Embed Size (px)
Citation preview
T H E C A R O T I D - B A S I L A R A R T E R Y
A REPORT AND DISCUSSION OF FIVE CASES
JOHN LAMB, M.B., CH.B., F.F.R., and LEON MORRIS, M.B., B.CH., F.F.R.
X-ray Department, Brook Hospital, Shooters Hill Road, London, S.E.18
Ay anomalous vessel joining the carotid and basilar arteries was first described by Quain in 1844 and subsequent descriptions, mainly in the German literature, show that its existence was well known to nineteenth century anatomists. The literature was reviewed by Oertel (1922) and the condition further discussed by Sunderland (1948).
The first case diagnosed by arteriography, during life, was described by Sutton (1950) and we have been unable to find any further such cases in the British literature since this time, although study of the American, Scandinavian and German literature shows that the anomaly has been described with greater frequency in recent years (Harrison and Luttrel 1953; Murtagh et al 1955; Zaclis 1955; Saltzman 1959; Wiedenmann 1959).
It was considered therefore that five further cases
were worthy of discussion, particularly as in three, both arteriography and autopsy were carried out.
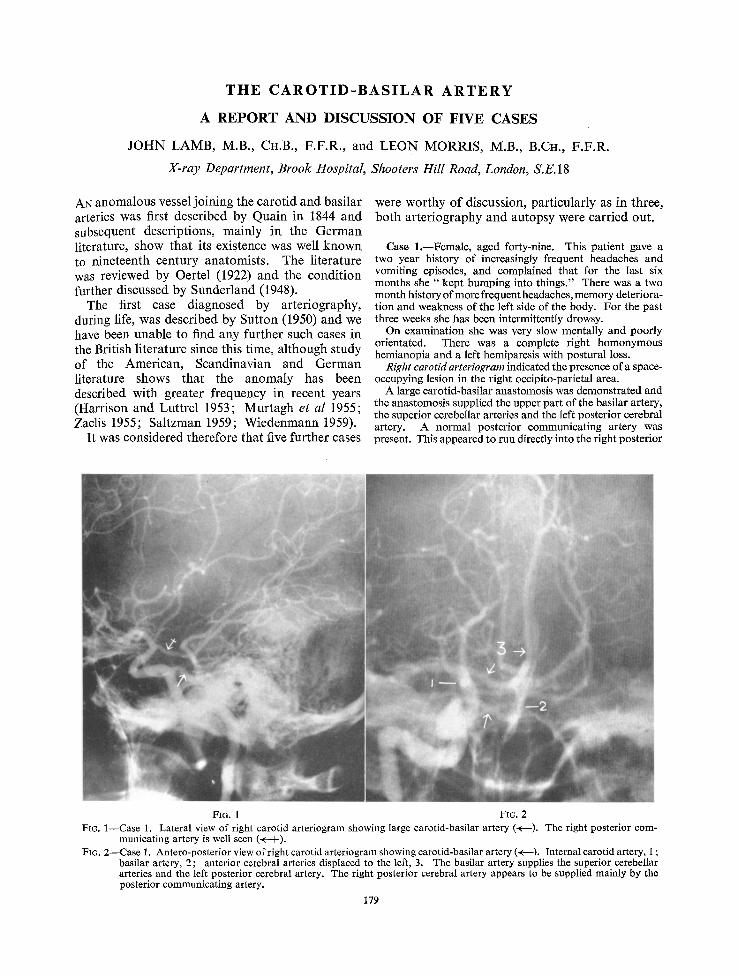
Case 1.--Female, aged forty-nine. This patient gave a two year history of increasingly frequent headaches and vomiting episodes, and complained that for the last six months she " k e p t bumping into things." There was a two month history of more frequent headaches, memory deteriora- t ion and weakness of the left side of the body. For the past three weeks she has been intermittently drowsy.
On examination she was very slow mentally and poorly orientated. There was a complete right homonymous hemianopia and a left hemiparesis with postural loss.
Right carotM arteriogram indicated the presence of a space- occupying lesion in the right occipito-parietal area.
A large carotid-basilar anastomosis was demonstrated and the anastomosis supplied the upper part of the basilar artery, the superior cerebellar arteries and the left posterior cerebral artery. A normal posterior communicating artery was present. This appeared to run directly into the right posterior
FIG. 1 FIG. 2 Fro. 1--Case 1. Lateral view of right carotid arteriogram showing large carotid-basilar artery (~---). The right posterior com-
municating artery is well seen (~( I ). FIG. 2--Case 1. Antero-posterior view of right carotid arteriogram showing carotid-basilar artery (+---). Internal carotid artery, 1 ;
basilar artery, 2 ; anterior cerebral arteries displaced to the left, 3. The basilar artery supplies the superior cerebellar arteries and the left posterior cerebral artery. The right posterior cerebral artery appears to be supplied mainly by the posterior communicating artery.
179
180 C L I N I C A L R A D I O L O G Y
I~IC4tT V ~ r E ~ R t ~ L
J
• \ ; °
~ FT
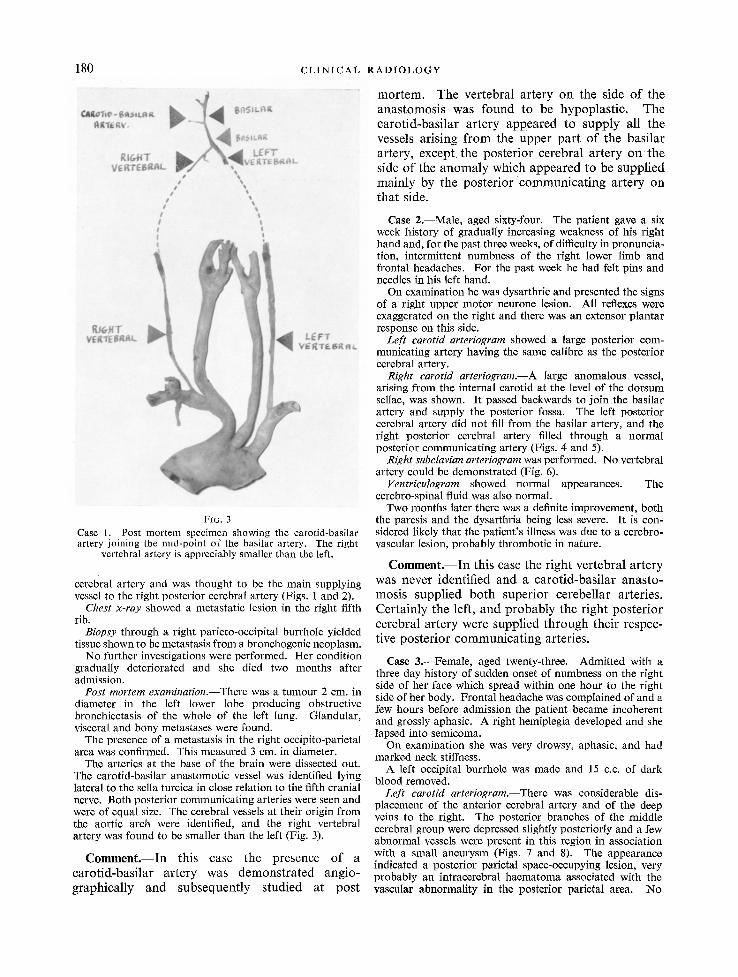
FIG. 3 Case 1. Post mortem specimen showing the carotid-basilar artery joining the mid-point of the basilar artery. The right
vertebral artery is appreciably smaller than the left.
cerebral artery and was thought to be the main supplying vessel to the right posterior cerebral artery (Figs. 1 and 2).
Chest x-ray showed a metastatic lesion in the right fifth rib.
Biopsy through a right parieto-occipital burrhole yielded tissue shown to be metastasis from a bronchogenic neoplasm.
No further investigations were performed. Her condition gradually deteriorated and she died two months after admission.
Post mortem examination.--There was a tumour 2 cm. in diameter in the left lower lobe producing obstructive bronchiectasis of the whole of the left lung. Glandular, visceral and bony metastases were found.
The presence of a metastasis in the right occipito-parietal area was confirmed. This measured 3 cm. in diameter.
The arteries at the base of the brain were dissected out. The carotid-basilar anastomotic vessel was identified lying lateral to the sella turcica in close relation to the fifth cranial nerve. Both posterior communicating arteries were seen and were of equal size. The cerebral vessels at their origin from the aortic arch were identified, and the right vertebral artery was found to be smaller than the left (Fig. 3).
C o m m e n t . - - I n t h i s c a se t h e p r e s e n c e o f a c a r o t i d - b a s i l a r a r t e r y w a s d e m o n s t r a t e d a n g l o - g r a p h i c a l l y a n d s u b s e q u e n t l y s t u d i e d a t p o s t
m o r t e m . T h e v e r t e b r a l a r t e r y o n t h e s ide o f t h e a n a s t o m o s i s w a s f o u n d to b e h y p o p l a s t i c . T h e c a r o t i d - b a s i l a r a r t e r y a p p e a r e d to s u p p l y a l l t h e vessels a r i s i n g f r o m the u p p e r p a r t o f t h e b a s i l a r a r t e ry , e x c e p t t h e p o s t e r i o r c e r e b r a l a r t e r y o n t h e side o f t h e a n o m a l y w h i c h a p p e a r e d to b e s u p p l i e d m a i n l y b y t h e p o s t e r i o r c o m m u n i c a t i n g a r t e r y o n t h a t s ide.
Case 2.--Male, aged sixty-four. The patient gave a six week history of gradually increasing weakness of his right hand and, for the past three weeks, of difficulty in pronuncia- tion, intermittent numbness of the right lower limb and frontal headaches. For the past week he had felt pins and needles in his left hand.
On examination he was dysarthric and presented the signs of a right upper motor neurone lesion. All reflexes were exaggerated on the right and there was an extensor plantar response on this side.
Left carotid arteriogram showed a large posterior com- municating artery having the same calibre as the posterior cerebral artery.
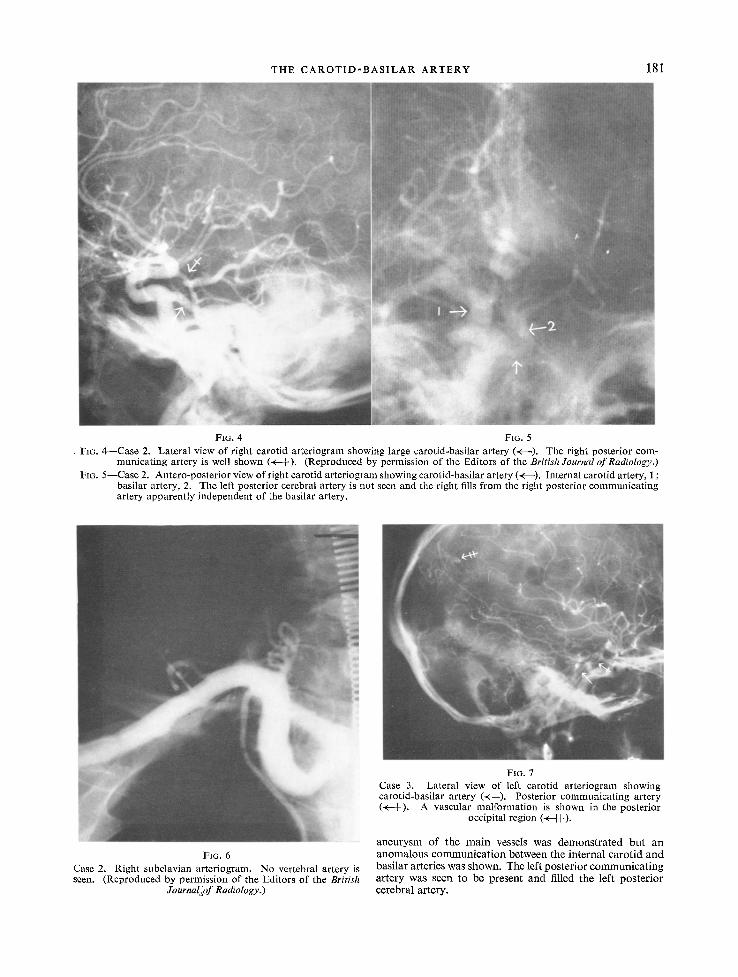
Right carotid arteriogram.--A large anomalous vessel, arising from the internal carotid at the level of the dorsum sellae, was shown. It passed backwards to join the basilar artery and supply the posterior fossa. The left posterior cerebral artery did not fill from the basilar artery, and the right posterior cerebral artery filled through a normal posterior communicating artery (Figs. 4 and 5).
Right subclavian arteriogram was performed. No vertebral artery could be demonstrated (Fig. 6).
Ventriculogram showed normal appearances. The cerebro-spinal fluid was also normal.
Two months later there was a definite improvement, both the paresis and the dysartbria being less severe. It is con- sidered likely that the patient's illness was due to a cerebro- vascular lesion, probably thrombotic in nature.
C o m m e n t . - - I n t h i s case t h e r i g h t v e r t e b r a l a r t e r y was n e v e r i d e n t i f i e d a n d a c a r o t i d - b a s i l a r a n a s t o - m o s i s s u p p l i e d b o t h s u p e r i o r c e r e b e l l a r a r t e r i es . C e r t a i n l y t h e left , a n d p r o b a b l y t h e r i g h t p o s t e r i o r c e r e b r a l a r t e r y we re s u p p l i e d t h r o u g h t h e i r r e spec - t ive p o s t e r i o r c o m m u n i c a t i n g a r te r ies .
Case 3.--Female, aged twenty-three. Admitted with a three day history of sudden onset of numbness on the right side of her face which spread within one hour to the right side of her body. Frontal headache was complained of and a few hours before admission the patient became incoherent and grossly aphasic. A right hemiplegia developed and she lapsed into semicoma.
On examination she was very drowsy, aphasic, and had marked neck stiffness.
A left occipital burrhole was made and 15 c.c. of dark blood removed.
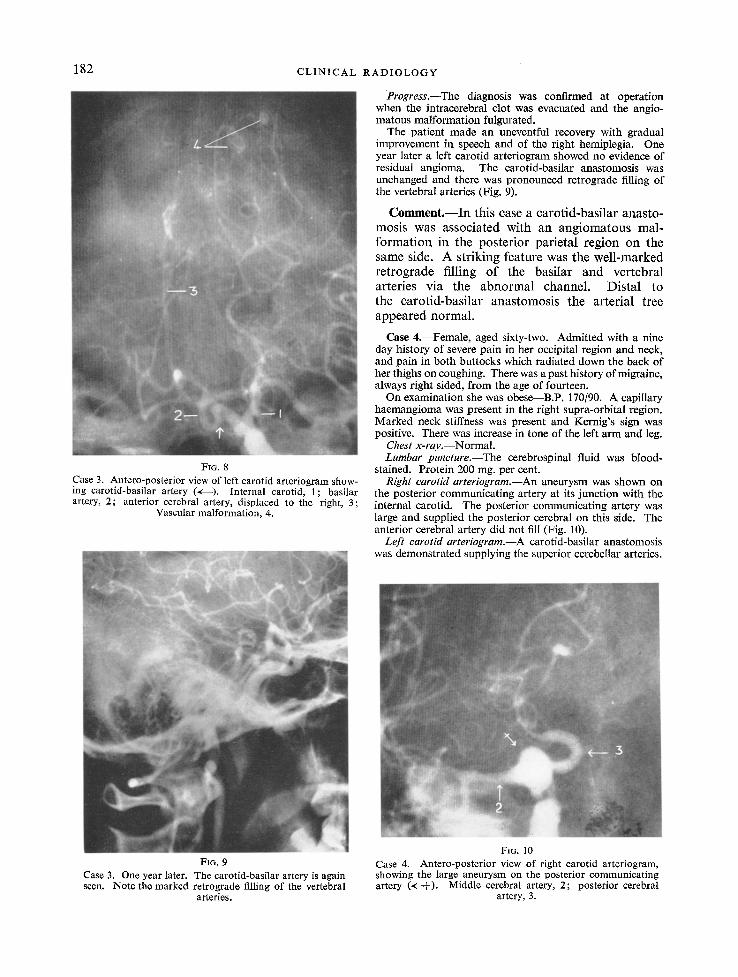
Left carotid arteriogram.--There was considerable dis- placement of the anterior cerebral artery and of the deep veins to the right. The posterior branches of the middle cerebral group were depressed slightly posteriorly and a few abnormal vessels were present in this region in association with a small aneurysm (Figs. 7 and 8). The appearance indicated a posterior parietal space-occupying lesion, very probably an intracerebral haematoma associated with the vascular abnormality in the posterior parietal area. No
T HE C A R O T I D - B A S I L A R A R T E R Y 181
FIG. 4 FIG. 5 Fro. 4 - -Case 2. Lateral view of right carotid arteriogram showing large carotid-basilar artery (+---). The right posterior com-
municating artery is well shown (+-4-). (Reproduced by permission of the Editors of the British Journal of Radiology.) Fro. 5- -Case 2. Antero-posterior view of right carotid arteriogram showing carotid-basilar artery (~----). Internal carotid artery, 1 ;
basilar artery, 2. The left posterior cerebral artery is not seen and the right fills from the right posterior communicat ing artery apparently independent of the basilar artery.
FIG. 6 Case 2. Right subclavian arteriogram. No vertebral artery is seen. (Reproduced by permission of the Editors of the British
Journal lo f Radiology.)
FIG. 7 Case 3. Lateral view of left carotid arteriogram showing carotid-basilar artery (+--), Posterior communicating artery (< i ), A vascular malformation is shown in the posterior
occipital region (<--H-),
a n e u r y s m of the m a i n vessels was demons t ra ted bu t an anoma lous c o m m u n i c a t i o n between the internal carot id and basi lar arteries was shown. The left poster ior c o m m u n i c a t i n g artery was seen to be present and filled the left pos te r ior cerebral artery.
182 C L I N I C A L R A D I O L O G Y
FIG. 8
Case 3. Antero-posterior view of left carotid arteriogram show- ing carotid-basilar artery (+---). Internal carotid, 1; basilar artery, 2; anterior cerebral artery, displaced to the right, 3;
Vascular malformation, 4.
Progress.--The diagnosis was confirmed at operation when the intracerebral clot was evacuated and the angio- matous malformation futgurated.
The patient made an uneventful recovery with gradual improvement in speech and of the right hemiplegia. One year later a left carotid arteriogram showed no evidence of residual angioma. The carotid-basilar anastomosis was unchanged and there was pronounced retrograde filling of the vertebral arteries (Fig. 9).
Comment . - - In this case a carotid-basilar anasto- mosis was associated with an angiomatous mal- formation in the posterior parietal region on the same side. A striking feature was the well-marked retrograde filling of the basilar and vertebral arteries via the abnormal channel. Distal to the carotid-basilar anastomosis the arterial tree appeared normal.
Case 4.--Female, aged sixty-two. Admitted with a nine day history of severe pain in her occipital region and neck, and pain in both buttocks which radiated down the back of her thighs on coughing. There was a past history of migraine, always right sided, from the age of fourteen.
On examination she was obese--B.P. 170/90. A capillary haemangioma was present in the right supra-orbital region. Marked neck stiffness was present and Kernig's sign was positive. There was increase in tone of the left arm and leg.
Chest x-ray.--Normal. Lumbar puneture.--The cerebrospinal fluid was blood-
stained. Protein 200 rag. per cent. Right carotid arteriogram.---An aneurysm was shown on
the posterior communicating artery at its junction with the internal carotid. The posterior communicating artery was large and supplied the posterior cerebral on this side. The anterior cerebral artery did not fill (Fig. 10).
Left earotM arteriogram.--A carotid-basilar anastomosis was demonstrated supplying the superior cerebellar arteries.
FIG. 9 Case 3. One year later. The carotid-basilar artery is again seen. Note the marked retrograde filling of the vertebral
arteries.
Fm. 10 Case 4. Antero-posterior view of right carotid arteriogram, showing the large aneurysm on the posterior communicating artery (~: I ). Middle cerebral artery, 2; posterior cerebral
artery, 3.
THE C A R O T I D - B A S I L A R ARTERY 183
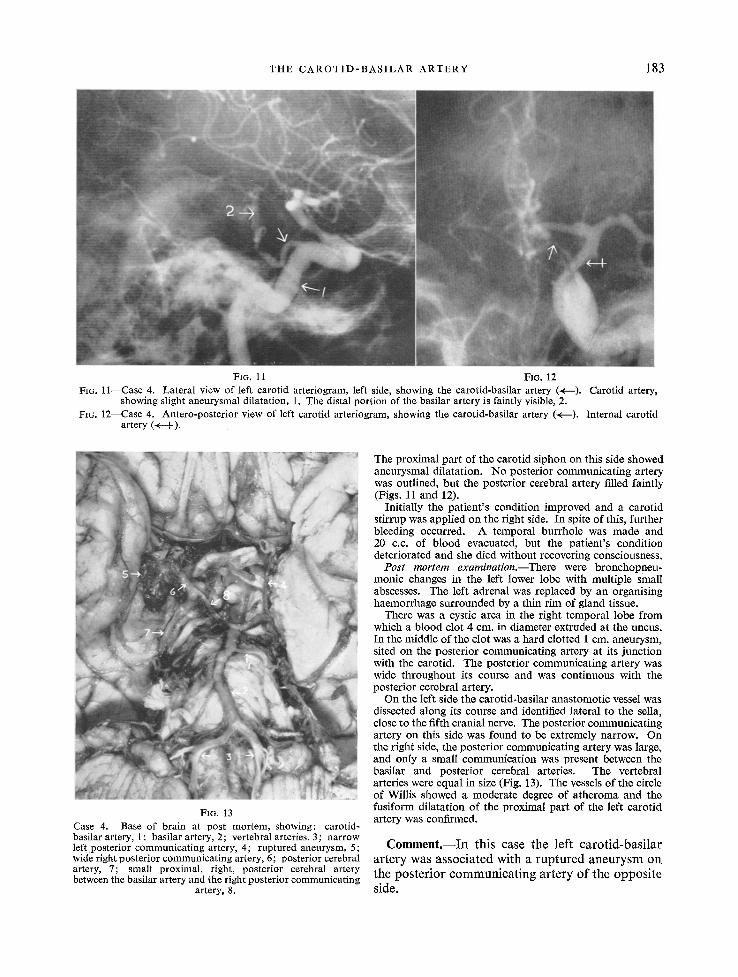
FIG. 11 FIG. 12 FIG. 11--Case 4. Lateral view of left carotid arteriogram, left side, showing the carotid-basilar artery (+ - ) . Carotid artery,
showing slight aneurysmal dilatation, 1. The distal portion of the basilar artery is faintly visible, 2. FIG. 12--Case 4. Antero-posterior view of left carotid arteriogram, showing the carotid-basilar artery (<---). Internal carotid
artery (+-+).
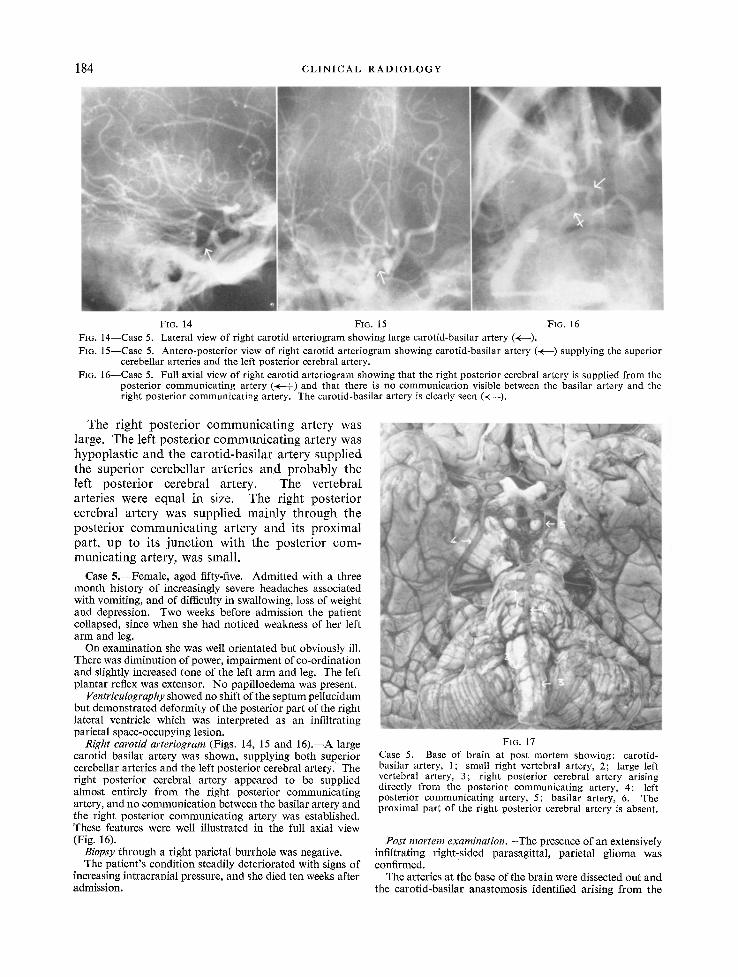
FIG. 13 Case 4. Base of brain at post mortem, showing: carotid- basilar artery, 1; basilar artery, 2; vertebral arteries, 3; narrow leftposterior communicating artery, 4; ruptured aneurysm, 5; wide right posterior communicating artery, 6; posterior cerebral artery, 7; small proximal, right, posterior cerebral artery between the basilar artery and the right posterior communicating
artery, 8.
The proximal part of the carotid siphon on this side showed aneurysmal dilatation. No posterior communicating artery was outlined, but the posterior cerebral artery filled faintly (Figs. 11 and 12).
Initially the patient 's condition improved and a carotid stirrup was applied on the right side. In spite of this, further bleeding occurred. A temporal burrhole was made and 20 c.c. of blood evacuated, but the patient 's condition deteriorated and she died without recovering consciousness.
Post mortem examination.--There were bronchopneu- monic changes in the left lower lobe with multiple small abscesses. The left adrenal was replaced by an organising haemorrhage surrounded by a thin rim of gland tissue.
There was a cystic area in the right temporal lobe from which a blood clot 4 cm. in diameter extruded at the uncus, In the middle of the clot was a hard clotted 1 cm. aneurysm, sited on the posterior communicating artery at its junction with the carotid. The posterior communicating artery was wide throughout its course and was continuous with the posterior cerebral artery.
On the left side the carotid-basilar anastomotic vessel was dissected along its course and identified lateral to the sella, close to the fifth cranial nerve. The posterior communicating artery on this side was found to be extremely narrow. On the right side, the posterior communicating artery was large, and only a small communication was present between the basilar and posterior cerebral arteries. The vertebral arteries were equal in size (Fig. 13). The vessels of the circle of Willis showed a moderate degree of atheroma and the fusiform dilatation of the proximal part of the left carotid artery was confirmed.
C o m m e n t . - - I n t h i s case t h e l e f t c a r o t i d - b a s i l a r a r t e r y w as a s s o c i a t e d w i t h a r u p t u r e d a n e u r y s m o n t h e p o s t e r i o r c o m m u r t i c a t i n g a r t e r y o f t h e o p p o s i t e side.
184 C L I N I C A L R A D I O L O G Y
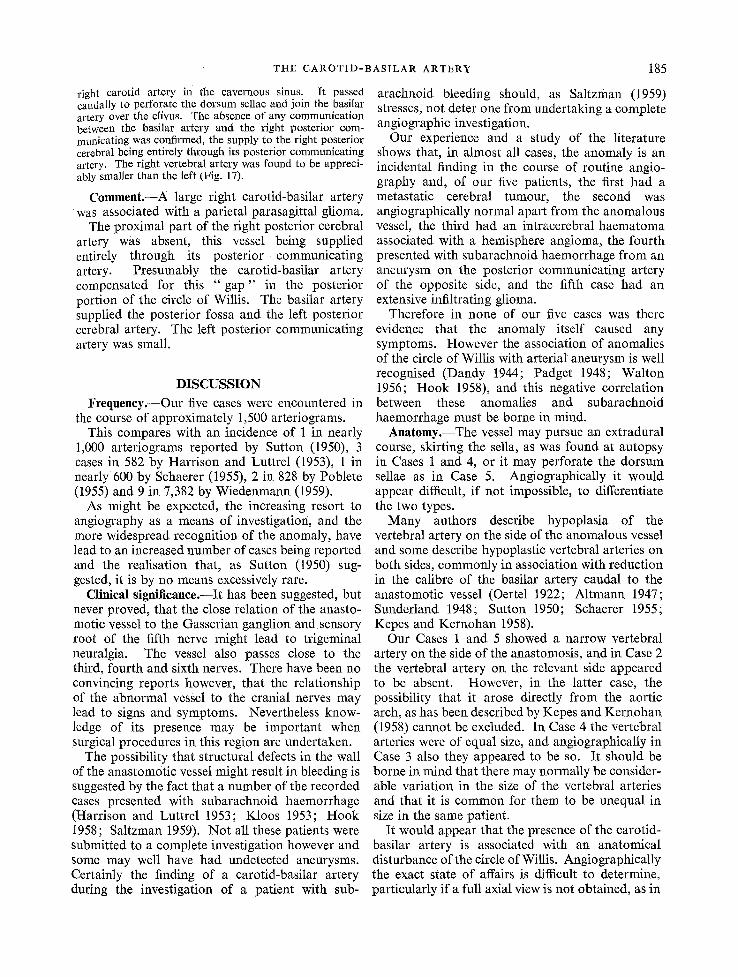
FIG. 14 Fie. 15 FIG. 16 FIG. 14--Case 5. Lateral view of right carotid arteriogram showing large carotid-basilar artery (~---). FIG. 15--Case 5. Antero-posterior view of right carotid arteriogram showing carotid-basilar artery (~---) supplying the superior
cerebellar arteries and the left posterior cerebral artery. Fro. 16--Case 5. Full axial view of right carotid arteriogram showing that the right posterior cerebral artery is supplied from lhe
posterior communicating artery (~-+) and that there is no communication visible between the basilar artery and the right posterior communicating artery. The carotid-basilar artery is clearly seen (~--).
T h e r i g h t p o s t e r i o r c o m m u n i c a t i n g a r t e ry was large . T h e le f t p o s t e r i o r c o m m u n i c a t i n g a r t e r y w as h y p o p l a s t i c a n d t h e c a r o t i d - b a s i l a r a r t e r y s u p p l i e d t he s u p e r i o r c e r e b e l l a r a r t e r i e s a n d p r o b a b l y t h e lef t p o s t e r i o r c e r e b r a l a r t e ry . T h e v e r t e b r a l a r t e r i e s we re e q u a l irt size. T h e r i g h t p o s t e r i o r c e r e b r a l a r t e r y was s u p p l i e d m a i n l y t h r o u g h t h e p o s t e r i o r c o m m u n i c a t i n g a r t e r y a n d i ts p r o x i m a l p a r t , u p to i t s j u n c t i o n w i t h t h e p o s t e r i o r c o m - m u n i c a t i n g a r t e ry , was smal l .
Case 5.--Female, aged fifty-five. Admitted with a three month history of increasingly severe headaches associated with vomiting, and of difficulty in swallowing, loss of weight and depression. Two weeks before admission the patient collapsed, since when she had noticed weakness of her left arm and leg.
On examination she was well orientated but obviously ill. There was diminution of power, impairment of co-ordination and slightly increased tone of the left arm and leg. The left plantar reflex was extensor. No paPilloedema was present.
Ventriculography showed no shift of the septum pellucidum but demonstrated deformity of the posterior part of the right lateral ventricle which was interpreted as an infiltrating parietal space-occupying lesion.
Right carotid arteriogram (Figs. 14, 15 and 16) .~A large carotid basilar artery was shown, supplying both superior cerebellar arteries and the left posterior cerebral artery.' The right posterior cerebral artery appeared to be supplied almost entirely from the right posterior communicating artery, and no communication between the basilar artery and the right posterior communicating artery was established. These features were well illustrated in the full axial view (Fig. 16).
Biopsy through a right parietal burrhole was negative. The patient 's condition steadily deteriorated with signs of
increasing intracranial pressure, and she died ten weeks after admission.
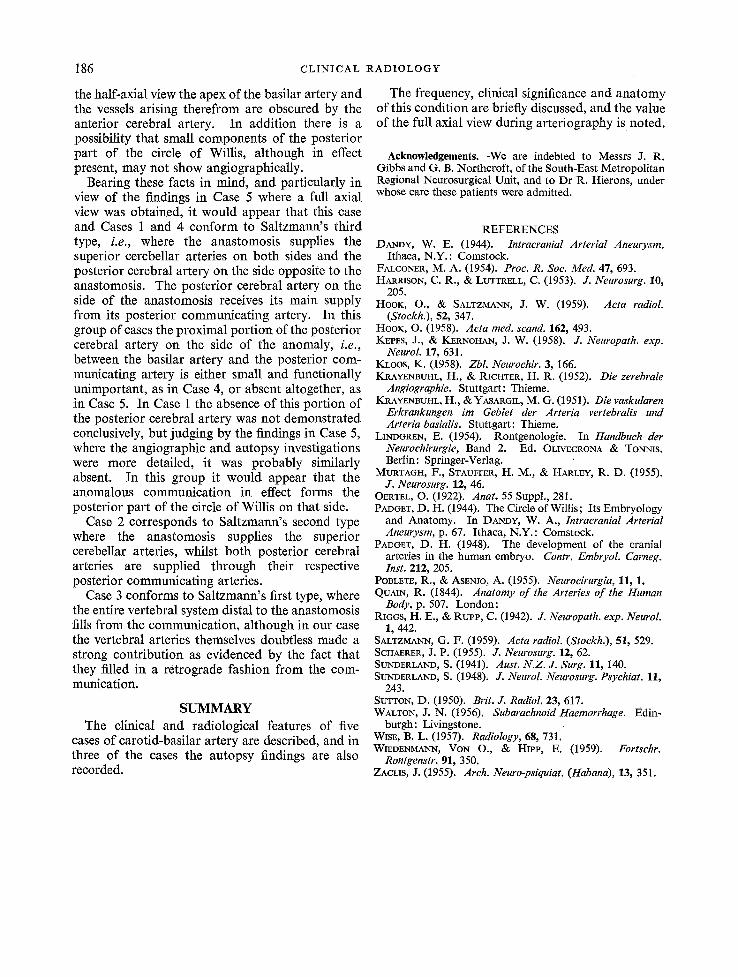
FIG. 17 Case 5. Base of brain at post mortem showing: carotid- basilar artery, 1; small right vertebral artery, 2; large left vertebral artery, 3; right posterior cerebral artery arising directly from the posterior communicating artery, 4; left posterior communicating artery, 5; basilar artery, 6. The proximal part of the right posterior cerebral artery is absent.
Post mortem examination.--The presence of an extensively infiltrating right-sided parasagittal, parietal glioma was confirmed.
The arteries at the base of the brain were dissected out and the carotid-basilar anastomosis identified arising from the
THE CAROTID-BASILAR ARTERY 185
right carotid artery in the cavernous sinus. It passed caudally to perforate the dorsum sellae and join the basilar artery over the clivus. The absence of any communication between the basilar artery and the right posterior com- municating was confirmed, the supply to the right posterior cerebral being entirely through its posterior communicating artery. The right vertebral artery was found to be appreci- ably smaller than the left (Fig. 17).
Comment.--A large right carotid-basilar artery was associated with a parietal parasagittal glioma.
The proximal part of the right posterior cerebral artery was absent, this vessel being supplied entirely through its posterior communicating artery. Presumably the carotid-basilar artery compensated for this " gap " in the posterior portion of the circle of Willis. The basilar artery supplied the posterior fossa and the left posterior cerebral artery. The left posterior communicating artery was small.
DISCUSSION
Frequency.--Our five cases were encountered in the course of approximately 1,500 arteriograms.
This compares with an incidence of 1 in nearly 1,000 arteriograms reported by Sutton (1950), 3 cases in 582 by Harrison and Luttrel (1953), 1 in nearly 600 by Schaerer (1955), 2 in 828 by Poblete (1955) and 9 in 7,382 by Wiedenmann (1959).
As might be expected, the increasing resort to angiography as a means of investigation, and the more widespread recognition of the anomaly, have lead to an increased number of cases being reported and the realisation that, as Sutton (1950) sug- gested, it is by no means excessively rare.
Clinical signifieanee.--It has been suggested, but never proved, that the close relation of the anasto- motic vessel to the Gasserian ganglion and sensory root of the fifth nerve might lead to trigeminal neuralgia. The vessel also passes close to the third, fourth and sixth nerves. There have been no convincing reports however, that the relationship of the abnormal vessel to the cranial nerves may lead to signs and symptoms. Nevertheless know- ledge of its presence may be important when surgical procedures in this region are undertaken.
The possibility that structural defects in the wall of the anastomotic vessel might result in bleeding is suggested by the fact that a number of the recorded cases presented with subarachnoid haemorrhage (Harrison and Luttrel 1953; Kloos 1953; Hook 1958; Saltzman 1959). Not all these patients were submitted to a complete investigation however and some may well have had undetected aneurysms. Certainly the finding of a carotid-basilar artery during the investigation of a patient with sub-
arachnoid bleeding should, as Saltzman (1959) stresses, not deter one from undertaking a complete angiographic investigation.
Our experience and a study of the literature shows that, in almost all cases, the anomaly is an incidental finding in the course of routine angio- graphy and, of our five patients, the first had a metastatic cerebral tumour, the second was angiographically normal apart from the anomalous vessel, the third had an intracerebral haematoma associated with a hemisphere angioma, the fourth presented with subarachnoid haemorrhage from an aneurysm on the posterior communicating artery of the opposite side, artd the fifth case had an extensive infiltrating glioma.
Therefore in none of our five cases was there evidence that the anomaly itself caused any symptoms. However the association of anomalies of the circle of Willis with arterial aneurysm is well recognised (Dandy 1944; Padget 1948; Walton 1956; Hook 1958), and this negative correlation between these anomalies and subarachnoid haemorrhage must be borne in mind.
Anatomy.--The vessel may pursue art extradural course, skirting the sella, as was found at autopsy in Cases 1 and 4, or it may perforate the dorsum sellae as in Case 5. Artgiographically it would appear difficult, if not impossible, to differentiate the two types.
Many authors describe hypoplasia of the vertebral artery on the side of the anomalous vessel and some describe hypoplastic vertebral arteries on both sides, commonly in association with reduction in the calibre of the basilar artery caudal to the anastomotic vessel (Oertel 1922; Altmann 1947; Sunderland 1948; Sutton 1950; Schaerer 1955; Kepes and Kernohan 1958).
Our Cases 1 and 5 showed a narrow vertebral artery on the side of the anastomosis, and in Case 2 the vertebral artery on the relevant side appeared to be absent. However, in the latter case, the possibility that it arose directly from the aortic arch, as has been described by Kepes and Kernohan (1958) cannot be excluded. In Case 4 the vertebral arteries were of equal size, and angiographically in Case 3 also they appeared to be so. It should be borne in mind that there may normally be consider- able variation in the size of the vertebral arteries and that it is common for them to be unequal in size irt the same patient.
It would appear that the presence of the carotid- basilar artery is associated with an anatomical disturbance of the circle of Willis. Angiographically the exact state of affairs is difficult to determine, particularly if a full axial view is not obtained, as in
186 CLINICAL
the half-axial view the apex of the basilar artery and the vessels arising therefrom are obscured by the anterior cerebral artery. In addition there is a possibility that small components of the posterior part o f the circle of Willis, although in effect present, may not show angiographicaUy.
Bearing these facts in mind, and particularly in view of the findings in Case 5 where a full axial view was obtained, it would appear that this case and Cases 1 and 4 conform to Saltzmann's third type, i.e., where the anastomosis supplies the superior cerebellar arteries on both sides and the posterior cerebral ar tery on the side opposite to the anastomosis. The posterior cerebral artery on the side of the anastomosis receives its main supply from its posterior communicating artery. In this group of cases the proximal port ion of the posterior cerebral artery on the side of the anomaly, i.e., between the basilar artery and the posterior com- municating artery is either small and functionally unimportant, as in Case 4, or absent altogether, as in Case 5. In Case 1 the absence of this portion of the posterior cerebral artery was not demonstrated conclusively, but judging by the findings in Case 5, where the angiographic and autopsy investigations were more detailed, it was probably similarly absent. In this group it would appear that the anomalous communication in effect forms the posterior part of the circle of Willis on that side.
Case 2 corresponds to Saltzmann's second type where the anastomosis supplies the superior cerebellar arteries, whilst both posterior cerebral arteries are supplied through their respective posterior communicating arteries.
Case 3 conforms to Saltzmann's first type, where the entire vertebral system distal to the anastomosis fills f rom the communication, although in our case the vertebral arteries themselves doubtless made a strong contribution as evidenced by the fact that they filled in a retrograde fashion from the com- munication.
SUMMARY The clinical and radiological features of five
cases of carotid-basilar artery are described, and in three of the eases the autopsy findings are also recorded.
RADIOLOGY
The frequency, clinical significance and anatomy of this condition are briefly discussed, and the value of the full axial view during arteriography is noted.
Acknowledgements.--We are indebted to Messrs J. R. Gibbs and G. B. Northcroft, of the South-East Metropolitan Regional Neurosurgical Unit, and to Dr R. Hierons, under whose care these patients were admitted.
REFERENCES DANDY, W. E. (1944). Intracranial Arterial Aneurysm.
Ithaca, N.Y. : Comstock. FALCONER, M. A. (1954). Proc. R. Soc. Med. 47, 693. HARRISON, C. R., t~ LUTTRELL, C. (1953). J. Neurosurg. 10,
205. HOOK, O., & SALTZMANN, J. W. (1959). Acta radiol.
(Stockh.), 52, 347. HOOK, O. (1958). Acta med. scand. 162, 493. KEPES, J., & KERNOHAN, J. W. (1958). 9". Neuropath. exp.
Neurol. 17, 631. KLOOS, K. (1958). Zbl. Neurochir. 3, 166. KRAYENBtmL, H., & RICHTER, H. R. (1952). Die zerebrale
Angiographie. Stuttgart: Thieme. KRAYENBUHL, H., & YASARGIL, M. G. (1951). Die vaskularen
Erkrankungen im Gebiet der Arteria vertebral& und Arteria basialis. Stuttgart: Thieme.
LINDGREN, E. (1954). Rontgenologie. In Handbuch der Neurochirurgie, Band 2. Ed. OLIVECRONA & TONNIS. Berlin: Springer-Verlag.
MURTA~rI, F., STAUFFER, H. M., & HARLEY, R. D. (1955). d. Neurosurg. 12, 46.
OERTEL, O. (1922). Anat. 55 Suppl., 281. PAD~ET, D. H. (1944). The Circle of Willis; Its Embryology
and Anatomy. In DANDY, W. A., lntracranial Arterial Aneurysm, p. 67. Ithaca, N.Y.: Comstock.
PAD~ET, D. H. (1948). The development of the cranial arteries in the human embryo. Contr. Embryol. Carneg. Inst. 212, 205.
POBLETE, R., & ASENJO, m. (1955). Neurocirurgia, 11, 1. QUAIN, R. (1844). Anatomy of the Arteries of the Human
Body, p. 507. London: RIGGS, H. E., & RoPP, C. (1942). d. Neuropath. exp. NeuroL
1, 442. SALTZMANN, G. F. (1959). Acta radiol. (Stockh.), 51, 529. SCHAERER, J. P. (1955). J. Neurosurg. 12, 62. StrNDERLAND, S. (1941). Aust. N.Z.J. Surg. 11, 140. SIYNDERLAND, S. (1948). J. NeuroL Neurosurg. Psychiat. I1,
243. SUTTON, D. (1950). Brit. d. Radiol. 23, 617. WALTON, J. N. (1956). Subarachnoid Haemorrhage. Edin-
burgh: Livingstone. WtSE, B. L. (1957). Radiology, 68, 731. WlED~NMANN, VON O., & Hrap, E. (1959). Fortschr.
Rontgenstr. 91, 350. ZACLIS, J. (1955). Arch. Neuro-psiquiat. (Habana), 13, 351.





























