Embed Size (px)
Citation preview

The Clinical Significance of HLA antibodies
detected by Solid Phase Assay in Renal
Transplant Recipients
Samantha Jane Fidler
MSc (Med), BSc (Hons)
A thesis submitted for the degree of PhD
2016
School of Pathology and Laboratory Medicine

2
Statement of candidate Contribution
All work was performed by the author unless otherwise stated in the
thesis
Samantha Fidler
Student
Lloyd D’Orsogna
Coordinating Supervisor
Ashley Irish
Supervisor

3
The data presented in Chapter 3 has been published. The bibliographic
details and percentage contribution of each author to the work are set out
below.
Fidler SJ, Irish AB, Lim W, Ferrari P, Witt C, Christiansen FT. Pre-transplant
donor specific anti-HLA antibody is associated with antibody-mediated
rejection, progressive graft dysfunction and patient death. Transplant Immunology 2013; 28(4): 148-153
Author contribution:
Fidler S J (80%)
Irish AB (10%)
Lim W (2%)
Ferrari P (2%)
Witt C (4%)
Christiansen FT (2%)
Lloyd D’Orsogna
Coordinating Supervisor

4
The data presented in Chapter 4 has been published. The bibliographic
details and percentage contribution of each author to the work are set out
below.
Fidler S, Swaminathan R, Lim W, Ferrari P, Witt C, Christiansen FT,
D’Orsogna L, Irish AB. Peri-operative third party red blood cell transfusion in
renal transplantation and the risk of antibody-mediated rejection and graft
loss. Transplant Immunology 2013; 29: 22-27
Author contribution:
Fidler S J (75%)
Swaminathan R (2%)
Lim W (2%)
Ferrari P (2%)
Witt C (2%)
Christiansen FT (2%)
D’Orsogna L (2%)
Irish AB (13%)
Lloyd D’Orsogna
Coordinating Supervisor

5
The data presented in Chapter 5 has been published. The bibliographic
details and percentage contribution of each author to the work are set out
below.
Ferrari, P., Fidler, S., Wright, J., Woodroffe, C., Slater, P., Van Althuis-
Jones, A., Holdsworth, R., Christiansen, F.T. Virtual Crossmatch Approach to Maximise Matching in Paired Kidney Donation. American Journal of Transplantation 2011: 11; 272-278
Author contribution:
Ferrari P (40%)
Fidler S J (40%)
Wright J (10%)
Woodroffe C (1%)
Slater P (2%)
Van Althuis-Jones A (2%)
Holdsworth R (2%)
Christiansen FT (3%)
Lloyd D’Orsogna
Coordinating Supervisor

6
The data presented in Chapter 6 has been published. The bibliographic
details and percentage contribution of each author to the work are set out
below.
Ferrari P, Fidler S, Holdsworth R, Woodroffe C, Tassone G, Watson N,
Cantwell L, Bennett G, Thornton A, Christiansen FT, D’Orsogna L. High transplant rates of highly sensitized recipients with virtual crossmatching in kidney paired donation. Transplantation 2012; 94: 744-749
Author contribution:
Ferrari P (40%)
Fidler S J (45%)
Holdsworth R (1%)
Woodroffe C (1%)
Tassone G (1%)
Watson N (2%)
Cantwell L (2%)
Bennett G (2%)
Thornton A (2%)
Christiansen FT (1%)
D’Orsogna L (1%)
Lloyd D’Orsogna
Coordinating Supervisor

7
The data presented in Chapter 7 has been published. The bibliographic
details and percentage contribution of each author to the work are set out
below.
Böhmig G, Fidler S, Christiansen FT, Fischer G, Ferrari P. Transnational
validation of the Australian algorithm for virtual crossmatch allocation in kidney paired donation. Human Immunology 2013; 74: 500-505
Author contribution:
Böhmig G (15%)
Fidler S J (55%)
Christiansen FT (10%)
Fischer G (10%)
Ferrari P (10%)
Lloyd D’Orsogna
Coordinating Supervisor

8
I Contents
i Contents..........................................................................................8
ii List of Tables..................................................................................13
iii List of Figures................................................................................16
iv Summary......................................................................................19
v Thesis overview..............................................................................20
vi Dedication....................................................................................22
vii Acknowledgments.........................................................................23
viii Abbreviations...............................................................................24
ix Publications...................................................................................26
1 Chapter 1 Literature Review...................................................27
1.1 The Human Leukocyte Antigen (HLA) system...............................28
1.1.1 HLA haplotypes and linkage disequilibrium..........................30
1.1.2 Expression of HLA...........................................................31
1.1.3 HLA polymorphism..........................................................31
1.2 Antigen presentation................................................................32
1.2.1 Endogenous antigen presentation......................................32
1.2.2 Exogenous antigen presentation........................................33
1.2.3 The MHC and allorecognition in renal transplantation...........34
1.2.4 Direct allorecognition.......................................................34
1.2.5 Indirect allorecognition....................................................35
1.3 The significance of HLA in transplantation....................................36
1.4 Humoral and cellular mechanisms of rejection..............................37
1.4.1 Hyperacute rejection........................................................37
1.4.2 Acute cellular rejection.....................................................38
1.4.3 Acute humoral rejection...................................................38

9
1.4.4 Chronic rejection.............................................................39
1.5 Production of antibody by B cells................................................39
1.5.1 T cell independent B cell activation....................................39
1.5.2 T cell dependent B cell activation.......................................40
1.6 Pre-transplant crossmatching and detection of HLA antibodies.......41
1.6.1 Crossmatching strategies.................................................41
1.6.2 HLA antibody detection by ELISA.......................................44
1.6.3 HLA antibody detection by Luminex bead assay...................46
1.7 Post-transplant HLA antibodies...................................................48
1.8 Therapies for the treatment of antibody mediated rejection............49
1.9 Allograft accommodation...........................................................51
1.10 Strategies for transplanting the sensitised patient.........................52
1.10.1 Desensitisation...............................................................52
1.10.2 Acceptable mismatch program..........................................53
1.10.3 Paired Kidney Exchange...................................................53
1.11 Aims of this thesis....................................................................56
2 Chapter 2 Materials and Methods...................................57
2.1 HLA antigen typing (HLA-A, -B, -C, -DRB1, -DR345, -DQB1, -DPB1)
by Sanger sequencing...............................................................58
2.1.1 DNA extraction...............................................................58
2.1.2 DNA quantitation using the Nanodrop spectrophotometer....58
2.1.3 PCR amplification of target DNA........................................58
2.1.4 Agarose gel electrophoresis..............................................59
2.1.5 Purification of PCR products for sequencing.........................60
2.1.6 Sequencing of PCR amplified template...............................61
2.1.7 Purification and concentration of Big Dye Terminator
sequencing products using ethanol precipitation..................62
2.1.8 Electrophoresis of sequencing products on 3730
sequencer......................................................................64
2.2 LABType® SSO for HLA-DQA1 typing...........................................65

10
2.2.1 DNA amplification............................................................65
2.2.2 Agarose gel electrophoresis..............................................66
2.2.3 Denaturation / neutralisation............................................66
2.2.4 Hybridisation..................................................................67
2.2.5 Labelling........................................................................68
2.2.6 Data analysis – OneLambda HLA Fusion™...........................68
2.3 Serological HLA typing..............................................................70
2.3.1 Isolation of T and B lymphocytes.......................................70
2.3.2 HLA antigen typing using commercial typing trays...............70
2.4 Crossmatching by complement-dependent lymphocytotoxicity
(CDC).....................................................................................71
2.4.1 Standard (NIH) CDC crossmatch.......................................71
2.4.2 Interpretation of standard crossmatch results.....................71
2.4.3 DTT crossmatch..............................................................72
2.4.4 Interpretation of DTT crossmatch results............................72
2.5 Luminex antibody testing..........................................................73
2.5.1 Characterisation of antibodies by Single Antigen bead
assay............................................................................73
2.5.2 Data analysis – OneLambda HLA Fusion™...........................74
2.6 Statistical analysis....................................................................75
3 Chapter 3 Pre-transplant donor specific anti-HLA antibody is
associated with antibody-mediated rejection,
progressive graft dysfunction and patient
death…………………………………………………………………..76
Fidler SJ, Irish AB, Lim W, Ferrari P, Witt C,
Christiansen FT. Transplant Immunology 2013;
28(4): 148-153

11
4 Chapter 4 Peri-operative third party red blood cell
transfusion in renal transplantation and the risk of
antibody-mediated rejection and graft
loss……………………………………………………………………..98
Fidler S, Swaminathan R, Lim W, Ferrari P, Witt C,
Christiansen FT, D’Orsogna L, Irish AB. Transplant
Immunology 2013; 29: 22-27
5 Chapter 5 Virtual crossmatch approach to maximise
matching in paired kidney donation................118
Ferrari, P., Fidler, S., Wright, J., Woodroffe, C., Slater, P., Van Althuis-Jones, A., Holdsworth, R.,
Christiansen, F.T. American Journal of Transplantation 2011: 11; 272-278
6 Chapter 6 High transplant rates of highly sensitized
recipients with virtual crossmatching in kidney
paired donation...........................................137
Ferrari P, Fidler S, Holdsworth R, Woodroffe C,
Tassone G, Watson N, Cantwell L, Bennett G, Thornton A, Christiansen FT, D’Orsogna L.
Transplantation 2012; 94: 744-749
7 Chapter 7 Transnational validation of the Australian
algorithm for virtual crossmatch allocation in
kidney paired donation.................................159
Böhmig G, Fidler S, Christiansen FT, Fischer G, Ferrari P. Human Immunology 2013; 74: 500-505

12
8 Chapter 8 Discussion and conclusions...........................176
8.1 The significance of preformed anti-HLA antibodies detected by
Luminex bead assay...............................................................177
8.2 Peri-operative blood transfusion is associated with AMR and renal
allograft loss..........................................................................180
8.3 Virtual crossmatching to facilitate transplantation......................181
8.4 Further research.....................................................................182
8.4.1 Post-transplant antibody testing......................................182
8.4.2 Rejection in the absence of HLA antibodies......................182
8.4.3 HLA DSA in the absence of rejection.................................183
8.4.4 Characterisation of HLA epitopes in kidney
transplantation..............................................................183
8.4.5 HLA specific B cells........................................................184
8.4.6 Complement-fixing HLA specific antibodies.......................185
8.5 Conclusions...........................................................................187
9 References.................................................................................188
10 Appendix...................................................................................210

13
ii List of Tables
Chapter 1
Table 1. A summary of studies investigating the association of graft
outcome with pre-transplant class I and II antibodies detected
by ELISA .......................................................................45
Table 2. A summary of studies investigating the association of graft
outcome with pre-transplant class I and II antibodies detected
by Luminex bead assay....................................................47
Table 3. A summary of studies investigating the association of graft
outcome with post-transplant class I and II antibodies detected
by Luminex bead assay....................................................49
Chapter 2
Table 1. PCR mastermix volumes per sample..................................59
Table 2. Expected number of PCR products and respective sizes for each
locus.............................................................................60
Table 3. Sequencing primers provided for use with each locus...........62
Table 4. 3730 instrument settings for HLA sequencing......................64
Table 5. PCR amplification mix volumes..........................................65
Table 6. Post-PCR reagent volumes................................................67
Table 7. SAPE volume requirements per sample..............................68
Chapter 3
Table 1. Demographic and clinical features at the time of transplant
according to entry antibody status.....................................84
Table 2. Longitudinal mixed-effects models of predictors of eGFR
(coefficient and 95% CI = mls/min) across the observed
follow-up (median 68 months) incorporating factors identified
as univariate predictors of eGFR........................................90

14
Chapter 4
Table 1. Demographic and clinical features at time of transplant by
entry HLA-antibody........................................................105
Table 2. Patient demographics, HLA antibody, rejection and outcomes
by transfusion status......................................................106
Table 3. Univariate and multivariate adjusted Cox Proportional Hazards
models for the effect of Delayed Graft Function (DGF), entry
HLA antibody, Antibody and Non-Antibody Mediated Rejection
(AMR and Non-AMR) and Transfusion status on death censored
and combined patient and graft loss.................................106
Chapter 5
Table 1. ABO blood group of donors and recipients in the Western
Australian paired kidney donation program.......................125
Table 2. Comparison of 3 test runs using different antibody resolution
and strength to excluded recipients with antibodies from
matching to donors in a pool of 32 incompatible donor-
recipient pairs...............................................................127
Table 3. Match results by blood type excluding recipients with donor
specific antibody at >2000 mean fluorescence intensity
(OneLambda) and using high-resolution antibody
definition......................................................................129
Chapter 6
Table 1. Match run conditions for the quarterly match runs of the
Australian KPD program.................................................142
Table 2. ABO blood group distribution of donors and recipients in the 4
initial match runs of the AKX program for KPD...................143
Table 3. Aggregated results of 149 CDC allogeneic crossmatches
performed between 37 matched donors and matched or
unmatched recipients, whose sera were available for
testing.........................................................................146

15
Chapter 7
Table 1. Baseline characteristics of donors and recipients in the 16 pairs
of the Vienna transplant center.......................................164
Table 2. CDC and flow cytometry crossmatch results from 112 donor-
recipient pair combinations where crossmatch data were
available in relation to the presence or absence of any donor-
specific antibodies (DSA) at >2000MFI.............................165
Table 3. Sensitivity and specificity of donor-specific antibody (DSA)
positive computer matching to predict a positive crossmatch
and negative predictive value of DSA negative matching to
identify crossmatch negative results using virtual
crossmatching in kidney paired donation...........................167
Chapter 8
Table 1. Summary of studies investigating the clinical significance of
HLA antibodies detected pre-transplant by Luminex bead
assay...........................................................................178
Table 2. Summary of studies investigating the clinical significance of
complement-fixing DSA..................................................186
Appendix
Table 1. Conexio Genomics HLA Sequencing Based Typing kit
details..........................................................................211

16
iii List of figures
Chapter 1
Figure 1. The human MHC map......................................................29
Figure 2. Structure of the HLA class I and II molecules......................30
Figure 3. Growth of the IMGT / HLA database...................................32
Figure 4. Exogenous and endogenous antigen processing...................34
Figure 5. Direct and indirect allorecognition......................................35
Figure 6. Death censored graft survival rates in relation to the number of
HLA-A, -B and –DR mismatches in two eras – 1985-1994 and
1995-2004.....................................................................36
Figure 7. Number of rejection episodes in the first year of transplant in
patients with a functioning graft at 1 year..........................37
Figure 8. Simplified representation of donor antigen recognition and the
induction of humoral immune response - T cell-independent
and T cell-dependent B cell activation................................41
Figure 9. A schematic representation of antibody mediated rejection
pathophysiology..............................................................51
Figure 10. Paired kidney exchange – simple two-way exchange...........54
Figure 11. Paired kidney exchange – non-directed donor chain.............55
Chapter 3
Figure 1. a. Time to first biopsy proven acute rejection (BPAR) excluding
24 patients with AMR by entry DSA....................................85
b. Time to antibody mediated rejection by entry DSA
status............................................................................86

17
c. Time to antibody mediated rejection by class of DSA at
entry.............................................................................86
Figure 2. a. Strength of antibody determined by the MFI of the highest
bead in the 37 patients with DSA according to rejection
category (no BPAR, non-AMR and AMR)..............................87
b. Time to AMR by category of the MFI of the highest DSA bead
compared with No-Antibody..............................................88
Figure 3. a. Time to patient or graft loss by entry DSA.......................89
b. Time to patient or graft loss by entry class of DSA...........89
Figure 4. Longitudinal mixed model of mean observed eGFR by entry
DSA status over time.......................................................91
Chapter 4
Figure 1. Kaplan-Meier plot of the time to AMR by transfusion status in
all patients...................................................................107
Figure 2. a. Time to Antibody Mediated Rejection (AMR) by antibody
status at the time of transplant in the combined 195 patients
receiving no-RBCT, Pre-RCBT and Post-RCBT....................108
b. Time to Antibody Mediated Rejection (AMR) by antibody
status at the time of transplant in the 65 patients with Pre +
Post-RBCT....................................................................108
Figure 3. Time to death censored graft loss by transfusion status.....110

18
Chapter 5
Figure 1. Matching diagram of test run 3 using 32 pairs, where donors
were excluded from matching to recipients with moderate and
strong (>2000 MFI) donor-specific antibodies defined at the 4-
digit level.....................................................................128
Chapter 6
Figure 1. Match probability by cPRA (-A, -B, -DR and –DQ) in 27
crossmatch-negative matched recipients among 53 registered
patients.......................................................................144
Figure 2. Pattern of cPRA (-A, -B, -DR, and –DQ) in 53 registered
recipients and in 20 recipients who underwent
transplantation..............................................................145
Figure 3. DSA strength and specificity in crossmatch–positive assays
from 112 crossmatches performed on unmatched panel
recipients in match runs 1 and 2 against available donor
cells.............................................................................147
Chapter 7
Figure 1. Probability of a positive crossmatch in relation to the
cumulative strength of donor-specific antibodies (DSA) in mean
fluorescence intensity (MFI) for class I and class II
DSA.............................................................................168
Chapter 8

19
Figure 1. Transplant activity by calculated panel reactive antibody
(cPRA) cohort...............................................................181
iv Summary
For patients with end stage renal failure there are only two options for renal replacement
therapy: dialysis and transplantation. Complications such as anaemia, hypertension and
infection along with the patient’s own co-morbidities contribute to the relatively short life
expectancy for dialysis patients of around seven years. Kidney transplantation remains the
treatment of choice, and can extend life expectancy by an additional five to ten years when
compared to staying on dialysis. One of the major immunological hurdles in transplantation is
the presence of pre-formed antibodies in the recipient directed against donor HLA antigens.
Whilst current immunosuppressive regimens have improved graft outcomes, the presence of
donor specific anti-HLA antibodies is associated with allograft rejection and poor long term
graft outcome. In recent years, the detection techniques for anti-HLA antibodies has evolved
from the relatively insensitive lymphocytotoxic crossmatch to the introduction of more
sensitive solid phase assays including ELISA and Luminex bead assays.
In this thesis I investigate the clinical significance of anti-HLA antibodies detected by Luminex
single antigen bead assay on renal transplant outcome.

20
v Thesis overview
Chapter 1 is a review of the human leukocyte antigen (HLA) system. It describes the role of
HLA in renal graft rejection and reviews pre-transplant crossmatching and detection of anti-
HLA antibodies and their role in transplant outcome. It also describes the protocols available
for transplanting highly sensitised kidney patients.
Chapter 2 describes the materials and methods used to perform the studies in this thesis. In
addition to HLA typing, crossmatching and Luminex antibody assays, the methods for statistical
testing performed in data analysis are recorded in this chapter.
The study described in chapter 3 investigates the clinical significance of pre-transplant HLA
antibodies detected by Luminex single antigen bead assay in the presence of a negative
lymphocytotoxic crossmatch on renal transplant outcome. The results confirm that pre-
transplant antibodies directed against donor HLA are associated with antibody mediated
rejection (AMR) and poor graft outcome in our cohort.
In chapter 4 we report the novel finding that the risk of AMR in patients with pre-transplant
donor specific HLA antibodies is greatly increased by peri-operative blood transfusion. Peri-
operative blood transfusion also increases the risk of graft loss in this group.
Chapter 5 describes the design of a paired kidney exchange program in which donors were
excluded from matching to recipients with donor specific antibodies detected by single antigen
bead assay. Modelling of the program using two different antibody cut-offs by mean
fluorescence intensity (MFI) was performed. In the simulation, using a conservative MFI cut-off
of 2000 resulted in greater than 50% of pairs having a match with a predicted negative
crossmatch (virtual crossmatch) whilst reducing the risk of AMR and poor long term graft
function.
In chapter 6 we review the first year of the Australian kidney exchange program. There were
concerns that using a conservative antibody assignment to avoid breakdown of identified
matches could potentially disadvantage sensitised patients by excluding crossmatch
compatible donors. However, we were able to demonstrate that 35% of the patients
transplanted in the first year of the program were highly sensitised.

21
In chapter 7 we were able to show using independent donor / recipient pair data from Austria
that virtual crossmatching in the Australian paired kidney exchange program reliably predicted
negative crossmatches with a sensitivity of 98.6% and specificity of 69.2%. Furthermore, the
number of compatible crossmatches which were not matched with the Australian criteria was
around 10%. Adjusting antibody cut-offs for highly sensitised patients may facilitate
transplantation in individuals who are extremely difficult to match.
Chapter 8 summarises the key findings of the studies reported in Chapters 3 to 7 and their
significance in context of contemporary studies. Further areas for additional research is also
addressed.
References are cited in chapter 9.

22
vi Dedication
This thesis is dedicated to two people who have influenced my life. Firstly, my late grandfather,
Flight Lieutenant Richard Colbourne. Secondly, my late friend and colleague, Linda Karen
Smith. I miss you both.

23
vii Acknowledgments
There are many people to thank who have helped and supported me during my studies.
Firstly I would like to thank my colleagues in the Nephrology departments of Fiona Stanley,
Royal Perth and Sir Charles Gairdner hospitals. A special thanks to Dr Ashley Irish, Dr Wai Lim,
Dr Suda Swaminathan and CNS Anne Warger who have given me much encouragement and
moral support.
Many thanks to all my collaborators, a special mention to the staff of the Australian Tissue
Typing laboratories in Brisbane, Sydney, Melbourne and Adelaide for all our useful discussions.
Thankyou to the patients without whose permission studies such as these would not be
possible.
I would like to thank the staff, past and present, of the Department of Clinical Immunology for
all their help along the way. In particular I would like to thank Alana Chin, Brittany King, Mary
Despot, Gabriella Tassone and Jacqueline Dey.
Finally, to my family, thankyou for all the support. It seems to have taken forever to get here.

24
viii Abbreviations
ADCC Antibody Dependent Cell Cytotoxicity
AKX Australian Kidney Exchange
AMR Antibody Mediated Rejection
APC Antigen presenting cell
BPAR Biopsy Proven Acute Rejection
Β2m Beta2 microglobulin
BXM B cell crossmatch
CAN Chronic Allograft Nephropathy
CLIP Class II-associated Ii peptide
CREG Cross-Reactive epitope group
CTLs Cytotoxic T lymphocytes
DGF Delayed graft function
DSA Donor Specific Antibody
DTH Delayed typed hypersensitivity
DTT Dithiothreitol
ELISA Enzyme-Linked ImmunoSorbant Assay
ER Endoplasmic reticulum
ERAPs ER amino peptidases
FITC Fluorescein Isothiocyanate
HIFCS McCoys 5A tissue Culture Medium + 5% Heat
inactivated Foetal Calf Serum
HLA Human Leukocyte Antigen
HR Hazard Ratio
HRP Horseradish Peroxidase
IFN-γ Interferon-gamma

25
Ig Immunoglobulin
IL Interleukin
IM Infectious Mononucleosis
IMGT International Immunogenetics information system
IVIG Intravenous immunoglobulin
KPD Kidney Paired Donation
LD Linkage Disequilibrium
MFI Mean Fluorescence Intensity
MHC Major Histocompatibility Complex
MIC MHC-Class I Related gene
NOMS National Organ Matching System
PBS Phosphate Buffered saline
PKE Paired Kidney Exchange
PRA Panel reactive antibody
PTC Peritubullar Capillary
PTLD Post Transplant Lymphoproliferative disorder
SAPE Streptavidin Phycoerythrin
TAP Transporter associated with antigen presentation
TCR T cell receptor
TG Transplant glomerulopathy
Th T helper
TMB Tetramethyl-benzidine
TNF Tumour necrosis factor
TXM T cell crossmatch
UNOS United Network Organ Sharing
XM Crossmatch

26
ix Publications
Publications completed during my candidature but not presented in this
thesis
Smith LK and Fidler S. HLA typing technologies. Chapter 10 in The HLA Complex in Biology and
Medicine – A resource book, pages 175-187. Ed N Mehra. Jaypee Brothers Medical Publishers
Ltd, New Delhi, India ISBN 978-81-8448-870-8 (2010)
D Trajanoski, SJ Fidler. HLA Typing Using Bead Based Methods. Chapter 4 in: Immunogenetics –
Methods and Applications in Clinical Practice. Ed: FT Christiansen, BD Tait. Humana Press (part
of the Springer publishing group), New York, USA.
G Tassone, S Fidler. Separation and Cryopreservation of Lymphocytes from Spleen and Lymph
Node. Chapter 20 in: Immunogenetics – Methods and Applications in Clinical Practice. Ed: FT
Christiansen, BD Tait. Humana Press (part of the Springer publishing group), New York, USA.
S Fidler. Crossmatching by Complement-Dependent Lymphocytotoxicity (CDC). Chapter 21 in:
Immunogenetics – Methods and Applications in Clinical Practice. Ed: FT Christiansen, BD Tait.
Humana Press (part of the Springer publishing group), New York, USA.
Ferrari, P., Fidler, S., Woodroffe, C., Tassone, G., D'Orsogna, L.J. Comparison of time on the
deceased donor kidney waitlist versus time on the kidney paired donation registry in the
Australian program. Transplant International 2012: 25; 1026-1031
Ferrari P, Hughes P, Cohney S, Woodroffe C, Fidler S, D’Orsogna L. ABO-incompatible matching
significantly enhances transplantation rates in Kidney Paired donation. Transplantation 2013;
96 (9): 821-826
Do Nguyen H, Wong G, Howard K, Claas F, Craig J, Fidler S, D’Orsogna L, Chapman J, Irish A,
Ferrari P, Christiansen F, Lim W. Modeling the benefits and costs of integrating an acceptable
HLA mismatch allocation model for highly sensitized patients. Transplantation 2014; 97 (7):
769-774)

27
Chapter 1. Literature Review

28
This literature review will cover literature published prior to the commencement
of this thesis (2008). Literature published after this time will be discussed in the
relevant chapters and in the final discussion chapter.
1.1 The Human Leukocyte Antigen (HLA) system
The genes of the HLA system are located within the Major Histocompatibility Complex
(MHC) on the short arm of chromosome 6. There are over 400 genes in the human MHC
region (Figure 1)1.
The class I region contains the classical HLA-A, -B and –C genes that encode the heavy
chains (α chain) of class I molecules. The α chain is associated with β2-microglobulin
encoded on chromosome 15. The α-chain consists of two peptide binding domains, an
immunoglobulin-like domain and a transmembrane region with a cytoplasmic tail (Figure
2).
The class II region consists of a series of subregions each containing A and B genes
encoding the α and β chains respectively. The α and β-chains consist of a peptide binding
domain, an immunoglobulin-like domain and a transmembrane region with a cytoplasmic
tail (Figure 2).
The class III region does not encode HLA molecules but does contain other
immunomodulatory genes such as Complement components and Tumour Necrosis Factor
(TNF)2.

29
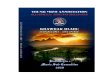
Figure 1. The human MHC map. The MHC is divided into class I, class III and class II subregions
from telomere to centromere. The white boxes denote expressed genes. The black, striped
and grey boxes show pseudogenes, non-coding genes and gene candidates respectively.
From: T Shiina et al. Journal of Human Genetics 2009; 54: 15-391

30
Figure 2. Structure of the HLA class I and II molecules.
From: http://what-when-how.com/acp-medicine/adaptiveimmunity
1.1.1 HLA haplotypes and Linkage Disequilibrium
The HLA genes are closely linked on chromosome 6 and the pattern of inheritance is
determined by Mendelian genetics. HLA alleles are not in random recombination
because of the genes close proximity on the chromosome, a phenomenon known as
linkage disequilibrium3,4. HLA-B and –C alleles are in linkage disequilibrium in the class I
region and HLA-DRB1, -DRB345, -DQB1 and –DQA1 are in linkage disequilibrium in the
class II region. A haplotype is defined as a combination of HLA genes carried on one
parental chromosome. Individuals inherit one haplotype from each parent.
Recombination of HLA genes is not common, 1-3% compared to the whole genome. The
distribution and frequency of HLA alleles differs between ethnic groups. Some alleles are
found in all populations but with varying frequencies. However, there are some alleles
which are found only in a specific population for example DRB1*04:12 has only been
identified in Australian Aborigines5.

31
1.1.2 Expression of HLA
HLA class I antigens are present on most nucleated cells. The level of expression varies,
with the lymphoid and myeloid cells having high expression6,7. HLA class II antigens are
present on professional antigen presenting cells (B cells, macrophages, dendritic cells,
Langerhans cells), thymic epithelium and activated T cells8. Cytokines such as interferon-
gamma (IFN-γ) can induce or upregulate the expression of HLA class II under certain
conditions9, 10. In the transplanted kidney, damage due to ischemia and reperfusion,
mechanical damage or cellular rejection for example, may induce a non-specific
inflammatory response. Antigen presentation to T cells is increased, and activated T cells
release cytokines which act on endothelial cells to upregulate class II HLA expression. The
increase in HLA class II expression can lead to a further increase in antigen presentation to
T cells amplifying the cellular immune response and also increase the antigen density of
donor (non-self) HLA target for an antibody response.
1.1.3 HLA polymorphism
The HLA system is highly polymorphic, the most polymorphic system in humans.
Polymorphism is not evenly spread throughout the HLA molecule but rather is
concentrated in the peptide-binding groove11. Polymorphisms resulting in amino acid
changes can modify the shape of the peptide binding groove and therefore alter the
peptide binding specificity of HLA molecules. The number of HLA alleles reported to the
international ImMunoGeneTics information system (IMGT) database increases by
approximately 500 every three months. The number of new alleles identified has
exponentially increased over the past several years, this may be a result of new HLA
typing technologies identifying polymorphisms outside regions previously sequenced
(Figure 3). There have been >10000 class I and 3500 class II alleles reported to the IMGT
HLA database in January 201612.

32
Figure 3. Growth of the IMGT / HLA Database. The number of new class I alleles reported
to the IMGT/HLA Database are shown in green whilst the number of class II alleles are
shown in black.
From: J Robinson, JA Halliwell et al. Nucleic Acids Research 2015; 43: D423-43113
1.2 Antigen Presentation
The major function of MHC molecules is to present unique peptides on the surface of cells
in an arrangement that permits their recognition by the T cell receptor (TCR) on T
lymphocytes14.
1.2.1 Endogenous Antigen presentation pathway
Endogenous peptides for HLA class I presentation are generated in the cytosol primarily by
the proteosome. Short peptides are transported to the endothelial reticulum (ER) by
Transporter associated with antigen presentation (TAP) where they are further processed
by ER amino peptidases (ERAPs) to produce peptides around 8 to 10 amino acids in length.
Assembly of the class I α chain with β2m and the peptides is coordinated by the peptide –
loading complex (tapasin and ERp57, calreticulin and TAP) (Figure 4). Some exogenous
proteins that are internalised by dendritic cells and macrophage subsets via phagosomes

33
or endosomes can be retranslocated into the cytosol where they are processed by this
pathway14, 15.
Class I restricted T cells recognise endogenous antigens synthesised within the target cell.
The class I molecule-peptide complex on the cell surface is recognised by the TCR of CD8+
lymphocytes.
1.2.2 Exogenous Antigen presentation pathway
Exogenous proteins are primarily presented by class II HLA. Antigens are internalised by
phagocytosis, macropinocytosis or endocytosis and traffic to the MHC class II
compartment (MIIC). Peptides of around 10 to 16 amino acids in length are generated in
the MIIC. HLA class I is assembled in the ER with invariant chain (Ii) which protects against
premature interaction with peptide in pre-lysosomal compartments. The complex traffics
to the MIIC where Ii is subjected to sequential proteolysis (Figure 4). The final cleavage
product, class II-associated Ii peptide (CLIP), occupies the peptide-binding groove.
Exchange of CLIP with peptide is facilitated by the chaperone-like molecule HLA-DM. Class
II restricted T cells recognise exogenously derived antigens. The class II molecule-peptide
complex is transported to the cell surface and recognised by the TCR of CD4+
lymphocytes14.

34
Figure 4. Exogenous and endogenous antigen processing.
From: JS Blum, PA Wearsch, P Cresswell. Annu Rev Immunol 2013; 31: 443-47314
1.2.3 The MHC and Allorecognition in renal transplantation
Allorecognition is initiated by CD4+ and CD8+ T cells which recognise either intact
allogeneic MHC molecules on the surface of donor APCs (direct allorecognition) or donor
peptides presented by class II HLA molecules after they have been processed and
presented by recipient APCs (indirect allorecognition)16, 17.
1.2.4 Direct allorecognition
Donor derived dendritic cells (passenger leucocytes) migrate from the transplanted kidney
to the recipient lymphoid organs where they stimulate the host immune response by
presenting host and donor derived peptides via intact donor MHC to recipient T cells

35
(Figure 5a)18. Direct allorecognition is believed to be the driving force behind early acute
graft rejection. The direct alloresponse diminishes as donor passenger leucocytes are
depleted because the graft parenchymal cells cannot drive T cell activation in the absence
of co-stimulatory molecules19, 20.
1.2.5 Indirect allorecognition
Recipient dendritic cells which infiltrate the transplanted kidney present peptides derived
from donor MHC. Following migration to recipient lymphoid organs, MHC-peptide
complexes are presented to recipient T cells (Figure 5b)21. The indirect alloresponse
persists causing chronic rejection via a delayed type hypersensitivity (DTH) mechanism and
the production of alloantibodies.
Figure 5. Direct and indirect allorecognition. A) direct allorecognition: T cells recognise
intact allogeneic MHC molecules on the surface of donor APCs; b) indirect
allorecognition: Alloantigens are recognised as peptides presented by class II HLA
molecules after they have been processed and presented by recipient APCs.
From: Nature reviews Immunology 2002; 2: 859-871. JA Bradley, EM Bolton, RA
Pedersen22

36
1.3 The significance of HLA in renal transplantation
Improvement in immunosuppressive therapies has been associated with better patient
and graft survival rates principally due to reduction in early acute T-cell mediated
rejection. However, despite the impressive reductions in early rejection, chronic allograft
rejection remains a leading cause of graft dysfunction and graft loss. Large collaborative
studies demonstrate that the number of HLA mismatches at HLA-A, -B and –DR loci have a
significant influence on graft survival23, 24. When stratified by two decades encompassing
improvements in immunosuppressive drugs, the effect of mismatching is still significant
(Figure 6). In addition, the need for rejection treatment is also associated with the number
of HLA mismatches in both eras (Figure 7).
Allograft rejection may occur at any time post-transplant and is categorised as early
(hyperacute), short-term (acute) or long-term (chronic).
Figure 6. Death censored graft survival rates in relation to the number of HLA-A, -B and –
DR mismatches in two eras- 1985-1994 and 1995-2004. P<0.001 in both decades.
From: G Opelz, B Dohler. Transplantation 2007; 84(2): 137-14324

37
Figure 7. Number of rejection episodes in the first year of transplant in patients with a
functioning graft at 1 year. P<0.001 in both decades
From: G Opelz, B Dohler. Transplantation 2007; 84(2): 137-14324
1.4 Humoral and cellular mechanisms of rejection
1.4.1 Hyperacute rejection
In hyperacute rejection the transplanted graft is rapidly rejected within minutes to hours
due to vascular injury via antibody-dependent cytotoxicity25, 26. Previous sensitisation
against HLA antigens through transfusion, pregnancy or previous transplant, or blood
group incompatibility allows pre-formed antibody binding to the vascular endothelium in
the presence of antigen and initiation of the complement cascade with the release of
inflammatory mediators and extensive microvascular thrombosis.
Hyperacute rejection has been virtually eliminated by the introduction of the pre-
transplant complement dependent lymphocytotoxicity (CDC) crossmatch27.

38
1.4.2 Acute cellular rejection
Acute cellular rejection can occur early, within days of transplant, but usually occurs within
weeks to months. Rejection is mediated by CD4+ and CD8+ lymphocytes that have been
activated against donor antigens28, 29. The stimulation of alloreactive T cells occurs in the
lymphoid tissues of the recipient by donor dendritic cells (passenger leucocytes) by direct
allorecognition. Donor passenger leucocytes stimulate HLA class II reactive CD4+ T cells,
which can stimulate the growth and differentiation of HLA class I reactive CD8+ cytotoxic T
cells. These alloreactive T cells enter the circulation and react with the allograft vascular
endothelium. The resulting cytokine release and inflammatory mediators leads to
migration of alloreactive T cells through the vascular wall. The infiltrating lymphocytes can
have a direct cytotoxic effect as well as mediating a DTH mechanism of graft rejection
involving recruitment of macrophages and release of cytokines30.
1.4.3 Acute humoral rejection
Acute humoral rejection is mediated by antibody and complement. Antibodies are either
pre-formed or produced de novo post-transplant and bind to donor antigens expressed on
the allograft which can activate the complement cascade. Damage to the endothelium can
be mediated either directly by formation of the membrane attack complex, or by the
infiltration of inflammatory cells recruited by soluble complement fragments or by
phagocytes that recognise complement fragments deposited on endothelial cells via a
complement receptor. There may also be complement independent antibody-dependent
cell cytotoxicity following antibody binding to endothelial cells. Endothelial damage can
initiate platelet activation and thrombosis, endothelial and smooth muscle cell
proliferation and direct graft damage from humoral and / or cellular infiltrates.
Mechanisms of acute humoral rejection are reviewed in 31-36.

39
1.4.4 Chronic rejection
Chronic rejection usually occurs years after transplantation and is characterised
functionally by a progressive loss of kidney function, which may be accompanied by
hypertension and proteinuria - both cellular and humoral mechanisms have been
implicated. Histologically, biopsies reveal vascular hypertrophy and hyalinosis with
interstitial fibrosis and chronic inflammation. Glomerular mesangial hypertrophy with
typical endothelial double contours and glomerulosclerosis are often associated with
chronic rejection and described as transplant glomerulopathy and are often refractory to
treatment37. Features of chronic humoral rejection include the histological features of
transplant glomerulopathy with evidence of chronic complement activation with binding of
C4d along the vascular compartment suggestive of humoral injury.
1.5 Production of antibody by B cells
1.5.1 T cell independent B cell activation
T cell independent B cell activation can be induced by direct interaction of antigen with the
B cell (Figure 8)38, 39, 40. Two mechanisms of independent activation are recognised: Type I
and Type II. In type I antigens, such as lipopolysaccharides, induce B cell activation through
Toll-like receptors directing inducing B cell division. At high antigen concentrations
polyclonal B cell activation occurs. Both immature and mature B cells can be activated. In
type II antigens, such as polysaccharides, induce an antigen specific B cell response via
interaction with the B cell immunoglobulin (Ig) receptor. Only mature B cells specific for
the antigen are activated by this process.
The antibodies produced by T cell independent activation are typically IgM and low affinity
compared to those derived using T cell help.

40
1.5.2 T cell dependent B cell activation
In T cell dependent activation, activation of B cells occurs following binding of antigen to
the B cell Ig receptor resulting in enhanced expression of co-stimulatory molecules on the
B cell surface (Figure 8)41. The antigen bound Ig receptor is internalised via receptor
mediated endocytosis. Antigen is processed internally and peptides are presented on the
B cell surface on MHC class II. As antigen processing occurs, B7-1 and B7-2 are expressed
by the B cell. CD4+ T helper (Th) cells which have been primed by previous encounter with
antigen presented by dendritic cells or macrophages recognise MHC-peptide complex on
the B cell and also bind B7 on the B cell surface via CD28 leading to Th cell proliferation.
Once activated, the T cells express CD40L which binds CD40 on the B cell, which in turn
leads to increased expression of B7 on the B cell surface and therefore more T cell
activation42. Antigen recognition by B cells enhances the expression of receptors for
cytokines released by the Th cells. CD4+ Th cell secreted cytokines IL-2, IL-4 and IL-5 induce
B cell proliferation and differentiation and determine the type of antibody produced by
promoting isotype class switching43-45.

41
Figure 8. Simplified representation of donor antigen recognition and the induction of
humoral immune response - T cell-independent and T cell-dependent B cell activation.
Upper panel – glycan antigens can be directly recognised by B cells and the cross-linking of the
B-cell receptors lead to IgM secretion through T cell-independent B cell activation. Lower panel
– Donor antigens can be endocytosed by antigen presenting cells and presented to helper T
cells leading to T cell activation and subsequent T cell-dependent B cell activation.
Adapted from S Julien, PA Videira, P Delannoy. Biomolecules 2012; 2: 435–46646
1.6 Pre-transplant crossmatching and detection of HLA antibodies
1.6.1 Crossmatching strategies
HLA antibodies can be formed following blood transfusion, pregnancy or transplant. In
1969 Patel and Terasaki published a landmark paper which showed that antibody directed
against donor class I HLA antigens, detected as a positive T cell crossmatch by the
complement-dependent lymphocytoxicity (CDC) assay, were associated with hyperacute
graft rejection27. Eighty percent (24/30) of grafts were lost to hyperacute rejection in
patients with HLA antibody. Following this report, the detection of pre-formed HLA class I

42
antibodies by the CDC crossmatch became the gold standard for pre-transplant testing and
has virtually eliminated hyperacute rejection. In the same year, Morris et al reported an
association of HLA antibodies detected post-transplant with renal graft failure47. HLA
antibodies were detected by CDC crossmatch in 38% (11/29) of patients whose grafts had
been rejected.
The CDC technique has historically been used to screen patients awaiting a transplant for
HLA antibodies, and an estimate of their sensitisation (Panel reactive antibody – PRA)
calculated as the percentage of donor lymphocytes with which a patient serum has a
positive reaction. The identification of donor-specific antibody detected in the screening
CDC assay can be used to predict a positive CDC crossmatch and is considered a
contraindication to transplantation.
The panel of donor lymphocytes was often variable from centre to centre and did not
represent the potential donor population. Therefore the same antibody profile could
result in a different PRA value between different centres. For this reason, calculation of
the PRA based on the frequency of HLA antigens in the donor population has helped to
standardise PRA48-51.
Immediately prior to transplant, patient serum is crossmatched against potential donor
lymphocytes to detect pre-formed cytotoxic antibodies. Incubation of donor lymphocytes
with patient serum in the presence of complement, usually sourced from rabbits, results in
binding of antibody to target antigens. Antibody binding can induce conformational change
in the antibody molecule exposing the Fc (fragment crystallisable) segment that binds to
complement. The complement cascade is activated leading to membrane damage and cell
lysis. The standard CDC technique detects complement fixing IgG and IgM antibodies.
Several studies have shown that IgM antibodies are frequently non-HLA auto-reactive
antibodies and are not detrimental to graft outcome52-56. However, IgM antibodies can
undergo class switching under the influence of cytokines and co-stimulation of B cells on
contact with donor HLA antigen to which the patient has previously been senstitised45.
This may lead to the production of donor specific IgG antibodies which may be harmful to
the graft.
Crossmatches are performed on separated T and B cells due to the differential expression
of HLA class I and II antigens on these cells. A positive T cell crossmatch is considered an

43
absolute contraindication to transplantation; however a positive B cell crossmatch can
sometimes be acceptable.
Antibodies directed against class I HLA antigens can be detected by both T- and B-cell
crossmatches. However, only B cell crossmatches can detect antibodies directed against
HLA class II antigens. There are several reasons for a positive B cell crossmatch in the
presence of a negative T cell crossmatch: i) Low titre class I antibodies due to higher
expression of class I HLA on B cells57; ii) Non-HLA antibodies reacting with respective
antigens expressed on B cells; iii) Non-specific binding of IgG antibodies to Fc receptor on B
cells; iv) Class II HLA antibodies; v) Therapeutic antibody such as anti-CD20 (Rituximab).
The heterogeneity of the B cell crossmatch contributes to the uncertainty of the relevance
of a positive B cell crossmatch with concomitant negative T cell crossmatch in renal
transplantation38-44. Early studies reported no difference in graft outcome between
patients with a negative T and B cell crossmatch compared with those with a negative T
cell and positive B cell crossmatch58-62. More recent studies demonstrate that a positive B
cell crossmatch alone was not correlated with graft outcome, but when the cause of the
positive crossmatch was elucidated a difference in outcomes could be demonstrated.
Karrupan et al63 showed a B cell crossmatch effect only if class I antibodies were
demonstrated. Mahoney et al64 showed in a large cohort study that a positive B cell
crossmatch was predictive of poor outcome in sensitised patients. Additional studies have
also confirmed the importance of a positive B cell crossmatch where donor specific
antibodies can be demonstrated65-68.
Although a positive CDC crossmatch is highly predictive of early graft failure, an
unequivocally negative T cell CDC crossmatch does not necessarily result in long term graft
survival. Patel and Terasaki also reported that early graft loss occurred in some patients
despite a negative crossmatch. This is because weak or low-titre HLA antibodies are not
detected by the CDC crossmatch and despite their initial low level they may cause or
contribute to later graft loss. In addition, clinically relevant non-HLA antibodies are not
detected by the CDC crossmatch. The relative low sensitivity, and the inability to detect
HLA antibodies which are not able to fix complement lead to the introduction of more
sensitive assays such as the extended incubation time CDC crossmatch69, anti-human
globulin enhanced CDC (AHG-CDC) and flow crossmatching (FCXM). The AHG-CDC

44
crossmatch is more sensitive than the CDC assay because it detects low-titre antibodies
and antibodies which do not activate complement70, 71. Flow cytometry crossmatching has
greater sensitivity than the CDC assays because it allows the direct detection of recipient
antibody binding to donor lymphocytes72, 73. However, the significance of a positive
crossmatch using these more sensitive crossmatch assays is still unclear and has some
potential limitations74-78. It is possible that the assays may be over-sensitive and, in some
circumstances, the detection of low titre antibodies in otherwise low-risk patients might
exclude patients from proceeding to transplantation. Further investigation into the
relevance of a positive flow crossmatch, in particular a positive B cell flow crossmatch
alone is warranted.
1.6.2 HLA antibody detection by ELISA
Cellular assays have the major drawback in that the target cells, lymphocytes express non-
HLA antigens as well as HLA antigens on their cell surface. B cells express both class I and II
antigens, therefore a positive B cell crossmatch can be due to class I, class II, class I and II
or non-HLA antibodies including immune complexes and Fc receptor binding antibodies79.
To attempt to solve this problem, solid phase assays using isolated HLA antigens as targets
for antibody detection were developed. ELISA was the first type of solid phase assay to be
developed, using purified HLA antigens (pooled or single) bound to an ELISA plate.
Reactivity is determined by reading optical density using a spectrophotometer so removes
the subjectivity in antibody detection by CDC. The assay is semi-quantitative and specific
for all subclasses of IgG antibody80-82.
Several studies, including a large retrospective international study, have shown an
association between HLA antibodies detected in pre-transplant sera by ELISA with poor
graft outcome (Table 1)83-89. The majority of these studies considered the presence of any
HLA antibodies of relevance to the graft outcome and did not differentiate between
whether the HLA antibodies were donor specific, or non-specific. Not all studies reported
an association of pre-transplant antibodies detected by ELISA only with an adverse kidney
transplant outcome. In those studies which looked at the association of antibody with
graft loss, all found a correlation with the presence of class I antibodies whether they were
DSA89 or not83, 84. Of the studies investigating acute rejection however, only those looking
at DSA87, 88 rather than overall sensitisation85 found a correlation with the presence of class

45
I, II or I and II antibody. Patel et al87 were able to demonstrate this association even in
patients with a negative pre-transplant flow crossmatch. These results suggest that the
presence of DSA in pre-transplant sera is an important risk factor in acute rejection
episodes. However, detection of any HLA antibody which is associated with graft loss
might be due to the presence of DSA which have not been identified in the study, or a
predisposition to make HLA antibodies leading to production of DSA post-transplant.
Table 1. A summary of studies investigating the association of graft outcome with pre-
transplant class I and II antibodies detected by ELISA in renal transplants.
Authors and year of publication
Number in study / number of antibody positive
Antibody detected (any antibody or DSA)
Clinical end-point End-point correlation with antibody class
Class I Class II Class I and II
Monteiro et al. 1997
83
124 / 28 Any antibody
Graft loss Yes NI NI
Susal and Opelz. 2002
84
4136 / 976 Any antibody
Graft loss Yes Yes NI
Slavcev et al. 2003
85
120 / 38 Any antibody
Acute rejection No No No
Susal and Opelz. 2004
86
5949 / 1388 Any antibody
Graft survival No Yes NI
Patel et al. 2007
87
330 / 20 DSA Acute humoral rejection
Yes Yes Yes
Lefaucheur et al. 2007
88
237 / 43 DSA Antibody mediated rejection
Yes Yes Yes
Susal et al. 2009
89
5315 / 121 Any antibody
Graft failure Yes Yes Yes
NI = Not tested / investigated
The Lefaucheur group demonstrated that both current and peak (historical) sera positive
for HLA antibodies were associated with AMR, and could show a relationship between the
strength of the HLA antibody and graft outcome88. Furthermore, Wu et al showed that
class I antibodies which were detected on multiple occasions prior to transplant were
associated with poor graft survival, whereas donor-specific antibodies detected on only
one occasion were not detrimental to the allograft90.

46
1.6.3 HLA antibody detection by Luminex bead assay
Further sensitivity in HLA antibody detection by solid phase assay was achieved with the
development of the Luminex bead assay. In these assays, HLA antigens are attached to a
latex bead and then detected by flow cytometry91. The assay is more sensitive than ELISA92-
94, and the development of beads carrying a single recombinant HLA antigen (Single
Antigen Beads) has further assisted in the precise determination of antibody specificity
including antibodies directed against HLA-C, -DQ, -DP and –DR51/52/53. The assay can be
modified by changing the secondary detection antibody to detect different IgG subclasses
or different immunoglobulin isotypes95, 96. In addition the assay can be modified for
detection of complement-fixing antibodies which may be more pathogenic than antibodies
which are not complement fixing97, 98.
The clinical relevance of antibodies detected by Luminex bead assay in the absence of a
positive CDC crossmatch remains uncertain. At the time of commencement of this study
there were few publications investigating clinical outcomes from transplantation across
donor-specific antibodies detected by Luminex Single Antigen bead99-102. These papers are
summarised in Table 2. Although not always consistent, these studies indicate that both
class I and class II HLA antibodies are associated with a detrimental effect on long term
graft function due to high rates of rejection and delayed graft function.

47
Table 2. A summary of studies investigating the association of graft outcome with pre-
transplant class I and II DSA detected by Luminex bead assay in renal transplants.
Authors and year of publication
Number in study / number of antibody (DSA) positive
Clinical end-point
Time to follow up
End-point correlation with antibody class
Class I Class II Class I and II
Gibney et al. 2006
99
136 / 20 DGF / Acute rejection / Graft loss
6 months Yes Yes Yes
Gupta et al. 2008
100
121 / 16 Acute rejection / DGF
1 and 5 years
No No No
Issa et al. 2008
101
598 / 103 Transplant glomerulopathy
Mean 54 months
No Yes Yes
Van den Berg-Loonen et al. 2008
102
34 / 13 Rejection episodes
180 days Yes Yes Yes
DGF = Delayed graft function
Gibney et al99 retrospectively studied 136 patients receiving a transplant between March
2003 and May 2004. Fifty-five patients had antibody detectable in pre-transplant sera by
Luminex PRA beads, of these 20 had demonstrable DSA. In the group of patients with DSA,
increased rates of primary non-function (10% vs 0%, P=0.06), delayed graft function (30%
vs 9%, P=0.04) and biopsy proven acute rejection (BPAR) (25% vs 3%, P=0.01) were
observed when compared to the group with no DSA. Graft survival at 6 months was also
significantly lower in those with DSA (75% vs 94%, P=0.04). Gupta et al100 could not confirm
these findings in their cohort of 121 patients transplanted between 1999 and 2001. HLA
antibodies were detected in 38 of the 121 patients, 16 patients had DSA. There was no
significant difference between 1 and 5 year patient and graft survival in patients with DSA,
non-DSA or no antibody. However, in a multivariate analysis, delayed graft function and
the presence of DSA were independent predictors of graft loss when using the non-
sensitised group as a reference. Issa et al101 studied a large cohort of 598 kidney recipients
transplanted between January 2000 and 2005. Of the 235 sensitised patients, 28% of the
patients with class I antibody had DSA and 55% of the patients with class II antibody had
DSA. In 100 patients with both class I and II antibodies, 31% had a class I DSA and 48% had
a class II DSA. The authors did not indicate the number of patients with both a class I and II

48
DSA. The group demonstrated that transplant glomerulopathy (TG) was associated with
the presence of class II antibodies (HR 1.89, 95%CI 1.42-2.52, p<0.0001) and that
association was significantly higher in patients with class II DSA (HR 3.524, 95%CI 1.67-7.44,
p=0.001). Furthermore, they showed graft survival in patients with TG to be significantly
lower than those without TG (62% versus 95%, p<0.001). In a smaller cohort of 34 highly
sensitised patients, van den Berg-Loonen et al102 showed a trend to earlier and higher
number of rejection episodes in 13 patients with DSA compared to those with no DSA
(p=0.08). They could not demonstrate a detrimental effect on graft function up to 8 years
post-transplant. These studies are all limited by including patients with a pre-transplant T
cell negative crossmatch which is likely to exclude any effect of high level class I antibody.
1.7 Post-transplant antibody monitoring
The presence of HLA antibodies detected at any time post-transplant has also been
associated with renal allograft rejection103-106. In addition, a number of studies have shown
the association of de novo HLA antibodies with acute and chronic rejection and poor graft
survival (Table 3)107-116. Terasaki et al108 showed that the production of any antibody post-
transplant (DSA or non-DSA) was associated with poor outcome. The group reported a 1
year survival rate after testing for HLA antibodies of 96% in those with no antibody versus
94% in those with any HLA antibody and 64% in those with DSA. The association of non-
DSA with poor outcome may be a marker of a general immune activation state rather than
HLA specific antibodies having a direct effect on the allograft, and may correspond to high
immunological responders. It has been hypothesized by some groups that DSA is ‘hidden’
and not detected in the serum by its binding to the graft. This concept is supported by the
finding that after nephrectomy of rejected kidneys, donor-specific antibodies are
subsequently detected in peripheral blood samples117-119. Eluates from kidney samples
have also shown donor-specific antibodies are bound to the endothelium120, 121.

49
Table 3. A summary of studies investigating the association of graft outcome with post-
transplant class I and II DSA detected by Luminex bead assay in renal transplants.
Authors and year of publication
Number in study / number of antibody (DSA) positive
Pre-transplant antibody status
Clinical end-point
End-point correlation with antibody class
Class I Class II Class I and II
Mihaylova et al. 2006
107
72 / 16 No antibody Chronic rejection
Yes Yes Yes
Terasaki et al. 2007
108
1329 / 158 No antibody Graft failure Yes Yes Yes
Mao et al. 2007
109
54 / 32 No antibody DGF, Acute rejection, graft failure
Yes Yes Yes
Scornik et al. 2007
110
103 / 16 No antibody AMR Yes Yes Yes
Lee et al. 2009
111
50 / 37 No DSA AMR Yes Yes Yes
Haririan et al. 2009
112
297 / 93 Crossmatch negative
AMR No Yes Yes
Kedanis et al. 2009
113
301 / 52 Crossmatch negative
AMR Yes Yes Yes
Stastny et al, 2009
114
137 /57 Negative T, neg / pos B flow crossmatch
Graft failure Yes Yes Yes
Cinti et al, 2009
115
100 / 16 Crossmatch negative
Acute rejection Yes Yes Yes
Hidalgo et al. 2009
116
145 / 54 No DSA Microvascular pathology (subclinical rejection)
No Yes Yes
DGF = Delayed graft function; AMR = Antibody mediated rejection
1.8 Therapies for the treatment of antibody mediated rejection
Antibody mediated rejection is associated with a poorer prognosis than cellular rejection,
is frequently unresponsive to therapy and accounts for a large proportion of graft losses122-
126. Therapies used to treat AMR are targeted either against the alloantibody itself, or
against the antibody producing B cells (Figure 8)127. The most commonly used therapies
are i) plasmapheresis, a temporary removal of the antibody usually used in conjunction
with other therapies; ii) IVIg, which neutralises the alloantibody, inhibits complement
activation and modulates cell-mediated immunity128-130 ; and iii) Rituximab, an anti-CD20

50
monoclonal antibody which depletes B cells excluding plasma cells which do not express
CD20. These therapies are all temporary but can be effective in AMR treatment.
Lefaucheur et al published results of a controlled trial comparing a combination of
plasmapheresis, IVIg and Rituximab versus plasmapheresis alone and demonstrated a
91.7% graft survival at 36 months versus 50% respectively131.
More recently a therapy was introduced which not act directly on the antibody or antibody
producing B cells. Eculizumab is a humanised monoclonal antibody directed against the
complement protein C5 blocking the complement pathway at the terminus originally used
to treat paroxysmal nocturnal hemoglobulinuria (PNH)132 and recently found to be
effective in the treatment of AMR133. Stegall et all demonstrated that eculizumab was
effective in decreasing AMR in sensitised patients reducing the incidence from 41.2% in the
control group to 7.7% in those treated with the antibody134. A later study by the same
group indicated that eculizumab was not always successful with 2/26 patients treated
undergoing early AMR135.
Another potential therapy, Bortezomib, acts by inhibiting the 26s proteosome and
inducing apoptosis of rapidly dividing cells including bone marrow resident plasma cells136.
This drug is therefore able to deplete HLA antibody derived from long-lived plasma cells in
patients who are resistant to other therapeutic agents. Everly et al were able to show in a
short series of six treated patients improved graft function, a reduction in antibody levels
and rapid reversal of antibody-mediated rejection with no recurrence at 5 months137.

51
Figure 9. A schematic representation of antibody-mediated rejection pathophysiology.
Mechanisms of action of therapies are indicated. Therapies currently used are in red; drugs under
evaluation are in dashed orange. AMR, antibody-mediated rejection; Conv, convertase; IV,
intravenous; MAC, membrane attach complex; MHC, major Histocompatibility complex; mTOR,
mammalian target of rapamycin; NK, natural killer.
From: E Pouliquen, A Koenig et al. F1000Prime Rep 2015; 7: 51127
1.9 Allograft accommodation
The term accommodation was first used in the 1980’s in the context of blood group
incompatible transplants as a lack of immune response138-140. Anti-donor (blood group)
antibodies were removed prior to transplantation, but rejection was expected when these
transiently removed antibodies returned. On the contrary, these transplants survived and
functioned as well as blood group compatible transplants139, 140. The group of Bannett et al
were able to show this lack of response was not due to absence of blood group antigens
on the graft endothelium141. Others have shown that donor specific antibodies are

52
detectable and interact with the graft endothelium by C4d staining of peritubullar
capillaries142, 143. Accommodation is very common in blood group incompatible
transplantation. Haas et al reported over 80% of protocol biopsies in blood group
incompatible transplants showed C4d deposition with no effect on long term graft
outcome142.
Accommodation of HLA antibodies does not appear to be a common phenomenon and
many studies have demonstrated the presence of HLA antibodies prior to rejection
(reviewed in 1.6.2, 1.6.3, 1.7). It is clear, however, that this correlation is not absolute and
many patients have detectable DSA and no clinical or histopathological symptoms. It is
possible that accommodation of HLA antibodies is temporary, as the antibodies can be
detected many years before rejection as shown in long term studies such as those
reported by Mizutani et al144. However the frequency and mechanism by which
accommodation may occur in some patients with donor specific HLA antibodies is
unknown and warrants further research and elucidation.
1.10 Strategies for transplanting the sensitised patient
Approximately 30% of patients awaiting a kidney transplant in Australia are sensitised
against HLA antigens. The presence of anti-HLA antibodies often presents an impenetrable
barrier to transplantation and these patients have a longer wait on the transplant list, due
to donor incompatibility, and poorer survival on dialysis than their transplanted
counterparts145, 146. A further 5% of patients are highly sensitised, defined as a PRA of
greater than 80%. The transplant rates of highly sensitised patients is even lower, with
many of these patients remaining on the transplant list for greater than 5 years.
1.10.1 Desensitisation
The aim of desensitisation is to clear or decrease the presence of circulating alloantibodies
to a level which does not cause a positive crossmatch in order to prevent antibody
mediated rejection and to facilitate transplantation in highly sensitised patients. The two
most commonly used protocols involve the use of low dose intravenous immunoglobulin
(IVIG) with plasma exchange (Johns Hopkins protocol)147 or high dose IVIG alone (Cedars-
Sinai protocol)148. These protocols are often used in conjunction with Rituximab, an anti-

53
CD20 antibody, which depletes B lymphocytes but not plasma cells which do not express
CD20149. IVIG has multiple effects on different immune pathways150. It was initially thought
to have a neutralising effect on anti-HLA antibodies though anti-idiotypic antibodies128.
Later it was shown to inhibit complement activation129. IVIG also interacts with cells
involved in immune activation including macrophages, neutrophils and NK cells via the Fcϒ
receptor130. Stegall et al151 have shown that low dose IVIG with plasma exchange is more
effective than high dose IVIG alone. However, despite acceptable short-term patient and
graft survival in desensitised patients, a higher rejection rate and increased incidence of
AMR compared with unsensitised patients has been reported152, 153.
1.10.2 Acceptable mismatch program
The acceptable mismatch program is an initiative which originated in Eurotransplant
intended to facilitate the transplant of highly sensitised patients Europe-wide. The
program relies on two strategies to identify acceptable HLA mismatches for an individual: i)
identification and definition of HLA antibodies (unacceptable antigens) and subsequent
identification of HLA antigens towards which an individual has never formed an antibody
response154, 155; ii) definition of acceptable HLA antigens by identification of the repertoire
of epitopes shared between an individual’s HLA type and other HLA antigens using the
HLAMatchmaker program (www.matchmaker.net)156-158. In 2015, Eurotransplant reached
the 25th anniversary of the Acceptable Mismatch program and reported over 1000 highly
sensitised patients transplanted over this time who otherwise might not have found a
negative crossmatch159.
1.10.3 Paired kidney exchange
Paired kidney exchange was first proposed in 1986 by Rappaport160 as a simple exchange
between two incompatible donor and recipient pairs to create two compatible transplants
(a two way exchange). South Korea161 and Holland162, 163 were the first countries to
implement a paired kidney exchange program initially based on two-way exchanges
(Figure 10). To expand the number of potential matches, variations of paired donation
have been designed including closed chain matches with multiple pairs (3-way or higher)
and open chain matches starting with an altruistic donor and ending with a wait-list

54
recipient (Figure 11). These programs have a distinct advantage over desensitisation as
they avoid pre-formed HLA antibodies and therefore the risk of early AMR is much
reduced.
Figure 10. Paired kidney exchange – simple two-way exchange.
Green arrows denote compatible transplants, red dotted arrows denote incompatibility. Donor
1 is incompatible with recipient 1 and donor 2 is incompatible with recipient 2 due to HLA
sensitisation or blood group incompatibility. However, donor 1 is compatible with recipient 2
and donor 2 is compatible with recipient 1 and an exchange of donors is possible resulting in
two transplants.

55
Figure 11. Paired kidney exchange – non-directed donor chain.
Green arrows denote compatible transplants, red dotted arrows denote incompatibility. Donor
1 is incompatible with recipient 1, donor 2 is incompatible with recipient 2 and donor 3 is
incompatible with recipient 3 due to HLA sensitisation or blood group incompatibility. Recipient
1 does not have a compatible donor in the paired exchange pool, however, donor 1 is
compatible with recipient 2 and donor 2 is compatible with recipient 3. Introduction of an
altruistic donor who is compatible with recipient 1 forms the primary transplant and allows the
chain to proceed, with the end donor in the chain donating to the transplant wait list pool.

56
1.11 Aims of this thesis
One of the major immunological hurdles in transplantation is the presence of pre-formed
antibodies in the recipient directed against donor HLA antigens. Whilst current
immunosuppressive regimens have improved graft outcomes, the presence of donor
specific anti-HLA antibodies is associated with allograft rejection and poor long term graft
outcome. In recent years, the detection techniques for anti-HLA antibodies has evolved
from the relatively insensitive lymphocytotoxic crossmatch to the introduction of more
sensitive solid phase assays including ELISA and Luminex bead assays. The clinical
significance of donor specific HLA antibodies detected by Luminex single antigen bead
assay in pre-transplant sera with concurrent negative CDC crossmatch is uncertain. The
aims of this thesis are to retrospectively test pre-transplant sera from kidney transplant
recipients by Luminex single antigen bead assay and determine their clinical significance in
terms of rejection and patient and graft outcomes. We further aim to use this knowledge
to design virtual crossmatching strategies that allow transplantation of highly sensitised
patients in paired kidney exchange.

57
Chapter 2
Materials and Methods

58
2.1 HLA Antigen typing (HLA-A, -B, -C, -DRB1, -DRB345, -DQB1, -DPB1) by Sanger
sequencing
2.1.1 DNA Extraction
Recipient and donor Genomic DNA was extracted from peripheral blood samples
collected in ACD (Acid citrate dextrose) by commercial (QIAGEN) or in-house salting-
out method modified from the published method from Miller et al. (SA Miller, DD
Dykes, HF Polesky. A simple salting out procedure for extracting DNA from human
nucleated cells. Nucleic Acids Res 1988; 16(3): 1215)
2.1.2 DNA Quantitation using the Nanodrop spectrophotometer
1. Add 2ul of sterile deionised water to the Nanodrop probe to set a blank reference
2. Add 2µl of DNA sample to the Nanodrop probe to measure absorbance
3. Concentration (A260) and purity (A260 / A280 ratio) of the DNA sample is recorded.
The optimal purity is 1.8.
2.1.3 PCR amplification of Target DNA
1. For each locus set up one reaction for each sample being amplified. Include
appropriate positive controls of known genotype and at least one negative control for
each group of samples being amplified.
2. CG-HLA Sequence Based Typing Kits™ (Conexio Genomics) are supplied as separate
aliquots of primer mix and polymerase (Appendix Table I). The polymerase needs to be
added to the primer mix just prior to setting up the PCR reactions. Thaw the required
number of vials of the appropriate PCR Mix. Once thawed, vortex briefly to mix
components.
3. Calculate the number of samples to be tested and dispense the required amount of
PCR mix and DNA polymerase into a sterile tube (Table 1). Vortex the solution 3-4
times, for approximately 1 second each time.

59
Table 1. PCR mastermix volumes per sample
LOCUS HLA-A HLA-B HLA-C HLA-DRB1 HLA-DQB1
Locus-specific PCR mix
(e.g. CG-HLA-A mix)
16ul 16ul 16ul 16.7ul 16.7ul
DNA-Pol 1ul 1ul 1ul 0.3ul 0.3ul
4. Dispense 17µL of the primer/polymerase mix prepared in step 3 above into each
reaction well of either a 96 well plate, or 8 tube strips.
5. Add 3uL of sample DNA or appropriate positive control DNA to each reaction well.
Add 3uL of sterile water to the negative control reaction well.
6. Seal the reaction wells or tubes. Mix thoroughly but gently by vortexing, then
centrifuge briefly to ensure all reaction components are at the bottom of the wells (i.e.
turn centrifuge on, allow it to reach a speed of approximately 185g then turn off).
7. Place the 96 well plate or tube strips into a thermal cycler and amplify the target
sequence according to the thermal cycling conditions below.
Thermal Cycling Program
95°C 10 mins
96°C 20 secs
60°C 30 secs 33 cycles
72°C 3 mins
15°C hold
NB: Amplification takes approximately 2.5 hours to complete.
8. When the PCR is completed, remove the plate from the thermal cycler and either
proceed directly to gel electrophoresis or store at 4°C until required. Purification of

60
amplicons by ExoSap-IT® treatment should occur within 24 hours of completion of
PCR.
2.1.4 Agarose Gel Electrophoresis
1. Confirm successful amplification of the template DNA by agarose gel electrophoresis
with a 1% gel using 2µl of each PCR product combined with 5µl loading buffer.
2. Photograph the gel using a BIO-RAD GEL DOC 2000 Transilluminator. The ethidium
bromide labelled DNA bands are illuminated by the UV light.
3. The number and expected sizes of the resultant amplicons will vary according to the
locus and sample genotype. Expected PCR amplicon sizes are indicated in Table 2.
Band intensities should be reproducible within each assay if DNA quality is consistent.
A sample with a slightly weaker band can still be processed for sequencing using a
lower post- ExoSAP-IT® dilution volume. Very weak products should not be sequenced.
Table 2. Expected number of PCR products and respective sizes for each locus.
Locus
Expected band sizes
HLA-A
≈ 2 kb
HLA-B
≈ 2 kb
HLA-C
≈ 1 kb and 1.4 kb
HLA-DRB1
≈ 450bp - 650bp (Banding pattern will vary depending on which of the specific
allele groups are present, maximum of 2 bands expected)
HLA-DQB1
≈ 300bp and 350bp
2.1.5 Purification of PCR products for Sequencing
PCR products contain excess primers and unconsumed dNTP’s which require removal
before sequencing reactions can be performed. They may interfere with the efficiency of
the sequencing reaction, or can result in background “noise” in the sequence.

61
1. Prepare a mastermix consisting of 4µl of ExoSAP-IT® and 8uL of 2mM MgCl2 per
sample. Dispense 12µl of the mastermix into each PCR sample to be sequenced. Seal
the tubes or plates, vortex or place on shaker for 2 minutes and centrifuge to ensure
all reagents are at the bottom of the wells, before placing into the thermal cycler.
2. Run the thermal cycler according to the following protocol:
37°C - 30mins
80°C - 15mins
4°C - hold
3. Upon completion, dilute the purified product 1:8 with sterile water. This dilution
step will ensure that there is sufficient template to perform the sequencing reactions
and ensure that the concentration of the template is sufficient to produce good quality
sequence data. Note that weaker PCR products may require a lower dilution factor
than 1:8.
4. ExoSAP-IT® treated samples may be stored at 4°C until ready for use.
2.1.6 Sequencing of PCR Amplified Template
All sequencing reactions must be set up in a designated (“post-PCR”) area. This cannot be
the same area as used to set up the PCR reactions.
1. Allow the vial of BDT and other reagents to thaw at room temperature. Expose BDT
to light as little as possible. Once thawed, transfer reagents to ice. Reagents should be
kept on ice and the sequencing reactions should be prepared on a cooling block or on
an ice bath.
2. For each reaction prepare a fresh sequencing primer reaction mix as follows:
Reagent Volume Required
Sequencing Primer 2.0µl
BDT v3.1 Ready reaction mix 1.0µl
5 X Sequencing Buffer 3.5µl
Water 11.5µl
Sequencing primers are summarised in Table 3.

62
Table 3. Sequencing primers provided for use with each locus
LOCUS SEQUENCING PRIMERS
HLA-A AEX1F, AEX1R, AEX2F, AEX2R, AEX3F, AEX3R, AEX4F, AEX4R
HLA-B BEX1F, BEX2F, BEX2R, BEX3F, BEX3R, BEX4F, BEX4R
HLA-C CEX1F, CEX1R, CEX2F, CEX2R, CEX3F, CEX3R, CEX4F, CEX4R, CEX5F, CEX5R, CEX6F, CEX6R, CEX7F, CEX7R, CEX8F
HLA-DRB1 DRB1EX2F, DRB1EX3R, DRB1EX3R, RB-TG344-R
HLA-DQB1 DQB1EX2F, DQB1EX2R, DQB1EX3F, DQB1EX3R
3. Mix each sequencing primer reaction mix gently by pulse (2-3 seconds) vortexing.
4. Dispense 18μl of the sequencing reaction mix to each appropriate reaction tube or
well of a 96 well plate. If 8-tube strips or individual tubes are used, they should be
placed in a carrier so as to avoid mixing up the positions during the procedure.
5. Add 2μl of purified PCR product to each appropriate well.
6. Cap or seal wells or plate tightly, mix gently then centrifuge briefly to ensure all
reagents are at the bottom of the tubes.
7. Place the reaction tubes or plate into a thermal cycler and run according to the
following program:
96C for 10 seconds
50C for 5 seconds 25 cycles
60C for 2 minutes
then 4C indefinitely
8. Once the program is complete, remove the reaction tubes or plate from the thermal
cycler and either proceed directly to purification of the sequencing reaction products
or store at 4C until required. It is recommended that sequence reaction samples are
purified and run on the DNA sequencer within 24 hours.

63
2.1.7 Purification and Concentration of Big Dye Terminator sequencing products using
ethanol precipitation
1. Remove the reaction tubes or 96 well plate from the thermal cycler (or 4C storage)
and centrifuge briefly. If reusable lids/caps have been used during thermal cycling label
the lids/caps to avoid cross-contamination.
2. Each reaction requires 5µl of 125mM EDTA and 60µl Ethanol. Make a mix of the
following for a full 96 well plate:
550µl of 125mM EDTA
6.6ml of 100% Ethanol
Add 65µl of the above mix to each sample
The final ethanol concentration is 70%
3. Replace caps and invert tubes or plate 4 times to ensure thorough mixing.
4. Centrifuge briefly and leave at room temperature, protected from light, for 15
minutes to precipitate the extension products. Slightly longer precipitation times are
acceptable, preferably no longer than one hour.
5. Place the tubes or plate in a centrifuge and spin according to the following
guidelines:
Centrifuge speed 1400g – 2000 g: 45 minutes
Centrifuge speed 2000g to 3000g: 30 minutes
Important: Proceed to the next step immediately. If this is not possible, then
spin the tray for an additional 10 minutes immediately before performing the next
step.
6. Without disturbing the precipitates, remove the strip lids and discard the
supernatant, by inverting the tubes or plate onto absorbent tissues (e.g. facial tissues).
7. Place the inverted tubes or plate with the tissues into the centrifuge and spin briefly.
8. Remove the plate from the centrifuge, discard tissues, and then add 60µl of freshly
prepared 80% ethanol to each pellet. Cap the tubes, and then invert the tubes or plate
4 times to mix.
9. Place the tubes or plate in centrifuge and spin at approximately 1700g for 15
minutes.
10. Repeat steps 7 to 9, then remove from centrifuge, discard tissues. Vacuum dry for
15 minutes, or air dry for 1 hour, in the dark. Reseal plate if not proceeding
immediately to denaturation step.

64
11. Resolubilise pellets by adding 12µl of Hi-Di™ formamide. Thoroughly vortex tubes
or plate for approximately 15 seconds.
12. Denature samples by placing in a thermal cycler which is already at 98 degrees, for
5 minutes.
13. At the end of 5 minutes, remove from thermal cycler and immediately place on ice
for at least 5 minutes. Centrifuge briefly to bring down any condensation.
ENSURE THAT THERE ARE NO AIR BUBBLES IN THE WELLS. THESE CAN ENTER AND
DAMAGE THE CAPILLARY.
14. Load the reaction plate onto the automated sequencer and prepare the data
collection file according to the sequencer manufacturer specifications. Samples should
be run within 24-36 hours otherwise the Hi-Di™ formamide will begin to break down
to formic acid and there will be significant loss of resolution. If it is not possible to run
the plate within this time frame, it should be stored at 4 degrees.
2.1.8 Electrophoresis of sequencing products on 3730 sequencer
1. Run the sequencing product plates according to Table 4.
2. Use the instrument’s data collection software to process the raw collected data and
create the sequence files.
3. Analyse sequences using Assign ATF™ software.
Table 4. 3730 instrument settings for HLA sequencing.
PARAMETER SETTING
Dye set Z- BigDye V3
Mobility file KB_3730_POP7_BDTV3
Basecaller KB.bcp
Run Module Regular FastSeq50_POP7
Injection time 15 secs
Run Time 2.5 hours

65
2.2 LABType® SSO for HLA-DQA1 Typing
2.2.1 DNA Amplification
1. Turn on thermal cycler to keep heated lid warm.
2. Select the appropriate HLA typing kit (locus and resolution, OneLambda Inc) and
thaw out Amplification Primers, and D-Mix. Make sure to keep on ice until ready to
use.
3. Vortex D-mix and Amplification Primer for at least 15 seconds, and perform a quick
centrifuge (5 seconds) to spin down any liquid trapped under lid.
4. Create the amplification mixture by adding correct volumes of D-Mix and
Amplification Primers in a 1.5ml eppendorf tube as detailed in Table 5.
Table 5. PCR amplification mix volumes.
Number
of
Reactions
D-mix
(µl)
Amplification
Primer (µl)
AmpliTaq Polymerase (µl)
1 13.8 4 0.2
10 138.0 40 2.0
50 690.0 200 10.0
96 1491.0 432 21.6
5. Pipette 2µl of each DNA template into a 96 well PCR microplate.
6. Add the appropriate amount of AmpliTaq Polymerase to the amplification mixture
and vortex for 5 seconds.
7. Aliquot 18µl of Amplification mixture into each well containing DNA.
8. Cap or seal the plate and give a quick vortex to mix contents in plate.

66
9. Place PCR plate in thermal cycler and run according to the following program:
96°C for 3 minutes
96C for 20 minutes
60C for 20 minutes 5 cycles
72°C for 20 minutes
96°C for 10 minutes
60°C for 15 minutes 30 cycles
72°C for 20 minutes
72° for 1 minute
then 4C indefinitely
10. Remove PCR plate and store in a 4°C fridge.
2.2.2 Agarose Gel Electrophoresis
1. Confirm successful amplification of the template DNA by agarose gel electrophoresis
with a 1% gel using 5uL of each PCR product combined with 5uL loading buffer.
2. Photograph the gel using a BIO-RAD GEL DOC 2000 Transilluminator. The ethidium
bromide labelled DNA bands are illuminated by the UV light.
2.2.3 Denaturation/Neutralisation
1. Turn on Thermal cycler and run program to 60° C HOLD. Make sure lid is heated to
optimum temperature before use.
2. Remove reagents in Table 6, supplied in the SSO genotyping kit, from -80° C freezer
to room temperature to thaw and then prepare all reagent volumes in an
appropriately sized disposable tube as necessary. Return any unused reagents to 2° C
to 8°C (Do not re-freeze bead mixture after thawing).

67
Table 6. Post-PCR reagent volumes.
Number of
tests
Denaturation
Buffer (µl)
Neutralisation
Buffer (µl)
Hybridisation
Buffer (µl)
Wash Buffer
(µl)
Bead Mixture
(µl)
1 2.5 5 34 480 4
10 25 50 340 4800 40
20 50 100 680 9600 80
50 125 250 1700 24000 200
96 240 480 3264 46080 384
3. Prepare a crushed ice bath
4. Transfer 5µl of each amplified DNA sample into the corresponding well of a clean 96
well PCR plate.
5. Add 2.5µl Denaturation Buffer to each well of the PCR plate and mix thoroughly by
pipetting up and down. Incubate at room temperature (20° C to 24° C) for 10min.
6. Add 5µl Neutralisation Buffer with pipette to each well of the PCR plate, and mix
thoroughly.
7. Place PCR plate on ice bath.
2.2.4 Hybridisation
1. Add 38µl hybridisation mixture to each well.
2. Cover with tray seal and give the PCR plate a quick mix using the vortex.
3. Place PCR plate into the pre-heated (60° C) Thermal cycler, cover with PCR pad and
close and tighten lid. Incubate for 15 min.
4. Remove the PCR plate seal and quickly add 100µl Wash Buffer to each well.
5. Cover PCR plate with plate seal and centrifuge plate for 5min at 1000-1300g.

68
6. Remove the tray seal, then remove the wash buffer by dumping/flicking plate
upside down. Gently pat on absorbent paper 3 times to remove any residual liquid.
7. Repeat steps 4 to 6 two more times for a total of three wash steps.
8 Prepare the appropriate volume of 1x SAPE solution at the third centrifugation stage
(Table 7).
Table 7. SAPE volume requirements per sample.
Number of tests SAPE Stock Volume (µl) SAPE Buffer Volume (µl)
1 0.5 49.5
10 5.0 495.0
20 10.0 990.0
50 25.0 2475.0
96 48.0 4752.0
2.2.5 Labelling
1. Add 50µl of 1x SAPE solution to each well of the PCR plate.
2. Cover plate with seal and vortex thoroughly at low speed.
3. Place PCR plate into the pre-heated (60° C) Thermal cycler, cover with PCR pad and
close lid. Incubate for 5min.
4. Remove the PCR plate seal and quickly add 100µl Wash Buffer to each well.
5. Cover PCR plate with plate seal and centrifuge plate for 5min at 1000-1300g.
6. Remove wash buffer by dumping/flicking plate upside down.
7. Add 70µl Wash Buffer to each well and gently mix by pipetting.
8. Transfer contents of each well to a 96 well V-bottom microplate (reading plate)
using an 8-channel pipette. To avoid contamination use fresh pipette tips each time.

69
9. Cover reading plate with seal and aluminium foil. Keep in dark and at 4° C until ready
to read using LABScan™ Flow Analyser.
2.2.6 Data Analysis - OneLambda HLA Fusion™
Data analysis for the HLA assays are performed with the software package HLA
Fusion™. The LABType® analysis feature of the program analyses Luminex.csv output
files and is based on catalogue specifications provided with the software. Import the
data files as specified by the manufacturer.
The analysis software establishes the HLA type by firstly categorising each of the beads
via its internal fluorescence, then determining whether a probe is bound or not by the
strength of external fluorescence on that bead produced by the SAPE.

70
2.3 Serological HLA typing
2.3.1 Isolation of T and B lymphocytes
1. Centrifuge 9mls ACD blood samples at 1800rpm for 10 minutes with the brake off.
2. Remove the platelet rich plasma and replace with citrated phosphate buffered
saline (PBSC).
3. Add 50µl of class I Dynabeads® or 80µl of class II Dynabeads® and mix on a rotator
for 5 minutes.
4. Place on a Dynal® magnet for 2 minutes and remove supernatant.
5. Add 9mls PBSC and incubate at room temperature for 2 minutes.
6. Place on a Dynal® magnet for 2 minutes and remove supernatant.
7. Repeat steps 5 and 6.
8. Add McCoys 5A tissue Culture Medium + 5% Heat inactivated Foetal Calf Serum
(HIFCS).
9. Using a Hamilton syringe spot 1ul of cell suspension in triplicate onto an oiled
Terasaki tray.
10. Add 5ul Fluoroquench™ (Acridine orange / Ethidium bromide) stain to each well.
Allow cells to settle for approximately 20 minutes.
11. View the cells under the fluorescent microscope to determine cell concentration
and viability. Concentration is adjusted by addition or removal of 5% FCS/McCoys.
2.3.2 HLA antigen typing using commercial typing trays
Commercial HLA typing trays are prefilled Terasaki trays containing mineral oil, antisera
with well-documented specificity and complement.
1. Add 1µl prepared T cells to 72 well commercial class I typing trays (LM144A and
LM144B, OneLambda Inc) and 1µl B cells to commercial class II typing tray (MDR172,
OneLambda Inc).
2. Incubate trays at room temperature for 1 hour.
Add 5µl Fluoroquench™ staining solution to each well and allow cells to settle for
approximately 20 minutes.

71
3. View the cells under the fluorescent microscope and determine the percentage cell
death in each well.
4. Assign HLA type according to cell reactivity using antisera information.
2.4 Crossmatching by complement-dependent lymphocytotoxicity
2.4.1 Standard (NIH) CDC Crossmatch
1. Add 1µl recipient serum, with 1µl of appropriate controls (Positive and negative) to
an oiled Terasaki tray. Make trays in duplicate for both T and B cell crossmatches.
2. Add 1µl T or B cells using an automated cell dispenser to avoid cross-contamination.
Ensure all wells are thoroughly mixed.
3. Incubate the trays for 45 minutes at room temperature
4. Add 5µl of pooled rabbit complement to each well using an automated dispenser to
avoid cross-contamination.
5. Incubate the trays for 45 minutes at room temperature.
6. Add 5µl Fluoroquench™ stain to each well. Allow cells to settle for approximately 20
minutes.
7. Score the percentage cell death semi-quantitatively under the fluorescent
microscope.
2.4.2 Interpretation of standard crossmatch results
1. A positive or negative crossmatch is determined by comparing the crossmatch score
with the background reactivity i.e. the AB negative control serum.
2. Results are reviewed with other immunological data to identify level of risk.
2.4.3 DTT crossmatch
1. Add 1µl recipient serum, with 1µl appropriate controls (IgG and IgM positive
controls) in triplicate to an oiled Terasaki tray. Make trays in duplicate for both T and
B cell crossmatches.
2. Add 1µl 5mM Dithiothreitol (DTT) to one of the triplicate wells.
3. Add 1µl PBS to a second triplicate well to act as a dilution control.

72
4. Incubate at 37°C for 30 minutes.
5. Add 1µl L-Cystine (saturated solution) to the DTT and PBS wells.
6. Perform steps 2 to 7 of the standard CDC crossmatch as detailed in 2.3.1.
2.4.4 Interpretation of DTT crossmatch results
1. A positive or negative crossmatch is determined by comparing the crossmatch score
with the background reactivity i.e. the AB negative control serum.
2. A crossmatch is considered positive if the neat, DTT and PBS wells are positive.
3. A crossmatch is considered negative if the neat well is negative, or the neat and PBS
wells are positive and the DTT well is negative. Note: The PBS well should retain
reactivity for a valid result. If this well is negative, dilution cannot be excluded as a
cause.

73
2.5 Luminex Antibody Testing
2.5.1 Characterisation of antibodies by Single Antigen bead assay
1. Bring the antibody kit (OneLambda Inc) to room temperature.
2. Centrifuge recipient serum at 14,000 rpm for 10 minutes to remove any debris / fat.
3. Place 20µl serum into a 96 well V-bottomed microplate.
4. Add 2.5µl Class I or Class II Single Antigen beads to each well. Ensure the vial
containing the beads is well vortexed prior to use.
5. Cover with plate seal and incubate in the dark on a shaker for 30 minutes.
6. Make stock wash buffer by diluting the 10 x concentrate with sterile deionised
water.
7. After incubation, add 150µl wash buffer to each well using a 8-channel pipette.
8. Cover with fresh plate seal and centrifuge at 1400g for 5 minutes.
9. Remove wash buffer by dumping / flicking plate upside down.
10. Gently pat on absorbent tissue 5 times and dry vortex.
11. Add 200µl wash buffer to each well and cover with a fresh plate seal.
12. Centrifuge at 1400g for 5 minutes.
13. Prepare secondary conjugate by diluting 1µl FITC conjugated Goat anti-human IgG
in 99µl wash buffer for each sample.
14. Repeat steps 9 to 12. Remove wash buffer by dumping / flicking plate upside down.
15. Add 100µl diluted secondary conjugate to each well and cover with a fresh plate
seal.
16. Incubate in the dark on a shaker for 30 minutes.
17. Centrifuge at 1400g for 5 minutes.
18. Remove secondary conjugate by dumping / flicking plate upside down.
19. Gently pat on absorbent tissue 5 times and dry vortex.
20. Add 200µl wash buffer to each well and cover with a fresh plate seal.
21. Centrifuge at 1400g for 5 minutes.
22. Remove wash buffer by dumping / flicking plate upside down.
23. Gently pat on absorbent tissue 5 times and dry vortex.
24. Repeat steps 20 to 23.
25. Add 65µl cold PBS to each well.

74
26. Cover plate with seal and aluminium foil. Keep in dark and at 4° C until ready to
read using LABScan™ Flow Analyser.
2.5.2 Data Analysis - OneLambda HLA Fusion™
Data analysis for the HLA assays is performed with the software package HLA Fusion™.
The LABScreen® analysis feature of the program analyses Luminex.csv output files and
is based on catalogue specifications provided with the software. Import the data files
as specified by the manufacturer.
The analysis software establishes the antibody specificity by firstly categorising each of
the beads via its internal fluorescence, then determining whether a probe is bound or
not by the strength of external fluorescence on that bead produced by the FITC.

75
2.6 Statistical Analysis
Statistical analyses were performed by using SPSSv18 (SPSS Inc., Chicago IL, USA). For
categorical data Fisher's exact test or Pearson's chi-square tests were used. Parametric
data were compared by ANOVA or t-test, and for non parametric data Mann–Whitney
U test or Kruskal–Wallis one-way ANOVA was used. Comparisons of within group
differences by z-test were made with Bonferroni adjustment reported at the p < 0.05
level. Time to event of interest (AMR, graft and patient survival) was estimated by the
method of Kaplan–Meier and Cox proportional hazard regression analysis with the
predictor satisfying the proportional hazard assumption. Covariates examined were
HLA-antibody at entry, rejection, gender, re-transplantation, and delayed graft
function. Results were expressed as hazard ratios (HR) with 95% CI.

76
Chapter 3
Pre-transplant donor specific anti-HLA
antibody is associated with antibody-
mediated rejection, progressive graft
dysfunction and patient death.

77
Pre-transplant donor specific anti-HLA antibody is associated with antibody-
mediated rejection, progressive graft dysfunction and patient death.
Samantha J Fidler, Ashley B Irish, Wai Lim, Paolo Ferrari, Campbell S Witt, Frank T
Christiansen
The long-term clinical outcomes in patients with antibodies detected by Luminex single
antigen bead assay in the context of a negative CDC crossmatch are unclear. Previous
studies have shown varying results and significance. We sought to elucidate the clinical
significance of Luminex-defined antibodies in a cohort of patients transplanted with a
negative CDC T cell crossmatch in an era before Luminex antibodies were routinely used.
We retrospectively tested pre-transplant sera from a cohort of Western Australian kidney
transplant patients by Luminex single antigen bead and stratified patients by class of
antibody and looked at the long-term effects of such antibodies on clinical outcome.
These findings were published in:
Transplant Immunology 2013; 28: 148-153
Contributions:
SJF Performed all antibody assays, participated in study design,
participated in data analysis, prepared the manuscript
ABI Participated in study design, participated in data analysis, participated
in writing of the manuscript
WL, PF, CSW, FT Participated in study design, participated in writing of the manuscript

78
Pre-transplant donor specific anti-HLA antibody is associated
with antibody-mediated rejection, progressive graft
dysfunction and patient death
Samantha J. Fidler a, b, 1, Ashley B. Irish c, d, 1, Wai Lim e, 2, Paolo Ferrari f, 2,
Campbell S. Witt c, d, 3, Frank T. Christiansen c, d, 3
a Department of Clinical Immunology, PathWest, Royal Perth Hospital, University of Western Australia, Australia
b School of Pathology and Laboratory Medicine, University of Western Australia, Australia
c Department of Nephrology, Royal Perth Hospital, University of Western Australia, Australia
d School of Medicine and Pharmacology, University of Western Australia, Australia
e Department of Nephrology, Sir Charles Gairdner Hospital, University of Western Australia, Australia
f Department of Nephrology, Fremantle Hospital, University of Western Australia, Australia
a r t i c l e i n f o
Article history: Received 15 April 2013
Received in revised form 28 April 2013
Accepted 1 May 2013
Keywords: Donor-specific antibody (DSA) Kidney transplant
Abbreviations: AMR, Antibody-mediated Rejection; CDC, Complement Dependant Cytotoxicity; cPRA, Calculated
Panel Reactive Antibody; DSA, Donor Specific Antibodies; HB-MFI, Highest bead MFI; DGF, Delayed
Graft Function; BPAR, Biopsy Proven Acute Rejection; MFI, Mean Fluorescence Intensity; SAB,
Single Antigen Bead.
* Corresponding author at: Department of Clinical Immunology, PathWest, Royal Perth Hospital, Wellington Street,
Perth, WA 6000, Australia. Tel.: +61 8 9224 1144; fax: +61 8 9224 2920.
E-mail address: [email protected] (S.J. Fidler).
1 Participated in data analysis, performance of the research and writing of the paper.
2 Participated in performance of the research.
3 Participated in data analysis and writing of the paper.

79
a b s t r a c t
Background: The long term effect of donor specific antibodies (DSA) detected by
Luminex Single Antigen Bead (SAB) assay in the absence of a positive complement-
dependant cytotoxicity (CDC) crossmatch is unclear. DSA at the time of transplant
were determined retrospectively in 258 renal transplant recipients from 2003 to 2007
and their relationship with rejection and graft function prospectively evaluated. After
a median of 5.6 years follow-up 9% of patients had antibody mediated rejection (AMR)
(DSA 11/37(30%), DSA-Neg 13/221 (6%), HR 6.6, p < 0.001). Patients with anti-HLA
class II (HR 6.1) or both class I + II (HR 10.1) DSA had the greatest risk for AMR. The
Mean Fluorescent Intensity (MFI) of the DSA was significantly higher in patients with
AMR than those with no rejection (p = 0.006). Moreover, the strength of the antibody
was shown to be important, with the risk of AMR significantly greater in those
with DSA > 8000 MFI than those with DSA < 8000 MFI (HR 23, p < 0.001). eGFR
progressively declined in patients with DSA but was stable in those without DSA (35.7
± 20.4 mls/min vs 48.5 ± 22.7) and composite patient and graft survival was
significantly worse in those with class II (HR 2.9) or both class I + II (HR 3.7) but not
class I DSA. Class II DSA alone, or in combination with class I DSA had the strongest
association with graft loss and patient death. Patients with DSA not only have
increased rates of acute AMR, but also chronic graft dysfunction, graft loss and death.
Antibody burden quantified by SAB assay may identify patients at highest
immunological risk and therefore influence patient management and improve long-
term patient outcome.
Introduction
The use of the CDC T cell crossmatch for the detection of preformed anti-HLA class I
antibody to eliminate hyperacute rejection has allowed renal transplantation to
become the preferred method of management of end stage renal disease (ESRD) in
eligible patients. Advances in immunosuppressive therapies have also reduced acute
cellular rejection rates to very low levels [1]. However, despite these advances,

80
improving long-term graft survival remains problematic [2]. Increasingly the role of
antibody mediated graft injury, manifested either as acute humoral rejection or
chronic AMR (transplant glomerulopathy), has been recognised as an important,
potentially modifiable cause of graft attrition [3–6].
The introduction of sensitive and specific solid phase antibody detection assays allow
detection of lower levels of antibody than those associated with a positive CDC T- or B-
cell crossmatch. These assays can accurately determine the strength and specificity of
antibodies, thereby improving the ability to examine their role in graft rejection. We,
and others, have previously shown that the presence of anti-HLA antibodies detected
after transplant is associated with a significant risk of subsequent graft loss [4,7–9]
though it was not known whether these antibodies were present at the time of trans-
plant or arose de novo. However, there is contradictory data on the significance of
antibodies detected only by solid phase assay in the presence of a negative T-cell CDC
crossmatch at the time of transplant. Whilst some recent studies have shown that DSA
at the time of renal transplant are associated with increased risk of acute AMR [10–12]
when the crossmatch is positive and others have shown that even with a negative
crossmatch [9,12–15], pre-transplant DSA are associated with early AMR and
rejection, there is little information on the influence of pre-transplant DSA on long
term renal function.
Current literature is unclear in terms of the importance of class I versus class II versus
strength of DSA with respect to AMR and graft loss, and these differences may be
related to differences in transplant management and immunosuppressive protocols.
We initially set out to determine how our data sit with respect to other publications in
terms of AMR and graft loss so that graft function, as measured by eGFR, could be
viewed in the context of the rest of our data.
Results presented here validate the association between pre- transplant DSA and
AMR. We show that, like some others, classes I and II DSA are more important than
either class I or II alone for AMR. However, we further propose that the class of DSA
may be unimportant and the effects of DSA on graft rejection and outcome can be
explained by antibody strength. These findings may help to explain the differing
importance of classes I and II antibody between centres. We also show that DSA is
associated with non-AMR though not as strongly as with AMR.

81
Subjects and methods
Patients
We studied 267 patients with a negative T cell CDC crossmatch who underwent 270
consecutive renal transplants between June 2003 and October 2007. We excluded one
patient with a simultaneous liver–kidney transplant, and those patients who died (n =
3) or lost their graft within the first 30 days of transplantation (n = 8; 3 of whom were
subsequently re-transplanted within the period of observation), leaving 258 patients
and allografts. Of the 258 patients, 173 were also B cell crossmatched. 246 patients
received a kidney transplant in Perth, Western Australia and 12 patients received
simultaneous kidney–pancreas transplants at Westmead Hospital in New South Wales.
Patients were managed with varying immunosuppressive regimes but all patients
received a Calcineurin inhibitor (CNI) (Tacrolimus or Cyclosporine) at the time of
transplantation in combination with mycophenolate mofetil or mycophenolate sodium
and corticosteroids. Consistent with Australian practice, the IL2R Antibody Basiliximab
was commonly used for induction but the use of anti-T-cell preparations for induction
was rare (Table 1). The need for biopsy, diagnosis and management of rejection,
medication adjustments was determined by the caring clinician and was not protocol
driven.
Prospective testing
The Department of Clinical Immunology (DCI), Royal Perth Hospital performed all T
and B-cell CDC crossmatching against WA donors. For organs donated from other
Australian states the crossmatch was performed at the state of donor origin. Pre-
transplant HLA typing and HLA antibody testing of the kidney recipients was
performed by DCI. All deceased donors were typed for HLA-A, -B, -DR, -DR51, -DR52, -
DR53 and -DQ by serology using commercial monoclonal antibody trays (OneLambda
Inc). Living donors and all potential recipients were typed for HLA-A, -B, -DRB1 by DNA
sequencing based typing (In-house) [16].
Donor and recipient HLA-A, -B and -DR matching, patient sensitisation (PRA) and
waiting time were considered in recipient allocation. Antibodies directed against HLA-
A and -B were determined by CDC crossmatch or Luminex PRA bead (OneLambda Inc).

82
The presence of class I DSA in current or historical sera and previous donor class I or
class II HLA mismatches (HLA-A, -B and -DR only) were exclusions for organ allocation.
A negative pre-transplant T cell CDC crossmatch using current (within 3 months prior
to the transplant) and historical sera was mandatory for transplantation. B cell
crossmatching was performed for 67% of the patients, however a positive B cell
crossmatch was not considered an absolute contraindication to transplantation.
Retrospective testing
For this study, sera collected at the time of transplant were screened retrospectively
for anti-HLA class I and class II antibodies using the Luminex Mixed Screen assay and
those with a positive screen were characterised for HLA class I and/or class II antibody
specificity using Single Antigen beads (LABScreen Single Antigen beads, OneLambda
Inc). The assays were performed in accordance with the manufacturer's protocol.
Antibodies were considered to be positive if the MFI for a particular bead was greater
than 500. HLA antibodies with an MFI > 500 directed against a donor HLA antigen
(HLA-A, -B, -C, -DRB1, -DRB3,4,5, -DQB1, or -DPB1) were considered to be DSA.
Calculated PRA (cPRA) was determined as the frequency of antibody against HLA-A, -B,
-DRB1, DRB3,4,5 and -DQ antigen in a reference cohort of 200 Australian individuals.
Donors were typed at all HLA loci (HLA-A, -B, -C, -DRB1, -DRB3,4,5, -DQB1 and -DPB1)
by in-house sequence based typing [16].
Clinical outcome parameters
Delayed graft function (DGF) was defined as the need for dialysis within the first 48 h
of transplantation. Graft loss was defined as the return to dialysis. All rejection
episodes were proven by biopsy, undertaken when clinically indicated, whilst those
episodes clinically defined in the absence of biopsy confirmation were not considered
biopsy proven acute rejection (BPAR). Histological reporting of renal biopsies was
undertaken by the local histopathologists as part of routine clinical care and was made
without information as to the presence or absence of DSA. The biopsy findings were
graded according to the Banff Classification 2003 [17]. BPAR that did not fulfil the

83
criteria for AMR was termed Non-AMR. The first BPAR was used to construct time to
event analysis and where multiple rejections occurred, the highest reported grade was
recorded. Time to AMR was recorded as a separate event to allow analysis by rejection
type (AMR vs non-AMR). eGFR was calculated at 1, 2, 3, 6 and 12 months and then
annually according to the abbreviated MDRD formula.
Statistical analysis
Statistical analyses were performed by using SPSSv18 (SPSS Inc, Chicago IL, USA) and
Stata (Version 11, StataCorp, Texas, USA). For categorical data Fishers Exact Test or
Pearson's chi-square tests were used. Parametric data were compared by ANOVA or t-
test, and for non parametric data Mann–Whitney U test or Kruskall Wallis 1 way
ANOVA were used. Time to event was estimated by the method of Kaplan–Meier and
Cox Proportional Hazards was used to determine Hazard Ratio's. Predictors of time
dependent eGFR estimates were determined by a Longitudinal Mixed Model with time
being treated as a random effect with observations at multiple but irregular time
intervals. Mean eGFR was estimated over the months following transplant. Graft loss
was censored when no further eGFR estimates occurred due to return to dialysis or
death.
Results
Features of the patient groups
Patients were initially divided into 3 groups according to their antibody status at the
time of transplant: i) DSA group n = 37 (14%) — patients with HLA antibody with
MFI >500 against one or more donor HLA antigens, ii) Non-DSA group n = 28 (11%) —
patients with HLA antibodies (MFI >500) but not directed against donor antigens or iii)
No-antibody group n = 193 (75%) — patients with no HLA antibodies defined using the
MFI cut-off of <500 or with a negative antibody screen. Baseline clinical and
demographic data of these groups is shown in Table 1. In the DSA group 13 (35%)
patients had class I DSA only, 11 (30%) had class II DSA only and 13 (35%) patients had
both class I and II DSA. Of the 258 patients, 173 were also B cell CDC crossmatched
(BXM). Only 4 patients had a positive BXM and DSA, however the Australian algorithm

84
at the time did not exclude patients with positive BXM. Thirty patients had a positive
BXM with no DSA, and only one patient with DSA was not B cell crossmatched. As
expected, patients in the DSA and non-DSA groups were more commonly female (p =
0.003), were more likely to have received prior transfusion (p = 0.011) and more likely
to have undergone prior kidney transplant (p < 0.001).
Table 1. Demographic and clinical features at time of transplant according to entry
antibody status. Results shown as mean ± SD, median (IQR) or proportion.
Pre-transplant DSA is associated with AMR and non-AMR BPAR
Because the non-DSA group had similar rejection events (Table 1) to the No-antibody
group, these groups were combined as the DSA-Neg group (n=221) in subsequent analysis.
Compared with the DSA-Neg group, patients with DSA had a significantly increased risk of
non-AMR (Figure 1a) (HR 1.9, P=0.033) and especially AMR (Figure 1b). 30% of the DSA
group experienced AMR compared with only 6% of the DSA-Neg group (HR 6.6, P<0.001).
AMR showed a bi-modal distribution: AMR occurred early with a median time of around 1
month (39 days) in the DSA group compared to a median time of 49 months in the DSA-
Neg group (Figure 1b). In the 26 DSA patients who did not have AMR, 22 (85%) received at
least 1 ‘for cause’ biopsy but histological features consistent with AMR were not identified.
The risk of AMR varied according to the specificity of HLA antibody at the time of
transplantation (Fig. 1c). Compared with the DSA-Neg group, patients with only class I

85
or only class II DSA had a 4–6 fold increased risk of AMR and those with both class I +
II DSA had the highest risk (HR 10.1).
Figure 1a. Time to first biopsy-proven acute rejection (BPAR) excluding 24
patients with AMR by entry DSA (HR 1.9, 95%CI 1.1–1.3, p = 0.033).

86
Figure 1b. Time to Antibody Mediated Rejection by entry DSA status (HR 6.6,
95%CI 2.9– 14.7, p < 0.001).
Figure 1c. Time to Antibody Mediated rejection by class of DSA at entry (Class I
HR 4.4, 95%CI 1.3–15.5, p = 0.021; Class II HR 6.1, 95%CI 1.7–21.4, p = 0.005;
Class I + II HR 10.1, 95%CI 3.5–28.2, p < 0.001).
b
a

87
Strength of pre-transplant DSA is associated with AMR and non-AMR
In order to determine whether the strength of DSA could be correlated with rejection
we compared the MFI of the highest DSA bead amongst the various rejection
categories (Fig. 2a). There was no significant difference between the strength of HLA-
antibody defined as the highest MFI, or in the breadth of sensitisation defined as
cPRA, between the DSA group and non-DSA groups. However, in the patients with
DSA, the MFI of the highest DSA (HB-MFI) bead was significantly higher in those
with both class I + II DSA (Mean MFI 8070) than those with class I alone (3549) or class
II DSA alone (2540) (p = 0.004) In most cases this was due to a high class II antibody
(data not shown).
Amongst the 37 patients with DSA, the HB-MFI in the AMR group was significantly
higher than the HB-MFI in patients with no rejection (Fig. 2a) (p = 0.006). Additionally,
analysis of time to AMR by HB-MFI showed that the risk of AMR was significantly
greater when the HB-MFI was >8000 compared to those with an HB-MFI between 500
and 8000 (HR 23 95%, p < 0.001) (Fig. 2b). This same effect was observed when the
sum of the DSA beads was analysed. In our laboratory, a positive CDC crossmatch is
anticipated with an MFI of >8000 (data not shown).
Figure 2a. Strength of antibody determined by the MFI of the highest DSA bead
in the 37 patients with DSA according to rejection category (No BPAR, non-
AMR and AMR) (p = 0.006 AMR versus No BPAR).

88
Figure 2b. Time to AMR by category of the MFI of the highest DSA bead
compared with No-Antibody (p < 0.0001, HR MFI 500–8000 3.0 (0.9–9.0) p =
0.06 and HR >8000 = 23 (8.9–59)).
Pre-transplant DSA is associated with graft loss and recipient death
There was a trend for death-censored graft loss to be associated with DSA at the
time of transplant: 16% (6/37) of the DSA group lost their graft compared to 9%
(21/221) of the DSA-Neg group (p = 0.075). There was a significant increase in the
composite outcome of the combined patient and graft loss in the DSA group
compared to the DSA-Neg group (Fig. 3a). All 6 graft losses in the DSA group were
directly attributed to rejection episodes whilst in the DSA-Neg group 18/21 graft
losses were attributed to chronic allograft nephropathy, acute or chronic rejection
and 3/21 were due to recurrent disease (n = 2) or BK virus nephropathy (n = 1).
We next examined the effect of the HLA class of the DSA upon patient and graft
loss. In the DSA group, patients with both class I + II antibodies had a
statistically significant increase in both cumulative death-censored graft loss
(HR 4.9, p = 0.022) and combined patient or graft loss (HR 3.7, p = 0.003) (Fig.
3b). Actual graft survival in patients with class I DSA only, class II only, class I + II
DSA and DSA-Neg was 92% (12/13), 62% (7/11), 54% (7/13) and 83% (184/221)
respectively.

89
Figure 3a. Time to Patient or Graft Loss by entry DSA (DSA versus DSA negative
HR 2.1, 95%CI 1.1–4.0, p = 0.030).
Figure 3b. Time to patient or graft loss by entry class of DSA. There was a
significantly higher incidence of patient or graft loss in those with class II DSA
(HR 2.9, 95%CI 1.0–8.0, p = 0.047) and those with class I + II DSA (HR 3.7,
95%CI 1.6–8.9, p = 0.003) but not class I DSA.

90
Pre-transplant DSA is associated with chronic graft dysfunction
A longitudinal model incorporating established clinical predictors and additional
exploratory predictors having a p < 0.1 in univariate analyses, including DSA, was used
to determine independent longitudinal predictors of eGFR. There was a significant
continuous decrement in eGFR over time within the DSA group when compared with
the DSA-Neg group which was apparent as early as 1 year post transplant (Fig. 4). After
6 years of follow up the estimated mean eGFR of the DSA group was 35.7 ± 20.5
mls/min (n = 8) compared to 48.5 ± 22.7 (n = 104) for those in the DSA-Neg group.
Factors shown to be significantly and independently associated with loss of eGFR over
the time of follow-up were increased donor age, female gender, DGF, AMR, DSA at the
time of transplant and CNI use (Cyclosporine vs Tacrolimus) but not non-AMR (Table
2).
Table 2. Longitudinal mixed-effects models of predictors of eGFR (coefficient and
95% CI = mls/min) across the observed follow-up (median 68 months) incorporating
factors identified as univariate predictors of eGFR. (Random Effects of subject ID and
time since transplant were not shown). IR test of mixed model versus linear
regression χ2 = 1074, p < 0.0001.

91
Figure 4. Longitudinal mixed model of mean observed eGFR by entry DSA status
over time p < 0.0001. Observed mean eGFR at 72 months is 48.5 ± 22.7 (n =
108) in the no-DSA (negative) group versus 35.7 ± 20.4 (n = 8) in the DSA
(positive) group.
Discussion
This study confirms that the presence of pre-transplant anti-HLA antibody directed
against donor antigens detected by Luminex Single Antigen Bead assay with a negative
CDC T-cell crossmatch impacts on subsequent graft outcome. Such antibodies are
significantly associated with an increased risk of rejection, as previously reported by
others [9,12–15] and contrary to the findings of the Collaborative Transplant Study
group [18]. However results presented here further these findings and suggest that
DSA is also associated with poorer long term graft function as shown by declining
eGFR, graft loss and patient death. Importantly, the effect of these DSA on loss of
eGFR is independent of their effects on AMR. Moreover, the risk is graded and appears
greatest in those with both class I + II DSA who also have the highest antibody levels,
and intermediate in those with either class I only or class II only DSA. In addition, we
demonstrate that irrespective of class I or class II specificity, the MFI of the highest
DSA bead (> 8000 MFI) was predictive of AMR consistent with the concept that
antibody burden as quantified by SAB is associated with risk.
14% of patients had DSA detected in their pre-transplant serum and AMR occurred in
11/37 (30%) of the DSA group, compared with 6% of patients in the DSA-Neg group

92
(HR = 6.6). Only patients with DSA had early AMR, and in those without DSA at entry
AMR occurred a median of 4 years after transplant and was associated with the
development of de novo DSA (data not shown). BPAR in the absence of AMR (i.e. T cell
mediated rejection) was also significantly associated with the presence of DSA,
indicating that both cellular and antibody mediated rejection are associated with DSA,
and that DSA prospectively identifies patients at the highest risk of all types of
rejection.
Although both class I and class II DSA were associated with an in- crease in rejection,
the presence of both class I + II DSA together appeared to confer the greatest risk (HR
= 10). This finding is contrary to many of the previously published studies in which
class I DSA shows the greatest effect [19–21,23], but supports other studies [14,21,22]
showing pre-existing class II DSA to be associated with rejection and graft loss. The
exclusion of strong class I DSA by pre-transplant screening and the exclusion of those
with a positive prospective T cell CDC crossmatch may in part explain the lack of a
significant class I effect in our study.
We have examined the relevance of the absolute values of the MFI of HLA antibody.
Patients with DSA had similar average MFI when compared with patients with non-
DSA antibody. They also had similar antecedents of sensitisation (more females, higher
prior transfusion or re-transplants) yet the outcomes of patients with non-DSA were
similar to those without any antibody suggesting that pathogenicity of antibody
requires donor specificity. We have demonstrated that higher antibody strength
measured as MFI increases the risk of AMR. Patients with both class I + II DSA had
higher MFI and the highest risk of AMR. When considering the MFI of the highest DSA
bead, an MFI > 8000 (a value which in our laboratory is associated with a positive CDC
crossmatch) conferred a > 20 fold increased risk of AMR. These data suggest that the
risk of AMR is better associated with the absolute strength of DSA rather than HLA
class, and suggests a threshold of antibody burden that triggers an acute humoral
pattern of injury.
In our study we examined the effects of DSA and AMR on long- term graft function.
We have shown a significant and continuous de- crease in graft function as measured
by eGFR in the DSA group. This loss is evident by 1 year post-transplant, and after 6
years of follow-up equates to a difference of 13 mls/min eGFR between the groups.

93
Furthermore, in the mixed-effect model we have shown that both DSA (-9mls/min)
and AMR (-3mls/min) are independently associated with loss of eGFR suggesting that
DSA have both acute and chronic humoral mechanisms of graft injury which translate
into loss of kidney function, reduced eGFR and premature graft loss. These incident
data are consistent with other prevalent studies [24–26] that identify chronic antibody
injury with graft impairment, proteinuria and early graft failure.
Most importantly DSA was associated with not only AMR but also increased graft loss
and patient death (HR = 2.1), and this was most marked in those with class II or class I
+ II DSA. Many patients died with a functioning graft suggesting that DSA is associated
with all cause mortality. Immunosuppressive therapy given to patients with DSA may
be associated with an increased risk of infection, vascular disease and/or malignancy
and therefore results presented here suggest that avoidance of pre-transplant DSA
may not only avoid acute AMR episodes but may actually improve patient morbidity
and mortality.
Detection of DSA in immediate pre-transplant serum in the absence of a positive T cell
CDC crossmatch is a significant risk factor for subsequent poorer graft outcome in
terms of both acute rejection episodes, long-term renal function and death. This risk
may be better predicted by the strength (MFI) of DSA and in our laboratory we now
consider an MFI >8000 regardless of crossmatch, to be a contraindication to
transplant. Alternative strategies including de-sensitisation, kidney-exchange
programmes and/or modification to Immunosuppressive regimens might be preferred
in patients with pre-existing high-level DSA in order to prolong the graft life and
reduce risk of rejection. Further studies to determine the utility of quantification of
the burden of antibody as measured by MFI in prediction of clinical risk are warranted.

94
Acknowledgements
The authors wish to acknowledge the clinicians and transplant nurses at Royal Perth
Hospital, Sir Charles Gairdner Hospital and Fremantle Hospital in Western Australia
involved in the collection of this data. We wish to thank the Department of Clinical
Immunology, Royal Perth Hospital for compatibility testing of the patients in this
study.
We also wish to thank Michael Phillips for statistical advice and help with statistical
analysis and A/Prof Lloyd D'Orsogna for critical reading of the manuscript.
Disclosure
This is an original work and the manuscript or parts of it have not been submitted
elsewhere for publication. All authors have read and approved submission of the
manuscript, and that material in the manuscript has not been published and is not
being considered for publication elsewhere in whole or part in any language except as
an abstract.

95
References
[1] Ekberg H, Tedesco-Silva H, Demirbas A, Vitko S, Nashan B, Gurkan A, et al. Reduced
exposure to calcineurin inhibitors in renal transplantation. N Engl J Med 2007;357:
2562–75.
[2] Lamb KE, Lodhi S, Meier-Kriesche HU. Long-term renal allograft survival in the United
States: a critical reappraisal. Am J Transplant 2011; 11: 450–62.
[3] Terasaki P, Mizutani K. Antibody mediated rejection: update 2006. Clin J Am Soc
Nephrol 2006; 1: 400–3.
[4] Langan LL, D'Orsogna L, Park LP, Hughes TL, Irish A, Luxton G, et al. HLA antibodies and
soluble CD30 are associated with poor renal graft outcome: updated results of a single-
center cross-sectional study. Clin Transpl 2006: 219–25.
[5] Kaposztas Z, Podder H, Mauiyyedi S, Illoh O, Kerman R, Reyes M, et al. Impact of
rituximab therapy for treatment of acute humoral rejection. Clin Transplant 2009; 23:
63–73.
[6] Einecke G, Sis B, Reeve J, Mengel M, Campbell PM, Hidalgo LG, et al. Antibody-mediated
microcirculation injury is the major cause of late kidney transplant failure. Am J
Transplant 2009; 9: 2520–31.
[7] Terasaki PI, Ozawa M. Predicting kidney graft failure by HLA antibodies: a
prospective trial. Am J Transplant 2004; 4: 438–43.
[8] Cooper JE, Gralla J, Cagle L, Goldberg R, Chan L, Wiseman AC. Inferior kidney allograft
outcomes in patients with de novo donor-specific antibodies are due to acute rejection
episodes. Transplantation 2011; 91: 1103–9.
[9] Gebel HM, Bray RA, Nickerson P. Pre-transplant assessment of donor-reactive, HLA-
specific antibodies in renal transplantation: contraindication vs. risk. Am J Transplant
2003; 3: 1488–500.
[10] Bachler K, Amico P, Honger G, Bielmann D, Hopfer H, Mihatsch MJ, et al. Efficacy of
induction therapy with ATG and intravenous immunoglobulins in patients with low-
level donor-specific HLA-antibodies. Am J Transplant 2010; 10: 1254–62.

96
[11] Bentall A, Cornell LD, Gloor JM, Park WD, Gandhi MJ, Winters JL, et al. Five-year
outcomes in living donor kidney transplants with a positive crossmatch. Am J
Transplant 2013; 13: 76–85.
[12] Eng HS, Bennett G, Tsiopelas E, Lake M, Humphreys I, Chang SH, et al. Anti-HLA
donor-specific antibodies detected in positive B-cell crossmatches by Luminex
predict late graft loss. Am J Transplant 2008; 8: 2335–42.
[13] Honger G, Hopfer H, Arnold ML, Spriewald BM, Schaub S, Amico P. Pretransplant IgG
subclasses of donor-specific human leukocyte antigen antibodies and development of
antibody-mediated rejection. Transplantation 2011; 92: 41–7.
[14] Otten HG, Verhaar MC, Borst HP, Hene RJ, van Zuilen AD. Pretransplant donor-specific
HLA class-I and -II antibodies are associated with an increased risk for kidney graft failure.
Am J Transplant 2012; 12: 1618–23.
[15] Lefaucheur C, Suberbielle-Boissel C, Hill GS, Nochy D, Andrade J, Antoine C, et al. Clinical
relevance of preformed HLA donor-specific antibodies in kidney transplantation. Am J
Transplant 2008; 8: 324–31.
[16] Sayer D, Whidborne R, Brestovac B, Trimboli F, Witt C, Christiansen F. HLA-DRB1 DNA
sequencing based typing: an approach suitable for high throughput typing including
unrelated bone marrow registry donors. Tissue Antigens 2001; 57: 46–54.
[17] Racusen LC, Halloran PF, Solez K. Banff 2003 meeting report: new diagnostic insights
and standards. Am J Transplant 2004; 4: 1562–6.
[18] Susal C, Ovens J, Mahmoud K, Dohler B, Scherer S, Ruhenstroth A, et al. No association
of kidney graft loss with human leukocyte antigen antibodies detected exclusively by
sensitive Luminex single-antigen testing: a Collaborative Transplant Study report.
Transplantation 2011; 91: 883–7.
[19] Rodriguez LM, Paris SC, Arbelaez M, Cotes JM, Susal C, Torres Y, et al. Kidney graft
recipients with pretransplantation HLA CLASS I antibodies and high soluble CD30 are at
high risk for graft loss. Hum Immunol 2007; 68: 652–60.
[20] Susal C, Opelz G. Kidney graft failure and presensitization against HLA class I and class II
antigens. Transplantation 2002; 73: 1269–73.

97
[21] Susal C, Opelz G. Good kidney transplant outcome in recipients with presensitization
against HLA class II but not HLA class I. Hum Immunol 2004; 65: 810–6.
[22] Song EY, Lee YJ, Hyun J, Kim YS, Ahn C, Ha J, et al. Clinical relevance of pretransplant
HLA class II donor-specific antibodies in renal transplantation patients with negative T-
cell cytotoxicity crossmatches. Ann Lab Med 2012; 32: 139–44.
[23] Lefaucheur C, Loupy A, Hill GS, Andrade J, Nochy D, Antoine C, et al. Preexisting donor-
specific HLA antibodies predict outcome in kidney transplantation. J Am Soc Nephrol
2010; 21: 1398–406.
[24] Hohage H, Kleyer U, Bruckner D, August C, Zidek W, Spieker C. Influence of proteinuria on
long-term transplant survival in kidney transplant recipients. Nephron 1997; 75: 160–5.
[25] Amer H, Fidler ME, Myslak M, Morales P, Kremers WK, Larson TS, et al. Proteinuria after
kidney transplantation, relationship to allograft histology and survival. Am J Transplant
2007; 7: 2748–56.
[26] Cherukuri A, Welberry-Smith MP, Tattersall JE, Ahmad N, Newstead CG, Lewington AJ,
et al. The clinical significance of early proteinuria after renal transplantation.
Transplantation 2010; 89: 200–7.

98
Chapter 4
Peri-operative third party red blood cell
transfusion in renal transplantation and
the risk of antibody-mediated rejection
and graft loss

99
Peri-operative third party red blood cell transfusion in renal transplantation and
the risk of antibody-mediated rejection and graft loss
Samantha Fidler, Ramyasuda Swaminathan, Wai Lim, Paolo Ferrari, Campbell Witt, Frank
T Christiansen, Lloyd J D’Orsogna, Ashley B Irish
In our previous publication we were able to demonstrate the association of pre-
transplant donor specific antibodies (DSA) detected by Luminex single antigen bead assay
with antibody mediated rejection (AMR) and progressive graft dysfunction. There was a
trend towards graft loss although this did not reach significance. However, a number of
patients with pre-transplant DSA did not develop AMR and we sought to elucidate
reasons for this. A coincidental finding in our preliminary study showed an association of
blood transfusions with AMR. We investigated in this paper the relationship of pre- and
post-transplant blood transfusions in patients with or without DSA.
These findings were published in:
Transplant Immunology 2013; 29: 22-27
Contributions:
SJF Performed all antibody assays, participated in study design,
participated in data collection, participated in data analysis, prepared
the manuscript
ABI Participated in study design, participated in data collection,
participated in data analysis, participated in writing of the manuscript
RS Participated in data collection and analysis
WL, PF Participated in data collection, participated in writing of the
manuscript
CSW, FTC Participated in study design, participated in writing of the manuscript
LD’O Participated in writing of the manuscript

100
Peri-operative third party red blood cell transfusion in renal
transplantation and the risk of antibody-mediated rejection and graft
loss
Samantha Fidler a,b,1, Ramyasuda Swaminathan c,d,2, Wai Lim e,3, Paolo Ferrari f,4,
Campbell Witt a,b,5, Frank T. Christiansen a,b,6, Lloyd J. D'Orsogna a,b,7, Ashley B. Irish c,d,⁎,8
a Department of Clinical Immunology, PathWest, Royal Perth Hospital, Western Australia, Australia b School of Pathology and Laboratory Medicine, University of Western Australia, Australia c Medical Renal Transplant Unit, Royal Perth Hospital, Western Australia, Australia d School of Medicine and Pharmacology, University of Western Australia, Australia e Department of Nephrology Sir Charles Gairdner Hospital, Perth, Western Australia, Australia f Department of Nephrology Fremantle Hospital, Fremantle, Western Australia, Australia
a r t i c l e i n f o
Article history: Received 12 August 2013
Received in revised form 23 September 2013
Accepted 23 September 2013
Keywords: Donor-specific antibody (DSA) Peri-operative transfusion Kidney transplantation Antibody mediated rejection
Abbreviations: AMR, antibody-mediated rejection; RBCT, red blood cell transfusion; cPRA, calculated panel reactive antibody; DSA, donor
specific antibodies; DGF, delayed graft function; BPAR, biopsy proven acute rejection; MFI, mean fluorescence intensity; SAB,
single antigen bead.
* Corresponding author at: Medical Renal Transplant Unit, Royal Perth Hospital, GPO Box X2213, Perth, Western Australia 6847, Australia.
Tel.: +61 8 9224 2162; fax: +61 89224 2160. E-mail address: [email protected] (A.B. Irish).
1 Participated in the performance of research laboratory methods, research design and writing the paper. 2 Participated with data collection and analysis. 3 Participated with data collection and writing the paper. 4 Participated with data collection and writing the paper. 5 Participated in research design, data analysis and writing the paper. 6 Participated in research design and writing the paper. 7 Participated in data analysis and writing the paper. 8 Participated in research design, data collection and analysis and writing the paper.

101
1. Introduction
The presence of pre-transplant anti-HLA antibody directed against the donor antigens
(DSA) in the presence of a negative CDC crossmatch is associated with increased risk of
antibody mediated rejection (AMR) and graft failure [1–3]. HLA antibodies are formed
as a consequence of prior transplantation, pregnancy and blood transfusion due to
exposure to foreign HLA antigens [4–9]. However blood transfusion prior to transplant
is immunomodulatory and appears to reduce the risk of acute allograft rejection and
graft loss despite an increased risk of sensitisation [10–12]. Historically it had been
observed that large volumes of third-party red blood cell transfusion (RBCT) (up to 20
units) over a prolonged period are required to induce enduring antibodies, especially in
males or nulliparous females [4,13–15]. However in the presence of another immune
stimulating process such as pregnancy or transplantation, co-administration of third
party RBCT results in broad HLA antibody production which is more potent and
enduring [6,16,17]. In the current transplant era, transfusion in patients with end stage
kidney disease is less frequent due to the widespread use of epoetins. However during
acute illness or surgery patients may still be exposed to blood products, although
specifically transfusing patients for immunological benefit is no longer routine [18–20].
Leucodepletion of blood products has also been shown not to prevent the risk of
allosensitisation associated with RBCT [14,21–23]. The majority of studies on the role of
blood transfusion were performed in the period before the use of sensitive and specific
solid phase antibody detection assays were available and cell-dependent cytotoxicity
assays were utilised. Although it is established that DSA detected at the time of
transplant is associated with an increased risk of AMR why some patients with DSA
develop AMR and others do not is unclear and may relate to variability in the antibody
subtype, complement binding ability, or the amount or breadth of antibody [1,24–26].
Transfusion in the peri-operative and early post- transplant period depends on
individualised patient management factors and is commonly thought not to be an
immunological stimulus because it is assumed that the concomitant use of
immunosuppression mitigates this risk. We hypothesised that post-transplant
transfusion in patients with preformed HLA antibody may provide additional
allostimulation or immunological recall and increase the risk of AMR. We therefore
investigated the relationship of pre-transplant and peri- operative transfusion in renal

102
transplant recipients with and without pre-transplant HLA antibody determined by
Luminex single antigen bead (SAB) assay.
2. Subject and methods
2.1. Patients
We studied 258 transplant recipients of which 246 patients received a kidney
transplant and 12 patients received a simultaneous pancreas– kidney transplant
between June 2003 and October 2007. Patients were transplanted at 3 tertiary centres
and peri-operative care and decision for transfusions was individualised, clinically
indicated and not mandated by protocol. No donor-specific transfusions occurred.
Leucocyte depleted packed red cells were used. All patients received a calcineurin
inhibitor (CNI) (tacrolimus or cyclosporine) at the time of transplantation in combination
with mycophenolate mofetil or mycophenolate sodium and corticosteroids and the
Interleukin-2 receptor antibody basiliximab was commonly used for induction. The need
for biopsy, medication adjustments and transfusion was determined by the caring
clinical teams and was not protocol driven. Transfusion history was obtained from the
West Australian Red Cross Blood Bank, the Westmead Hospital Transfusion Laboratory,
patient medical records and direct patient interrogation. Patient follow-up was a
median of 67 months (IQR 54–77). Patients provided written consent for participation
in this study.
2.2. Laboratory methods
These are reported in detail elsewhere however stored donor DNA was typed by
sequence based typing at HLA-A, -B, -C, -DRB1, DQB1, DPB1 loci and DRB3, 4, 5 and
DQA1 where required [27]. All recipients were transplanted with a negative T cell CDC
crossmatch. B cell crossmatching was performed for 80% of the patients; however a
positive B cell crossmatch was not considered an absolute contraindication to
transplantation. Sera collected at the time of transplant were screened retrospectively
for anti-HLA class I and/or class II antibodies using the Luminex Mixed Screen assay
(OneLambda Inc.) and those with a positive screen were characterised for HLA class I

103
and/or class II antibodies specificity using single antigen beads (LABScreen Single
Antigen beads, OneLambda Inc.). Antibodies were considered to be positive if the
normalised mean fluorescence intensity (MFI) value for a particular bead was greater
than 500. HLA antibodies with an MFI > 500 directed against a donor HLA antigen were
considered to be DSA.
2.3. Clinical outcome parameters
Transfusion history was recorded as never transfused (No-RBCT), transfused at any
time prior to renal transplant but not after renal transplant surgery (Pre-RBCT), not
transfused prior to transplant but transfused at the time of, or within 30 days of
transplant surgery (Post-RBCT) and transfused both prior to and within 30 days of the
transplant (Pre + Post-RBCT). Delayed graft function (DGF) was defined as the need
for dialysis within the first 48 h of transplantation. Graft loss was defined as the return
to dialysis (i.e. death-censored) unless otherwise indicated. All rejection episodes were
proven by biopsy (BPAR) and the first BPAR was used to construct time to event
analysis and where multiple rejections occurred, the highest reported grade was
recorded. Time to AMR was recorded as a separate event to allow analysis by rejection
type (AMR vs Non-AMR). Treatment of rejection was at the treating clinician's
discretion and was not mandated by protocol. Histological reporting of renal biopsies
was undertaken by the local histopathologists as part of routine clinical care and was
initially made without information as to the presence or absence of DSA (due to
varying laboratory testing and reporting changes over the period of study). The biopsy
findings were graded according to the Banff classification 2003. AMR was defined as
C4d positivity in PTC alone or in conjunction with transplant glomerulitis and/or peri-
tubular capillaritis and/or arteritis, and also in the absence of C4d when transplant
glomerulitis and peritubular capillaritis were detected.

104
2.4. Statistical analysis
Statistical analyses were performed by using SPSSv18 (SPSS Inc., Chicago IL, USA).
For categorical data Fisher's exact test or Pearson's chi-square tests were used.
Parametric data were compared by ANOVA or t-test, and for non parametric data
Mann–Whitney U test or Kruskal–Wallis one-way ANOVA was used. Comparisons of
within group differences by z-test were made with Bonferroni adjustment reported at
the p < 0.05 level. Time to event of interest (AMR, graft and patient survival) was
estimated by the method of Kaplan–Meier and Cox proportional hazard regression
analysis with the predictor satisfying the proportional hazard assumption. Covariates
examined were HLA-antibody at entry, rejection, gender, re-transplantation, and
delayed graft function. Results were expressed as hazard ratios (HR) with 95% CI.
3. Results
Sixty-five patients had pre-transplant HLA-antibody: DSA group n = 37 (14%) and
Non-DSA group n = 28 (11%) while the remaining 193 (75%) patients had no HLA
antibody defined using the MFI cut-off of <500 or with a negative antibody screen.
Baseline clinical and demographic data of these groups is reported in detail
elsewhere and summarised in Table 1. [27] As expected, patients with any HLA
antibody were more commonly female (41/65 vs 53/193, p = 0.003) and more
likely to have undergone prior kidney transplant (20/65 vs 7/193, p < 0.001) and to
have received Pre-RBCT (39/65 vs 70/193, p = 0.011). There was no difference in
haemoglobin between the groups either at time of transplant (DSA 124 ± 19, Non-
DSA 124 ± 18, No-Antibody 124 ± 15 g/L, p = 0.99) or at 30 days post transplant
(DSA 109 ± 17, Non-DSA 113 ± 13, No-Antibody 114 ± 17 g/L, p = 0.19). Patients
with pre-transplant DSA were significantly more likely to have been transfused
within the first 30 peri-operative days (DSA 70%) than those with Non-DSA (43%)
or no HLA antibody (38%, p < 0.001) although the amount of RBCT was not
different [DSA 4 (2–4), Non-DSA 2 (2–4) and No- Antibody 2 (2–4) units median
and IQR, p = 0.17] and > 90% of all post-transplant RBCT given within the first 2
peri-operative days.

105
Table 1. Demographic and clinical features at time of transplant by entry HLA-
antibody.
In order to explore further the relationship between transfusion and pre-
transplant DSA we divided the patients into four groups according to their
transfusion status — No- RBCT, Pre-RBCT, Post-RBCT and Pre + Post-RBCT groups
as previously defined (Table 2). Overall 109/258 (42%) received Pre-RBCT and
111/258 (43%) of patients received Post- RBCT. The prevalence of HLA antibody
amongst these groups varied significantly as expected. The No-RBCT group were
much more likely to have no HLA antibody (86%) than the other groups (p < 0.05).
Conversely however, the Pre + Post-RBCT group were more likely to have DSA (p <
0.05), receive a repeat transplant and less likely to receive a pre-emptive or living
donor transplant, although time on dialysis was similar to those with Pre- and
Post-RBCT. Patients with Pre-RBCT only were significantly less likely to have Non-
AMR rejection than all other groups (p < 0.05, Table 3). Patients in the Pre +
Post-RBCT group were more likely to have DGF than all other groups, and had a 4
fold increased risk of AMR (Table 3 and Fig. 1, p = 0.004) with a median time to
AMR of 2 months.

106
Table 2. Patient demographics, HLA antibody, rejection and outcomes by transfusion
status.
Table 3. Univariate and multivariate adjusted Cox Proportional Hazards models for
the effect of Delayed Graft Function (DGF), entry HLA antibody, Antibody and Non-
Antibody Mediated Rejection (AMR and Non-AMR) and Transfusion status on death
censored (n=27) and combined patient and graft loss (n=51).

107
Figure 1. Kaplan–Meier plot of time to AMR by transfusion status in all patients.
Patients with Pre + Post-RBCT had HR 4.1 (95%CI 1.6–10.8 p = 0.004) for AMR
compared with No-RBCT. Note Y-axis is truncated.
Given the association of Pre + Post RBCT with AMR we next examined the
importance of pre-transplant DSA, a known risk for AMR, in the various transfusion
groups. When stratified by the presence of DSA there was no difference in the risk
of AMR between those with or without DSA in either of the No-RBCT, Pre-RBCT or
Post-RBCT groups individually (data not shown) or when these 3 groups were
combined (Fig. 2a). In the Pre + Post RBCT group the risk of AMR was 13.9 times
greater in those patients with DSA than in patients with Non-DSA or No-Antibody
(Fig. 2b p = 0.001). Indeed all 13 episodes of AMR in the DSA group occurred
exclusively in patients who had received Pre + Post-RBCT. On the other hand, 0/6
patients with Non-DSA and 2/37 in the No- antibody group who had received Pre +
Post-RBCT developed AMR. The median time between post-operative transfusion
and AMR in the DSA patients was 25 days (IQR 5–761 days).

108
Figure 2a. Time to antibody mediated rejection (AMR) by antibody status at the
time of transplant in the combined 195 patients receiving No-RBCT, Pre-RBCT and
Post-RBCT (p = 0.56)
Figure 2b. Time to antibody mediated rejection (AMR) by antibody status at the
time of transplant in the 63 patients with Pre + Post-RBCT (p = 0.001, HR 13.9 DSA
vs No-antibody) Note different Y axis origin.

109
Univariate predictors of AMR were pre-transplant DSA (HR 6.6 95%CI 2.9–
14.7, p < 0.001), DGF (HR 2.6. 1.1–6.1, p = 0.039), re-transplant (HR 3.3 1.3–8.3 p =
0.024) and Pre + Post-RBCT (HR 4.1, 1.6–10.8 p = 0.005) but not females (HR 0.9
0.38–2.1). There was a significant interaction between Pre-RBCT and Post-RBCT
(HR 4.4 2.0–9.8 p = 0.001) and between DSA and Post-RBCT (HR 10.6 4.7–23.8 p <
0.0001) on the risk of AMR. In a multivariate Cox model incorporating the above
univariate factors and adding interaction terms, only the interaction between DSA
and Post-RBCT (HR 7.2, 2.9–18.0, p = 0.001) remained a significant predictor of
AMR.
Death-censored graft loss (Fig. 3 and Table 3) and combined patient and graft loss
(Table 3) was significantly increased in the Pre + Post-RBCT group (HR 7.1 p <
0.001) compared with all other transfusion groups. This difference persisted even
after exclusion of the 37 patients with preformed DSA (HR 4.9 95% CI 1.5–15.8 p =
0.007 and 3.9 1.7–7.8 p = 0.001 respectively). Neither gender nor retransplant
were associated with graft or patient loss. We used significant univariate
predictors of graft loss including DGF, HLA antibody (DSA and Non-DSA), AMR and
Non-AMR rejection and transfusion history in a multivariate Cox Proportional
Hazards model (Table 3). AMR, Non-AMR rejection and Pre + Post RBCT were
independently associated with death censored and all cause graft loss. However
DGF and DSA were no longer predictive by multivariate analysis.

110
Figure 3. Time to death censored graft loss by transfusion status HR 7.1 (2.4–21.3) p
< 0.001 for Pre + Post-RBCT compared with No-RBCT.
4. Discussion
We show that the risk of AMR associated with the presence of DSA at the time of
transplant is modulated by exposure to RBCT. In our cohort, AMR was predominantly
observed only in sensitised patients with DSA all of whom had received RBCT prior to
transplant and were then transfused within the first 30 days (usually 48 h). Pre-
transplant DSA and Pre + Post-RBCT were each independent predictors of AMR.
However, there was a strong interaction between pre-transplant DSA and Post-RBCT,
which eliminated all other predictors (DGF, re-transplant, gender), and conferred a 7.2
fold increase in the risk of AMR. In contrast, patients with DSA who received only Pre-
RBCT or Post-RBCT, or who received no transfusion did not experience AMR.
Overall, patients with DSA had the highest rate of post-operative transfusion. In our
centres, the decision to give peri-operative transfusion was solely determined by clinical
need, authorised by different clinical teams and, in all cases, made without knowledge
of the patient's anti-HLA antibody status. Our reported post-operative transfusion rate
of 43% is very similar to those reported elsewhere [28,29]. The reason for the higher
rate of peri-operative transfusion in patients with DSA compared with Non-DSA is
therefore uncertain. It may be due to the greater medical and surgical complexities of

111
this patient group and their greater waiting time on dialysis for example. However, it is
notable that there was no difference in gender, re-transplantation, deceased donors or
Pre-RBCT between the DSA and Non-DSA groups at time of surgery, or between the
haemoglobin at surgery or at 1 month post- surgery. Although residual confounding by
indication remains possible, it is not possible to either entirely adjust or explain and
this difference requires further testing.
The immunological interaction of blood transfusion and transplantation is complex. Pre-
RBCT is associated with better graft outcomes and less acute rejection, and this is
suggested to be due to immunomodulation with down-regulation of an immune response
and the induction of regulatory T-cells [11,30]. Indeed our study confirms the continued
benefit of Pre-RBCT alone with this group having the lowest rate of Non-AMR. We also
confirm that Pre-RBCT is still associated with an increased risk of HLA-antibody
sensitisation. Several recent reports [28,29] raise some concern that post-operative
transfusion is associated with poor graft outcome. However these studies did not consider
sensitisation or prior transfusion as potential modifiers and these factors may account for
their conflicting conclusions. Here we report that peri-operative blood transfusion is
associated with an increased risk of AMR, but only in recipients with pre-transplant DSA
detected using solid phase assays, all of whom had been previously exposed to RBCT and
other sensitising events. This effect of peri-operative transfusion was not found in
recipients without DSA, suggesting that the combination of DSA and peri-operative blood
transfusion may be particularly detrimental to the transplanted graft. Importantly, adverse
events after peri-operative blood transfusion included not only antibody mediated
rejection, but also poorer long term graft outcome and recipient death, independent of
the risk of AMR and Non-AMR, consistent with the findings of O'Brien et al. [28].
In light of our findings it is worth considering the immunological mechanisms whereby
blood transfusion could increase the pathogenicity of pre-existing DSA. This might be
through direct quantitative or qualitative alterations in antibody or indirectly via specific
transfusion factors. Scornik et al. [16] have previously identified that re-exposure to
blood in those with prior sensitising events such as transplant or pregnancy elicits a
broad antibody response; findings that are consistent with our study. Interestingly,
broad recall of an antibody response to previously exposed transplant antigens, rather
than to the transfusion antigens, was induced by third party transfusions. [31] Qian et al.

112
[32] have shown in a cardiac rodent model that pre-sensitisation with allogeneic RBCT
causes accelerated graft rejection in the presence of complement and antibody binding
to graft endothelium. Complement activation products and quantitative changes in
cytokines may be present within stored blood products [33,34]. Norda and colleagues
found that stored plasma components may differ significantly in the amount and
timing of complement activation products, particularly C3a, which could specifically
trigger pathological changes if pre-existing effector DSA is present. Theoretically
cytokines and other factors present in blood products could also induce non-
complement activating DSA to class switch to IgG1 and/or IgG3 complement activating
antibodies. Mice models of transfusion related acute lung injury suggest that MHC
class I specific antibody binding to nonhematopoietic cells drives complement activation
and production of reactive oxygen species [35]. T cell allorecognition of allogeneic HLA
molecules, present even in leucodepleted blood products, may be associated with
specific and non-specific immune activation including increased cytokine production and
cytotoxicity function. Whether exposure to RBCT in sensitised patients stimulates an
increase in the absolute amount or breadth of DSA and/or class switching and
complement binding was beyond the scope of this study. Serially monitoring these
changes would be informative however the frequency of sampling and interventions for
management of rejection which alter antibody measurement confound interpretation.
These putative adverse effects of peri-operative blood transfusion could be investigated
further using in-vivo animal models.
This data suggests that avoidance of peri-operative blood transfusion or, given the
impossibility of eliminating all transfusion risk, establishing a new paradigm for RBCT in
sensitised transplant recipients should be considered. It is established that
leucodepleted unmatched RBCT does not reduce sensitisation [23] and therefore
selecting HLA matched blood with its significantly reduced risk of HLA specific antibody
production may be particularly suited to patients with DSA [36]. The use of HLA
matched blood transfusion products for renal transplantation patients is feasible and
may be effective within a clinical setting [36,37]. Furthermore recipients with high levels
of sensitization may even benefit from pre-operative storage of autologous blood
products for use in the event of requiring a peri-operative blood transfusion [38]. The
beneficial effects of blood transfusion on graft survival have been reported to be
associated with HLA-DR matching, and while HLA typing of the blood donors was not

113
available for this study it is highly likely that the observed adverse effect is associated
with specific HLA mismatches between the blood donor and organ recipient [36].
In conclusion, we have shown that Pre-RBCT alone is still associated with a lower rate of
Non-AMR rejection and an increased risk of HLA antibody. However, peri-operative blood
transfusion in sensitised renal recipients with DSA and prior transfusion is associated
with AMR. Post- RBCT may therefore be an additional factor modifying the risk of AMR
in patients with HLA-antibody. We also confirm and expand upon the previous findings
that perioperative blood transfusion is associated with poorer graft and patient
survival, and show that this is most evident in those with previous exposure to RBCT,
independent of acute rejection episodes. These findings suggest that RBCT remains a
potent and complex modifiable immunomodulator of renal transplant outcomes and
additional studies to further define mechanisms for these effects are warranted.
Disclosure
This is an original work and the manuscript or parts of it have not been submitted
elsewhere for publication. All authors have read and approved submission of the
manuscript, and that material in the manuscript has not been published and is not
being considered for publication elsewhere in whole or part in any language except as
an abstract.
Acknowledgements
The authors wish to acknowledge the clinicians and transplant nurses at Royal Perth
Hospital, Sir Charles Gairdner Hospital and Fremantle Hospital in Western Australia
involved in the collection of this data. We wish to thank the Department of Clinical
Immunology, Royal Perth Hospital for compatibility testing of the patients in this
study.

114
References
[1] Lefaucheur C, Loupy A, Hill GS, Andrade J, Nochy D, Antoine C, et al. Preexisting
donor-specific HLA antibodies predict outcome in kidney transplantation. J Am Soc
Nephrol 2010; 21: 1398–406.
[2] Otten HG, Verhaar MC, Borst HP, Hene RJ, van Zuilen AD. Pretransplant donor-
specific HLA class-I and -II antibodies are associated with an increased risk for kidney
graft failure. Am J Transplant 2012; 12: 1618–23.
[3] Song EY, Lee YJ, Hyun J, Kim YS, Ahn C, Ha J, et al. Clinical relevance of pretransplant
HLA class II donor-specific antibodies in renal transplantation patients with negative T-cell
cytotoxicity crossmatches. Ann Lab Med 2012; 32: 139–44.
[4] Opelz G, Graver B, Mickey MR, Terasaki PI. Lymphocytotoxic antibody responses to
transfusions in potential kidney transplant recipients. Transplantation 1981; 32: 177–83.
[5] Sanfilippo F, Vaughn WK, Bollinger RR, Spees EK. The influence of pretransplant
transfusions, using different blood products, on patient sensitization and renal allograft
survival. Transplantation 1984; 37: 350–6.
[6] Scornik JC, Ireland JE, Howard RJ, Fennell III RS, Pfaff WW. Role of regular and
leukocyte-free blood transfusions in the generation of broad sensitization.
Transplantation 1984; 38: 594–8.
[7] Pfaff WW, Howard RJ, Scornik JC, Day C, Renderer J, Scott J, et al. Incidental and
purposeful random donor blood transfusion. Sensitization and transplantation.
Transplantation 1989; 47: 130–3.
[8] Chow MP, Hu HY, Lyou JY, Lin JS, Yung CH, Lee A, et al. Red cells, HLA and platelet
antibody formation in patients with multiple transfusions. Acta Haematol 1994; 92:
57–60.
[9] Novotny VM, van Doorn R, Witvliet MD, Claas FH, Brand A. Occurrence of allogeneic
HLA and non-HLA antibodies after transfusion of prestorage filtered platelets and red
blood cells: a prospective study. Blood 1995; 85: 1736–41.
[10] Blajchman MA. Immunomodulatory effects of allogeneic blood transfusions: clinical
manifestations and mechanisms. Vox Sang 1998; 74(Suppl. 2): 315–9.

115
[11] Claas FH, Roelen DL, van Rood JJ, Brand A. Modulation of the alloimmune response by
blood transfusions. Transfus Clin Biol 2001; 8: 315–7.
[12] Opelz G, Graver B, Terasaki PI. Induction of high kidney graft survival rate by multiple
transfusion. Lancet 1981; 1: 1223–5.
[13] Scornik JC, Meier-Kriesche HU. Blood transfusions in organ transplant patients:
mechanisms of sensitization and implications for prevention. Am J Transplant 2011;
11: 1785–91.
[14] Karpinski M, Pochinco D, Dembinski I, Laidlaw W, Zacharias J, Nickerson P. Leuko-cyte
reduction of red blood cell transfusions does not decrease allosensitization rates in
potential kidney transplant candidates. J Am Soc Nephrol 2004; 15: 818–24.
[15] Scornik JC, Pfaff WW, Howard RJ, Fennell III RS, Ramos E, Peterson JC, et al. Increased
antibody responsiveness to blood transfusions in pediatric patients. Transplantation 1994;
58: 1361–5.
[16] Scornik JC, Ireland JE, Howard RJ, Pfaff WW. Assessment of the risk for broad
sensitization by blood transfusions. Transplantation 1984; 37: 249–53.
[17] Sanfilippo F, Vaughn WK, Bollinger RR, Spees EK. Comparative effects of pregnancy,
transfusion, and prior graft rejection on sensitization and renal transplant results.
Transplantation 1982; 34: 360–6.
[18] Fox KM, Yee J, Cong Z, Brooks JM, Petersen J, Lamerato L, et al. Transfusion burden in
non-dialysis chronic kidney disease patients with persistent anemia treated in routine
clinical practice: a retrospective observational study. BMC Nephrol 2012; 13: 5.
[19] Ibrahim HN, Skeans MA, Li Q, Ishani A, Snyder JJ. Blood transfusions in kidney
transplant candidates are common and associated with adverse outcomes. Clin Transpl
2011; 25: 653–9.
[20] Aalten J, Bemelman FJ, van den Berg-Loonen EM, Claas FH, Christiaans MH, de Fijter
JW, et al. Pre-kidney-transplant blood transfusions do not improve transplantation
outcome: a Dutch national study. Nephrology, dialysis, transplantation. Off Publ Eur
Dial Transplant Assoc Eur Ren Assoc 2009; 24: 2559–66.

116
[21] Balasubramaniam GS, Morris M, Gupta A, Mesa IR, Thuraisingham R, Ashman N.
Allosensitization rate of male patients awaiting first kidney grafts after leukodepleted
blood transfusion. Transplantation 2012; 93: 418–22.
[22] Scornik JC. Leukoreduced blood and sensitization of organ transplant candidates.
Transfusion 2012; 52: 1838–9 [author reply 9].
[23] van de Watering L, Hermans J, Witvliet M, Versteegh M, Brand A. HLA and RBC
immunization after filtered and buffy coat-depleted blood transfusion in cardiac
surgery: a randomized controlled trial. Transfusion 2003; 43: 765–71.
[24] AlMahri A, Holgersson J, Alheim M. Detection of complement-fixing and non-fixing
antibodies specific for endothelial precursor cells and lymphocytes using flow
cytometry. Tissue Antigens 2012; 80: 404–15.
[25] Chen G, Sequeira F, Tyan DB. Novel C1q assay reveals a clinically relevant subset of
human
Leukocyte antigen antibodies independent of immunoglobulin G strength on single
antigen beads. Hum Immunol 2011; 72: 849–58.
[26] Mujtaba MA, Goggins W, Lobashevsky A, Sharfuddin AA, Yaqub MS, Mishler DP, et al.
The strength of donor-specific antibody is a more reliable predictor of antibody-
mediated rejection than flow cytometry crossmatch analysis in desensitized kidney
recipients. Clin Transplant 2011; 25: E96-102.
[27] Fidler SJ, Irish AB, Lim W, Ferrari P, Witt CS, Christiansen FT. Pre-transplant donor
specific anti-HLA antibody is associated with antibody-mediated rejection, progressive
graft dysfunction and patient death. Transpl Immunol Jun. 2013; 28(4): 148–53.
[28] O'Brien FJ, Lineen J, Kennedy CM, Phelan PJ, Kelly PO, Denton MD, et al. Effect of
perioperative blood transfusions on long term graft outcomes in renal transplant
patients. Clin Nephrol 2012; 77: 432–7.
[29] Scornik JC, Schold JD, Bucci M, Meier-Kriesche HU. Effects of blood transfusions
given after renal transplantation. Transplantation 2009; 87: 1381–6.
[30] Bushell A, Karim M, Kingsley CI, Wood KJ. Pretransplant blood transfusion without
additional immunotherapy generates CD25 + CD4+ regulatory T cells: a potential
explanation for the blood-transfusion effect. Transplantation 2003; 76: 449–55.
[31] Scornik JC, Ireland JE, Howard RJ, Pfaff WW, Fennell III RS. Sensitization by blood
transfusions in previously transplanted patients. Transplantation 1983; 35: 505–6.

117
[32] Qian Z, Lee CY, Murata K, Liu J, Fox-Talbot K, Wasowska BA, et al. Antibody and
complement mediated injury in transplants following sensitization by allogeneic blood
transfusion. Transplantation 2006; 82: 857–64.
[33] Norda R, Schott U, Berseus O, Akerblom O, Nilsson B, Ekdahl KN, et al. Complement
activation products in liquid stored plasma and C3a kinetics after transfusion of
autologous plasma. Vox Sang 2012; 102: 125–33.
[34] Pandey P, Chaudhary R, Aggarwal A, Kumar R, Khetan D, Verma A. Transfusion-
associated immunomodulation: quantitative changes in cytokines as a measure of
immune responsiveness after one time blood transfusion in neurosurgery patients.
Asian J Transf Sci 2010; 4: 78–85.
[35] Strait RT, Hicks W, Barasa N, Mahler A, Khodoun M, Kohl J, et al. MHC class I-specific
antibody binding to nonhematopoietic cells drives complement activation to induce
transfusion-related acute lung injury in mice. J Exp Med 2011; 208: 2525–44.
[36] Magee BA, Martin J, Cole MP, Morris KG, Courtney AE. Effects of HLA-matched blood
transfusion for patients awaiting renal transplantation. Transplantation 2012; 94: 1111–6.
[37] Scornik JC. HLA-matched blood transfusions? Transplantation 2012; 94: 1085.
[38] Sasaki H, Chikaraishi T, Furuhata S, Tsutsumi H, Miyano S, Nakazawa R, et al. Autologous
blood transfusion for kidney transplant recipients. Transplant Proc 2008; 40: 1371–2.

118
Chapter 5
Virtual crossmatch approach to
maximise matching in paired kidney
donation

119
Virtual crossmatch approach to maximise matching in paired kidney donation
Paolo Ferrari, Samantha Fidler, Jenni Wright, Claudia Woodroffe, Paul Slater, Aaron Van
Althuis-Jones, Rhonda Holdsworth, Frank T Christiansen
Paired kidney exchange may be an option where an individual awaiting kidney transplant
has a living donor who is medically suitable, but cannot donate due to blood group
incompatibility or the presence of donor specific HLA antibodies. Exchanges can be very
simple between two pairs, or more complex involving three or more pairs. Identification
of compatible pairs relies on the exclusion of incompatible pairs rather than HLA
matching. Sophisticated computer software was created for the Australian kidney
exchange (AKX) program utilising exclusion of clinically relevant HLA antibodies based on
our previous studies, with high resolution donor typing. The design and validation of this
computer algorithm is discussed in this chapter.
These findings were published in:
American Journal of Transplantation 2011: 11; 272-278
Contributions:
PF Prepared the manuscript, participated in study design, participated in
data analysis
SJF Performed all computer matching, participated in study design,
participated in data collection, participated in data analysis,
participated in writing the manuscript
JW, PS, AAA-J Programmed the computer module, participated in study design
CW Participated in data collection
RH, FTC Participated in study design, participated in writing of the
manuscript

120
Virtual Crossmatch Approach to Maximize Matching
in Paired Kidney Donation
P. Ferraria,b,c,∗, S. Fidlerc,d,e, J. Wrightf, C. Woodroffea,c, P. Slaterf, A. Van Althuis-
Jonesf, R. Holdsworthg and F. T. Christiansend,e
a Department of Nephrology, Fremantle Hospital, Perth, Western Australia
bSchool of Medicine and Pharmacology, University of Western Australia cAustralian Paired Kidney Exchange Program, Perth, Western Australia dDepartment of Immunology, PathWest, Royal Perth Hospital, Perth, Western Australia eSchool of Pathology and Laboratory Medicine, University of Western Australia, Perth, Western Australia fNational Organ Matching Service, Australian Red Cross Blood Service, Sydney, New South Wales gMedical, Transplantation and Quality Services Division, Australian Red Cross Blood Service, Melbourne, Victoria, Australia *Corresponding author: Paolo Ferrari, [email protected]
We developed and tested a new computer program to match maximal sets of
incompatible live donor/recipient pairs from a national paired kidney donation
(PKD) registry. Data of 32 incompatible pairs included ABO and 4 digit-high-
resolution donor and recipient HLA antigens and recipient’s HLA antibodies.
Three test runs were compared, in which donors were excluded from matching to
recipients with either donor-specific antibodies (DSA) >8000MFI (mean
fluorescent intensity) at low-resolution (Run 1) or >8000MFI at high-resolution
(Run 2) or >2000MFI and high-resolution (Run 3). Run 1 identified 22 703 possible
combinations, with 20 pairs in the top ranked, Run 2 identified 24 113
combinations, with 19 pairs in the top ranked and Run 3 identified 8843
combinations, with 17 pairs in the top ranked. Review of DSA in Run 1 revealed
that six recipients had DSA 2000–8000MFI causing a possible positive crossmatch
resulting in breakdown of two 3-way and three 2-way chains. In Run 2, four
recipients had DSA 2000–8000MFI, also potentially causing breakdown of three
2-way chains. The more prudent approach of excluding from matching recipients
with DSA with >2000MFI reduces the probability of matched pairs having a
positive crossmatch without significantly decreasing the number of possible
transplants.
Key words: ABO, computerization, HLA, incompatibility, kidney transplantation,
matching, paired kidney donation

121
Abbreviations: CDC, complement-dependent cytotoxicity; IPMM, ignoring
previous mismatched antigens; MP, match probability; NOMS, National Organ
Matching System; PKD, paired kidney donation; SAB, single antigen bead;
WAPKD, Western Australian PKD.
Received 20 July 2010, revised 22 August 2010 and accepted for publication 08 September 2010
Introduction
The shortage of kidneys from deceased organ donors and longer kidney transplant waiting
lists in many countries (1,2) have placed greater emphasis on living kidney donation to
meet the increasing demand for transplantation in patients with renal failure. Results of
living donor kidney transplantation, irrespective of tissue typing matches, are superior to
those achieved with deceased donor kidneys (3). Based on the prevalence of ABO blood
groups and recipients’ HLA sensitization it is estimated that approximately 30% of
recipients are biologically incompatible with their intended donor and do not proceed to
live donor kidney transplantation. Traditionally, these recipients are left to wait for a
deceased donor kidney for a variably long period of time. There is ample evidence that
waiting time on dialysis is the strongest modifiable risk factor for renal transplant
outcomes (4). To overcome immunological barriers of blood group or HLA sensitization,
new strategies to expand living kidney donations have been introduced, including paired
kidney donation (PKD) and altruistic donation, or HLA-desensitization and transplantation
across the blood type barrier. PKD is a strategy that helps patients finding a suitable donor
when their intended living donors are blood group or HLA incompatible (5). In a simple PKD,
two donor/recipient pairs surmount each other’s incompatibility problem by simply
exchanging donors (6,7). PKD can be arranged involving three or more pairs, which can be
matched optimally in large numbers only using sophisticated matching software.
The experience of the Western Australian PKD (WAPKD) program (8,9), has been used to
establish a national PKD program and to develop a matching protocol for PKD pairs in
Australia. There are 14 Australian transplantation centers with a living donation program,
but only 4 performing over 25 live donations yearly. The effectiveness of a PKD program
depends largely on the size of the donor/recipient pool and this has led to the development
of a national PKD program in which all Australian kidney transplantation centers
participate. To ensure an equitable and objective matching of participating pairs, matching

122
is performed by the National Organ Matching System (NOMS) using a newly developed
computer program. The software was based on the principles guiding the Dutch algorithm
(10), but taking advantage of advances in HLA technology to enable virtual crossmatching.
In this study, the allocation criteria are described and the outcomes of test runs obtained
with the NOMS matching software using pairs enrolled in the WAPKD program are
presented.
Materials and Methods
The WAPKD program was established in October 2007 as a new initiative of a single
transplantation service performing annually approximately 80 live and deceased donor
kidney transplants. As of December 2009, 32 incompatible donor/recipient pairs were
enrolled in the program. Before development of the NOMS PKD program, the software
used for matching was rudimentary, searching for recipients who were ABO compatible
with each of the registered donors and eliminating those recipients who had HLA
antibodies to an HLA antigen present in the donor. Loops of reciprocal compatible
donor/recipient pairs and combinations of those pairs had to be selected manually, a task
only achievable using 2-way chains with a low degree of complexity in a small pool of PKD
pairs.
HLA typing
Donor HLA-typing for the loci-A, -B, -Cw, -DRB1, -DPB1 and -DQB1 was performed by the
PathWest Department of Clinical Immunology, Royal Perth Hospital using direct DNA
sequencing according to published methods (11). HLA-alleles of each locus were entered in
the computer program at the 4- digit level.
Detection of anti-HLA antibodies
Recipients were tested for HLA class I and class II directed IgG antibody against HLA-A, -B, -
Cw, -DRB1, -DQB1 and -DPB1 in their sera, using single antigen bead (SAB) Luminex
technology (Lab Screen Single Antigen® , One Lambda, Inc., Canoga Park, CA, USA). Using the
vendor’s HLA-Fusion software, the mean fluorescence intensity (MFI) signal for each SAB
was normalized against the negative control to correct for nonspecific binding. Beads with

123
normalized MFIs of <500 were considered negative. HLA antibody specificities were
reported at the 4-digit level. According to the MFI of each SAB the strength of each
antibody was classified as strong (>8000), moderate (2000–8000) or weak (500–2000). HLA
antibody testing was per- formed every 2 months from the time of listing. Except for
individuals whose antibody strength declined over time, there was very little variation in
the range and strength of the HLA antibodies detected. For matching purposes, the highest
MFI for each HLA antibody was used.
Computer program matching rules and ranking
The NOMS developed a computer program to match participating pairs based on the
Dutch experience (7,10,12). The basic principle of the match algorithm is to ensure that
sensitized recipients with alloantibodies against HLA antigens in the donor pool have the
best chance to receive a kidney, ignoring any rules on mismatches between donor and
recipient HLA. Donors must have a recorded HLA typing at the 4-digit level for the loci HLA-
A, -B, -Cw, -DRB1, -DPB1 and -DQB1. Typing for loci HLA-DQA1, -DRB3, -DRB4 and -DRB5
may also be included. Recipients must be tested for both Class I and Class II HLA antibodies
by Luminex SAB assay and all antibodies with >500MFI are considered positive and entered
into the module.
The NOMS computer program matches each recipient’s HLA antibody against each of the
donor’s HLA antigens using a 3 steps process. First, matched pairs are found by comparing
the AB0 blood groups of each donor and each recipient, then by checking the donor
specific antibodies (DSAs) of recipients and comparing these in turn with the HLA-typing of
each ABO compatible donor. This is done for all potential recipients against all potential
donors. To maximize the number of O recipients being matched to an O donor, allocation
occurs first amongst ABO blood group identical pairs. When all possible ABO identical
matches are identified, the remaining recipients are matched against AB0-compatible
donors.
Second, the program looks for 2-way or 3-way chains of donor recipient pairs, if for
recipient X a match is possible with donor Y, the computer determines whether donor X is a

124
blood group compatible and HLA-acceptable donor for recipient Y. If recipient Y is indeed a
match to donor X, a new chain is formed.
Third, the program creates possible combinations using the following six ranking rules: (1)
prioritize combinations which maximize the number of potential transplants (i.e. favour
combinations allowing 10 possible transplants over combinations resulting only in 8
possible transplants), (2) maximize the number of ABO identical pairs (i.e. favour those
combinations with more O-to-O pairs over O-to-A or B or AB pairs), (3) minimize the
number of simultaneous transplants in a single center (i.e. favour combinations with an
even spread across centers for logistic reasons), 4) maximize the number of shortest chains
(i.e. favour combinations with shorter chains to minimize problems if a donor or recipient
drops out), (5) match probability (MP) of the recipients in the combination (i.e. favour
combinations with more patients with lower match probabilities) and (6) waiting time (i.e.
favour combinations with longer waiting patients). The MP is calculated as MP = (a/b),
where a = number of acceptable donors in the run (i.e. ABO compatible donors having no
unacceptable HLA antigens) and b = total number of ABO compatible donors in the run. The
MP range is 0 to 1, 0 indicating no compatible donors and 1 indicating all ABO compatible
donors are suitable match.
All mismatched HLA antigens from previous transplants are by default considered in the
allocation of deceased donor kidneys in Australia and result in exclusion of a potential
donor bearing any of the previous mismatched antigens. The NOMS PKD computer
program has an option that allows ignoring previous mismatched antigens (IPMM), in the
absence of specific DSAs in the recipient to the previous mismatch or because the
previously mismatched antigen may be considered an acceptable mismatch based on the
epitopes present (13). This results in a patient not being excluded for a donor bearing the
ignored previous mismatched HLA antigen allele. Where previous peak sera are no longer
available for SAB testing to demonstrate absence of the DSAs to mismatched antigens the
decision to assign IPMM antigens is made by the recipient’s transplant team.

125
Testing and validation of the new computer program
Three test runs were undertaken using the data from the 32 pairs identified in the WAPKD
program. Data included blood groups and high-resolution HLA antigens of donors and
recipients and recipients’ HLA antibody specificities (by One Lambda SAB assay). Donors
were excluded from matching to recipients with (a) strong (>8000MFI) DSA defined at the
2-digit level (Run 1), (b) strong (>8000MFI) DSA defined at the 4-digit level (Run 2) or (c)
moderate and strong (>2000MFI) DSA defined at the 4-digit level (Run 3), respectively.
Run 1 with low resolution and a cut-off of >8000MFI was chosen because it was considered
to best simulate the Dutch program. In the Netherlands antibodies are defined at 2-digit
level and are based on complement- dependent cytotoxicity (CDC) reactivity. The antibody
specificity and threshold for Run 2 was chosen because the higher specificity of 4-digit
typing is likely to result in a lower number of potential donors being excluded from
matching to sensitized recipients with multiple antibodies. The presence of DSA 2000–
8000MFI still has the potential of positive CDC or flow cross- match (14). Run 3 was chosen
because DSA with values of <2000MFI are unlikely to have a positive CDC or flow
crossmatch (14), thus enabling a virtual crossmatch.
Table 1: ABO blood group of donors and recipients in the Western Australian paired
kidney donation program
Donor
A
Donor
AB
Donor
B
Donor
O
Total
Recipient A 3 – – 7 10
Recipient AB – – 1 – 1
Recipient B 2 – – – 2
Recipient O 11 1 2 5 19
Total 16 1 3 12 32
Results
Outcome of the WAPKD program
Between October 2007 and December 2009, 32 incompatible pairs and 2 altruistic donors
were entered into the WAPKD database. Of the 32 pairs, 50% participated because of ABO
incompatibility and 50% because of positive crossmatch, 59% recipients and 38% donors

126
were blood group O (Table 1). In sensitized recipients, HLA antibody distribution was 78%
anti-HLA-A, -B and -DRB1, 16% anti- HLA-Cw, -DPB1, -DQA1 and 6% anti-HLA-DQB1, -DRB3 or
-DRB5. Two patients were highly sensitized with a calculated PRA >85%. During the 2-year
period of the WAPKD program the maximum number of pairs per run was 14 and up to 135
possible matches were identified. The majority of these matches involved the same pairs
being present in multiple exchanges. After limiting possible exchanges to 2-way chains and
eliminating multiple matches, 11 PKD and 2 deceased donor list recipients (4×2-way +
1xaltruistic donor 3-way + 1x altruistic donor 2-way) were matched and transplanted
through the WAPKD program. All had a negative CDC T- and B-cell crossmatch. Of the 11
PKD recipients transplanted in the WAPKD program, 7 had anti- HLA antibodies and 4 were
ABO incompatible with their intended donors. Eight subjects were transplanted in the
presence of multiple ‘weak’ (500–2000MFI) DSAs. No flow crossmatch was performed for
these patients, but none had acute humoral rejection. Of the remaining PKD recipients, six
received a deceased donor kidney transplant, four were transplanted using an ABO
incompatible program, three left the transplant program and eight recipients remain on
the transplant waiting list.
Validation of the new computer software
In the first step, the NOMS computer program compares each donor in turn against all
recipients and determines whether they are a match. Only a few seconds processing time
are necessary to find matching pairs. For the 32 recipients, although 992 (= (N-1) x N)
combinations are possible, depending on the antibody resolution and HLA antigen
specificity, only 355 (Run 3) to 445 (Run 2) combinations were found. In the second step,
these separate matched pairs (donor with new recipients) are used to identify all possible 2-
way or 3-way chains. This process takes a few minutes and results in between 191 to 316
chains with a maximum chain size of 3 (Table 2). In the third step, the computer program
selects all possible combinations of chains in which each matched pair appears only once
in a combination and ranks all possible combinations according to the preset conditions. As
the program finds all possible combinations of chains, the number of results increases
exponentially leading to 8000–25 000 possibilities when 32 pairs are enrolled and takes up
to several hours computing time (Table 2).

127
Table 2: Comparison of 3 test runs using different antibody resolution and strength to
exclude recipients with antibodies from matching to donors in a pool of 32 incompatible
donor - recipient pairs.
Run 1 used 2-digit HLA typing, with antibodies for exclusion >8000 MFI; run 2 used 4-digit HLA typing with
antibodies for exclusion >8000 MFI; and run 3 used 4-digit HLA typing with antibodies for exclusion >2000
MFI.
Run 1 Run 2 Run 3
Low
Resolution
High
Resolution
High
Resolution MFI > 8000 MFI > 8000 MFI > 2000
Time to match 3h 45 min 3h 58 min 0h 50 min
No. of matched pairs 439 445 355 No. of chains 308 316 191 No. of combinations 22 703 24 113 8843 No. of patients in 1st combination 20 19 17 3-way chains in 1st combination 4 5 5 2-way chains in 1st combination 4 2 1 Recipients with DSA 2000–8000MFI 6 4 0 No. of patients in chains with predicted negative
crossmatch
8 10 17 Donor/Recipient age difference (years) 0.9 ± 14.2 1.2 ± 13.6 4.0 ± 14.7
(–24 to 24) (–25 to 29) (–24 to 29)
Run 1 was completed in 3h 45min and identified 22703 possible combinations, with the
highest ranking comprising 20 pairs in 4 × 3-way and 4 × 2-way exchanges, of whom 10
(50%) were O recipients (Table 2). Run 2 was completed in 3h 58min and identified 24113
combinations, with the highest ranking comprising 19 pairs in 5 × 3- way and 2 × 2-way
exchanges, of whom 9 (47%) were O recipients. Run 3 was completed in 50 min and
identified 8843 combinations, with the highest ranking comprising 17 pairs in 5 × 3-way and
1 × 2-way exchanges (Figure 1), of whom 6 (35%) were O recipients (Tables 2 and 3).
Comparison of donor and recipient HLA antigens at conventional HLA-A, -B and -DRB1 loci
for those pairs matched in test Run 3 revealed and average of 4.8 ± 1.2 mismatches (A-
/B- 3.2 ± 0.9, DRB1- 1.6 ± 0.5) between each matched donor and recipient. In test Run 1,
a review of each recipient’s DSA revealed that 6 recipients had DSA with MFI of between
2000 and 8000 and may have had a positive flow crossmatch, causing breakdown of chain
1 + 2 (3-way) and 3 + 4 + 6 (2-way) if a negative flow crossmatch is a prerequisite for
transplantation. This would have resulted in only eight PKD pairs with predicted negative
flow and CDC crossmatch. In test Run 2 DSA 2000–8000MFI were present in 4 recipients
resulting in only 10 pairs with predicted negative flow and CDC crossmatch suitable for
transplantation (Table 2).

128
Figure 1: Matching diagram of test run 3 using 32 pairs, where donors were
excluded from matching to recipients with moderate and strong (>2000MFI) donor-
specific antibodies defined at the 4-digit level.
Fine lines indicate all possible chains; bold lines with arrows indicate chains in the 1st
combination with the highest number of pairs matched at the lowest match probability with the
highest number of blood group identical matches.
Table 3: Match results by blood type excluding recipients with donor specific antibody at >2000 mean fluorescence intensity (OneLambda) and using high-resolution antibody definition

129
In the 16 patients enrolled because of positive crossmatch to their intended recipients,
median class I PRA was 36 (range 10–89) in the 11 matched recipients and 60 (range 20–
73) in the residual 5 unmatched recipients (p = 0.30 Mann-Whitney test). Median class II
PRA was 42 (range 10–99) in the 11 matched recipients and 23 (range 14–95) in the
residual 5 unmatched recipients (p = 0.76).
Discussion
Using the matching algorithm developed by the NOMS, simulations using different
definitions of antibody specificity and strength in sensitized recipients to match
donor/recipient pairs in a PKD pool showed that 53% of pairs could find a suitable match
with predicted negative virtual crossmatch even in a relatively small pool of 32
donor/recipient pairs. Outcomes of the WAPKD program used to provide testing data for
the NOMS computer program support the probability of a high success rate of matched
pairs progressing to actual kidney transplantation and support the view that the strategy
selected in Australia to achieve the maximum number of transplants with a given pool of
incompatible donors and recipients is highly effective. Algorithms used in other countries
select possible exchanges based on a points scoring system that includes the number of
HLA-mismatches, % PRA, distance between the exchange centers, donor age differences,
CMV status and other factors (15,16). These algorithms have some inherent disadvantages,
such as limiting the maximum number of potential matches, or a subsequent high rate of
positive CDC crossmatches after computer matching of pairs, with consequent breakdown
of chains. This has been demonstrated in a testing environment with the UK algorithm,
showing a simulated 25% match-rate with 30 pairs and 35–40% with 50 pairs (15) and one
of the US algorithms, showing 24% match-rate with 45 recipients (16). Johnson et al.
reported performing only 8 PKD transplants in the UK over a 16 months period despite
identification of 28 matches among 85 pairs (15).
A direct comparison of the performance of the NOMS and the Dutch programs was not
undertaken. However, a simulation was tested using a match run with low resolution HLA
antibody definition and a cut-off of >8000MFI, thereby only including strong antibodies likely

130
to have CDC reactivity. In the Dutch program antibody specificities are entered at low-
resolution and matching is based on antibodies defined by CDC reactivity, as those
antibodies are considered a contraindication for transplantation, whereas Luminex is
considered a risk factor, but not contraindication to transplantation. In test Run 1 although
20/32 (63%) of recipients had a matched donor, 6 (30%) of the patients matched by low
resolution and a cut-off of >8000MFI would have had a DSA with a 2000–8000MFI or
antibody against splits within the broad antigen specificity. These results are in keeping
with the reported incidence of 34% pairs having a positive crossmatch in the 183
computer-matched combinations from the Dutch experience (7). Although the attempt to
exclude all potentially incompatible pairs with high levels of DSA to replicate the Dutch
experience for purposes of comparison has the disadvantage that it may exclude
individuals without true DSA, our strategy indicates a prudent approach that minimizes the
risk of break- down of chains. It is worth noting that in the WAPKD cohort used to validate
the new software none of the identified matches had a positive CDC crossmatch prior to
transplantation.
In recent years, solid phase assays using beads coated with HLA antigens have become the
preferred method of detecting HLA antibodies in transplant candidates (17). These assays
can identify the precise HLA-specificities of antibodies and donor cells are not required. It is
still unclear what strength of Luminex detected antibodies is considered equivalent to CDC
reactivity. In our experience the presence of DSA >8000MFI will often result in a positive
CDC crossmatch, whereas HLA antibodies with a DSA 2000–8000MFI may result in a positive
flow crossmatch. Our approach, where we exclude any donor against whom a recipient has
a HLA antibody at a strength of >2000MFI in the PKD pool, may be considered excessively
prudent because it does not take into account the possibility of noncomplement fixing
IgG2 or IgG4 antibodies. Noncomplement fixing anti-HLA alloantibodies are responsible for
discrepant results observed between solid phase assays and negative CDC reactivity.
Conventional solid phase assays cannot distinguish between complement fixing and
noncomplement fixing antibodies, therefore possibly leading to an overestimation of
sensitized patients than with the CDC assay (18,19). This brings into question whether it is
safe to transplant patients who may be CDC negative, but positive solid phase DSAs.
Recent studies in kidney transplant recipients indicate that even with a negative CDC
crossmatch, the presence of DSA detected by flow cytometry (20) or Luminex (19,21,22) is

131
associated with higher rates of graft failure compared to antibody negative patients.
Recently, C4d-fixing capability of DSAs has been reported and was found to be a negative
predictor of graft survival in cardiac and kidney transplantation (23,24). However, C4d-fixing
DSAs have generally significantly higher MFI values than non-C4d-fixing DSA (>10000MFI
73% vs.18%; ) (25). Introducing the additional step of in vitro detection of C4d-fixing
alloantibodies would therefore probably not significantly increase the specificity of
antibody used for the exclusion of matches in our PKD program. Our conservative
approach would result in only 3 less matched pairs than using high titer, low definition
antibody to identify DSA. However, this virtual crossmatch approach is most likely to result
in a negative CDC crossmatch (14) allowing all matched pairs a better chance to proceed to
transplantation.
Because HLA typing of donors and the definition of unacceptable donor HLA antigens for
recipients are the basic parameters used in the NOMS matching algorithm, donor HLA
typing and recipient antibody profile are registered in more detail than that used for the
regular allocation of deceased donor kidneys. The advantage of listing antigens and
antibodies at 4-digit level is that in recipients with HLA antibodies it increases the specificity
and reduces the number of donors excluded from matching. For example, a recipient with
an HLA-B∗44 antibody will be excluded from matching with any donor with a B∗44
antigen. However, if the antibody specificity of the recipient is B∗44:02, donors with the
B∗44:02 antigen, but not B∗44:03 will be excluded from matching. This explains the higher
number of combinations identified in Run 2 using high-resolution matching compared to
the low-resolution matching results in Run 1.
The Australian PKD program limits the number of chains to 3-way exchanges because this
restriction does not significantly reduce the maximum number of possible matches (26),
but minimizes the complexity of logistics required to coordinate 4 or more simultaneous
donor surgeries. Although donor–donor or donor–recipient age differences are not used as a
scoring parameter in ranking match combinations, the NOMS program will not accept
exchanges with a donor-donor age difference of >30 years. In the 3 test runs the average
donor/recipient age difference of matched pairs was between 1 and 4 years depending on

132
the matching rules employed and no recipient was matched with a donor ≥30 years older
than the recipient’s age. This should ensure an excellent graft survival and function
unaffected by donor age (27).
A limitation of the current study is that we did not perform CDC or flow crossmatches on
patients with DSA 2000– 8000MFIs to substantiate the use of the more conservative
approach. Nevertheless, there are strong arguments to support such an approach. First,
our experience shows that using a cut off of 2000MFI, >95% of DSA negative recipients will
have a negative flow and CDC crossmatch, whereas approximately 50% of DSA positive
recipients will have a positive flow or CDC crossmatch. The finding of a 34% rate of positive
crossmatches in the Dutch study (25) provides additional support for this conclusion.
Second, a survey among transplant centers participating in the Australian PKD program has
indicated that clinicians are willing to perform transplants in the setting of DSA <2000MFI
with a negative CDC crossmatch, but, in the presence of DSAs with a strength of 2000–
8000MFI the majority would request a flow crossmatch and if positive, not proceed to
transplantation. This is likely to lead to delays in the exchanges and the breakdown of
matched donor/recipient chains. Third, even if such cases have negative crossmatches, there
is increasing evidence that transplantation in such circumstances is associated with higher
rates of acute rejection and poorer graft survival (19,21,22). It would seem prudent to avoid
such transplants and our approach allows this without compromising the viability of the
exchange program.
In conclusion, our data demonstrate that using a computer matching algorithm based on
the high definition of recipient HLA antibody and donor HLA antigens to match PKD pairs,
the number of possible matches with predicted negative virtual crossmatch can be
maximized. As with other PKD programs sensitized patient who are not matched tend to
be more highly sensitized. Although the sensitivity of non anti-human globulin enhanced
cytotoxic crossmatches is clearly lower than a virtual crossmatch based on DSA antibody
defined by SAB and which is likely to exclude matches with a negative cytotoxic
crossmatch, our data suggest that the more prudent approach of excluding from matching
recipients with antibody MFI-values >2000 does not result in a significantly lower number
of possible transplants compared to exclusion of recipients with antibody MFI-values

133
>8000 (χ 2 = 0.57), a threshold that may result in a higher number of matched pairs having
a positive crossmatch using standard or enhanced CDC or flow crossmatch techniques.
Acknowledgments
The authors wish to acknowledge the support of the Australian Organ and Tissue Donation
and Transplantation Authority for the establishment and funding of the Australian Paired
Kidney Donation program.
Disclosure
The authors of this manuscript have no conflicts of interest to disclose as described by
the American Journal of Transplantation.

134
References
1. Mathew T, Faull R, Snelling P. The shortage of kidneys for transplantation in Australia.
Med J Aust 2005; 182: 204–205.
2. Harter TD. Overcoming the organ shortage: Failing means and radical reform. HEC Forum
2008; 20: 155–182.
3. Cecka JM. Kidney transplantation in the United States. Clin Transpl 2008; 22: 1–18.
4. Meier-Kriesche HU, Kaplan B. Waiting time on dialysis as the strongest modifiable risk
factor for renal transplant outcomes: A paired donor kidney analysis. Transplantation
2002; 74: 1377– 1381.
5. Rapaport FT. The case for a living emotionally related international kidney donor exchange
registry. Transplant Proc 1986; 18(3 Suppl 2): 5–9.
6. Park K, Moon JI, Kim SI, Kim YS. Exchange-donor program in kidney transplantation.
Transplant Proc 1999; 31: 356–357.
7. de Klerk M, Witvliet MD, Haase-Kromwijk BJ, Claas FH, Weimar W. Hurdles, barriers, and
successes of a national living donor kidney exchange program. Transplantation 2008; 86:
1749–1753.
8. Ferrari P, Woodroffe C, Christiansen FT. Paired kidney donations to expand the living donor
pool: The Western Australian experience. Med J Aust 2009; 190: 700–703.
9. Ferrari P, De Klerk M. Paired kidney donations to expand the living donor pool. J Nephrol
2009; 22: 699–707.
10. Keizer KM, de Klerk M, Haase-Kromwijk BJ, Weimar W. The Dutch algorithm for allocation
in living donor kidney exchange. Transplant Proc 2005; 37: 589–591.
11. Sayer D, Whidborne R, Brestovac B, Trimboli F, Witt C, Christiansen F. HLA-DRB1 DNA
sequencing based typing: An approach suitable for high throughput typing including
unrelated bone marrow registry donors. Tissue Antigens 2001; 57: 46–54.
12. de Klerk M, Witvliet MD, Haase-Kromwijk BJ, Claas FH, Weimar W. A highly efficient living
donor kidney exchange program for both blood type and crossmatch incompatible donor-
recipient combinations. Transplantation 2006; 82: 1616–1620.
13. Duquesnoy RJ. A structurally based approach to determine HLA compatibility at the
humoral immune level. Hum Immunol 2006; 67: 847–862.
14. Morris GP, Phelan DL, Jendrisak MD, Mohanakumar T. Virtual crossmatch by identification
of donor-specific anti-human leukocyte antigen antibodies by solid-phase immunoassay: A

135
30-month analysis in living donor kidney transplantation. Hum Immunol 2010; 71: 268–273.
15. Johnson RJ, Allen JE, Fuggle SV, Bradley JA, Rudge C. Early experience of paired living kidney
donation in the United Kingdom. Transplantation 2008; 86: 1672–1677.
16. Saidman SL, Roth AE, Sonmez T, Unver MU, Delmonico FL. In- creasing the opportunity of
live kidney donation by matching for two- and three-way exchanges. Transplantation
2006; 81: 773– 782.
17. Tait BD. Solid phase assays for HLA antibody detection in clinical transplantation. Curr Opin
Immunol 2009; 21: 573–577.
18. Tambur AR, Bray RA, Takemoto SK, Mancini M, Costanzo MR, Kobashigawa JA et al. Flow
cytometric detection of HLA-specific antibodies as a predictor of heart allograft rejection.
Transplantation 2000; 70: 1055–1059.
19. Gibney EM, Cagle LR, Freed B, Warnell SE, Chan L, Wiseman AC. Detection of donor-
specific antibodies using HLA-coated microspheres: Another tool for kidney transplant risk
stratification. Nephrol Dial Transplant 2006; 21: 2625–2629.
20. Bielmann D, Honger G, Lutz D, Mihatsch MJ, Steiger J, Schaub S. Pretransplant risk
assessment in renal allograft recipients using virtual crossmatching. Am J Transplant 2007;
7: 626–632.
21. Amico P, Honger G, Mayr M, Steiger J, Hopfer H, Schaub S. Clinical relevance of
pretransplant donor-specific HLA antibodies detected by single-antigen flow-beads.
Transplantation 2009; 87: 1681–1688.
22. Lefaucheur C, Loupy A, Hill GS, Andrade J, Nochy D, Antoine C et al. Preexisting donor-
specific HLA antibodies predict outcome in kidney transplantation. J Am Soc Nephrol
2010; 21: 1398– 1406.
23. Wahrmann M, Exner M, Schillinger M, Haidbauer B, Regele H, Kormoczi GF et al. Pivotal
role of complement-fixing HLA alloantibodies in presensitized kidney allograft recipients.
Am J Transplant 2006; 6(5 Pt 1): 1033–1041.
24. Smith JD, Hamour IM, Banner NR, Rose ML. C4d fixing, luminex binding antibodies – a
new tool for prediction of graft failure after heart transplantation. Am J Transplant 2007;
7: 2809– 2815.
25. Honger G, Wahrmann M, Amico P, Hopfer H, Bohmig GA, Schaub
S. C4d-fixing capability of low-level donor-specific HLA antibodies is not predictive for
early antibody-mediated rejection. Transplantation 2010; 89: 1471–1475.

136
26. de Klerk M, Van Der Deijl WM, Witvliet MD, Haase-Kromwijk BJ, Claas FH, Weimar W. The
optimal chain length for kidney paired exchanges: An analysis of the Dutch program.
Transpl Int 2010; 23: 1120–1125.
27. Ferrari P, Lim W, Dent H, McDonald SP. Effect of donor- recipient age difference on graft
function and survival in live-donor kidney transplantation. Nephrol Dial Transplant 2010.

137
Chapter 6
High transplant rates of highly sensitized
recipients with virtual crossmatching in
kidney paired donation

138
High transplant rates of highly sensitized recipients with virtual crossmatching
in kidney paired donation
Paolo Ferrari, Samantha Fidler, Rhonda Holdsworth, Claudia Woodroffe, Gabriella
Tassone, Narelle Watson, Linda Cantwell, Greg Bennett, Alycia Thornton, Frank T
Christiansen, Lloyd D’Orsogna
The Australian paired kidney exchange (AKX) program was designed on the basis of
exclusion of clinically relevant antibodies detected by Luminex single antigen bead assay.
The low threshold for antibody exclusion, a mean fluorescence intensity (MFI) of greater
than 2000, conservatively excludes patients with a predicted positive complement-
dependent crossmatch. A concern was that highly sensitised patients might be
disadvantaged by excluding crossmatch compatible donors. This paper reviews the
match and transplant rates in the first year of the AKX program with respect to
recipient and donor characteristics, including blood group distribution, level of
recipient’s sensitization, and crossmatches.
These findings were published in:
Transplantation 2012: 94; 744-749
Contributions:
PF Prepared the manuscript, participated in study design,
participated in data analysis
SJF Performed all computer matching, participated in study
design, participated in data collection, participated in data
analysis, participated in writing the manuscript
RH, FTC, LD’O Participated in study design
CW Participated in data collection
GT, NW, LC, GB, AT Participated in study design, participated in data collection

139
CLINICAL AND TRANSLATIONAL RESEARCH
High Transplant Rates of Highly Sensitized Recipients With Virtual Crossmatching in
Kidney Paired Donation
Paolo Ferrari,1,2,10
Samantha Fidler,3,4
Rhonda Holdsworth,5 Claudia Woodroffe,
1
Gabriella Tassone,3 Narelle Watson,6 Linda Cantwell,7 Greg Bennett,8 Alycia
Thornton,9Frank T. Christiansen,
3,4 and Lloyd D’Orsogna
3,4
Background. In kidney paired donation (KPD), flexibility in the allocation of
incompatible pairs is required if a critical mass of pairs to efficiently find matches
cannot be reached.
Methods. In the Australian KPD program, virtual crossmatch is used for the allocation
of suitable donors to registered recipients. Matching is based on acceptable
mismatches, and donors are excluded from matching to recipients with donor-specific
antibodies (DSAs) greater than 2000 mean fluorescence intensity (MFI). Match and
transplant rates in the first year of the program were reviewed with respect to
recipient and donor characteristics, including blood group distribution, level of
recipient’s sensitization, and post allocation crossmatches.
Results. Four quarterly match runs were performed, which included 53 pairs and 2
altruistic donors. Human leukocyte antigen incompatibility accounted for 90% of the
listed pairs. In the second run, the DSA threshold was increased to greater than 8000
MFI, because no matches were found with standard allocation. Optional ABO-
incompatible matching was introduced from run 3. Matches were identified in 37
(70%) patients, of whom 92% had a negative crossmatch with their matched donor.
Crossmatch positive results were found only in recipients with DSAs greater than 2000
MFI in the second run. In 4 cases immunological reasons and in 4 cases other reasons
resulted in breakdown of chains and 17 patients not progressing to transplantation.
Eventually, 20 (38%) patients received a KPD transplant, and 35% of these had a
calculated panel-reactive antibody greater than 90%.
Conclusions. KPD using virtual crossmatch is a valid and effective solution for patients
with immunologically incompatible donors even in the context of highly sensitized
recipients.

140
Keywords: Kidney paired donation, ABO incompatibility, HLA incompatibility, Matching,
Computerization.
(Transplantation 2012; 94: 744-749)
The study was supported by the Australian Organ and Tissue Donation and Transplantation
Authority through the establishment of the National Paired Kidney Donation program and
funding of part of the staff (P.F., S.F., and C.W.).
The authors declare no conflicts of interest.
1Department of Nephrology, Fremantle Hospital, Perth, Western Australia, Australia.
2School of Medicine and Pharmacology, University of Western Australia, Perth, Western Australia,
Australia.
3Department of Immunology, PathWest, Royal Perth Hospital, Perth, Western Australia, Australia.
4School of Pathology and Laboratory Medicine, University of Western Australia, Perth, Western
Australia, Australia.
5National Transplant Services, Australian Red Cross Blood Service, Melbourne, Victoria, Australia.
6New South Wales Transplantation and Immunogenetics Service, Australian Red Cross Blood
Service, Sydney, New South Wales, Australia.
7Victorian Transplantation and Immunogenetics Service, Australian Red Cross Blood Service,
Melbourne, Victoria, Australia.
8 South Australian Transplantation and Immunogenetics Service, Australian Red Cross Blood
Service, Adelaide, South Australia, Australia.
9 Tissue Typing Laboratory, Pathology Queensland, Royal Brisbane and Women’s Hospital,
Herston, Queensland, Australia.
10Address correspondence to: Paolo Ferrari, M.D., Australian Paired Kidney Exchange Program,
Department of Nephrology, Fremantle Hospital, School of Medicine and Pharmacology,
University of Western Australia, Perth WA 6160, Australia.
E-mail: [email protected]
P.F., S.F., C.W., and L.D. participated in data analysis, performance of the research, and writing
of the paper. R.H. participated in performance of the research and data analysis. C.W., G.T.,
N.W., L.C., G.B., and A.T. participated in performance of the research. F.T.C. participated in data
analysis and writing of the paper.
Received 5 April 2012. Revision requested 24 April 2012. Accepted 23 May 2012.

141
Despite the increase in the number of deceased organ donors in recent years, live
kidney donation still remains a major source of kidney transplantations in Australia.
Not infrequently, a willing and healthy living donor is deemed incompatible owing to
blood group incompatibility or unacceptable donor-specific antibodies (DSAs). Kidney
paired donation (KPD) provides a solution to this dilemma by pairing two or more
incompatible pairs together to facilitate the exchange of live-donor kidneys between
the willing donors (1-4). The success of KPD depends on several factors, such as the
number of incompatible pairs in the database, the proportion of blood group-
incompatible versus human leukocyte antigen (HLA)-incompatible pairs, the level of
sensitization of enrolled patients, and the rules for allocation of KPD donors to
recipients. The Netherlands (1, 5) and the United Kingdom (UK) (3) have well-
established national KPD programs, whereas in the United States, several regional (6) or
single-center (2, 7) programs have established successful programs in the past few
years.
In Australia a national KPD program was established in August 2010. The
implementation of the Australian Paired Kidney Exchange (AKX) program required that
all participating transplant centers agree on donor and recipient medical suitability
criteria and the variables and rules used for allocation. We previously reported on the
allocation rules agreed for the AKX program (4), which were based on simulations
using different algorithms and data from a previous single-center KPD experience (8).
Our proposed approach was to ignore any HLA matching rules and to use matching
based on acceptable mismatches by excluding donors from matching to recipients
with DSAs greater than 2000 mean fluorescence intensity (MFI) for any class I or II
antibodies by Luminex single-antigen bead (SAB). This conservative approach to
antibody assignment was chosen to avoid the breakdown of identified chains due to
positive crossmatches (9) and to reduce the risk of inferior long-term outcome in the
presence of strong DSAs in patients with negative crossmatch at transplantation (10).
Depending on the level of sensitization of patients enlisted in a KPD program, our
approach could potentially disadvantage sensitized patients by excluding crossmatch-
compatible donors. We therefore undertook the task to review the activity of the first
12 months of the AKX program.

142
RESULTS
A total of 53 donor-recipient pairs were included in the 4 match procedures
performed between August 2010 and August 2011. There were 24 couples who
participated in 1, 14 in 2, 8 in 3, and 7 in all 4 rounds. Match run conditions are
summarized in Table 1. Twenty pairs were included in the first, 25 in the second, 26
in the third, and 33 in the fourth match run. In match runs 2 and 3, an additional
altruistic donor each contributed to the donor pool.
Table 1. Match run conditions for the quarterly match runs of the Australian KPD
program
Type of Immunological Incompatibility in Enlisted Pairs
Only 10% of recipients were included because of ABO blood group incompatibility
without HLA antibody against their coregistered donor. Most recipients (90%) were
included because of HLA sensitization; 40% were HLA and ABO incompatible with their
coregistered donor, and 50% were HLA incompatible (but ABO compatible) with their
coregistered donor. Table 2 summarizes the blood type distribution of donors and
recipients; 30% of the donors were blood group O, and there were twice as many
blood group O recipients. In the 53 registered recipients, the median calculated panel-
reactive antibody (cPRA) for loci -A, -B, -DR, and -DQ was 81% (mean, 71 ± 32). cPRAs of
greater than 75% and greater than 90% were found in 58% and 42% of the registered
recipients, respectively.

143
Table 2. ABO blood group distribution of donors and recipients in the 4 initial match
runs of the AKX program for KPD
Computer Matching
The matching algorithm does not consider any HLA matching rules, and allocation is
only based on acceptable mismatches by excluding donors from matching to recipients
with DSAs greater than 2000 MFI for any class I or II antibodies against any of the
donor HLA loci (4). The computer program selects between competing match offers on
the basis of prespecified ranking rules, such as favoring 3-way over 2- way exchanges,
to maximize the number of patients receiving a transplant, and then favoring patients
with low versus high match probability, which primarily gives an advantage to a
recipient with high versus low PRA. In match run 2, and despite the inclusion of an
altruistic donor, no suitable matches were identified using the 2000-MFI cutoff for
unacceptable mismatches, and a subsequent run was performed using the 8000-MFI
cutoff (Table 1). From match run 3, we agreed with referring centers that ABO-
incompatible matching could be considered as an option for selected patients with low
blood group-specific titers. After limiting possible ex- changes to 2-way and 3-way
chains, without limitation of chain length with altruistic donors and eliminating
multiple matches, 31 KPD and 2 cadaveric list recipients were matched through the
AKX program. Three recipients were matched with multiple donors in subsequent
match runs. The match probability by cPRA in the 27 crossmatch-negative matched
recipients compared with the 53 registered patients is shown in Figure 1.

144
Figure 1. Match probability by cPRA (-A, -B, -DR, and –DQ) in 27 crossmatch-negative
matched recipients among 53 registered patients. Whereas the probability of matching
was inversely correlated with the cPRA, a matching donor was found for most highly
sensitized recipients, and recipients with a cPRA greater than 90% still had a 43% match
probability
Calculated Panel-Reactive Antibody in Listed Versus Matched Recipients
There was an inverse relationship between cPRA and match probability. Of the 37
matched recipients, the matched rate was 86% if the cPRA was less than 25% but was
43% if the cPRA was 90% to 100% (Fig. 1). However, a matching donor in a chain
combination could still be identified in a significant proportion of highly sensitized
patients. Of the 53 listed recipients, 58% had a cPRA greater than 75%, and in 42% of
them the cPRA was greater than 90%. In patients who underwent transplantation, a
cPRA greater than 75% was present in 45%, and a cPRA greater than 90% was
present in 35% of the recipients (Fig. 2).

145
Figure 2. Pattern of cPRA (-A, -B, -DR, and -DQ) in 53 registered recipients and in 20
recipients who underwent transplantation.
Complement-Dependent Cytotoxic Crossmatches
In total, 37 complement-dependent cytotoxic (CDC) crossmatches were performed
between matched donors and recipients. All the KPD donors and the altruistic
donor re- called for CDC crossmatch testing in the first 2 rounds were also
crossmatched against all recipients on the trays. Thus, an additional 112 T-cell
crossmatches (TCXMs) and B-cell crossmatches (BCXMs) results were available for
analysis, in which 60% of recipients were tested against the donors despite the
presence of single or multiple DSAs. The aggregated results of all crossmatches are
reported in Table 3.

146
Table 3. Aggregated results of 149 CDC allogeneic crossmatches performed between 37
matched donors and matched or unmatched recipients, whose sera were available for
testing.
Crossmatch Results of Matched Recipients
All 27 recipients who were matched using the 2000-MFI cutoff for unacceptable
mismatches had a negative CDC TCXM and BCXM. In match run 2, a less stringent
exclusion of unacceptable mismatches setting the cutoff at 8000 MFI resulted in 10
patients finding a possible donor. In 7 patients, 1 or more DSAs at strengths ranging
from 2254 to 6753 MFI were present; in 4 patients with a low-level single DSA
(2254-3373 MFI), both TCXM and BCXM were negative. However, 3 patients with 1 or
more DSAs at a strength greater than 6000 MFI had a positive BCXM, but negative
TCXM, against their matched donor and were not accepted for transplantation
resulting in the breakdown of chains.
Three patients were matched to an ABO-incompatible donor because an initial blood
group titer indicated that they were suitable for ABO-incompatible transplantation.
How- ever, in 2 patients, additional testing against donor red blood cells revealed an
excessively high blood group antibody titer, and it was decided not to progress to
transplantation. Thus, after computer matching and CDC crossmatch testing, 27
recipients were booked for live-donor kidney transplantation.
Panel Crossmatch Results
There were 21 positive TCXM with positive BCXM and 32 with positive BCXM and
negative TCXM results. All patients with positive TCXM had 1 or more class I DSA at
greater than 8000 MFI. In two patients, the initial testing suggested a weak or

147
moderate DSA, but the strength of the DSA was found to be greater than 8000 MFI
when the Luminex assay was repeated in the immunoglobulin (Ig)M-depleted serum
sample. A positive BCXM was found in 47% of patients with DSAs at greater than 8000
MFI and in 38% with DSAs at 2000 to 8000 MFI (Fig. 3A). DSAs against C-locus were
responsible for 15% of positive TCXMs, and DSA against DQB1 accounted for 50% of
positive BCXMs (Fig. 3B).
Figure 3. DSA strength and specificity in crossmatch-positive assays from 112
crossmatches performed on unmatched panel recipients in match runs 1 and 2 against
available donor cells. A, Strength of DSA. B, Specificity of DSA in those with
crossmatch-positive assays.

148
Kidney Paired Donation Transplants and Outcomes
In the first year of the AKX program, 20 recipients have undergone successful kidney
transplantation. One 3-way chain and two 2-way chains did not progress to
transplantation. One offer was refused by the transplant surgeon because of concerns
in relation to the vascular anatomy of the donor kidney, 1 because of a donor
withdrawing consent, and 1 because of an acute illness of a matched recipient. The
breakdown of these chains resulted in 7 patients not under- going transplantation. Of
the patients who underwent transplantation, 18 were KPD recipients, and 2 were
transplant wait-list recipients who received the kidney from the last KPD donor in an
altruistic donor chain. This represents 34% transplant rate of all registered KPD
recipients, 49% of all matched recipients, and 74% of crossmatch-negative matches.
The mean follow-up period was 256 - 131 days, and 95% of the patients remained
rejection-free throughout this period. Fourteen patients underwent a total of 18
kidney biopsies (3 per cause, 15 protocol), and 6 patients did not have a kidney biopsy
either per cause or protocol. One patient with delayed graft function not requiring
dialysis demonstrated mild acute tubular necrosis on day 3 and showed BK virus
nephropathy at 3 months. One recipient with a cPRA of 99% who received a kidney
from an ABO-incompatible donor showed abundant C4d deposition and possible
antibody-mediated rejection with mild peritubular capillaritis. Records on renal
allograft function available to date revealed that serum creatinine levels were 108 ± 27
Kmol/L at discharge, 94 ± 22 Kmol/L at 3 months (n=20), 96 ± 29 Kmol/L at 6 months
(n=15), and 88 ± 11 Kmol/L at 1 year (n=5).
DISCUSSION
The first-year experience of the Australian KPD program demonstrates that by
using a stringent virtual crossmatch approach, it is possible to achieve match rates
of greater than 50% even with a small donor-recipient pool where most recipients
are highly sensitized. Thus, using a conservative approach to antibody assignment
to avoid positive crossmatches does not seem to significantly disadvantage
sensitized recipients.
These results are of particular importance in view of the relatively small number of
unsensitized ABO-incompatible recipients enrolled in the program, reducing the ability
to easily match donors to multiple recipients. In many instances, the barrier of blood
group incompatibility can be easily overcome without substantial changes in the
immunosuppressive regime (11, 12), and this has become standard practice in many

149
transplant centers in Australia, where the costs for apheresis for ABO-incompatible
transplants are not capped. This has contributed to the small number of ABO-
incompatible patients without HLA antibodies being listed in AKX.
The options for patients with high-level HLA sensitization are more limited, and there
are still concerns with regard to expense, increased morbidity, and inferior long-term
outcomes associated with desensitization techniques (10, 13, 14), although they have
been shown to provide a significant survival benefit for HLA-incompatible patients, as
compared with waiting for a compatible organ (15). If directed donation is not possible
because DSAs are not amenable to desensitization and conventional HLA matching in
the cadaveric program results in exceedingly long waiting time, the only hope for
highly sensitized recipients could be KPD. With the use of our virtual crossmatch
approach to KPD allocation (4), sensitized patients, with the exception of those with a
cPRA greater than 90%, do not seem to be overtly disadvantaged in favor of the
unsensitized patients. Moreover, that 35% of recipients who underwent
transplantation had a cPRA greater than 90% is a remarkable outcome. To perform
transplantation on a larger number of these more highly sensitized patients, a less
conservative approach to antibody assignment may be required. A restrictive policy to
reduce the increased risk for antibody-mediated rejection and the increased long-term
graft dysfunction will result in such transplantations being avoided in patients who
have no other options. Match run 2 demonstrates that a higher threshold for exclusion
from matching in the presence of DSAs of up to 8000 MFI resulted in 3 recipients with
negative TCXM and BCXM despite DSAs greater than 2000 MFI undergoing
transplantation without evidence of anti- body-mediated rejection on protocol
biopsies after up to 12 months of follow-up. On the other hand, the only instances of
positive BCXM in matched recipients were found with this level of antibody assignment,
leading to breakdown of chains. Moreover, the results of the crossmatch testing
performed against the panel of unmatched recipients demonstrate that all positive
TCXM and 85% of positive BCXM were found in the presence of DSAs at greater than
2000 MFI, which is in line with previously reported data (9). It is worth noting that a
significant proportion of recipients had HLA-C or DQ antibodies. This underlines the
importance of using SAB assay for better definition of the exact specificities in view of
the higher rates of acute rejection episodes especially antibody-mediated acute
rejections and graft losses for immunologic reasons among recipients with
pretransplant DSAs against HLA-C, -DP, and -DQ (14, 16, 17). We do not routinely
perform flow crossmatches because CDC cross- matching and SAB assay are well-
established techniques for transplantation organ assignment, and flow crossmatching is a

150
very sensitive technique that could unnecessarily disadvantage highly sensitized
recipients with a negative CDC crossmatch and low-level DSAs. However, in some of the
patients with DSAs 2000 to 4000 MFI, flow crossmatches were performed and found
to be positive and would therefore suggest that our approach is also a good
predictor of flow crossmatch results.
The threshold of 2000 MFI to exclude donors from matching to recipients with a DSA
seems to be an excellent predictor of negative CDC crossmatch for class I antigens.
This prediction is dependent on the accuracy of HLA anti- body testing. Initially, 1
sample was found to be crossmatch positive despite absence of DSAs greater than
2000 MFI. One possible explanation for this result is the presence of blocking IgM
antibodies (18), and, indeed, after IgM depletion, the index serum demonstrated a
significantly higher strength of the DSAs. This observation highlights the need to have
exactly agreed laboratory standards for correct anti- body assignment. An alternative
explanation would be the prozone effect (19), where steric hindrance from a high-level
HLA antibody could compete for binding by anti-IgG detection antibody on the SAB.
However, although we do not routinely perform testing to unmask prozone in our
laboratories, this problem seems to be uncommon, because we rarely encounter
positive crossmatches without apparent DSA.
An alternative consideration to allow highly sensitized recipients the chance of live-
donor kidney transplantation is to leave the decision about whether and how to
proceed to the discretion of the transplant center, when low levels of DSA are
amenable to early therapeutic intervention. A review of all crossmatch data available
indicates that approximately 20% of donor-recipient combinations that were excluded
by virtual crossmatching because of DSAs 2000 to 8000 MFI had a negative TCXM and
BCXM, and in most instances, there were only 1 or 2 DSAs at a strength of greater than
4000 MFI. The risk of this approach is that identified matches have a greater risk of
breakdown, because the initial acceptance by the transplant center may later be
withdrawn. The result will be that the other immunologically suitable pairs that were
in the same chain will miss out on the potential organ exchange. Because donors have
to be re-called to provide fresh samples for crossmatches, the psychological and
emotional implications of informing them of a potential match but to be told later that
the match had been undone should not be discounted. In our program, there were 7
pairs (two 2-way and one 3-way chains) who were scheduled for exchange surgeries
and who did not progress to transplantation. Anecdotal reports by clinicians caring for
these patients would indicate significant emotional distress to those pairs who did not

151
progress to transplantation after the initial promise was not fulfilled.
When compared with available data from the first-year activity of other programs in
the Netherlands (1), the UK (3), and Texas (7), the transplant rates of the AKX program
(34% of enrolled pairs) seem to be excellent. Compared with the cumulative number
of enrolled recipients, the transplant rate in the first year was 40% in the Dutch
program (1), 9% in the UK (3), and 14% in the Austin (7). It is worth noting that these
programs differ significantly in the proportion of recipients included because of pure
ABO incompatibility with their coregistered recipients without the presence of
significant HLA sensitizations. Recipients who were ABO incompatible with their
intended donor were 56% in the Dutch program (1), 44% in the UK (3), and 36% in the
Austin (7), compared with only 10% in Australia. On the other hand, in contrast to our
program, neither the Dutch nor the UK program included altruistic donors in their first
year. The inclusion of altruistic donors is an effective approach to facilitate matching in a
KPD program (20). The inclusion of 2 altruistic donors in AKX resulted in a 4-way chain (3
KPD recipients and 1 wait-list recipient) and a 3-way chain (2 KPD recipients and 1 wait-
list recipient). If the altruistic donors were removed, only 2 KPD recipients could have
been matched in a 2-way chain. Thus, the total number of transplants purely by KPD
matching would have been 15, resulting in a transplant rate of 28%.
Early outcomes of the 20 recipients who underwent transplantation were excellent; all
patients left the hospital within the center’s usual length of stay without any surgical
complications or early rejection episodes, with only 1 case of delayed graft function not
requiring dialysis, unrelated to the relatively short cold ischemia of 6 hours of the
shipped kidney. At this stage, there are not sufficient data to comment on long-term
allograft outcomes. However, the observation that with the currently available follow-
up data, a biopsy-proven rejection was found in only 1 recipient, who had a cPRA of
99% and received a kidney from an ABO-incompatible donor, of the 20 patients who
underwent transplantation indicates that avoiding moderate and strong DSAs against
all HLA loci is a valid strategy to minimize the risk of rejection. The major stumbling
block in the AKX program to date has been the failure to progress to transplantation
surgery in 25% of crossmatch-negative matched pairs for non-immunological reasons.
Strategies to minimize the rate of non-conversion of matches to transplantations have
been devised.
In conclusion, high transplant rates in a KPD program using virtual crossmatching can
be achieved even with a small pool consisting largely of highly sensitized recipients,
indicating that KPD is a valid and effective solution for patients with immunologically

152
incompatible donors even in the context of highly sensitized recipients.
MATERIALS AND METHODS
The AKX program was established in August 2010 as a new national initiative to
enhance live kidney donation. Within the first 12 months, 78 incompatible donor-
recipient pairs had been referred to the program. Allocation procedures to match
compatible combinations were scheduled every 3 months. Only pairs who satisfied all
agreed medical criteria for donor and recipient registration, molecular HLA typing, and
HLA alloantibody testing were included in match run procedures. Thus, 53 donor-
recipient pairs were included in any of the 4 match procedures performed between
October 2010 and August 2011. Crossmatches between the new donors and recipients
were performed in the histocompatibility laboratory of the matched donors’ state.
Human Leukocyte Antigen Typing and Detection of Anti-Human Leukocyte Antigen
Antibodies
Donor molecular HLA typing and recipient HLA antibody testing for the loci -A, -B, -C, -
DRB1, -DPB1, -DQB1, and -DRB3/4/5 were performed at the 5 state histocompatibility
laboratories as previously reported (4). Donor HLA typing was performed using direct
DNA sequencing. Recipients were tested for HLA class I and II directed IgG antibody in
their sera using SAB Luminex technology (Luminex, One lambda Inc., Conga Park, CA);
the MFI signal for each SAB was normalized against the negative control to correct for
nonspecific binding.
Calculated Panel-Reactive Antibody
The cPRA of enrolled recipients was based on HLA-A, -B, -DR, and -DQ antigen
frequencies derived from the phenotypes of 200 representative participants in the
Busselton Health Study, which were found to have similar frequencies for HLA-A, -B,
and -DR of donors in the National Organ Matching System (NOMS) registry and the
United Network for Organ Sharing (data not shown). The correlation between the
cPRA derived using phenotypes from our cohort and the cPRA obtained using the
OPTN calculator was R2=0.981. We compared the cPRA distribution for patients who
were registered, were matched, and underwent transplantation.
Computer Program Matching
Allocation of suitable live-donor matches was performed using a software module
developed by the NOMS as previously described (4). The software takes advantage of
advances in HLA technology to enable virtual crossmatching. HLA alleles of each locus

153
and HLA antibody specificities were entered in the computer program at the 4-digit
level. Briefly, the algorithm does not consider any HLA matching rules for allocation,
and matching is only based on acceptable mismatches by excluding donors from
matching to recipients with DSAs greater than 2000 MFI for any class I or II antibodies
against any of the donor HLA loci -A, -B, -C, -DRB1, -DPB1, -DQB1, -DQA1, and -
DRB3/4/5 (4). By default, the program considers exclusively ABO-compatible
matching, but the option of ABO-incompatible matching is available in selected cases.
Complement-Dependent Cytotoxic Crossmatches of Matched Pairs
After suitable matches in a chain were identified and the peak and historical antibody
record was reviewed, TCXM and BCXM between a matched donor and recipient were
performed in the histocompatibility laboratory of the matched donor’s state using
fresh donor cells in duplicate. If all links within a chain had negative CDC crossmatches,
donation procedures in the centers were arranged within 3 months of allocation and
performed simultaneously. Sera from all recipients were distributed 1 week before
match runs 1 and 2, but from match run 3 onward, only sera from matched recipients
were sent to the laboratory of the matched donor. Donors re-called for CDC
crossmatch in runs 1 and 2 were crossmatched against all recipients on the trays to test
the accuracy of the virtual crossmatch in predicting a negative crossmatch in relation to
SAB antibody strength.
ACKNOWLEDGMENTS
The authors thank the collaborators of all participating transplant centers, in particular,
those involved in exchange transplant surgeries at Westmead Hospital, Royal Prince Alfred
Hospital, John Hunter Hospital, Prince of Wales Hospital, Royal North Shore Hospital, and
The Children’s Hospital at Westmead, in New South Wales; Monash Medical Centre and Royal
Melbourne Hospital, in Victoria; and Sir Charles Gairdner Hospital and Royal Perth Hospital,
in Western Australia. The authors also thank Ms Jenni Wright and the NOMS team for their
support throughout the program and Dr Scott Campbell, chair of the National Renal
Transplant Advisory Committee, for his advice and support. Finally, the authors thank the
patients and their donors for agreeing to participate in this pioneering study.

154
REFERENCES
1. de Klerk M, Keizer KM, Claas FH, et al. The Dutch national living donor kidney exchange program.
Am J Transplant 2005; 5: 2302.
2. Montgomery RA, Zachary AA, Ratner LE, et al. Clinical results from transplanting
incompatible live kidney donor/recipient pairs using kidney paired donation. JAMA 2005;
294: 1655.
3. Johnson RJ, Allen JE, Fuggle SV, et al. Early experience of paired living kidney donation in the
United Kingdom. Transplantation 2008; 86: 1672.
4. Ferrari P, Fidler S, Wright J, et al. Virtual crossmatch approach to maximize matching in
paired kidney donation. Am J Transplant 2011; 11: 272.
5. de Klerk M, Witvliet MD, Haase-Kromwijk BJ, et al. Hurdles, barriers, and successes of a
national living donor kidney exchange program. Transplantation 2008; 86: 1749.
6. Hanto RL, Reitsma W, Delmonico FL. The development of a successful multiregional kidney
paired donation program. Transplantation 2008; 86: 1744.
7. Bingaman AW, Wright FH, Murphey CL. Kidney paired donation in live-donor kidney
transplantation. N Engl J Med 2010; 363: 1091.
8. Ferrari P, Woodroffe C, Christiansen FT. Paired kidney donations to expand the living donor
pool: the Western Australian experience. Med J Aust 2009; 190: 700.
9. Morris GP, Phelan DL, Jendrisak MD, et al. Virtual crossmatch by identification of donor-
specific anti-human leukocyte antigen anti- bodies by solid-phase immunoassay: a 30-month
analysis in living donor kidney transplantation. Hum Immunol 2010; 71: 268.
10. Lefaucheur C, Loupy A, Hill GS, et al. Preexisting donor-specific HLA antibodies predict outcome
in kidney transplantation. J Am Soc Nephrol 2010; 21: 1398.
11. Flint SM, Walker RG, Hogan C, et al. Successful ABO-incompatible kidney transplantation
with antibody removal and standard immunosuppression. Am J Transplant 2011; 11: 1016.
12. Montgomery JR, Berger JC, Warren DS, et al. Outcomes of ABO- incompatible kidney
transplantation in the United States. Transplantation 2012; 93: 603.
13. Gloor J, Stegall MD. Sensitized renal transplant recipients: current protocols and future
directions. Nat Rev Nephrol 2010; 6: 297.
14. Ntokou IS, Iniotaki AG, Kontou EN, et al. Long-term follow up for anti-HLA donor specific
antibodies postrenal transplantation: high immunogenicity of HLA class II graft molecules.
Transpl Int 2011; 24: 1084.
15. Montgomery RA, Lonze BE, King KE, et al. Desensitization in HLA- incompatible kidney recipients
and survival. N Engl J Med 2011; 365: 318.
16. Gilbert M, Paul S, Perrat G, et al. Impact of pretransplant human leukocyte antigen-C
and -DP antibodies on kidney graft outcome. Transpl Proc 2011; 43: 3412.
17. Tran TH, Dohler B, Heinold A, et al. Deleterious impact of mismatching for human leukocyte

155
antigen-C in presensitized recipients of kidney transplants. Transplantation 2011; 92: 419.
18. Kosmoliaptsis V, Bradley JA, Peacock S, et al. Detection of immunoglobulin G human
leukocyte antigen-specific alloantibodies in renal transplant patients using single-antigen-
beads is compromised by the presence of immunoglobulin M human leukocyte antigen-
specific alloantibodies. Transplantation 2009; 87: 813.
19. Schnaidt M, Weinstock C, Jurisic M, et al. HLA antibody specification using single-antigen
beads: a technical solution for the prozone effect. Transplantation 2011; 92: 510.
20. Roodnat JI, Zuidema W, van de Wetering J, et al. Altruistic donor triggered domino-paired
kidney donation for unsuccessful couples from the kidney-exchange program. Am J
Transplant 2010; 10: 821.

156
Chapter 7
Transnational validation of the
Australian algorithm for virtual
crossmatch allocation in kidney paired
donation

157
Transnational validation of the Australian algorithm for virtual crossmatch
allocation in kidney paired donation
Georg A Böhmig, Samantha Fidler, Frank T Christiansen, Gottfried Fischer, Paolo Ferrari
Validation of the negative predictive value of the Australian paired kidney exchange (AKX)
program was achieved by the crossmatching of identified pairs. An unexpected positive
crossmatch was rare in the first year of the program, however whether further matches
with negative crossmatches were being excluded by the low threshold for antibody
exclusion was unclear. The transplant unit in Vienna, Austria supplied HLA antibody and
typing data from sixteen pairs in their recently developed paired exchange program. The
Austrian program matches compatible pairs based on a negative complement-dependent
and flow crossmatch, with donor specific HLA antibody with a mean fluorescence
intensity (MFI) less than 2000. The recipient HLA antibody data and donor HLA typing of
the Austrian pairs was matched using the Australian kidney exchange (AKX) computer
algorithm in order to compare virtual and actual crossmatch results. This paper reviews
the match and virtual crossmatch results in the Austrian paired kidney exchange
cohort.
These findings were published in:
Human Immunology 2013: 74; 500-505
Contributions:
PF Prepared the manuscript, participated in data analysis
SJF Performed all computer matching, participated in study
design, participated in data collection, participated in data
analysis, participated in writing the manuscript
GB, GF Participated in study design, participated in data collection
FTC Participated in study design

158
Human Immunology 74 (2013) 500–505
Transnational validation of the Australian algorithm for virtual
crossmatch allocation in kidney paired donation
Georg A. Böhmig a, Samantha Fidler b,c, Frank T. Christiansen b,c, Gottfried Fischer d, Paolo Ferrari e,f,⇑ a Division of Nephrology and Dialysis, Medical University Vienna, Vienna, Austria
b Department of Immunology, PathWest, Royal Perth Hospital, Perth, Western Australia, Australia
c School of Pathology and Laboratory Medicine, University of Western Australia, Perth, Western Australia, Australia
d Department for Blood Group Serology, Medical University Vienna, Vienna, Austria
e Department of Nephrology, Fremantle Hospital, Perth, Western Australia, Australia
f School of Medicine and Pharmacology, University of Western Australia, Australia
a r t i c l e i n f o
Article history:
Received 1 November 2012
Accepted 24 January 2013
Available online 1 February 2013
Abbreviations: AKX, Australian paired Kidney eXchange; BCXM, B-cell crossmatch; PRA,
Panel-reactive antibody; DSA, Donor-specific antibodies; KPD, Kidney paired donation;
MFI, Mean fluorescence intensity; NOMS, National Organ Matching System; TCXM, CDC
T-cell crossmatch.
⇑ Corresponding author at: Department of Nephrology, Fremantle Hospital, Perth,
Western Australia 6160, Australia. Fax: +61 8 9431 3619.
E-mail address: [email protected] (P. Ferrari).
a b s t r a c t
An independent pool of 16 incompatible live donor–recipient pairs registered
at the Vienna transplant unit was applied to test whether virtual crossmatch
allocation used in the Australian kidney paired donation (KPD) program reliably
predicts negative crossmatches. High resolution HLA data were entered into
the computer-matching algorithm and allocation was performed excluding any
www.ashi-hla.org
journal homepage: www.
elsevier.com/locate/ humimm

159
DSA > 2000MFI. CDC and flow crossmatch data of recipients against any of the
donors were available for 112 crossmatch combinations. The computer
program identified 19 possible pairings in 2-way or 3-way chains in multiple
combinations. The top ranked combination included one 3-way and two 2-way
ABO-compatible chains. Where crossmatches were available all recipients
were CDC crossmatch negative with the computer-matched donor. Excluding
allocation of KPD donors in the presence of DSA > 2000MFI had a negative
predictive of 99.9% for CDC and 96.4% for flow crossmatch. In the 12 pairings
with ≥1 DSA against crossmatched donors there was a negative CDC and flow
crossmatch. These results show excellent correlation between matching using
virtual crossmatch and actual crossmatch results. Using the 2000MFI cut-off
the number of potentially unacceptable CDC and flow crossmatch positive
pairings identified by virtual crossmatching is low, but some potential
crossmatch negative pairings are missed.
1. Introduction
Live kidney donation is an important source of kidney transplantations in many
countries. When live donors are unable to donate to their intended recipients
because of blood group or HLA-incompatibility, kidney paired donation (KPD) can
help overcome this barrier by pairing two or more incompatible pairs together to
facilitate the exchange of live donor kidneys between the willing donors [1–4]. The
rules for allocation of suitable pairings are paramount for the success of a KPD
program. We previously reported on the allocation algorithm of the Australian
paired Kidney eXchange (AKX) program [4], which was based on simulations using
different algorithms and data from a previous single center KPD experience [5]. Our
proposed approach was to ignore any HLA antigen matching rules and to use
matching based on acceptable mismatches by excluding donors from matching to
recipients with donor-specific antibodies (DSA) > 2000 mean fluorescence
intensity (MFI) for any class I or II antibodies detected by Luminex single-antigen
bead (SAB), in order to avoid the breakdown of identified chains due to positive
crossmatches [6] and to reduce the risk of inferior long-term outcome in the
presence of strong DSA in patients with negative crossmatch at transplantation
[7]. The proposed approach has been criticized [8], on the basis that the ability of
solid phase HLA antibody assays to provide quantifiable data are controversial and

160
although we suggested that the flow cytometric crossmatches may have been
positive in some cases, no actual flow cytometric crossmatches were performed [4].
Further validation of the proposed virtual crossmatch allocation based on exclusion
of unacceptable HLA antibodies by solid phase is therefore required.
The Vienna renal transplant service is in the preliminary stages of introducing a
KPD program to the country including the establishment of efficient serological
allocation strategies to accurately predict crossmatch outcomes and select HLA
antibody-compatible 2- to 3-way chains. The aim of this study was to compare if
the virtual crossmatch approach using the Australian KPD computer allocation
would predict negative crossmatches using the Austrian pool and whether these
stringent criteria would exclude potential crossmatch negative pairings to be
considered for matching.
2. Subjects and methods
2.1. Study subjects
As of September 2011, 16 incompatible donor–recipient pairs were registered at
the Vienna transplant unit. Baseline characteristics of donors and recipients are
given in Table 1. Recipients’ panel-reactive antibody (PRA) values for HLA class I
specificities were directly calculated according to the results obtained by CDC
screening against a panel of 50 HLA-typed volunteers using peripheral blood
mononuclear cells. Because many recipients had class II HLA antibodies and the
occurrence of antibody against HLA-DQ was high in recipients with previous
transplant, recipients’ calculated PRA (cPRA) for HLA-A, -B, -DR and -DQ antigen
was derived based on antigen frequencies from the UNOS registry for Caucasians
[9].

161
2.2. Solid phase antibody detection
All laboratory evaluations were performed at the Vienna unit as described
elsewhere [10]. Donor molecular HLA-typing and recipient HLA antibody testing
for HLA-A, -B, -C, -DRB1, -DPB1, -DQB1 and DRB3/4/5 were performed in
accordance with the standards used in the AKX program as previously reported
[4]. Donor HLA- typing was performed using direct DNA sequencing. Recipients
were tested for HLA class I and class II directed IgG antibody in their sera
using single antigen bead (SAB) technology (One Lambda, Canoga Park, CA, USA)
on a Luminex platform performed on neat, non-IgM depleted samples. The MFI
signal for each SAB was normalized against the negative control to correct for non-
specific binding. Recipients without DSA (<500MFI) or with only weak DSA
(<2000MFI) were considered to have no HLA antibodies against matched donors
(Luminex negative).
2.3. Complement-dependent cytotoxic (CDC) and flow cytometry crossmatches
After what was considered a sufficiently large pool of blood group or HLA-
incompatible pairs who joined the Vienna program, all recipients underwent T-
and B-CDC (no enhancement) and T- and B-cell flow crossmatching against any of
the donors in the program. However, some of the patients were only typed and
screened because they joined the register after the initial series of crossmatches.
Thus, full crossmatch data (CDC and flow) of recipients against any of the donors,
excluding co-registered donor–recipient pairs, was available for a total of 112
crossmatch combinations. No crossmatch data were available for 4 recipients. The
crossmatch data were kept blinded to the Australian team running the computer
matching until the matrix and potential KPD chains were identified.
2.4. Computer program matching
Allocation of suitable live donor matches was performed using a software module
developed by the National Organ Matching System (NOMS) as previously
described [4]. HLA data of all Austrian donors and recipients was entered into the
NOMS computer module. HLA-alleles of each locus and HLA antibody specificities
were entered in the computer program at the 4-digit level. The computer program

162
enables virtual crossmatching by matching recipients to suitable donors based on
acceptable mismatches. The algorithm does not consider any HLA antigen
matching rules for allocation and donors are excluded from matching to
recipients with DSA > 2000MFI for any class I or II antibodies against any of the
do- nor HLA-A, -B, -C, -DRB1, -DPB1, -DQB1, -DQA1 and -DRB3/4/5 loci [4]. For KPD
allocation purposes only HLA antibody with strength >2000MFI were authorized
for exclusion from matching to donors with the target HLA antigen. A cumulative
approach of total DSA strength was not considered for KPA allocation. By default
the program now considers ABO-incompatible matching, but ABO compatible
matching only is available on demand. The computer program selects between
competing match offers based on pre- specified ranking rules, such as favouring 3-
way over 2-way exchanges, in order to maximize the number of patients receiving
a transplant, and then favouring patients with low versus high match probability,
which primarily gives an advantage to recipients with a higher PRA. The computer
program also excludes previous donor HLA-mismatches or donor–donor age
difference of >30 years.
2.5. Comparison of virtual and actual crossmatch results
The probability of a positive crossmatch in relation to the strength of DSA for class I and
class II DSA was analysed for both T- and B-cell CDC and flow crossmatches. For donor-
recipient combinations where the recipient had ≥1 DSA the cumulative strength of DSA
was determined by adding the MFI for each DSA. The cumulative strength of DSA was
grouped in five categories, 0-2000 (DSA negative), 2000-4000, 4000-10000, 10000-20000
and >20000MFI. Because T cells do not constitutively express HLA class II, the results for
class II DSA were compared to the B-cell crossmatch results only. B cells express both HLA
class I and II so a positive B-cell crossmatch may be due to antibodies directed against
HLA class I or II or both. Therefore data for class I DSA was compared to the results
of both T- and B-cell crossmatches.

163
2.6. Statistical analysis
The sensitivity and specificity of predicting positive crossmatch results for pairings
matched in the presence of DSA and the predictive value for negative
crossmatches for pairings matched without DSA was estimated for two cut-off
threshold of 2000MFI and 4000MFI, respectively [11].
3. Results
3.1. Computer matching
Most pairs (69%) were included because of HLA-incompatibility, five pairs were
ABO-incompatible with a PRA of <5%, the proportion of blood group O donors and
recipients (31%) was identical (Table 1). Of the 240 possible one-way combinations
achievable with 16 pairs (i.e. (N-1) x N), the computer program identified 75
suitable one-way donor-recipient matches based on the virtual crossmatch
criteria. Six recipients did not have any match because they had 1 or more DSA
against any of the donors in the pool. The one-way matches resulted in 19 possible
pairings in 2-way or 3- way chains in multiple combinations. Without consideration
of crossmatch results the top ranked combination where each pair appeared only
once in any chain included one 3-way and two 2- way ABO-compatible chains
(chain 5, 9 and 28). The second ranked combination included again the same 3-
way chain and two different 2-way chains (chain 5, 15 and 22), although in one
case an acceptable match was found between an AB donor and an A recipient. In
all instances where crossmatch data were available, these recipients were
complement-dependent cytotoxic (CDC) and flow-crossmatch negative with the
computer-matched donor (P < 0.001).

164
Table 1. Baseline characteristics of donors and recipients in the 16 pairs of the
Vienna transplant center.
3.2. Analysis of available HLA antibodies and crossmatch data
All recipients had complete Luminex HLA data and 12 had complete or partial
crossmatch data, but no crossmatch data were available for four recipients
who were listed at a later stage. Excluding crossmatch results between co-
registered donors and recipients, 112 full CDC and flow crossmatch data were
available for analysis. Of these, 28 pairings were DSA negative and 84 had at
least 1 DSA against their crossmatched donors, 61 had both ≥1 class I and ≥1
class II DSA, 3 pairings had ≥1 class I DSA only, and 20 had ≥1 class II DSA only.
In the 28 DSA negative pairings there were 27 with both negative flow and CDC
crossmatches and 1 with positive flow, but negative CDC crossmatch (Table 2).

165
In the DSA positive pairings 41 had a positive and 43 had a negative CDC
crossmatch. Of those with positive CDC crossmatch 40 had both positive flow
and CDC crossmatches. In the 43 DSA positive and CDC negative, 30 had positive
flow and 13 had both negative CDC and flow crossmatches (Table 2). In these
cases 2 or more DSAs were present in only 18% of pairings, compared to ≥2 DSA
in 80% of those with positive crossmatch. Moderate DSA in the range of 2000–
4000MFI were present in 8 crossmatch negative Luminex positive pairings.
Interestingly, all these cases only had class II DSA with specificities to DP and DQ
antigens against the crossmatched donor.
In the pairings without crossmatch data, 68 had 1 or more DSA against any of
the donors in the pool and 60 were Luminex DSA negative. The total number of
DSA negative pairings with or without crossmatch data were 88, which is
higher than the total number of DSA negative pairings identified by the
computer matching algorithm (N = 75), because the computer program
excludes previous mismatches or donor–donor age difference of >30 years.
Table 2. CDC and flow cytometry crossmatch results from 112 donor-recipient
pair combinations where crossmatch data were available in relation to the
presence or absence of any donor-specific antibodies (DSA) at >2000MFI.

166
3.3. Value of DSA strength to predict crossmatch results
The probability of a positive T- or B-cell CDC or flow crossmatch in relation to DSA
strength by class I and class II antibodies is shown in Fig. 1. The sensitivity and
specificity of any DSA positive (class I and/or II) computer matching to predict a
positive (T- and/ or B-cell) crossmatch and the negative predictive value of DSA
negative matching to identify crossmatch negative results is reported in Table 3.
The cutoff of 2000MFI for DSA to exclude recipients from matching to donors with
unacceptable antigens had a sensitivity of 98.6% and a specificity of 69.2% for a
positive CDC and flow crossmatch result (Table 3). If only a positive CDC
crossmatch result was considered sensitivity was 97.6% and a specificity of 38.6%.
If the cut off for DSA to exclude recipients from matching to donors with
unacceptable antigens were increased to 4000MFI sensitivity would be 97.6% and
a specificity of 89.7% for a positive CDC and flow crossmatch result. The negative
predictive value for both negative CDC and flow crossmatches was 99.9% using the
2000MFI cut off. If the cut off were increased to 4000MFI negative predictive
value for negative CDC and flow crossmatch would be 94.4% (Table 3). The
relationship between number of DSA and crossmatch results was also analyzed.
There was however no ‘dose–response’ relationship between increasing number
of DSA and crossmatch positivity. For instance, for CDC T-cell crossmatch a positive
result was found in 50%, 55%, 46%, 67% if there were 1, 2, 3 or ≥4 DSA
respectively. If there were no DSA the crossmatch was negative in 99% of cases.
The MFI for each DSA in pairings with 1–2 DSA and a positive crossmatch were
generally high (>10000MFI), whereas some pairings with ≥4 DSA as a cause of
positive had multiple moderate DSA.

167
Table 3. Sensitivity and specificity of donor-specific antibody (DSA) positive
computer matching to predict a positive crossmatch and negative predictive
value of DSA negative matching to identify crossmatch negative results using
virtual crossmatching in kidney paired donation.
Estimations were calculated using two cut-offs of Luminex HLA antibodies to exclude
recipients from matching to incompatible donors. Results are in % (and confidence
interval).
Figure 1. Probability of a positive crossmatch in relation to the cumulative
strength of donor-specific antibodies (DSA) in mean fluorescence intensity (MFI)
for class I (panel A) and class II (panel B) DSA.
The top panels show results for CDC crossmatches, the bottom panels show data for flow
crossmatch results. The results for class II DSA are reported for B-cell crossmatches only,
because T cells do not constitutively express HLA class II antigens.

168
4. Discussion
This analysis provided a unique opportunity to evaluate a KPD allocation algorithm
that utilizes virtual crossmatch strategy based on the allocation of recipients to
suitable donors that takes into consideration acceptable mismatches based on Luminex
HLA antibody assignment in an attempt to address the concerns previously raised by
Bingaman et al. [8] with regard to the proposed virtual allocation for KPD [4]. The present
findings demonstrate that the Australian KPD allocation algorithm allows computer
matching of live donors to recipients that will result in nearly 99% of identified matches
having a negative CDC and flow crossmatch. On the other hand this high sensitivity comes
at a cost of a low specificity, with many Luminex positive patients with DSA above the
threshold used for exclusion of matching that could potential have a negative CDC and/or
flow crossmatch. Although a weakness of this study relates to the nature of the
population studied, which is small and with only a modest degree of sensitization
based on cytotoxic PRA for class I only, the immunological profile of our recipients
compares favourably with cohorts of other national programs [3,12,13]. Many
recipients from the Vienna center were sensitized against class II HLA antibody
and not surprisingly anti- DQ antibody were frequently observed in recipients with
previous transplant resulting in a cPRA of 66 ± 41% and half of the recipients having
a cPRA >90%. In the Austrian program 75% of recipients were enrolled because of
HLA incompatibility to their co-registered donor, which is similar to the rate
observed in the Australian program (85%) [13], and significantly higher than the
rate observed in the Dutch (44%) [12] and the UK (56%) programs [3].
In recent years several algorithms for allocation of KPD pairs have been developed
to select possible exchanges based on a points scoring system that includes the
number of HLA-mismatches, % PRA, distance between the exchange centers,
donor age differences, CMV status and other factors [3,14,15]. The sensitivity and
specificity of these algorithms has not been widely tested and most of the
information on expected matched rates in relation to the number of registered
donor–recipients pairs have been based on simulation [3,15]. Once the computer
finds a match, crossmatches between matched donors and recipients are still
required before proceeding to transplantation and not infrequently even a single
unpredicted positive crossmatch prevents two or more pairs progressing to kidney
transplantation [16]. Because CDC and flow crossmatches are both cost and labor
intensive, if a recipient has a positive crossmatch with a computer matched donor,
additional crossmatches for this recipient against any other donors whose cells

169
may be available are usually not performed and/or reported.
The advantage of the cohort we used in our study is that for a large number of
recipients, both CDC and flow crossmatches had been performed in advance without
consideration of any putative compatibility. This has allowed us to assess whether the
allocation rules adopted for the Australian KPD program, and that were mainly based
on simulated data, are appropriate. The Australian matching algorithm uses high
definition of recipient HLA antibodies and donor HLA antigens to match KPD pairs with
the objective to achieve the maximum number of possible matches with predicted
negative crossmatch [4]. The Luminex threshold of 2000MFI was chosen because in
our experience a CDC crossmatch between a donor and recipient with a weak DSA is
almost invariably negative. If no DSA > 2000MFI was present, the probability of a
positive CDC crossmatch was negligible and the probability of a positive flow
crossmatch was 4%. The specific reason for a positive flow in the absence of DSA was
not investigated. Clearly the sensitivity of flow cytometry is higher than CDC
crossmatching [17], and positive flow crossmatches are not unusual in the presence of
a weak DSA (500–2000MFI). An alternative explanation is that some donor HLA alleles
are not represented in the bead panels and our algorithm does not take into account
serotypes for missing alleles. There was a clear dose–response relationship between
the cumulative DSA strength and the probability of a positive B-cell crossmatch for
class II DSA. Although not so clear-cut, this relation- ship was also present for the
association between cumulative strength of class I DSA and T- or B-cell crossmatches.
Interestingly, the difference in sensitivity values between CDC + flow results and CDC
only was not statistically significant (Table 3), whereas the difference in specificity
values between CDC + flow results and CDC results only was highly significant. The
present data indicates that using a threshold of 2000MFI will predict a negative CDC
crossmatch in virtually all of cases and rising the threshold to 4000MFI it would still
provide a negative predictive value of 97.2%. Thus, this prudent approach seems to
meet the objective to minimize the number of positive CDC crossmatches.
Attempts to define a cut off for Luminex technology, allowing the prediction of a
positive cross-match using either CDC or flow crossmatch have been hampered by the
complexity of the problem and differences in experimental design [18–20]. Our
data, along with the recent findings reported by Moreno et al. [21], contribute in
improving our understanding of the clinical predictive value of HLA antibodies by
Luminex technology in the context of virtual crossmatch. One drawback of the
current allocation rules of the Australian algorithm is that it doesn’t use different

170
values for HLA-C, DRB3/4/5, DQ and DP compared to HLA-A, B, and DRB1.
However, based on correlation with crossmatch results and density of antigen on
the beads these should be treated differentially. The observation in our cohort
that eight crossmatch negative cases had moderate DSA in the range of 2000–
4000MFI and all these cases had exclusively class II DSA with specificities to DP and
DQ antigens corroborates this view. Indeed, if anti-HLA antibody directed against
the HLA-C, DRB3/4/5 and DP locus were ignored the specificity of DSA positive
computer matching to predict a positive crossmatch would increase, without
affecting the negative predictive value of DSA negative matching to identify
crossmatch negative results.
For patients with high-level HLA-sensitisation the option of HLA-incompatible live
kidney transplantation [7,22,23] is often limited by the presence of multiple and
high-titre DSA that are not amenable to desensitisation. These patients also have
exceedingly long waiting time on the deceased donor list. Since many programs do
transplant patients with DSA ranging from 2000 to 8000MFI when the actual
crossmatch is negative, our approach could disadvantage such patients by
excluding crossmatch compatible donors and inappropriately deny a patient
access to transplantation.
The task of assigning an antigen as unacceptable in a KPD program where multiple
centers with differing expertise in managing immunological complex patient are
involved is daunting. Cut-offs must be sufficiently stringent to prevent positive
crossmatches, but should not be so rigid that they disallow transplants that some
centers would consider compatible. One interesting observation is that in pairings
with DSA in the 2000–4000MFI range a significant proportion of CDC and also flow
crossmatches have a negative result. Thus, by increasing the allocation cut-off to
4000MFI in the present cohort, 65% of the Luminex positive, but crossmatch
negative pairings would have been matched in the KPD allocation, increasing the
pool size of one-way donor–recipient pairs to be linked in chains and combinations
by 25%. This increase in the cut-off level appears to be associated with an
acceptable predicted rate of positive CDC crossmatches (rv3%), but undoubtedly
higher rates of positive flow crossmatches (rv10%). While transplantation will
likely not proceed in the setting of a positive CDC in the presence of a DSA,
desensitisation to enhance transplant rates using donor exchange may be

171
considered in the setting of a single weak-to-moderate DSA and positive flow
crossmatch [24]. Cut-offs may need to be tailored to the level of HLA sensitisation
and blood group distribution of recipients registered in the program. Continuous
adjustment of the cut-off may be subject to regulatory control in a national or
regional program and thus may be difficult to achieve. Such decision must also
take account of the likelihood of long-term allograft outcome with increasing
evidence that solid phase assays, even in the absence of a positive crossmatch is
associated with poorer long-term outcome [7,25,26]. Even if our exact same
protocol was used it is likely that each laboratory will need to define their own
clinically relevant MFI threshold, because of issues such as batch-to-batch
variation in SABs, difference in anti- body affinity, DSA definition using C1q-assay
and other sources of variation. Ultimately the main problem with using virtual
cross match in highly sensitized patients is that solid phase assays at present still
do not predict complement binding antibodies. This problem could be overcome
by newer assays that may detect complement [10,27], therefore improving the
utility of the virtual crossmatch. We recently demonstrated that C4d-fixation to
detect complement-activating DSA significantly improved predictive accuracy of
CDC crossmatch, with better performance for T-cell than B-cell crossmatch [10].
Avoiding antibody is important, but there may be a greater survival benefit for a
highly sensitized recipient of a living donor kidney who has a negative crossmatch,
but positive DSA. Thus, an alternative consideration to allow highly sensitized
recipients the chance of live donor kidney transplantation is to leave the decision
as to whether and how to proceed to the discretion of each trans- plant center,
when low levels of DSA are amenable to early therapeutic intervention, with the
goal of finding a better immunologic match rather than a completely compatible
pairing. The risk of this approach is that identified matches have a greater risk of
breakdown, because the initial acceptance by the transplant center may later be
withdrawn. However, the likelihood of a chain breakdown would still be lower
than the predicted rate of positive crossmatches if all pairings were allowed at a
higher MFI cut-off.
The aim of this study was to identify a strategy to optimize virtual crossmatch
allocation for KPD using solid phase assay technology. Clearly, the role of DSA in
the context of crossmatch results cannot be dissociated from antibody-mediated

172
rejection and long-term survival [7], and the limitation of the current analysis is
that it does not address these points because it is prediction without
transplantation. However, maximizing the number of crossmatch negative
matches, while minimizing the risk of break- down of chains is an important
measure to reduce the emotional burden that KPD pairs are exposed when a
match is proposed, but later cancelled because of positive crossmatch results.
In conclusion, these results show excellent correlation between matching using
virtual crossmatch and actual crossmatch results. The number of potentially
acceptable CDC crossmatch negative pairings excluded by virtual crossmatching is
approximately 10%, suggesting that the Australian algorithm won’t disallow too
many potential compatible transplants.
Disclosure
The authors of this manuscript have no conflicts of interest to disclose as
described by the Journal.
Acknowledgments
The authors wish to acknowledge the support of the Australian Organ and Tissue
Donation and Transplantation Authority for the establishment of the National
Paired Kidney Donation program and funding of part of the staff (PF, SF). We wish
to thank Elisabeth Lehner for her valuable contribution to patient management
and data collection.

173
References
[1] de Klerk M, Keizer KM, Claas FH, Witvliet M, Haase-Kromwijk BJ, Weimar W. The
Dutch national living donor kidney exchange program. Am J Transplant 2005; 5: 2302.
[2] Montgomery RA, Zachary AA, Ratner LE, Segev DL, Hiller JM, Houp J, et al. Clinical
results from transplanting incompatible live kidney donor/recipient pairs using kidney
paired donation. JAMA 2005; 294: 1655.
[3] Johnson RJ, Allen JE, Fuggle SV, Bradley JA, Rudge C. Early experience of paired living
kidney donation in the United Kingdom. Transplantation 2008; 86: 1672.
[4] Ferrari P, Fidler S, Wright J, Woodroffe C, Slater P, Van Althuis-Jones A, et al. Virtual
crossmatch approach to maximize matching in paired kidney donation. Am J
Transplant 2011; 11: 272.
[5] Ferrari P, Woodroffe C, Christiansen FT. Paired kidney donations to expand the living
donor pool: the Western Australian experience. Med J Aust 2009; 190: 700.
[6] Morris GP, Phelan DL, Jendrisak MD, Mohanakumar T. Virtual crossmatch by
identification of donor-specific anti-human leukocyte antigen antibodies by solid-
phase immunoassay: a 30-month analysis in living donor kidney transplantation. Hum
Immunol 2010; 71: 268.
[7] Lefaucheur C, Loupy A, Hill GS, Andrade J, Nochy D, Antoine C, et al. Preexisting
donor-specific HLA antibodies predict outcome in kidney transplantation. J Am Soc
Nephrol 2010; 21: 1398.
[8] Bingaman AW, Bray RA, Gebel HM, Newell KA. Paired kidney donation: a (virtual)
balancing act. Am J Transplant 2011; 11: 194.
[9] Cecka JM, Kucheryavaya AY, Reinsmoen NL, Leffell MS. Calculated PRA: initial results
show benefits for sensitized patients and a reduction in positive crossmatches. Am J
Transplant 2011; 11: 719.
[10] Wahrmann M, Hlavin G, Fischer G, Marinova L, Schwaiger E, Hörl WH, et al.
Modified solid-phase alloantibody detection for improved crossmatch prediction.
Hum Immunol 2013; 74: 32.
[11] Mackinnon A. A spreadsheet for the calculation of comprehensive statistics for the
assessment of diagnostic tests and interrater agreement. Comput Biol Med 2000; 30:
127.

174
[12] de Klerk M, Witvliet MD, Haase-Kromwijk BJ, Claas FH, Weimar W. Hurdles, barriers,
and successes of a national living donor kidney exchange program. Transplantation
2008; 86: 1749.
[13] Ferrari P, Fidler S, Holdsworth R, Woodroffe C, Tassone G, Watson N, et al. High
transplant rates of highly-sensitised recipients with virtual crossmatching in
kidney paired donation. Transplantation 2012; 94: 744
[14] Keizer KM, de Klerk M, Haase-Kromwijk BJ, Weimar W. The Dutch algorithm for
allocation in living donor kidney exchange. Transplant Proc 2005; 37: 589.
[15] Saidman SL, Roth AE, Sonmez T, Unver MU, Delmonico FL. Increasing the
opportunity of live kidney donation by matching for two- and three-way exchanges.
Transplantation 2006; 81: 773.
[16] Miyata R, Shimazu M, Tanabe M, Kawachi S, Hoshino K, Wakabayashi G, et al.
Clinical characteristics of thrombotic microangiopathy following ABO incompatible
living donor liver transplantation. Liver Transplant 2007; 13: 1455.
[17] Vaidya S, Partlow D, Susskind B, Noor M, Barnes T, Gugliuzza K. Prediction of
crossmatch outcome of highly sensitized patients by single and/or multiple antigen
bead luminex assay. Transplantation 2006; 82: 1524.
[18] Setoguchi K, Ishida H, Shimmura H, Shimizu T, Shirakawa H, Omoto K, et al. Analysis
of renal transplant protocol biopsies in ABO-incompatible kidney transplantation. Am
J Transplant 2008; 8: 86.
[19] Tanabe K. Interinstitutional variation in the measurement of anti-A/B antibodies:
the Japanese ABO-incompatible transplantation committee survey. Transplantation
2007; 84: S13.
[20] Tanabe K. Japanese experience of ABO-incompatible living kidney transplantation.
Transplantation 2007; 84: S4.
[21] Roth AE, Sonmez T, Unver MU. Kidney paired donation with compatible pairs.
Am J Transplant 2008; 8: 463.
[22] Gloor J, Stegall MD. Sensitized renal transplant recipients: current protocols and
future directions. Nature Rev Nephrol 2010; 6: 297.
[23] Ntokou IS, Iniotaki AG, Kontou EN, Darema MN, Apostolaki MD, Kostakis AG, et
al. Long-term follow up for anti-HLA donor specific antibodies postrenal
transplantation: high immunogenicity of HLA class II graft molecules. Transplant
Int 2011; 24: 1084.

175
[24] Montgomery RA, Lonze BE, Jackson AM. Using donor exchange paradigms with
desensitization to enhance transplant rates among highly sensitized patients. Curr
Opin Organ Transplant 2011; 16: 439.
[25] Gebel HM, Moussa O, Eckels DD, Bray RA. Donor-reactive HLA antibodies in renal
allograft recipients: considerations, complications, and conundrums. Hum Immunol
2009; 70: 610.
[26] Gupta A, Sinnott P. Clinical relevance of pretransplant human leukocyte antigen
donor-specific antibodies in renal patients waiting for a transplant: a risk factor.
Hum Immunol 2009; 70: 618.
[27] Chen G, Sequeira F, Tyan DB. Novel C1q assay reveals a clinically relevant subset
of human leukocyte antigen antibodies independent of immunoglobulin G
strength on single antigen beads. Hum Immunol 2011; 72:849.

176
Chapter 8
Discussion and conclusions

177
8 Discussion and conclusions
The aims of this thesis were to evaluate the clinical relevance of preformed antibodies
directed against HLA detected by Luminex bead assay in the absence of a positive CDC
crossmatch in renal allograft transplantation. Furthermore, whether this data could be
utilized prospectively in clinical practice to facilitate transplantation was studied. This
chapter summarises the key findings of the studies presented in this thesis and will
address further research in these areas.
8.1 The significance of preformed anti-HLA antibodies detected by Luminex bead assay
The Western Australian tissue typing laboratory has been performing pre-transplant
antibody detection and analysis by Luminex bead assay since 2004. This assay has several
key advantages such as increased sensitivity and the ability to accurately determine
specificity including, importantly, definition of antibodies against class II HLA antigens.
There is, however, some controversy over whether antibodies detected by the more
sensitive solid phase assays are clinically significant when found with a negative
crossmatch. Our study has shown a high risk (HR 6.6, 95%CI 2.9-14.7, p<0.001) of AMR in
patients with DSA detected by Luminex single antigen bead assay. A number of studies
have investigated the association of Luminex detected DSA with kidney graft outcome and
are summarised in chronological order in Table 1164-177. Consistent with our findings,
several groups have demonstrated a significant correlation between the presence of pre-
transplant DSA by Single Antigen bead assay and AMR164, 167,168, 170, 172-177. However, in
contrast, Phelan et al reported no AMR in their small cohort of 64 patients165 whilst Gupta
et al could not demonstrate a significant association of acute rejection with DSA at 1 and 5
years follow-up100.
We found the risk of AMR was increased substantially (HR 10.1, 95%CI 3.5-28.2, p<0.001)
in patients with both class I and class II antibodies. Otten et al reported similar findings
with a 30% graft survival at 10 years in those with both class I and II DSA compared to 72%
graft survival in patients with no DSA171. However, this group found no association of class
I or class II DSA alone, whilst we were able to demonstrate a significant association with
both (Class I HR 4.4, 95%CI 1.3-15.5, p=0.021; Class II HR 6.1, 95%CI 1.7-21.4, p=0.005).

178
Table 1. Summary of studies investigating the clinical significance of HLA antibodies
detected pre-transplant by Luminex bead assay.
Authors and year of
publication
Number in
study / DSA
positive
Incidence of
AMR
(No DSA vs DSA)
P value Graft survival (No DSA vs DSA)
P value
Vlad et al. 2009164
325 / 27 6.7% vs 45% P<0.0001 90% vs 81% (1yr) P=0.21
Gupta and Sinnott 2009
165
121 / 16 Not reported 92% vs 86% (1yr) 77% vs 62% (5yr)
NS NS
Phelan et al. 2009166
64 / 12 7.6% vs 8.3% NS 88% vs 83% (4yr) NS
Aubert et al. 2009167
113 / 11 0% vs 9% P<0.005 99% vs 100% (1yr) NS
Amico et al. 2009168
334 / 67 35% vs 71% P<0.0001 89% vs 68% #(5yr) P=0.002
Lefaucheur et al.
2010169
237 / 83 Not reported 84% vs 61% (8yr) P<0.001
Riethmüller et al.
2010170
155 / 20 6% vs 35% P=0.048 Not reported
Otten et al. 2012171
837 / 290 Not reported 72% vs 30% (10yr, class I+II DSA) 72% vs 65% (10yr,class I only ) 72% vs 69% (10yr, class II only)
<0.001 NS NS
Thammanichanoud
et al. 2012172
116 / 28 14.7% vs 25% P=0.252 96.6% vs 92.9% (1yr) 92.7% vs 92.9% (5yr)
NS NS
David-Neto et al.
2012173
94 / 16 0% vs 19% P=0.004 82% vs 68.7% (6yr) P=0.21
Pérez-Flores et al.
2013174
190 / 13 30% vs 77% P=0.03 100% vs 60% (1yr) P=0.01
Wu et al. 2013175
221 / 15 3.4% vs 26.7% P=0.0001 99% vs 87% (2yr) P=0.0009
Tsapepas et al. 2014
176
174 / 62 7.1% vs 32.3% P<0.001 Not reported
Malheiro et al.
2015177
462 / 40 0.9% vs 35% P<0.001 94.9% vs 84.8% (5yr)
P=0.006
# In DSA positive group with AMR
NS= Not significant
We reported that the MFI of the DSA was higher in those patients with AMR than those
without AMR. This finding was independently reported by two groups. Lefaucheur et al
reported the prevalence of AMR increased with increasing pre-transplant DSA169. The rate
of AMR in the DSA negative group was 0.9%, compared with 18.7% if the DSA was 466-
3000 MFI, 36.4% if the DSA was 3001-6000 MFI and 51.3% if the DSA was greater than
6000 MFI. Wu et al also reported the rate of AMR increased with increasing MFI127.
Others could not show a significant association of antibody strength with AMR172. These
contrary findings might be related to the difficulties in measuring the strength of HLA
antibodies using MFI in Luminex assays. It is now recognised that there may be an

179
underestimation of HLA antibodies due to weak or false negative reactions. Two potential
causes of weak reactivity have been described. The phenomenon of prozone has been
shown in Luminex assays178, which may mask strong antibodies if serial dilutions are not
performed. One of the major causes of prozone has been identified as complement
interference. The prozone effect has been found to be related to the amount of antibody-
triggered C1q, C4 or C3 split product deposition179-182. This problem can be resolved by
dilution, treatment with DTT, heat treatment or addition of EDTA to test sera183. A second
cause of false negative or weak reactivity in Luminex bead assays was identified in the
serial dilution of sera which showed IgG antibody binding appearing or increasing as the
sera were diluted. This can be due to the presence of IgM antibodies, which block IgG
antibody binding to the antigen coated bead184. This blocking can be eliminated by serial
dilution, heat treatment, treatment with DTT or hypotonic dialysis184, 185.
In addition to the problems of underestimation of antibody levels, overestimation can also
occur. It is recognised that the density of HLA antigen present on Luminex beads can vary
from bead to bead, from batch to batch, and from locus to locus. In particular, HLA-C,
HLA-DQ and HLA-DP antigens are over-represented on Luminex beads when compared to
cell density186, 187. This can lead to detection of antibodies against these antigens by in vitro
Luminex assay alone, which may not be harmful in vivo in the context of clinical
transplantation. Secondly, the process of manufacture of HLA specific beads may result in
the exposure of cryptic epitopes. Morales-Buenrostro et al found reactivity in the Luminex
antibody assay in 63% of non-sensitized males188. The reactivity was found to be against
epitopes on denatured antigen189, 190. Otten et al found that antibodies against intact but
not denatured HLA are associated with kidney graft function and loss, with 5 year serum
creatinine levels of 177µmol/l in patients with antibody against intact antigen versus
144µmol/l in patients with antibody directed against denatured antigen (P=0.02)191.
We also showed graft function, as measured by estimated glomerular filtration rate
(eGFR), progressively declined over time in the DSA group but was stable in patients
without DSA. Wu et al also demonstrated that a decline in eGFR was preceded by the
presence of DSA, either pre-existing or de novo post-transplant192. This suggests that
chronic antibody mediated injury exerts a longer term deleterious effect hastening graft
loss.
Although we could not show a significant association, there was a trend for graft loss to be
associated with the presence of pre-transplant DSA in our study (p=0.075). However,
when we stratified graft loss by antibody class we saw a significant effect of class II DSA
(HR 2.9, 995%CI 1.0-8.0, p=0.047) and class I and II DSA (HR 3.7, 95%CI 1.6-8.9, p=0.003)

180
but not class I DSA. Graft survival in the class I and II DSA group was 54% at 8 years
compared with 83% in the DSA negative group. Graft survival was better in patients with
class I DSA (92% at 8 years); this may be due to the differences in cause of graft loss. In the
DSA positive group, all losses were due to rejection, however in the DSA negative group
graft losses occurred due to rejection, disease recurrence and BK nephropathy. Otten et al
also showed graft survival was only significantly influenced by class I and II antibodies171
and other groups have shown a significant association between graft survival and pre-
transplant DSA168, 169, 174, 175, 177. Studies are not consistent however, as many groups have
not reported a significant association165-167, 172, 173.0
8.2 Peri-operative blood transfusion is associated with AMR and renal allograft loss
Blood transfusion pre-renal-transplant is associated with sensitization against HLA antigens
but is not associated with an adverse allograft outcome; indeed it can be beneficial by
reducing episodes of acute rejection193, 194. One of the reasons suggested for this
phenomenon is that patients who are susceptible to antibody formation become broadly
sensitised, and these antigens are subsequently avoided in transplantation. In our
preliminary study we found an association of DSA detected by Luminex bead assay, in
crossmatch negative patients, with AMR and graft dysfunction. It was noted that AMR was
more prevalent in patients receiving a blood transfusion at, or shortly after, the time of
transplant and this was further explored. We found in our second study that the risk of
AMR was 13.9 times greater in patients with DSA (p=0.001), than those with no DSA, if
they received a transfusion both pre- and post-transplant. We also showed that graft loss
was significantly increased in patients who received pre- and post-transplant transfusions
(HR 7.1, p<0.001), even in the group of patients without DSA. Patients with DSA who
received transfusions only pre- or post-transplant did not experience AMR. We postulate
that there is a broad recall of antibody response following re-exposure to blood as
described by Scornik et al195. These findings are novel and have not been reported
elsewhere, and may have important implications for clinical practice. As blood
transfusions are associated with AMR and graft loss, methods to avoid transfusion at the
time of kidney transplant such as iron infusions, erythropoietin or autologous blood
transfusion could potentially have a positive effect on transplant outcome and may
prevent or reduce rejection episodes and graft loss.

181
8.3 Virtual crossmatching to facilitate transplantation.
Chapters 5, 6 and 7 addressed the use of Luminex antibody data in virtual crossmatching
for paired kidney donation. The Australian kidney exchange (AKX) program was based on
the principles guiding the Dutch algorithm162, but using high resolution HLA typing of
donors and Luminex single antigen bead analysis of recipient antibodies to enable virtual
crossmatching. We aimed to use an antibody threshold which would exclude positive
crossmatches but not at the detriment to highly sensitised patients. We, and others, have
shown the utility of the virtual crossmatch in predicting crossmatch results in the clinical
setting196- 200. In the first 4 years of the Australian paired kidney exchange program 105
patients were transplanted in matches from 215 registered donor / recipient pairs
(49%)201. A further 4 patients on the deceased donor wait-list were transplanted from the
end of a non-directed altruistic donor chain. Matching using conservative antibody cut-offs
did not appear to be detrimental to highly sensitised patients (Figure 1) who had
acceptable transplant rates even in those with a PRA >90%. One year patient and graft
survival were excellent at 97% and 96% respectively.
% of programme registrants, % of registrants transplanted, % of cPRA group transplanted
Figure 1. Transplant activity by calculated panel reactive antibody (cPRA) cohort: cPRA
97% is the true threshold for diminished access; the 95-96% groups are transplanted at a
proportion equivalent to their proportion in the registry, comparable with any other
cPRA cohort.

182
From: L Cantwell, C Woodroffe, R Holdsworth, P Ferrari. Nephrology 2015; 20(3): 124-
131201
8.4 Further research
8.4.1 Post-transplant antibody testing
Our two studies investigating the significance of pre-transplant HLA antibodies in chapters
3 and 4 showed the association of donor specific antibodies with rejection and poor
transplant outcome. We hypothesise that those patients who did not have DSA pre-
transplant but did undergo AMR developed de novo DSA post-transplant. Other groups
have shown the association of DSA found at any time post-transplant with poor allograft
outcome as reviewed in section 1.7107-116. Our group has collected sera from all kidney
transplant patients at 0, 1, 3, 6 months and yearly since 2003. Antibody analysis of these
sera to determine the prevalence of de novo DSA in our cohort is currently being
performed. Preliminary results, not shown, confirm the association of de novo DSA with
graft rejection consistent with current literature.
8.4.2 Rejection in the absence of HLA antibodies
Despite the very sensitive techniques available for detecting HLA antibodies,
histopathological features of antibody mediated rejection can be found in the absence of
demonstrable DSA in the peripheral blood. One explanation for this is that circulating DSA
is sequestered onto the donor kidney endothelium causing damage, but at levels in the
circulation undetectable by current assays. This hypothesis is supported by studies
showing DSA detection following nephrectomy of rejected kidneys117-119 and elution of
antibody from kidney endothelium120, 121.
In addition to HLA antibodies and the risk of AMR, non-HLA antibodies such as antibodies
directed against MHC Class I related gene-A (MICA), vimentin or angiotensin type I
receptor (AT1R) may also play an important role in graft rejection and give a similar
histological appearance. The role of non-HLA antibodies in allograft rejection are
comprehensively reviewed in publications by Dragun et al202, 203 and Sumitran-
Holgersson204. Preliminary investigation of MICA antibodies by our group has not found an
association of presence of MICA antibodies with graft outcome. We believe this is due to
the low prevalence of MICA antibodies in our cohort, and the finding that all patients with
MICA antibody also had HLA DSA.

183
8.4.3 HLA DSA in the absence of rejection
Although detection of DSA prior to transplant has been associated with poor graft
outcome, not all patients with DSA undergo rejection or lose their grafts. A potential
explanation for this may be accommodation of the graft in some patients. It has been
shown in highly sensitised patients who have undergone desensitisation to temporarily
remove DSA prior to transplant, that they do not always experience accelerated rejection
despite having return or persistence of antibody and can have excellent long term
outcomes205, 206. More recently, in a study of 1025 kidney transplant recipients who
received an HLA incompatible transplant from a living donor following desensitisation,
graft survival at 8 years was better than in controls who either received a compatible
deceased donor transplant or remained on the wait list (76% versus 62.9% versus
43.9%)207. The frequency and mechanisms by which accommodation may occur in some
patients with donor specific HLA antibodies is unknown and warrants further research and
elucidation.
An additional parameter to consider that may impact upon the detection of antibody and
the initiation of immune injury is the antibody affinity and avidity. Whilst Luminex
antibody detection provides a sensitive means of detecting HLA antibodies, it provides no
data regarding the strength of interaction between the antibody and corresponding
epitope. Antibody binding may be influenced by the epitope orientation and accessibility
and the physiochemical properties of amino acids in the binding site. Kosmoliaptsis et al
have shown in experiments analysing surface electrostatic potentials that some changes in
amino acids do not result in a change in electrostatic motif, whereas other changes at
critical positions can affect antibody binding208,209. This is a potential area for further
research and may help us to understand the pathogenicity of HLA antibodies.
8.4.4 Characterisation of HLA epitopes in kidney transplantation
HLA matching between donor and recipient is a major component in kidney allocation as
the greater number of HLA mismatches is associated with increasing risk of allograft
rejection23, 24. The crossreactivity between HLA antigens was first recognised by serological
analysis of antisera210. The definition of HLA epitopes followed the elucidation of the
three-dimensional structure of the HLA molecule and the availability of amino acid
sequence data. Duquesnoy developed a computer-based algorithm, HLAMatchmaker,
based upon linear triplets of amino acids on the HLA molecule which are critical for

184
antibody recognition211. Subsequently the algorithm was updated to include non-linear
amino acid triplets, referred to as eplets212. Further refinement followed the recognition
that in some cases self-epitopes are required for antibody binding213, 214. El-Awar et al
showed in in vitro experiments evidence of epitopes by absorption / elution studies using
Luminex single antigen bead assays215. Furthermore, Duquesnoy and Marrari were able to
correlate class I and II epitopes determine by HLAMatchmaker with those identified by El-
Awar et al 216, 217.
Several studies have associated an increasing number of epitope mismatches with a
greater chance of producing HLA antibodies218-220. In addition it has been demonstrated
that patients matched at the epitope level, in broad antigen level mismatches, have similar
outcomes to broad antigen matched transplants156. HLAMatchmaker can be used
successfully as a tool to facilitate transplantation, particularly in highly sensitised patients.
The Eurotransplant Acceptable Mismatch program reports considerably shorter waiting
times for highly sensitised patients, whilst achieving allograft outcomes similar to that of
unsensitised patients157, 158. Validation of these findings in the Australian kidney transplant
setting is essential for the ongoing improvement of the allocation algorithm.
8.4.5 HLA specific B cells
Donor specific antibodies are associated with acute and chronic rejection, however DSA
are not always found in patients undergoing rejection even when using the sensitive
Luminex antibody assays. There are a number of suggestions why this may occur i) very
low titre antibodies; ii) antibodies are sequestered to the transplanted organ; iii) patient
unresponsiveness; or iv) timing of antibody testing. In all these situations it is unclear
whether the patient immune system is primed for a rapid response on re-exposure to
antigen.
It is possible to detect HLA-specific B cells which produce alloantibody in vitro. The first
assays utilised HLA tetramers to detect HLA antibody producing B cells221. The surface
immunoglobulin antigen receptor of B cells binds to HLA molecules on the tetramer with a
comparable specificity to that of secreted antibody. The tetramer staining can then be
quantified by flow cytometry. The next assays involved in vitro culture of B cells and testing
of supernatants by Luminex single antigen bead assay for HLA antibody. Han et al found
DSA in all B cell supernatants from patients who had rejected their organs (13/13) and no
DSA in unsensitised patients222. In four patients DSA was only found in the B cell
supernatant and not in peripheral blood, two patients had rejected kidneys in situ.

185
Heidt et al developed an ELISPOT assay, allowing a straightforward sensitive and specific
laboratory test to quantify HLA-specific B cells223. The group showed that patients with low
numbers of HLA-specific B cells could be re-transplanted, with good outcomes at 18
months follow-up, and hypothesised that there may be a level which can be interpreted as
below clinical significance. Lucia et al used a similar in-house ELISPOT to detect HLA-
specific B cells and were able to correlate detection of antibody with a high risk of humoral
rejection224. This group also found HLA specific B cells in the absence of HLA specific
antibodies in peripheral blood.
These experiments suggest that an increase in HLA-specific B cells post-transplant may be
a precursor to antibody formation, and therefore may be a target for adjusting
immunosuppression. In addition detection of HLA-specific B cells may reveal sensitisation
when HLA antibodies are not found in peripheral blood, and pre-transplant testing may
assist in evaluating risk.
8.4.6 Complement fixing HLA specific antibodies
The presence of DSA detected pre- or post-transplant is associated with AMR and graft
loss. However, not all patients with DSA develop rejection or lose their grafts. The ability
to activate complement has come under scrutiny in a bid to understand the pathogenicity
of antibodies due to the finding of depositions of the complement component C4d on the
kidney in rejection. The Luminex antibody assay can be modified, via the use of different
secondary detection antibodies to immunoglobulin isotypes, subclasses or complement
components, to assess the significance of complement-fixing versus non-fixing HLA
antibodies225. Studies investigating clinical outcomes in patients with DSA stratified by
their complement-fixing ability are summarised in Table 2.

186
Table 2. Summary of studies investigating the clinical significance of complement-fixing
DSA.
Authors and
year of
publication
Number in
study (DSA
positive) /
Number of
C’-fixing
DSA
Incidence of
AMR
(DSA vs C’-fixing
DSA)
P value Graft survival (DSA vs C’-fixing DSA)
P value
Wahrmann et
al. 2009226
46 / 21 4% vs 24% P<0.001 90% vs 76% P=0.01
Hönger et al.
2010227
64 / 11 53% vs 55% NS Not reported
Yabu et al.
2011228
31 / 12 Not reported 37% vs 21% P=0.026
Hönger et al.
201195
74 / 21 25% vs 57% P=0.23 100% vs 78% P=0.74
Sutherland et
al. 2012229
35 / 15 16.7% vs 60% P=0.04 85% vs 53.3% P=0.04
Lawrence et
al. 2013230
42 / 13 8% vs 24% P <0.01 91.7% vs 80% P=0.001#
Crespo et al.
2013231
28 / 15 30.8% vs 26.7% P=0.67 76.9% vs 80% P=0.8
Loupy et al.
2013232
239 / 77 16% vs 48% P<0.001 93% vs 54% P<0.001
C’ = complement; abs = antibodies, DSA = Donor specific antibodies; NS = Not significant
#AMR free graft survival
Several groups have demonstrated a significant association of pre-transplant complement-
fixing DSA with AMR when compared to non-complement-fixing DSA226, 230, 232. Others
could not find a significant association95, 227, 231. All groups reported an increased risk of
AMR with DSA when compared to patients with no DSA. Yabu et al228 and Sutherland et
al229 investigated de novo DSA in the post-transplant period and were able to demonstrate
a strong association of complement-fixing DSA with AMR. These results suggest that

187
complement-fixing ability of DSA might only be important in the post-transplant period.
Most groups reported a correlation between complement-fixing DSA and poor graft
survival226, 228-230, 232, and all groups reported lower graft survival in patients with DSA
compared to no DSA.
Zeevi et al studied complement-fixing antibodies in heart transplants and showed high
titre antibodies correlated with the ability to fix complement and were associated with
AMR (P=0.005)233. In our own publication, we were able to demonstrate a correlation
between strong DSA assessed by MFI and renal graft outcome (Chapter 3). It may be
possible to use MFI as a surrogate test for complement-fixing antibodies, and other groups
have suggested that pre-transplant the strength of DSA rather than complement-fixing
ability is important 231, 234, 235. Larger cohort or collaborative studies are required to
determine the clinical utility of testing for complement-fixing antibodies as a further tool
to stratify transplant risk.
In addition to the complement-activating ability of different subclasses of IgG antibodies, it
has been recognised the glycosylation of antibody may be important in modulating
complement fixation. The process of glycosylation in the context of transplantation is
reviewed by Thomas et al236 and appears to influence the affinity of the Fcϒ receptor,
shifting IgG activity from a pro-inflammatory to an anti-inflammatory pathway237.
8.5 Conclusions
The studies in this thesis have shown that pre-transplant donor specific HLA antibodies
detected by Luminex single antigen bead assay with a concurrent negative CDC crossmatch
are associated with increased risk of rejection episodes, AMR, chronic graft dysfunction
and graft loss. We have shown that the risks are increased with increasing strength of
antibody as measured by MFI. In addition we have described the novel finding that that
the risk of AMR was significantly increased in patients with DSA, than those with no DSA, if
they received a transfusion both pre- and post-transplant. These findings have important
implications for clinical practice.
We have also shown that use of antibodies detected by the sensitive Luminex method for
virtual crossmatching and transplant allocation is successful in the Australian paired kidney
exchange program with minimal adverse affects on the transplantation of highly sensitised
patients.
Further investigation into the reasons why some patients with DSA do not undergo graft
rejection is warranted.

188
References

189
References
1. T Shiina, K Hosomichi, H Inoko, JK Kulski. The HLA genomic loci map: Expression,
interaction, diversity and disease. J Hum Genet 2009; 54: 215-39
2. J Klein, A Sato. The HLA system. N Engl J Med 2000; 343: 702-709
3. JD Wall, JK Pritchard. Haplotype blocks and linkage disequilibrium in the human
genome. Nat Rev Genet 2003; 4: 587-597
4. AB Begovich, GR McClure, VC Suraj, RC Helmuth, N Fildes, TL Bugawan, HA Erlich, W
Klitz. Polymorphism, recombination, and linkage disequilibrium within the HLA class II
region. J Immunol 1992; 148: 249-258
5. X Gao, A Veale, SW Serjeantson. HLA class II diversity in Australian aborigines:
Unusual DRB1 alleles. Immunogenetics 1992; 36: 333-337
6. AS Daar, SV Fuggle, JW Fabre, A Ting, PJ Morris. The detailed distribution of HLA-A, B,
C antigens in normal human organs. Transplantation 1984; 38: 287-293.
7. J Klein, A Sato. The HLA system. First of two parts. NEJM 2000; 343: 702-709
8. P Cresswell. Regulation of HLA class I and class II antigen expression. Br Med Bull
1987; 43: 66-80
9. Y Watanabe, CO Jacob. Regulation of MHC class II antigen expression. Opposing
effects of tumor necrosis factor-alpha on IFN-gamma-induced HLA-DR and Ia
expression depends on the maturation and differentiation stage of the cell. J
Immunol 1991; 146: 899-905
10. FJ Salgado, J Lojo, CM Fernández-Alonso, JE Viñuela, OJ Cordero, M Nogueira.
Interleukin-dependent modulation of HLA-DR expression on CD4 and CD8 activated T
cells. Immunology and Cell Biology 2002; 80: 138-147
11. KR Prilliman, D Crawford, HD Hickman, KW Jackson, J Wang, WH Hildebrand. Alpha-2
domain polymorphism and HLA class I peptide loading. Tissue Antigens 1999; 54:
450-460
12. http://www.ebi.ac.uk/imgt/hla
13. J Robinson, JA Halliwell, JD Hayhurst, P Flicek, P Parham, SGE Marsh. The IPD and
IMGT / HLA database: Allele variant databases. Nucleic Acids Res 2015; 43: D423-431
14. JS Blum, PA Wearsch, P Cresswell. Pathways of antigen processing. Annu Rev
Immunol 2013; 31: 443-473

190
15. P Cresswell, AL Ackerman, A Giodini, DR Peaper, PA Wearsch. Mechanisms of MHC
class-I-restricted antigen processing and cross-presentation. Immunol Rev 2005; 207:
145-157
16. NJ Rogers, RI Lechler. Allorecognition. Am J Transplant 2001; 1: 97-102
17. G Benichou, AW Thomson. Direct versus indirect allorecognition pathways: On the
right track. Am J Transplant 2009; 9: 655-656
18. AN Warrens, G Lombardi, RI Lechler. Presentation and recognition of major and
minor histocompatibility antigens. Transpl Immunol 1994; 2: 103-107
19. RI Lechler, JR Batchelor. Restoration of immunogenicity to passenger cell-depleted
kidney allografts by the addition of donor strain dendritic cells. J Exp Med 1982;
155(1): 31-41
20. DS Game, RI Lechler. Pathways of allorecognition: implications for transplantation
tolerance. Transpl Immunol 2002; 10: 101-108
21. DA Shoskes, KJ Wood. Indirect presentation of MHC antigens in transplantation.
Immunol Today 1994; 15: 32-38
22. JA Bradley, EM Bolton, RA Pederson. Stem cell medicine encounters the immune
system. Nat Rev Immunol 2002; 2: 859-871
23. L Martins, I Fonseca, S Sousa, C Matos, J Santos, L Dias, AC Henriques, AM Sarmento,
A Cabrita. The influence of HLA mismatches and immunosuppression on kidney graft
survival: An analysis of more than 1300 patients. Trans Proc 2007; 39: 2489-2493
24. G Opelz, B Döhler. Effect of human leukocyte antigen compatibility on kidney graft
survival: Comparative analysis of two decades. Transplantation 2007; 82: 137-143
25. P Gailiunas Jr, M Suthanthiran, GJ Busch, CB Carpenter, MR Garovoy. Role of humoral
presensitization in human renal transplant rejection. Kidney Int 1980; 17(5): 638-646
26. RB Colvin, RN Smith. Antibody-mediated organ-allograft rejection. Nat Rev Immunol
2005; 5: 807-817
27. R Patel, P Terasaki. Significance of the positive crossmatch test in kidney
transplantation. N Eng J Med 1969; 280: 735-739
28. AS Rosenberg, T Mizuochi, SO Sharrow, A Singer. Phenotype, specificity, and function
of T cell subsets and T cell interactions involved in skin allograft rejection. J Exp Med
1987; 165: 1296-1315
29. F Boisgérault, Y Liu, N Anosova, E Ehrlich, MR Dana, G Benichou. Role of CD4+ and
CD8+ T cells in allorecognition: lessons from corneal transplantation. J Immunol 2001;
167(4): 1891-1899
30. E Ingulli. Mechanism of cellular rejection. Pediatr Nephrol 2010; 25: 61-74

191
31. BA Wasowska. Mechanisms involved in antibody- and complement-mediated
allograft rejection. Immunol Res 2010; 47: 25-44
32. NM Valenzuela, EF Reed. Antibodies in transplantation: The effects of HLA and non-
HLA antibody binding and mechanisms of injury. Methods Mol Biol 2013: 1034
33. S Mauiyyedi, RB Colvin. Humoral rejection in kidney transplantation: New concepts in
diagnosis and treatment. Curr Opin Nephrol Hypertens 2002; 11: 609-618
34. S Moll, M Pascual. Humoral rejection of organ allografts. Am J Transplant 2005; 5:
2611-2618
35. RB Colvin, RN Smith. Antibody mediated organ-allograft rejection. Nat Rev Immunol
2005; 5: 807-817
36. RB Colvin. Antibody-mediated renal allograft rejection: Diagnosis and pathogenesis. J
Am Soc Nephrol 2007; 18: 1045-1056
37. H Regele, GA Böhmig, A Habicht, D Gollowitzer, M Schillinger, S Rockenschaub, B
Watschinger, D Kerjaschki, M Exner. Capillary deposition of complement split product
C4d in renal allografts is associated with basement membrane injury in peritubullar
and glomerular capillaries: A contribution of humoral immunity to chronic allograft
rejection. J Am Soc Nephrol 2002; 13: 2371-2380
38. TV Obukhanych, MC Nussenzweig. T-independent type II immune responses generate
memory B cells. J Exp Med 2006; 203(2): 305-310
39. JJ Mond, A Lees, CM Snapper. T cell independent antigens type 2. Annu Rev Immunol
1995; 13: 655-692
40. JJ Mond, Q Vos, A Lees, CM Snapper. T cell independent antigens. Curr Opin Immunol
1995; 7: 349-354
41. DC Parker. T cell-dependent B cell activation. Annu Rev Immunol 1993; 11: 331-360
42. Y Yang, JM Wilson. CD40 ligand-dependent T cell activation: Requirement of B7-CD28
signalling through CD40. Science 1996; 273: 1862-1864
43. M Croft, SL Swain. B cell responses to fresh and effector T helper cells. Role of
cognate T-B interactions and the cytokines IL-2, IL-4, and IL-6. J Immunol 1991; 146:
4055-4064
44. WE Paul, RA Seder. Lymphocyte responses and cytokines. Cell 1994; 76: 241-251
45. JM Purkerson, PC Isakson. Interleukin 5 (IL-5) provides a signal that is required in
addition to IL-4 for isotype switching to immunoglobulin (Ig) G1 and IgE. J Exp Med
1992; 175: 973-982
46. S Julien, PA Videira, P Delannoy. Sialyl-Tn in cancer: (How) did we miss the
target? Biomolecules 2012; 2: 435–466

192
47. P Morris, P Kincaid-Smith, V Marshall. Leukocyte antigens in cadaver transplantation.
Transplant Proc 1969; 1: 376-378
48. MS Leffell, AG Steinberg, WB Bias, CH Machan, AA Zachary. The distribution of HLA
antigens and phenotypes among donors and patients in the UNOS registry.
Transplantation 1994; 58(10): 1119-1130
49. AA Zachary, JT Sholander, JA Houp, MS Leffell. Using real data for a virtual
crossmatch. Hum Immunol 2009; 70: 574-579
50. JM Cecka. Calculated PRA (cPRA): the new measure of sensitization for transplant
candidates. Am J Transplant 2010; 10: 26-29
51. AR Tambur, J Leventhal, DB Kaufmann, J Friedwald, J Miller, MM Abecassis. Tailoring
antibody testing and how to use it in the calculated panel reactive antibody era: The
Northwestern University experience. Transplantation 2008; 86: 1052-1059
52. JR Chapman, CJ Taylor, A Ting, PJ Morris. Immunoglobulin class and specificity of
antibodies causing positive T cell crossmatches. Relationship to renal transplant
outcome. Transplantation 1986; 42: 608-612
53. CJ Taylor, JR Chapman, A Ting, PJ Morris. Characterization of lymphocytotoxic
antibodies causing a positive crossmatch in renal transplantation. Relationship to
primary and regraft outcome. Transplantation 1989; 48: 953-958
54. DE Cross, R Greiner, FC Whittier. Importance of the autocontrol crossmatch in human
renal transplantation. Transplantation 1976; 21: 307-311
55. Y Iwaki, M Lau, PI Terasaki. Successful transplants across T-warm positive
crossmatches due to IgM antibodies. Clin Transplant 1998; 2: 81-94
56. C Baron, M Pastural, P Lang, R Bentabet, N el Kassar, T Seror, D Dahmane, D Desvaux,
D Chopin, G Fruchard, P Remy, P Grimbert, E Lepage, P Bieling. Long-term kidney
graft survival across a positive historical but negative current sensitized cross-match.
Transplantation 2002; 73: 232-236
57. MA Pellegrino, M Belverdere, AG Pellegrino, S Ferrone. B peripheral lymphocytes
express more HLA antigens than T peripheral lymphocytes. Transplantation 1978;
25(2): 93-95
58. T Mohanakumar, MA Gledlin, CL Rhodes. Relationship of B cell alloantibodies to renal
allograft survival. Transplantation 1979; 27(4): 273-8
59. G Ayoub, MS Park, PI Terasaki, Y Iwaki, G Opelz. Transplantation 1980; 29(3): 227-229
60. RB Ettinger, PI Terasaki, G Opelz, M Malekzadeh, C Uittenbogaart, C Pennisi, R Fine.
Successful renal allografts across a positive crossmatch for donor B-lymphocyte
alloantigens. Lancet 1976; 1: 56-58

193
61. M Jeannet, G Benzonana, I Arni. Donor-specific B and T lymphocyte antibodies and
kidney graft survival. Transplantation 1981; 31(3): 160-163
62. A Ting, PJ Morris. Renal transplantation and B-cell crossmatches with autoantibodies
and alloantibodies. Lancet 1977; 2: 1095-1097
63. SS Karuppan, A Lindholm, W Möller. Characterisation and significance of donor-
reactive B cell antibodies in current sera of kidney transplant patients.
Transplantation 1990; 49(3): 510-515
64. RJ Mahoney, S Taranto, E Edwards. B-cell crossmatching and kidney allograft
outcome in 9031 United States transplant recipients. Human Immunology 2002;
63(4): 324-335
65. S Le Bas-Bernardet, M Hourmant, N Valentin, C Paitier, M Giral-Classe, S Curry, G
Follea, JP Soulillou, JD Bignon. Identification of the antibodies involved in B-cell
crossmatch positivity in renal transplantation. Transplantation 2003; 75(4): 477-482
66. A Goh, E Oei, A Vathsala. Successful transplantation across positive B-cell cross-match
in deceased donor renal transplants. Transplant Proc 2012; 44(1): 193-199
67. HS Hwang, HE Yoon, BS Choi, EJ Oh, JI Kim, IS Moon, YS Kim, CW Yang. B–cell
complement dependent cytotoxic crossmatch positivity is an independent risk factor
for long term renal allograft survival. J Korean Med Sci 2011; 26(4): 528-533
68. HS Eng, G Bennett, P Bardy, P Coghlan, GR Russ, PT Coates. Clinical significance of
anti-HLA antibodies detected by Luminex: Enhancing the interpretation of CDC-BXM
and important post-transplantation monitoring tools. Hum Immunol 2009; 70(8):
595-599
69. DE Cross, FC Whittier, P Weaver, J Foxworth. A comparison of the antiglobulin versus
extended incubation time crossmatch: Results in 223 renal transplants. Transplant
Proc 1977; 9: 1803-1806
70. TC Fuller, AB Cosimi, PS Russell. Use of an antiglobulin-ATG reagent for detection of
low levels of alloantibody – improvement of allograft survival in presensitized
recipients. Transplant Proc 1978; 10: 463-466
71. AH Johnson, RD Rossen, WT Butler. Detection of alloantibodies using a sensitive
antiglobulin microcytotoxicity test: Identification of low levels of preformed
antibodies in accelerated allograft rejection. Tissues Antigens 1972; 2: 215-226
72. Y Iwaki, M Lau, DJ Cook, S Takemoto, PI Terasaki. Crossmatching with B and T cells
and flow cytometry. Clin Transpl 1986; 277-284
73. M Karpinski, D Rush, J Jeffery, M Exner, H Regele, S Dancea, D Pochino, P Birk, P
Nickerson. Flow cytometric crossmatching in primary renal transplant recipients with

194
a negative anti-human globulin enhanced cytotoxicity crossmatch. J Am Soc Nephrol
2001; 12: 2807-2814
74. AA Zachary, L Klingman, N Thorne, AR Smerglia, GA Teresi. Variations of the
lymphocytotoxicity test: An evaluation of sensitivity and specificity. Transplantation
1995; 60: 498-503
75. MH Christiaans, R Overhof, A ten Haaft, F Niemann, JP van Hoof, EM van den Berg-
Loonen. No advantage of flow cytometry crossmatch over complement-dependent
cytotoxicity in immunologically well-documented renal allograft recipients.
Transplantation 1996; 62: 1341-1347
76. RH Kerman, B Süsskind, I Buyse, P Pryzbylowski, J Ruth, S Warnell, SA Gruber, S Katz,
CT van Buren, BD Kahan. Flow cytometry-detected IgG is not a contraindication to
renal transplantation: IgM may be beneficial to outcome. Transplantation 1999; 68:
1855-1858
77. MC Bittencourt, JM Rebibou, Y Saint-Hillier, J Chaboud, I Dupont, JM Chalopin, P
Herve, P Tiberghien. Impaired renal graft survival after a positive B-cell flow-
cytometry crossmatch. Nephrol Dial Transplant 1998; 13: 2059-2064
78. HM Gebel, RA Bray. Sensitization and sensitivity: Defining the sensitized patient.
Transplantation 2000; 69: 1370-1378
79. JC Scornik. Detection of alloantibodies by flow cytometry: Relevance to clinical
transplantation. Cytometry 1995; 22: 259-263
80. WW Alterman, B Seliger, S Sel, D Wendt, G Schlaf. Comparison of the established
standard complement-dependent cytotoxic and flow cytometric crossmatch assays
with a novel ELISA-based HLA crossmatch procedure. Histol histopathol 2006; 21:
1115-1124
81. AW Harmer, M Sutton, A Bayne, RW Vaughan, KI Welsh. A highly sensitive rapid
screening method for the detection of antibodies directed against HLA class I and
class II antigens. Transpl Int 1993; 6: 277-280
82. KJ Kao, JC Scornik, SJ Small. Enzyme-linked immunoassay for anti-HLA antibodies –
Alternative to panel studies by lymphocytotoxicity. Transplantation 1993; 55: 192-
196
83. F Monteiro, C Mineiro, H Rodrigues, J Kalil. Pretransplant and posttransplant-
monitoring of anti-HLA class I IgG1 antibodies by ELISA identifies patients at high risk
of graft loss. Transpl Proc 1997; 29: 1433-1434
84. C Susal, G Opelz. Kidney graft failure and presensitization against HLA class I and class
II antigens. Transplantation 2002; 73: 1269-1273

195
85. A Slavcev, J Lacha, E Honsova, H Sajdlova, A Lodererova, S Vitko, S Valhova, I Striz, E
Ivaskova. Clinical relevance of antibodies to HLA antigens detectable by the standard
complement-dependent cytotoxicity test. Transpl Int 2003; 16: 872-878
86. C Susal, G Opelz. Good kidney graft outcome in recipients with presensitization
against HLA class II but not HLA class I. Hum Immunol 2004; 65: 810-816
87. AM Patel, C Pancoska, S Mulgaonkar, FL Weng. Renal transplantation in patients with
pre-transplant donor-specific antibodies and negative flow cytometry crossmatches.
Am J Transplant 2007; 7: 2371-2377
88. C Lefaucheur, C Suberbielle-Boissel, GS Hill, D Nochy, J Andrade, C Antoine, C
Gautreau, D Charron, D Glotz. Clinical relevance of preformed HLA donor-specific
antibodies in kidney transplantation. Am J Transplant 2008; 8: 324-331
89. C Susal, B Döhler, G Opelz. Presensitized kidney graft recipients with HLA class I and II
antibodies are at increased risk for graft failure: A collaborative transplant study
report. Hum Immunol 2009; 70: 569-573
90. H-H Wu, Y-C Tien, C-I Huang, Y-J Chiang, S-H Chu, P-C Lai. HLA class I antibodies in
patients awaiting kidney transplantation and the association with graft survival.
Transpl Proc 2008; 40: 2191-2194
91. R Pei, J-H Lee, T Chen, S Rojo, PI Terasaki. Flow cytometric detection of HLA
antibodies using a spectrum of microbeads. Hum Immunol 1999; 60: 1293-1302
92. W Herczyk. Luminex. ASHI Quarterly 2013: 104; PC Lee, M Ozawa, CJ Hung, YJ Lin, SS
Chang, TC Chou. Reappraisal of HLA antibody analysis and crossmatching in kidney
transplantation. Clin Transpl 2007: 219-226
93. N El-Awar, J Lee, PI Terasaki. HLA antibody identification with single antigen beads
compared to conventional methods. Hum Immunol 2005; 66: 989-997
94. S Jung, EJ Oh, CW Yang, WS Ahn, Y Kim, YJ Park, K Han. Comparative evaluation of
ELISA and Luminex panel reactive assay for HLA alloantibody screening. Korean J Lab
Med 2009; 29(5): 473-480
95. G Hönger, H Hopfer, ML Arnold, BM Spriewald, S Schaub, P Amico. Pretransplant IgG
subclasses of donor-specific human leukocyte antigen antibodies and development of
antibody-mediated rejection. Transplantation 2011; 92: 41-47
96. ML Arnold, FM Heinemann, P Horn, M Ziemann, N Lachmann, A Mulbacher, A Dick, A
Ender, D Thammanichanoud, GF Fischer, S Schaub, M Hallensleben, J Mytilineos, WE
Hitzler, C Seidl, II Doxiadis, BM Spriewald. 16(th) IHIW: Anti-HLA alloantibodies of the
IgA isotype in re-transplant candidates. Int J Immunogenet 2013; 40: 17-20

196
97. JD Smith, IM Hamour, NR Banner, ML Rose. C4d fixing, Luminex binding antibodies –
A new tool for prediction of graft failure after heart transplantation. Am J Transplant
2007; 7: 2809-2815
98. N Lachmann, K Todorova, H Schulze, C Schonemann. Systematic comparison of four
cell- and Luminex-based methods for assessment of complement-activating HLA
antibodies. Transplantation 2013; 95: 694-700
99. EM Gibney, LR Cagle, B Freed, SE Warnell, L Chan, AC Wiseman. Detection of donor-
specific antibodies using HLA-coated microspheres: Another tool for kidney
transplant risk stratification. Nephrol Dial Transplant 2006; 21: 2625-2629
100. A Gupta, V Iveson, M Varagunum, S Bodger, P Sinnott, RC Thuraisingham.
Pretransplant donor-specific antibodies in cytotoxic negative crossmatch kidney
transplants: Are they relevant? Transplantation 2008; 85: 1200-1204
101. N Issa, FG Cosio, JM Gloor, S Sethi, PG Dean, SB Moore, S DeGoey, MD Stegall.
Transplant glomerulopathy: Risk and prognosis related to anti-human leukocyte
antigen class II antibody levels. Transplantation 2008; 86: 681-685
102. EM van den Berg-Loonen, EVA Billen, CEM Voorter, LWE van Heurn, FHJ Claas,
JP van Hooff, MHL Christiaans. Clinical relevance of pretransplant donor-directed
antibodies detected by Single Antigen beads in highly sensitized renal transplant
patients. Transplantation 2008; 85: 1086-1090
103. N Lachmann, PI Terasaki, C Schonemann. Donor-specific HLA antibodies in
chronic renal allograft rejection: A prospective trial with four-year follow-up. Clin
Transpl 2006; 171-199
104. C Wiebe, IW Gibson, TD Blydt-Hansen, M Karpinski, J Ho, LJ Storsley, A
Goldberg, PE Birk, DN Rush, PW Nickerson. Evolution and clinical pathologic
correlations of de novo donor-specific HLA antibody post kidney transplant. Am J
Transplant 2012; 12: 1157-1167
105. MJ Everly, JJ Everly, LJ Arend, P Brailey, B Susskind, A Govil, A Rike, P Roy-
Chaudhury, G Mogilishetty, RR Alloway, A Tevar, ES Woodle. Reducing de novo
donor-specific antibody levels during acute rejection diminishes renal allograft loss.
Am J Transplant 2009; 9: 1063-1071
106. M Houmant, A Cesbron-Gautier, PI Terasaki, K Mizutani, A Moreau, A
Meurette, J Dantal, M Giral, G Blancho, D Cantarovich, G Karam, G Follea, JP Soulillou,
JD Bignon. Frequency and clinical implications of development of donor-specific and
non-donor specific HLA antibodies after kidney transplantation. J Am Soc Nephrol
2005; 16: 2804-2812

197
107. A Mihaylova, D Baltadjieva, P Boneva, M Ivanova, K Penkova, D Marinova, S
Mihailova, E Paskalev, P Simeonov, E Naumova. Clinical relevance of anti-HLA
antibodies detected by flow-cytometry bead-based assays – Single-center
experience. Hum Immunol 2006; 67: 787-794
108. PI Terasaki, M Ozawa, R Castro. Four-year follow-up of a prospective trial of
HLA and MICA antibodies on kidney graft survival. Am J Transplant 2007; 7: 408-415
109. Q Mao, PI Terasaki, J Cai, N El-Awar, L Rebellato. Analysis of HLA class I specific
antibodies in patients with failed allografts. Transplantation 2007; 83: 54-61
110. JC Scornik, G Guerra, JD Schold, TR Srinivas, D Dragun, H-U Meier-Krieshe.
Value of posttransplant antibody tests in the evaluation of patients with renal graft
dysfunction. Am J Transplant 2007; 7: 1808-1814
111. P-C Lee , L Zhu, PI Terasaki, MJ Everly. HLA-specific antibodies developed in the
first year posttransplant are predictive of chronic rejection and renal graft loss.
Transplantation 2009; 88: 568-574
112. A Haririan, B Kiangkitiwan, D Kukuruga, M Cooper, H Hurley, C Drachenberg, D
Klassen. The impact of C4d pattern and donor-specific antibody on graft survival in
recipients requiring indication renal allograft biopsy. Am J Transplant 2009; 9: 2758-
2767
113. RL Kedainis, MJ Koch, DC Brennan, H Liapis. Focal C4d+ in renal allografts is
associated with the presence of donor-specific antibodies and decreased allograft
survival. Am J Transplant 2009; 9: 812-819
114. P Stastny, S Ring, C Lu, J Arenas, M Han, B Lavingia. Role of immunoglobulin
(Ig)-G and IgM antibodies against donor human leukocyte antigens in organ
transplant recipients. Hum Immunol 2009; 70: 600-604
115. P Cinti, R Pretagostini, Q Lai, ML Tamburro, M Rossi, L Poli, P Berloco.
Alloantibodies and outcomes of deceased donor kidney allografts. Hum Immunol
2009; 70: 651-654
116. LG Hidalgo, PM Campbell, B Sis, G Einecke, M Mengel, J Chang, J Sellares, J
Reeve, PF Halloran. De novo donor-specific antibody at the time of kidney transplant
biopsy associates with microvascular pathology and late graft failure. Am J Transplant
2009; 9: 2532-2541
117. EV Billen, MH Christiaans, J Lee, EM van den Berg-Loonen. Donor-directed HLA
antibodies before and after transplantectomy detected by the Luminex single antigen
assay. Transplantation 2009; 87: 563-569

198
118. M Marrari, RJ Duquesnoy. Detection of donor-specific HLA antibodies before
and after removal of a rejected kidney transplant. Transpl Immunol 2010; 22: 105-
109
119. D Tittelbach-Helmrich, P Pisarski, G Offermann, M Geyer, O Thomusch, UT
Hopt, O Drognitz. Impact of transplant nephrectomy on peak PRA levels and outcome
after kidney re-transplantation. World J Transplant 2014; 4: 141-147
120. L Martin, F Guignier, C Mousson, D Rageot, E Justrabo, G Rifle. Detection of
donor-specific anti-HLA antibodies with flow cytometry in eluates and sera from renal
transplant recipients with chronic allograft nephropathy. Transplantation 2013; 76:
395-400
121. A Girnita, E Portwood, P Brailey, M Cuffy, A Tica, F Paterno, T Diwan, S Shah, G
Mogilishetty, M Cardi, A Govil, RA Alloway, ES Woodle. Epitope cluster analysis for
donor-specific antibody identification in eluates from fine-needle allograft biopsy.
Hum Immunol 2015; 76: 125-126
122. SR Lederer, B Kluth-Pepper, H Schneeberger, E Albert, W Land, HE Feucht.
Impact of humoral alloreactivity early after transplantation on the long-term survival
of renal allografts. Kidney Int 2001; 59(1): 334-341
123. RS Gaston, JM Cecka, BL Kasiske, AM Fieberg, R Leduc, FC Cosio, S
Gourishankar, J Grande, P Halloran, L Hunsicker, R Mannon, D Rush, AJ Matas.
Evidence for antibody-mediated injury as a major determinant of late kidney allograft
failure. Transplantation 2010; 90(1): 68-74
124. S Mauiyyedi, M Crespo, AB Collins. Acute humoral rejection in kidney
transplantation. II. Morphology, immunopathology, and pathologic classification. J
Am Soc Nephrol 2002; 13: 779-789
125. G Einecke, B Sis, J Reeve, M Mengel, PM Campbell, LG Hidalgo, B Kaplan, PF
Halloran. Antibody-mediated microcirculation injury is the major cause of late kidney
transplant failure. Am J Transplant 2009; 9: 2520-2531
126. J Sellarés, DG de Freitas, M Mengel, J Reeve, G Einecke, B Sis, LG Hidalgo, K
Famulski, A Matas, PF Hallpran. Understanding the causes of kidney transplant
failure: The dominant role of antibody-mediated rejection and nonadherence. Am J
Transplant 2012; 12: 388-399
127. E Pouliquen, A Koenig, CC Chen, A Sicard, M Rabeyrin, E Morelon, V Dubois, O
Thaunat. Recent advances in renal transplantation: Antibody mediated rejection
takes center stage. F1000Prime Rep 2015; 7: 51
128. DB Tyan, VA Li, L Czer, A Trento, SC Jordan. Intravenous immunoglobulin
suppression of HLA alloantibody in highly sensitized transplant candidates and

199
transplantation with a histoincompatible organ. Transplantation 1994; 57 (4): 553-
562
129. J Watanabe, JC Scornik. IVIG and HLA antibodies. Evidence for inhibition of
complement activation but not for anti-idiotypic activity. Am J Transplant 2005; 5:
2786-2790
130. T Tha-In, J Bayry, HJ Metselaar, SV Kaveri, J Kwekkeboom. Modulation of the
cellular immune system by intravenous immunoglobulin. Trends Immunol 2008; 29:
608-615
131. C Lefaucheur, D Nochy, J Andrade, J Verine, C Gautreau, D Charron, GS Hill, D
Glotz, C Suberbielle-Boissel. Comparison of combination plasmapheresis / IVIg / anti-
CD20 versus high-dose IVIg in the treatment of antibody mediated rejection. Am J
Transplant 2009; 9: 1099-1107
132. P Hillmen, NS Young, J Schubert, RA Brodsky, G Socié, P Muus, A Röth, J Szer,
MO Elebute, R Nakamura, P Browne, AM Risitano, A Hill, H Schrezenmeier, C-L Fu, J
Maciejewski, SA Rollins, CF Mojcik, RP Rother, L Luzzatto. The complement inhibitor
Eculizumab in Paroxysmal Nocturnal Hemoglobinuria. N Engl J Med 2006; 355: 1233-
1243
133. A Barnett, R Nicholas, E Asgari, P Chowdhury, SH Sack, A Dorling, N Mamode.
The use of Eculizumab in renal transplantation. Clinical transplantation 2013; 27:
E216-229
134. MD Stegall, T Diwan, S Raghavaiah, LD Cornell, J Burns, PG Dean, FG Cosio, MJ
Gandhi, W Kremers, JM Gloor. Terminal complement inhibition decreases antibody-
mediated rejection in sensitized renal transplant recipients. Am J Transplant 2011;
11(11): 2405-2413
135. A Bentall, DB Tyan, F Sequeira, MJ Everly, MJ Gandhi, LD Cornell, H Li, NA
Henderson, S Raghavaiah, JL Winters, PG Dean, MD Stegall. Antibody-mediated
rejection despite inhibition of terminal complement. Transplant Int 2014; 27(12):
1235-1243
136. DK Perry, JM Burns, HS Pollinger, BP Amiot, JM Gloor, GJ Gores, MD Stegall.
Proteosome inhibition causes apoptosis of normal human plasma cells preventing
alloantibody production. Am J Transplant 2009; 9(1): 201-209
137. MJ Everly, JJ Everly, B Süsskind, P Brailey, LJ Arend, RR Alloway, P Roy-
Chaudhury, A Govil, G Mogilishetty, AH Rike, M Cardi, G Wadih, A Tevar, ES Woodle.
Bortezomib provides effective therapy for antibody- and cell-mediated acute
rejection. Transplantation 2008; 86(12): 1754-1761

200
138. AD Bannett, RF McAlack, R Raja, A Baquero, M Morris. Experiences with
known ABO-mismatched renal transplants. Transplant Proc 1987; 19: 4543-4546
139. MW Chopek, RL Simmons, JL Platt. ABO-incompatible renal transplantation:
Initial immunopathologic evaluation. Transplant Proc 1987; 19: 4553-4557
140. GPJ Alexandre, JP Squifflet, M De Bruyere, D Latinne, R Reding, P Gianello, M
Carlier, V Pirson. Present experiences in a series of 26 ABO-incompatible living donor
renal allografts. Transplant Proc 1987; 19: 4538-4542
141. AD Bannett, RF McAlack, M Morris, MW Chopek, JL Platt. ABO incompatible
renal transplantation: A qualitative analysis of native endothelial tissue ABO antigens
after transplant. Transplant Proc 1989; 21: 783-785
142. M Haas, MH Rahman, LC Racusen. C4d and C3d staining in biopsies of ABO-
and HLA-incompatible renal allografts: Correlation with histologic findings. Am J
Transplant 2006; 6: 1829-1840
143. M Mengel, J Bogers, JL Bosmans. Incidence of C4d stain in protocol biopsies
from renal allografts: Results from a multicenter trial. Am J Transplant 2005; 5: 1050-
1056
144. K Mizutani, P Terasaki, A Rosen, V Esquenazi, J Miller, RNJ Smith, R Pei, M
Ozawa, J Lee. Serial ten-year follow-up of HLA and MICA antibody production prior to
kidney graft failure. Am J Transplant 2005; 5(9): 2265-2272
145. FK Port, RA Wolfe, EA Mauger, DP Berling, K Jiang. Comparison of survival
probabilities for dialysis patients vs cadaveric renal transplant recipients. JAMA 1993;
270: 1339-1343
146. RA Wolfe, VB Ashby, EL Milford, AO Ojo, RE Ettenger, LY Agodoa, PJ Held, FK
Port. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting
transplantation, and recipients of a first cadaveric transplant. N Engl J Med 1999; 341:
1725-1730
147. RA Montgomery, AA Zachary. Transplanting patients with a positive donor-
specific crossmatch: A single center’s perspective. Pediatr Transplant 2004; 8: 535-
542
148. SC Jordan, A Vo, S Bunnapradist, M Toyoda, A Peng, D Puliyanda, E Kamil, D
Tyan. Intravenous immune globulin treatment inhibits crossmatch positivity and
allows for successful transplantation of incompatible organs in living-donor and
cadaver recipients. Transplantation 2003; 76: 631-636
149. MD Pescovitz. Rituximab, an anti-CD20 monoclonal antibody: History and
mechanism of action. Am J Transplant 2006; 6: 859-866

201
150. H-P Hartnug. Advances in the understanding of the mechanisms of IVIG. J
Neurol 2008; 255: 3-6
151. MD Stegall, J Gloor, JL Winters, SB Moore, S Degoey. A comparison of
plasmapheresis versus high-dose IVIG desensitization in renal allograft recipients with
high levels of donor specific alloantibody. Am J Transplant 2006; 6: 346-351
152. K Marfo, A Lu, M Ling, E Akalin. Desensitization protocols and their outcome.
CJASN 2001; 6(4): 922-936
153. RA Montgomery, BE Lonze, KE King, ES Krause, LM Kucirka, JE Locke, DS
Warren, CE Simpkins, NN Dagher, AL Singer, AA Zachary, DL Segev. Desensitization in
HLA-incompatible kidney recipients and survival. N Engl J Med 2011; 365(4): 318-326
154. FH Claas, Y Gijbels, A von Veen, LP de Waal, J D’Amaro, GG Persijn, JJ van
Rood. Selection of cross-match negative HLA-A and/or –B mismatched donors for
highly sensitized patients. Transpl Proc 1989; 21: 665-667
155. FH Claas, J De Meester, MD Witvliet, JM Smits, GG Persijn, II Doxiadis.
Acceptable HLA mismatches for highly immunized patients. Rev Immunogenet 1999;
1(3): 351-8
156. RJ Duquesnoy, S Takemoto, P De Lange, IIN Doxiadis, GM Schreuder, GG
Persijn, FH Claas. HLAMatchmaker: a molecularly based algorithm for
histocompatibility determination. III. Effect of matching at the HLA-A, B amino acid
triplet level on kidney transplant survival. Transplantation 2003; 75(6): 884-889
157. FHJ Claas, MD Witvliet, RJ Duquesnoy, GG Persijn, IIN Doxiadis. The acceptable
mismatch program as a fast tool for highly sensitised patients awaiting a cadaveric
kidney transplantation: Short waiting time and excellent graft outcome.
Transplantation 2004; 78(2): 190-193
158. FHJ Claas, A Rahmel, IIN Doxiadis. Enhanced kidney allocation to highly
sensitised patients by the acceptable mismatch program. Transplantation 2009;
88(4): 447-452
159. S Heidt, MD Witvliet, GW Haasnoot, FHJ Claas. The 25th anniversary of the
Eurotransplant Acceptable Mismatch program for highly sensitized patients. Transpl
Immunol 2015; 33(2): 51-57
160. FT Rappaport. The case for a living emotionally related international kidney
donor registry. Transplant Proc 1986; 18: 5-9
161. K Park, JI Moon, SI Kim, YS Kim. Exchange donor program in kidney
transplantation. Transplantation 1999; 67(2): 336-338

202
162. M de Klerk, KM Keizer, FH Claas, M Witvliet, BJ Haase-Kromwijk, W Weimar.
The Dutch national living donor kidney exchange program. Am J Transplant 2005;
5(9): 2302-2305
163. M de Klerk, MD Witvliet, BJ Haase-Kromwijk, FH Claas, W Weimar. A highly
efficient living donor kidney exchange program for both blood type and crossmatch
incompatible donor-recipient combinations. Transplantation 2006; 82: 1616–1620
164. G Vlad, EK Ho, ER Vasilescu, AI Colovai, MB Stokes, GS Markowitz, VD D’Agati,
DJ Cohen, LE Ratner, N Suciu-Foca. Relevance of different antibody detection
methods for the prediction of antibody-mediated rejection and deceased-donor
kidney allograft survival. Hum Immunol 2009; 70: 589-594
165. A Gupta, P Sinnott. Clinical relevance of pretransplant human leukocyte
antigen donor-specific antibodies in renal patients waiting for a transplant: A risk
factor. Hum Immunol 2009; 70: 618-622
166. D Phelan, T Mohanakumar, S Ramachandran, MD Jendrisak. Living donor renal
transplantation in the presence of donor-specific human leukocyte antigen antibody
detected by solid-phase assay. Hum Immunol 2009; 70: 584-588
167. V Aubert, J-P Venetz, G Pantaleo, M Pascual. Low levels of human leukocyte
antigen donor-specific antibodies detected by solid phase assay before
transplantation are frequently clinically irrelevant. Hum Immunol 2009; 70: 580-583
168. P Amico, G Honger, M Mayr, J Steiger, H Hopfer, S Schaub. Clinical relevance of
pretransplant donor-specific HLA antibodies detected by Single Antigen flow-beads.
Transplantation 2009; 87: 1681-1688
169. C Lefaucheur, A Loupy, GS Hill, J Andrade, D Nochy, C Antoine, C Gautreau, D
Charron, D Glotz, C Suberbielle-Boissel. Preexisting donor-specific HLA antibodies
predict outcome in kidney transplantation. J Am Soc Nephrol 2010; 21: 1398-1406
170. S Riethmüller, S Ferrari-Lacraz, MK Müller, DA Raptis, K Hadaya, B Rüsi, G
Laube, G Schneiter, T Fehr, J Villard. Donor-specific antibody levels and three
generations of crossmatches to predict antibody-mediated rejection in kidney
transplantation. Transplantation 2010; 90: 160-167
171. HG Otten, MC Verhaar, HP Borst, RJ Hene, AD van Zuilen. Pretransplant donor-
specific HLA class-I and –II antibodies are associated with an increased risk for kidney
graft failure. Am J Transplant 2012; 12: 1618-1623
172. D Thammanichanoud, A Ingsathit, T Mongkolsuk, S Rattanasiri, S
Kantachuvesiri, C Sakhonrat, C Leenanupan, S Worawichawong, P Kitpoka. Pre-
transplant donor specific antibody and its clinical significance in kidney
transplantation. Asian Pac J Allergy Immunol 2012; 30: 48-54

203
173. E David-Neto, P Souza, N Panajotopoulos, H Rodrigues, CG Ventura, DSR David,
FBC Lemos, F Agena, WC Natias, JE Kalil, MCR Castro. The impact of pretransplant
donor-specific antibodies on graft outcome in renal transplantation: A six-year
follow-up study. Clinics 2012; 67: 355-361
174. I Pérez-Flores, JL Santiago, N Calvo-Romero, A Barnentos-Guzmán, AI
Sáanchez-Fructuoso. Pretransplant anti-HLA antibodies detected by Luminex in highly
sensitized renal transplanted patients. Biomed Res Int 2013: 738404
175. P Wu, J Jin, MJ Everly, C Lin, PI Terasaki, J Chen. Impact of alloantibody
strength in crossmatch negative DSA positive kidney transplantation. Clin Biochem
2013; 46: 1389-1393
176. DS Tsapepas, R Vasilescu, B Tanriover, Y Coppleson, Y Rekhtman, MA Hardy, G
Dube, RJ Crew, LE Ratner, DJ Cohen, S Mohan. Preformed donor-specific antibodies
and risk of antibody-mediated rejection in repeat renal transplantation.
Transplantation 2014; 97: 642-647
177. J Malheiro, S Tafulo, L Dias, LS Martins, I Fonseca, I Beirão, A Castro-Henriques,
A Cabrita. Analysis of preformed donor-specific anti-HLA antibodies characteristics
for prediction of antibody-mediated rejection in kidney transplantation. Transpl
Immunol 2015; 32: 66-71
178. D Lowe, M Hathaway, D Briggs. The high dose hook effect in the detection and
monitoring of HLA specific antibody by Luminex assay. Int J Immunogenet 2007; 34:
288
179. C Weinstock, M Schnaidt. The complement-mediated prozone effect in the
Luminex single-antigen bead assay and its impact on HLA antibody determination in
patient sera. Int J Immunogenet 2013; 40(3): 171-177
180. E Schwaiger, M Wahrmann, G Bond, F Eskandry, GA Böhmig. Complement
component C3 activation: The leading cause of the prozone phenomenon affecting
HLA antibody detection on single-antigen beads. Transplantation 2014; 97(12): 1279-
1285
181. G Guidicelli, G Anies, T Bachelet, V Dubois, JF Moreau, P Merville, L Couzi, L
Taupin. The complement interference phenomenon as a cause for sharp fluctuations
of serum anti-HLA antibody strength in kidney transplant patients. Transpl Immunol
2013; 29: 17-21
182. J Visentin, M Vigata, S Daburon, C Contin-Bordes, V Fremeaux-Bacchi, C
Dromer, MA Billes, M Neau-Cransac, G Guidicelli, JL Taupin. Deciphering
complement interference in anti-human leukocyte antigen detection with flow beads
assays. Transplantation 2014; 98(6): 625-631

204
183. M Schnaidt, C Weinstock, M Jurisic, B Schmid-Horch, A Ender, D Wernet. HLA
antibody specification using single-antigen beads – A technical solution for the
prozone effect. Transplantation 2011; 92(5): 510-515
184. V Kosmoliaptsis, JA Bradley, S Peacock, AN Chaudhry, CJ Taylor. Detection of
immunoglobulin G human leukocyte antigen-specific alloantibodies in renal
transplant patients using single-antigen beads is compromised by the presence of
immunoglobulin M human leukocyte antigen-specific alloantibodies. Transplantation
2009; 87(6); 813-820
185. AA Zachary, DP Lucas, B Detrick, MS Leffell. Naturally occurring interference in
Luminex® assays for HLA-specific antibodies: Characteristics and resolution. Hum
Immunol 2009; 70(7): 496-501
186. PR Warner, D Youngs, KA Nelson. HLA density on microparticles versus
antibody detection sensitivity: Implications for crossmatch prediction. Hum Immunol
2007; 68(1): 528
187. S Hemmatpour, S Todd, D Sage. Variation of antigen density on HLA single
antigen beads – Implications for sensitised patients awaiting kidney transplantation.
Transpl Int 2011; 24(52): 354
188. LE Morales-Buenrostrom PI Terasaki, LA Marino-Vázquez, JH Lee, N El-Awar, J
Alberu. “Natural” human leukocyte antigen antibodies found in nonalloimmunized
healthy males. Transplantation 2008; 86(8): 1111-1115
189. N El-Awar, PI Terasaki, A Nguyen, N Sasaki, LE Morales-Buenrostro, H Saji, E
Maruya, F Poli. Epitopes of HLA antibodies found in sera of normal healthy males and
cord blood. Clin Transpl 2008: 199-214
190. N El-Awar, JH Lee, C Tarsitani, PI Terasaki. HLA class I epitopes: Recognition of
binding sites by mAbs or eluted alloantibodies confirmed with single recombinant
antigens. Hum Immunol 2007; 68(3): 170-180
191. HG Otten, MC Verhaar, HPE Borst, M van Eck, WGJ van Ginkel, RJ Hene, AD van
Zuilen. The significance of pretransplant donor-specific antibodies reactive with
intact or denatured human leucocyte antigen in kidney transplantation. Clin Exp
Immunol 2013; 173: 536-543
192. P Wu, MJ Everly, LM Rebellato, CE Haisch, KP Briley, P Bolin, WT Kendrick, C
Morgan, RC Harland, PI Terasaki. Trends and characteristics in early glomerular
filtration rate decline after post transplantation alloantibody appearance.
Transplantation 2013; 96: 919-925
193. G Opelz, B Graver, PI Terasaki. Induction of high kidney graft survival rate by
multiple transfusion. Lancet 1981; 1: 1223-1225; MA Blajchman. Immunomodulatory

205
effects of allogeneic blood transfusions: Clinical manifestations and mechanisms. Vox
Sang 1998; 74: 315-319
194. FH Claas, DL Roelen, JJ van Rood, A Brand. Modulation of the alloimmune
response by blood transfusion. Transfus Clin Biol 2001; 8: 315-31
195. JC Scornik, JE Ireland, RJ Howard, WW Pfaff. Assessment of the risk for broad
sensitization by blood transfusions. Transplantation 1984; 37: 249-253
196. S Vaidya, D Partlow, B Susskind, M Noor, T Barnes, K Gugliuzza. Prediction of
crossmatch outcome of highly sensitized patients by single and / or multiple antigen
bead luminex assay. Transplantation 2006; 82: 1524-1528
197. AR Tambur, DS Ramon, DB Kaufman, J Friedwald, X Luo, B Ho, A Skaro, J
Caicedo, D Ladner, T Baker, J Fryer, L Gallon, J Miller, MM Abecassis, J Leventhal.
Perception versus reality?: Virtual crossmatch – How to overcome some of the
technical and logistic limitations. Am J Transplant 2009; 9: 1886-1893
198. GP Morris, DL Phelan, MD Jendrisak, T Mohanakumar. Virtual crossmatch by
identification of donor-specific anti-human leukocyte antigen antibodies by solid-
phase immunoassay: A 30-month analysis in living donor kidney transplantation. Hum
Immunol 2010; 71: 268-273
199. CM Worsley, ES Mayne, MS Suchard. Luminex-based virtual crossmatching for
renal transplantation in South Africa. S Afr Med J 2012; 102: 40-43; G Schlaf, B Pollok-
Kopp, WW Alterman. Solid phase-based cross-matching in order to avoid kidney
allografting against donor-specific anti-HLA antibodies: Long term experience with a
procedure allowing highly reliable diagnoses. Austin J Nephrol Hypertens 2014; 1:
1028
200. A Piazza, G Ozzella, E Poggi, D Caputo, A Manfreda, D Adorno. Virtual
crossmatch in kidney transplantation. Transplant Proc 2014; 46: 2915-2918
201. L Cantwell, C Woodroffe, R Holdsworth, P Ferrari. Four years of experience
with the Australian kidney paired donation programme. Nephol 2015; 20(30): 124-
131
202. D Dragun. Humoral responses directed against non-human leukocyte antigens
in solid organ transplantation. Transplantation 2008; 86(8): 1019-1025
203. D Dragun, A Phillippe, R Catar. Role of non-HLA antibodies in organ
transplantation. Curr Opin Organ Transplant 2012; 17(4): 440-445
204. S Sumitran-Holgersson. Relevance of MICA and other non-HLA antibodies in
clinical transplantation. Curr Opin Immunol 2008; 20(5): 607-613
205. D Glotz, C Antoine, P Julia, C Suberbielle-Boissel, S Boudjeltia, R Fraoui, C
Hacen, A Duboust, J Bariety. Desensitization and subsequent kidney transplantation

206
of patients using intravenous immunoglobulin (IVIg). Am J Transplant 2002; 2: 758-
760
206. RA Montgomery, BE Lonze, KE King, ES Kraus, LM Kucirka, JE Locke, DS Warren,
CE Simpkins, NN Dagher, AL Singer, AA Zachary, DL Segev. Desensitization in HLA-
incompatible kidney recipients and survival. N Engl J Med 2011; 365: 318-326
207. BJ Orandi, X Luo, AB Massie, JM Garonzik-Wang, BE Lonze, R Ahmed, KJ Van
Arendonk, MD Stegall, SC Jordan, J Oberholzer, TB Dunn, LE Ratner, S Kapur, RP
Pelletier, JP Roberts, ML Melcher, P Singh, DL Sudan, MP Posner, JM El-Amm, R
Shapiro, M Cooper, GS Lipkowitz, MA Rees, CL Marsh, BR Sankari, DA Gerber, PW
Nelson, J Wellen, A Bozorgzadeh, AO Gaber, RA Montgomery, DL Segev. Survival
benefit with kidney transplants from HLA-incompatible live donors. N Engl J Med
2016; 374: 940-950
208. V Kosmoliaptsis, LD Sharples, AN Chaudhry, DJ Halsall, JA Bradley, CJ Taylor.
Predicting HLA class II alloantigen immunogenicity from the number and
physiochemical properties of amino acid polymorphisms. Transplantation 2011; 91:
183-190
209. V Kosmoliaptsis, TR Dafforn, AN Chaudhry, DJ Halsall, JA Bradley, CJ Taylor.
High-resolution, three-dimensional modelling of human leukocyte antigen class I
structure and surface electrostatic potential reveals the molecular basis for
alloantibody binding epitopes. Hum Immunol 2011; 72(11): 1049-1059
210. VC Joysey, E Wolf. HLA-A, -B and –C antigens, their serology and cross-
reaction. Br Med Bull 1978; 34: 217-222
211. RJ Duquesnoy. HLAMatchmaker: A molecularly based algorithm for
histocompatibility determination: I. Description of the algorithm. Hum Immunol
2002; 63: 339-352
212. RJ Duquesnoy, M Askar. HLAMatchmaker: A molecularly based algorithm for
histocompatibility determination v. Eplet matching for HLA-DR, HLA-DQ and HLA-DP.
Hum Immunol 2007; 68(1): 12-25
213. RJ Duquesnoy. The antibody response to an HLA mismatch: a model for
nonself-self discrimination in relation to HLA epitope immunogenicity. Int J
Immunogenet 2012; 39(1): 1-9
214. M Resse, R Paolillo, BP Minucci, G Moccia, C Napoli. Antibody-reactive class I
epitopes defined by pairs of mismatched eplets and self-eplets. Tissue Antigens 2015;
86(5): 368-372

207
215. N El-Awar, JH Lee, C Tarsitani, PI Terasaki. HLA class I epitopes: Recognition of
binding sites by mAbs or eluted alloantibody confirmed with single recombinant
antigens. Hum Immunol 2007; 68: 170-180
216. RJ Duquesnoy, M Marrari. Correlations between Terasaki’s HLA class I epitopes
and HLAMatchmaker-defined eplets on HLA-A, -B and –C antigens. Tissue Antigens
2009; 74(2): 117-133
217. M Marrari, RJ Duquesnoy. Correlations between Terasaki’s HLA class II
epitopes and HLAMatchmaker-defined eplets on HLA-DR and -DQ antigens. Tissue
Antigens 2009; 74(2): 134-146
218. MKA Dankers, MD Witvliet, DL Roelen, P De Lange, N Korfage, GG Persijn, R
Duquesnoy, IIN Doxiadis, FH Claas. The number of amino acid triplet differences
between patient and donor is predictive for the antibody reactivity against
mismatched human leukocyte antigens. Transplantation 2004; 77(8): 1236-1239
219. RS Goodman, CJ Taylor, CM O’Rourke, A Lynch, JA Bradley, T Key. Utility of
HLAMatchmaker and single-antigen HLA-antibody detection beads for identification
of acceptable mismatches in highly sensitised patients awaiting kidney
transplantation. Transplantation 2006; 81(9): 1331—1336
220. V Kosmoliaptsis, JA Bradley, LD Sharples, A Chaudhry, T Key, RS Goodman, CJ
Taylor. Predicting the immunogenicity of human leukocyte antigen class I
alloantigens using structural epitope analysis determined by HLAMatchmaker.
Transplantation 2008; 85(12): 1817-1825
221. AA Zachary, D Kopchaliiska, RA Montgomery, MS Leffell. HLA-specific B cells. i.
A method for their detection, quantification, and isolation using HLA tetramers.
Transplantation 2007; 83(7): 982-988
222. M Han, JA Rogers, B Lavingia, P Stastny. Peripheral blood B cells producing
donor-specific HLA antibodies in vitro. Hum Immunol 2009; 70: 29-34
223. S Heidt, DL Roelen, YJH de Vaal, MGD Kester, C Eijsink, S Thomas, NM van
Besouw, HD Volk, W Weimer, FHJ Claas, A Mulder. A novel ELISPOT assay to quantify
HLA-specific B cells in HLA-immunized individuals. Am J Transplant 2012; 12: 1469-
1478
224. M Lucia, S Luque, E Crespo, E Melilli, JM Cruzado, J Martorell, M Jarque, S Gil-
Vernet, A Manonelles, JM Gringό, O Bestard. Preformed circulating HLA-specific
memory B cells predict high risk of humoral rejection in kidney transplantation.
Kidney International 2015; 88: 874-887
225. DB Tyan. New approaches for detecting complement-fixing antibodies. Curr
Opin Organ Transplant 2012; 17: 409-415

208
226. M Wahrmann, G Bartel, M Exner, H Regele, GF Körmöczi, GF Fischer, GA
Böhmig. Clinical relevance of preformed C4d-fixing and non-C4d-fixing HLA single
antigen reactivity in renal allograft recipients. Transpl Int 2009; 22(10): 982-989
227. G Hönger, M Wahrmann, P Amico, H Hopfer, GA Böhmig, S Schaub. C4d-fixing
capability of low-level donor-specific HLA antibodies is not predictive for early
antibody-mediated rejection. Transplantation 2010; 89(12): 1471-1475
228. JM Yabu, JP Higgins, G Chen, F Sequeira, S Busque, DB Tyan. C1q-fixing human
leukocyte antigen antibodies are specific for predicting transplant glomerulopathy
and late graft failure after kidney transplantation. Transplantation 2011; 91(3): 342-
347
229. SM Sutherland, G Chen, FA Sequeira, CD Lou, SR Alexander. Complement-fixing
donor-specific antibodies identified by a novel C1q assay are associated with allograft
loss. Pediatr Transplantation 2012; 16(1): 12-17
230. C Lawrence, M Willicombe, PA Brookes, E Santos-Nunez, R Bajaj, T Cook, C
Roufosse, D Taube, AN Warrens. Preformed complement-activating low-level donor-
specific antibody predicts early antibody-mediated rejection in renal allografts.
Transplantation 2013; 95(2): 341-346
231. M Crespo, A Torio, V Mas, D Redondo, MJ Pérez-Sáez, M Mir, A Faura, R
Guerra, O Montes-Ares, MD Checa, J Pascual. Clinical relevance of pretransplant anti-
HLA donor-specific antibodies: Does C1q fixation matter? Transpl Immunol 2013; 29:
28-33
232. A Loupy, C Lefaucheur, D Vernerey, C Prugger, J-P Duong van Huyen, N
Mooney, C Suberbielle, V Frémeaux-Bacchi, A Méjean, F Desgrandchamps, D
Anglicheau, D Nochy, D Charron, J-P Empana, M Delahousse, C Legendre, D Glotz, GS
Hill, A Zeeva, X Jouven. Complement-binding anti-HLA antibodies and kidney-allograft
survival. N Engl J Med 2013; 369: 1215-1226
233. A Zeevi, J Lunz, B Feingold, M Shullo, C Bermudez, J Teuteberg, S Webber.
Persistent strong anti-HLA antibody at high titer is complement binding and
associated with increased risk of antibody-mediated rejection in heart transplant
recipients. J Heart Lung Transplant 2013; 32(1): 98-105
234. M Yell, BL Muth, DB Kaufman, A Djarnali, TM Ellis. C1q binding activity of de
novo donor-specific HLA antibodies in renal transplant recipients with and without
antibody-mediated rejection. Transplantation 2015; 99: 1151-1155
235. D Thammanichanond, P Wiwattanathum, T Mongkolsuk, S Kantachuvesiri, S
Worawichawong, SA Vallipakorn, P Kitpoka. Role of pretransplant complement-fixing

209
donor-specific antibodies identified by C1q assay in kidney transplantation.
Transplant Proc 2016; 48(3): 756-760
236. KA Thomas, NM Valenzuela, EF Reed. The perfect storm: HLA antibodies,
complement, FcϒRs and endothelium in transplant rejection. Trends Mol Med 2015;
21(5): 319-329
237. RM Anthony, F Nimmerjahn. The role of differential IgG glycosylation in the
interaction of antibodies with FcγRs in vivo. Curr Opin Organ Transplant 2011; 16(1):
7-14

210
Appendix

211
Appendix
Table I. Conexio Genomics HLA Sequencing Based Typing kit details. The PRE-PCR
component of each kit consists of a vial/s of a locus-specific PCR mix (e.g. CG-HLA-A mix )
consisting of PCR buffer, dNTPs, MgCl2, locus specific PCR primers, and a single vial of
DNA polymerase (DNA Pol ). The POST-PCR kit contains sequencing primers (e.g. AEX1F).
Kit Catalogue
No
No Tests Pre-PCR contents Post PCR contents
Reagent Volume Primer
Name
Volume
HLA-A XH-PD1.1-2(50) XH-PD1.1-
2(100)
50 tests 100 tests
DNA Pol
CG-HLA-A mix
DNA Pol
CG-HLA-A mix
1 x 55ul
1x 880ul
1 x 110ul
2 x 880ul
AEX1F,
AEX1R,
AEX2F,
AEX2R,
AEX3F,
AEX3R,
AEX4F,
AEX4R
AEX1F,
AEX1R,
AEX2F,
AEX2R,
AEX3F,
AEX3R,
AEX4F,
AEX4R
1 x 110ul of each
1 x 220ul of each
HLA-B BS-PD2.1-2(50) BS-PD2.1-
2(100)
50 tests
100 tests
DNA Pol
CG-HLA-B mix
DNA Pol
1 x 55ul
1x 880ul
1 x 110ul
BEX1F,
BEX2F,
BEX2R,
BEX3F,
BEX3R,
BEX4F,
BEX4R
BEX1F,
BEX2F,
1 x 110ul of each
1 x 220ul of each

212
CG-HLA-B mix
2 x 880ul
BEX2R,
BEX3F,
BEX3R,
BEX4F,
BEX4R
HLA-C HH-PD 3.2-2(50) HH-PD
3.2-2(100)
50 tests
100 tests
DNA Pol
CG-HLA-C mix
DNA Pol
CG-HLA-C mix
1 x 55ul
1x 880ul
1 x 110ul
2 x 880ul
CEX1F,
CEX1R,
CEX2F,
CEX2R,
CEX3F,
CEX3R,
CEX4F,
CEX4R,
CEX5F,
CEX5R,
CEX6F,
CEX6R,
CEX7F,
CEX7R,
CEX8F
CEX1F,
CEX1R,
CEX2F,
CEX2R,
CEX3F,
CEX3R,
CEX4F,
CEX4R,
CEX5F,
CEX5R,
CEX6F,
CEX6R,
CEX7F,
CEX7R,
CEX8F
1 x 110ul of each
1 x 220ul of each
DRB1 HH-PD5.2-4(50) HH-PD5.2-4(100)
50 tests
100 tests
DNA Pol
CG-HLA-DRB1
mix
DNA Pol
1 x 18ul
1 x 920ul
1 x 36ul
DRB1EX2F,
DRB1EX3R,
DRB1EX3R,
RB-TG344-R
DRB1EX2F,
DRB1EX3R,
DRB1EX3R,
RB-TG344-R
1 x 110ul of each
1 x 220ul each

213
CG-HLA-DRB1
mix
2 x 920ul
DQB1 PQ-PD6.2-1(50) PQ-PD6.2-
1(100)
50 tests
100 tests
DNA Pol
CG-HLA-DQB1
mix
DNA Pol
CG-HLA-DQB1
mix
1 x 18ul
1 x 920ul
1 x 36ul
2 x 920ul
DQB1EX2F,
DQB1EX2R,
DQB1EX3F.
DQB1EX3R
DQB1EX2F,
DQB1EX2R,
DQB1EX3F.
DQB1EX3R
1 x 110ul of each
1 x 220ul of each