-
8/10/2019 The Anatomy Of Medical Research
1/16
Copyright 2014 American Medical Association. All rig hts
reserved.
The Anatomy ofMedical Research
US and International Comparisons
Hamilton Moses III, MD; DavidH. M. Matheson, JD,MBA;
SarahCairns-Smith, PhD;BenjaminP. George, MD,MPH;
ChasePalisch,MPhil; E. RayDorsey, MD, MBA
IMPORTANCE Medical research is a prerequisiteof clinical
advances, while healthservice
research supports improved delivery, access, and cost. Few
previous analyses have compared
the United States with other developed countries.
OBJECTIVES To quantify total public and private investment and
personnel (economic inputs)
and to evaluate resulting patents, publications, drug and device
approvals, and value created
(economic outputs).
EVIDENCE REVIEW Publicly available data from 1994 to 2012 were
compiled showing trends
in US and international research funding, productivity, and
disease burden by source and
industry type. Patents and publications (1981-2011) were
evaluated using citationrates and
impact factors.
FINDINGS (1)Reduced science investment: Total US funding
increased6% per year
(1994-2004),but rate of growthdeclined to 0.8% per year
(2004-2012), reaching $117 billion
(4.5%) of totalhealth care expenditures. Private sources
increasedfrom 46% (1994)to 58%
(2012). Industry reduced early-stage research, favoring medical
devices, bioengineered
drugs, and late-stage clinical trials, particularly for cancer
and rare diseases. National Insitutes
of Health allocations correlate imperfectly with disease burden,
with cancer and HIV/AIDS
receiving disproportionate support. (2) Underfunding of service
innovation: Health services
research receives $5.0 billion (0.3%of total healthcare
expenditures) or only 1/20thof
science funding. Private insurers ranked last(0.04% of revenue)
and health systems 19th
(0.1% of revenue) among 22 industries in their investment in
innovation. An incrementof
$8 billion to $15billion yearly would occur if service firms
were to reach medianresearch
and development funding. (3) Globalization: US government
research funding declined from57%(2004) to 50%(2012) of theglobal
total,as did that of US companies (50% to 41%),
with thetotal US (public plus private)share of
globalresearchfunding decliningfrom 57%to
44%. Asia, particularly China, tripled investment from $2.6
billion (2004) to $9.7 billion
(2012)preferentiallyfor educationand personnel. The US share of
life science patents
declined from 57%(1981) to 51%(2011),as didthoseconsidered most
valuable, from 73%
(1981)to 59%(2011).
CONCLUSIONS AND RELEVANCE New investment is required if the
clinical valueof past
scientific discoveriesand opportunities to improve care are to
be fully realized. Sources could
include repatriation of foreign capital, new innovation bonds,
administrative savings, patent
pools, and public-private risk sharing collaborations. Given
internationaltrends, the United
Stateswill relinquish itshistoricalinternational lead in thenext
decade unlesssuch measures
are undertaken.
JAMA. 2015;313(2):174-189. doi:10.1001/jama.2014.15939
Editorials pages 143and 145
Supplementalcontent at
jama.com
Author Affiliations: TheAlerion
Instituteand Alerion Advisors LLC,
North Garden, Virginia (Moses);
Johns Hopkins School of Medicine,
Baltimore,Maryland(Moses);BostonConsultingGroup, Boston,
Massachusetts (Matheson, Cairns-
Smith, Palisch); Universityof
Rochester School of Medicine,
Rochester,New York (George,
Dorsey); StanfordUniversity School
of Medicine,Stanford, California
(Palisch).
Corresponding Author: Hamilton
Moses III, MD, Alerion,PO Box 150,
North Garden, VA22959
([email protected]).
Clinical Review& Education
Special Communication | SCIENTIFIC DISCOVERY AND THE FUTURE OF
MEDICINE
174 (Reprinted) jama.com
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
2/16
Copyright 2014 American Medical Association. All rig hts
reserved.
Thepromiseofnewdrugs,vaccines,medicalprocedures,and
devices captures the imaginations of the public, scien-
tists, and physicians alike. Forthe lastcentury, medical re-
search,includingpublichealthadvances,hasbeentheprimarysource
ofandanessentialcontributortoimprovementinthehealthandlon-
gevity of individuals and populations in developed countries.
The
United States has historically been where research has found
the
greatest supportand hasgenerated more than half
theworldsfund-ing for many decades. Although US-based companies,
founda-
tions, and public agencies have sponsored most research, that
re-
search is conducted by an array of autonomous university
laboratories,studygroups,and coalitionsof researchers.
Thisorga-
nization contrasts with that found in most other countries,
where
government laboratories are predominant and where health
sys-
tems and insurers conduct and finance service innovations
di-
rectly.
Expectations for medical research vary sharply, depending on
theobserversperspective.For a patient affected by disease, it is
a
source of hope. For a parent of a child with a serious
condition, it
evokes bothexpectationand frustration overthe paceof
progress.
Wherea physicianmayseeka routeto bettercare, aneconomistsees
an engine of growth and a politician sees high-skill jobs and
im-
proved national competitiveness. Hospital executives expect
re-
search tospawn new services, whereas pharmaceutical CEOsmust
havenewproducts.Aninsuranceexecutivedoubtsinstinctivelythat
the value of research will outweigh its incremental cost. A
regula-
toraims for the appropriate amountof risk while still getting
inno-
vations that matter to the market. For philanthropists and
public
health campaigners,researchrepresents thebest hopefor
alleviat-
ing the worlds most immediate health-related problems. To a
sci-
entist, research deepens critical knowledge and the way
intelli-
gence and organized effort can improve health. All of these
constituentsplay a rolein howresearchis funded
andbroughtfrom
bench to bedside. Meeting their collective needs produces a
com-
plex setof hurdles.ThisSpecialCommunication
examinesdevelopmentsover the
past 2 decades in the pattern of who conducts and who
supports
medicalresearch,as wellas resulting patents, publications,
andnew
drug and device approvals. We place the United States in an
inter-
national context to understand the key forces of change and
sug-
gest remedies for the various stakeholders to explore as they
seek
greater benefit for their investment.
Key Questions
We address 3 major trends:
1. Diminishedfunding inthe UnitedStates from both publicand
pri-vate sponsors at a time when scientific opportunity has
never
been greater but whensupport for sustained, long-terminvest-
ments is limited and short-term performance is rewarded dis-
proportionately
2. Establishingstrongincentivesfor investment inhealthservice
and
delivery innovations andbetter ways to deliver care
3. The implications of globalization
Betterunderstandingofthesefactorsisrequiredifthefullprom-
iseof the cumulative investment in biomedical science
andoppor-
tunityfor improvedservices are to be realized.
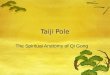
Information in 8 areas has been assembled to inform the dis-
cussion(Figure 1). Twoareas involve thecurrentand
historicalland-
scapein the United States of investment andemployment in
medi-
cal research, placing the United States in an international
context.
Two areas examine funding on biomedical and health services
re-
search separately. Four areasquantify the value of
thatinvestment
as judged by resulting patents, publications, drug and device
ap-
provals, and public market performance of life science and
health
service companies.
Methods
To describeand document thecurrent anatomyand
historicaltrends
ofmedical research, weassembledan arrayof
informationfromvari-
ous datasources.We relied on publicly available data,
recalculated
those data for display when necessary, reconciled
inconsistentsources, and included years for which data are complete
(in gen-
eral,from1994to2012).TheBox containsa list ofthe includedand
supplementary figures and tables.
Methods were similar to those we have used previously.1-3Ad-
ditionally, in this study, the 40 largest developed nations were
ex-
Figure 1. TheAnatomyof Medical Research:US and International
Comparisons
Medical Research ActivitiesMedical Research Funding
Sources of funding
Government, industry,
foundations, charities,
and universities Historical trends
International comparisons
Biomedical research
Historical funding trends
Funding by phase of
research
Funding by therapeutic area
Workforce size
Historical trends
International comparisons
Science and TechnologyWorkforce
Health services research
Historical funding trends
Industrial sector comparisons Market performance
Health care sector
performance compared
with market average
New drugs and devices
New drug and device
approvals by FDA and EMA
Patents
International comparison
of patenting activity
Publications
International comparison
of publication activity
Medical Research Output
EMA indicates European Medicines
Agency; FDA, USFoodand Drug
Administration.
TheAnatomy of Medical Research Special Communication
ClinicalReview & Education
jama.com (Reprinted) JAMA January 13,2015 Volume 313, Number2
175
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
3/16
Copyright 2014 American Medical Association. All rig hts
reserved.
amined using comparable, standard measures of investment,
em-
ployment, economic value, patents, and publications.
Althoughreliable internationalcomparisons of biomedicalsci-
ence funding are possible, comparable data for healthservices
re-
search are notavailable because other countries do
notdistinguish
themfromcostsof insurance andexpenditures onprovisionof
care.
A complete description of methods is included in the foot-
notes accompanying each table and figure.
Information, Trends, and Analysis
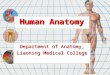
Medical Research FundingIn 2012, total US funding of biomedical
and health services
research was $116.5 billion (Figure 2and eTable 1 in the
Supple-
ment), or 0.7% of gross domestic product (GDP). The largest
increase in funding occurred between 1994 and 2004, when
funding grew at 6% per year. However, from 2004 to 2012, the
rate of investment growth declined to 0.8% annually and (in
real
terms) decreased in 3 of the last 5 years (eFigure 1 in the
Supple-
ment). The exceptions were 2009 and 2010, accountable to
stimulus from the American Recovery and Reinvestment Act
(ARRA). As a percentage of national health expenditures,
medical
research investment remained stable, ranging between 4.2%
and
4.7% from 2004 to 2012 (eFigure 1).
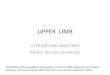
In 1994, the National Institutes of Health (NIH) budget
totaled $17.6 billion and in 2004 reached a peak of $35.6
billion
(Figure 3). Following a decade of remarkable public
sponsorship
of medical research with growth exceeding 7% per year in
the1990s, funding from the NIH declined nearly 2% per year
in
real terms (Figure 3) after the mid-2000s. This decrease
repre-
sents a 13% decrease in NIH purchasing power (after
inflation
adjustment) since 2004 (eFigure 2 in the Supplement), which
may be more severe when considering NIH appropriations
through 2013.5 Other sources of US investment were not
immune
to slowed growth. Funding from major sources of investmenteither
slowed or declined over the past 10 years, with the excep-
tion of other federal support, which includes organizations
such
as the Agency for Healthcare Research and Quality (AHRQ).
From 1994 to 2004, the medical device, biotechnology, and
pharmaceutical industries had annual growth rates greater
than
6% per year (Figure 3), with biotechnology demonstrating the
largest increases. The share of US medical research funding
from
industry accounted for 46% in 1994 and grew to 58% in 2012.
Although much of the growth in medical research funding over
the past 20 years can be attributed to industry, investment
still
Box. Listof Included and SupplementaryFiguresand Tables
Included figures
Figure 1.The Anatomy of Medical Research: US and
International
Comparisons
Figure 2.US Funding for Medical Research by Source, 1994-
2012
Figure 3.Growth in US Funding for Medical Research by
Source,1994-2012
Figure 4.Pharmaceutical Industry Medical Research Funding by
Phase of Research, 2004-2011
Figure 5. Medicines in Development for Top 10 Therapeutic
Areas,
2013
Figure6. USFunding forHealth ServicesResearchby Source,2004-
2011
Figure 7.Researchand Development Investment Ranking of
Indus-
trialSectorsAmong US-BasedCompanies, 2011
Figure 8.Global Medical Research Funding in Select
Countries/
Regions, 2011
Figure9. Top 10 Countriesby Sizeof Scienceand
TechnologyWork-
force, 1996-2011
Figure 10.Global Life Science Patent Applications by Country
of
Origin, 1981-2011
Figure 11. US LifeSciencePatent Applications by Country of
Origin,
1981-2011
Figure 12.Highly Valuable US Life Science Patents by Country
of
Origin, 1981-2011
Figure 13.Medical Research Articles and Citations by
Selected
Countries/Regions, 2000-2010
Figure 14.Market Performance of Publicly Traded Life
Sciences
and Health CareCompanies, 2003-2013
Supplementary figures and tables
eFigure1. Historical GrowthTrajectory ofUS
MedicalResearchFund-
ing, 1994-2012
eFigure 2.Historical Trajectory of NIH Medical Research
Funding,
1994-2012
eFigure 3.Venture Capital Investment in Biotechnology
Compa-nies, 1995-2013
eFigure 4.Relationship Between NIH Disease-Specific Research
Funding and Burden of Disease forSelectedConditions
eFigure 5.GrowthinGlobalMedicalResearchFundinginSelectCoun-
tries/Regions, 2004-2011
eFigure 6.Medical Research and Development Funding and Sci-
enceand TechnologyWorkforces in Select
Countries/Regions,2011
eFigure 7.EuropeanLife SciencePatent Applications by Country
of
Origin, 1981-2011
eFigure 8. Highly ValuableEuropean LifeSciencePatentsby
Coun-
try of Origin, 1981-2011
eFigure 9. Comparisonof NewApprovalsby USFood andDrugAd-
ministration and EuropeanMedicinesAgency, 2003-2013
eTable1. US Fundingfor Medical Researchby Source, 1994-2012
eTable2. NIHMedical Research Funding by Type ofResearch,
2004-
2012
eTable3. NIH Disease ResearchFunding and Burden of Disease
for
Selected Conditions
eTable 4.Medical Research Funding From (A) Public Charities
and
(B) Private Foundations, 2011
eTable 5. USFundingforHealthServicesResearchby Source,2004-
2012
eTable6. Methods andData Sourcesfor Medical ResearchFunding
by Select Countries/Regions
Clinical Review & Education SpecialCommunication TheAnatomy
of Medical Research
176 JAMA January 13,2015 Volume 313, Number2 (Reprinted)
jama.com
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
4/16
Copyright 2014 American Medical Association. All rig hts
reserved.
slowed (medical device, 6.6% to 6.2% in 1994-2004 vs 2004-
2012; biotechnology, 14.1% to 4.6% in 1994-2004 vs 2004-
2012), or declined (pharmaceutical firms, 6.8% to 0.6% in
1994-
2004 vs 2004-2012).
Research Funding
Biomedical Research
The distribution of investments across the types of medical
re-search changed from 2004 to 2011. Pharmaceutical companies
shifted funding to late-phase clinical trials and away from
discov-
ery activity such as target identification and validation. The
share
of pharmaceutical industry funding (including that by US
compa-
nies outside ofthe UnitedStates)spenton phase 3
trialsincreased
by 36% (5%/year growth rate) from 2004 to 2011 (Figure 4),
and
the share of investment in prehuman/preclinical activities
de-
creased by 4% (2%/yearaveragedecline). Thisshift toward
clinical
research and development reflects the increasing costs,
complex-
ity, andlength of clinical trialsbut may also reflecta
deemphasis of
earlydiscovery efforts by theUS pharmaceuticalindustry.
Whilein-
dustry hasshifted funding to clinical trials, the share of
NIHcontri-
butions dedicated to basic science and clinical research was
un-
changed (eTable 2 in the Supplement), with the majority of
funds
still focused on basic research. These data may not accurately
re-
flectthetruedivisionofNIHinvestmentforbasicsciencevsdisease-
focused research, as a growing proportion of NIH expenditures
is
forprojectshavingpotentialclinicalapplication in manydiseases
or
organ systems.7
Inreal terms,venture capitalinvestmentin biotechnology com-
panies steadilyincreased from $1.5 billion in 1995 to a peak of
$7.0
billion in 2007 (eFigure 3 in the Supplement). During that
period,
investmentin biotechnologycompanies as a shareof total
venture
capital investment increasedfrom 10%to 18%, and thenumber of
investments increased from 176to 538. Investment levelsand
the
number of transactions of biotechnology decreased following
the
financial crisis in 2008-2009, declining to a low of $4.3
billion in2009. Venture capital investment still has notrecoveredto
its pre-
2008 levels, with only $4.5 billion invested in 2013. Size of
invest-
mentper transaction(median,$11 million, inflation adjusted)
hasre-
mainedunchanged for 2 decades.
Public funding of medical research by condition was only
mar-
ginally associated withdisease burden in the United States in
2010
(eFigure 4 in the Supplement). A set of 27 diseases that
account
for 84% of US mortality, 52% of years of life lived with
disability,
84% of years of life lost, and 70% of disability-adjusted
life-years
receive 48% of NIH funding (R2 = 0.26) (eTable 3 in the
Supple-
ment). Several factors other than disease burden may
influence
funding, including the quality of research, scientific
opportunity,
portfolio diversification, or building of infrastructure, and
the com-bination of these factorscomplicatesthe relationshipof
funding to
particular conditions.8,9 Cancer and HIV/AIDS were funded
well
above the predicted levels based on US disability alone (eFigure
4
in the Supplement), with cancer accounting for 16% ($5.6
billion)
of total NIH funding and 25% of all medicines currently in
clinical
trials (Figure 5).
Rare diseases have emerged for industry as a preferential
area
of therapeutic development, with nearly as many compounds in
trials as analgesics and antidiabetic drugs (Figure 5).
Industry
favors rare diseases because they are commercially attractive
due
to provisions of the Orphan Drug Act and relative ease of
clinical
trials. Investment can be expected to increase as diseases
are
defined by biomarkers that allow the development of targeted
therapies.12
Support from private foundations, public charities, and
other
entities comes from only a feworganizations.In 2011,42% of
total
not-for-profitfundingwas by thetop 10 public
medicalcharitiesand
top10 private foundations (eTable4 in theSupplement).
TheHow-
ardHughesMedicalInstitute(which supports domestic
researchpri-
marily) and the Billand Melinda GatesFoundation(which
supports
international research primarily)accountfor 87%of biomedical
re-search funding by private foundations (eTable 4, panel B).
United
Statesbased medical charities direct most monies in the
United
States, thoughthe amountspenton research (asopposed to edu-
cation, disease screening, and other activities) cannot be
quanti-
fied using publicdata.
HealthServices Research Funding
Health services research, which examines access to care, the
qual-
ity and cost of care, and the health and well-being of
individuals,
communities, and populations, accounted for between 0.2% and
Figure 2. US Fundingfor Medical Researchby Source, 1994-2012
120
140
100
80
60
40
20
0
1994 1996 1998 2000 2002 2004 2006 2008 2010 2012
MedicalResearchFunding,$,inBillionsa
Year IncludesARRA Fundingb
Compound annual growthrate, 6.3%d
Compound annual growthrate, 0.8%d
Foundations, charities, and other private funds
State and local government
Other federalb
Medical device firms
Biotechnology firmsc
Pharmaceutical firms
National Institutes of Healthb
Funding source
Data were calculated accordingto methods outlinedin eTable 1
inthe
Supplement. ARRA indicates American Recoveryand
ReinvestmentAct.
a Data were adjusted to2012dollars usingthe Biomedical
Researchand
Development PriceIndex.4
b TheNationalInstitutes of Health and other federal sources
includestimulus
provided byARRA in 2009 and2010.
c Datafrom 1994-2002 and 2011-2012were estimatedbased on
linear
regression analysis of industry market share.
d Compoundannualgrowthrate(CAGR) supposingthatyearA isxand yearB
is
y, CAGR = (y/x){1/(BA)}1.The CAGRwas calculated separatelyfor 2
different
periods witha singleoverlapping year: 1994-2004 and 2004-2012.
Thecut
pointwas chosenat 2004 giventhe changes seen in funding from
theNational Institutesof Health in thatyear.
TheAnatomy of Medical Research Special Communication
ClinicalReview & Education
jama.com (Reprinted) JAMA January 13,2015 Volume 313, Number2
177
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
5/16
Copyright 2014 American Medical Association. All rig hts
reserved.
0.3% of national health expenditures between 2003 and 2011,
an
approximately 20-fold difference in comparison with total
medical
research funding (eFigure 1 in the Supplement). Health
services
research funding increased 4.6% per year from $3.7 billion
in
2004 to $5.0 billion in 2011 (Figure 6and eTable 5 in the
Supple-
ment). Investment fromfoundations decreased in real terms at
1%
per year over the period, following declines after the recession
of
2008. Increases in health services research funding were
largely
driven by AHRQ (15.8%/year growth) and the health care
services
industry (11.0%/year growth), which includes hospitals,
ambula-
tory health care services, and nursing care facilities.
Although
health care industry funding is likely underestimated
because
research funds may not account for hidden costs of quality
improvement, research investment was especially low when
com-
pared with other industrial sectors (Figure 7). Insurers and
health
systems rank among the lowest in research and development
(funding $1.3 billion, or 0.1% of revenue), which was well
below
the median for industrial sectors ($5.5-$7.3 billion for total
fund-
ing, or 1.7%-2.5% of revenue). Health insurers may provide
addi-
tional health services research funding that cannot be
distin-
guished from the insurance industry as a whole, although
these
funds are small and unlikely to change the results for
industry
funding (Figure 7).
International Medical Research Funding
Global medical research expendituresby publicand industry
sources
in theUnited States, Europe, Asia, Canada, andAustralia
combined
increasedfrom$208.8billionin2004to$265.0billionin2011,grow-
ingat 3.5%annually(Figure 8 and eTable 6 inthe
Supplement).Al-
thoughthere may be medical research funding from
otherareasof
theworld (eg, South America),these data represent the most
reli-
able and current sources of global medical research
investment.
Among theregionsincludedin theanalysis, theUnited States
dem-
onstrated the slowestannual growthin investment (1.5%/year),
fol-
lowed by Europe (4.1%/year)and Canada (4.5%/year).
Asiancoun-
tries increased from $28.0 billion in 2004 to $52.4 billion in
2011,
Figure 3. Growth in US Fundingfor Medical Researchby Source,
1994-2012
120
100
80
60
40
20
0
MedicalResearchFunding,
$,inBillio
nsa
Medical Research Funding,
$ (%), in Billions a
Funding Source
Foundations, charities, other private
State and local government
Other federal
National Institutes of Health
Medical device firms
Overall
Biotechnology firms
1994
2.6 (4)
3.9 (7)
8.0 (13)
17.6 (29)
3.8 (6)
59.5
3.7 (6)
20.0 (34)
2004
3.9 (4)
5.9 (5)
4.8 (4)
35.6 (33)
7.1 (6)
109.7
13.7 (12)
38.6 (35)
2012
4.2 (4)
6.3 (5)
7.1 (6)
30.9 (27)
11.5 (10)
116.5
19.6 (17)
36.8 (32)
Compound Annual
Growth Rate, %b
1994-2004
4.2
4.1
4.9
7.3
6.6
6.3
14.1
6.8
2004-2012
0.8
1.0
0.9
5.0
1.8
6.2
4.6
0.6Pharmaceutical firms
Year
1994 2004 2012
Data were calculated accordingto methods outlined ineTable 1
inthe
Supplement.
a Adjusted to 2012dollars usingthe BiomedicalResearchand
Development
PriceIndex.4
bCompoundannualgrowthrate(CAGR) supposingthatyearA isxand yearB
is
y, CAGR = (y/x){1/(BA)}1.
Figure 4. PharmaceuticalIndustryMedicalResearchFunding by Phase
of Research,2004-2011
50
40
30
20
10
0IndustryMedicalResearch
Funding,$,inBillionsa
2004 2011
Phase of Research
Uncategorizedc
Phase 4
Approval
Phase 3
Phase 2
Overall
Phase 1
Industry Medical Research
Funding,$, (%), in Billions a
2004
4.2 (9)
6.4 (13)
4.5 (9)
12.6 (26)
4.9 (10)
48.3
3.2 (7)
12.5 (26)
2011
1.7 (3)
4.8 (10)
4.1 (8)
17.6 (36)
6.2 (13)
49.3
4.3 (9)
10.6 (22)
Compound Annual
Growth Rate, %b
2004-2011
0.3
11.9
3.9
1.2
4.9
3.3
4.1
2.3Prehuman/preclinical
Pharmaceutical industry funding by phasewas obtained
fromPharmaceuticalResearchand Manufacturers of America (PhRMA)
annual reports,2004-2011.6
Data were 2 yearsold at time of publication andincludeboth
domestic and
international research funding fromPhRMA members.
a
Data were adjustedto 2012 dollars using theBiomedicalResearch
andDevelopment PriceIndex.4
bCompoundannualgrowthrate(CAGR) supposingthatyearA isxand yearB
is
y, CAGR = (y/x){1/(BA)}1.
c Uncategorized funding could notbe allotted toa singlephaseof
research.
Clinical Review & Education SpecialCommunication TheAnatomy
of Medical Research
178 JAMA January 13,2015 Volume 313, Number2 (Reprinted)
jama.com
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
6/16
Copyright 2014 American Medical Association. All rig hts
reserved.
or 9.4%per year, withespeciallylargeincreases in China, India,
South
Korea, and Singapore.
These trendsresultedin therestructuring of theshareof total
global investment (eFigure 5 in the Supplement). As a
percentage
of global funding,the United States declinedby
approximately13%
from 2004 to 2012, and Asian economies increased by approxi-
matelythe same share (13% in2004to 20%in 2011). Althoughab-
solutegrowthof Asianinvestmentfrom2004to 2011 reached
$24billion, the United States remained the leading sponsor of
global
medical research in 2011 (44% share), and Europethe next
largest
sponsor (33% share).
Overall growth was slightly greater for industry outside the
United States compared withpublicsources (4.3%vs 2.2%),and
in-
dustry accountedfor two-thirdsof fundsin 2011. However, US
con-
tributions increasedslowlyfrom bothpublic(0.1%/year)and
indus-
try sources (1.7%/year).
Public funding in the United States decreased to a 49% share
of theworldspublic research investment by 2011,downfrom57%
in 2004 (Figure 8). United States industry, which accounted
for
nearlyhalf ofglobal industry medical researchexpendituresin
2004,
declined to41% ofglobal industry funding in2011(Figure
8).Japan
demonstrated the greatest increase in the worlds share of
indus-
tryfunding(+3.9%),andEuropeancountriesgainedthemostinpub-
licinvestment(+3.5%).Despite decreasesin theUS share of
invest-
ment, the United States remained the worlds leading sponsor
for
both publicand industry medical research funding in 2011.
Science and Technology Workforce
From 1996 to 2011, the US science and technology workforce
in-
creased by 2.7% annually to reach 1.25 million workers (Figure
9).
Over the sameperiod, Chinas workforce increased6% annually
to
reach1.31millionworkers,makingit thelargestnationalscience
and
technology workforce in the world. Reliable information about
the
proportion of medical researchers could not, however, be ob-
tained.
AlthoughChina ledthe world inthe overall size oftheirscience
and technology workforce, it had only 1.9 science and
technology
workers per 100 000 full-time equivalents, the lowest among
the
countriesincludedin theanalysis(Figure9). TheUnited States
em-
ployed 8.1 science and technology workers per 100 000
full-time
equivalents in its total workforce, or the median for the 10
largest
workforcesin theworld.
Theinvestmentin capital terms andin labor terms differ
widelyacross countriesand regions.The United States contributes
44.2%
of global medical research funding butcomprisesonly 21.2% of
the
Figure5. Compoundsin Developmentfor Top 10Therapeutic
Areas,2013
200 400 600 800 1200 1400 1600 18001000
Rare diseasec
Anti-inflammatory
Recombinant vaccine
Cognition enhancer
Anticancer,immunological
Anticancer, otherb
Therapeutic areaa
Prophylactic vaccine,anti-infective
Antidiabetic
Analgesic
0
No. of Compounds in Clinical Trialsa
Data forthenumber of compoundsin developmentwerefromthe
Citeline
PharmaR&D AnnualReview 2014.10 Data forrarediseases were
from the
Pharmaceutical Researchand Manufacturers of America.11
a Numberof compoundsin clinicaltrials orunderreviewby theUS
Foodand
DrugAdministration. Thisincludes a totalof 10 479compoundsin
2013.
b Includes all nonimmunologicalanticancer compounds.
c Rare diseases were defined as those affecting200 000or
fewerpeople in the
United States.
Figure 6. US Fundingfor Health ServicesResearch by Source,
2004-2011
6
4
2
0HealthServicesResearch
Funding,$,inBillionsa
2004 2011
Funding source
Health services industryc
AHRQ
NIH
Other federald
Foundationse
Overall
Health Services Research
Funding,$, in Millions (%)a
2004
653 (18)
365 (10)
1158 (32)
442 (12)
1034 (28)
3652
2011
1352 (27)
1018 (20)
1189 (24)
494 (10)
967 (19)
5019
Compound Annual
Growth Rate, %b
2004-2011
4.6
11.0
15.8
0.4
1.6
1.0
AHRQindicatesAgency for HealthcareResearch and Quality;
NIH,National
Institutesof Health. Datawere calculated accordingto methods
outlined in
eTable 5 in theSupplement.
a Adjusted to 2012dollars usingthe Biomedical Researchand
Development
PriceIndex.4
b Compound annualgrowth rate (CAGR)supposing that year A isxand
yearB is
y, CAGR = (y/x){1/(BA)}1.
c Health services industry includes funding
fromhospitals,ambulatory health
careservices,nursing and residentialfacilities.Health
insurancecompanies
were not included.Datamay notfullycapturethe entiretyof funding
for
health services researchand quality improvement initiativesfor
theUS health
careservices industry.
d Other federal funding includes theCenters forDisease Control
and Prevention,
Centers for Medicare & Medicaid Services, Veterans
HealthAdministration,
Health Resourcesand Services Administration,and Patient
Centered
OutcomesResearchInstitute(in 2011only).
e Foundationfundingincludes totalgiving fromthe Robert Wood
Johnson
Foundation, CaliforniaEndowment, PewCharitableTrusts, W.K.
Kellogg
Foundation, and CommonwealthFund.
TheAnatomy of Medical Research Special Communication
ClinicalReview & Education
jama.com (Reprinted) JAMA January 13,2015 Volume 313, Number2
179
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
7/16
Copyright 2014 American Medical Association. All rig hts
reserved.
globalscience andtechnology workforce (eFigure 6 in
theSupple-
ment).Conversely, Chinacontributesonly 1.8%of globalfunding
for
medicalresearchbutcomprises22.3%oftheglobalscienceandtech-
nology workforce.This differencein investment representsa
natu-
ralexperiment in productivity management and hasbroad
implica-
tions for patents and intellectual property ownership, which
will
evolveover the next fewyears.
Outputs of Medical ResearchLife Science Patent Filings
China filed30% of global lifesciencepatentapplications in 2011,
in-
creasing from 1% of globalapplications in 1991 (Figure 10). This
in-
cludesapplications froma number of
patentingofficesthroughout
the world, including offices in China, the United States, and
the
EuropeanUnion.The United States followedwith24% of
patentfil-
ings globally, increasing from an 11%sharein 1991.
United States inventors led in the number of life science
pat-
ent filings in both the United States and EU, where China
ac-
counted for less than 2% of filings in both regions ( Figure
11and
eFigure 7 in the Supplement). The proportionof US inventors
filing
patents inthe UnitedStates decreasedfrom57% to51% from 1981
to 2011. During the same period, the share of highly valuable
pat-
ents filed by US inventors decreased between from 73% to 59%
(Figure 12), while allothercountries in theanalysisincreased
their
share of highly valuable patents. Similar trends were observed
for
highly valuable patents filed through the European Patent
Office
(eFigure 8 in the Supplement). Highly valuablepatentsare
defined
by the frequency they are cited by other inventors in
subsequentpatent applications (Figure 12, footnote b)
Publications
The UnitedStates ledthe world with 33% of
publishedbiomedical
researcharticlesin2009(Figure13A).IntheUnitedStates,thenum-
ber of biomedicalresearcharticles increasedat 0.6%per
yearfrom
2000to 2009.Duringthesame period, thenumberof articlespub-
lished in China increased by 18.7% annually.
The United States also leads the world inits share of the
most
highly citedbiomedical research articles, with63% of thetop
cited
Figure 7. Researchand DevelopmentInvestment Ranking of
IndustrialSectorsAmong US-BasedCompanies, 2011
20 40 60 800
Research and DevelopmentSpending, $, in Billionsb
Domestic
Foreign
Transportation services
Insurance carriers
Utilities
Health care servicesc
Architectual engineering
Physical, engineering, and life sciences
Telecommunications
Banking, credit, and securities
Data processing and hosting
Mining, extraction, and support activities
Food and beverage
Internet service provider and web search
Plastics, minerals, and metal products
Aerospace and defense
Chemicals
Computer software and systems design
Machinery
Medical devicesAutomobiles and parts
Software and paper publishing
Computer and electronics manufacturing
Pharmaceuticals and biotechnology
Median
Total research and development fundinga
5 10 150
Research and DevelopmentSpending as % of Revenue
Pharmaceuticals and biotechnology
Median
Share of revenue spent on research and developmenta
Internet service provider and web search
Software and paper publishing
Physical, engineering, and life sciences
Computer and electronics manufacturing
Medical devices
Aerospace and defense
Computer software and systems design
Data processing and hosting
Machinery
Automobiles and parts
Chemicals
Plastics, minerals, and metal products
Mining, extraction, and support activities
Architectual engineering
Food and beverageTelecommunications
Utilities
Banking, credit, and securities
Health care servicesc
Transportation services
Insurance carriers 0.040.2
0.04
Researchand development expenditures forUS-based
companiesperforming
research by theindustrialsector wereobtainedfrom the National
Science
Foundation.13 Datainclude researchfunds spentboth
domesticallyand abroad.
Industry revenues wereobtainedfrom the National Science
Foundation13
orUSCensusBureau14 based onthe availabilityof data. Revenuesand
researchand
development expenditures werematchedby industry usingNorth
American
Industry ClassificationSystemcodes.
a Thepharmaceuticals and biotechnology, medical devices, and
health care
services industriesare highlightedin red.
bAdjusted to 2012dollars usingthe BiomedicalResearchand
Development
PriceIndex.4
c Healthcare services industry includes US-based
hospitals,ambulatoryhealth
careservices, and nursing and residentialfacilities.
Clinical Review & Education SpecialCommunication TheAnatomy
of Medical Research
180 JAMA January 13,2015 Volume 313, Number2 (Reprinted)
jama.com
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
8/16
Copyright 2014 American Medical Association. All rig hts
reserved.
articles in 2000 and 56% in 2010; however, the growth of
highly
citedliteraturepublishedbytheUnitedStatestrailsothermajorcoun-
tries, regions, and economies(Figure13B). Aftercontrollingfor
theshareof theworldsbiomedical research articles usinga
citationin-
dex, the United States declined from 2000 to 2010 at 0.2%
per
yearastherestoftheworldincreasedbyapproximately1%peryear.
NewDrugs andDevices
Since 2003, drug approvals by the US Food and Drug
Administra-
tion(FDA) have remainedunchanged withan averageof 26approv-
als per year. Althoughdrug approvals increasedslightlyin
2011and
2012,theyreturnedclosertoaveragein2013with27approvals(eFig-
ure 9 in the Supplement). United States device approvalshave
also
remained relatively constantover thelast decade. While
thenum-
ber of approvalssteadily increasedfrom 15 approvals in 2009to
39
approvals in 2012,only 22 newdevices were approved in
2013.Duringthe sameperiod, theEuropean Medicines Agency(EMA)
averaged a higher number of both applications (55/year) and
ap-
provals (42/year) than the FDA (eFigure 9). In 2013, the EMA
re-
ceived22 more applications andapproved16 more drugs than the
FDA.
Life Sciences Market Performance
Equity (stock) markets reflect broad public perception of one
in-
dustrys value in comparison with others. Since 2003, market
re-
turn for the entire health care industry (including medical
device,
pharmaceutical, and biotechnology companies as well as
hospi-
tals, nursing homes, and other health service suppliers) as
mea-
sured by the Dow Jones US Health Care Index increased 8.2%
an-nually, closelytrailingthe Standard & Poors500
(8.3%)(Figure14).
Market returns for biotechnology and health insurance
companies
outperformedthe market, growingat 18.5% and13.8%per year,
re-
spectively. Medical device companies, pharmaceutical
companies,
and hospital chains underperformed compared with the
Standard
& Poors500, increasing annuallyat 7.3%,6.8%,
and5.8%,respec-
tively. The financial crisis of 2008 led to a decrease in market
per-
formancefor alllife sciencesindustries. Generally,
allsectorsrecov-
eredin theyears following, andbiotechnology
companies,hospital
chains,and
healthinsurancecompaniesperformedexceptionallywell
since their decline in 2008-2009.
Discussion and Implications
Medical research in the United States remains the primary
source
of new discoveries, drugs, devices, and clinical procedures for
the
world,although theUS lead in these categories is declining. For
ex-
ample, whereas the United States funded 57% of medical
research
in2004,in2011thathaddeclinedto44%.Basicresearchandprod-
uct development are central to the health of countries
economies.
However, changes in the pattern of investment, particularly
level
funding by US government and foundation sponsors, with a de-
Figure 8. Global Medical ResearchFunding in Select
Countries/Regions, 2011
100
20
40
80
60
0
200
120140
180
160
220
240
280
260
MedicalResearchFu
nding,inBillionsa
Medical research funding,
$, in billions (%)a
Overall
Publicb
Industryc
Compound annual growth
rate, % (2004-2011)d
Globale
265.0 (100)
102.8 (100)
162.2 (100)
3.5
UnitedStates
117.2 (44)
50.5 (49)
66.6 (41)
1.0
Europe
88.6 (33)
26.9 (26)
61.6 (38)
4.1
Japan
37.8 (14)
17.0 (17)
20.8 (13)
6.8
China
4.9 (1.2)
1.3 (2)
3.6 (0.8)
16.9
OtherAsiaf
9.7 (4)
2.4 (2)
7.3 (4)
20.8
Canada
3.1 (1.2)
1.8 (2)
1.3 (0.8)
4.5
Australia
3.8 (1.4)
2.8 (3)
1.0 (0.6)
9.3
Publicb
Industryc
Theregions/countries/economies in the analysis include the
majorcountries of
NorthAmerica(United States, Canada), Europe (including the10
largest
European countriesin the Organisation for
EconomicCo-operationand
Development),and Asia-Oceania (Australia,China, India,Japan,
Singapore,and
SouthKorea). Datafor African and SouthAmericancountries and
Russiawere
notavailable.Data were calculatedaccordingto methods outlined
ineTable 6 in
the Supplement.
a Datawere convertedto US currency usingan average annual
exchangerate
forthe respectiveyear15 andadjustedto 2012 dollars using
theBiomedical
Researchand Development PriceIndex.4
b Publicresearchand development funding included thatfrom
government
agencies,higher educationalinstitutes, and not-for-profit
organizations.
c Industry researchand development funding included
pharmaceutical,
biotechnology, and medical devicefirms.
d Compoundannualgrowthrate(CAGR) supposingthatyearA isxand yearB
is
y, CAGR = (y/x){1/(BA)}1.
e Global totalfor medical research funding includes researchand
development
expenditures from36 majorworld countriesacross 4 continents.
f Other Asia includes India,Singapore, and SouthKorea.
TheAnatomy of Medical Research Special Communication
ClinicalReview & Education
jama.com (Reprinted) JAMA January 13,2015 Volume 313, Number2
181
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
9/16
Copyright 2014 American Medical Association. All rig hts
reserved.
cline in real terms, combined with companies focus on
late-stage
products(with diminished discovery-level investment)indicate
that
difficulties may soon appear in the ability of clinicians to
fully real-
izethe value of past investments in basic biology.
In addition, the limited support of ambitious but
scientifically
rigorous methods to improve delivery of health services
repre-sentsamajormissedopportunitytoimprovemanyaspectsofhealth,
especially as the burden of chronic illness, aging populations,
and
theneed formore effectiveways to deliver care
areappreciated.1
Overthe past 2 decades,the periodof thisanalysis,medicalre-
searchhasbecomeglobal.Ithasbeentransformedbymultiple,com-
plex and subtle transitions, from small laboratories to large,
in-
dustrial-scale institutes, from hypothesis-driven inquiries to
data-
drivencompilations, fromexperimentsby singleindividualsto
those
requiringlargeteams, and from finding causesof specific
diseases
to learning how entire systems become disordered.21
The information assembled demonstrates that 3 factors, wa-
vering financialsupport for science, underinvestment in service
in-
novation, and globalization, pose the chief challenges of the
cur-
rent era.
Biomedical ResearchNew knowledge about disease has a 15- to
25-year gestation from
basic discovery to clinical application, an interval that may
be
lengthening.22,23 Hence, the cumulative investment in
biomedical
research of the past 3 decades will soon mature. Therefore,
ensur-
ingsufficientsupportforitsclinicaldevelopmentisapressingneed.
Equally important are stable academic institutions and
companies
along with skilled researchers that have the capability to
organize
theresearchprocessand to sustainthe innovation
cycle,24particu-
larly since the size of research teams and scale of activities
have
grown.Year toyear variabilityin funding is a threatto that
stability.
Figure 9.Top 10 Countriesby Sizeof Science and Technology
Workforce, 1996-2011
1400
1200
1000
800
600
400
200
0
Full-timeEquivalents,in
Thousands
Chinac
6.0
UnitedStates
2.7
Japan
0.4
RussianFederation
1.5
Germany
2.6
UnitedKingdom
3.7
Korea
7.4
France
3.2
Canada
3.8
Spain
6.4
Work force sizeaA
1996
2011
Compound annual growthrate, % (1996-2011)b
12
10
8
6
4
2
0
No.per1000TotalEmployment
Korea
6.2
Japan
0.5
France
2.5
Canada
2.2
UnitedStates
1.8
Germany
2.2
UnitedKingdom
2.9
RussianFederation
2.1
Spain
4.1
Chinac
5.2
Work force size per 1000 total employmentB
1996
2011
Compound annual growth
rate, % (1996-2011)b
Thesizes of national science and technology workforces
wereobtainedfrom
the Organisation for EconomicCo-operationand Development.16
a Workforce sizewas measured in number of full-time
equivalentsand includes
all science and technologysectors(eg, engineering, physical
sciences) in
addition to themedical and health sciences.
bCompoundannualgrowthrate(CAGR) supposingthatyearA isxand yearB
is
y, CAGR = (y/x){1/(BA)}1.
c Annualgrowth in Chinas science and technology workforce may
be
underestimatedbecause of a change in reportingmethodsfor Chinain
2009.
Clinical Review & Education SpecialCommunication TheAnatomy
of Medical Research
182 JAMA January 13,2015 Volume 313, Number2 (Reprinted)
jama.com
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
10/16
Copyright 2014 American Medical Association. All rig hts
reserved.
Althoughthe biomedicalresearch enterpriseis
basicallyhealthy,
to fully capture theclinicalvalue of past investment in science
and
itspromisefor thefuture,2 areas require particularattention:
(1)in-
creased financial support for critical early studies that
validate ba-
sic biological discoveries and demonstrate their relevance to
dis-
ease (establishing proof of concept) and (2) greater
productivity,
especially acceleration of the application of new findings to
dis-
ease.
Financing ThatCan Sustain Long-termInvestmentIn the United
States and Europe, private companies will not likely
havethe latitude fromtheir investors, or governments the
political
will,to continueto make long-terminvestments at historical
levels.
Todays politicaland commercial environment leadsto
thisconclu-
sion. Many new basic discoveries that have probable clinical
value
are stymied by financialconstraintsat the critical
proof-of-concept
stage, where utility in humans is demonstrated. That number
can
be expected to increase onceplatformtechnologies(such as
high-
resolutionmapping of thecentralnervoussystem,analysis of
com-
plex biological systems and networks, or insights into
develop-
mentof cell maturation and differentiation) showpotential
clinical
value. This is an unfortunate paradox because many of the
dis-
easesassociated withsubstantial morbidity andmortalitymay
ben-
efit themost from these newdiscoveries.
Variousnew sourcesfor long-terminvestmentshave beenpro-
posed. Most often, public fundshavebeen sought,by expansion
of
the NIH budget, appropriationsby state legislatures, or
earmarked
federal appropriations for threatened epidemics or defense-
relatedbiologicalrisks.Mostadvocateslookto governmentfor
sup-
portof high-risk, early-stage research,given privatecompanies
fo-cuson developmentof newtechnologies attheirlater
stage.Private
foundations andpubliccharities, thoughsmall,playan
essentialrole
in filling thatgap, especially for the mostspeculative
undertakings
or where commercial incentives areinsufficient. However, it is
un-
likely that these conventional sources of research investment
will
be sufficient tomeet thechallengesof anaging population,
theag-
gregate burdenof disease, or thepromise of emerging science.
The reduced funding of large pharmaceutical and biotechnol-
ogy companieson early, basic, discovery-stage research (with
con-
comitant growth of late-stage clinical trials) is apparent from
our
Figure 11.US LifeSciencePatentApplicationsby Country of Origin,
1981-2011
100
80
60
40
20
0
Percentage
80000
60000
40000
20000
0
No.
Year
1981 1991 2001 2011
Other
Netherlands
China
Taiwan
Switzerland
Korea
Great Britain
Germany
Japan
United States
France
No. of patent application familiesin life science by country of
inventor a
Year
1981 1991 2001 2011
Other
Netherlands
China
Taiwan
Switzerland
Korea
Great Britain
Germany
Japan
United States
France
Percentage distributionby country of inventor
Thenumber of patent application
families by country was calculated
counting the mostrecentapplication
in familyof patents based ondata
obtained fromThomsonInnovation.17
Data areincludedfor allcountries
available inthe Thomsondata set.
a Life science wasdefinedto include
thefollowingcategories: analysis of
biological materials, medical
technology, organic fine chemistry,
biotechnology, pharmaceuticals,macromolecular chemistryand
polymers,and microstructural and
nanotechnology.
Figure 10.Global LifeSciencePatentApplicationsby Country of
Origin, 1981-2011
400000
300000
200000
100000
0
No.
Year
1981 1991 2001 2011
Other
Germany
Japanb
Russia
TaiwanIndia
Australia
Korea
United States
China
Canada
No. of patent family applicationsin life sciencea
100
80
60
40
20
0
Percenta
ge
Year
1981 1991 2001 2011
Other
Germany
Japanb
Russia
TaiwanIndia
Australia
Korea
United States
China
Canada
Percentage distribution by country
Thenumberof patentfamilyapplicationsby country filed
wascalculatedbased
on data obtained fromThomsonInnovation.17 Onlythe
mostrecentpatent
application ina patentfamily wascountedforthis analysis.Dataare
included for
allcountries available in theThomson data set.
a Lifescience was defined to include thefollowingcategories:
analysis of
biologicalmaterials,medical technology, organic fine
chemistry,
biotechnology, pharmaceuticals,macromolecularchemistry and
polymers,
and microstructural and nanotechnology.
b Onlypatent grants, not all patent applications, are counted
forJapan, which
tends toward patent applicationswith narrowerdefinitions and
therefore
muchgreaternumbers relative to the number of patents ultimately
granted.
TheAnatomy of Medical Research Special Communication
ClinicalReview & Education
jama.com (Reprinted) JAMA January 13,2015 Volume 313, Number2
183
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
11/16
Copyright 2014 American Medical Association. All rig hts
reserved.
Figure 12. Highly ValuableUS LifeSciencePatentsby Country of
Origin, 1981-2011
8000
6000
4000
2000
0
No.
Year
1981 1991 2001 2011
Other
China
Netherlands
Korea
CanadaSwitzerland
France
Germany
Japan
United States
Great Britain
No. of life science patent applicationsin top 10% of patents by
inventor countrya,b
100
80
60
40
20
0
Percenta
ge
Year
1981 1991 2001 2011
Other
China
Netherlands
Korea
CanadaSwitzerland
France
Germany
Japan
United States
Great Britain
Percentage distribution of top 10%of patents by country of
inventor b
Thenumber of patent applicationfamilies by country was
calculated counting
themostrecentapplicationin familyof patents based ondata
obtainedfrom
Thomson Innovation.17 Data areincluded forall
countriesavailablein the
Thomson dataset.
a Lifescience was defined to include the followingcategories:
analysis of
biologicalmaterials,medical technology,organicfine
chemistry,
biotechnology, pharmaceuticals,macromolecularchemistry and
polymers,
and microstructural and nanotechnology.
bTop10% ofpatents rankedby year usingBCG Quality Index.TheBCG
Quality
Indexis made up of3 components; specifically, forward
citationsof a patentin
newerpatents adjustedfor thepatents age, thenumberof
patentclaims, and
the strengthof a patentsbackwardcitations. Thecomponents and
correspondingweights usedby the quality indexare a product of
proprietary
Boston ConsultngGroup research.
Figure 13.Medical ResearchArticlesand Citations by
SelectedCountries/Regions, 2000-2010
400000
300000
200000
100000
0
No.
2000 2009
Otherb
Other Asiac
China
Japan
European Uniond
Overall
United States
No. of Medical
Research Articles
2000
49946
10029
3937
26755
114970
321795
116156
2009
63483
20790
18399
21477
120421
367229
122659
Annual
Growth Rate, %a
2000-2009
1.5
2.7
8.4
18.7
2.4
0.5
0.6
No. of medical research articlesA
Year
12000
10000
8000
6000
4000
2000
0
No.
2000 2009
Otherb
Other Asiac
China
Japan
European Uniond
Overall
United States
No. of Highly Cited
Medical Research
Articles
2000
763
20
16
345
2079
8626
5402
2010
1034
113
82
294
2936
10189
5729
Citation Index
of Highly
Cited Articles
2000
NA
0.57
0.1
0.22
0.5
0.68
1.67
2010
NA
0.59
0.22
0.22
0.45
0.86
1.63
Compound
Annual Growth
Rate (Citation
Index), %a
2000-2009
NA
0.4
8.6
0.3
1.0
2.5
0.2
No. of highly cited medical research articlesB
Year
NA indicates notavailable.Medical researchwas defined as
thelifesciencesand
psychology, excludingagricultural science. Article counts
reportedby the
National Science Foundationwere fromthe Thomas Reuters Science
Citation
Indexand Social Science Citation Index,18 classifiedby year of
publicationand
assigned tocountries onthe basis ofinstitutional addresseslisted
oneach
article.Articleswerecounted ona fractional basis;ie, forarticles
with
collaborating institutions frommultiple countries,each country
received
fractionalcredit on the basisof proportionof its participating
institutions.
Citationswerebasedon a 3-yearperiodwith 2-year lag; eg,citations
for2000
arereferences made inarticles in 2000 toarticlespublishedin
1996-1998.The
citationindexof highlycitedarticles wasdefinedas theshare ofthe
worlds top
1% citedbiomedical researcharticles divided bythe shareof
theworlds
biomedicalresearcharticles in the citedyear window.
a Compoundannualgrowthrate(CAGR) supposingthatyearA isxand yearB
is
y, CAGR = (y/x){1/(BA)}1.
bOtherincludesthe remaining159 nations ofthe world withinthe
original
database.
c Other Asia includes India,Indonesia, Malaysia,
Philippines,Singapore, South
Korea, Taiwan,and Thailand.
dTheEuropeanUnion includes 27 Europeannations.
Clinical Review & Education SpecialCommunication TheAnatomy
of Medical Research
184 JAMA January 13,2015 Volume 313, Number2 (Reprinted)
jama.com
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
12/16
-
8/10/2019 The Anatomy Of Medical Research
13/16
Copyright 2014 American Medical Association. All rig hts
reserved.
shouldbe aimed atobviating currentlimitationsof
theexistingbal-
kanized corporate, venture capital, NIH, and university
practices.
Examplesof newmodels arethe BroadInstitutein Cambridge,Mas-
sachusetts (genomics), BioDesign Institute at Arizona State
Uni-
versity, Tempe (biomedical engineering), and Allen Institute
for
Brain Sciences, Seattle,Washington(neurological and
psychiatric
disease). Each of these seeks to optimize individual and
institu-
tionalcontributions while ensuringfunding. Eachorchestrates
ex-ternal relationships.
Underinvestment in Improving Delivery of Health Services
Investment in new ways to deliver better, more effective, and
less
expensive medical care has neither economic impetus nor
profes-
sional recognition compared with technological innovation or
ba-
sic discovery.
Funding for health services research has increased 37% from
$3.7 billion to $5.0 billion over the lastdecade (Figure 6).
However,
thisgrowthhasoccurredonaverysmallbase.Totalfundingforhealth
services research is 0.3% of total health care funding (eFigure
1 in
the Supplement) compared with 4% toward new drugs and de-
vices.Thatis, theUnited States spends$116billion on research
aimed
at 13% of total health care costs but only $5.0 billion aimed at
the
remaining 87% of costs.1
Why the disparity in investment? One major difference is
that
new drugs anddevices command favorable prices, and their
value
accrues directly to the firm that invests in them. In contrast,
ser-
vice innovations canreducemorbidity andmortality while also
re-
ducing cost, butfinancial returns toinnovatorsmay be negligible
or
even negative.Forexample, asshown byArriagaet al32and Prono-
vost and Wachter,33procedure checklists andother simple
precau-
tions are effectivebut may result in lower paymentsto
hospitals.34
This mismatch between who invests (the hospital) and who is
re-
warded(the insurer) is a fundamental barrier, even
thoughclinical
benefitisenormousandtotalsavingsmayexceedthereturnonmany
categories of blockbuster drugs.35
Three other factors pose barriers:
Behavior
change.Disruptionofthecurrentpatternsofcareisthreat-
ening to physicians and hospitals, even when shown to
produce
comparable or better clinical outcomes, higher patient
satisfac-
tion, andlowercost than traditionalcare.36Examplesinclude
tele-
medicine, daily monitoring, and intensive in-home services.
Data quality. Claims databases, electronic medical records,
and
other sources of clinical information are not yet sufficiently
reli-
ableto informresearch.Recentinitiatives areaimed at linking
sepa-
rate sources of data and introducing standards to support
research34-37 and are a specific goal of international
measure-
mentcollaborationsfor chronic illnesses (eg,the International
Con-
sortium for Health Outcomes Measurement),
38
and alliancesamong insurers, hospitals, and clinicians for the
most severely ill
patients (eg, Wellpoint/Emory Health).39
Communications. Clinicalservice innovation is
moredifficultthan
the introduction of a new drug or procedure because it
requires
manyindividualsto adjust theway theyinteract, communicate,
and
useinformation.Moreover,tohaveanyeffect,culturechangemust
occur throughout large, hierarchical organizations. Cultural
barri-
ersare potentreasons whysmall-scale demonstrationprojectsare
rarely generalized,even whenthey areinitially
effective.40There-
fore, research should focus on devising reliable, effective
inter-
ventionsthat sustainbetter practices,with lessons adopted
from
other complex organizations (eg, military or
transportation).
Neither the organizations norfinancesexist to innovate on
the
scale required. Small, incremental federal or foundation grants
are
an ineffective spur of sustainedchange in clinical practice
because
behavioraland culturalissues remainunaddressed.It is
unlikelythat
recent federal and state risk sharing (accountable care
organiza-
tions)orotherincentiveswillprovetobeadequateforthesamerea-son.Therefore,
morefundamental changes are needed. In particu-
lar, 3 changes should be considered.
Additional investment by insurers and health systems in
delivery
innovation to bring them to the median of other service
indus-
tries. This increment could produce an annual influx of $8
billion
to$15 billion,potentiallyquadruplingthe levelof
effortoverall,and
can be funded from administrative simplification and
savings.
Sharply increasing federal support of service sector
innovation,
which canbe channeled through theCenters forDisease Control
and Prevention, Public Health Service, AHRQ, Centers for
Medi-
care& Medicaid (CMS), Patient-Centered Outcomes
ResearchIn-
stitute,and NIH. Fundsmightbe generatedby allocating 50%all
savings generated over the next decade by CMS demonstration
projects andby creatingnew regionalprivatehospitalphysician
insurer innovationconsortia toundertake wholesale changein
de-
livery.
Encouragementofnewentrantswhoarepreparedtomakebasic,
highly disruptive changes in service delivery (via tax credits
and
other incentives thatare comparable withthosenow available
for
investment in plant and equipment). Examples now on the
hori-
zon include provision by pharmacies of chronic disease care
(for
hypertension and depression) and use of simple
self-monitoring
technologies linked by a ubiquitous internet-of-things to
auto-
mated artificialintelligence agents forasthmaand
diabetescon-
trol. Such examples are threatening to many physicians
andhos-
pitals but have the potential to lowercosts and improve
quality.41
The Challenge of Globalization
Biomedical science and improved health are tied closely to
growth
of a countrysgeneral economy.42Theprimacyof theUnited States
as the source of biomedicaltechnology (anduntil recently,
longev-
ity)has correspondedwith a 4-decade-long improvement inreal
per-
sonal incomes. In turn, investment in science and technology
has
been a potent force producing higher personal incomes and
total
GDP,withthelongerlifeexpectancythatwasachievedbetween1970
and1990estimatedtohaveaddedabout35%toUSGDPby2000.43
Some have suggested thata domestic, US-centric perspective
is antiquatedand parochial in an era of globalization
becausepeople,
ideas,capital,andinformationarehighlymobile.44TheUnitedStates
hasbeen theworlds leader for6 decades in investment in
scienceand technology research and development. In 2012, the
United
States spent$366 billionon allresearchand development,or
2.8%
of GDP.45 However, the UnitedStates declined from sixth in
2000
to 10th in 2012 in its proportion of research and development
in-
vestment compared with the 34-country Organisation for Eco-
nomic Co-operation and Development. In Asia, South Korea and
Chinanoweachspendabout2%ofGDP,withChinaexpectedtosur-
pass theUnited States in absolute funding withina decade.45
This
trend,along withaggressivepatent practices
bysomecountries(no-
tablyChina)ordisregardofintellectualpropertyrights(inAfrica,Cen-
Clinical Review & Education SpecialCommunication TheAnatomy
of Medical Research
186 JAMA January 13,2015 Volume 313, Number2 (Reprinted)
jama.com
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
14/16
Copyright 2014 American Medical Association. All rig hts
reserved.
tral Europe, and India), raise barriers to the diffusion of
clinical in-
novations between countries.
Two areas are ofparticular concern:erosionof thepublicssup-
portforscienceintheUnitedStatesandhesitancytoreformthepat-
ent system.
PublicOpinion
Recent polls show erosion of public support for biomedical
re-searchcomparedwithother priorities. Supporthas
declinedsteadily
since 2000 and is now well behind concerns about the
economy,
domestic security, immigration, crime, and the US role in
interna-
tionalaffairs.46,47The trendis not confinedto the
UnitedStatesbut
is alsoevidentin Europe. Despitethe demonstrablesuccessesof
ear-
lierdecades,theprimacyofscienceasthesourceofimprovedhealth
is todayquestioned because of theconvergence of several
forces.
First,despitebold promises, advances visibleto thepublichave
been less frequent because solutions to many conditions like
au-
tism, Alzheimerdisease, andmost cancersremain elusive,with
nei-
ther effective prevention nor treatment, despite intensive
re-
search. Second, drug discovery has proven more difficult and
less
predictable than many hadexpected,witha decline overthe past
2
decades in altogether newclasses of drugs,new registrations,
and
drugsin clinicaltrials.Third,the economicsof medical
advancesare
being scrutinized as a source of added insurance cost, with
grow-
ing pressure to justify clinical value using objective criteria,
formal
tools of technology assessment, and consideration of
quality-of-
lifemeasures separatelyfrom thosethat affectmortality.Some
tech-
nology skeptics have evenurgedthatthe United Statestakea
tech-
nologyholiday for a decade, suggesting that the money saved
be
spent on ensuring that everyone receives existing preventive
and
therapeutic means, even if this slows scientific
discovery.48
Such tensions are perhaps inevitable, given the high cost
and
poorperformanceof US health careas judged by international
mor-
tality comparisons. Skepticismof medical research is evident in
re-
cent US budget discussions, which have favored the physical
sci-ences as faster, reliable, and more predictable routes to
US
competitiveness than the uncertainties of medicine. Also,
medical
devices and new manufacturing practices for large-molecule
bio-
pharmaceuticals areheavilydrivenby engineeringadvances,
which
in turn depend more on the physical sciences and less on the
bio-
logical sciences.Thesetrends imply that pressure will mount to
di-
vertresources away fromchallenging
buthigh-potentialavenuesin
biology.
Patents and Intellectual Property
As this analysis demonstrates, at the same time support for
bio-
medical research in theUnited States haswavered,
globalinterest
in biomedicalresearch is increasing.
49
Asia andEurope arenow onparwiththe UnitedStatesin
therelativenumber ofresearchers, and
Asia, especially China, is making rapid gains in life science
patents
andhighlycited publications. Althoughthe United States is
farfrom
losing its preeminent role in biomedical research, similar
historical
changeshave occurredin other industries (eg,electronics,
automo-
biles, industrial manufacturing) thatover time reshaped the
coun-
trys competitiveness. Many in the United States applaud the
new
interest in other countries as a reflection of the truly
international
reach of science, since discoveriesmade anywherecan be ap-
plied here. This optimistic view neglects the strong barriers
cre-
atedby intellectualpropertypractices,which reward patenting
any
discovery or technique, no matter how incremental or
trivial.
Apatentsprimarypurposeistofosterinnovationbymakingnew
knowledge generally available in order that successors may
im-
proveontheoriginalinvention.Inreturn,theinventorreceivesatem-
porarymonopoly. Recently, however, patentshave beenused
tocap-
turefinancialvalueofadiscoveryorproductattheexpenseoffurther
invention, a practice known as rent-seeking. Current
intellectualproperty practices inhibit rather thanenhance
biological discovery
and clinical innovation.50
Several factors bear on the global pattern we observed in
this
analysis: patents on basic discoveries before utility is
demon-
strated (such as of cancer-related genes), tying surgical
proce-
dures (such as deep brain stimulation) to specific patented
de-
vices, abuseof thelitigationprocess by patent
aggregators(known
formallyas nonperforming entities orpejorativelyas
patenttrolls),
andthehighcostof patentfiling anddefensein multiple
countries.
Universitiesandinvestigatorsalike seethat
patentingearly-stagedis-
coveriesrarelyresultsin financial returns
becausecostsexceedroy-
alty revenue, except for occasional, high-value findings, which
are
serendipitous and economically unpredictable.
Threechangescan alignintellectualproperty protections with
incentives forsubstantive, clinically important advancesand
would
be accomplishedby changes to current federal law.51,52
Defer patents to later in thediscovery chain, awardingto the
en-
tity demonstrating clinical utility as well as the inventor.
Because
costs aregreatestand riskshighest to those whofinanceand
con-
duct later-stage clinical development, those risks should be
re-
flected in intellectual property protections.
Ensure that patents are granted only for truly novel, not just
in-
cremental, technologies, withclinicalprocedures remainingin
the
public domain.
Establish patent pools, which allow innovators to share value
and
cost to encourage free exchange of information and set
technol-
ogy standards. Patent pools haveoperatedsuccessfully
sincethe19th century and are today common in semiconductors,
aero-
space, and entertainment.51,53
Taken together, these changes could foster fundamental, not
incremental,innovation andcould facilitate moreeffective
collabo-
rations. They are also prerequisites for generating new sources
of
investment.
Conclusions
The informationassembled inthis article does notdo justice
tothe
breadthanddepthofmedical researchin theUnitedStates andother
countries. For anycurrent orfuturepatient,research provides
hope.Forthe researcher, unanswered biologicaland
clinicalquestionsare
endlessly fascinating.For a company or its investors, new
products
and services promise financial return, often at levels greater
than
other industries.For thepolicymaker, biomedicalresearch isa
route
tonationalcompetitivenessas well asto enhancedpublic
healthand
economic vitality.
Our perspective for this examination has been primarily eco-
nomic, although the value of research surely is not solely
eco-
nomic. Therefore, in our view, biomedical science and
technology
must be seen in a broader context, with its myriad roles
recog-
TheAnatomy of Medical Research Special Communication
ClinicalReview & Education
jama.com (Reprinted) JAMA January 13,2015 Volume 313, Number2
187
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
15/16
Copyright 2014 American Medical Association. All rig hts
reserved.
nized: as a source of competitiveness on theinternational stage;
as
a vehicle tosatisfy curiosity; asa meansto provide
realistichopeto
patientsand familieswho mustconfront grave conditions.
Noneof
thoseroleswillnecessarilybereflectedinreducedhealthcarecosts.
Therefore, a newcalculus isrequired toweighthemas decisions
of
cost andvalueare made.
Clearly,thepaceofscientificdiscoveryandneedforserviceim-
provement have outstripped the capacity of current financial
andorganizational models to support the opportunities afforded.
Theanalysis underscores theneed forthe United States to find
newsources to support medical research,if theclinicalvalue of
its
past science investment and opportunities to improve care are
to
be fully realized. Substantial new private resources are
feasible,
thoughpublic funding canplay a greater role.Bothwill require
non-
traditionalapproaches if theyare to be politically and
economically
realistic.Givenglobaltrends, theUnitedStateswillrelinquishits
his-
toricalinnovationlead in thenext decade unless
suchmeasuresareundertaken.
ARTICLE INFORMATION
Author Contributions: DrMoseshad full accessto
allof thedatain thestudy andtakes responsibility
fortheintegrity ofthe data andthe accuracy ofthe
data analysis. Dr George and Mr Palisch contributed
equally.
Study concept and design: Moses, Matheson,
Cairns-Smith, Dorsey.
Acquisition, analysis, or interpretation of data: All
authors.
Drafting of the manuscript: Moses, Matheson,
Cairns-Smith, George, Palisch.
Critical revision of the manuscriptfor important
intellectual content: All authors.
Statistical analysis: Moses, George, Palisch.
Administrative, technical, or material support:
Moses, Matheson, Cairns-Smith,Dorsey.
Study supervision: Moses, Matheson, Cairns-Smith,
Dorsey.
Conflict of Interest Disclosures: All authors have
completedand submitted theICMJE Form for
Disclosureof PotentialConflicts of Interest.Dr
Moses reports membership in a variety of
foundation andcompanyboards in healthcareand
financial services. Dr Moses, Messrs Matheson and
Palisch, and Dr Cairns-Smith report providing
management consultingservices to hospital
systems, insurers,foundations, and
pharmaceutical, device, and IT companies.DrDorsey reports
consultancyfor Amgen, Avid
Radiopharmaceuticals, Clintrex, Lundbeck,
Medtronic,the National Instituteof Neurological
Disordersand Stroke,and TransparencyLife
Sciences;a filed patent related to telemedicine and
neurology;and stock/stock options in Grand
Rounds (a second opinion service). No other
disclosureswere reported.
REFERENCES
1. MosesH III, MathesonDHM,Dorsey ER,George
BP, Sadoff D, Yoshimura S. Theanatomyof health
care in theUnited States.JAMA. 2013;310(18):1947-
1963.
2. Moses H III, DorseyER, MathesonDH, ThierSO.
Financial anatomy of biomedical research. JAMA.
2005;294(11):1333-1342.
3. DorseyER, deRoulet J,Thompson JP, etal.
Funding of US biomedicalresearch,2003-2008.
JAMA. 2010;303(2):137-143.
4. National Institutesof Health Officeof Budget.
Price indexes. 2013. http://officeofbudget.od.nih
.gov/gbiPriceIndexes.html. Accessed December 23,
2013.
5. Johnson JA. Brief Historyof NIHFunding: Fact
Sheet. Washington, DC: Congressional Research
Service; 2013. http://www.fas.org/sgp/crs/misc
/R43341.pdf. Accessed April15, 2014.
6. Pharmaceutical Researchand Manufacturers of
America.2013 Biopharmaceutical Research Industry
Profile. July 2013. http://www.phrma.org/sites
/default/files/pdf/PhRMA%20Profile%202013.pdf.
Accessed November24, 2014.
7. Chatterjee SK, RohrbaughML. NIH inventions
translateinto drugsand biologics withhigh public
health impact. Nat Biotechnol. 2014;32(1):52-58.
8. Gross CP, Anderson GF, Powe NR. Therelation
between funding by the National Institutesof
Healthand theburdenof disease. N EnglJ Med.
1999;340(24):1881-1887.9. GillumLA, Gouveia C, DorseyER, etal.
NIH
disease funding levelsand burden of disease. PLoS
One. 2011;6(2):e16837.
10. Citeline. Citeline Pharma R&D AnnualReview
2014. 2014. http://www.citeline.com/resource
-center/whitepapers/. Accessed April21, 2014.
11. Pharmaceutical Researchand Manufacturers of
America. Rare Disease:A Report onOrphan Drugs
in the Pipeline. http://www.phrma.org/sites/default
/files/pdf/Rare_Diseases_2013.pdf. Accessed April 21,
2014.
12. Reardon S. Regulatorsadopt moreorphan
drugs. Nature. 2014;508(7494):16-17.
13. National Science Foundation. Business R&D and
innovation survey.http://www.nsf.gov/statistics
/srvyindustry/about/brdis/.AccessedApril 21, 2014.
14. USCensusBureau.Annual andquarterly
services.http://www.census.gov/services/. Accessed
April21, 2014.
15. Currency converterforeign exchangerates. http:
//www.oanda.com/currency/converter/. Accessed
December23, 2013.
16. Organisation forEconomicCo-operationand
Development. OECDscience,technology and R&D
statistics. http://www.oecd-ilibrary.org/science
-and-technology/data/oecd-science-technology
-and-r-d-statistics_strd-data-en. Accessed April 21,
2014.
17. Thomson Innovation. http://info
.thomsoninnovation.com/. Accessed April21, 2014.
18. NationalScience Foundation. Science andengineering
indicators2012: outputs of S&E
research: articles and patents. http://www.nsf.gov
/statistics/seind12/c5/c5s4.htm. Accessed April 21,
2014.
19. McGrawHillFinancial. S&PDowJonesindices
data services. http://www.djindexes.com
/dataservices/?go=sectorclassification. Accessed April
21, 2014.
20. New York Stock Exchange.Index services. http:
//www1.nyse.com/about/listed/mkt_indexes_other
_us.shtml. Accessed November 24, 2014.
21. Stevens H. Life Outof Sequence:A Data-Driven
Historyof Bioinformatics. Chicago, IL: Universityof
Chicago Press; 2013.
22. Goodwin I. Engineersproclaimtop
achievements of 20thcentury, but neglect
attributing featsto roots in physics. PhysToday.
2000;53(5):48-49.
23. FortunatoS. Prizes: Growing timelag threatens
Nobels. Nature. 2014;508(7495):186.
24. Daniels RJ,RothmanP. Howto reverse
the graying of scientific research.March 4, 2014.
http://online.wsj.com/news/articles/SB10001424052702304026804579411293375850348.
Accessed April15, 2014.
25. Moses H III, MartinJB. Biomedical research and
health advances. N EnglJ Med. 2011;364(6):567-571.
26. Crowley WFJr,SherwoodL, SalberP,et al.
Clinicalresearch in theUnitedStates ata
crossroads: proposal fora novel public-private
partnership to establish a national clinical research
enterprise.JAMA. 2004;291(9):1120-1126.
27. Bridgingthe gap. The Economist. June 28,2014.
http://www.economist.com/news/united-states
/21605932-country-where-everyone-drives-
america-has-shoddy-roads-bridging-gap. Accessed
November26, 2014.
28. Greenbonds: springin theair. The Economist.
March 22, 2014. http://www.economist.com/news
/finance-and-economics/21599400-bonds-tied
-green-investments-are-booming-spring-air.Accessed
April21, 2014.
29. OrszagPR, Emanuel EJ. Healthcarereform and
costcontrol.N EnglJ Med. 2010;363(7):601-603.
30. CallahanD. Taming the Beloved Beast:How
Medical Technology Costs Are Destroying Our Health
CareSystem. Princeton,NJ: PrincetonUniversity
Press; 2009.
31. Mullard A. Drug makersand NIHteamup tofind
and validate targets. NatRev Drug Discov. 2014;13
(4):241-243.
32. Arriaga AF, Gawande AA,Raemer DB,et al;
Harvard Surgical Safety Collaborative. Pilottesting
of a model for insurer-driven, large-scalemulticenter simulation
training foroperating room
teams.Ann Surg. 2014;259(3):403-410.
33. Pronovost PJ, Wachter RM. Progressin patient
safety: a glass fullerthanit seems.Am J Med Qual.
2014;29(2):165-169.
34. EappenS, Lane BH,RosenbergB, etal.
Relationship between occurrence of surgical
complications and hospital finances.JAMA. 2013;
309(15):1599-1606.
35. Semel ME,ReschS, HaynesAB, etal. Adopting
a surgical safetychecklistcouldsavemoneyand
Clinical Review & Education SpecialCommunication TheAnatomy
of Medical Research
188 JAMA January 13,2015 Volume 313, Number2 (Reprinted)
jama.com
Copyright 2014 American Medical Association. All rig hts
reserved.
wnloaded From: http://jama.jamanetwork.com/ on 01/15/2015
-
8/10/2019 The Anatomy Of Medical Research
16/16
improve thequalityof care in UShospitals. Health
Aff (Millwood). 2010;29(9):1593-1599.
36. CryerL, Shannon SB,VanAmsterdam M,Leff
B. Costs forhospital at homepatientswere19%
lower, withequal or better outcomescomparedto
similarinpatients. HealthAff (Millwood). 2012;31(6):
1237-1243.
37. Pearl R. KaiserPermanenteNorthern California:
current experiences withInternet, mobile, and
video technologies. HealthAff (Millwood).
2014;33(2):251-257.
38. International Consortiumfor Health Outcomes
Measurement. http://www.ichom.org/the-global
-standard/. Accessed April15, 2014.
39. Mathews AW. WellPoint advises
health-care providers.March 18, 2014.
http://online.wsj.com/news/articles
/SB10001424052702303563304579447632330535824.
Accessed April 15, 2014.
40. UrbachDR, GovindarajanA, SaskinR, Wilton
AS, Baxter NN.Introduction of surgical safety
checklistsin Ontario, Canada. N EnglJ Med. 2014;
370(11):1029-1038.
41. Cortese DA.A healthcareencounterof the21st
century.JAMA. 2013;310(18):1937-1938.
42. MokyrJ. The Lever of Riches: Technological
Creativity and Economic Progress. Oxford, England:
Oxford UniversityPress; 1990.
43. Murphy K, Topel R. Diminishingreturns?the
costs and benefits of improving health. Perspect
BiolMed. 2003;46(3)(suppl):S108-S128.
44. FingarT,JisheF.Ties that bind: strategic
stability in theUS-Chinarelationship. Wash Q. 2013;
36(4):125-138.
45. Battelle.2012 Global R&D Funding Forecast.
December 2011. http://www.google.com
/url?sa=t&rct=j&q=&esrc=s&source=web&cd
=1&sqi=2&ved=0CB4QFjAA&url=http%3A%2F
%2Fbattelle.org%2Fdocs%2Fdefault-document
-library%2F2012_global_forecast.pdf&ei
=F2Z2VOXTOK_0iAL9t4HwBQ&usg
=AFQjCNHrfksQwizVx6NpJHsMu-3D52dXGw&sig2
=J1eOrORABYjbIfm9GPTDmA&bvm=bv
.80642063,d.cGE. Accessed November26, 2014.
46. Emanuel EJ.The futureof biomedical research.
JAMA. 2013;309(15):1589-1590.
47. Pew ResearchCenter. Publicpraises science;
scientistsfault public,media. July 9,2009.http:
//www.people-press.org/2009/07/09/public
-praises-science-scientists-fault-public-media/.
Accessed April15, 2014.
48. Hoffman A, Emanuel EJ.Reengineering US
health care.JAMA. 2013;309(7):661-662.
49. ChakmaJ, SunGH, SteinbergJD,Sammut SM,
JagsiR. Asias ascentglobal trends in biomedical
R&D expenditures. N EnglJ Med. 2014;370(1):3-6.
50. StewartTA. The Wealth of Knowledge:
IntellectualCapital and the Twenty-FirstCentury
Organization. New York, NY: CrownPublishingGroup;
2007.
51. Lerner J,Tirole J. Intellectual property: a better
routeto techstandards.Science. 2014;343(6174):
972-973.
52. Azoulay P, Lerner J. Technological innovation
and organizations. In: Gibbons R, Roberts J, eds.
The Handbook of Organizational Economics.
Princeton, NJ:Princeton UniversityPress;2013:575-
603.
53. RaiAK, EisenbergRS. B