Embed Size (px)
Citation preview
The Endocrine System Diseases
Associate Professor Dr. Alexey Podcheko
Spring 2015
Intended Learning Outcomes
• NON-NEOPLASTIC– HYPER-function– HYPO-function
• NEOPLASTIC– FUNCTIONAL– NON-FUNCTIONAL– Functional endocrine
malignancies are RARE. Why?
1. PITUITARY-ANTERIOR
-POSTERIOR
2. THYROID
3. PARATHYROID
4. PANCREAS (endo.)
5. ADRENAL-CORTEX
-MEDULLA
Types of the signaling by extracellular secreted molecules
• Autocrine- is a form of signaling in which a cell secretes a hormone or chemical messenger (called the autocrine agent) that binds to autocrine receptors on the same cell, leading to changes in the cell (example insulin and beta-cells)
• Paracrine- a form of cell signaling in which the target cell is near the signal-releasing cell (testosterone – being produced by Leydig interstitial cells stimulates spermatogenesis in the adjacent seminiferous tubules)
• Endocrine - secreted molecules, which are frequently called hormones, act on target cells that are distant from their site of synthesis. An endocrine hormone is frequently carried by the blood from its site of release to its target.
• Feedback inhibition – is a secretion by target tissue factors that down-regulate the activity of the gland that produces the stimulating hormone

FEEDBACK SYSTEMS• HYPOTHALAMUS • ANTERIOR PITUITARY • ENDOCRINE GLAND • END ORGAN • HYPOTHALAMUS

Q1: What happened with feedback system if exogenous hormone is added (e.g. Thyroxin)?Q2: What will happened with the gland producing the same hormone (e.g. Thyroid gland/Thyroxin) ?
• A 45-year-old Caucasian female with a several year history of systemic lupus erythematosus being treated with multiple medications is found dead at home. On her most recent physical exam, her blood pressure was 150/90 mm Hg and she was noted to have truncal obesity, mild hirsutism, facial plethora, and proximal muscle weakness. Laboratory studies showed hyperglycemia. At autopsy, she was found to have a left coronary artery mainstem thrombus that caused sudden cardiac death. Evaluation of her adrenal glands will most likely show which of the following?
• A. Diffuse hyperplasia • B. Nodular hyperplasia• C. Bilateral cortical atrophy• D. Unilateral atrophy • E. Adrenocortical adenoma Tophat
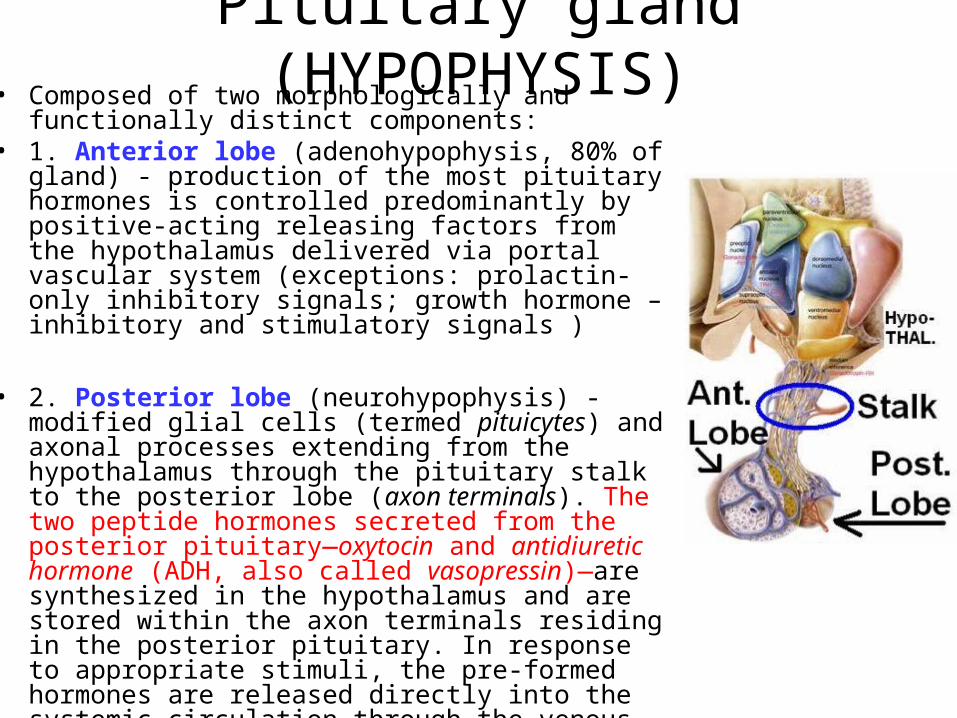
Pituitary gland (HYPOPHYSIS)• Composed of two morphologically and functionally
distinct components: • 1. Anterior lobe (adenohypophysis, 80% of gland) -
production of the most pituitary hormones is controlled predominantly by positive-acting releasing factors from the hypothalamus delivered via portal vascular system (exceptions: prolactin- only inhibitory signals; growth hormone – inhibitory and stimulatory signals )
• 2. Posterior lobe (neurohypophysis) - modified glial cells (termed pituicytes) and axonal processes extending from the hypothalamus through the pituitary stalk to the posterior lobe (axon terminals). The two peptide hormones secreted from the posterior pituitary—oxytocin and antidiuretic hormone (ADH, also called vasopressin)—are synthesized in the hypothalamus and are stored within the axon terminals residing in the posterior pituitary. In response to appropriate stimuli, the pre-formed hormones are released directly into the systemic circulation through the venous channels of the pituitary.
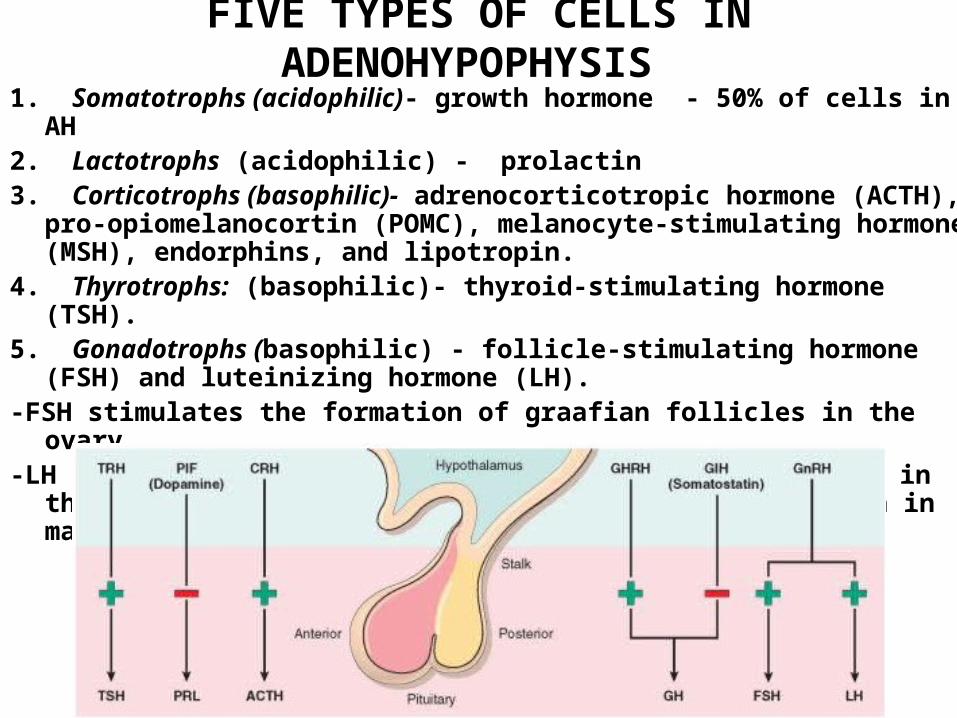
FIVE TYPES OF CELLS IN ADENOHYPOPHYSIS 1. Somatotrophs (acidophilic)- growth hormone - 50% of cells in AH 2. Lactotrophs (acidophilic) - prolactin3. Corticotrophs (basophilic)- adrenocorticotropic hormone (ACTH), pro-
opiomelanocortin (POMC), melanocyte-stimulating hormone (MSH), endorphins, and lipotropin.
4. Thyrotrophs: (basophilic)- thyroid-stimulating hormone (TSH). 5. Gonadotrophs (basophilic) - follicle-stimulating hormone (FSH) and
luteinizing hormone (LH). -FSH stimulates the formation of graafian follicles in the ovary-LH induces ovulation and the formation of corpora lutea in the ovary
(spermatogenesis and testosterone production in males)
• A 16-year-old Caucasian girl who aspires to be a fashion model presents for a routine examination She wishes to modify her diet and exercise plans so that she can lose an additional 20 lbs (9 kg) because she believes she is currently "too fat" to participate in a beauty pageant later this year. She is frustrated that she "cant seem to drop these extra pounds' in spite of strict dietary limitations and vigorous exercise for two hours each day. Her menstrual history is significant for amenorrhea for the past four months. Her height is 5*5" (165 cm) and her weight is 100 lbs (45.3 kg), resulting in a BMI of 16.6 Kg/m2. On physical examination, she is pale and emaciated. Fine hair is noted on her trunk. Which of the following is the most likely mechanism of her amenorrhea?
A. Primary ovarian failureB. Primary pituitary dysfunctionC Hypothyroidism D. Hyperprolactinemia E. Hypothalamic Dysfunction

• Amenorrhea in anorexic patients results from loss of pulsatile GnRH release from the hypothalamus
• There is no pulsatile GnRH release when the level of body fat falls below a certain critical level
• Loss of this cyclic gonadotropin release leads to a decrease in LH and FSH secretion from the pituitary
• Administration of pulsatile GnRH in individuals with anorexia nervosa allows for the normalization of estrogen levels and subsequent ovulation

Normal Pituitary
1. Somatotrophs (acidophilic)2. Lactotrophs (acidophilic) 3. Corticotrophs (basophilic)4. Thyrotrophs: (basophilic)5. Gonadotrophs (basophilic)
Immunostaining for human growth hormone
ACIDOPHILS
BASOPHILS
CHROMOPHOBES
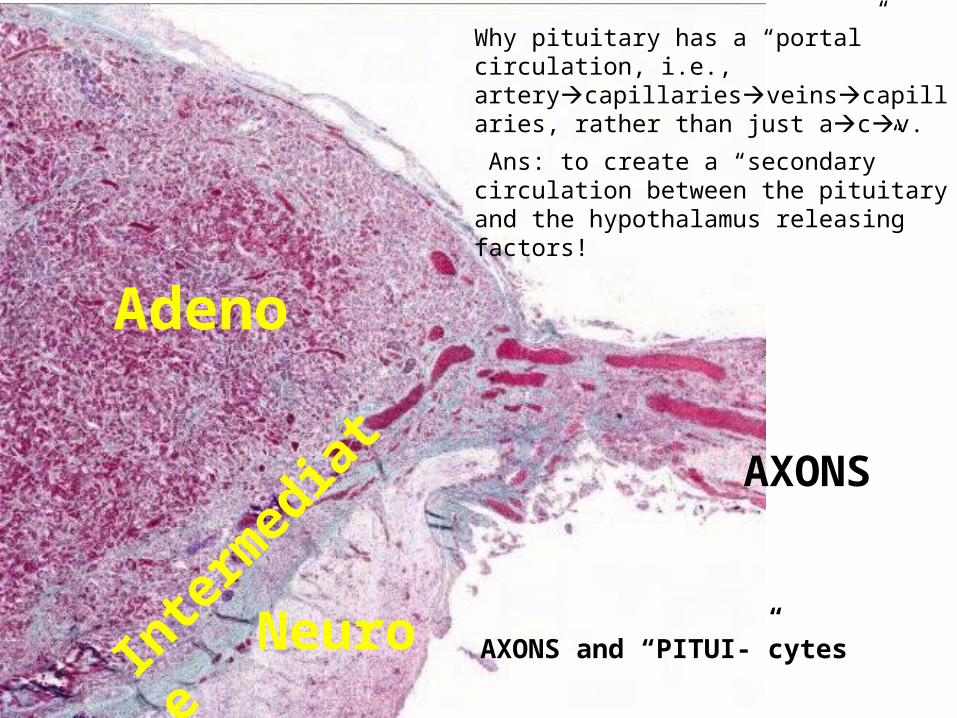
AXONS
AXONS and “PITUI-”cytes
Adeno
Inte
rmed
iate
Neuro
Why pituitary has a “portal” circulation, i.e., arterycapillariesveinscapillaries, rather than just acv.
Ans: to create a “secondary” circulation between the pituitary and the hypothalamus releasing factors!
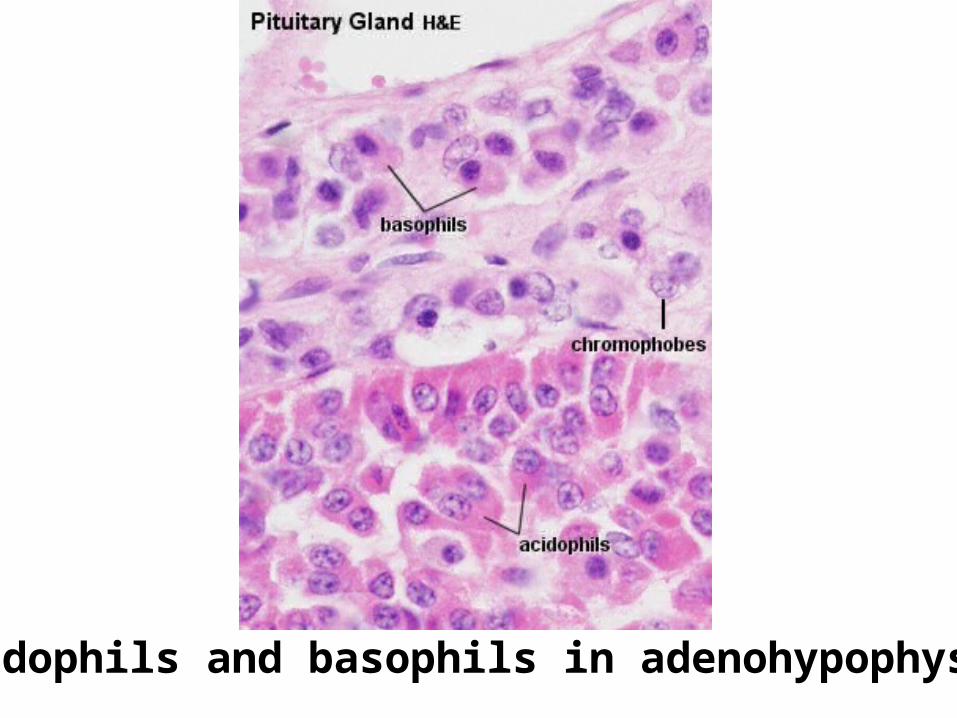
acidophils and basophils in adenohypophysis

ANTERIOR PITUITARY• ACIDOPHILS
–GROWTH HORMONE
–PROLACTIN
• BASOPHILS–TSH
–ACTH
–LH, FSH
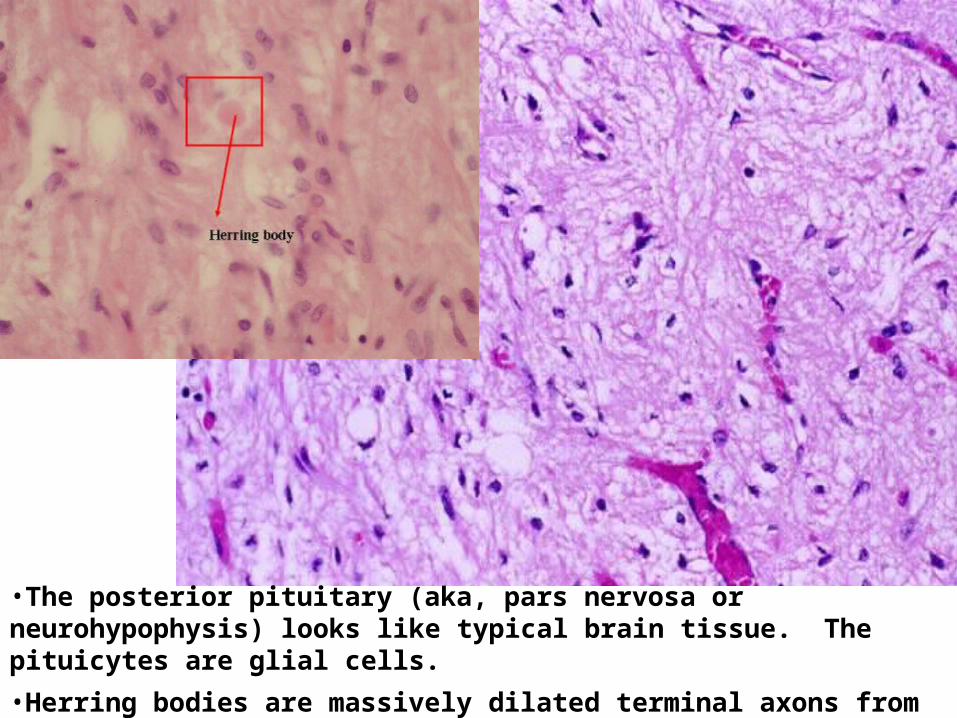
•The posterior pituitary (aka, pars nervosa or neurohypophysis) looks like typical brain tissue. The pituicytes are glial cells.
•Herring bodies are massively dilated terminal axons from the hypothalamus.
POSTERIOR PITUITARY
• OXYTOCIN (contracts uterine smooth muscle)
• VASOPRESSIN (ADH) (vasoconstriction, gluconeogenesis, platelet aggregation, release of Factor-VIII and vWb factor, concentrates urine, main effects on kidney and brain)
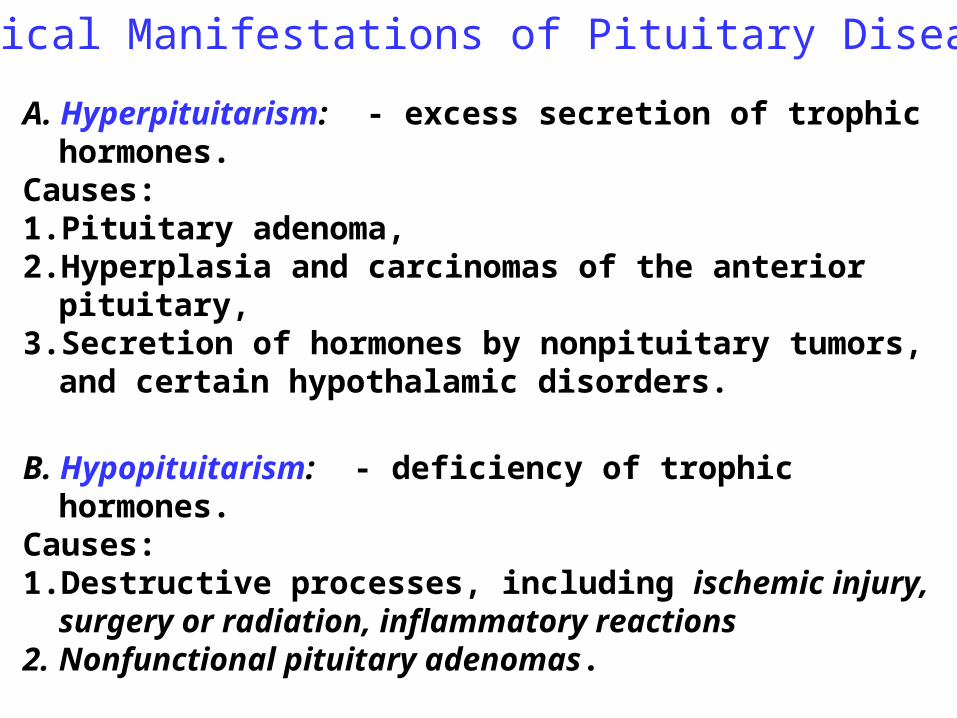
A. Hyperpituitarism: - excess secretion of trophic hormones. Causes: 1. Pituitary adenoma, 2. Hyperplasia and carcinomas of the anterior pituitary, 3. Secretion of hormones by nonpituitary tumors, and certain
hypothalamic disorders.
B. Hypopituitarism: - deficiency of trophic hormones. Causes: 1. Destructive processes, including ischemic injury, surgery
or radiation, inflammatory reactions2. Nonfunctional pituitary adenomas.
C. Local mass effects Causes: pressure of the tumor on the surrounding tissues
:
Clinical Manifestations of Pituitary Disease

Local mass effects1. Radiographic abnormalities of
the sella turcica, including sellar expansion, bony erosion, and disruption of the diaphragma sella.
2. Visual field abnormalities (bitemporal hemianopsia ) - expanding pituitary lesions often compress decussating fibers in the optic
3. Signs and symptoms of elevated intracranial pressure: headache, nausea, and vomiting.
-Pituitary apoplexy - acute hemorrhage into an adenoma
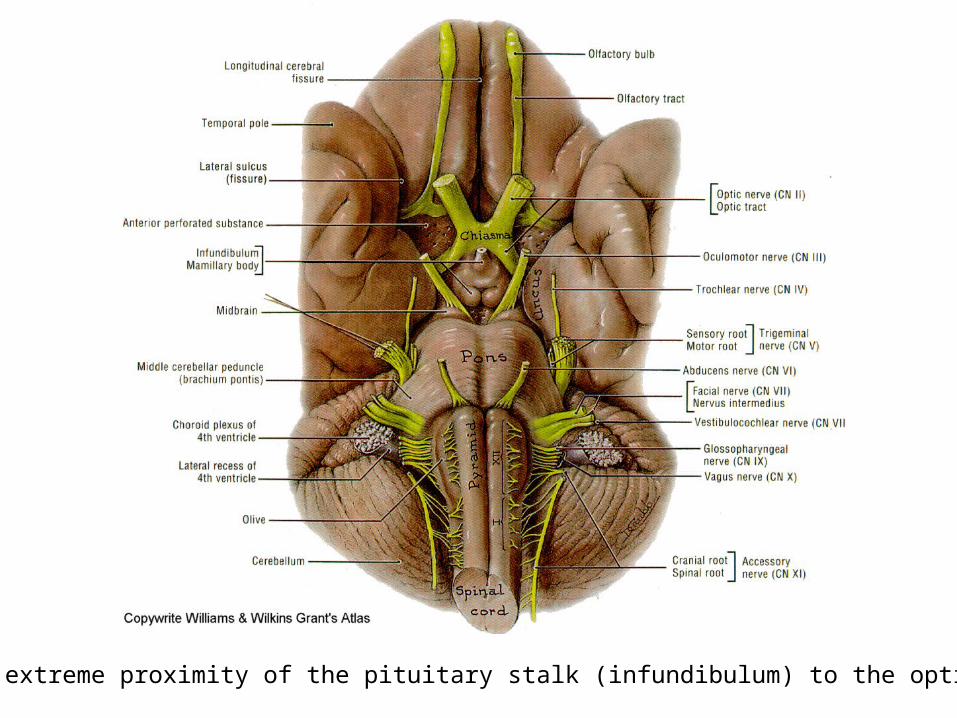
Note the extreme proximity of the pituitary stalk (infundibulum) to the optic chiasm
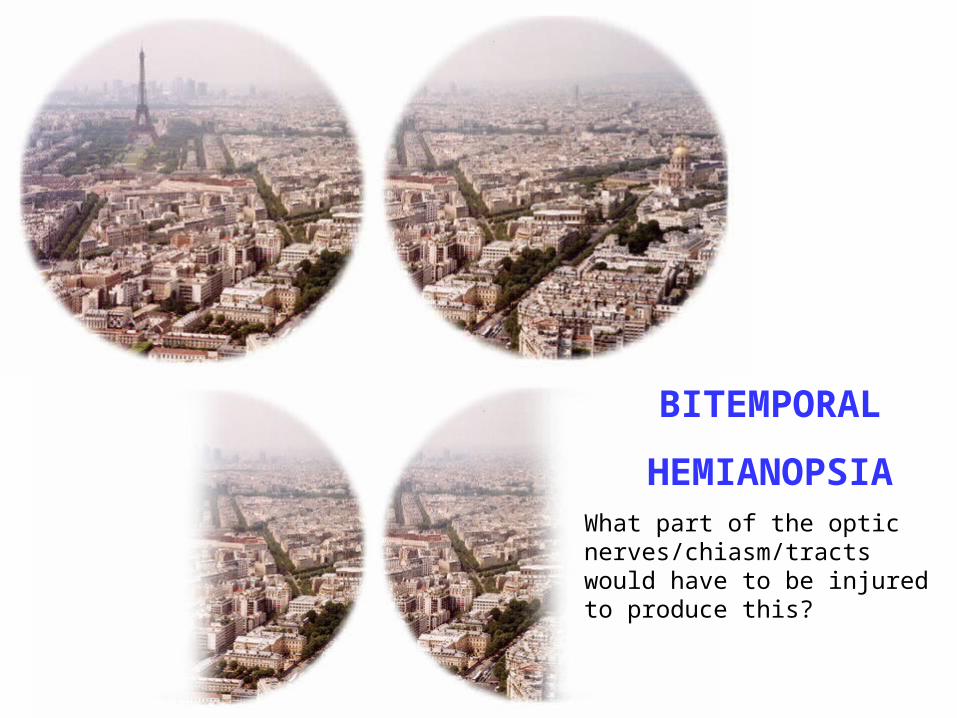
BITEMPORAL
HEMIANOPSIAWhat part of the optic nerves/chiasm/tracts would have to be injured to produce this?
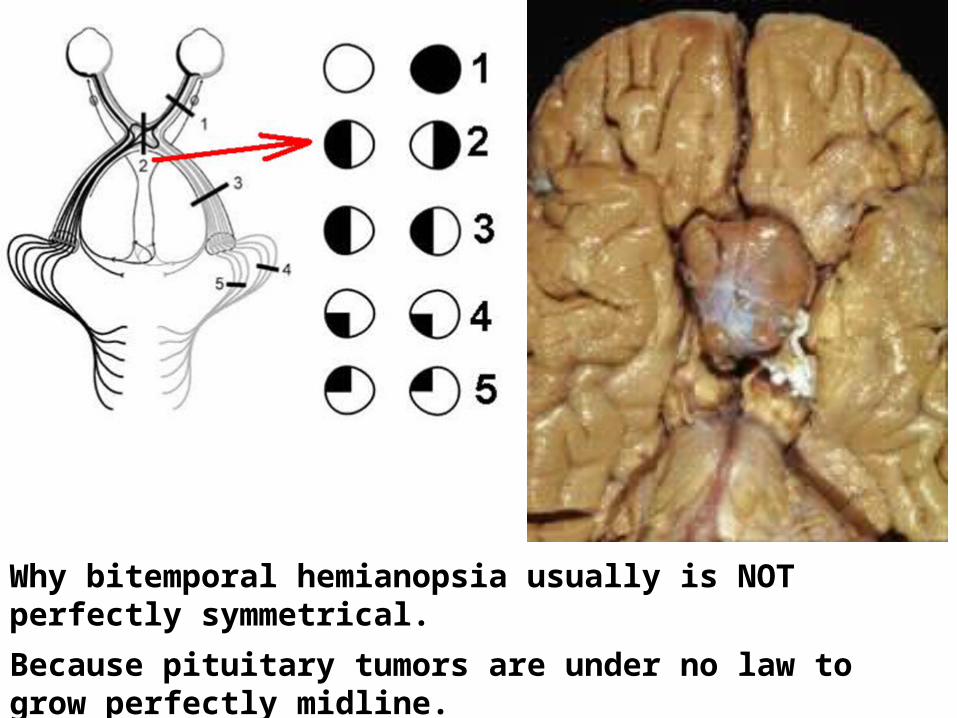
Why bitemporal hemianopsia usually is NOT perfectly symmetrical.
Because pituitary tumors are under no law to grow perfectly midline.

Classification of Pituitary Adenomas
-Adenoma is most common cause of hyperpituitarism-Pituitary adenomas are classified on the basis of hormone(s) produced by the neoplastic cells (see the table)
-Pituitary adenomas are usually found in adults, with a peak incidence from 35 to 60 years of age.
-Some pituitary adenomas can secrete two hormones (GH and prolactin being the most common combination)-Functional adenoma (with hormone excess) or nonfunctioning (without clinical symptoms of hormone excess). -Microadenomas if less than 1 cm in diameter -Macroadenomas if they exceed 1 cm in diameter-Population prevalence of pituitary adenomas is about 14% and they are incidentally diagnosed microadenomas (“pituitary incidentaloma”).
Pituitary Adenomas and Hyperpituitarism
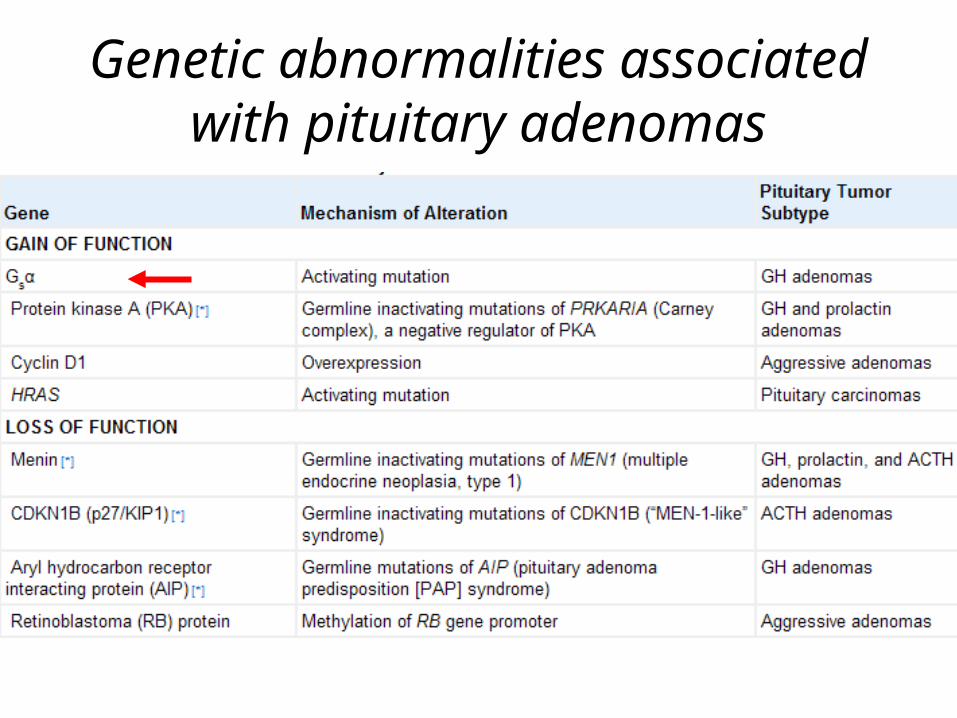
Genetic abnormalities associated with pituitary adenomas

G-protein mutations and pituitary adenomas
• Composed of a specific α-subunit that binds guanine nucleotide and interacts with both cell surface receptors and intracellular effectors, β- and γ-subunits are noncovalently bound to the specific α-subunit.
• On interaction with the ligand-bound cell surface receptor, GDP dissociates, and guanosine triphosphate (GTP) binds to Gsα, activating the G protein. The activation of Gsα results in the generation of cAMP, which acts as a potent mitogenic stimulus
• A mutation in the α-subunit that interferes with its intrinsic GTPase activity will result in constitutive activation of Gsα, persistent generation of cAMP, and unchecked cellular proliferation
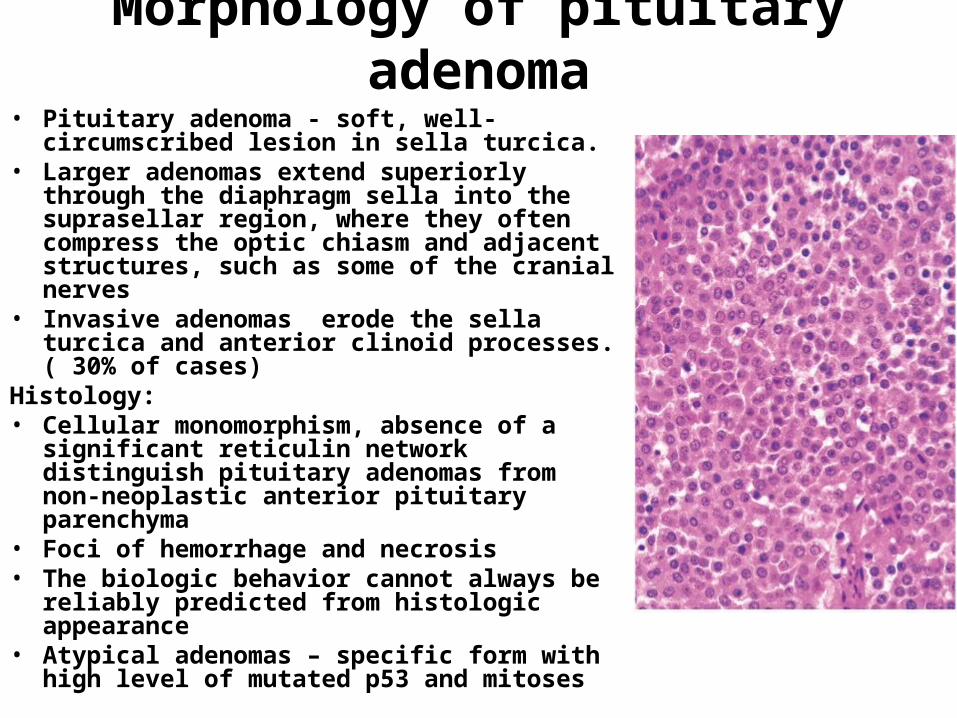
Morphology of pituitary adenoma• Pituitary adenoma - soft, well-circumscribed
lesion in sella turcica. • Larger adenomas extend superiorly through
the diaphragm sella into the suprasellar region, where they often compress the optic chiasm and adjacent structures, such as some of the cranial nerves
• Invasive adenomas erode the sella turcica and anterior clinoid processes. ( 30% of cases)
Histology: • Cellular monomorphism, absence of a
significant reticulin network distinguish pituitary adenomas from non-neoplastic anterior pituitary parenchyma
• Foci of hemorrhage and necrosis • The biologic behavior cannot always be
reliably predicted from histologic appearance• Atypical adenomas – specific form with high
level of mutated p53 and mitoses

Pituitary adenoma. This massive, nonfunctional adenoma has grown far beyond the confines of the sella turcica and has distorted the overlying brain. Nonfunctional adenomas tend to be larger at the time of diagnosis than those that secrete a hormone.

Mechanisms of prolactin secretion
• Stimulate prolactin production:-Thyrotropin releasing hormone-Serotonin-antipsychotics-Tricyclic antidepressants-MAO inhibitors-hypothalamic and pituitary tumors• Inhibit prolactin production:-Dopamin-Bromcriptine (parlodel)
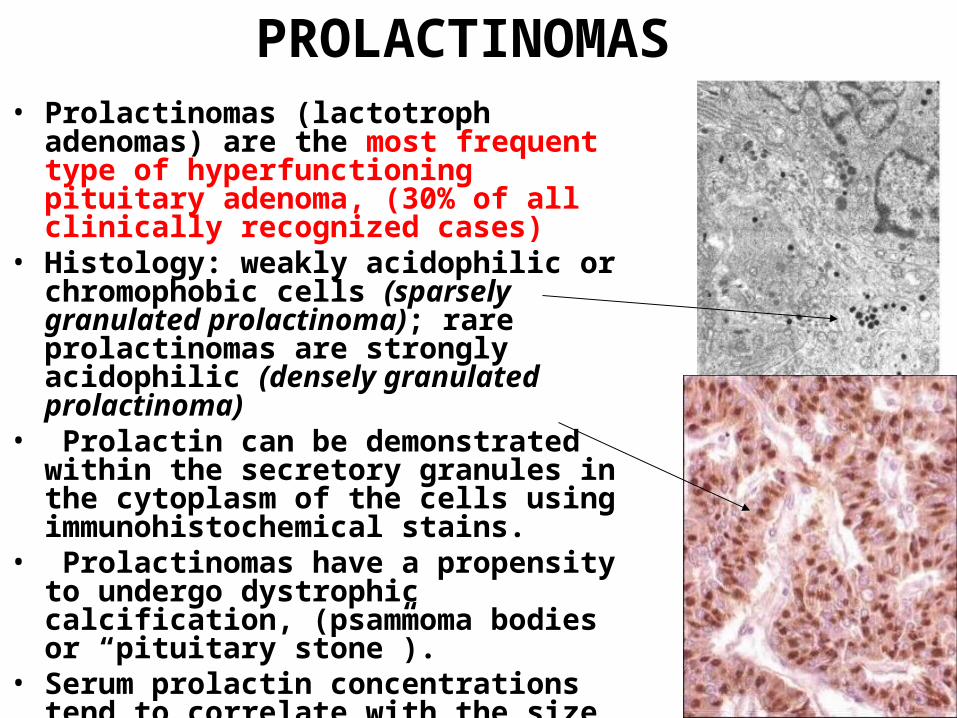
PROLACTINOMAS • Prolactinomas (lactotroph adenomas)
are the most frequent type of hyperfunctioning pituitary adenoma, (30% of all clinically recognized cases)
• Histology: weakly acidophilic or chromophobic cells (sparsely granulated prolactinoma); rare prolactinomas are strongly acidophilic (densely granulated prolactinoma)
• Prolactin can be demonstrated within the secretory granules in the cytoplasm of the cells using immunohistochemical stains.
• Prolactinomas have a propensity to undergo dystrophic calcification, (psammoma bodies or “pituitary stone”).
• Serum prolactin concentrations tend to correlate with the size of the adenoma.
Prolactinoma, Clinic• Hyperprolactinemia cause
amenorrhea, galactorrhea, loss of libido, and infertility.
• Prolactinoma underlies 25% of cases of amenorrhea.
• In men and older women, the hormonal manifestations may be subtle, allowing the tumors to reach considerable size
• Prolactinomas are treated by surgery (transsphenoidal operation ) or, more commonly, with bromocriptine, a dopamine receptor agonist that causes the lesions to diminish in size.
G
A
L
A
C
T
O
R
R
H
E
A
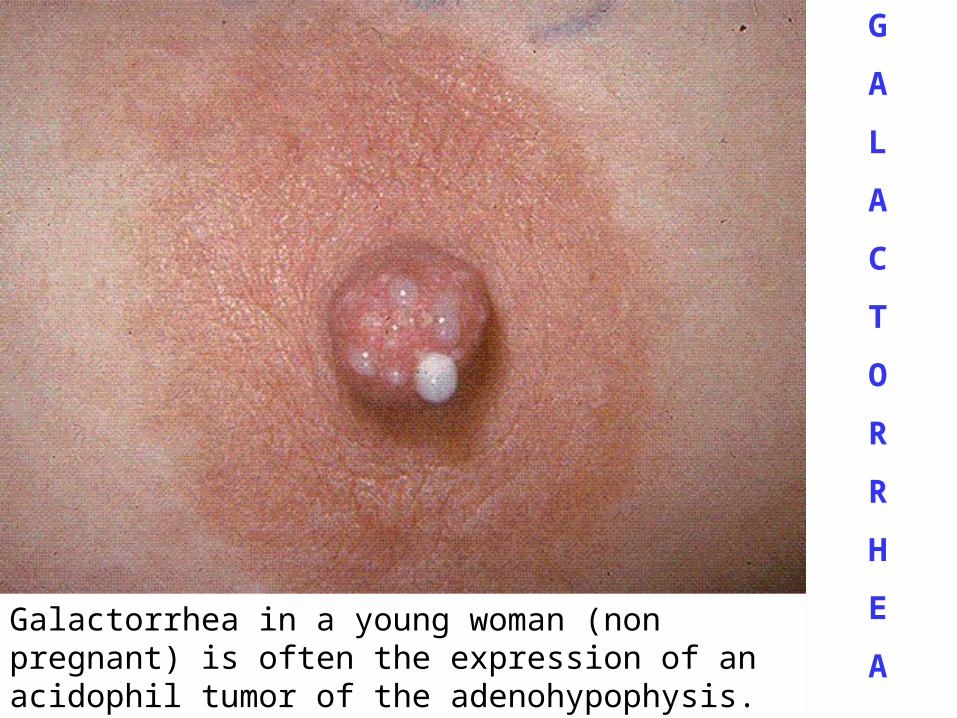
Galactorrhea in a young woman (non pregnant) is often the expression of an acidophil tumor of the adenohypophysis.
Other reasons for hyperprolactinemia:Physiologic hyperprolactinemia: 1. pregnancy2. during breastfeeding in lactating women3. response to many types of stress. Pathologic hyperprolactinemia (Lack of dopamine inhibition of
prolactin secretion) :1. Damage to the dopaminergic neurons of the hypothalamus2. Damage to the pituitary stalk (e.g., due to head trauma or
any tumour in the suprasellar compartment )3. Drugs (such as dopamine antagonists), estrogens4. Renal failure5. Hypothyroidism
• A 32-year-old Caucasian male comes to your office complaining of visual problems. He has had several “near-misses” in his car lately, being nearly hit by cars coming from both the right and the left. He also admits to having headaches that respond to acetaminophen. Which of the following hormones is most likely elevated in this patient?
• A. Growth hormone • B. Adrenocortical-stimulating hormone • C. Thyroid-stimulating hormone • D. Prolactin • E. Follicle-stimulating hormone
tophat

GROWTH HORMONE CELL (SOMATOTROPH) ADENOMAS
• Manifestations of excessive GH may be subtle for prolonged period of time
• Histology: densely granulated and sparsely granulated acidophilic or chromophobe cells
• Some adenomas are bihormonal ( GH and prolactin) • Clinical features: Gigantism or Acromegaly• Mechanism : Persistently elevated levels of GH stimulate the
hepatic secretion of insulin-like growth factor 1 (IGF-1 or somatomedin C)
• If adenoma appears before the epiphyses have closed, the elevated levels of GH (and IGF-1) -result in gigantism -increase in body size with disproportionately long arms and legs.
• If adenoma appears after closure of the epiphyses - acromegaly.

GIGANTISM
(excess somatotropin [GH]
BEFORE
epiphyseal
closure)

ACROMEGALY:
(excess somatotropin
[GH] AFTER epiphyseal closure)

GROWTH HORMONE CELL (SOMATOTROPH) ADENOMAS
• Other symptoms: -hyperostosis, -prognathism, -gonadal dysfunction, -diabetes mellitus, -generalized muscle weakness,-hypertension, -arthritis, -congestive heart failure, -increased risk of gastrointestinal cancers.
GROWTH HORMONE CELL (SOMATOTROPH) ADENOMAS
• Lab Diagnosis: Failure to suppress GH production in response to an oral load of glucose is one of the most sensitive tests for acromegaly.
• Treatment: The underlying pituitary adenoma can be either removed surgically or treated via pharmacologic means (somatostatin analogs or the use of GH receptor antagonists)
• Prognosis: When effective control of high GH levels is achieved, the characteristic tissue overgrowth and related symptoms gradually recede, and the metabolic abnormalities improve.
• Most common cause of death in patients with acromegaly is CHF - (up to 70% of cases)
ACTH CELL (CORTICOTROPH) ADENOMAS
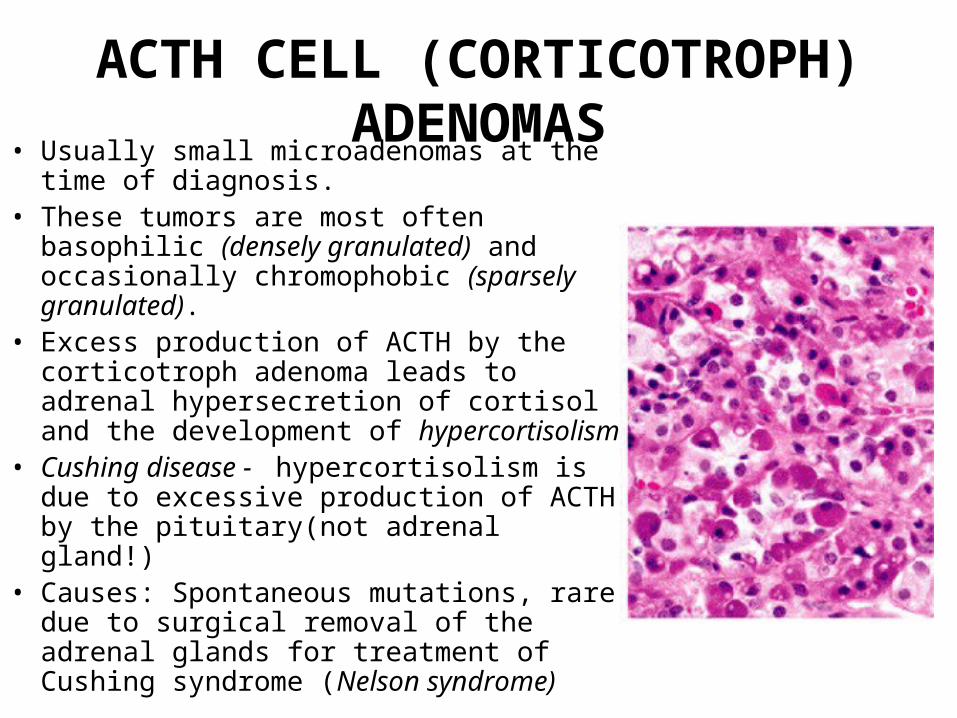
• Usually small microadenomas at the time of diagnosis.
• These tumors are most often basophilic (densely granulated) and occasionally chromophobic (sparsely granulated).
• Excess production of ACTH by the corticotroph adenoma leads to adrenal hypersecretion of cortisol and the development of hypercortisolism
• Cushing disease - hypercortisolism is due to excessive production of ACTH by the pituitary(not adrenal gland!)
• Causes: Spontaneous mutations, rare due to surgical removal of the adrenal glands for treatment of Cushing syndrome (Nelson syndrome)
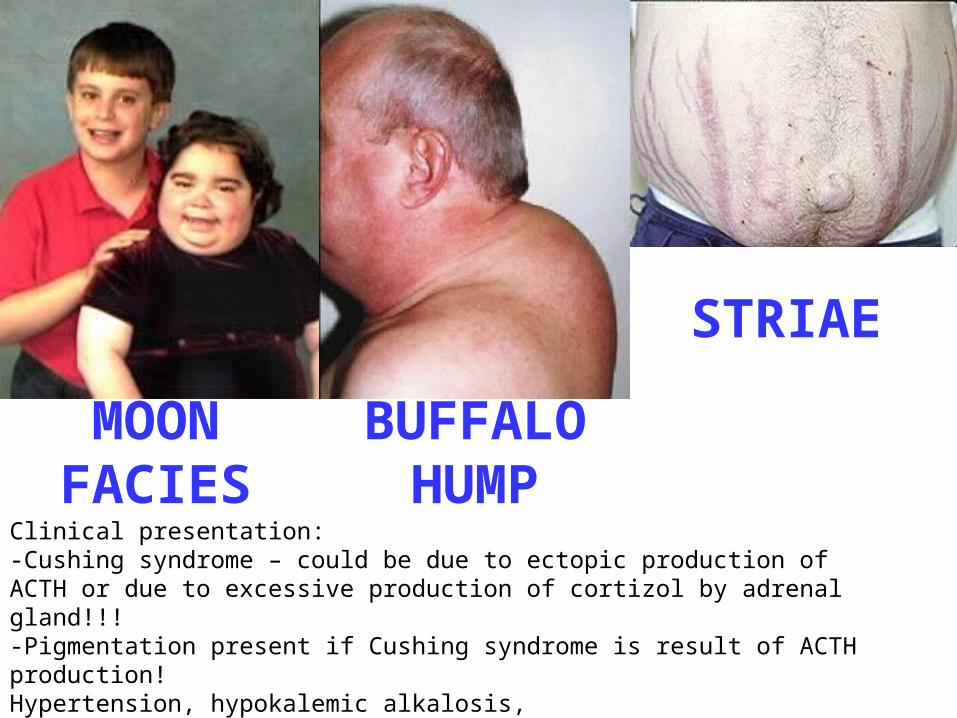
MOON FACIES
BUFFALO HUMP
STRIAE
Clinical presentation: -Cushing syndrome – could be due to ectopic production of ACTH or due to excessive production of cortizol by adrenal gland!!!-Pigmentation present if Cushing syndrome is result of ACTH production!Hypertension, hypokalemic alkalosis, For diagnosis – Dexamethasone suppression test (high dose suppression test +ve for pituitary tumors and negative for ectopic ACTH tumors!!!!)

Nelson syndrome• Surgical removal of the adrenal
glands for treatment of Cushing syndrome induces loss of the inhibitory effect of adrenal corticosteroids on a preexisting corticotroph microadenoma and this lead to progressive growth of hypophyseal tumor
• Symptoms: -No signs of hypercortisolism, but
hypocortisolism. -Singns of “mass effects” in
Hypophysis-Hyperpigmentation because of the
stimulatory effect of other products of the ACTH precursor molecule on melanocytes.
OTHER ANTERIOR PITUITARY ADENOMAS
• Gonadotroph (LH-producing and FSH-producing) adenomas:
• Symptoms: impaired vision, headaches, diplopia, impaired secretion of LH - decreased energy and libido in men (due to reduced testosterone) and amenorrhea in premenopausal women.
• Thyrotroph (TSH-producing) adenomas are rare, accounting for approximately 1% of all pituitary adenomas. Thyrotroph adenomas are a rare cause of hyperthyroidism.
• Nonfunctioning pituitary adenomas - 25% to 30% of all pituitary tumors. (aka silent variants or null-cell adenomas).
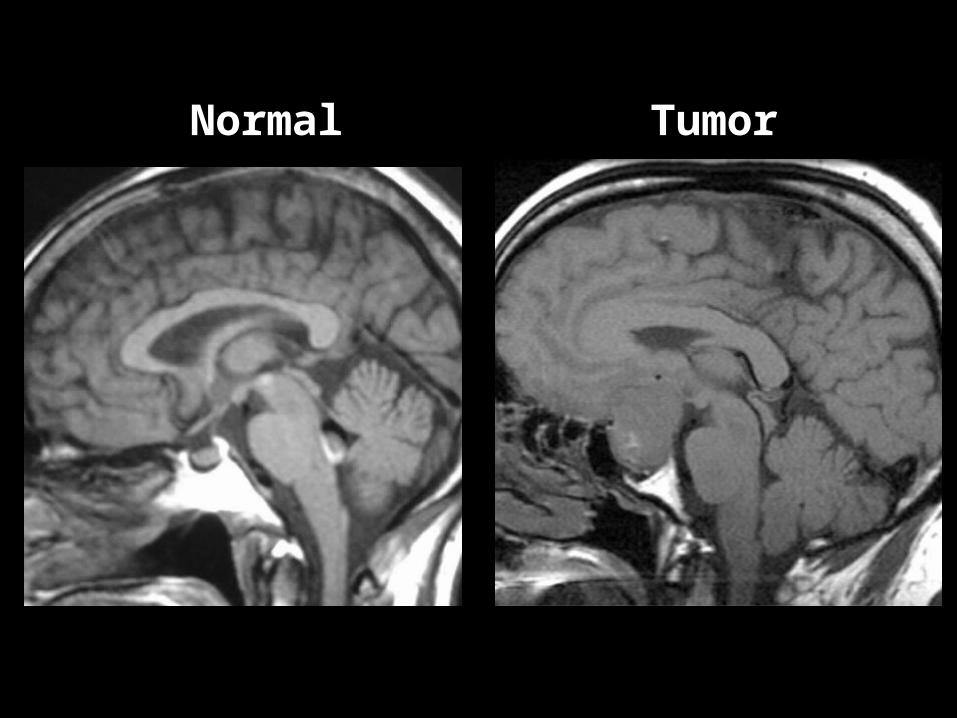
Normal Tumor
Hypopituitarism, Definitions
• Definition: Decreased secretion of pituitary hormones, which results from diseases of the hypothalamus or of the pituitary.
• Hypofunction of the anterior pituitary : congenital or the result of a variety of acquired abnormalities that are intrinsic to the pituitary.
• Hypofunction of the posterior pituitary: diabetes insipidus is almost always of hypothalamic origin.
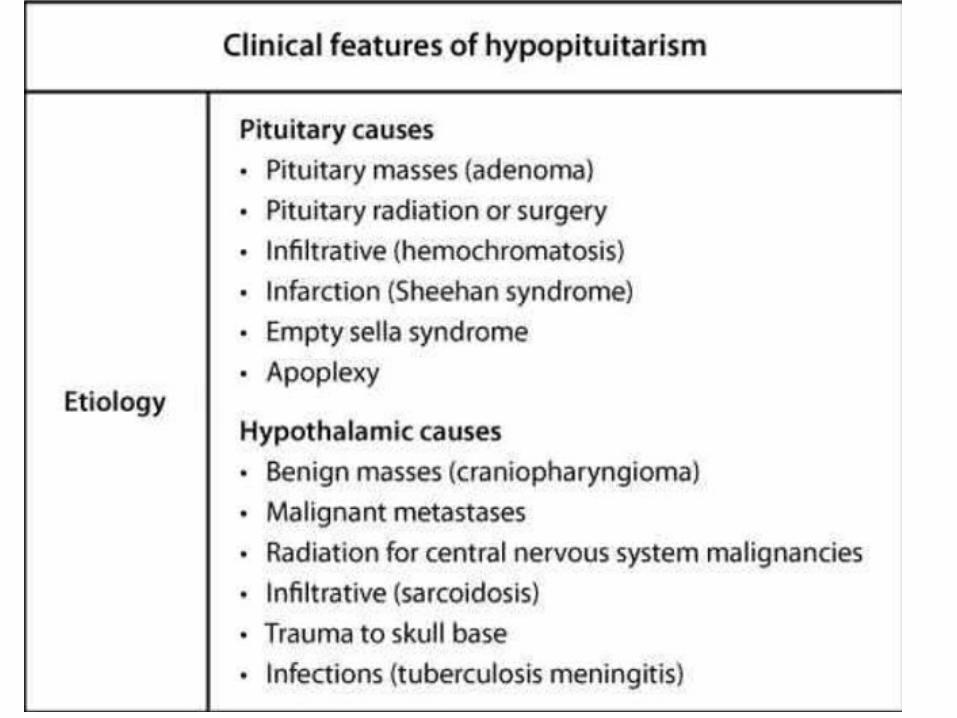

Causes of pituitary hypofunction • Traumatic brain injury and subarachnoid hemorrhage• Tumors and other mass lesions ( Pituitary adenomas, other
benign tumors arising within the sella, primary and metastatic malignancies, and cysts )
• Pituitary surgery or radiation: Surgical excision, radiation of the pituitary,
• Pituitary apoplexy ( sudden hemorrhage into the pituitary gland)• (sudden onset of excruciating headache, diplopia due to
pressure on the oculomotor nerves, cardiovascular collapse, loss of consciousness, sudden death).
• Sheehan syndrome (postpartum necrosis of the anterior pituitary) - the most common form of clinically significant ischemic necrosis of the anterior pituitary.
• Rathke cleft cyst: can expand and press on the the normal gland.
• Genetic defects (PIT1 gene mutations)• Hypothalamic lesions: tumors, infections
Empty sella syndrome
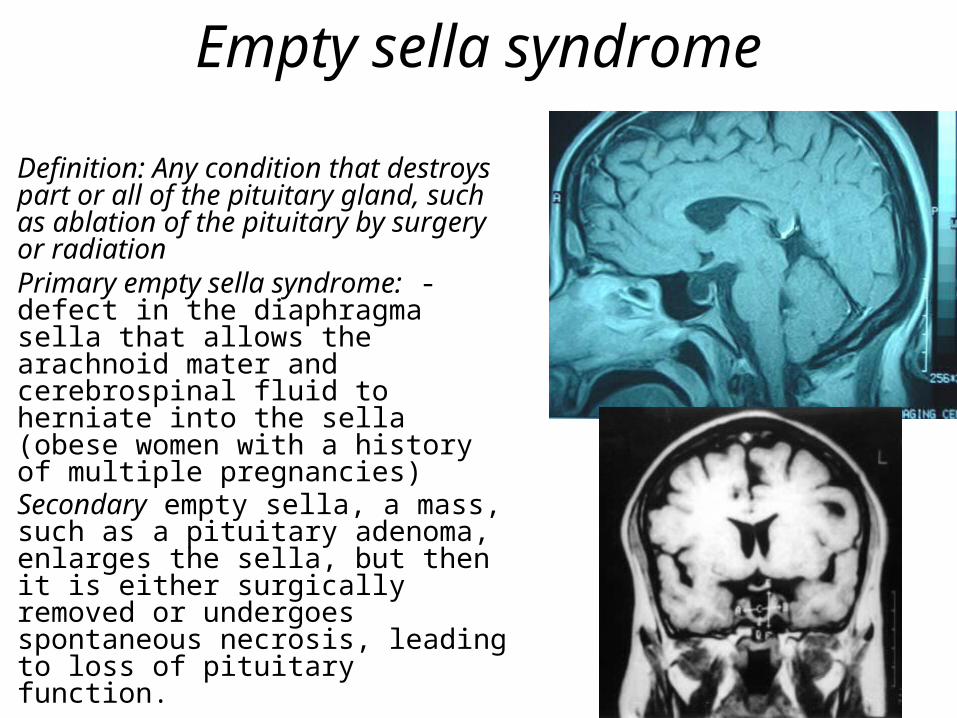
• Definition: Any condition that destroys part or all of the pituitary gland, such as ablation of the pituitary by surgery or radiation
• Primary empty sella syndrome: - defect in the diaphragma sella that allows the arachnoid mater and cerebrospinal fluid to herniate into the sella (obese women with a history of multiple pregnancies)
• Secondary empty sella, a mass, such as a pituitary adenoma, enlarges the sella, but then it is either surgically removed or undergoes spontaneous necrosis, leading to loss of pituitary function.
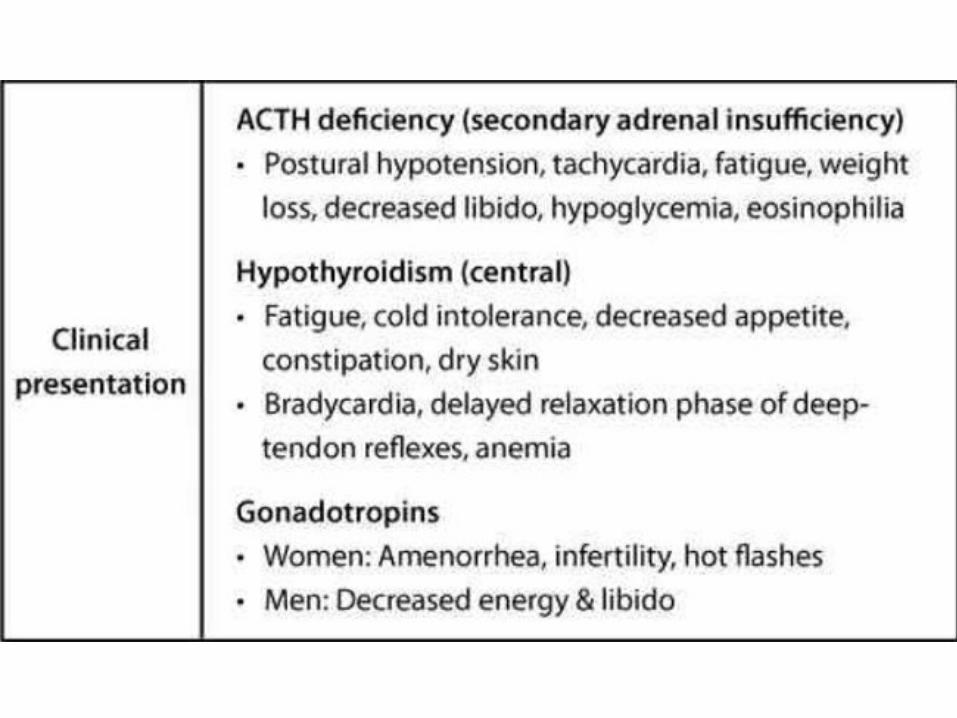
• A 24-year-old Caucasian female presents to your office two weeks after delivery. She is concerned because she has not yet lactated. She says that she knew she would lose weight and be tired after the baby was born, but she complains of excessive fatigue and has had significant weight loss. Thorough evaluation of this patient reveals decreased serum T4 level and decreased 24-hour urine cortisol excretion. Which of the following pathologic processes is most likely responsible for this patient’s symptoms?
• A. Inflammation • B. Apoplexy • C. Ischemic necrosis • D. Non-malignant infiltration • E. Malignant infiltration
tophat
• Explanation:• Classical description of Sheehan’s syndrome • High estrogen levels during pregnancy stimulate
growth of the pituitary, causing it to both enlarge and become more vascular.
• If significant hypotension occurs while the pituitary is still enlarged (the most common cause is postpartum hemorrhage) ischemic necrosis of the pituitary occurs.
• A deficiency of multiple pituitary hormones (panhypopituitarism) follows this ischemia.
• Prolactin deficiency is one sequelae of the necrosis, which has important symptomatic and diagnostic significance.
• Patients suffering from Sheehan syndrome also commonly have hypothyroidism and hypocortisolism.

POSTERIOR PITUITARY Diseases
• DIABETES INSIPIDUS – ADH deficiency
• SIADH (Syndrome of Inappropriate Andi- Diuretic Hormone) – ADH excess
Diabetes insipidus
Definition: condition characterized by excessive urination (polyuria) due to an inability of the kidney to resorb water properly from the urine.
Causes: 1. Head trauma2. Cerebral tumors3. Inflammatory disorders of the hypothalamus and pituitary4. Surgical procedures on hypothalamus and pituitary5. not known
Types of Diabetes Insipidus:1. Central - ADH deficiency2. Nephrogenic diabetes insipidus ( renal tubular unresponsiveness to
circulating ADH)Clinic: Polyuria with an inappropriately low specific gravity and osmolality.
Serum sodium and osmolality are increased as a result of excessive renal loss of free water, resulting in thirst and polydipsia.
•Primary (Psychogenic) polydypsia - - low plasma and low urine osmolality
• A 34-year-old man comes to the physician with a 2-month history of excessive thirst and frequent urination. His past medical history is significant for a prolonged intensive care unit stay due to complications following a motorcycle accident. He takes no medications and has no known drug allergies. Physical examination, including a complete neurologic examination, is unremarkable. Laboratory evaluation shows a fasting blood glucose level of 90 mg/dL. His urinary osmolality after 2-hours of water restriction is 250 mOsm/L, but it increases to 700 mOsm/L after an injection of antidiuretic hormone. The patient is started on the appropriate therapy with improvement of his symptoms. He follows up regularly with his physician over the next several years, but his condition never resolves. Dysfunction of which of the following structures is most likely responsible for this patient's persistent condition?
• A. Posterior Hypophysis • B. Anterior Hypophysis • C. Kidneys • D. Thalamic nuclei • E. Hypothalamic nuclei
Inappropriate ADHSyndrome of inappropriate ADH (SIADH) secretion.• Pathogenesis: ADH excess causes resorption of
excessive amounts of free water, resulting in hyponatremia• Causes: • 1. secretion of ectopic ADH by malignant neoplasms
(small-cell carcinomas of the lung) • 2. drugs that increase ADH secretion (antidepressants,
chemo)• 3. infections and trauma• The clinical manifestations of SIADH are dominated by
hyponatremia, cerebral edema, and resultant neurologic dysfunction.
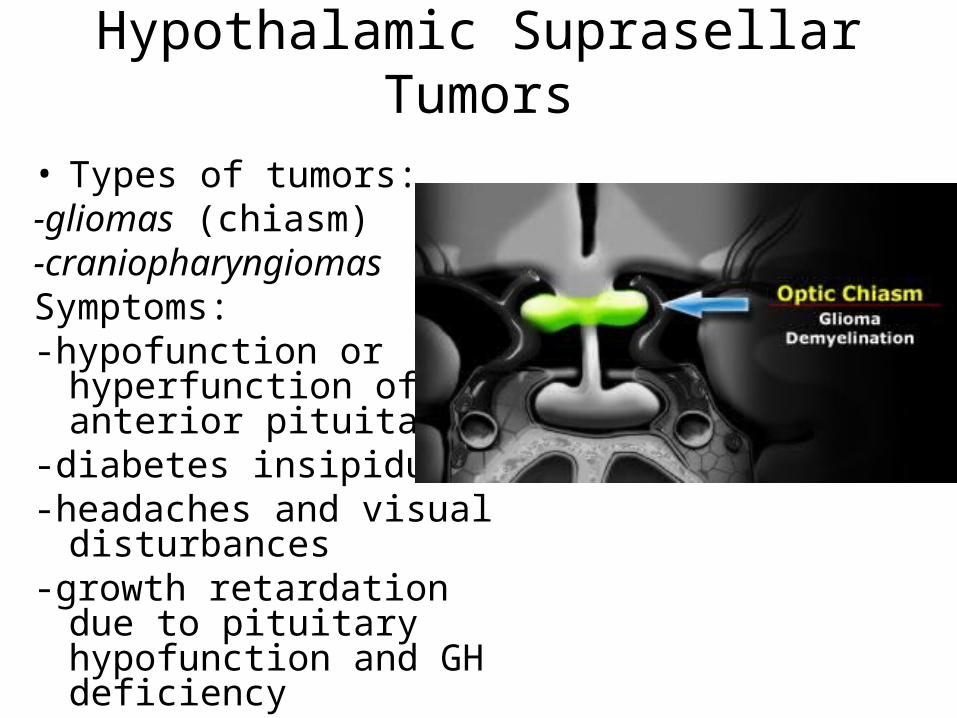
Hypothalamic Suprasellar Tumors
• Types of tumors: -gliomas (chiasm)-craniopharyngiomasSymptoms: -hypofunction or
hyperfunction of the anterior pituitary
-diabetes insipidus-headaches and visual
disturbances-growth retardation due to
pituitary hypofunction and GH deficiency

Morphology of Suprasellar Tumors• -Craniopharyngiomas average 3 to 4 cm in diameter• Three components: 1. solid, comprised of the actual
tumor cells; 2. cystic, filled with "machinery oil" liquid, 3. calcified component
Adamantinomatous craniopharyngioma “Palisading” epithelium+ “wet keratin”s tumor. The cysts contain a “machine oil.”
Papillary craniopharyngiomas
Craniopharyngiomas• Craniopharyngiomas are usually tumors of childhood,
being most frequently discovered between the ages of 5 and 10 years of age.
• Arising from remnants of Rathke's pouch (out-pouching of the pharyngeal roof)
• During the time of pituitary development, remnants of Rathke's pouch cells can remain in the diencephalon (the posterior region of the forebrain).
• Craniopharyngioma symptoms include headaches, visual field defects, and hypopituitarism, evidenced by the growth retardation of this child.
• Compression of the pituitary stalk by craniopharyngioma leads to hyperprolactinemia by loss of dopaminergic inhibition
• A 7-year-old boy is being evaluated for growth retardation. Brain MRI shows a 4 cm multiloculated, cystic, suprasellar lesion, which is bulging into the floor of the third ventricle and base of the brain. Calcifications are present. From which of the following structures is this mass most likely derived?
• A. Prolactin secreting cells of the anterior pituitary • B. Remnants of the Rathke pouch • C. Astrocytes • D. Arachnoid cap cells • E. Posterior pituitary cells
Craniopharyngiomas, prognosis
• Patients with craniopharyngiomas, especially those < 5 cm in diameter, have an excellent recurrence free and overall survival.
• >5 cm tumors are more invasive but this does not impact on the prognosis.
• Malignant transformation of craniopharyngiomas into squamous carcinomas is exceptionally rare and usually occurs after irradiation.