Embed Size (px)
Citation preview

THE CARDIAC AXIS & AXIS DEVIATION(Lecture 2 )
1
Associate Professor Dr. Alexey Podcheko
Spring 2015

INTENDED LEARNING OBJECTIVES:
To know : CARDIAC AXISAXIS DEVIATIONCAUSES OF CARDIAC AXIS
DEVIATION AXIS DETERMINATION ON ECG
2


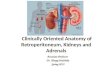
Geometry of the vertical leads
(-30°)
(+90°)(+120°)
(+210°)

“The Cardiac Axis”• Six ECG leads (I, II, III, aVR, aVL, aVF)
examine the flow of depolarization and repolarization in the heart in the frontal plane. In this plane, depolarizing forces of differing magnitudes are moving through the ventricles in many different directions during the normal process of ventricular depolarization.
If we sum together all of the depolarization vectors occurring in the frontal plane throughout the duration of ventricular depolarization, we can generate an overall vector which has a magnitude and direction. 5

• The direction of this total frontal QRS vector, defined by the angle (alpha) it makes with lead I, is the cardiac axis
• In normal circumstances, the direction of the frontal QRS vector is dominated by the depolarization forces generated in the large left ventricular muscle mass.
• The pattern of depolarization of the left ventricle is in turn dictated by the precise anatomy of the intraventricular conducting system.
6
“The Cardiac Axis”

• Shortly after the anatomical bifurcation of the bundle of His into Right and Left Bundle Branches the left bundle branch itself quickly divides into anterior fascicle (the left anterior fascicle-LAF) and a posterior fascicle (the left posterior fascicle-LPF).
• Left anterior fascicle depolarizes the anterior and lateral walls of the left ventricle,
• Left posterior fascicle simultaneously depolarizes the posterior and inferior surfaces of the chamber. 7
“The Cardiac Axis”

In a normal heart these two depolarizing forces (LAF & LPF) are the prime determinant of the cardiac axis.
When added together, the total vector generated is travelling downwards and to the left, more or less straight down lead II at approximately 60 degrees relative to lead I. 8

• There are extensive anastomoses between the LAF and LPF at their termination.
o If one of these major branches is damaged and flow through it blocked, the ventricle can be depolarized by retrograde flow of depolarization from the intact branch via these anastomoses.
o This will have a dramatic effect on the direction of the frontal
QRS vector.9
“The Cardiac Axis”

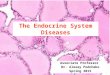
o If disease blocks conduction in the anterior fascicle (LAF) and the lateral and anterior ventricular wall are depolarized by current flowing upwards from the LPF, the cardiac axis is now travelling upwards and to the left (due northeast). This is termed “left axis deviation (or LAD)”.
o With blocked conduction in the posterior fascicle (LPF) the inferior surface is depolarized by current flowing from above and the sum of these two major vectors is now moving downwards and towards the right. This is termed “right axis deviation (or RAD)”. 10
Red Arrow shows direction of the electrical axis of the heart
LAFB - LEFT
LPFB - RIGHT

“Axis Deviation”• Although the cardiac axis lies close to
lead II in many cases, its position demonstrates a wide normal variation. For example,
short fat people tend to have an axis towards the left
while in tall thin individuals the axis tends to be towards the right.
• The normal range lies between +90 degrees, or straight down aVF, to -30 degrees (…0 degree), straight along aVL.
11

• “Left axis deviation”, that is, deviation of the cardiac axis beyond – minus 30 degrees , is characterized by a Strongly Negative QRS complex in lead III combined with an Overall Negative QRS in lead II and a Positive lead I.
The commonest cause of this abnormality is left anterior fascicular block (LAFB).
• With “right axis deviation” – deviation of cardiac axis beyond +90 degrees
The commonest cause of this abnormality is leftposterior fascicular block (LAFB).
12

“Axis Deviation – Causes”• While conduction defects in the left ventricle are
the primary cause of axis deviation on the ECG, we should point out that in some situations other
vectors may come to the fore and shift the axis independent of damage to conduction in this chamber. Some of these are intuitively obvious. For example,
a large Left lateral myocardial infarction, with loss of left-directed depolarization vectors can shift the cardiac axis to the Right.
Equally, a large Right sided infarction can shift the axis to the Left by loss of rightward vectors. 13

“LEFT AXIS DEVIATION: CAUSESLEFT AXIS DEVIATION: CAUSES”• Left Anterior Fascicular BlockLeft Anterior Fascicular Block
* Left anterior descending artery (ischemia/infarction) * LVH (Fibrosis / Ischemia) * Cardiomyopathy
• Loss of vectorsLoss of vectors * Large right sided infarct
• Gain of vectorsGain of vectors * LVH (unusual) 14

“RIGHT AXIS DEVIATION: CAUSESRIGHT AXIS DEVIATION: CAUSES”• Left Posterior Fascicular BlockLeft Posterior Fascicular Block
*Diffuse ischemia/infarction*Cardiomyopathy
• Loss of vectorsLoss of vectors*Left lateral infarction
• Gain of vectorsGain of vectors*RVH (unusual)
Note: There are many other causes of axis deviation…………………………. 15

• Although ventricular hypertrophy in the absence of conduction defects is a potential cause of axis deviation, this is very unusual.
The great majority of patients with left ventricular hypertrophy from whatever cause do Not have LAD on their ECG.
Furthermore, and perhaps surprisingly, the presence or otherwise of LAD in patients with LVH bears No relation to the degree of hypertrophy present.
16

The same is true for right ventricular hypertrophy acquired in adult life.
The majority of adult patients with RVH do Not demonstrate RAD on their ECG.
Remember, axis deviation usually results from conduction defects in the ventricles
axis deviation on an ECG is neither sensitive nor specific in the diagnosis of ventricular hypertrophy.
17

“Axis Determination/Estimation”• Many methods to determine cardiac axis
deviation:General determination of electrical axis using
“Lead I & Lead aVF” methodMore precise “Trigonometry/calculation”
method
18

19
“Lead I & Lead aVF” method

Trigonometry/calculation” method• 1. Find limb lead (I, II, III, aVR, aVL,
aVF) where QRS is most isoelectric (height and depth of R and S waves are close to equal)
• 2. On the frontal axial chart draw the line perpendicular to isoelectric lead, put arrows on the both ends of the line
• 3. Analyze morphology of QRS complex in the leads near the line you just have drawn (in this case -leads II and aVR)
• The electrical axis is pointing in the direction of the lead with positive QRS complex (in this case – lead II)
• Measure angle between lead I and your arrow – this is a value of an electrical axis in this case (in this case is +60degrees)


22
Exercise: Determine electrical axis on the ECG films below

23

24

25