Embed Size (px)
Citation preview

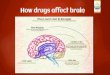
The Brain & Drugs
Including the actions of Cocaine, Opiates, and Marijuana

Objectives
1. Understand the basic geography of the brain and its relationship to function.
2. Know the anatomy and function of the neuron. 3. Understand the chemical synapse including the basic
mechanism of nervous communication. 4. Know the function, components and location of the
reward pathway. 5. Understand the signs and symptoms of use and the
mechanism of action of cocaine, opiates and THC. 6. Apply knowledge to a case study.


Case Study – Part 1a • Parents of a 33 year old man called 911 after finding their son
lying unresponsive on the floor of the basement • The parents report he is a drug addict and may have used
earlier • Paramedics arrive and get the following vital signs:
– BP: 124/80 – Pulse: 104 – Respirations: 10, shallow – Pupils: constricted and non‐reactive – Skin: cool and cyanotic (blue) – Glucose: 55 mg/dL
• Are these vital signs normal? • Are there any other questions you would ask or observations
you should make before you take the patient to the hospital?

Case Study – Part 1b • BP: 124/80 – prehypertensive but not an emergency • Pulse: 104 – slightly tachycardic • Respirations: 10, shallow – hypoventilating • Pupils: constricted and non‐reactive ‐ abnormal • Skin: cool and cyanotic (blue) ‐ abnormal • Glucose: 55mg/dL – hypoglycemic
– We did not cover this, but 70‐180 for non‐fasting glucose is normal
• There are many possible questions or observations but you should be trying to figure out what he took. Do the parents know? Is there any of it lying around the room?
• There is a tourniquet and a needle in the room.

The Brain • The brain is the center of the
nervous system • Cells in the brain are grouped into
neurons and glia – Neurons are the functional units – Glia is a term for a broad class of
supporting cells
• The lobes of the brain: Frontal, Parietal, Occipital, and Temporal
• Neurons are connected by synapses which allow them to communicate with each other

The Neuron • Dendrites and soma (cell
body) receive chemical information from neighboring neuronal axons
• The chemical information is converted to electrical currents which travel toward and converge on the soma
• A major impulse is produced (the action potential) and travels down the axon toward the terminal.

The Synapse and Synaptic Neurotransmission
• The action potential traveling down the axon starts a series of events at the terminal that results in vesicles containing a neurotransmitter, such as dopamine (the stars), to become exocytosed into the synaptic cleft.
• Once inside the synaptic cleft, the dopamine can bind to specific proteins called dopamine receptors (in blue) on the membrane of a neighboring neuron
• Occupation of receptors by neurotransmitters causes various actions in the cell • activation or inhibition of enzymes • entry or exit of certain ions
• These actions can be excitatory or inhibitory

Reuptake
• Neurotransmitters (NTs) in the synaptic cleft are removed by: – Enzymatic degradation – Reuptake by specific proteins (in purple) to return the NT to presynaptic terminal – Diffusion
• Removing the NT is important to prevent constant stimulation of the receptor

Neuromodulation • Synaptic clefts
sometimes include more than two neurons that allow for neuromodulators, such as endorphin (gray), to act on the same neuron
• Neuromodulators act on a different receptor, opiate in this case, which adds another signal to the postsynaptic membrane
• The sum of all the signals determines what occurs in the next neuron

The Reward Pathway
• There are pathways in the brain that have been identified for specific functions such as sight, movement or reward.
• The reward pathway is activated by a rewarding stimulus such as food, water, sex and some drugs.
• Reward Pathway Components (In order): – Ventral Tegmental Area (VTA) – Nucleus Accumbens – Pre‐Frontal Cortex
• This pathway and many others were identified by placing probes into rat brains

Case Study – Part IIa • En route to the hospital, the paramedics give dextrose and 5.2mg of
Narcan – Why give dextrose? – We will discuss Narcan later.
• When the patient arrives at the hospital, he is alert and responsive, new vital signs: – BP: 117/88 – Pulse: 111 – Respirations: 24 – Pupils: not observed – Skin: 97.4 °F – Glucose: 120 mg/dL
• Classify these vital signs. • At this point, what do you think the patient took?

Case Study – Part IIb • Dextrose given to raise blood sugar
• BP: 117/88 ‐ prehypertensive • Pulse: 111 ‐ tachycardia • Respirations: 24 ‐ hyperventilating • Pupils: not observed • Skin: 97.4 ‐ normal • Glucose: 120 mg/dL – normal
• Place your bets on what he took, we will review some drugs now

Cocaine
• A central nervous system stimulant
• Can be snorted, injected or smoked
• Is the active ingredient in crack • Gives a euphoric and energetic feeling
• Risks: Heart attack, respiratory failure, strokes, seizures, abdominal pain, nausea, death
• 2009: 4.8 million Americans 12 or older had abused cocaine
Possible presenting signs and symptoms: body temperature blood pressure heart rate confusion paranoia dilated pupils irritability scratching hallucinations short temperament Anxiety/panic attacks Sleeplessness Loss of appetite sex drive Very talkative

Mechanism of Action Of Cocaine • Cocaine (teal) localizes in the reward
pathway of the brain and mimics dopamine
• Cocaine blocks reuptake of dopamine, leaving more dopamine in the synapse and causing more receptors to be activated
• Increased activation of the dopamine receptor results in an abnormally high firing rate in the post synaptic terminal
• The reward pathway is maximized and addiction results from prolonged use and the inability to reproduce cocaine affect without the drug

Localization of Cocaine

Opiates
• A class of drugs that share a similar chemical structure originally obtained as natural products of the opium poppy plant
• Includes: heroin, morphine, fentanyl, oxycodone, methadone, codeine
• Many routes of administration, injection is common
• Creates a feeling of euphoria and relaxation – a depressant
• The major risk is depression of breathing possibly resulting in death
• Mixing opiates together or with stimulants (cocaine) greatly increases the dangers of abuse
• Overdose should be immediately treated with an opiate antagonist
Possible presenting signs and symptoms: Fade in and out
wakefulness Flushing of skin Dry mouth Slowed breathing Constricted pupils “Heavy” extremities Nod off suddenly Unclear thinking Itching Vomiting Nausea Constipation

Mechanism of Action of Opiates • Opiates act in the dopamine synaptic cleft with three neurons • Opiates activate the opiate receptor causing more dopamine to be
released into the synaptic cleft • Opiates, like cocaine over stimulate the reward pathway causing
addiction

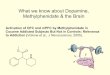
Marijuana and THC • Marijuana is dried up parts of the Cannabis sativa hemp plant
• THC is the active ingredient, delta‐9‐tetrahydrocannabinol
• Method of abuse is usually smoking
• It gives a euphoric feeling, distorted perceptions, memory impairment and difficulty solving problems
• It is the most commonly used illegal drug in the US
Possible presenting signs and symptoms: Bloodshot eyes Compulsive eating Squinty eyes that may be
difficult to keep open Dry mouth Forgetfulness Uncontrollable laughter Short‐term memory loss Lethargy Delayed motor skills Paranoia Hallucinations

THC and the Brain
• THC acts with a similar mechanism to opiates
• THC binds to THC receptors in the following areas: – Reward Pathway (VTA, NA) ‐
Pleasure – Hippocampus – Affecting memory – Cerebellum – Loss of coordination
and balance

The Reward Pathway and Drugs
• The reward pathway is only one area that each drug acts
• It is what makes the user feel good and can be involved in the addiction process
• Each drug acts on other areas as well, which is why each can have different affects such as stimulating or depressing

Prescription Drug Abuse
• Defined as taking a prescription medication that is not prescribed to you or taking it for reasons or dosages other than prescribed
• Different classes and varieties that are abused include: – Opiods – Vicodin, Oxycontin, Darvon, Dilaudid, Demerol, Lomotil
– Depressants – barbituates, benzodiazepines (Valium, Xanex)
– Stimulants – Ritalin, Concerta, Adderall • It a serious and growing problem
– About 20% of people in the US have used prescription meds for nonmedical reasons
– Prescription drug abuse now exceeds illicit drug abuse worldwide

Case Study – Part 3a
• What drug do you think the patient took? • What do you think Narcan is?

Case Study – Part IIIb • Narcan is a brand name for naloxone, an opiate antagonist, given for opiate overdoses
• The patient says he took too much heroin. • Urine toxicology is positive for opiates and cocaine. • The patient is evaluated by a physician and reports he has normal neurologic function and normal mentation.
• Three hours after getting to the hospital a nurse reports decreased lung sounds on both sides.
• Five hours after getting to the hospital his vital signs have returned to normal.
• The ED and the waiting room are full. What should you do? Discharge, admit or keep in the ED?

Case Study – Part IIIc
• The attending physician decides to discharge the patient to his parents.
• Five hours after discharge, the patient is once again found unresponsive in his bed.
• Paramedics arrive, find him in asystole, attempt resuscitation but have no success
• Patient is pronounced dead at the scene • How could this have been prevented?

Case Study – Part IIId
• Presence of cocaine in the urine should have tipped the physician off that there was more to the story.
• Decreased breath sounds was another clue that should have prompted further evaluation.
• Cocaine can cause pulmonary edema and myocardial infarctions, which is what occurred in this patient.
• The physician did not follow the standards of care for this situation.

This is your brain on drugs…
Any Questions?