Embed Size (px)
Citation preview

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 1 1
THE BIOPSYCHOSOCIAL APPROACH TO PAIN MANAGEMENT
Robert J. Gatchel, Ph.D., ABPP, Krista J. Howard, Ph.D. Candidate
Department of Psychology, College of Science
The University of Texas at Arlington
and
Nancy D. Kishino
West Coast Spine Restoration Center,
Riverside, CA

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 2 2
“For all the happiness mankind can gain,
Is not in pleasure, but in rest from pain”
- John Dryden (1631-1700)
Given that pain affects approximately 50 million Americans, and the costs associated
with both the treatment of pain and lost productivity range from $70 to $100 billion annually 1, 2
,
the pursuit for understanding the underlying mechanisms of pain and identifying the best
possible treatment options has prevailed because of these staggering costs. Indeed, in a study
released by the Centers for Disease Control and Prevention’s (CDC) National Center for Health
Statistics 3 1 in 4 U.S. adults reported a pain experience that lasted a full day during the previous
month, and 1 in 10 reported an experience of pain lasting a year or more. The study also
revealed that one-fifth of adults over the age of 65 reported pain that lasted more than 24 hours,
with three-fifths of these older adults reporting that their pain had lasted for more than 1 year.
Although pain research has traditionally focused on the sensory modalities and the
neurological transmissions identified solely on a biological level, more recent theories
(integrating the body, mind, and society) have been developed. The most heuristic perspective is
known as the biopsychosocial model, with pain viewed as a dynamic interaction among and
within the biological, psychological and social factors unique to each individual. Indeed, as
reported by Gatchel 4, Figure 1 presents a conceptual model of these interactive processes
involved in health and illness. Pain is not purely a perceptual phenomenon in that the initial
injury that has caused the pain also disrupts the body’s homeostatic systems which, in turn,
produce stress and the initiation of complex programs to restore homeostasis (to be discussed
later in this article). In this paper, we will also examine the following: the evolution of the
biopsychosocial perspective from earlier pain theories; the fundamental attributes associated with

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 3 3
chronic pain conditions; and the biopsychosocial approach to the assessment and management of
pain.
------------------------------
INSERT FIGURE 1 ABOUT HERE
------------------------------
PROGRESSION THROUGH THE EARLY THEORIES OF PAIN
TO THE BIOPSYCHOSOCIAL MODEL
The earliest theories of pain had focused primarily on the understanding of the biological
or pathophysiological component of pain. Cartesian Dualism, or separation of the mind and the
body, dates back to the 17th
century when Rene Descartes conceptualized pain as an exclusive
process within the sensory nervous system 5. At that time, diseases and illnesses were described
purely as mechanistic biological processes. Even without empirical evidence, it was conceived
that the experience of pain was conveyed directly to the brain from the skin, without any
psychosocial interplay. Termed biomedical reductionism, this point of view remained constant
through the late 19th
century. During the late 1800s, two additional theories arose, providing a
clearer conceptualization of the biological view of pain. The specificity theory of pain, put forth
by Maximilian von Frey in 1894, proposed that there were subcutaneous receptors unique to the
different types of sensory input 6. The distinctions between these receptors varied with respect to
their functionality, such that they were designed explicitly to allow for the interpretation of
sensations such as touch, temperature, pressure, or pain.
The pattern theory of pain, presented by Goldschneider in 1894, differed from von Frey’s
theory by stating that, not only were all subcutaneous receptors were alike, but the unique

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 4 4
patterns of stimulation at the nerve endings were what distinguished the variability in the
interpretations of the sensory signals 6. It was assumed that the central nervous system was
responsible for coding these nerve impulse patterns that resulted in the pain experience.
Although this theory helped to explain incidences of phantom limb pain, which is described as
experiencing pain after the termination of the input, the pattern theory of pain disregards receptor
and fiber evidence which has come to fruition in recent developments.
Today, there is much more known about the different types and functions of receptors,
such that mechanoreceptors respond to touch and pressure, while thermoreceptors activate in
response to changes in temperature. Nociceptors are affiliated with pain perception and,
depending on the specific fiber (A or C) associated with the type of nociceptor (mechanical,
thermo-mechanical, or polymodal) stimulated, the perception of pain can range from sharp and
prickly, to burning or freezing 7.
Although the specificity and pattern theories of pain were fundamental in the
development of the understanding of biological modalities, the detachment from this dualistic
view corresponded with the lack of integration of mind-body phenomena. The lack of adequate
explanations for pain and suffering spurred the next advance in our understanding of nociception
and the individual experience of pain. In the 1960s, Melzack and Wall 8 postulated a more
integrative model—The Gate Control Theory of Pain. Although the underlying mechanisms of
this proposed theory are often debated, the implications that there is an interaction between the
psychosocial and physiological processes have been widely accepted 5.
The gate control theory of pain emphasized the significant role that psychosocial factors
potentially play in the perception of pain. The term gate-control refers to the proposed
mechanism of the substantia gelatinosa located in the dorsal horn of the spinal cord. Melzack and

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 5 5
Wall 8 claimed that this gate-like function modulated the amount of afferent impulses from the
periphery to the transmission cells (T-cells) of the dorsal horn through inhibitory processes at the
neuronal level, and thereby controlling the quantity and intensity of the signals to the central
nervous system. Furthermore, it was posited that higher cortical functions contribute to this
gating mechanism, which allow for psychological phenomena to directly affect the subjective
experience of pain.
From a clinical perspective, Gatchel 5 suggests that the psychosocial component in the
gate control theory contributes a great deal in treating patients with pain. Negative states of
mind, such as helplessness, hopelessness and anger, tend to amplify the intensity of the sensory
input, while strategies focusing on coping and stress reduction help to “close” the gate. Also,
behaviors found to facilitate keeping this gate “open” include poor eating habits, smoking,
inadequate sleep, and lack of exercise. By promoting positive health behaviors, proactive
choices can be factors in lessening the perception of pain.
Compared to the earlier dualistic approaches to understanding pain, the gate control
theory can be viewed as the first mind-body perspective to introduce the integration of the
central nervous system with cognitive processes. An extension to this theory, termed the
Neuromatrix Model of Pain, was proposed by Melzack in 1999. The neuromatrix theory
incorporates the stress component into the pain equation. Based on the original work put forth
by Selye9, stress serves as a mechanism of adaptation, such that the body will respond to
challenging or dangerous situations in an attempt to lessen any problematic consequences. The
two neuroendocrine systems, the sympathetic-adrenomedullary system and the hypothalamic-
pituitary-adrenocortical axis (HPA), serve to activate this fight or flight system 10
. However,
hyperactivity of the HPA system can be seen to intensify the pain condition. When dealing with

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 6 6
chronic pain, individuals experiencing elevated levels of stress may actually exacerbate the pain
experience. As stress intensifies pain, the increased level of pain, in turn, inevitably becomes a
stressor that continues to threaten homeostasis. Based on the theory provided by Melzack 11
,
each individual’s distinct neuromatrix, comprised from genetics, sensory modalities and
memory, determines the overall interpretation of the experience of pain 12
.
THE BIOPSYCHOSOCIAL PERSPECTIVE OF PAIN
As the gate control and neuromatrix theories provided the opportunity to explore how the
mind-body relationship relates to the pain experience, the biopsychosocial perspective has
become the most heuristic approach to truly understanding the concept of pain. This approach
views a physical disorder as the result of an intricate and dynamic interaction among biological,
psychological and social factors that can often antagonize the pain condition. Individuals tend to
express variability in their pain experiences due to the range of physiological, psychological and
social factors that interact, which thereby modulate the interpretation of symptoms 5, 12
.
The biopsychosocial model was first introduced in medicine by Engel 13
when he
highlighted the fact that, as a medical illness became more chronic in nature, then psychosocial
“layers” (e.g., distress, illness behavior and the sick role) emerged to complicate assessment and
treatment. Subsequently, Loeser 14
, applied this model to pain (Figure 2). From this perspective,
there were four dimensions related to the idea of pain: nociception, pain, suffering and pain
behavior 5.
------------------------------
INSERT FIGURE 2 ABOUT HERE
------------------------------

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 7 7
Nociception refers to the physiological components associated with sensory input, such as
nerve receptors and fibers; and pain is described as a subjective perception resulting from
sensory input. While nociception and pain provide methods of communication to the central
nervous system, suffering and pain behavior, on the other hand, are described as reactions to
those signals that can be influenced by both previous experiences and anticipation of potential
consequences. Suffering can be seen as a negative affective response to nociception or pain.
Oftentimes, individuals who experience a painful encounter will exhibit various emotional
responses such as depression, anxiety and fear. Pain behavior is described in one’s actions while
suffering from pain. For example, fear of recurrence of injury often leads to inactivity which, in
turn, can delay the progression of recovery 5.
Similar to the distinction between nociception and pain, Turk and Monarch 12
identify the
differences between disease and illness in chronic pain patients. The term disease describes an
altered condition resulting from the disruption of normal physiological systems and is considered
to be an “objective, biological event.” Illness, on the other hand, refers also to the “subjective
experience” associated with the disease state represented by a unique interaction among
biological, psychological and social factors. Chronic pain is viewed as an illness which cannot be
cured, but only managed. Therefore, the biopsychosocial perspective is directed at the illness,
rather than the disease, and this approach focuses on the diversity and the individual differences
in the overall pain experience 5. Thus, a management, rather than a merely curative, approach is
taken. Indeed, most chronic illnesses, such as diabetes mellitus, asthma, essential hypertension,
etc. cannot be cured, but only managed.
Knowing that not all individuals who experience an injury develop a chronic pain
condition, it is important to recognize how an acute situation transitions to a chronic pain state.

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 8 8
Acute pain is generally viewed as an indicator of tissue damage and is interpreted through
noxious sensations 7. In general, as the level of nociception decreases, the acute pain state
diminishes. While the individual experiencing acute pain may report an increased level of
anxiety, it is typically temporary. Anxiety, fear and worry in acute pain situations are often
viewed as being adaptive in that the negative emotions influence proactive recovery behaviors,
such as seeking medical care and attending to the injury.
An intermittent stage occurs following the acute phase, such that the pain condition is
seen to last for two to four months post injury. During this stage, the patient is described as
experiencing more psychological and behavioral distress, such as anger, somatization and
learned helplessness 15
. Chronic pain typically lasts for at least six months past the injury, which
surpasses the time for which general musculoskeletal disorders heal sufficiently 16
. Syndromes
producing long-term pain conditions are often associated with depression and resentment 17
.
Chronic pain patients frequently develop a “physical deconditioning syndrome” for which
atrophy, reflected by a decrease in strength, flexibility and stamina, is the product of neglect of
the injured area 18
. Along with the physical deconditioning component, chronic pain patients can
also be characterized with a “mental deconditioning” dilemma. As their emotional well-being is
compromised, these chronic pain patients often become avoidant and lose touch with their daily
responsibilities so that others in their social group need to not only “pick up the slack,” but also,
by doing so, reinforce the avoidant behaviors 19
. In this type of situation, chronic pain patients
are seen to lose motivation, specifically with their family, in their physical activities, and within
their careers. When the lack of motivation interferes with their occupation, the chronic pain
patient may also experience a significant financial burden, which can exacerbate the affective
state as well.

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 9 9
The interwoven affiliation of the biological, psychological and social elements unique to
each chronic pain patient must be attended to if a full understanding of the situation is warranted.
Standard treatment protocols are found to be deficient if any one of these components is ignored
17. Because patients with the same diagnosis can respond differently to a standard treatment
protocol, the goal in the biopsychosocial approach to assessment and management is to tailor the
treatment to the specific needs of the individual.
THE BIOPSYCHOSOCIAL APPROACH TO PAIN ASSESSMENT
The biopsychosocial approach to understanding pain has been identified as the most
successful model to date, in that it encapsulates the broader issues embedded in the interactions
among the biological, psychological and social components unique to each individual. Thus
said, the concept of pain cannot be broken down into discrete physical or psychosocial elements
17. Rather, the complexity of pain manifests not only within the range of psychological, social
and physical attributes, but also with respect to chronicity, such that these intertwined
components are seen to modulate the patient’s perception of pain and disability. The
biopsychosocial model, therefore, uses physical, psychological, social, cognitive, affective and
behavioral measures, along with their interactions, to best assess the individual’s unique pain
condition 17
.
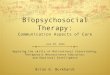
A recent enhancement of this model is reflected in the better understanding of how the
neuroendocrine system affects the chronic pain condition 4, 5
. In addition to the impact of general
emotional distress, elevations of stress hormones produced by the hypothalamic-pituitary-
adrenocortical (HPA) system, such as cortisol, have been found to exacerbate pain conditions
(Figure 3). Earlier, McEwen 20
had highlighted the importance of evaluating cortisol
dysregulation under condition of allostatic load increases due to stress. Underlying mechanisms

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 10 10
related to the HPS axis may therefore help to explain individual differences in stress and pain, as
well as other medical condition such as fibromyalgia. Indeed, several recent studies have
associated HPA dysfunction with chronic pain conditions, such as fibromyalgia, chronic fatigue
syndrome, chronic pelvic pain 21
, temporomandibular pain disorder (TMD 22
), rheumatoid
arthritis and multiple sclerosis 23
.
------------------------------
INSERT FIGURE 3 ABOUT HERE
------------------------------
Furthermore, growing technologies have allowed for a better understanding of the pain
experience through various modalities, such as functional magnetic resonance imaging (fMRI)
and positron emission tomography (PET). These types of imaging techniques focus on the
displacement of blood flow within specified regions of the brain. Although there is some
controversy regarding the implications derived from imaging procedures, these non-invasive
technologies have provided knowledge about the anatomy and pathways related to the central
nervous system 24
. In addition to the brain imaging techniques, other developments in pain
research have been found in areas of genetics, electrophysiology, molecular biology and
pharmacology 24
. The unification of disciplines focused on pain provides the most effective
methods to understanding pain because it gives a comprehensive view of how the nervous
system perceives, deciphers and responds to pain 6, 24
.
When attempting to assess an individual’s pain condition, there are two essential
confounds or “traps” to avoid. First, although there are numerous pain assessments available, the
practitioner cannot assume that any one assessment will have more validity or reliability than
another measure. Secondly, while physical measures of pain are more objective than self-report

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 11 11
instruments, both must be taken under consideration in the evaluation of the pain condition.
Regardless the level of accuracy in the objective analysis of pain, the interpretation on the part of
the health care professional must be considered for an adequate diagnosis to be made.
Furthermore, the individual’s psychological state can influence the performance on a physical
assessment, such that fear of re-injury and lack of motivation may affect the outcome measures
15.
When considering the types of assessments to use, the measure is only valid if it is
aligned with the purpose at hand. Assessments used in chronic pain populations that focus solely
on biological and physiological aspects may not be valid in predicting impairment or disability
17. Not only is it important to consider each measure to be used but, moreover, to be able to
identify how the various tools assimilate into a complete analysis of the individual’s pain
condition. A step-wise approach to assessment has been advised, beginning with a general
evaluation of the factors under consideration, leading up to a more definitive diagnosis 25
. By
taking this multidimensional view, the biopsychosocial approach to assessment will lead not only
to a better understanding of the patient’s pain condition, but ultimately will lead to a
comprehensive treatment protocol customized to the individual’s unique situation.
THE BIOPSYCHOSOCIAL APPROACH TO PAIN MANAGEMENT
As noted earlier, similar to other chronic illnesses, such as diabetes or asthma, a chronic
pain condition cannot be cured, but it can be managed. Due to the heterogeneity with respect to
the biological and psychosocial elements within a chronic pain population, not only is greater
diversification of treatment options necessary, it is essential to properly match the treatment to
the patient. Because two patients with the same diagnosis differ in physical, social and

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 12 12
psychological compositions, “lumping” these patients into the same treatment program will not
likely produce the best outcomes compared to a tailored treatment regimen 5.
The overall outcome goal when treating patients which chronic pain conditions is
improving functional capacity, which correlates with better physical strength and mobility, along
with an improved affective state and self-esteem. Depending on the circumstances and duration
of the injury, there are different levels of care, specifically primary, secondary and tertiary care,
for patients experiencing pain. The focus of primary care is to relieve the symptoms associated
with the acute pain condition while increasing movement and functionality in the affected area
26. In general, the psychological factors addressed in primary care settings correspond to
alleviating any anxiety or fear associated with the occurrence of pain. At this phase, it is
important to educate the patient about medication compliance and following the prescribed
exercise protocol in order to expedite the healing process.
Most patients who incur an injury recover well following the primary care treatment.
When psychological factors and social issues merge with the physiological impairment, though,
a more integrated rehabilitation process is necessary to help the patient avoid entering into a full
chronic pain condition. Commonly, a subset of the injured population finds recuperation to be
difficult at the level of primary care, and will therefore require an expanded treatment program
for their injury, which is called secondary care. At this level, an interdisciplinary team works
together to help the patient to prevent physical deconditioning and to reduce psychological
barriers that interfere with recovery. Most patients for whom primary care is not sufficient
experience positive outcomes following secondary care 27
.
Some patients do not respond well to either primary or secondary care for reasons
relating to poor physical and psychological recovery, or other factors such as legal and work-

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 13 13
related issues that may contribute to more pronounced emotional distress. Functional restoration,
which is a form of tertiary care, has been developed for this chronic pain population. The focus
of functional restoration is to avert permanent disability by utilizing a biopsychosocial approach.
Within the scope of this treatment, the patient receives assistance from an interdisciplinary team
of health care professionals, often including, but not limited to, a primary care physician, a
psychiatrist or psychologist, a physical therapist, an occupational therapist, and a disability case
manager. Together, this team develops a comprehensive plan to help the patient not only regain
mobility and function, but also to teach the patient stress management techniques and coping
skills necessary for dealing with any lifestyle or work issues that develop as a result of the pain
and impairment 28
. Oftentimes, chronic pain patients admitted to a tertiary care program are
found to be reliant on their pain medications. Although relief from pain symptoms is an
appropriate course of action in the primary and secondary care programs, substance use,
specifically opioid dependency, is far too common 29
. In most functional restoration programs,
detoxification is found to be an essential part of treatment which is found to produce positive
lifetime outcomes.
Following sufficient assessment measures and the resultant tailored treatment regimen, it
is necessary to routinely evaluate the progress of the patient and amend or modify the program
when deemed appropriate. The interdisciplinary team should meet together on a regular basis to
discuss each patient’s progress. It is through effective communication, not only within the
medical team, but also with the patient, that the biopsychosocial approach to pain management is
successful 17
.
Functional restoration programs have repeatedly been shown to produce positive
outcomes within the chronic pain population. It is through this biopsychosocial approach to pain

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 14 14
management that patients experiencing chronic pain are able to regain mobility and function, to
improve psychological conditions such as depression and anxiety, and to allow the patient to
return to normal life activities. Besides decreasing self-reported pain and disability, as well as
increasing physical functioning, this functional restoration approach (first developed by Mayer &
Gatchel18
) has also produced substantive improvement in various important socioeconomic
outcome measures (e.g., return-to-work and resolution of outstanding medical issues). For
example, in patients who were chronically disabled with spinal disorders, Mayer, Gatchel et al. 30
found that 87% of the functional restoration group was actively working two years after
treatment, as compared with only 41% of a non-treatment comparison group. Moreover, about
twice as many of the comparison group patients had both additional spine surgery and unsettled
workers’ compensation legal cases, relative to the treatment group. The comparison group
continued with an approximately five-times-higher rate of patient visits to health care
professionals and higher rates of recurrence or re-injury. Thus, these results displayed the
striking impact that a functional restoration program can have on these important measures in a
chronic pain group consisting primarily of workers’ compensation patients (traditionally the
most difficult cases to treat successfully).
The effectiveness of this original functional restoration program has been independently
replicated by Hazard et al.31
and Patrick, Ahmaier, and Found32
in the United States.
Randomized controlled trials demonstrating positive outcomes include: Bendix et al.33
and
Bendix and Bendix34
in Denmark; Hildebrandt, Pfingsten, Saur, and Jansen35
in Germany;
Corey, Koepfler, Etlin, and Day36
in Canada; Jousset et al.37
in France; and Shirado, Ito,
Kikumoto et al.38
in Japan. The fact that different clinical treatment teams, functioning in
different states and different countries, with markedly different economic and social conditions

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 15 15
and workers' compensation systems, produced comparable positive outcome results speaks
highly for the robustness of the research findings and utility, as well as the fidelity, of this
approach to pain management in occupational settings. Gatchel and Mayer 39
have further
reviewed this evidence.
This functional restoration approach has also been found to be effective with chronic
upper extremity disorders.40
In addition, this type of approach has been found to be an effective
early intervention treatment for preventing chronic disability. For example, in a randomized
controlled study, acute low-back-pain patients who were identified as “high risk” for developing
chronic back pain disability were randomly assigned to an early functional restoration group or a
treatment-as-usual group,41
The functional restoration group displayed significantly fewer
indexes of chronic pain disability at 1-year follow-up on a wide range of work, healthcare
utilization, medication use, and self-reported pain variables. For example, the functional
restoration group was less likely to be taking narcotic analgesics (odds ratio = 0.44), and also less
likely to be taking psychotropic medications (odds ratio = 0.24). Moreover, the treatment-as-
usual group was less likely to have returned to work (odds ratio = 0.55). The cost-comparison
savings data from this study were also quite impressive: The treatment-as-usual group cost twice
as much as the functional restoration group over a 1-year period.
Besides functional restoration, there have been a host of other studies demonstrating the
treatment effectiveness of interdisciplinary pain-management programs (based on the
biopsychosocial model) in general in successfully treating various other prevalent chronic pain
syndromes. In fact, Gatchel and Okifuji 42
comprehensively reviewed the literature in
demonstrating the therapeutic- and cost-effectiveness of such comprehensive programs, relative
to simple, single-modality approaches such as pharmacotherapy, surgery, injections, etc., on a

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 16 16
number of measures (see Table 1), as well as on the important variable of return-to-work (see
Table 2).
------------------------------
INSERT TABLES 1 AND 2 ABOUT HERE
------------------------------
This has led Guzman and colleagues 43
to conclude, on the basis of a comprehensive Cochrane
Review, that
“There was strong evidence that intensive multidisciplinary biopsychosocial
rehabilitation with functional restoration improves function when compared with
inpatient or outpatient non-multidisciplinary treatment.”
CONCLUSIONS
Due to the high prevalence of chronic pain conditions, that results either from injury or
disease, identifying and implementing the most effective treatment options available is a primary
concern. Although the biological mechanisms associated with pain have been recognized and
accepted, the biopsychosocial approach to understanding and managing pain is the most heuristic
approach available. The pain experience can be viewed from a systematic perspective, so that as
the biological condition worsens, psychological and social factors follow, that need also be
managed. It emphasizes the unique interactions among biological, psychological, and social
factors that need to be considered to better understand pain syndromes. Thus, treating the
“whole” person is far more important than focusing merely on a disease. Managing the illness is
the most appropriate approach to take. By using the appropriate assessments to adopt the most
suitable interdisciplinary treatment program, the chronic pain patient is far more likely to regain
function and to show vast improvements in his/her quality of life. Indeed, this biopsychosocial

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 17 17
approach to pain has led to the development of the most therapeutic- and cost-effective
interdisciplinary pain management programs, that far exceed in their effectiveness any of the
earlier overly simplistic biomedical reductionist approaches to the treatment of pain.

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 18 18
REFERENCES
1. Gatchel RJ, Turk DC. Psychological Approaches to Pain Management: A Practitioner's
Handbook. New York: Guilford Publications, Inc.; 1996.
2. Gatchel RJ, Mayer TG. Occupational Musculoskeletal Disorders: Introduction and
Overview of the Problem. In: Mayer TG, Gatchel RJ, Polatin PB, eds. Occupational
Musculoskeletal Disorders: Function, Outcomes, and Evidence. Philadelphia: Lippincott
Williams & Wilkins; 2000:3-8.
3. National Center for Health Statistics. Health, United States, 2006, with Chartbook on
Trends in the Health of Americans with Special Feature on Pain. Press Release.
Available at: http://www.cdc.gov/nchs/pressroom/06facts/hus06.htm. Accessed
November 29, 2006.
4. Gatchel RJ. Comorbidity of chronic mental and physical health disorders: The
biopsychosocial perspective. Am Psychol. 2004; 59:792-805.
5. Gatchel RJ. Clinical Essentials of Pain Management. Washington, DC: American
Psychological Association; 2005.
6. Gatchel RJ. Perspectives on Pain: A Historical Overview. In: Gatchel RJ, Turk DC, eds.
Psychosocial Factors in Pain: Critical Perspectives. New York: Guilford Publications;
1999:3-17.
7. Basbaum AI, Jessell TM. The perception of pain. In: Kandel ER, Schwartz JH, Jessell
TM, eds. Principles of Neural Science. New York: McGraw Hill Companies; 2000:472-
491.
8. Melzack R, Wall PD. Pain mechanisms: A new theory. Science. 1965;50:971-979.
9. Selye H. Stress. Montreal, Quebec: CA: Acta Medical Publishers; 1950.

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 19 19
10. Henderson BN, Baum A. Biological mechanisms of health and disease. In: Sutton S,
Baum A, Johnston M, eds. SAGE Handbook of Health Psychology. London, UK: SAGE;
2004:69-93.
11. Melzack R. Pain and stress: A new perspective. In: Gatchel RJ, Turk D, eds.
Psychosocial Factors in Pain: Critical Perspectives. New York: Guilford Press;
1999:89-106.
12. Turk DC, Monarch ES. Biopsychosocial perspective on chronic pain. In: Turk DC,
Gatchel RJ, eds. Psychological Approaches to Pain Management: A Practitioner's
Handbook. 2nd ed. New York: Guilford; 2002.
13. Engel GL. The need for a new medical model: A challenge for biomedicine. Science.
1977;196(4286):129-136.
14. Loeser JD. Concepts of Pain. In: Stanton-Hicks J, Boaz R, eds. Chronic Low Back Pain.
New York: Raven Press; 1982.
15. Gatchel RJ. A biopsychosocial overview of pre-treatment screening of patients with pain.
Clin J Pain. 2001;17:192-199.
16. Gatchel RJ. Early development of physical and mental deconditioning in painful spinal
disorders. In: Mayer TG, Mooney V, Gatchel RJ, eds. Contemporary Conservative Care
for Painful Spinal Disorders. Philadelphia: Lea & Febiger; 1991:278-289.
17. Gatchel RJ, Maddrey AM. The Biopsychosocial Perspective of Pain. In: Raczynski J,
Leviton L, eds. Healthcare Psychology Handbook. Vol II. Washington, D.C.: American
Psychological Association Press; 2004.
18. Mayer TG, Gatchel RJ. Functional Restoration for Spinal Disorders: The Sports
Medicine Approach. Philadelphia: Lea & Febiger; 1988.

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 20 20
19. McMahon MJ, Gatchel RJ, Polatin PB, Mayer TG. Early childhood abuse in chronic
spinal disorder patients. A major barrier to treatment success. Spine. 1997;22(20):2408-
2415.
20. McEwen BS. Protective and damaging effects of stress mediators. New England Journal
of Medicine. 1998;338:171-179.
21. Tanriverdi F, Karaca Z, Unluhizarci K, Kelestimure F. The hypothalamo-pituitary-
adrenal axis in chronic fatigue syndrome and fibromyalgia syndrome. Stress. The
International Journal on the Biology of Stress. 2007;10(1):13-25.
22. Garofalo JP, Robinson RC, Gatchel RJ. Hypothalamic-Pituitary-Adrenal Axis
Dysregulation in acute temporomandibular disorder and low back pain: A marker for
chronicity? Journal of Applied Biobehavioral Research. 2006;11(3-4):166-178.
23. Bomholt SF, Ballerup D, Harbuz MS, Blackburn-Monro G, Blackburn-Monro RE.
Involvement and role of the hypothalamo-pituitary-0adrenal (HPA) stress axis in animal
models of chronic pain and inflammation. Stress. The International Journal on the
Biology of Stress. 2004;7(1):1-14.
24. Gatchel RJ, Peng Y, Peters ML, Fuchs PN, Turk DC. The Biopsychosocial Approach to
Chronic Pain: Scientific Advances and Future Directions. Psychological Bulletin.
2007;133:581-624.
25. Gatchel RJ. How practitioners should evaluate personality to help manage chronic pain
patients. In: Gatchel RJ, Weisberg JN, eds. Personality Characteristics of Patients with
Pain. Washington, DC: American Psychological Association; 2000.
26. Mayer TG, Gatchel RJ, Porter S, Theodore B. Postinjury rehabilitation management. In:
Marras WS, Karwowski W, eds. The Occupational Ergonomics Handbook: Intervention,

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 21 21
Controls and Applications in Occupational Ergonomics. 2nd ed. Boca Raton, FL: CRC
Press; 2006.
27. Karjalainen K, Malmivaara A, Mutanen P, Roine R, Hurri H, Poholainen T. Min-
intervention for subacute low back pain: Two-year follow-up and modifiers of
effectiveness. Spine. 2004;10:1069-1076.
28. Mayer TG, Gatchel RJ, Kishino N, et al. Objective assessment of spine function
following industrial injury: A prospective study with comparison group and one-year
follow-up. Spine. 1985;10:482-493.
29. Dersh J, Polatin P, Gatchel R. Chronic pain and psychopathology: Research findings and
theoretical considerations. Psychosomatic Medicine. 2002;64:773-786.
30. Mayer TG, Gatchel RJ, Mayer H, Kishino ND, Keeley J, Mooney VA. A prospective
two-year study of functional restoration in industrial low back injury. An objective
assessment procedure [published erratum appears in JAMA 1988 Jan 8;259(2):220].
JAMA. 1987;258(13):1763-1767.
31. Hazard RG, Fenwick JW, Kalisch SM, et al. Functional restoration with behavioral
support: A one-year prospective study of patients with chronic low-back pain. Spine.
1989;14:157-161.
32. Patrick L, Altmaier E, Found E. Long-term outcomes in multidisciplinary treatment of
chronic low back pain: Results of a 13-year follow-up. Spine. 2004;29:850-855.
33. Bendix AE, Bendix T, Vaegter K, Lund C, Frolund L, Holm L. Multidisciplinary
intensive treatment for chronic low back pain: A randomized, prospective study. Cleve
Clin J Med. 1996;63(1):62-69.

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 22 22
34. Bendix T, Bendix A. Different training programs for chronic low back pain--A
randomized, blinded one-year follow-up study. Paper presented at: International Society
for the Study of the Lumbar Spine, 1994; Seattle.
35. Hildebrandt J, Pfingsten M, Saur P, Jansen J. Prediction of success from a
multidisciplinary treatment program for chronic low back pain. Spine. 1997;22:990-1001.
36. Corey DT, Koepfler LE, Etlin D, Day HI. A limited functional restoration program for
injured workers: A randomized trial. Journal of Occupational Rehabilitation.
1996;6:239-249.
37. Jousset N, Fanello S, Bontoux L, et al. Effects of functional restoration versus 3 hours per
week physical therapy: A randomized controlled study. Spine. 2004;29(5):487-493.
38. Shirado O, Ito T, Kikumoto T, Takeda N, Minami A, Strax TE. A novel back school
using a multidisciplinary team approach featuring quantitative functional evaluation and
therapeutic exercises for patients with chronic low back pain. Spine. 2005;30:1219-1225.
39. Gatchel RJ, Mayer TG. Evidence-Based Review of the Effectiveness of Functional
Restoration for the Management of Chronic Low Back Pain. The Spine Journal.
2008;8:65-69.
40. Evans RI, Gergen PJ, Mitchell H, et al. A randomized clinical trial to reduce asthma
morbidity among inner-city children: results of the national Cooperative Inner-city
Asthma Study. J Pediatr. 1999;135(3):332-338.
41. Gatchel RJ, Polatin PB, Noe CE, Gardea MA, Pulliam C, Thompson J. Treatment- and
cost-effectiveness of early intervention for acute low back pain patients: A one-year
prospective study. Journal of Occupational Rehabilitation. 2003;13:1-9.

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 23 23
42. Gatchel RJ, Okifuji A. Evidence-based scientific data documenting the treatment- and
cost-effectiveness of comprehensive pain programs for chronic nonmalignant pain.
Journal of Pain. 2006;7(11):779-793.
43. Guzman J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C.
Multidisciplinary rehabilitation for chronic low back pain: Systematic review. Br Med J.
2001;322:1511-1516.
44. Turk DC. Clinical effectiveness and cost effectiveness of treatment for patients with
chronic pain. Clin J Pain. 2002;18(6):355-365.
45. Turk DC. Treatment of chronic pain patients: Plus ca change, plus c'est la meme. Paper
presented at: Taking the Pain out of Complex Pain Management: Practical Approaches
for Improved Services across the Continuum of Care, 2008; Edmonton, Alberta, Canada.

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 24 24
Table 1. Outcomes for Interdisciplinary Pain Rehabilitation Programs (IPRPs) Compared to
Other Care (from Gatchel & Okifuji, 2006 42
and Turk, 2002 44
, as summarized by
Turk45
)
Criteria IPRP Other Care
Pain reduction ± ±
Reduction of medication + -
Reduction of health care
utilization
+ ?
Return-to-work _ -
Increased activity + +?
Closure disability claims + ?
Iatrogenic consequences - +
Cost benefit + -?

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 25 25
Table 2. Rates of Return-to-Work for IPRP 45
Study % RTW IPRP % RTW Controls
Roberts & Reinhardt, 1980 77 5
Sturgis et al., 1984 29 14
Duckro et al., 1985 71 33
Guck et al., 1985 75 25
Finlayson et al., 1986 65 44
Mayer et al., 1987 87 41
Hazard et al., 1989 81 29
Tollison et al., 1989 56 27
Sachs et al., 1990 63 42
Deardorff et al., 1991 48 0
Tollison, 1991 57 20
Feuerstein et al., 1993 74 40
Tyre et al., 1994 86 --
Bendix et al., 1996 64 29
Hildebrandt et al., 1997 62 --
Pfingsten et al., 1997 63 --
Vending et al., 2000 65 --
Rivero-Anas et al., 2005 24 20
Schiltenwolf et al., 2006 59 10
Norrefalk et al., 2007 52 13
Total 63% 24.5%

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 26 26
Figure 1

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 27 27
Figure 2.

Manuscripts\biopsychosocial-pain-mgt-rjg-ndk.804\August 10, 2010 28 28
Figure 3.
Hypothalamus
Pituitary
Stressor/Pain
Adrenal
CortexCorticosteroids
(Cortisol)
ACTHACTH
CRH
HPA Axis