Embed Size (px)
Citation preview

427
THE DIAGNOSIS OF VARICOSE VEINSBy HAROLD DODD, Ch.M., F.R.C.S.
Surgeon to King George Hospital, Ilford; The Royal Hospital, Richmond; Assistant Surgeon to Thte LondonHomeopathic Hospital
The treatment of varicose veins has de-veloped until, when the correct remedy isselected for each presentation it has becomecurative. This article aims to sketch thediagnosis of this ubiquitous condition whichcauses a degree of incapacitation and sufferinggenerally unrealized. It is an interestingclinical exercise and leads to effective treat-ment satisfying alike to patient and doctor.Ochsner and Mahorner, Varicose Veins, p.7,say ' . . . the use of appropriate diagnostic testspermits the formulation of a rational therapy.'
Other ailments causing pain in the legsFirst it must be recalled that there are other
causes of discomfort in the legs besides varicoseveins; for such ailments are often attributed tovaricosities when they are present. There maybe complaints of weight, weakness, weariness,burning, swelling, bursting sensations, cold-nessl, early tiredness, excessive perspiration,itching, eczema or incapacitating pain. Thesesymptoms are associated also with flat feet,neuritis, fibrositis and joint lesions of the feet,ankles and knee or hips. Patients whosepostures are bad, whose habits are slack (e.g.,housewives working in soft slippers) and thosein whom unnecessary joint and muscle strainabout the pelvis, knees and feet occur are alsotroubled, as are the constitutionally debilitatedand fatigued. Dead teeth are a source ofvariable and persistent pain, which is some-times referred to the lower limbs. Pain in thelegs may follow the resumption of duty aftertonsillitis, a quinsy or toxic condition, fromloss of muscle tone.
Obliterative arteriosclerosis -(in men mostlyand occasionally women), and a failing heart
will cause early tiredness and weakness in thelower limbs, as well as a previous white leg.Some of these factors may be concurrent withvaricose veins and when they are recognizedand treated the results are further enhanced.
It has been claimed by American writersthat tonsillar sepsis is an aetiological factor invaricose veins, and since testing this theory,my experience is that the tonsils, especiallyremnants, merit critical inspection in cases ofvaricose veins without apparent cause, suchas pregnancy or an inherited tendency.
Compensatory or Varicose veins?Another question is, ' Are the enlarged veins
truly varicose, or are they distended vessels,compensatory to obliterated main deep veinsor to the pressure on the iliac veins by anabdominal tumour such as a pregnant uterus,an impacted ovarian cyst or fibroid ?'The deep veins accompanying the arteries of
the lower limb are usually patent, but they areblocked occasionally as, after the white leg ofpregnancy, typhoid, a compound infectedfracture of the tibia, fibula or femur, septicperitonitis, etc. In these circumstances theirfunction is transferred in part to the superficialveins and gradually these enlarge and look likevaricose veins. Attempts to obliterate super-ficial compensatory vessels, as if they werevaricosities is a disservice to patients. For-tunately, injections of sclerosing fluids usually'fail, the circulation in them is *too brisk toallow time for effective scarifying of the endo-thelium and the pain from the resultingchemical phlebitis is so great as to dissuadepatients from further treatment.
The Diagnosis of Compensatory Veins.-
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

428 POST GRADUATE MEDICAL JOURNAL September I947
Compensatory veins can be detected by signsand tests. The previous history of white leg,phlebitis, etc., is important and should alwaysbe taken. A limb so affected, including thefoot is coolish, heavy with non-pitting oedema,white with scaly eczema, possibly ulcerated.It has an unshapely or ' elephant' leg outline,and is soon fatigued, aches and is weak. Theveins may be visible or if not obvious, feel likesoft elastic gutters under the skin.A dependable although not completely
certain test for blocked deep veins is asfollowsA tourniquet is applied to the middle of the
thigh, tight enough to occlude the superficialveins. The person is requested to walk roundhe Out-patient Hall. If the deep veins are notfunctioning, blood can only escape by thesuperficial venous conduits, and as these arecompressed by the touniquet the limb becomesdusky and the vessels tense. The patientshortly suffers great pain and urgently requeststo be released from the constricting band. Bycontrast, if the deep vessels are patent, the testcauses no difficulty or discomfort and the con-clusion is made that the enlarged superficialveins are truly varicose. The tourniquet mustnot be tight enough to occlude the deep veinsand should be reasonably padded, otherwisethe pain of the constriction will affect theresults of the trial. The final certain test isto expose the femoral vein at the groin and seeif it is patent.
Varicose VeinsA varicose vein is one whose elasticity is
lost, and as a result it has become dilated,elongated, tortuous, pouched, friable, and itsvalves incompetent. From this dilation andpossibly from defects congenital or acquiredin the valves themselves, the terminal valveguarding the union of the internal saphenousvein with the femoral vein and less often of theexternal saphenous vein with the poplitealvein, ultimately become inefficient and bloodregurgitates into them from the trunk veins, ina retrograde circulation away from the heart.The varying pressures in the main venoussystem is exerted on these superficial veinssetting up a vicious circle increasing the dis-tension and vascular stagnation and converting
the subcutaneous venous system of the legsinto a cul-de-sac of the main venous system.Another source allowing a back-flow to the
surface vessels is in the communicating veinswhich connect them to the deep veins-theirvalves also may become defective. There areseveral such connections in the thigh and leg,especially in the lower third of each. They arenot conspicuous as causes of the varicosity norso frequent, as incompetent long or shortsaphenous veins.
The Diagnosis and Evaluation of VaricoseVeins.-Varicose veins which are incurable byinjection but are curable by the operation ofligature and injection are denoted by a positiveTrendelenberg test and in the more advancedcases, by the presence in them when thepatient coughs or strains of an impulse. Inadvanced cases a thrill is palpable. Both testsneed some experience to assess.
The Exposure of the Patient.-To diagnosevaricose veins the patient must be undressed toabove the groins. A good light is essential.Frequent errors are made through insufficientexposures and shadows cast by clothes.Associated conditions like herniae, hydroceles,abdominaI tumours and intertrigo are dis-covered. A partial diagnosis leads to irritatingfailures or qualified successes in treatment. Anexplanation for this unexpected amount of dis-robing is given to patients.
The Cough Impulse.-The cough impulse isa less delicate but easier test than the Trendel-enberg. A hand is placed on the enlargedveins in the leg or thigh, the patient turns theface to the ceiling and is asked to coughvigorously. Nothing, grading up to a just per-ceptible impulse, to an expansile impulse and athrill may be felt. The impulse is felt best atthe termination of the internal saphenous veinin the groin. The landmark for this is where aline starting from the pubic spine intersects thecrease of the groin at right angles. ('The pubicspine is found by tracing the pubic crestoutwards.) Sometimes a varix is seen here oran enlarged vein can be felt in the thinnishsubject and occasionally enlarged saphenousglands when there is varicose eczema or ulcers.A possible error in the cough impulse test is
to mistake for an expansile impulse, the slightjerk in the leg when some patients cough. The
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

.September I947 DODD: Diagnosis of Varicose Veins 429
cough impulse is a coarser test than the Trendel-enberg sign, and when it is present, then opera-tion is needed to cure these vessels, no injec-tion is of permanent use. Less often a coughimpulse is present over the external saphenousvein in the popliteal space, so denoting its in-competence and also its ligature and injectionto cure.
The Trendelenberg and Tourniquet Tests.The findings are accurate and significant.Trendelenberg's name is given to the singletourniquet test, but two bands at varying levelsare also necessary.The patient undressed to the umbilicus, lies
on a couch. The affected limb is raised andthe veins are stroked from the ankle to thegroin to empty them completely. This step isdone thoroughly to obtain clear-cut results.A tourniquet is applied moderately tight roundthe upper thigh, and the patient stands, in awell-lighted position. An assistant removes theband (taking care not to cast a shadow) whilstthe surgeon -watches the prominent vessels,which if necessary are marked out. The veinsmay slowly re-appear so that it is difficult tosay whether the filling is from above or below,this would be regarded as a negative result, ora vigorous down-filling wave or cascade maypromptly distend the vein which is a positiveresponse. Repetition is often necessary for aclear result. Veins normally fill imperceptiblyfrom below and any degree of obvious fillingfrom above indicates incompetent valves andback pressure in the internal saphenous vein.An additional step to decide if the varicositiesfill from above is to place another band belowthem, therefore they can only fill from abovewhen the upper constriction is released.Should they fail to distend then clearly the testis negative.
Sometimes the thickness of the skin and fatmakes observations uncertain. A possiblealternative then is by palpation, and the fingersare placed lightly on the prominent vessels (theveins having been emptied, the tourniquetapplied and the patient standing). When theconstriction is released the vessels can, inmature varicosities, be felt to distend under thefingers from above downwards, the fillingappears in a variable period after the band isundone, sometimes surprisingly long, i.e.
several seconds. The test is applied also -to theexternal saphenous vein with a slight modifica-tion. An estimation of the pressure of thedistension in the vein is also made by palpationand is most helpful when the visual result isdoubtful.
The Efficiency of the External SaphenousVein.-The competence or otherwise of theexternal saphenous vein is determined by theuse of two constricting bands.
First filling from the saphena magna must beexcluded, this is done by raising the leg ver-tically, emptying the veins, and placing aclipping garter at the lower third of the thigh.Another band is placed round the leg im-mediately below the crease behind the knee,this prevents blood flowing backwards througha possibly defective short saphenous vein (thisvessel joins the popliteal vein about the centreof the back of the knee, its last two inches orso lies under the deep fascia and it is thereforenot visible and possibly not palpable). Thepatient stands and the lower tourniquet isreleased. If there is a downward filling it canonly have come by the blood leaking past anineffective valve at the termination of the ex-ternal saphenous vein. In this case ligatureand injection of this vessel is needed.
Difficulty may arise when the varicosities areonly in the leg and not in the leg and thigh.Do they fill from the groin or from thepopliteal space ? Differentiation is asfollows:-The veins are emptied, the uppertourniquet is applied below the groin, thepatient stands and the veins are watched. Theymay fill steadily suggesting that they have filledfrom the external saphenous vein or possiblyfrom the communicating veins between thedeep and superficial venous systems. Bothpossibilities are rare. Differentiation betweenthese two will be mentioned shortly.
If the veins remain comparatively empty, theupper band is released and the probable fillingfrom above observed thus declaring the defectin the long saphenous vein, easily the com-monest finding.On the other hand, the result may be doubt-
ful in which event the leg is again raised, theveins emptied and an upper band, appliedabove the knee while the end of the externalsaphenous vein is controlled by the fingers of
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

430 POST GRADUATE MEDICAL JOURNAL September I947
the surgeon pressing on the end of the smallsaphenous vein in the middle of the poplitealspace. The patient then stands and the bandholding the long saphenous is released and thevessels watched. If they fill with a down-filling wave, the long saphenous vein isvaricose because the external saphenous veinis controlled by the diagnostician's fingers.By contrast when the test is repeated and
the band is released if nothing happens in thevaricosities the internal saphenous vein isefficient, but if on releasing the fingers, thevaricosities fill, then this is clear proof of thesmall saphenous vein being inefficient.When the test is done as above and a wave is
not seen then palpation of the varicositiesduring and after release of the band or fingerswill sometimes confirm that they have becometense indicating filling from above. Perhapsno clear observation may be forthcoming andif tests have been carefully done then con-sideration of defective communicating veinsarises.
Indefinite Findings.-Occasionally, when theconstrictions are still in place, and the personstands the veins appear filled, but on palpatingthem there is no pressure in them, they arebut slightly filled, possibly from incompleteemptying, a too tight or too loose constrictionor from slightly defective communicatingveins. Repetition of the tests may be necessarythree or four times before the results are clearenough to articulate a diagnosis.
It may be apposite here to mention thevariability of veins and that their anatomicalsituation is of qualified significance as to wherethe defect is. For instance, vessels on theinside of the leg can be filled by an inefficientshort saphenous vein and those on the outsideof the calf and ankle from the internal saphen-ous defects whilst those in the lower two-thirds of the thigh may be filled from the backand upward pressure from a faulty externalsaphenous vein below. Even a defective com-municating vein will distend veins for anappreciable amnount above it. An open mindand systematic and repeated testing of thepossibilities leads to correct diagnosis.
Incompetent Communicating Veins.-Incom-petence of the valves in the communicatingveins connecting the deep and superficial
venous systems is a third primary diagnosis;they are situated mainly in the lower third ofthe thigh and leg.
In testing for communicating vein failure,the tourniquet is applied as before, first in theupper thigh and later at various lower levels.When the patient stands it is kept on and thevaricosities are watched for 30 seconds, duringwhich the veins will refill in some amount fromslight to tense distension. Veins normally fillfrom below, but it takes longer than 30 secondsfor healthy ones to fill to distension and it isalmost imperceptible. When the communi-cating veins allow an outward and downwardflow then filling of the subcutaneous vari-cosities is prompt and the back pressure issurprisingly high, easily within half a minute.The filling occurs mainly downwards but canalso be upwards. Again, some experienceassists in the interpretation of the results andmany patients must be examined to find clearcut examples. In my experience, it is muchless common than internal saphenous failure.Ochsner and Mahorner describe a test
whereby applying two tourniquets and varyingthe levels and space between them, andwatching the sections of the limb between thebands, e.g., the thigh, upper and lower partsand also below the knee, it is possible to locatewith precision the part of the legs where thecommunicating veins are defective, becausewhere defects are, the affected vessels afteremptying and constricting bands appliedabove and below them, they fill up within 30seconds on standing. In the lower third of theleg the defective communicating vein can oftenbe palpated with the tip of the finger, it feelslike a button-hole in the deep fascia. Whenoedema is present, this may be the only way tolocate them. In some instances, there is abulb-like distension or ' blow-out ' of thesuperficial vein immediately at the defectivecommunicating vessels. In the extreme caseblood can be felt running through a faultycommunicating vein like water from a tap;this is just as the constricting band is released.Three primary diagnoses have now been
described, i.e., incompetence of the internalsaphenous, external saphenous, and com-municating veins. Combinations of thesethree may occur and these will now bedescribed.
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

September Ig47 DODD: Diagnosis of Varicose Veins 43'
The Diagnosis of Simultaneous Incompetenceof the Internal and External Saphenous Veins.The diagnosis of simultaneous incompetenceof the internal and external saphenous veinshas already been hinted at. The limb is raisedand the varices are emptied. Two tourniquetsare applied, one below the groin and the otherbelow the knee. The two main superficialvenous groups are thereby controlled. Thepatient stands up and the upper tourniquet isremoved. The external saphenous vein beingheld, therefore, if the varices in the thigh fillfrom above, they must do so from the internalsaphenous vein. The test is repeated with theupper band at the lower third of the thigh andthe second at the crease of the knee. Theperson stands and the lower grip is released, adown filling wave incriminates the shortsaphenous branch. If the veins are only in theleg, then the varices are emptied again, the endof the external saphenous vein is controlled bythe surgeon's fingers pressing in the middle ofthe popliteal space, whilst the saphena magnais held by an upper thigh band. The patientstands, the latter is released. If the leg varicesdilate from above, the internal saphenous veinis defective.The observations vary from being clear-cut
to doubtful and they may require repetition toclinch the diagnosis. I find that there is somedegree of internal saphenous fault in nearly allshort saphenous deficiencies.
Simultaneous Incompetence of the ExternalSaphenous Vein and Communicating Veins.This is detected by carrying out the appro-priate tests with one or two constrictions asdescribed for the individual veins. Thesevarices are mainly in the leg, but are somewhatunexpectedly occasionally in the lower third ofthe thigh. The efficiency of the internalsaphenous is first ensured.The tests for the short saphena vein and the
communicating veins are performed. Oneresult may be more positive than another.
Simultaneous Incompetence of the InternalSaphenous and Communicating Veins.-This isdeclaredly doing the appropriate tests andfinding them negative for the externalsaphenous vein and positive for the internalsaphenous and communicating veins.
Simultaneous Incompetence of the Com-
municating Veins and of the Internal and -Ex-ternal Saphenous Vessels.-This rare diagnosisis found by applying the two touniquets aboveand below the knee and seeing the varicositiesdistend within 30 seconds. This proves thefault in the communicating veins. Furtherpalpation of the prominent veins will generallyreveal the button-holes in the deep fascia andfrequently the bulbous veins immediately closeto them. This is more difficult in fat patients.The tests described in the previous para-
graphs for simultaneous incompetence of theinternal and external saphenous veins arecarried out. They are performed carefully andquickly so that the results are not obscured bythe communicating vein failure. The coughimpulse over the terminations of the major andminor veins when present is certain evidenceof their failure in function.
DiscussionThe diagnosis of the type of veins may re-
quire 5-I5 minutes observation and possibly asecond session. Occasionally incompetence ofthe internal saphenous system will be found inone leg and of the external saphenous systemin the other. Less often, the internal andexternal saphenous system are incompetent inthe same leg.
Effective treatment depends on the truediagnosis, for the operation is but an elemen-tary surgical exercise requiring meticulousattention to asepsis and detail.There are seven basic diagnoses of varicose
veins made up of combinations of lesions of theintemal and external saphenous and of thecommunicating veins. All require operationvaried according to the type and degree ofdevelopment. The diagnoses are varicosityand incompetence of the valves controlling:
I. The Internal Saphenous Vein.2. The External Saphenous Vein.3. The Internal and External Saphenous
Veins together.4. The Communicating Veins in the thigh
or leg or both.5. The Internal Saphenous Vein and Faulty
Communicating Veins together.6. The External Saphenous and Defective
Communicating Veins.
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

432 POST GRADUATE MEDICAL JOURNAL September 1947
7. The Great and Small Saphenous Veinsplus leaky Communicating Veins.
There are lesser groups of varicose veins notfulfilling these conditions, found either in theleg or thigh; these will respond to injection.
Upper Thigh and Buttock Varicosities.Other varices develop in the upper andpostero-internal parts of the thigh.They arise from the gluteal and pudenal
veins. They are infrequent and part of ex-tensive varicosities affecting the whole limb.They are amenable to injection treatment afterthe kev conditions have been recognized anddealt with.
Pudendal and Superficial Epigastric Veins.-The pudic and superficial epigastric veins inparticular should be recalled as possible com-pensatory pathways when thie external iliacvein is blocked. They should not be injected.They raise alsb critical evaluation of the vari-cose veins in the leg.
The Abdomen.-Surgeons who handle num-bers of patients with varicose veins will find,once or twice a year, an abdominal tumour,particularly in women. Therefore this pos-sibility is kept in mind. An eye and a handexamines the abdomen, thereby fibroids,ovarian cysts, unsuspected pregnancies and adistended bladder are occasionally found.
Constitutional Disease.-Further sensitive-ness to the general health of the patient isessential for other constitutional diseases havebeen found with varicose veins and ulcers,such as pernicious anaemia, diabetes andsyphilis. Particularly in the case of varicoseeczema and ulcer. Phlebitis migrans willsuggest a septic focus somewhere and occasion-ally thrombo-angitis obliterans even in women.An ulcer unassociated with varicose veins mayvery rarely be a manifestation of acholuricfamilial jaundice or lymphatic leukaemia.Further in the aged obliterative arteritis is apossibility to be considered and can be quicklyexcluded by palpating the dorsalis pedis. arteryand feeling the temperature of the foot. Acalcified artery is revealed by an X-ray.
Varicose Veins recurrinlg afteroperationThese are a fairly common occurrence and
they depend on the operation performed. Theywere frequent after all the operations exceptafter the modern procedure of ligature of themain trunk and of all their associated branchesand introduction of an adequate amount of anefficient sclerosing agent. Even after thisradical procedure all the veins may not besclerosed if the agent has not reached theoffending vessels, they do, however, readilyrespond to injection.Again varicose veins may persist after even
the modern operation when the completediagnosis has not been made; e.g., incom-petence of the external saphenous or com-municating veins may have been overlooked.(The plan I follow is that of making a systematicdiagnosis as described here, and to treat thecondition accordingly. Almost invariably theyfall into one of the seven types.)
Pregnancy and Varicose Veins.-Pregnancy isoften associated with the appearance of varicoseveins, generally these' should be' treatedradically after parturition.
Conception often considerably aggravatesalready established varicosities; these can thenwith advantage be treated according to thediagnosis by injection or operation. I do theoperation up to seven months.Age and Varicose Veins.-Age is no bar to
radical cure of varicose veins for many patientsover 70 and one over 8o have been operated on.They are diagnosed as already described andtreated appropriately. Particular care to ex-clude arterial and constitutional disease isnecessary..
ConclusionThe types and diagnoses of varicose veins
are detailed with particular reference to thoserequiring treatment by operation. There'areseven possibilities and these make the diagnosisattractive but essential, leading to permanentlyeffective treatment.
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

September I947 DODD: Diagnosis of Varicose Veins 433
£ :
i ..4 .
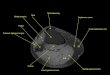
FIG. I.-NORMAL VENOUS ANATOMY OF LEGS
Note the communicating veitis between the great andsmall saphenous veins; there is usually one above and
below the knee.Note especially that the last 2 in. of the externalsaphenous vein is under the deep fascia also the upward
running branches from the end of this vein.(a) Superficial epigastric veins (usually 3).(b) External iliac vein.(c) Internal or (great) saphenous vein (saphena magna).(d) Communicating veins between the internal and ex-
ternal saphena veins in thigh and leg.(e) Commuricating veins between the superficial venous
system (internal and external saphenous veins) andthe deep return vessels (femoral, anterior andposterior tibial). (Cotinud at foot
(f) Anterior tibial vena comites, of next colvmn)
... ...,..
uElL
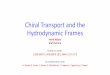
FIG. 2.-COMPENSATORY VEINS due to thrombosed ex-ternal iliac vein (f) with compensatory enlargement ofthe internal saphenous vein. These might be mistakenfor varicose veins. The tortuous veins (a) on the lowerabdomen (if the patient is sufficiertly undressed) willrai3e the surgeon's suspicion of the possibility. Thebars (i) indicate competent valves at the terminations
of the intemal and external saphenous veins.
(g) Common femoral vein(h) Popliteal vein.(i) A fairly constant upward branch given off from the
end of the short saphenous vein. This mustalways be tied in the operation on. the externalsaphenous vein.
(j) Posterior tibial vein(k) Extemal saphenous vein.
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

434 POST GRADUATE MEDICAL JOURNAL September I947
alStg
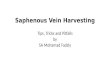
FIG. 3.-COMPENSATORY VEINS (c) due to a thrombosedcommon femoral vein (g). The history, the tourniquetand walking tests differentiate from varicose veins.
v....
.'." .
FIG. 4.-Thrombosis of the anterior and posteriortibial venae comites (f and j). It may occur after acompound fracture of the tibia and fibula. Com-
pensatory superficial veins of the leg (c) and (k).
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

September I947 DODD: Diagnosis of Varicose Veins 435
.....................
ser~~~~~~~.,.
.........
........j'... ... ..j.;';.'.. ....... ... ... .................~~~~~~~~~~~~~....|;~~ ~ ~ ~ ~..,;S^',............ml | S
.....:-i2. --
........o; & .. E 1 , , l
...~~...,.:.'.".:\....~~.
... .. .. ... .. ..
'~~~ '' ..: ..' .: ..'
...
-.- ......;s. ...;.-. ..... ;.. .... . / . .,.o .............:j,h ~~~~. .. ... .. G..............C.-....-; j.o;-.... ...,.. .;.--........:.w..................
:- -.-.:.: .~~~~~.....
FIG. 5.-Varicosity of the internal (great or saphenamagna) saphenous vein (c) with an incompetent valve(i.v.) at its termination, notice the open or incompetent
valve (i.v.) in the groin.
FIG. 6.-Varicosty of the external (or small) saphenousvein (j), the valve (i.v.) at its termination, in the popliteal
space is inefficient.Note the varicose veins in the lower thigh which un-
expectedly may arise from this defect.
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

436 POST GRADUATE MEDICAL JOURNAL September 1947
X.k.:.|.. s ^n ; &
|.'.:::a.:.....::
B1.,...............,C,
°~.-.
................
............. ,
:.
... ..-...A ,.,ff .'a'e
..... .......... ... .....
FIG. 7.-Varicosity of the internal and externalsaphenous combined both of their terminal valves (i.v.)
have failed.
.. .. ..........
FIG. 8.-Varicosity and incompetence of the communi-cating veins between the superficial and deep venous
s5 stems in the thigh and leg.
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

September I947 DODD: Diagnosis of Varicose Veins 437
FIG. 9.-Varicosity and incompetence of the communi-cating veins between the superficial and deep venouissystems in the thigh and leg confined to the com-
municating veins in the thigh.
..-......
....
FIG. IO.-Varicosity and incompetence of the com-municating veins between the superficial and deepvenous systems in the thigh and leg confined to the
communicating veins in the leg.
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

POST GRADUATE MEDICAL: JOURNAL September 1947
..I.
...
Fic. I I.-Varicosity of the internal saphenous veins andcommunicating veins combined. Note the open valve
(i.v.) et the groin.
.:..:-...- :i'.Z-:.;.
..~~~~~~~~~~~~~~. ...>;;<.....
:............': S0 ...... ...... ........
FIG. I2.-Varicosity of the external saphenous vein andcommunicating veiris in the leg.
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

September 1947 DODD: Diagnosis of Varicose Veins 439
LL^-| -- ---- - ---- - --
-S Pi
- U | -- 6 s -- Z Z -- g |I- S SE
R | |- 9- N |- { { || | || E | || | i || | | | |- fig | | | |- | | | |- R2 g eE al
R N E E |iS- IS R R R- a9ffi-Iffl | | S E- S | R R- | | g |- E | |
2 i i |I - S- ri- B FxC fi | E.- -s a a^ ^XS 11! E
X I E I !
1! i E |n.... f11 I::..:
FIG. 13.-Varicosity of the internal and externalsaphenous and communicating veins combined.
w.MI S
FIG. I4.-A further stage than Fig. 13 is when there arevaricose branches from the pedenal and gluteal veins.
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from

POST GRADUATE MEDICAL JOURNAL September I947
*.:L.-.
Patient aged 44 years suffering from Simmonds' disease.Note normal nutrition and absence of axillary and pubic hair.
Protected by copyright.
on June 9, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.263.427 on 1 Septem
ber 1947. Dow
nloaded from