Embed Size (px)
Citation preview

The Effect of Constraint-Induced Movement Therapy on Upper Extremity Function and Unilateral Neglect in Person with Stroke
1Choi, Yoo-Im
1, First & corresponding Author Dept. of Occupational Therapy, College of Health & Welfare, Howon University, Rep. of Korea, [email protected]
Abstract
The purpose of this study was to investigate the effect of constraint–induced movement therapy (CIT) on upper extremity function and unilateral neglect in person with stroke. The subject was a man who was diagnosed with stroke. A single subject experimental research with ABA design was employed in this study. The experiment formed 20 sessions in total: 5 sessions for baseline, 10 sessions for CIT, and 5 sessions for the second baseline. CIT consisted of restraint of movement of the unaffected upper extremity by placing it in a sling and resting splint for 90% of waking time for 10 days combined with 6 hours/day of intensive training affected upper extremity. Upper extremity function was assessed using the Box and Block Test, and unilateral neglect was measured by Line Bisection Test and Baking Tray Task. The results showed that the tests score of upper extremity function and unilateral neglect were all improved. CIT was an effective method to reduce unilateral neglect and improve the affected upper extremity function in person with stroke.
Keywords: CIT, Stroke, Unilateral neglect, Upper extremity function
1. Introduction
Stroke is a major cause of death and disability globally [1]. After stroke, many patients experience
hemiplegia and upper extremity dysfunction [2][3]. Upper extremity dysfunction is one of the major factors that make it difficult for patients to perform activities of daily living (ADLs) and to return to society [4]. Therefore, intensive rehabilitation therapy for the treatment of upper extremity dysfunction is important.
Learned nonuse phenomenon has been reported as one of the causes of sustained upper extremity dysfunction [5][6]. After stroke, patients initially attempt to use their affected side however, since they inevitably experience repeated failure, they eventually stop using it. Although they may recover motor dysfunction on their affected side, they do not use it. This process in known as learned nonuse. Theses patients eventually use only the unaffected side and the function on the affected side worsens [7].
Constraint-induced movement therapy (CIT), the most commonly used method in clinical practice to reduce the learned nonuse phenomenon and treat upper extremity dysfunction, is characterized by short-term high-intensity training [8][9]. CIT increases the function and use of the affected upper extremity by restricting the unaffected upper extremity and inducing the affected upper extremity. CIT restricts the movement of the unaffected upper extremity during 90% of the patient’s waking period and treats the affected upper extremity intensively for 6h daily over a 2-week period. Meta-analysis studies on CIT have reported that it effectively improves upper extremity function in patient after stroke [8][9].
Unilateral neglect is another problem caused by stroke. Despite a proper sense of sensory and motor, patients with unilateral neglect cannot detect a stimulus applied to the opposite side of the damaged hemisphere or fail to respond appropriately to it [10]. Patients with unilateral neglect can experience severe body image damage and can struggle with ADLs and independent living [11]. Unilateral neglect is a negative predictor that can interfere with a patient’s rehabilitation [11], and its treatment is important.
Several methods for treating unilateral neglect intervention are being used. CIT treats both unilateral neglect and upper extremity dysfunction [12][13]. Because CIT trains patients to intensively use their affected side, the unilateral neglect can be improved by teaching them to recognize stimulation on affected side. van der Lee et al. [14] reported that patients with unilateral neglect showed reduced unilateral neglect as well as improved upper extremity function with the use of CIT and suggested that improved visual attention on the left side caused the improvement and further research is needed.
The Effect of Constraint-Induced Movement Therapy on Upper Extremity Function and Unilateral Neglect in Person with Stroke Choi Yoo-Im
Advances in information Sciences and Service Sciences(AISS) Volume5, Number15, October 2013
475

Although CIT has been reported to effectively improve upper extremity function and unilateral neglect, most studies have focused on upper extremity function and studies on unilateral neglect are few. This is because the symptoms of unilateral neglect are very diverse and subjective, making it difficult to conduct group experimental study. In the field of rehabilitation therapy, the single subject experimental research design has been used to establish the scientific foundation through the proper identification of treatment effects and verification of intervention effects.
In this study the single subject experimental research design is used to determine the effect of CIT on upper extremity function and unilateral neglect in patient with stroke.
2. Methods
2.1. Subject
The study subject selection criteria included diagnosis of stroke, onset for > 6 months, symptoms
of unilateral neglect, no cognitive impairment, no experience of CIT, and the ability to grasp and release an object using paretic hand. This subject of this study was a 53-year old male patient with left hemiplegia who had been diagnosed with stroke due to hemorrhage 11 months earlier. His cognitive function was considered normal since his Mini-Mental State Examination Korean Version (MMSE-K) result was 30. His Line Bisection Test (LBT) result was 49.0 mm, which indicated severe unilateral neglect.
2.2. Design
A single subject experimental research with ABA design was employed in this study. The study
period was August 27, 2012 to September 22, 2012 (4 weeks). The total number of experimental session was 20, including 5 times of a baseline process (A), 10 times of an intervention (CIT) process (B), and 5 times of a second baseline process (A).
2.3. Instruments
The MMSE-K is a reliable tool to evaluate person’s cognitive level in the rehabilitation field [15].
In this study, the MMSE-K was used to assess the subject’s cognitive function. The BBT is a standardized reliable tool to assess upper extremity ability and dexterity of the hand [16]. In this study, to measure affected upper extremity function, the number of blocks that the subject could pick up and move to the opposite side using paretic hand in 1 min was measured. The LBT is a reliable tool used to measure unilateral neglect by calculating errors in markings of the center of each line [17]. Lengths of the off-center regions of <6.3 mm, ≥6.3 mm, and ≥12.5 mm are considered normal, mild, and severe, respectively. The Baking Tray Task is a tool to check neglect by having the subject place 16 wood blocks on a wooden tray and checking whether the wood blocks are one-sided. Baking Tray Task is a functional test with little learning effect [18]. In this study, the number of wood blocks on the left side was measured.
2.4. Experiment 2.4.1. Baseline
During the baseline period, upper extremity function was measured using the Box and Block Test, and unilateral neglect was measured suing LBT and Baking Tray Task once daily without CIT (five times).
2.4.2. Intervention
In this study, CIT consisted of a constraint of movement of the unaffected upper extremity by
placing it in a sling and resting splint for 90% of waking time for 10 days, combined with 6 hours/day of intensive training the affected upper extremity. The intensive training included
The Effect of Constraint-Induced Movement Therapy on Upper Extremity Function and Unilateral Neglect in Person with Stroke Choi Yoo-Im
476
ROM exercise, muscular strengthening exercise, sensory stimulation, gross motor and fine motor training, functional activities, recreational activities, et al. All tasks were modified to make them suitable for the subject. Task difficulty increased progressively to match subject’s ability. If improvements in task performance were seen, verbal encouragement was provided. A 10-min break was provided after every 50 min of training. A checklist was followed to ensure that the subject used the affected upper extremity at home, which was verified by the researcher. During intervention period, upper extremity function and unilateral neglect after CIT were measured once daily. Thirty minutes after the end of CIT, the subject was evaluated (ten times).
2.4.3. Second baseline
During second baseline period, upper extremity function and unilateral neglect without CIT were measured once daily as in the baseline period. At the end of the training process, upper extremity function and unilateral neglect were measured once daily in the same manner as in the baseline process (five times).
2.5. Data analysis
In this study, the effect of CIT on upper extremity function and unilateral neglect was analyzed
using mean values and visual graphs.
3. Results
3.1. Affected upper extremity function
3.2.1. Box and Block Test
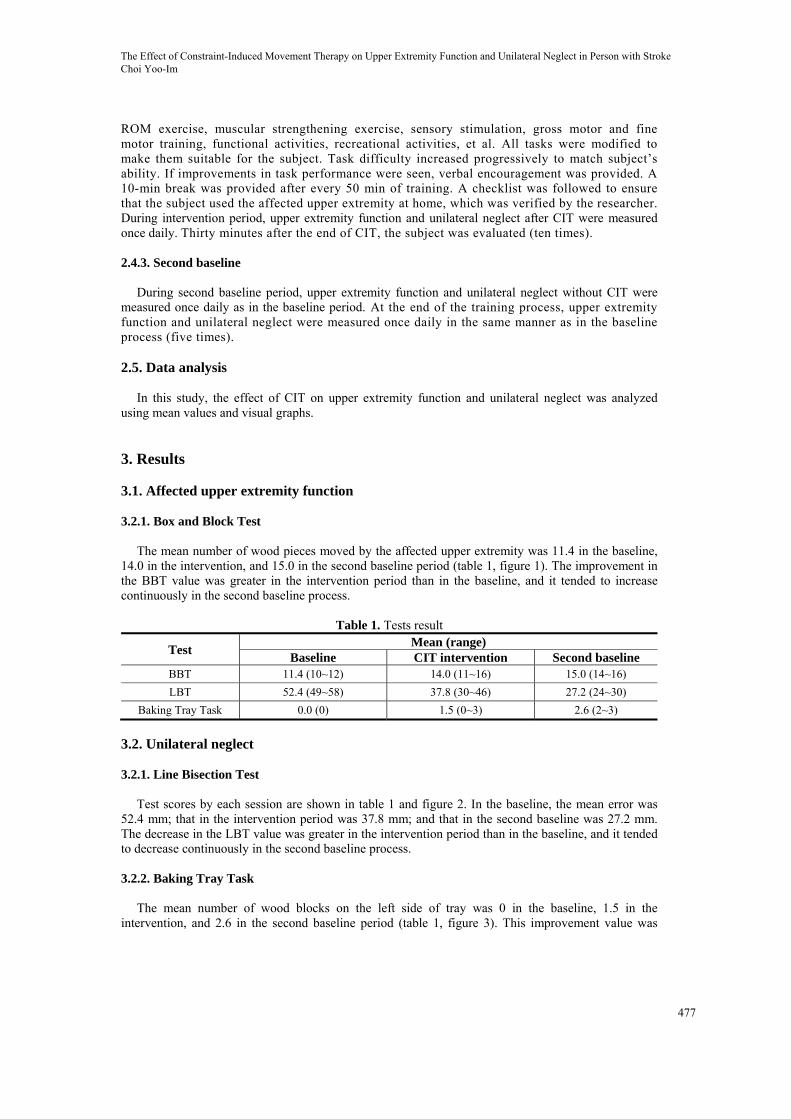
The mean number of wood pieces moved by the affected upper extremity was 11.4 in the baseline,
14.0 in the intervention, and 15.0 in the second baseline period (table 1, figure 1). The improvement in the BBT value was greater in the intervention period than in the baseline, and it tended to increase continuously in the second baseline process.
Table 1. Tests result
Test Mean (range)
Baseline CIT intervention Second baseline BBT 11.4 (10~12) 14.0 (11~16) 15.0 (14~16)
LBT 52.4 (49~58) 37.8 (30~46) 27.2 (24~30)
Baking Tray Task 0.0 (0) 1.5 (0~3) 2.6 (2~3)
3.2. Unilateral neglect
3.2.1. Line Bisection Test
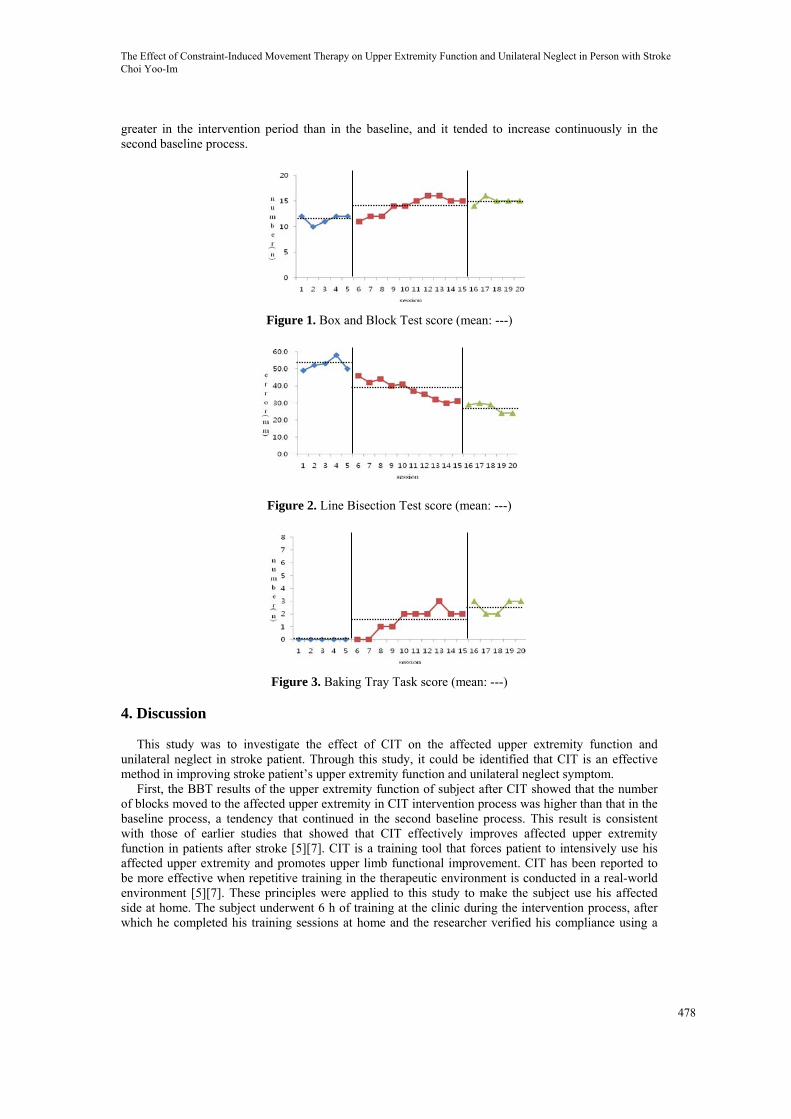
Test scores by each session are shown in table 1 and figure 2. In the baseline, the mean error was
52.4 mm; that in the intervention period was 37.8 mm; and that in the second baseline was 27.2 mm. The decrease in the LBT value was greater in the intervention period than in the baseline, and it tended to decrease continuously in the second baseline process.
3.2.2. Baking Tray Task
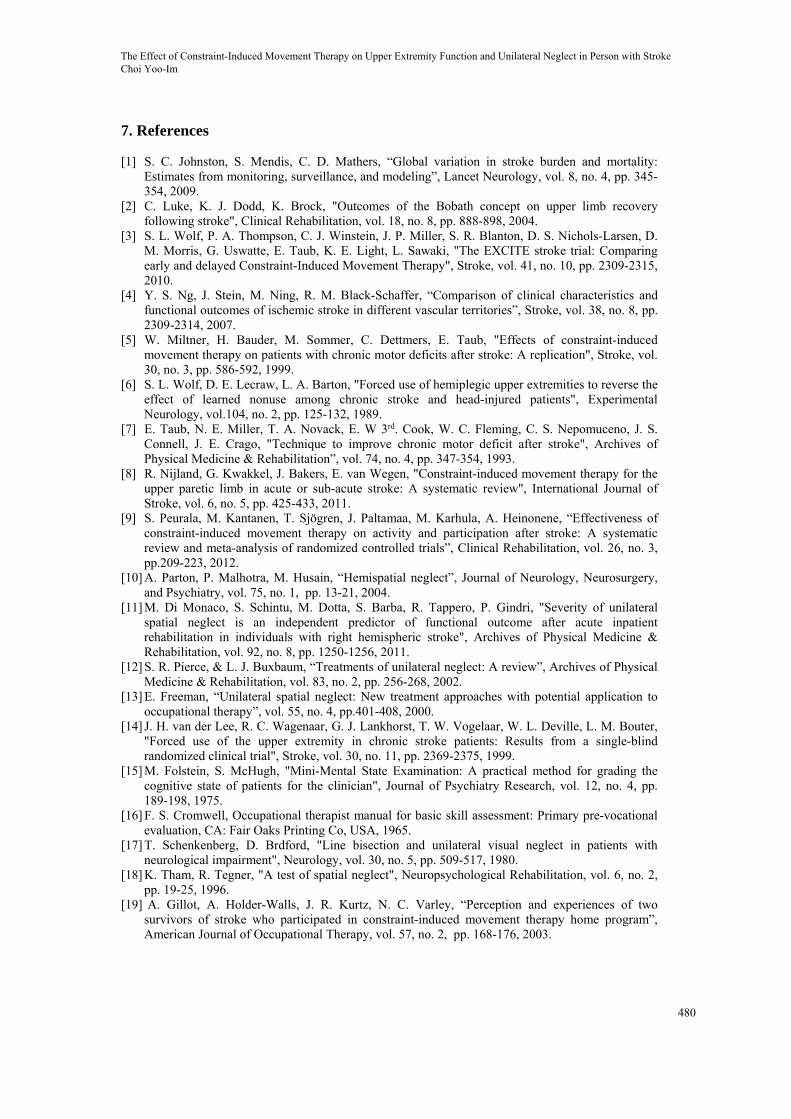
The mean number of wood blocks on the left side of tray was 0 in the baseline, 1.5 in the
intervention, and 2.6 in the second baseline period (table 1, figure 3). This improvement value was
The Effect of Constraint-Induced Movement Therapy on Upper Extremity Function and Unilateral Neglect in Person with Stroke Choi Yoo-Im
477
greater in the intervention period than in the baseline, and it tended to increase continuously in the second baseline process.
Figure 1. Box and Block Test score (mean: ---)
Figure 2. Line Bisection Test score (mean: ---)
Figure 3. Baking Tray Task score (mean: ---)
4. Discussion
This study was to investigate the effect of CIT on the affected upper extremity function and
unilateral neglect in stroke patient. Through this study, it could be identified that CIT is an effective method in improving stroke patient’s upper extremity function and unilateral neglect symptom.
First, the BBT results of the upper extremity function of subject after CIT showed that the number of blocks moved to the affected upper extremity in CIT intervention process was higher than that in the baseline process, a tendency that continued in the second baseline process. This result is consistent with those of earlier studies that showed that CIT effectively improves affected upper extremity function in patients after stroke [5][7]. CIT is a training tool that forces patient to intensively use his affected upper extremity and promotes upper limb functional improvement. CIT has been reported to be more effective when repetitive training in the therapeutic environment is conducted in a real-world environment [5][7]. These principles were applied to this study to make the subject use his affected side at home. The subject underwent 6 h of training at the clinic during the intervention process, after which he completed his training sessions at home and the researcher verified his compliance using a
The Effect of Constraint-Induced Movement Therapy on Upper Extremity Function and Unilateral Neglect in Person with Stroke Choi Yoo-Im
478

checklist every morning. Training of the affected side at home is thought to have improved the subject’ upper extremity functioning.
CIT is a therapy which can prevent pain and overuse syndrome that can be caused by excessively relying on unaffected side and bring positive changes to body image about affected side that has been negatively perceived by patients due to learned-nonuse phenomenon [19]. In this study, the subject had almost no perception that they should use the left side of his body. However, after using the affected side intensively and practicing a lot the exercises for the affected part, the perception about his left body has been improved, and the patient got motivation to use his left upper limb. Maybe it is owing to positive change of perception about using the affected upper extremity resulting from decrease of learned-nonuse phenomenon.
The results of unilateral neglect of the subject after CIT showed severe unilateral neglect in the baseline process that decreased during the intervention process and tended to continue decreasing in the second baseline process. The LBT is useful for determining the unilateral neglect in activities such as reading and writing, whereas the Baking Tray Task is useful for determining the spatial neglect. Therefore, both tests were used. Because of unilateral neglect, the subject could not read the left figures, ignored the left space in activities such as reading and writing, and could make few spontaneous movements using his affected upper extremity. However, as the intervention progressed, his attempts to use the affected side and awareness to look to the left side increased. Use of CIT increased awareness on the left side and increased the sensory stimulation of the affected side. As such, unilateral neglect in the subject was thought to be reduced.
It is reported that active movements of the affected extremity, especially in the affected hemispace, can decrease unilateral neglect [20]. In CIT program in this study, there were different activities to cause the subject use the affected upper extremity in the affected hemispace. It seems that those activities contributed to decreasing unilateral neglect by stimulating the affected cerebral hemispheres. Therefore, it may be helpful to apply CIT to the patients who have active movements in affected upper extremity among the patients with unilateral neglect for decreasing neglect as well as improvement of upper extremity function.
This study has its limit that it is easy to see individuals’ changes, but there is no control group, because it used the study method of single-subject experimental research design. So the number of the subjects was small. Therefore, further studies would need to prove effect of CIT to a lot of stroke patients.
5. Conclusion The purpose of this study was to investigate the effect of CIT on upper extremity function and
unilateral neglect in person with stroke. The subject was a man who was diagnosed with stroke. A single subject experimental research with ABA design was employed in this study. The experiment formed 20 sessions in total: 5 sessions for baseline, 10 sessions for CIT, and 5 sessions for the second baseline. The CIT consisted of a restraint of movement of the unaffected upper extremity by a sling and resting splint for 90% of waking time, combined with 6 hours/day of intensive training of the affected upper extremity. The upper extremity function was assessed using the Box and Block Test and unilateral neglect was measured by Line Bisection Test and the Baking Tray task. The study results are as follow: the mean number of wood pieces moved by the affected upper extremity was 11.4 in the baseline, 14.0 in the intervention, and 15.0 in the second baseline period. And in Line Bisection Test (unilateral neglect test), in the baseline, the mean error was 52.4 mm; that in the intervention period was 37.8 mm; and that in the second baseline was 27.2 mm. In Baking Tray Task, the mean number of wood blocks on the left side of tray was 0 in the baseline, 1.5 in the intervention, and 2.6 in the second baseline period. These tests results indicated that CIT was an effective method to improve the affected UE function and reduce unilateral neglect in person with stroke.
6. Acknowledgement
This study was carried out with the financial support of the University of Howon.
The Effect of Constraint-Induced Movement Therapy on Upper Extremity Function and Unilateral Neglect in Person with Stroke Choi Yoo-Im
479
7. References
[1] S. C. Johnston, S. Mendis, C. D. Mathers, “Global variation in stroke burden and mortality: Estimates from monitoring, surveillance, and modeling”, Lancet Neurology, vol. 8, no. 4, pp. 345-354, 2009.
[2] C. Luke, K. J. Dodd, K. Brock, "Outcomes of the Bobath concept on upper limb recovery following stroke", Clinical Rehabilitation, vol. 18, no. 8, pp. 888-898, 2004.
[3] S. L. Wolf, P. A. Thompson, C. J. Winstein, J. P. Miller, S. R. Blanton, D. S. Nichols-Larsen, D. M. Morris, G. Uswatte, E. Taub, K. E. Light, L. Sawaki, "The EXCITE stroke trial: Comparing early and delayed Constraint-Induced Movement Therapy", Stroke, vol. 41, no. 10, pp. 2309-2315, 2010.
[4] Y. S. Ng, J. Stein, M. Ning, R. M. Black-Schaffer, “Comparison of clinical characteristics and functional outcomes of ischemic stroke in different vascular territories”, Stroke, vol. 38, no. 8, pp. 2309-2314, 2007.
[5] W. Miltner, H. Bauder, M. Sommer, C. Dettmers, E. Taub, "Effects of constraint-induced movement therapy on patients with chronic motor deficits after stroke: A replication", Stroke, vol. 30, no. 3, pp. 586-592, 1999.
[6] S. L. Wolf, D. E. Lecraw, L. A. Barton, "Forced use of hemiplegic upper extremities to reverse the effect of learned nonuse among chronic stroke and head-injured patients", Experimental Neurology, vol.104, no. 2, pp. 125-132, 1989.
[7] E. Taub, N. E. Miller, T. A. Novack, E. W 3rd. Cook, W. C. Fleming, C. S. Nepomuceno, J. S. Connell, J. E. Crago, "Technique to improve chronic motor deficit after stroke", Archives of Physical Medicine & Rehabilitation”, vol. 74, no. 4, pp. 347-354, 1993.
[8] R. Nijland, G. Kwakkel, J. Bakers, E. van Wegen, "Constraint-induced movement therapy for the upper paretic limb in acute or sub-acute stroke: A systematic review", International Journal of Stroke, vol. 6, no. 5, pp. 425-433, 2011.
[9] S. Peurala, M. Kantanen, T. Sjögren, J. Paltamaa, M. Karhula, A. Heinonene, “Effectiveness of constraint-induced movement therapy on activity and participation after stroke: A systematic review and meta-analysis of randomized controlled trials”, Clinical Rehabilitation, vol. 26, no. 3, pp.209-223, 2012.
[10] A. Parton, P. Malhotra, M. Husain, “Hemispatial neglect”, Journal of Neurology, Neurosurgery, and Psychiatry, vol. 75, no. 1, pp. 13-21, 2004.
[11] M. Di Monaco, S. Schintu, M. Dotta, S. Barba, R. Tappero, P. Gindri, "Severity of unilateral spatial neglect is an independent predictor of functional outcome after acute inpatient rehabilitation in individuals with right hemispheric stroke", Archives of Physical Medicine & Rehabilitation, vol. 92, no. 8, pp. 1250-1256, 2011.
[12] S. R. Pierce, & L. J. Buxbaum, “Treatments of unilateral neglect: A review”, Archives of Physical Medicine & Rehabilitation, vol. 83, no. 2, pp. 256-268, 2002.
[13] E. Freeman, “Unilateral spatial neglect: New treatment approaches with potential application to occupational therapy”, vol. 55, no. 4, pp.401-408, 2000.
[14] J. H. van der Lee, R. C. Wagenaar, G. J. Lankhorst, T. W. Vogelaar, W. L. Deville, L. M. Bouter, "Forced use of the upper extremity in chronic stroke patients: Results from a single-blind randomized clinical trial", Stroke, vol. 30, no. 11, pp. 2369-2375, 1999.
[15] M. Folstein, S. McHugh, "Mini-Mental State Examination: A practical method for grading the cognitive state of patients for the clinician", Journal of Psychiatry Research, vol. 12, no. 4, pp. 189-198, 1975.
[16] F. S. Cromwell, Occupational therapist manual for basic skill assessment: Primary pre-vocational evaluation, CA: Fair Oaks Printing Co, USA, 1965.
[17] T. Schenkenberg, D. Brdford, "Line bisection and unilateral visual neglect in patients with neurological impairment", Neurology, vol. 30, no. 5, pp. 509-517, 1980.
[18] K. Tham, R. Tegner, "A test of spatial neglect", Neuropsychological Rehabilitation, vol. 6, no. 2, pp. 19-25, 1996.
[19] A. Gillot, A. Holder-Walls, J. R. Kurtz, N. C. Varley, “Perception and experiences of two survivors of stroke who participated in constraint-induced movement therapy home program”, American Journal of Occupational Therapy, vol. 57, no. 2, pp. 168-176, 2003.
The Effect of Constraint-Induced Movement Therapy on Upper Extremity Function and Unilateral Neglect in Person with Stroke Choi Yoo-Im
480

[20] I. H. Robertson, N. North, “Active and passive activation of left limbs: Influence on visual and sensory neglect”, Neuropsychologia, vol. 31, no. 3, pp. 293-300, 1993.
The Effect of Constraint-Induced Movement Therapy on Upper Extremity Function and Unilateral Neglect in Person with Stroke Choi Yoo-Im
481





























