Embed Size (px)
Citation preview
Journal ofNeurology, Neurosurgery, and Psychiatry, 1978, 41, 865-873
The Babinski sign and the pyramidal syndromeJ. VAN GIJN
From the Department of Neurology, Academic Hospital Dijkzigt, Rotterdam, the Netherlands
S U M M AR Y The presence or absence of a Babinski sign can be puzzling, but in the light ofexisting pathological studies it is more fruitful to consider which pyramidal tract fibres releaseit than whether they release it. This was investigated clinically, by looking for correlations withother reflex changes and with motor deficits in the leg. A survey of 50 patients with a unilateralBabinski sign and six patients who lacked it in spite of other pyramidal tract signs was supple-mented with follow-up of the patients who had acute lesions. Appearance of the Babinski signproved to depend on the interaction of two factors: (1) activity (not necessarily hyperactivity)in the segmental pathways of the flexion synergy; (2) a motor deficit of the foot, in some casesconsisting only in an impairment of rapid foot movements, and probably representing adisturbance of direct pyramidal tract projections to distal motoneurones.
In 1896 Babinski described the upgoing toe sign inpatients with "organic affections of the centralnervous system", and one year later he linked itmore specifically to disturbances of the pyramidaltract. Since then, the Babinski sign has becomefirmly established as the cornerstone of the clin-ician's "pyramidal syndrome." Although it hasbeen objected that the sign could appear in manytemporary derangements of brain function (Lassek,1944), or after partial cordotomies without sub-sequent degeneration of corticospinal fibres(Nathan and Smith, 1955), the absence of sec-ondary degeneration does not necessarily implyfunctional integrity (Walshe, 1956). This is ratherobvious in the case of an epileptic seizure or in-toxication. But it applies equally to the cordotomystudies, where the lesions bordered upon the pyra-midal tract and may well have caused loss offunction by focal demyelination (Babinski, 1885;McDonald and Sears, 1970). Babinski's originalview has received new support from two recent casereports which mention the appearance of a Babin-ski response after an almost pure lesion (infarc-tion) of the contralateral pyramid (Chokroverty etal., 1975; Leestma and Noronha, 1976). Moreover,there is no other spinal cord pathway in man thatis crossed and descends low enough in the spinalcord.
It remains to be explained why the Babinskisign can be absent in cases of proven pyramidaltract degeneration (Nathan and Smith, 1955). IfAccepted 8 May 1978
the lesion is complete, we must assume interrup-tion of the reflex arc. If not, we should keep inmind that corticospinal fibres do not only originatein different parts of the precentral and postcentralcortex, but also have different terminations. Therestriction that a Babinski response can be ex-pected only when "leg fibres" of the pyramidaltract are involved (Potts and Weisenburg, 1910) isstill crude: the motoneurones of the leg muscles aregrouped into separate columns within the anteriorhorn of the cord, depending on whether theysupply proximal or distal muscles, flexor or exten-sor muscles (Sharrard, 1955; Kuypers, 1973). Inaddition, there are important pyramidal tract pro-jections to the intermediate (interneuronal) zone,and even to cells in the dorsal horn of the cord(Kuypers, 1973).
This divergence of pyramidal tract projectionsallows two explanations of the Babinski sign.(a) The Babinski sign might be released by dys-function of pyramidal tract fibres that project onthe interneuronal zone, at least on those inter-neurones that subserve the flexion reflex synergy,of which the Babinski sign is part (Marie andFoix, 1912; Walshe, 1914). As these interneuronesare necessarily interconnected across the segmentsof the lumbosacral spinal cord, a Babinski signwould always be accompanied by hyperactivity inother, more proximal, flexor muscles; and in thiscase a Babinski response would not necessarilyimply a disturbance of voluntary leg movementsrelayed by projections to motoneurones.
865
Protected by copyright.
on 7 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.10.865 on 1 O
ctober 1978. Dow
nloaded from
866
(b) Alternatively, the Babinski sign might resultfrom interference with pyramidal fibres projectingdirectly on motoneurones. In that case the effectorof the sign, the extensor hallucis longus (Landauand Clare, 1959; van Gijn, 1975), would at thesame time be less responsive to descending im-pulses. We should expect impairment of voluntarydorsiflexion of the great toe, perhaps also of dorsi-flexion and eversion of the foot, mediated byneighbouring motoneurones. Pyramidal tract con-trol of distal muscles subserves not only muscleforce, but also the capacity to perform fraction-ated and rapid movements (Tower, 1940; Kuypers,1973). Therefore the motor deficit accompanying a
Babinski sign might manifest itself not only byweakness, but also by loss of skill. The release ofthe flexion reflex would not necessarily involveproximal muscles.Thus a study of the coincidence of the Babinski
response and other pathological signs in the lowerlimbs might give insight into physiological andanatomical relationships. Earlier workers have in-vestigated the concurrence of various deficits andrelease phenomena in the lower limbs (Graeffner,1906; Lassek, 1945; Dohrmann and Nowack, 1974).But none of these reports mentioned the clinicalfeatures that are most needed to elucidate thepathophysiology of the Babinski sign: first, possibleasymmetry of the flexion reflex in proximalmuscles, secondly the distribution of weakness or
-in the absence of weakness-the capacity toperform skilled foot movements.
Patients and methods
Two groups of patients were studied.1. Fifty patients (27 men and 23 women) with a
strictly unilateral and unequivocal Babinski signwere found among inpatients and outpatientsduring a period of six months. To be selected forstudy they also had to be well enough to co-operatein the various tests, and they had to be free of un-
related motor disorders (diseases of cerebellum,basal ganglia, or peripheral nerves). A cerebrallesion was diagnosed in 42 of the patients: infarc-tion in 33, tumour in three, Mills' syndrome in two(Mills, 1900), trauma in two, angioma in one, andinfantile hemiplegia in one. In 19 of these 42patients the onset of disease had been less thanfour weeks before the examination. The othereight patients had a (presumably) spinal lesion: sixwere thought to have multiple sclerosis, one had an
old traumatic lesion, and one a recent infarction ofthe thoracic spinal cord.2. In the same time span six patients were foundto show unilateral pyramidal tract signs without a
J. van Gijn
Babinski sign. Four of these suffered from cerebralinfarction, one had motor neurone disease, and onehad uindergone surgery for an intracerebralhaematoma.
All patients in these two groups who had acutelesions were re-examined every few days, untilno further change occurred. Three patients ingroup 1 "lost" a unilateral Babinski response,while other pyramidal tract signs remained. Con-versely, two patients in group 2 developed an up-going toe response only after an initial period inwhich it had been unexpectedly absent. These fivepatients will be considered separately.
EXAMINATION
Plantar reflexAll patients were examined in the supine position.Stimulation was performed with a small woodenstick (orange stick), at the lateral plantar borderand plantar arch. If voluntary movements inter-fered, the stimulus was repeated on the lateralborder of the dorsum of the foot.
Flexion reflexApart from the extensor hallucis longus, specialattention was paid to activation of the tibialisanterior muscle and more proximal flexors: tensorfasciae latae, knee flexors, and hip flexors. Anarbitrary grading scale was used to record thefindings:
- no visible activity+ flicker of movement+ slight knee or hip flexion
+ + knee lifted from couch+ + + similarly, but even on slight stimulation
with finger
PowerThe following movements were tested: extensors-hip extension, knee extension, knee adduction, footplantar flexion, toe plantar flexion; flexors-hipflexion, knee flexion, dorsiflexion of foot (startingfrom a dorsiflexed as well as from a relaxed posi-tion), foot eversion, dorsiflexion of hallux. Gradingwas according to the MRC scale (Medical Re-search Council 1943); slight weakness was recordedas 4+ or even 5-.
SkillFour tests were used: dorsiflexion of the great toe,separately from the foot; wriggling of the littletoes; rapid foot tapping against the examiner'shand (with the patient supine); rapid up-and-downmovements of the great toe, with the foot on thefloor. The results of the latter two tests werequantified by counting the number of taps in 10
Protected by copyright.
on 7 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.10.865 on 1 O
ctober 1978. Dow
nloaded from
The Babinski sign and the pyramidal syndrome
seconds. Skill was considered to be impaired whenthis number was less than three-quarters of thaton the control side, or when there were obviousqualitative differences, such as dysrhythmia orsimultaneous movement of the great and littletoes on one side only.
Associated dorsiflexion of the great toeThis was investigated in three ways: ipsilateral hipflexion against resistance; contralateral hipflexion against resistance; contralateral rapid toemovements.
Tendon reflexesExamined were: ankle jerk (when necessary alsoin the kneeling position), knee jerk, adductor re-
flex, and biceps femoris reflex. These were recordedon a nine point scale (Mayo Clinic, 1963) rangingfrom -4 (absent) through zero (normal) up to+4 (clonus).
TonePassive resistance was separately examined at theankle (by shaking the leg and foot with the patientsupine, the knee (if possible also by comparingpendular movements with the patient sitting), andthe hip.
Abdominal reflexesTwo levels were tested on each side, above andbelow the umbilicus. In men, the cremasteric reflexwas also included.
WastingThe circumference of the thigh was measured150 mm above the medial margin of the kneejoint, the calf at its maximal girth. Wasting was
assumed to be present when the difference was20 mm or more at one of these levels.
Results
UNILATERAL BABINSKI SIGNS
Voluntary movementsThe most frequent finding accompanying the up-going toe response was weakness of foot move-ments: 76% (Table 1). In almost half of thisnumber (32%) the weakness was only slight. Thisalways concerned dorsiflexion of the foot, dorsi-flexion of the hallux, foot eversion, or a combina-tion of these movements. In 10% the weakness was
confined to the foot.Loss of skill in the foot was always a relative
judgment-that is, on comparison with the controlside. If a difference was found, it almost alwaysconcerned the capacity to perform rapid foot or
867
Table 1 Weakness and loss of skill (%) on the sideof unilateral Babinski response (50 patients)
Response Percentage change
WeaknessParalysis of foot 28Marked weakness 16 weakness of foot: 76Slight weakness offoot (> MRC 4) 32JOnly proximal weakness 14
nNo weakness 10 no weaknessoffoot: 24
100Loss of skillWith paralysis or markedweakness of foot (44) 44With slight weakness of foot (32) 30With only proximal weakness (14) 12 no weakness of footWithout weakness 4 f but loss of skill: 16No loss of skill 10
100
toe movements. The ability to dorsiflex the greattoe apart from the foot was found in almost everypatient who could dorsiflex the great toe at all,at least after a few attempts. Asymmetry in wrig-gling the little toes was also rare in the absence ofweakness. Comparing the rate and rhythm ofrapid foot or toe movements appeared to be amuch more sensitive test. The two procedures gavesimilar results in most patients, but occasionallyone or other was more sensitive. In either test,normal values range from 20 to 40 taps in 10seconds.Of the 12 patients without evidence of foot
weakness, loss of skill could be demonstrated ineight. Six of these eight patients had slight proxi-mal weakness, two had normal power. Only fourpatients showed neither weakness nor loss of skill.On comparing the occurrence of other signs inthese exceptional patients with their frequency inthe entire group, the only statistically significantdifference was to find in all four the relativelyrare sign of hallux dorsiflexion on contralateralhip flexion against resistance (occurrence in thewhole group 22%, the Fisher test gives P=0.001).However, this phenomenon was also found on thecontrol side of other patients (Table 2), and thusit can hardly explain in itself why a Babinski signoccurs without a demonstrable motor deficit in thefoot.
In summary, 92% of the patients with a uni-lateral Babinski sign showed some motor deficit inthe foot, 16% having a disturbance of rapid move-ments alone.
Reflex changesThe flexion reflex on the side of the Babinski signalmost invariably involved simultaneous activityin tensor fasciae latae, hamstrings, or iliopsoas;there were only two exceptions among the 50patients. Exaggeration of the flexion reflex in these
Protected by copyright.
on 7 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.10.865 on 1 O
ctober 1978. Dow
nloaded from
868
Table 2 Associated dorsiflexion of the great toe (%)on the side of unilateral Babinski response (50 patients)
On ipsilateral On contralateral On contralateralhip flexion hip flexion rapid toe
movements(mirrormovements)
Not possible 14 2 2Positive 14 18 2Bilaterally positive 20 4 2On control sideonly 18 6 14Absent 34 70 80
100 100 100
proximal limb muscles in comparison with the con-trol side was found in not more than 58%. Thismeans that the Babinski sign is not dependent uponhyperactivity of the flexion reflex as a whole.
Increase of tendon jerks was found in three outof four patients with a Babinski sign (74%). Table3 shows that asymmetry usually affected severalreflexes together. The ankle jerk was rarely in-creased alone (10%), and not preferentially incases with a purely distal motor deficit. The jerkselicited from the adductor and biceps femorismuscle rarely gave extra information. In otherwords, the release of tendon reflexes generallyinvolves different lumbosacral segments, and flexoras well as extensor muscles. It is, therefore, strik-ing to find that the presence of increased tendonjerks is not statistically correlated (Fisher test)with exaggeration of the flexion reflex, which is
Table 3 Additional reflex changes (%) on the side ofunilateral Babinski response (50 patients)
Reflex Percentage change
Flexion reflex in proximal musclesExaggerated 58Symmetrical 38Diminished 4
Tendon reflexesIncrease of ankle jerk only 10Increase of ankle jerk plus increase of one orother reflexes 60 more tendon reflexes74%Only other reflexes increased 4JSymmetrical 22Only other reflexes decreased 2Ankle jerk decreased 2
ToneIncreased in ankle (at least) 10Increased in knee only 6Symmetrical 62Decreased in knee only 8Decreased in ankle 14
Abdominal reflexesDiminished 42Only cremasteric reflexesdiminished 6 (11 /Y of men)Symmetrical 22Absent 26Decreased on control side 4
J. van Gijn
also a multisegmental release phenomenon. Thelack of correlation, positive or negative, betweenthese two forms of hyperreflexia also holds truewhen "absolute" values on both sides are con-sidered instead of asymmetry: every activity levelof the flexion reflex was found together with a widerange of myotatic reflex activity, and vice versa.
Disorders of tone varied with time. In the 42patients with cerebral lesions, hypotonia occurredsignificantly more often when the onset of diseasehad been less than four weeks before (10/19 versus1/23; Fisher test gives P=0.001), and a reversetendency was found for spasticity (1 / 19 versus7/23; P=0.05). The presence of the other physicalsigns did not depend on the duration of disease.Abdominal reflexes, represented much higher in
the spinal cord, were reduced in 42%, but the highabsence rate of the reflex on both sides (26%)makes it difficult to estimate correlations. Wastingwas rare (10%); in two instances it was found insyndromes known to be associated with "supra-nuclear atrophy" (Mills' syndrome, infantilehemiplegia).
PYRAMIDAL TRACT SIGNS WITHOUT BABINSKIRESPONSESix patients lacked a Babinski response whileother pyramidal tract signs were present. Twodeveloped it at a later stage and will be discussedseparately. In the remaining four patients, reflexchanges on the side in question consisted in exag-gerated tendon jerks (cases 1, 2, and 4) and re-duced abdominal reflexes (cases 3 and 4). Theflexion in proximal muscles was (symmetrically)present in all four patients, giving no reason tosuppose a disturbance in the spinal pathways ofthe plantar reflex.
Because, in the first group of patients, theBabinski sign was so closely associated with dis-orders of voluntary innervation of the foot, it wasimportant to find that of these four patients inwhom the Babinski sign was unexpectedly absent,only one showed definite motor impairment of thefoot (case 1, suffering from motor neurone disease,with weakness (MRC 4) of dorsiflexion andeversion, and with slowing down of foot move-ments). Case 2 showed equivocal weakness of footdorsiflexion but no loss of skill, case 3 had onlyproximal weakness, also with symmetry of rapidfoot movements, and case 4 had no motor deficitat all.
BABINSKI SIGNS APPEARING IN OR DISAPPEARINGFROM THE PYRAMIDAL SYNDROMEUntil now, the relationship between upgoing toeresponse and other pyramidal tract signs has been
Protected by copyright.
on 7 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.10.865 on 1 O
ctober 1978. Dow
nloaded from
The Babinski sign and the pyramidal syndrome
studied by a cross-sectional survey. Obviously it isalso of great interest to study temporal relation-ships: when a Babinski sign disappears while othersigns remain, or, conversely, appears only aftersome time, what other findings change with it?
Vanishing Babinski signsThree patients in the first group of 50 patients"lost" their Babinski response while other ab-normal features remained.Case S (improvement of power and skill) A 60year old driver with an infarction in the left cere-bral hemisphere showed, on the ninth day of hisillness, a mild right sided weakness of hip flexion(4+) and foot dorsiflexion (4+), with reduced skilland hyperreflexia. The right plantar response wasupgoing, with a brisk flexion reflex (++; controlside +). Six weeks later, power and skill werenormal. Both plantar responses were absent, theflexion reflex + on the previously weak side and+L on the other. The tendon jerks were still in-creased on the right.Case 6 (improvement of skill) A 53 year oldmaintenance technician suffered a mild stroke inthe territory of the left middle cerebral artery.On the tenth day his only deficit was some weak-ness of hip flexion (4+) and slowing of rapid footand toe movements. All tendon reflexes of theright leg were increased, and there was a Babinskiresponse on the same side; the flexion reflex wasweak on both sides. Three weeks later he had nolonger any motor disability, nor a Babinski sign;only definite hyperreflexia remained.Case 7 (waning of flexion reflexes) A 56 year oldpublican sustained an acute right sided hemiparesis.On the second day he was found to have moderateweakness of the right leg (all flexor movements
with impaired skill and hyperreflexia. Flexionreflexes were bilaterally brisk (+ +), with aBabinski sign on the right. On the tenth day theclinical picture was practically unchanged but forthe right plantar response which was now down-going, and for both flexion reflexes which wereweak (+).
Late Babinski signsTwo patients initially lacked a Babinski sign in thepresence of other pyramidal tract signs, but de-veloped it later. Both had a dense hemiplegia.Case 8 (initial absence of flexion reflex) A 58 yearold nurse sustained a subarachnoid haemorrhagefrom one of two left sided berry aneurysms. On thefourth day she had a paralysed right foot, sym-metrical tendon jerks, and no flexion reflex orBabinski sign on either side. On the thirteenth dayshe developed a right hemiplegia. Examination on
day 24 showed a paralysed right leg, increased ten-don reflexes, and again no flexion reflexes. On day39, while the right leg was still paralysed, plantarstimulation resulted on both sides in slight reflexdorsiflexion of the foot, on the right accompaniedby weak contraction of the extensor hallucislongus.Case 9 (initial depression of flexion reflex) A 50year old industrial manager suddenly developed aright hemiplegia, without impairment of conscious-ness. On the third day his right leg was still para-lysed. No tendon reflexes could be obtained oneither side (this had been noted before by insurancephysicians). Plantar stimulation on the left gave adowngoing response of the toes, together with con-traction of tensor fasciae latae, tibialis anterior,and biceps femoris (+). On stimulation of theright sole the toes remained immobile, and therewas only weak action of the ipsilateral bicepsfemoris and adductor (+4). Three months later, thepatient had regained some power in the right leg,but not in the foot. At this time the right plantarreflex was clearly upward, with exaggeration of theflexion reflex (+ +) as compared with the otherside (still +), and some weak tendon jerks couldbe elicited in the right leg.
Discussion
Two principal features emerge from the cross-sectional and longitudinal case studies presentedabove. First, there seems to be a close associationbetween occurrence of the Babinski sign and im-pairment of voluntary foot movements, the lattereither in the form of weakness or only as a reducedcapacity to perform rapid alternating movements.Secondly, the Babinski sign is not necessarilyfound in association with hyperactivity of theflexion reflex in other muscles than the extensorhallucis longus. Nevertheless, a Babinski sign canappear only if the intraspinal pathways of theflexion reflex synergy are operative, howeversevere the motor deficit in the foot. Both thesefactors, impaired corticospinal control and theactivity of the flexion reflex, will be reviewedseparately before considering how their inter-action results in a Babinski sign.
IMPAIRED CORTICOSPINAL CONTROL OF THE FOOTIf a disturbance of the pyramidal tract affectsprojections to motoneurones of distal muscles butis not more than slight, the only clinical manifesta-tion may be impairment of rapid or fractionatedmovements. For the foot this is less well-knownthan for the hand, but such tests proved to beequally rewarding. In the group of 50 patients with
B
869
Protected by copyright.
on 7 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.10.865 on 1 O
ctober 1978. Dow
nloaded from
870
a unilateral Babinski sign, normal power of footmovements was found in 24%, but reduced skillcould still be demonstrated in two-thirds of these,leaving only 8% of Babinski signs unassociatedwith a motor deficit in the foot. In addition, two ofthe three patients in this group who were eventu-ally found to have "lost" their Babinski sign, atthe same time regained full control of foot move-ments while other pathological signs persisted(cases 5 and 6). Lesions of the neuraxis whichcause proximal weakness alone should not lead usto expect a Babinski sign. One patient who"lacked" it (case 3) showed weakness of hip andknee flexion (MRC 4) and reduced abdominalreflexes, but power and skill in the foot werenormal.The next most frequent sign accompanying the
Babinski response was increase of tendon reflexes(74%). However, apart from being absent in a
quarter of the 50 patients with a unilateral Bab-inski sign, it also persisted in two cases where up-going toe sign and motor impairment of the footsimultaneously disappeared. In other words, theBabinski response and hyperreflexia regularlyoccur without one another, and patients with in-creased tendon jerks alone are not "entitled" to aBabinski sign (cases 2 and 4). All other signs werefound in half the patients at most, and could beattributed even less to the same part of the lesionas the Babinski response. Associated dorsiflexionof the hallux on ipsilateral or contralateral hipflexion was found infrequently, and on the controlside as well as on the side of the Babinski sign(Table 2). A recent claim that the "crossed up-going toe sign" can be regarded as a reliable andsometimes superior test (Hindfelt et al., 1976) isnot confirmed by my study, nor by earlier work(Striimpell, 1887; Brain and Wilkinson, 1959).
Within the pyramidal tract syndrome, only im-pairment of skilled foot movements is so intimatelyconnected with occurrence of the Babinski signthat these two pathological features can be assumedto result from a disturbance of identical or closelyrelated pyramidal tract fibres.
ACTIVITY OF THE FLEXION REFLEX
The Babinski sign is part of the flexion reflexsynergy, and it is rarely the minimal response, asnoted earlier (Walshe, 1914). Of 50 patients inwhom the stimulus intensity was not higher thannecessary to elicit a clear upgoing toe response,more proximal leg muscles were activated in 48.In cases where a Babinski sign is absent in a weakfoot, we may, therefore, infer from an absent orfeeble response in proximal leg flexors that thereis insufficient activity in the reflex pathways con-
J. van Gijn
verging upon the extensor hallucis longus muscle.This inexcitability may be the result of individualvariation (case 8) or of initial reflex depression(case 9), common after acute spinal transection(Guttmann, 1976). Also, a Babinski sign candisappear after the acute episode because theactivity of the flexion reflex dwindles (case 7).
If a Babinski sign does appear, it cannot be ex-plained simply by a pathological overactivity of theflexion reflex as a whole, because it was as often asnot accompanied by an exaggerated response inproximal flexor muscles. Moreover, asymmetry ofthe flexion reflex can persist after disappearance ofa Babinski sign (case 5). As release of the entireflexion reflex involves several segments, it is prob-ably caused by dysfunction of projections to inter-neurones in the intermediate zone of the spinalgrey matter.The identity of the descending pathways con-
cerned with control of the flexion reflex has beeninvestigated only in animals. In the cat, inter-neurones mediating the flexion reflex are tonicallyinhibited by the medial portion of the reticularformation of the brainstem (Eccles and Lundberg,1959; Holmqvist and Lundberg, 1961), and theyare facilitated by the pyramidal tract (Lundbergand Voorhoeve, 1962) and by the rubrospinal tract(Hongo et al., 1972). In man, an argument for atleast partial control of the flexion reflex by brain-stem centres is that flexor spasms are much morecommon after spinal lesions than in cerebraldisease.
RELEASE OF THE BABINSKI SIGNThe results show that the Babinski response can bereleased separately from the flexion reflex as awhole, and that it is almost invariably associatedwith motor impairment of the foot. In some casesthis motor impairment is manifested only by sloing down, dysrhythmia, or reduced fractionationof foot movements. The capacity for independentand fast movements is mediated by direct corticalprojections to individual motoneurones (Kuypers,1973). Because loss of this ability alone is ap-parently sufficient to permit release of the Babinskisign, the corticospinal "shielding" of extensorhallucis longus motoneurones from activity in theflexion reflex arc must have its impact at or nearthese motoneurones. In other words, an excitatoryaction (direct and selective innervation of distalmotoneurones) is closely connected with an in-hibitory action (counteracting the recruitment ofthe extensor hallucis longus via the flexion reflexpathways). The inhibitory neurone might be acti-vated by collaterals of corticomotoneuronal fibresfor the extensor hallucis longus, or consist in
Protected by copyright.
on 7 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.10.865 on 1 O
ctober 1978. Dow
nloaded from
The Babinski sign and the pyramidal syndrome
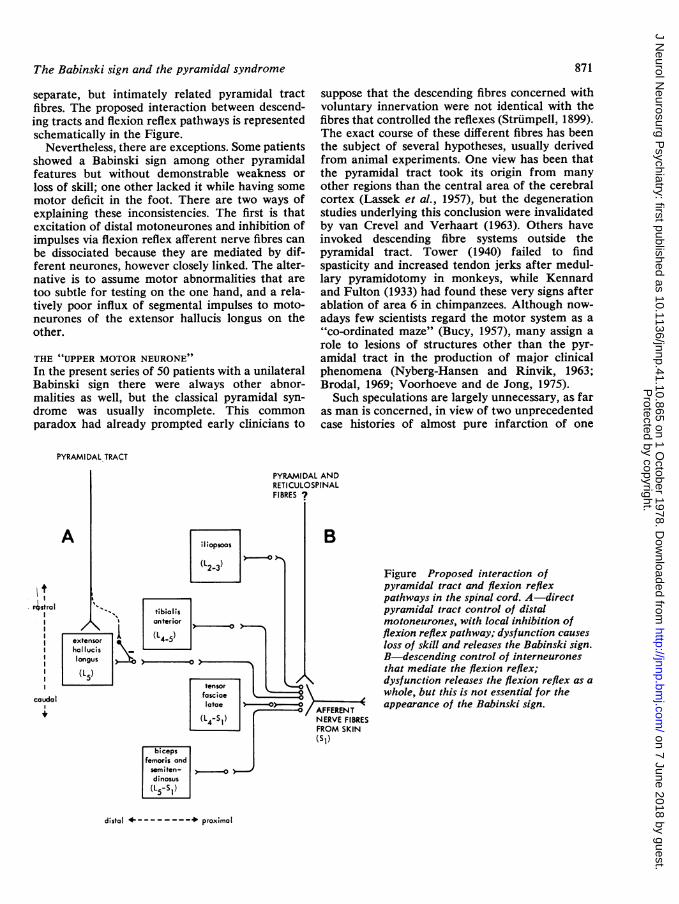
separate, but intimately related pyramidal tractfibres. The proposed interaction between descend-ing tracts and flexion reflex pathways is representedschematically in the Figure.
Nevertheless, there are exceptions. Some patientsshowed a Babinski sign among other pyramidalfeatures but without demonstrable weakness orloss of skill; one other lacked it while having somemotor deficit in the foot. There are two ways ofexplaining these inconsistencies. The first is thatexcitation of distal motoneurones and inhibition ofimpulses via flexion reflex afferent nerve fibres canbe dissociated because they are mediated by dif-ferent neurones, however closely linked. The alter-native is to assume motor abnormalities that aretoo subtle for testing on the one hand, and a rela-tively poor influx of segmental impulses to moto-neurones of the extensor hallucis longus on theother.
THE "UPPER MOTOR NEURONE"In the present series of 50 patients with a unilateralBabinski sign there were always other abnor-malities as well, but the classical pyramidal syn-drome was usually incomplete. This commonparadox had already prompted early clinicians to
suppose that the descending fibres concerned withvoluntary innervation were not identical with thefibres that controlled the reflexes (Strumpell, 1899).The exact course of these different fibres has beenthe subject of several hypotheses, usually derivedfrom animal experiments. One view has been thatthe pyramidal tract took its origin from manyother regions than the central area of the cerebralcortex (Lassek et al., 1957), but the degenerationstudies underlying this conclusion were invalidatedby van Crevel and Verhaart (1963). Others haveinvoked descending fibre systems outside thepyramidal tract. Tower (1940) failed to findspasticity and increased tendon jerks after medul-lary pyramidotomy in monkeys, while Kennardand Fulton (1933) had found these very signs afterablation of area 6 in chimpanzees. Although now-adays few scientists regard the motor system as a"co-ordinated maze" (Bucy, 1957), many assign arole to lesions of structures other than the pyr-amidal tract in the production of major clinicalphenomena (Nyberg-Hansen and Rinvik, 1963;Brodal, 1969; Voorhoeve and de Jong, 1975).Such speculations are largely unnecessary, as far
as man is concerned, in view of two unprecedentedcase histories of almost pure infarction of one
PYRAMIDAL TRACT
A
4stralI
_caudal
PYRAMIDAL ANDRETICULOSPINALFIBRES ?
Figure Proposed interaction ofpyramidal tract and flexion reflexpathways in the spinal cord. A-directpyramidal tract control of distalmotoneurones, with local inhibition offlexion reflex pathway; dysfunction causesloss of skill and releases the Babinski sign.B-descending control of interneuronesthat mediate the flexion reflex;dysfunction releases the flexion reflex as awhole, but this is not essential for theappearance of the Babinski sign.
distal + proximol
871
Protected by copyright.
on 7 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.10.865 on 1 O
ctober 1978. Dow
nloaded from
872
medullary pyramid (Chokroverty et al., 1975;Leestma and Noronha, 1976). The following signswere noted on the contralateral side: weakness,Babinski sign, increased tendon jerks, and-in onlyone patient-spasticity. These observations cannotexclude that interference with other descendingfibre systems contributes to the appearance ofclinical signs, and changes in abdominal and flexionreflexes were not recorded. However, it is evenmore important to realise that the fibres passingthrough the medullary pyramids are heterogeneousin terms of termination, regardless of origin(Kuypers, 1973). The tract consists only partly of"upper motor neurones" in the sense of directcorticomotoneuronal connections (Verhaart, 1962).Within the pyramidal syndrome of the leg, onlyan impairment of skilled foot movements and-closely linked to it-the Babinski sign, can beattributed to a disturbance of these direct connec-tions. Other signs must depend on different pro-jections, to the interneuronal zone in particular.Partial lesions of this diverging pyramidal tractcannot give a uniform clinical picture.
I am grateful to Dr H. van Crevel (Rotterdam)and Dr I. R. Williams (Liverpool) for many help-ful comments. Dr H. J. A. Schouten gave adviceon statistics.
References
Babinski, J. (1885). Recherches sur l'anatomie patho-logique de la sclerose en plaques et etude compara-tive des diverses varietes de scleroses de la moelle.Archives de Physiologie Normale et Pathologique,17, 186-207.
Babinski, J. (1896). Sur le reflexe cutan6 plantaire danscertaines affections organiques du syste;me nerveuxcentral. Comptes Rendus des Seances de la Societede Biologie, 48, 207-208.
Babinski, J. (1897). Discussion, Congres internationalde Neurologie, Brussels. Bulletin Medical, 11, 896.
Brain, W. R., and Wilkinson, M. (1959). Observationson the extensor plantar reflex and its relationshipto the functions of the pyramidal tract. Brain, 82,297-320.
Brodal, A. (1969). Neurological Anatomy in Relationto Clinical Medicine. Second edition. Oxford Univer-sity Press: New York and London.
Bucy, P. C. (1957). Is there a pyramidal tract? Brain,80, 376-392.
Chokroverty, S., Rubino, F. A., and Haller, C. (1975).Pure motor hemiplegia due to pyramidal infarction.Archives of Neurology (Chicago), 32, 647-648.
Crevel, H. van, and Verhaart, W. J. C. (1963). The"exact" origin of the pyramidal tract. Journal ofAnatomy, 97, 495-515.
Dohrmann, G. J., and Nowack, W. J. (1974). Relation-ship between various clinical signs in lesions of the
J. van Gijn
descending motor system. Diseases of the NervousSystem, 35, 375-377.
Eccles, R. M., and Lundberg, A. (1959). Supraspinalcontrol of interneurones mediating spinal reflexes.Journal of Physiology, 147, 565-584.
Gijn, J. van (1975). Babinski response: stimulus andeffector. Journal of Neurology, Neurosurgery, andPsychiatry, 38, 180-186.
Graeffner (1906). Einige Studien uiber Reflexe, be-sonders an Hemiplegikern. Munchener MedizinischeWochenschrift, 53, 489-491.
Guttmann, L. (1976) Spinal Cord Injuries-Compre-hensive Management and Research. Second edition.Blackwell: Oxford.
Hindfelt, B., Rosen, I., and Hanko, J. (1976). Thesignificance of a crossed extensor hallucis responsein neurological disorders: a comparison with theBabinski sign. Acta Neurologica Scandinavica, 53,241-250.
Holmqvist, B., and Lundberg, A. (1961). Differentialsupraspinal control of synaptic actions evoked byvolleys in the flexion reflex afferents in alpha moto-neurones. Acta Physiologica Scandinavica, 54, 1-51.
Hongo, T., Jankowska, E., and Lundberg, A. (1972).The rubrospinal tract. IV. Effects on interneurones.Experimental Brain Research, 15, 54-78.
Kennard, M. A., and Fulton, J. F. (1933). The local-ising significance of spasticity, reflex grasping, andthe signs of Babinski and Rossolimo. Brain, 56, 213-225.
Kuypers, H. G. J. M. (1973). The anatomical organisa-tion of the descending pathways and their contri-butions to motor control especially in primates. InNew Developments in Electromyography and Clini-cal Neurophysiology. Vol. 3, pp. 38-68. Edited byJ. E. Desmedt. Karger: Basel.
Landau, W. M., and Clare, M. H. (1959). The plantarreflex in man, with special reference to some con-ditions where the extensor response is unexpectedlyabsent. Brain, 82, 321-355.
Lassek, A. M. (1944). The human pyramidal tract. X.The Babinski sign and destruction of the pyramidaltract. Archives of Neurology and Psychiatry(Chicago), 52, 484-494.
Lassek, A. M. (1945). The human pyramidal tract. Xi.Correlation of the Babinski sign and the pyramidalsyndrome. Archives of Neurology and Psychiatry(Chicago), 53, 375-377.
Lassek, A. M., Woolsey, C. N., Walker, A. E., Boshes,B., and Rose, A. S. (1957). The pyramidal tractsymposium of inquiry. Neurology (Minneapolis), 7,496-509.
Leestma, J. E., and Noronha, A. (1976). Pure motorhemiplegia, medullary pyramid lesion, and olivaryhypertrophy. Journal of Neurology, Neurosurgery,and Psychiatry, 39, 877-884.
Lundberg, A., and Voorhoeve, P. (1962). Effects fromthe pyramidal tract on spinal reflex arcs. A ctaPhysiologica Scandinavica, 56, 201-219.
McDonald, W. I., and Sears, T. A. (1970). The effectsof experimental demyelination on conduction in thecentral nervous system. Brain, 93, 583-598.
Protected by copyright.
on 7 June 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.10.865 on 1 O
ctober 1978. Dow
nloaded from
The Babinski sign and the pyramidal syndrome
Marie, P., and Foix, Ch. (1912). Les reflexes d'auto-matisme medullaire et le phenomene des raccourcis-seurs; leur valeur semiologique, leur significationphysiologique. Revue Neurologique, 23, 657-676.
Mayo Clinic (1963). Clinical Examination inNeurology. Second edition. Saunders: Philadelphia.
Medical Research Council (1943). Aids to the Investi-gation of Peripheral Nerve Injuries. (War Memoran-dum No. 7). Her Majesty's Stationery Office:London.
Mills, C. K. (1900). A case of unilateral progressiveascending paralysis, probably representing a newform of degenerative disease. Journal of Nervousand Mental Disease, 27, 195-200.
Nathan, P. W., and Smith, M. C. (1955). The Babinskiresponse: a review and new observations. Journal ofNeurology, Neurosurgery, and Psychiatry, 18, 250-259.
Nyberg-Hansen, R., and Rinvik, E. (1963). Somecomments on the pyramidal tract, with special refer-ence to its individual variations in man. A cta Neuro-logica Scandinavica, 39, 1-30.
Potts, C. S., and Weisenburg, T. H. (1910). Tumourlimited to the arm centre, with a discussion of therelation of the Babinski reflex to motor lesions, itbeing present only if the leg fibres are implicated.Review of Neurology and Psychiatry, 8, 577-586.
873
Sharrard, W. J. W. (1955). The distribution of thepermanent paralysis in the lower limb in poliomy-elitis-a clinical and pathological study. Journal ofBone and Joint Surgery, 37, 540-558.
Striumpell, A. von (1887). Ueber einige bei Nerven-kranken haufig vorkommende abnorme Mitbewe-gungen im Fusse und in den Zehen. NeurologischesCentralblatt, 6, 1-4.
Strumpell, A. von (1899). Zur Kenntnis der Haut- undSehnenreflexe bei Nervenkranken. Deutsche Zeit-schrift fur Nervenheilkunde, 15, 254-273.
Tower, S. S. (1940). Pyramidal lesions in the monkey.Brain, 63, 36-90.
Verhaart, W. J. C. (1962). The pyramidal tract-itsstructure and functions in man and animals.World Neurology, 3, 43-53.
Voorhoeve, P. E., and de Jong, J. M. B. V. (1975).Proposal for a new nomenclature of some well-known clinical syndromes. Clinical Neurology andNeurosurgery, 78, 10-18.
Walshe, F. M. R. (1914). The physiological significanceof the reflex phenomena in spastic paralysis of thelower limbs. Brain, 37, 269-336.
Walshe, F. M. R. (1956). The Babinski plantar re-sponse, its forms, and its physiological and pathologi-cal significance. Brain, 79, 529-556. P
rotected by copyright. on 7 June 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.41.10.865 on 1 October 1978. D
ownloaded from














![Index [assets.cambridge.org]assets.cambridge.org/97805211/92583/index/9780521192583_index… · autonomic dysreflexia, SCI, 552, 573 Babinski response methodology, 341 upper motoneurone](https://img.pdfslide.us/doc/110x75/5edd2d3bad6a402d66682b6a/index-autonomic-dysreflexia-sci-552-573-babinski-response-methodology-341.jpg)














