Embed Size (px)
Citation preview

I CASE REPORT
Babinski-Nageotte Syndrome due toVertebral Artery Dissection
Fumi Irie, Kazunori TOYODA,Noriko HAGIWARA,Shigeru FUJIMOTOand Yasushi OKADA
Abstract
Hemimedullary infarction, which presents Babinski-Nageotte syndrome, has been mainly reported to resultfrom atherosclerotic occlusion of the vertebral artery. A54-year-old housewife with right nuchal pain developedWallenberg's syndrome followed by left hemiparesis.Diffusion-weighted magnetic resonance imaging docu-mented fresh infarcts in the right hemimedulla and rightdorsal cerebellum. Angiography revealed dissection ofthe right vertebral artery as a cause of the infarcts.Anterograde progression of the dissection might causestepwise evolution of her neurological symptoms.(Internal Medicine 42: 871-874, 2003)
Key words: brain infarction, medulla oblongata, brainstem,Babinski-Nageotte syndrome, dissection, verte-bral artery
Introduction
Since Babinski and Nageotte described an autopsy case ofischemic lesion involving the unilateral medulla oblongataone hundred years ago (1), the identity of hemimedullarystroke has been in dispute because both medial and lateralmedullary infarctions rarely occur simultaneously and vascu-lar supplies of medial and lateral medulla usually differ. Themedulla oblongata can be divided into 4 zones according toits arterial circulation; the medianzone which is perfused bythe anterior spinal artery (ASA) at the level of lower medullaand the upper bulbar branches at the level of upper medulla,the paramedian zone by ASA, posterior inferior cerebellarartery (PICA) and middle bulbar branches, the lateral zoneby PICA and lower bulbar branches, and the dorsal zone byPICA and posterior spinal artery (2, 3). Dissection of thevertebral artery (VA) is a possible pathology that involves
ASA, PICA, and multiple bulbar branches and causes infarc-tions in both the medial and lateral medulla, although suchinfarctions due to dissection of the VAhas not yet been re-ported in detail. Here we describe a patient with hemi-medullary syndrome caused by unilateral VA dissection.Diffusion-weighted magnetic resonance imaging (DWI-MRI) was available for demonstration of her hyperacuteischemic lesion.
Case ReportA 54-year-old housewife without risk factors for arterio-sclerosis including hypertension, diabetes, and hyper-
lipidemia started to suffer from right nuchal pain after onehour of swimming, which she habitually enjoyed three timesa week. One month later, she suddenly felt nausea and thenlost consciousness for several minutes at her home, and wasadmitted to a local hospital. She complained of vertigo then.The next morning, she suddenly developed weakness of theleft limbs and was transferred to our stroke center.On arrival 3 hours after progression of the symptoms, shewas somnolent but cooperative and oriented. Her blood pres-sure was 184/88 mmHgand pulse rate was 66/min and regu-lar. Her pupils were round and isocoric. Her ocularmovements were full and smooth, with multidirectionalnystagmus on vertical and horizontal gaze. There was rightside paresis of her face, palate, and tongue. She was
dysarthric and dysphagic, with impaired gag reflex. She hadan almost complete motor palsy of the left limbs with in-creased left deep tendon reflexes and positive left Babinskireflex. Her right limbs were ataxic. Perception of pain andtemperature was decreased on the right side of the face andleft limbs. Deep sensations were intact. Paresthesia was pre-sent in all extremities.
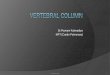
DWI on the hospitalization day demonstrated hyper-intense lesions at the right half of the medulla oblongata andthe ipsilateral dorsal cerebellar hemisphere corresponding toPICA territory (Fig. 1A). Magnetic resonance angiography
From the Department of Cerebrovascular Disease and Clinical Research Institute, National Kyushu Medical Center, FukuokaReceived for publication January 23, 2003; Accepted for publication May 2, 2003Reprint requests should be addressed to Dr. Kazunori Toyoda, the Department of Cerebrovascular Disease, National Kyushu Medical Center, 1-8-1
Jigyohama, Chuo-ku, Fukuoka 8 10-8563
Internal Medicine Vol. 42, No. 9 (September 2003) 871

Irie et al
Figure 1. A: Diffusion-weighted MRIon the hospitalization day. Areas of hyperintense signal in the right medial (arrow-head) and lateral (arrow) half of the medulla oblongata and ipsilateral dorsal cerebellar hemisphere (PICA territory) aredemonstrated. B: Digital subtraction angiography of right VAon day 3. A frontal view shows a long segment of high-gradestenosis extending from Cl level with irregularity and occlusion at the base of the skull (arrow). C: Tl-weighted (fat sup-pressed) magnetic resonance imaging on day 9 of axial section demonstrates "crescent sign" in the right VA(arrow). D: MRangiography on day 22 revealed right VAand PICA (arrow), although indistinct compared with left VA.
(MRA) did not delineate right VA or right PICA. Cervicalechography documented narrow right VAwithout diastolicflow signal, indicating occlusion of right VAproximal toright PICA (4). These neuroradiological studies did not
document any parenchymal or vascular lesions in the ante-rior circulation. Blood tests were normal. Neither echocardi-ography nor prolonged electrocardiography revealed anycardiac source of emboli. Under probable diagnosis of dis-section of right VA, we started continuous intravenous infu-sion of heparin (10,000 U/day, 14 days) within an hour afterher arrival. The left hemiplegia suddenly recovered 2 hourslater, but returned to the severe state again during the next 4hours. Intravenous administration of urokinase (12,000 U)was then added. On day 3, right Homer's sign became appar-ent.On digital subtraction angiogram (DSA) on day 3, rightVAbecame narrow from the Cl level and occluded at thelevel of foramen magnum(Fig. IB). The basilar artery and
its branches were intact via left VA. Anterior circulation wasalso intact. Tl-weighted fat-suppressed MRI on day 9showed a crescentic hyperintense area in the right VAat thelevel of foramen magnumindicating intramural hematoma inthe false lumen (Fig. 1C). MRA on day 22 documentedrecanalization of right VA to the union (Fig. ID). T2-
weighted MRI on the same day delineated medullary andcerebellar infarcts in an area identical to that in the initialDWI. Based on these findings, we finally diagnosed rightVApathology as arterial dissection.Her nystagmus and right facial paresis disappeared within2 weeks. Bulbar palsy and motor and sensory deficits in theleft limbs were improved to some extent. Ataxia in the rightlimb persisted. On discharge 3 weeks after admission, sheneeded a wheelchair for transfer.
872 Internal Medicine Vol. 42, No. 9 (September 2003)

Hemimedullary Infarction
Discussion
This is the first detailed case report of hemimedullary in-farction due to VAdissection with radiological confirmation.Sudden onset of symptoms, tapering occlusion and laterrecanalization of VA, crescent sign on MRI, and lack ofatherosclerosis or cardioembolic sources indicate VAdissec-tion as a cause of infarction in this patient (5). Neck pain wasreported to precede other manifestations of VAdissectionfor « 12 days up to a maximumof 30 days, although head-ache preceded for a much shorter time (6). Thus in this case,the one-month history of nuchal pain after swimming mighthave been a warning sign of severe VAdissection.
Hemimedullary infarction is a rare disease. Twelve pa-
tients with infarction have been reported, to our knowledge,with pathological or radiological documentation (Table 1) (1 ,3, 7-16). All patients had a unilateral medullary lesion anda patient by Nakane et al (13) had ipsilateral cerebellar in-farct in the PICA territory, like the present patient. VAoc-clusion was a leading vascular pathology, caused by syphilisand endartertis in earlier reports, and by atherosclerosis withhypertension or diabetes in recent reports. VAdissection wasreported as an etiology of hemimedullary infarction in onlyone study, without a detailed case presentation (3).Spontaneous VAdissection occurs in 1 to 1.5 per 100,000person-years, and is an important cause of ischemic stroke inyoung and middle-aged patients (5). This vascular disease isa frequent cause of lateral medullary infarction. A neuro-radiological study indicates that more than half of patientswith lateral medullary infarction had definite or probable VAdissection (17). Contrarily, the dissection was rarely reportedto cause medial medullary infarction (18, 19). In our analysis
of 1 1 patients with medial medullary infarction, only one pa-tient (9%) was suspected to have VA dissection (19).Another study however, reported the 3 among 7 patients(43%) with medial medullary infarction had spontaneousextracranial VA dissection (3). Thus, the frequency of VAdissection in medial medullary infarction has been disputed.Because bilateral ASAsusually supply the medial medullaand unilateral PICA supplies the lateral medulla, unilateralVAdissection does not seem to cause medial medullary in-farction as often as lateral one. The initial symptomsfor thepresent patient correspond to PICA-territorial syndrome.
Pyramidal symptoms, resulting from medial medullary in-farction, appeared on the second day. The time course sug-gests anterograde progression of her arterial dissection; itmight have reached the orifice of PICA on the day of strokeonset, and the orifice of ASAand upper bulbar branches onday2.
In early clinical reports, hemimedullary syndrome wasgenerally fatal, especially if complicated with respiratorydisturbances. The syndrome was so uncommonthat it wasdifficult to make the topographical and etiological diagnoseswhile patients were alive. Here, the advent of new
neuroimaging strategies including DWIand MRAled todefinite topographical diagnosis and the probable etiologicaldiagnosis as arterial dissection and to the immediatestart oftreatment using urokinase and heparin within 4 hours afterstroke progression of this patient. The quick treatment mightcause transient recovery from the hemiparesis, but did notend in good functional outcome without assistance on dis-charge. Although intravenous and local intra-arterial
thrombolysis is feasible in stroke caused by cervical arterialdissection (20, 21), further studies are necessary to establish
Table 1. Previous Reports on Hemimedullary InfarctionAuthors ^ Siteof o. ,. ., , . .T Meansof
Year . _ Site of arterial occlusion Etiology([ ] ; reference) infarct diagnosis
Reinhold [7] 1 894 R RVA (intracranial) Endarteritis AutopsyBabinski and Nageotte [1] 1902 L LVA(distal end), BA Meningovascular syphillis AutopsyMarinesco and Draganesco 1923 R RVA,stenosis of BA Atherosclerosis Autopsy
[8] Lipoid, crystalline
Pines and Gilinsky [9] 1930 L LVA Thrombus AutopsyHarris and Hauser [10] 1931 R stenosis of RVA(distal end) Thrombus, infection AutopsyDavison [11] 1937 L Not verified in the autopsy Atherosclerosis Autopsy
Mossuto-Agatiello and 1990 L LVA(rudimentary), Atherosclerosis MRI, angiographyKniahynicki [12] stenosis of RVANakane et al [13] 1991 L LVA, stenosis ofRVA Atherosclerosis, hyperten- MRI, angiography
sion, diabetesChang et al [14] 1993 L Not documented Atherosclerosis, hyperten- MRI
sion
Bassetti et al [3] 1997 L Not documented Dissection of VA MRI, angiographyBassetti et al [3] 1997 L Not documented Cardiac embolism MRI, angiography
Minami et al [15] 2000 R RVA Hypertension, smoking MRI, MRADe Freitas et al [16] 2001 R Severe stenosis of RVA Hypertension, diabetes MRI, MRA
R: right, L: left, VA: vertebral artery, BA: basilar artery.
Internal Medicine Vol. 42, No. 9 (September 2003) 873

Irie et al
the appropriate acute management.
Acknowledgements: This study was partially supported by the JapaneseMinistry of Health, Labour and Welfare (12C-2).
References1) Babinski J, Nageotte J. Hemiasynergie, lateropulsion et myosis
bulbaires avec hemianesthesie et hemiplegie croisees. Rev Neurol(Paris) 10: 358-365, 1902.
2) Duvernoy HM. The Human Brain Stem and Cerebellum. SpringerVerlag, Wien, 1995.3) Bassetti C, Bogousslavsky J, Mattle H, Bernasconi A. Medial
medullary stroke: report of seven patients and review of the literature.Neurology 48: 882-890, 1997.4) Kimura K, Yasaka M, Moriyasu H, Tsuchiya T, Yamaguchi T.
Ultrasonographic evaluation of vertebral artery to detect vertebrobasilaraxis occlusion. Stroke 25: 1006-1009, 1994.
5) Schievink WI. Spontaneous dissection of the carotid and vertebral ar-teries. N Engl J Med 344: 898-906, 2001.
6) Silbert PL, Mokri B, Schievink WI. Headache and neck pain in sponta-neous internal carotid and vertebral artery dissections. Neurology 45:1517-1522, 1995.
7) Reinhold H. Beitrage zur Pathologie der acuten Erweichungen des Ponsund der oblongata. Zugleich ein Beitrag zur Lehre von der "bulbarenAtaxie". Dtsch Z Nervenheilkd 5: 351-374, 1894.
8) Marinesco G, Draganesco S. Hemisyndrome bulbaire relevant d'unramollissement de l'etage moyen du bulbe, suite de trombus de l'arterevertebrale droite. Ann Med 13: 1-199, 1923.
9) Pines L, Gilinsky E. Zur Vaskularization der Medulla oblongata. Arch.
Psychiatr Nervenkr 90: 177-184, 1930.10) Harris TH, Hauser A. Occlusion of the right posterior inferiorcerebellar artery and right vertebral artery. Arch Neurol Psychiatry 26:
396-400, 1931.
ll) Davison C. Syndrome of the anterior spinal artery of the medulla ob-longata. Arch Neurol Psychiatry 37: 91-107, 1937.
12) Mossuto-Agatiello L, Kniahynicki C. The hemimedullary syndrome:case report and review of the literature. J Neurol 237: 208-212, 1990.
13) Nakane H, Okada Y, Sadoshima S, Fujishima M. Babinski-Nageottesyndrome on magnetic resonance imaging. Stroke 22: 272-275, 1991.
14) Chang YY, Wu HS, Chen WH, Liu JS, Chen SS. Babinski-Nageottesyndrome: a case report. Kaohsiung J Med Sci (Gaoxing Yi Xue KeXue Za Zhi) 9: 595-598, 1993.
15) Minami M, Ono S, Nawa T, Miki K, Mizutani T. A case report of cen-tral respiratory failure due to hemimedullary syndrome. Clin Neurol(Rinsho Shinkeigaku) 40: 746-749, 2000.
16) De Freitas GR, Moll J, Araujo AQ. The Babinski-Nageotte syndrome.Neurology 56: 1604, 2001.
17) Hosoya T, Nagahata M, Yamaguchi K. Prevalence of vertebral arterydissection in Wallenberg syndrome: neuroradiological analysis of 93patients in the Tohoku District, Japan. Radiat Med 14: 241-246, 1996.
18) Ho KL, Meyer KR. The medial medullary syndrome. Arch Neurol 38:385-387, 1981.
19) Toyoda K, Imamura T, Saku Y, et al. Medial medullary infarction:analyses of eleven patients. Neurology 47: 1 141-1 147, 1996.
20) Derex L, Nighoghossian N, Turjman F, et al. Intravenous tPA in acuteischemic stroke related to internal carotid artery dissection. Neurology
54: 2159-2161, 2000.
21) Arnold M, Nedeltchev K, Sturzenegger M, et al. Thrombolysis in pa-tients with acute stroke caused by cervical artery dissection: analysis of9 patients and review of the literature. Arch Neurol 59: 549-553, 2002.
874 Internal Medicine Vol. 42, No. 9 (September 2003)