.36 2.29
220 3.66 3.39 2.41 2.94 3.19 2.29
225 3.99 3.86 2.82 2.94 3.24 2.50
Average Attenuation: 2.68 2.78 1.44 2.38 3.17 2.03
The EXACT couch also showed a significant change in surface dose from 45% of
Dmax to 92% of Dmax with the introduction of the treatment couch into the 6MV beam for the
5x5cm2 field with the rails under the couch center. An example of the Tissue Maximum
Ratio curve for this couch can be found in Figure 2.7.
Figure 2.7. Tissue maximum ratio curve produced for the Varian EXACT couch using a 6MV, 10x10cm2 treatment beam.
The depth of maximum dose also decreased by 0.5cm across all experimental setups
when the EXACT couch was introduced into the treatment beam. Using the structure set
included in the Varian Eclipse Planning System for the Varian EXACT couch, the maximum

27
difference between the measured attenuation and planning system attenuation calculation is
7%, at the angle of maximum attenuation for the EXACT couch for the 6MV, 5x5cm2 field
with rails pushed in. When the rails were positioned under the sides of the couch, the
calculated values were within a range of 1.21% of the measured values.
2.4.3 IGRT Couch Attenuation As previously stated the Varian IGRT treatment couch was studied in three separate
sections determined by thickness divisions. As the IGRT couch is designed without the use
of support rails, the direct attenuation measurements increased as the gantry angle and
subsequent angle of incidence increased, reaching a maximum value at an oblique angle
between 240° and 250°, when the beam traversed through the side of the couch, depending
on field size. The IGRT couch produced a maximum attenuation of 7.22% with the treatment
beam passing through the thickest section of the couch. The maximum attenuation values for
each energy and field size can be found in Tables 2.7 and 2.8. Figure 2.8 shows distribution
of the attenuation measurements as the gantry angle increased.
Table 2.7. Attenuation Measurements for a 6MV Photon Beam Passing Intersecting the Varian IGRT Couch for Thickness Divisions
6MV Beam
Thinnest Section
Angle of Maximum
Attenuation
Measured
Attenuation
Calculated
Attenuation
5x5 field 240 6.7 5.47
10x10 field 240 5.93 4.48
20x20 field 240 5.29 3.73
Medium Thickness
Section
Angle of Maximum
Attenuation
Measured
Attenuation
Calculated
Attenuation
5x5 field 240 5.95 5.33
10x10 field 245 5.69 4.24
20x20 field 245 5.05 3.51
Thickest Section
Angle of Maximum
Attenuation
Measured
Attenuation
Calculated
Attenuation
5x5 field 250 7.22 5.87
10x10 field 250 6.88 4.97
20x20 field 250 6.18 4.41

28
Table 2.8. Attenuation Measurements for a 15MV Photon Beam Passing Intersecting the Varian IGRT Couch for Thickness Divisions
15MV Beam
Thinnest Section
Angle of Maximum
Attenuation
Measured
Attenuation
Calculated
Attenuation
5x5 field 240 4.45 3.86
10x10 field 240 3.88 3.17
20x20 field 240 3.48 2.71
Medium Thickness
Section
Angle of Maximum
Attenuation
Measured
Attenuation
Calculated
Attenuation
5x5 field 240 3.84 3.74
10x10 field 245 3.45 3.06
20x20 field 245 3.1 2.71
Thickest Section
Angle of Maximum
Attenuation
Measured
Attenuation
Calculated
Attenuation
5x5 field 250 4.96 4.21
10x10 field 250 4.78 3.5
20x20 field 250 4.34 2.92
Figure 2.8. Measured Attenuation values for the thickest section of the Varian IGRT couch for a 6MV treatment beam, using a 10x10cm2 field size.

29
Figure 2.9. Percent depth dose measurements for a 6MV beam, 10x10cm2 field, using the thickest section of the Varian IGRT couch.
As previously stated a Percent Depth Dose curve was produced for the thickest
section of the IGRT couch, using a 6MV beam with a 10x10 field size (see Figure 2.9). In
such a set up the IGRT couch showed an increase in surface from 68% of Dmax to 97% of
Dmax. The Percent Depth Dose curve also shows a decrease in the depth of maximum
delivered dose. Usually the depth of maximum dose delivery is considered to be 1.5cm for a
clinical 6MV beam, and the Gafchromic film measured dose delivered, without the couch in
the beam, a depth of maximum dose to be 1.45cm. However when the beam passes through
the IGRT treatment couch, the depth of maximum dose delivery was measured as 0.81cm, a
decrease of 0.64cm.
A structure set for each thickness delineated section is pre-existing in the Eclipse
treatment planning system. For each section of the couch, the treatment planning system’s
calculated values were within 2% of the direct measurement made in this study. The largest
separation between the measured and predicted value was 1.94% on the thickest section of
the couch, using a 6MV beam under a 10x10 field size.
2.4.4 CIVCO Couch Attenuation The original Universal CIVCO treatment couch extension was measured to have a
maximum attenuation of 6.47% when a 6MV treatment beam passed a 5x5 field through the

30
couch surface at an angle of 245°. Similar to the Varian IGRT couch, the Universal treatment
couch extension does not have an additional support rail beneath the treatment couch. As
such, the attenuation profile of the Universal couch insert resembles that of the IGRT couch,
with attenuation increasing as the gantry angle increased, increasing the angle of incidence
(Figure 2.10).
Figure 2.10. Attenuation measurements for the CIVCO universal extension using a 6MV treatment beam, with a 10x10cm2 field size.
On the other hand, the CIVCO Sample couch extension has a small immobile support
rail under a thinner couch surface. The resulting attenuation measurements produced a profile
with peak attenuation at a gantry angle of 245° for all field sizes at both energies. The
Sample extension had a measured maximum attenuation of 7.7% for the 6MV treatment
beam using a 10x10 field size, as seen in Figure 2.11.
It should be noted, however, that although the Sample insert produced a larger
maximum attenuation than the Universal insert, over the area through which the treatment
field did not intersect the Sample insert’s support rail, the Sample CIVCO measured much
smaller and more consistent attenuation, when compared to the Universal insert (Figure
2.12).
The imported CT images of the CIVCO extensions showed measured Hounsfield
units of -995 HU for the internal foam core, and -750HU for the surrounding carbon layers.

31
Figure 2.11. Attenuation measurements for the CIVCO sample extension using a 6MV treatment beam, with a 10x10cm2 field size.
Figure 2.12. Comparison for attenuation measurements between the CIVCO universal and CIVCO sample extensions for a 6MV beam, 10x10cm2 field.
By CT scanning the Universal CIVCO insert and the Sample CIVCO insert, the two CIVCO
products were reasonably modeled in the Varian Eclipse planning system. Once the planning
system had the CT scans uploaded and the Hounsfield units measured using eclipse tools, the
inclusion of the traced structures modeled attenuation values within approximately 2.4% of

32
the measured values for both inserts. The treatment planning system was then used to
produce Percent Depth Dose curves for both inserts under a 6MV beam with a 10x10 field
size, producing the results found in Figure 2.13.
The introduction of the Universal insert changed the surface dose from 52% of Dmax
to 85% of Dmax. The Sample insert changed the surface dose from 55% of Dmax to 68% of
Dmax, without any change in the depth at which maximum dose is delivered.
Figure 2.13. Eclipse modeled percent depth dose curves for the CIVCO universal and CIVCO sample extensions.

33
CHAPTER 3
DISCUSSION
Overall, the attenuation characteristics of the studied treatment couches followed the
expected trends of attenuation dependence. As the angle of incidence increases the beam path
through the treatment couch will also increase allowing the beam to interact for a longer
distance with the couch materials. This causes less of the beam to be transmitted through the
couch (inverse square law) and used for patient treatment. Our results also showed that the
treatment couches have a larger effect on the 6MV treatment beam rather than the 15MV
treatment beam, and greatest effects for smaller field sizes.
Of the studied couches, the EXACT couch was shown to have the highest attenuation,
19.2%, of the treatment beam, specifically during treatments intersecting the adjustable
support rail with a 5x5cm2 treatment field. Our measurement falls within the values
previously published values between 15 and 26.8%. The EXACT couch also produced the
most significant change in surface dose almost doubling the delivered dose to the surface of
the phantom.
As expected the IGRT couch affects the treatment the most at its widest section. This
section would generally be used during treatments conducted on the abdomen and pelvis of a
patient. As such, the interference of this section of the couch must be fully accounted for
because such cases are more likely to need to reach a larger depth of penetration before
delivering maximum dose. However if the interference of the couch into the beam causes the
beam to enter a patient with a higher initial dose, the beam may not have the desired dose
characteristics by the time it interacts with a tumor located deeper within a patient.
The differences between the two CIVCO extensions show a reduction in the overall
attenuation of the Sample extension compared to the Universal extension. The introduction
of the small immobile support rail under the couch top, however, makes it possible for this
newer construction to attenuate the beam more severely than original Universal extension
when treatment techniques utilize an oblique beam intersecting the support rail. The new
construction therefore is an improvement for treatments that would not need to utilize

34
multiple beams or gantry angles but for multi-field treatment techniques the support rail
would need to be avoided for even dose distribution or compensated for during treatment
planning.
During the Eclipse modeling of both CIVCO extensions, some data was missing near
the edge of the couch structures traced from the CT scans. This meant that for the 10x10 and
20x20 field size, the beam passed through sections of the couch, which were missing or
incomplete when taken from the contoured image for the 245° and higher gantry angles. Still,
the modeled delivered dose fell within 2.4% of the measured values. This variation is very
close to the expected difference of 2% predicted when using the techniques as described the
Mihaylov, et al. study.19
Based on the Eclipse modeling of the Percent Depth Dose curves of the CIVCO
Universal and Sample extensions, both couches have far less impact on the delivered surface
dose than the other studied couches. The Sample insert, specifically only increased the
surface dose by 13% of Dmax, which when compared to the 47% of Dmax increase produced
by the Varian EXACT couch, lends itself to the argument that the Sample CIVCO insert goes
a long way towards being less intrusive in treatment delivery.
The Eclipse treatment planning system calculated attenuations within a reasonable
2.4% range for the IGRT couch and CIVCO extensions. The 7% variation for the EXACT
couch planned dose predictions represents a significant difference between the planned
treatment dose and the actual measured dose at the point of reference. This difference has
already surpassed the ICRU suggested tolerance of 5% between delivered and prescribed
dose. Also, the differences in planned and delivered dose for all of the couches fell outside
the 2% tolerance, suggested by the ICRU 42. It is also noteworthy that the point at which the
treatment planning system differed the most from the measured values in every case was the
angle with the highest measured attenuation for each energy and field size combination.
All the treatment couches show a significant change in the surface dose delivered to
patients which could be detrimental for the ability of treatments to avoid external radiation
skin burns. Traditionally, higher energy beams are chosen for their ability to spare skin dose,
while still administering effective dose to target regions below the skin. The attenuation
caused by treatment couches can undermine this reasoning and practice since while a higher
energy beam should spare skin superficial skin tissue, if the couch attenuates the beam such

35
that it is already delivering 80 to 90% of its maximum delivered dose, the skin is no longer
spared a high radiation dose; therein defeating a major use of megavolt energy beams.
Furthermore, it should be noted that for some cases the interference of the treatment
couch in the beam, the depth at which the treatment dose delivered its maximum dose was
also reduced. In a clinical setting this could cause maximum dose to be delivered outside or
off set in the planned target volume, for small treatment volumes. This change in dmax lends
itself to the possibility of inefficient, if not ineffective treatment procedures. If the effect of
the treatment couch is not accounted for in treatment planning, patients may be required to
undergo more radiation in order for the same treatment efficiency produced through the
accounting for treatment couch interference in planning. The principles of ALARA require
that prescribers strive for efficiency and effectiveness without exposing patients to
unreasonable radiation.
Now while the treatment couch may not produce ‘unreasonable’ increases in the skin
dose exposure and severely alter the dose distribution through the treatment area, it is
possible that the couch could cause unnecessary changes in dose delivery. Future research
should be done to evaluate how a redefinition of density and Hounsfield units used in the
Eclipse treatment planning system could compensate for the differences between planned and
delivered dose. Data presented by Wagner and Vorwerk suggests that these changes could
perfect dose planning. At the very least, it should be recognized that multi-field treatment
techniques need to take treatment couch attenuations into consideration during the treatment-
planning period.
3.1 CONCLUSION Treatment of patients through a treatment couch or even a section of a treatment
couch can alter the dose received by that patient in a clinical setting. The largest effect the
treatment couch may occur in a clinical setting, may take the form of the increase in surface
dose when the beam intersects the treatment couch surface. In cases such as the Varian
EXACT couch this can approximately double the surface dose, relative to the maximum
delivered dose, on the skin of the patient and increase the risk of external negative reactions.
This interference by the treatment couch is most prevalent for lower treatment energies, when
using smaller field sizes.

36
REFERENCES
1E. N. Marieb, Essentials of Human Anatomy and Physiology, 9th ed. (Pearson Benjamin Cummings, San Francisco, CA, 2009).
2F. M. Kahn, The Physics of Radiation Therapy, 4th ed. (Lippincott Williams & Wilkins, Philadelphia, PA, 2010).
3United States Nuclear Regulatory Commission, “Standards For Protection Against Radiation.” Code of Federal Regulations Title 20, (2007).
4International Commission on Radiation Units and Measurements, “The Quality Factor in Radiation Protection”, ICRU Report 40 (1986).
5E. B. Podgorsak and J. H. Hendry, Radiation Oncology Physics: A Handbook for Teachers and Students (International Atomic Energy Association, Vienna, 2005).
6J. E. Turner, Atoms, Radiation, and Radiation Protection, 3rd ed. (Wiley-VCH, Berlin, Germany, 2007).
7United States Food and Drug Administration, Overview of Device Regulation (2009). <http://www.varian.com/us/oncology/treatments/treatment_techniques/IMRT/benefits.html>.
8E. M. Goldin, Radiation Biology (Montezuma Publishing, San Diego, 2008) p. 67. 9J. Bushberg, J. Seibert, E. Leidholdt Jr., and J. Boone, The Essential Physics of Diagnostic
Radiology, 4th ed. (Lippincott Williams and Wilkins, Philadelphia, 2001). 10L. Chao and W. Chou, Reviews for Accelerator Science and Technology: Medical
Aplications of Accelerators, Volume 2. (World Scientific Publishing Co., Singapore, Thailand, 2010).
11Varian Medical Systems, The Benefits of SmartBeam IMRT (2012). <http://www.varian.com/us/oncology/treatments/treatment_techniques/IMRT/benefits.html>.
12L. Marcu, E. Bezak, and B. Allen, Biomedical Physics in Radiotherapy for Cancer (Springer Science and Business Media B.V., New York, 2012).
13D. Jolly, D. Alahakone, and J. Meyer, "A rapidarc planning strategy for prostate with silumtaneous integrated boost" J. Appl. Clin. Med. Phys., 12 (1), 3320 ( 2009).
14Varian Medical Systems, Benefits of IGRT, (2012). <http://www.varian.com/us/oncology/treatments/treatment_techniques/IGRT/benefits.html>.
15K. Pulliam, R. Howell, D. Followill, D. Luo, R. White, and S. Kry, “The clinical impact of the couch top and rails on IMRT and arc therapy,” Phys. Med. Biol. 56, 7435 (2011).

37
16J. K. H. Seppala, and J. A. J. Kulmala, “Increased beam attenuation and surface dose by different couch inserts of treatment tables used in megavoltage radiotherapy,” J. Appl. Clin. Med. Phys. 12 (4), 15 (2011).
17D. Smith and, D. Christophides, “Dosimetric characterization of the iBEAM evo carbon fiber couch for radiotherapy,” J. Med. Phys. 37, 3595 (2010).
18L. H.Gerig, M. Niedbala, and, B. Nyiri, “Dose perturbations by two carbon fiber treatment couches and the ability of a commercial treatment planning system to predict these effects,” J. Med. Phys. 37, 322 (2010).
19I. B. Mihaylov, P.Corry, Y. Yan, V. Ratanatharathorn, and, E. G. Moros, “Modeling of carbon fiber couch attenuation properties with a commercial treatment planning system,” J. Med. Phys. 35, 4982 (2008).
20Z. Hu, J. Dai, L. Li, Y. Cao, and G. Fu, “Evaluating and modeling of photon beam attenuation by a standard treatment couch,” J. Appl. Clin. Med. Phys. 12 (4), 139 (2011).
21R. K. Munjal, P. S. Negi, A. G. Babu, S. N. Sinha, A. K. Anand, and, T. Kataria, “Impact of 6MV photon beam attenuation by carbon fiber couch and immobilization devices in IMRT planning and dose delivery,” J. Med. Phys. 31 (2), 67 (2006).
22D. Wagner and, H. Vorwerk, “Treatment couch modeling in the treatment planning sytem eclipse,” Int. J. Cancer. Sci Ther. 3, 7 (2011).
23S. Vieira, R Kaatee, M. Dirkx, and B. Heijmen, “Two dimensional measurement of photon beam attenuation by the treatment couch and immobilization devices using an electronic portal imaging device,” J. Med. Phys. 30 (11), 2981 (2003).
24H. Li, A. K. Lee, J. L. Johnson, R. X. Zhu, and R. J. Kudchadker, “Characterization of dose impact on IMRT and VMAT from couch attenuation for two varian couches,” J. Appl. Clin. Med. Phys. 12 (3), 23 (2011).
25M. Prooijen, T. Kanesalingam, M. K. Islam, and, R. K. Heaton, “Assessment and management of radiotherapy beam intersections with the treatment couch,” J. Med. Phys. 11 (2), 128 (2010).
26L. Court, J. Urribarri, and M. Makrigiorgos, “Carbon fiber couches and skin sparing,” J. Appl. Clin. Med. Phys. 11 (2), 220 (2010).
27Varian Medical Systems, EXACT Couch and Indexed Mobilization, (2012). <http://www.varian.com/us/oncology/radiation_oncology/trilogy/exact_couch.html>.
28Varian Medical Systems, EXACT IGRT Couch Overview (2012). <http://www.varian.com/us/oncology/radiation_oncology/trilogy/exact_igrt_couch.html>.





























