Embed Size (px)
Citation preview

Frans GJ Waanders
Perfusionist
StAntonius Ziekenhuis
The Netherlands
The Antonius experience of 14 years using MiECC
Off-Pump mid 90rsquos Cardiac Surgery
less invasive than ECC
the quality and amount of anastomoses is
doubtfull
Not many surgeons skilled in off-pump surgery
Technical more demanding for surgeon and
anesthesiologist
Market penetration world wide 15-20
Totally minimized extracorporeal
circulation an important benefit
for coronary artery bypass grafting
in Jehovahs witnessesVaislic C Bical O Farge C Gaillard D Ponzio O Ollivier Y Abdelmoumen Y
Robine B Souffrant G Bouharaoua T
Centre Medico Chirurgical Parly 2 Le Chesnay France Claudevaislichotmailcom
No homologous Bloodtransfusion
Prospective randomized n=40 (20 MECC)
Study results - Inflammation
Elastase IL-6 β-TG S-100βTNF-α
Conclusion bdquoThe MECC system may provide a minimally invasive solution to maintain the high surgical standards of CABG with CPB and it may avoid many deleterious effects of standard CPB methodsldquo
Increased higher risk population
Older age
Lungdisease (COPD etc)
Kidney dysfunction
Brain (former stroke)
Poor LV-contractions
Peripheral vascular disease
Carotid disease
Aorta Calcium plaques
Combinations
cECC
Large Foreign Surface
High volume Cardioplegia
Cardiotomy
Suction
Roller-Pump
BloodGas
Interface
Hemodilution
Development Equipment
mECC provides the safety and surgical quality of CABG with ECC while achieving the biocompatibility of OPCAB
2002 Visit
Regensburg group
mECC Principle and Goal
Less hemodilution
Less surface arae ndash limiting strange surface area
Closed system ndash limiting blood-air contact
Better Organ protection
Less heparin
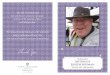
From cECC to mECC (2002)
Start Antonius Hospital
mECC 2002
bull Aorta venting intermittently
bull Air possibility in system
bull Aortic needle
bull Sample line
bull Venous line
mECC Air DripChamber
DripChamber
Aortic needle
vent to CS
Aortic needle vent to
Drip chamber
From DripChamber
to venous inlet
Sample line to
DripChamber
Venous line
2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
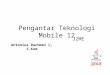
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Off-Pump mid 90rsquos Cardiac Surgery
less invasive than ECC
the quality and amount of anastomoses is
doubtfull
Not many surgeons skilled in off-pump surgery
Technical more demanding for surgeon and
anesthesiologist
Market penetration world wide 15-20
Totally minimized extracorporeal
circulation an important benefit
for coronary artery bypass grafting
in Jehovahs witnessesVaislic C Bical O Farge C Gaillard D Ponzio O Ollivier Y Abdelmoumen Y
Robine B Souffrant G Bouharaoua T
Centre Medico Chirurgical Parly 2 Le Chesnay France Claudevaislichotmailcom
No homologous Bloodtransfusion
Prospective randomized n=40 (20 MECC)
Study results - Inflammation
Elastase IL-6 β-TG S-100βTNF-α
Conclusion bdquoThe MECC system may provide a minimally invasive solution to maintain the high surgical standards of CABG with CPB and it may avoid many deleterious effects of standard CPB methodsldquo
Increased higher risk population
Older age
Lungdisease (COPD etc)
Kidney dysfunction
Brain (former stroke)
Poor LV-contractions
Peripheral vascular disease
Carotid disease
Aorta Calcium plaques
Combinations
cECC
Large Foreign Surface
High volume Cardioplegia
Cardiotomy
Suction
Roller-Pump
BloodGas
Interface
Hemodilution
Development Equipment
mECC provides the safety and surgical quality of CABG with ECC while achieving the biocompatibility of OPCAB
2002 Visit
Regensburg group
mECC Principle and Goal
Less hemodilution
Less surface arae ndash limiting strange surface area
Closed system ndash limiting blood-air contact
Better Organ protection
Less heparin
From cECC to mECC (2002)
Start Antonius Hospital
mECC 2002
bull Aorta venting intermittently
bull Air possibility in system
bull Aortic needle
bull Sample line
bull Venous line
mECC Air DripChamber
DripChamber
Aortic needle
vent to CS
Aortic needle vent to
Drip chamber
From DripChamber
to venous inlet
Sample line to
DripChamber
Venous line
2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Totally minimized extracorporeal
circulation an important benefit
for coronary artery bypass grafting
in Jehovahs witnessesVaislic C Bical O Farge C Gaillard D Ponzio O Ollivier Y Abdelmoumen Y
Robine B Souffrant G Bouharaoua T
Centre Medico Chirurgical Parly 2 Le Chesnay France Claudevaislichotmailcom
No homologous Bloodtransfusion
Prospective randomized n=40 (20 MECC)
Study results - Inflammation
Elastase IL-6 β-TG S-100βTNF-α
Conclusion bdquoThe MECC system may provide a minimally invasive solution to maintain the high surgical standards of CABG with CPB and it may avoid many deleterious effects of standard CPB methodsldquo
Increased higher risk population
Older age
Lungdisease (COPD etc)
Kidney dysfunction
Brain (former stroke)
Poor LV-contractions
Peripheral vascular disease
Carotid disease
Aorta Calcium plaques
Combinations
cECC
Large Foreign Surface
High volume Cardioplegia
Cardiotomy
Suction
Roller-Pump
BloodGas
Interface
Hemodilution
Development Equipment
mECC provides the safety and surgical quality of CABG with ECC while achieving the biocompatibility of OPCAB
2002 Visit
Regensburg group
mECC Principle and Goal
Less hemodilution
Less surface arae ndash limiting strange surface area
Closed system ndash limiting blood-air contact
Better Organ protection
Less heparin
From cECC to mECC (2002)
Start Antonius Hospital
mECC 2002
bull Aorta venting intermittently
bull Air possibility in system
bull Aortic needle
bull Sample line
bull Venous line
mECC Air DripChamber
DripChamber
Aortic needle
vent to CS
Aortic needle vent to
Drip chamber
From DripChamber
to venous inlet
Sample line to
DripChamber
Venous line
2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Prospective randomized n=40 (20 MECC)
Study results - Inflammation
Elastase IL-6 β-TG S-100βTNF-α
Conclusion bdquoThe MECC system may provide a minimally invasive solution to maintain the high surgical standards of CABG with CPB and it may avoid many deleterious effects of standard CPB methodsldquo
Increased higher risk population
Older age
Lungdisease (COPD etc)
Kidney dysfunction
Brain (former stroke)
Poor LV-contractions
Peripheral vascular disease
Carotid disease
Aorta Calcium plaques
Combinations
cECC
Large Foreign Surface
High volume Cardioplegia
Cardiotomy
Suction
Roller-Pump
BloodGas
Interface
Hemodilution
Development Equipment
mECC provides the safety and surgical quality of CABG with ECC while achieving the biocompatibility of OPCAB
2002 Visit
Regensburg group
mECC Principle and Goal
Less hemodilution
Less surface arae ndash limiting strange surface area
Closed system ndash limiting blood-air contact
Better Organ protection
Less heparin
From cECC to mECC (2002)
Start Antonius Hospital
mECC 2002
bull Aorta venting intermittently
bull Air possibility in system
bull Aortic needle
bull Sample line
bull Venous line
mECC Air DripChamber
DripChamber
Aortic needle
vent to CS
Aortic needle vent to
Drip chamber
From DripChamber
to venous inlet
Sample line to
DripChamber
Venous line
2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Increased higher risk population
Older age
Lungdisease (COPD etc)
Kidney dysfunction
Brain (former stroke)
Poor LV-contractions
Peripheral vascular disease
Carotid disease
Aorta Calcium plaques
Combinations
cECC
Large Foreign Surface
High volume Cardioplegia
Cardiotomy
Suction
Roller-Pump
BloodGas
Interface
Hemodilution
Development Equipment
mECC provides the safety and surgical quality of CABG with ECC while achieving the biocompatibility of OPCAB
2002 Visit
Regensburg group
mECC Principle and Goal
Less hemodilution
Less surface arae ndash limiting strange surface area
Closed system ndash limiting blood-air contact
Better Organ protection
Less heparin
From cECC to mECC (2002)
Start Antonius Hospital
mECC 2002
bull Aorta venting intermittently
bull Air possibility in system
bull Aortic needle
bull Sample line
bull Venous line
mECC Air DripChamber
DripChamber
Aortic needle
vent to CS
Aortic needle vent to
Drip chamber
From DripChamber
to venous inlet
Sample line to
DripChamber
Venous line
2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Development Equipment
mECC provides the safety and surgical quality of CABG with ECC while achieving the biocompatibility of OPCAB
2002 Visit
Regensburg group
mECC Principle and Goal
Less hemodilution
Less surface arae ndash limiting strange surface area
Closed system ndash limiting blood-air contact
Better Organ protection
Less heparin
From cECC to mECC (2002)
Start Antonius Hospital
mECC 2002
bull Aorta venting intermittently
bull Air possibility in system
bull Aortic needle
bull Sample line
bull Venous line
mECC Air DripChamber
DripChamber
Aortic needle
vent to CS
Aortic needle vent to
Drip chamber
From DripChamber
to venous inlet
Sample line to
DripChamber
Venous line
2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

mECC provides the safety and surgical quality of CABG with ECC while achieving the biocompatibility of OPCAB
2002 Visit
Regensburg group
mECC Principle and Goal
Less hemodilution
Less surface arae ndash limiting strange surface area
Closed system ndash limiting blood-air contact
Better Organ protection
Less heparin
From cECC to mECC (2002)
Start Antonius Hospital
mECC 2002
bull Aorta venting intermittently
bull Air possibility in system
bull Aortic needle
bull Sample line
bull Venous line
mECC Air DripChamber
DripChamber
Aortic needle
vent to CS
Aortic needle vent to
Drip chamber
From DripChamber
to venous inlet
Sample line to
DripChamber
Venous line
2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

mECC Principle and Goal
Less hemodilution
Less surface arae ndash limiting strange surface area
Closed system ndash limiting blood-air contact
Better Organ protection
Less heparin
From cECC to mECC (2002)
Start Antonius Hospital
mECC 2002
bull Aorta venting intermittently
bull Air possibility in system
bull Aortic needle
bull Sample line
bull Venous line
mECC Air DripChamber
DripChamber
Aortic needle
vent to CS
Aortic needle vent to
Drip chamber
From DripChamber
to venous inlet
Sample line to
DripChamber
Venous line
2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

From cECC to mECC (2002)
Start Antonius Hospital
mECC 2002
bull Aorta venting intermittently
bull Air possibility in system
bull Aortic needle
bull Sample line
bull Venous line
mECC Air DripChamber
DripChamber
Aortic needle
vent to CS
Aortic needle vent to
Drip chamber
From DripChamber
to venous inlet
Sample line to
DripChamber
Venous line
2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

mECC 2002
bull Aorta venting intermittently
bull Air possibility in system
bull Aortic needle
bull Sample line
bull Venous line
mECC Air DripChamber
DripChamber
Aortic needle
vent to CS
Aortic needle vent to
Drip chamber
From DripChamber
to venous inlet
Sample line to
DripChamber
Venous line
2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

mECC Air DripChamber
DripChamber
Aortic needle
vent to CS
Aortic needle vent to
Drip chamber
From DripChamber
to venous inlet
Sample line to
DripChamber
Venous line
2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

2004
Venous Bubble Trap
mECC Air Handling
Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Level
DetectorAir Vent
mECC set Principle
Cell Saver
Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Further reducing primingvolume lt800 ml to 200 ml
Reduces hemodilution
Higher hematocrits
Empty heart
Luxation the heart to make proper anastomoses
Less backflow
Bloodfree field intra cardial defects like AVR
Philosophy of the mECC no blood storage
Autologous Prime
St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

St Antonius Hospital Nieuwegein The Netherlands
Retrospective 9-2002 9-2003 N =114 mECCcECC
cECC 37 vs mECC 13 Bloodproducts
Mini extracorporeal circuit for CABG initial clinical and biochemical results A comparison with conventional and off-
pump artery bypass graft concerning global oxidative stress and alveolar function WJ van Boven et al St Antonius Hospital Nieuwegein the Netherlands Perfusion 200419239-246
Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Calcified aorta
Conversion from OFF PUMP
All other CABGrsquos (80)
Indications CABG
MECC + Beating Heart MECC + Arrested Heart Off Pump
bull High risk patients for
neurologic events
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
MECC
OPCAB
CECC
0
100
200
300
400
500
600
700
800
900
1000
Tota
l num
ber
of patie
nts
per
techniq
ue
Year
MECC OPCAB CECC
Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Significant reduction in blood loss in
patients undergoing mini
extracorporeal circulation
Significantly reduced bloodloss and number of
rethoracotomies
compared to the conventional technique
Transfusion medicine 2006
Gerritsen WB van Boven WJ Wesselink RM Smelt M Morshuis WJ van Dongen HP Haas FJ
St Antonius Hospital Nieuwegein the Netherlands
van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

van Boven WJ Gerritsen WB Zanen P Grutters JC van Dongen HP Bernard A Aarts LP
Chest 2005 Apr127(4)1190-5
Pneumoproteins (CC16) as a Lung-Specific
Biomarker of Alveolar Permeability in
Conventional On-Pump CABG Surgery
vs
Mini-Extracorporeal Circuit
a Pilot Study
Significantly reduced alveolar permeability
compared to the conventional technique
Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Malondialdehyde in plasma a biomarker
of global oxidative stress during mini-
CABG compared to on- and off-pump
CABG surgery a pilot study
Wim B Gerritsena Wim-Jan P van Bovenb David S Bossa Fred J Haasa Eric P
van Dongenc and Leon P Aartsd
Interactive Cardio Vascular and Thoracic Surgery 2006527-31
doi101510icvts2005116061
Significantly reduced malondialdehyde in plasma
compared to the conventional technique
Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Myocardial oxidative stress and cell injury
comparing three different techniques for coronary
artery bypass grafting
Boven WJ Gerritsen WB Driessen AH Morshuis WJ Waanders FG
Haas FJ van Dongen EP Aarts LP
Eur J Cardiothorac Surg 2008 Sep 26
Significantly reduced myorcardial cell injury
compared to the conventional technique
Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Summary CABG surgery with MECC (2002-2015)
0
5
10
15
20
25
30
35
40
45
2002
2003
2004
2005
2006
nm
on
th
bull Aproxx 7500 MECC procedurersquos since 2002
bull 550 MECC CABG per year
bull 80 of the CABG cases
bull Mortality rate mECC10-15 vs cECC 14-18
bull Convert to cECC lt01
2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

2005 Valve with mECC
Connection MECC
Pulmonary arterial venting
Reservoir (collabsible)
Suction possibility
Mild hypothermia 34 degC
Bloodcardioplegia
ACT gt 400
Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Pulmonary Artery Venting
Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Interact Cardiovasc Thorac Surg 2010 Dec11(6)754-7 Epub 2010 Sep
16
Combined coronary artery bypass grafting and aortic valve
replacement with minimal extracorporeal closed circuit circulation
versus standard cardiopulmonary bypass
Yilmaz A Sjatskig J van Boven WJ Waanders FG Kelder JC Sonker U
Kloppenburg GT
Retrospectieve study
bull patients MECC 65 CECC 135
bull Demographics data comparablebull Reduced Red Cell units use in MECC groupbull No difference in postoperative complications and mortality
bull Conclusion AVR with CABG using MECC is feasible and provides better clinical results compared to standard CPB with regard to blood productsrequirements without compromising operative morbidity or mortality
Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Minimal access AVR using MECC is feasible and provides excellent
clinical results decreasing pain and improving postoperative
recovery compared to standard median sternotomy
Ann Thorac Surg 2009 Mar87(3)720-5
Minimal access aortic valve replacement using a minimal
extracorporeal circulatory systemYilmaz A Rehman A Sonker U Kloppenburg GT
Source
Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein the Netherlands ayilmazantoniusnetnl
Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Valve surgery with MECC (2006-2016)
700 isolated AVR (350 mini AVR)
20 isolated MVPR
200 combined valve ndash CABG
59 Double valves
4 Bentall
1 VSD VSR Free wall rupture Morrow MAZE
25 re-operations
AVR standard for some surgeons
AVR + CABG standard for some surgeons
FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

FEASABILITY OF MITRAL VALVE SURGERY
USING MINIMAL EXTRACORPOREAL CIRCULATION
Alaadin Yilmaz MD1 Jelena Sjatskig MSc1 Jan Willem van Boven MD1 Uday Sonker MD1
Frans G Waanders2 Geoffrey T L Kloppenburg MD PhD11Department of Cardiothoracic Surgery St Antonius Hospital Nieuwegein The Netherlands2Department of Clinical Perfusion St Antonius Hospital Nieuwegein the Netherlands
Mitral valve surgery using MECC is feasible and leads to less blood
products requirementscompared to standard CPB without
compromising operative morbidity or mortality
Submitted 2011
Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Change from an Collabsable to Cardiotomie reservoir
Only for AVR and AVRCABG at the moment
2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

2009
Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Cardioplegia administration during surgery with MECC Roller or no-Roller
randomized controlled trial
Mizja FaberNieuwegein The Netherlands June 13 2014
Minimal Invasive Extracorporeal Circulation Technologies (MiECT)
Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Roller Non - Roller
Resistance dependend
Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Study endpoints
Pre-op
(T0)
ICU
(T1)
4 h ICU
(T2)
first day post-op
(T3)
Troponin T X X X X
hFABP X X X X
NT-pro-BNP X X X X
C-reactive protein X X X X
Administration of blood cardioplegia
roller vs non - roller pomp
No statistically significant difference
- Troponin T hFABP NT-pro-BNP en CRP
- Blood cardioplegia flow
- Blood cardioplegia line pressure
- Aortic root pressure
Conclusion
Perioperative myocardial injury reflected bypostoperative biomarker release
Blood cardioplegia delivery without the use of a roller pump is safe to use
bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

bull Suction- Development Reservoirs Vacuum separate
bull Air Handling ndash micro emboly
bull Cannulaersquos ndash Seldinger technique Endo balloon
bull Implementing MiECT Class Type IV
bull MiECC CABG is standard
bull Feasible
bull MiECC Valve needs more prove
bull Prospective study
14 years of MiECC in StAntonius
Developments
Thank you
MiECC procedure with Cardiohelp

Thank you
MiECC procedure with Cardiohelp

MiECC procedure with Cardiohelp