Embed Size (px)
Citation preview
The ABCs of CBT
Melissa A. Novak, LCSW, CST Licensed Clinical Social Worker Certified Sex Therapist MN Therapies www.mntherapies.com [email protected]
Melissa A. Novak, LCSW © 2016
Understanding the basic foundation and implementation of Cognitive Behavioral
Therapy
Objectives u Knowledge of the cognitive model and the
rationale for treatment
u Basic knowledge of key components to cognitive therapy such as the cognitive model, cognitive conceptualization and their components.
u Understanding of the cognitive conceptualization, its formulation and how it is used to guide treatment.
u Integrate various skills and techniques you already know into the conceptualization
Melissa A. Novak, LCSW © 2016
Why CBT? u It is an adaptable,
cohesive structure.
u Holds the therapist and client accountable.
u Helps focus sessions and treatment.
u Clients love it.
u Research.
Melissa A. Novak, LCSW © 2016
Cognitive Therapy Competency
u ACT Certification u http://www.academyofct.org/i4a/ams/
public/memberapp_description.cfm
u 2 Part Process u Part I: Preliminary Review of training and
knowledge of CBT
u Part II: Clinical Review of an actual case, including a taped session
u http://www.ucl.ac.uk/clinical-psychology/CORE/CBT_Competences/CBT_Competences_Map.pdf
Melissa A. Novak, LCSW © 2016
1
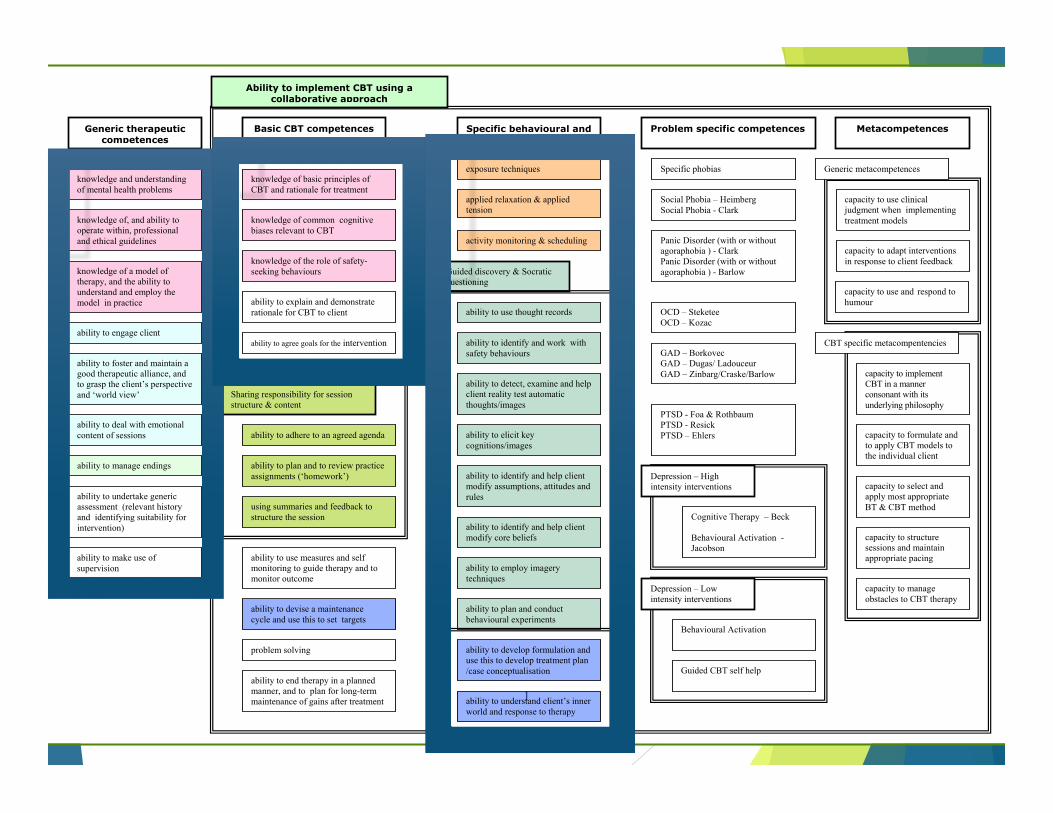
applied relaxation & applied tension
problem solving
Cognitive Therapy – Beck Behavioural Activation -Jacobson
exposure techniques Specific phobias
Specific behavioural and cognitive therapy
Problem specific competences
GAD – Borkovec GAD – Dugas/ Ladouceur GAD – Zinbarg/Craske/Barlow
Social Phobia – Heimberg Social Phobia - Clark
OCD – Steketee OCD – Kozac
activity monitoring & scheduling
Basic CBT competences
Sharing responsibility for session structure & content
ability to agree goals for the intervention
ability to plan and to review practice assignments (‘homework’)
using summaries and feedback to structure the session
ability to devise a maintenance cycle and use this to set targets
Guided discovery & Socratic questioning
ability to elicit key cognitions/images
ability to use thought records
ability to detect, examine and help client reality test automatic thoughts/images
ability to identify and help client modify assumptions, attitudes and rules
PTSD - Foa & Rothbaum PTSD - Resick PTSD – Ehlers
Behavioural Activation
ability to plan and conduct behavioural experiments
ability to develop formulation and use this to develop treatment plan /case conceptualisation
Panic Disorder (with or without agoraphobia ) - Clark Panic Disorder (with or without agoraphobia ) - Barlow
Metacompetences
ability to adhere to an agreed agenda
knowledge of common cognitive biases relevant to CBT
ability to identify and work with safety behaviours
ability to employ imagery techniques
ability to identify and help client modify core beliefs
capacity to implement CBT in a manner consonant with its underlying philosophy
capacity to manage obstacles to CBT therapy
capacity to use clinical judgment when implementing treatment models
knowledge of basic principles of CBT and rationale for treatment
ability to explain and demonstrate rationale for CBT to client
knowledge of the role of safety-seeking behaviours
Ability to structure sessions
ability to understand client’s inner world and response to therapy
Guided CBT self help
Depression – Low intensity interventions
Depression – High intensity interventions
capacity to adapt interventions in response to client feedback
capacity to formulate and to apply CBT models to the individual client
capacity to select and apply most appropriate BT & CBT method
CBT specific metacompentencies
capacity to structure sessions and maintain appropriate pacing
capacity to use and respond to humour
Generic metacompetences
ability to end therapy in a planned manner, and to plan for long-term maintenance of gains after treatment
ability to use measures and self monitoring to guide therapy and to monitor outcome
Ability to implement CBT using a collaborative approach
Generic therapeutic competences
knowledge and understanding of mental health problems
knowledge of, and ability to operate within, professional and ethical guidelines
knowledge of a model of therapy, and the ability to understand and employ the model in practice
ability to engage client
ability to foster and maintain a good therapeutic alliance, and to grasp the client’s perspective and ‘world view’
ability to deal with emotional content of sessions
ability to manage endings
ability to undertake generic assessment (relevant history and identifying suitability for intervention)
ability to make use of supervision
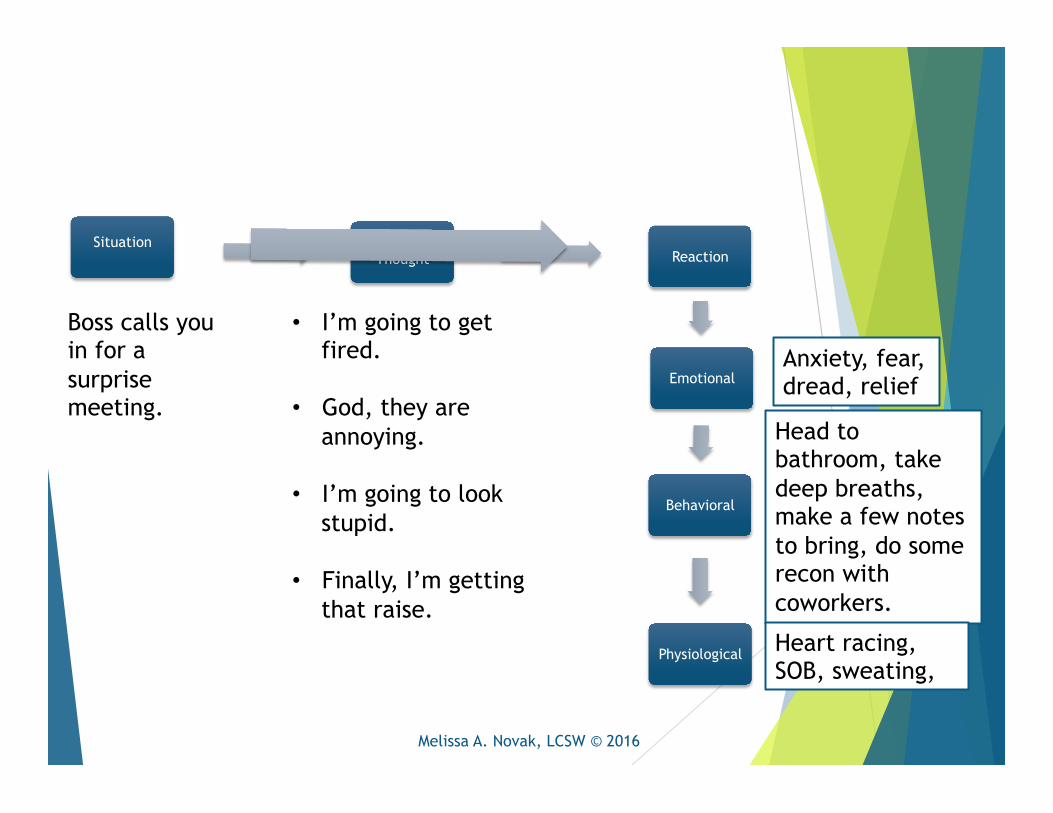
Situation
Boss calls you in for a surprise meeting.
Anxiety, fear, dread, relief
Head to bathroom, take deep breaths, make a few notes to bring, do some recon with coworkers.
Heart racing, SOB, sweating,
• I’m going to get fired.
• God, they are annoying.
• I’m going to look stupid.
• Finally, I’m getting that raise.
Reaction
Emotional
Behavioral
Physiological
Automatic Thought
Melissa A. Novak, LCSW © 2016
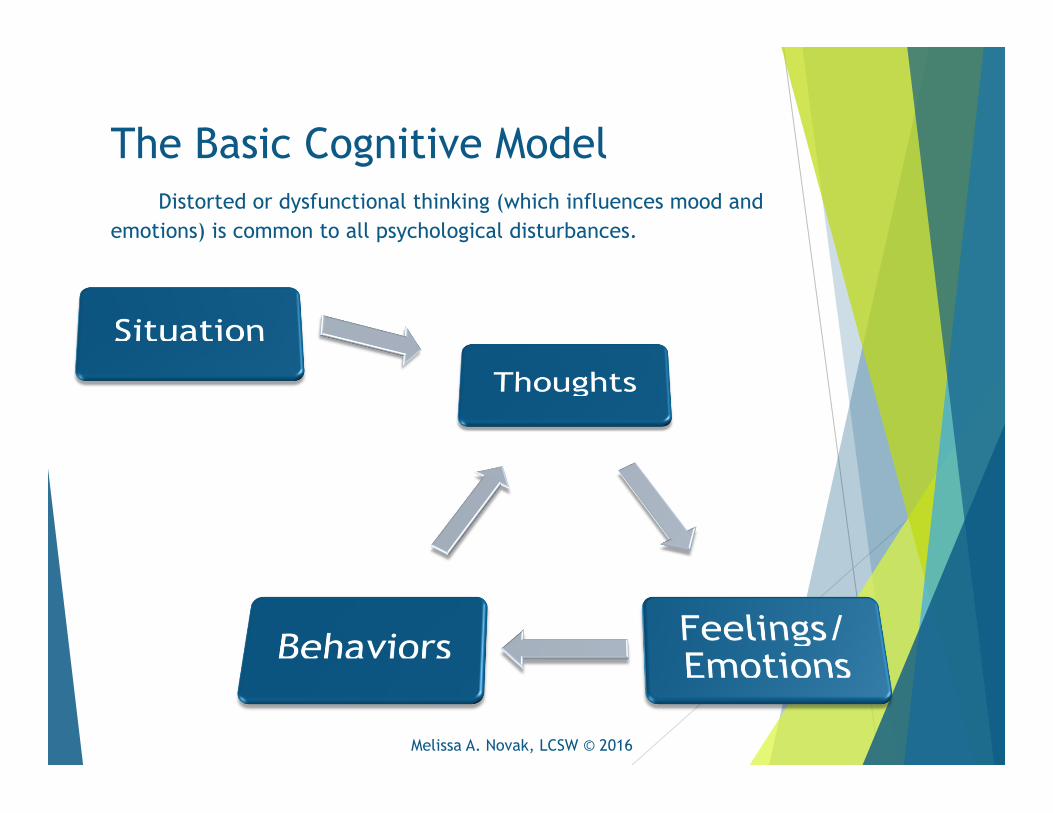
The Basic Cognitive Model Distorted or dysfunctional thinking (which influences mood and
emotions) is common to all psychological disturbances.
Melissa A. Novak, LCSW © 2016
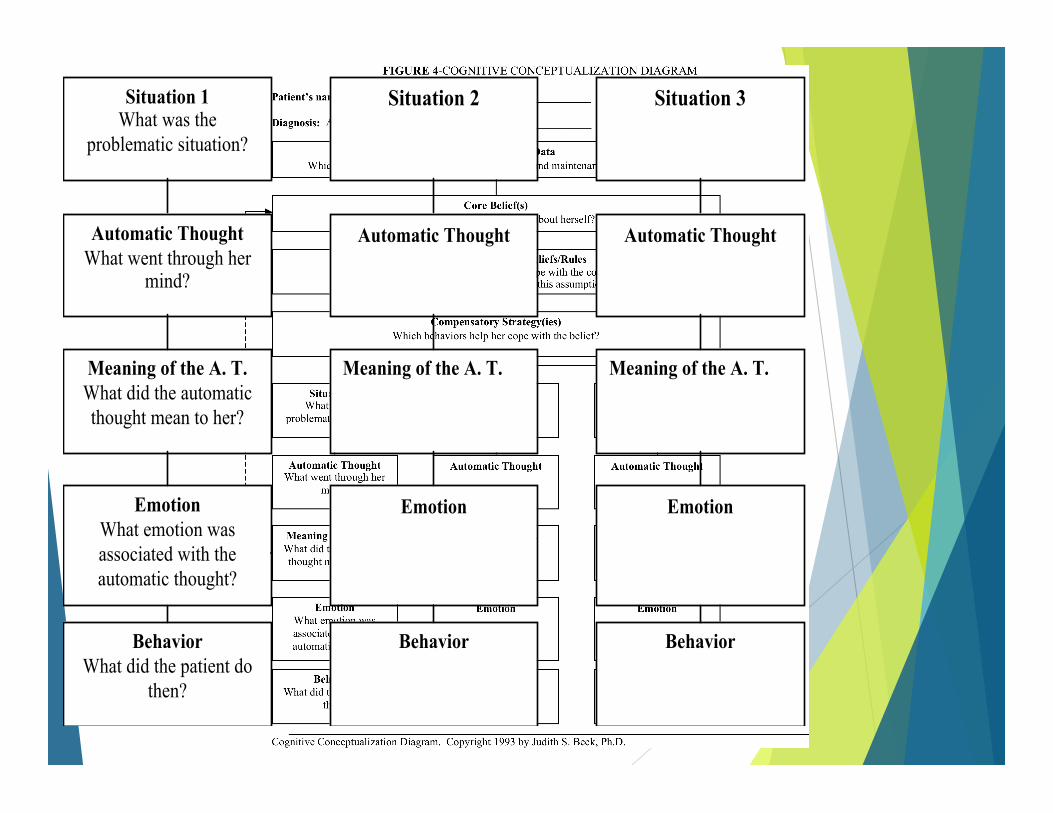
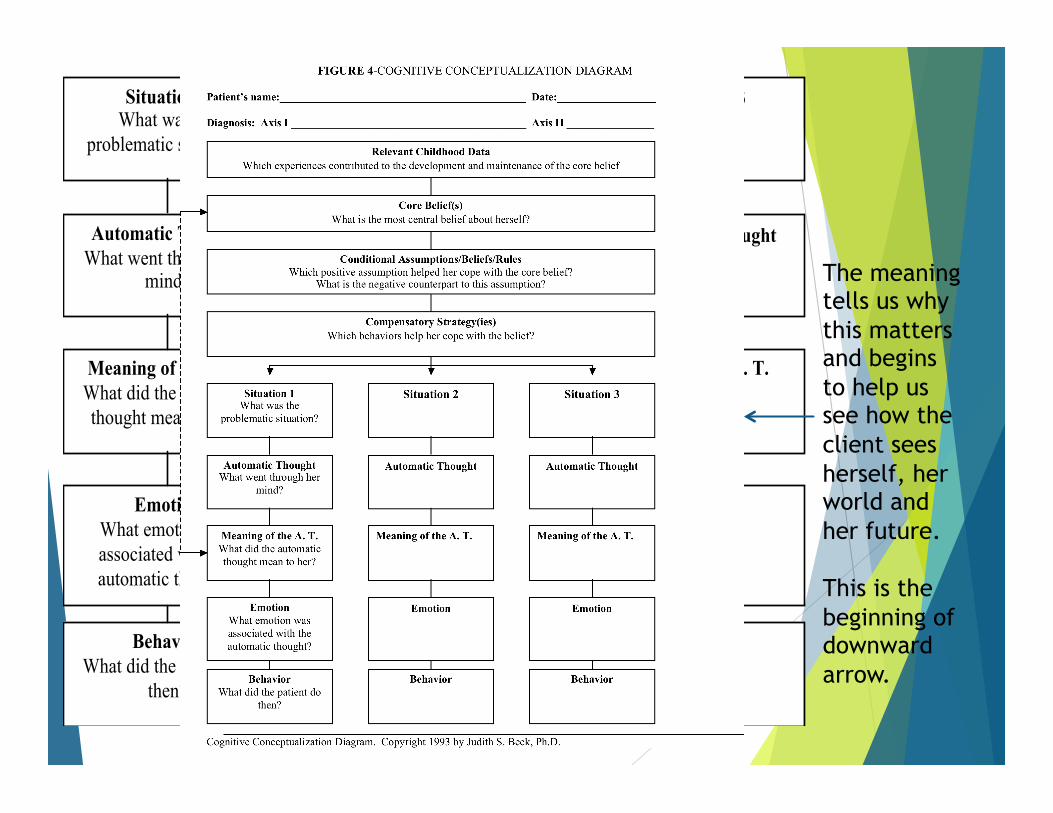
Situation 1 What was the
problematic situation?
Situation 2 Situation 3
Automatic Thought What went through her
mind?
Automatic Thought Automatic Thought
Meaning of the A. T. What did the automatic thought mean to her?
Meaning of the A. T.
Emotion What emotion was associated with the automatic thought?
Behavior What did the patient do
then?
Meaning of the A. T.
Emotion Emotion
Behavior Behavior
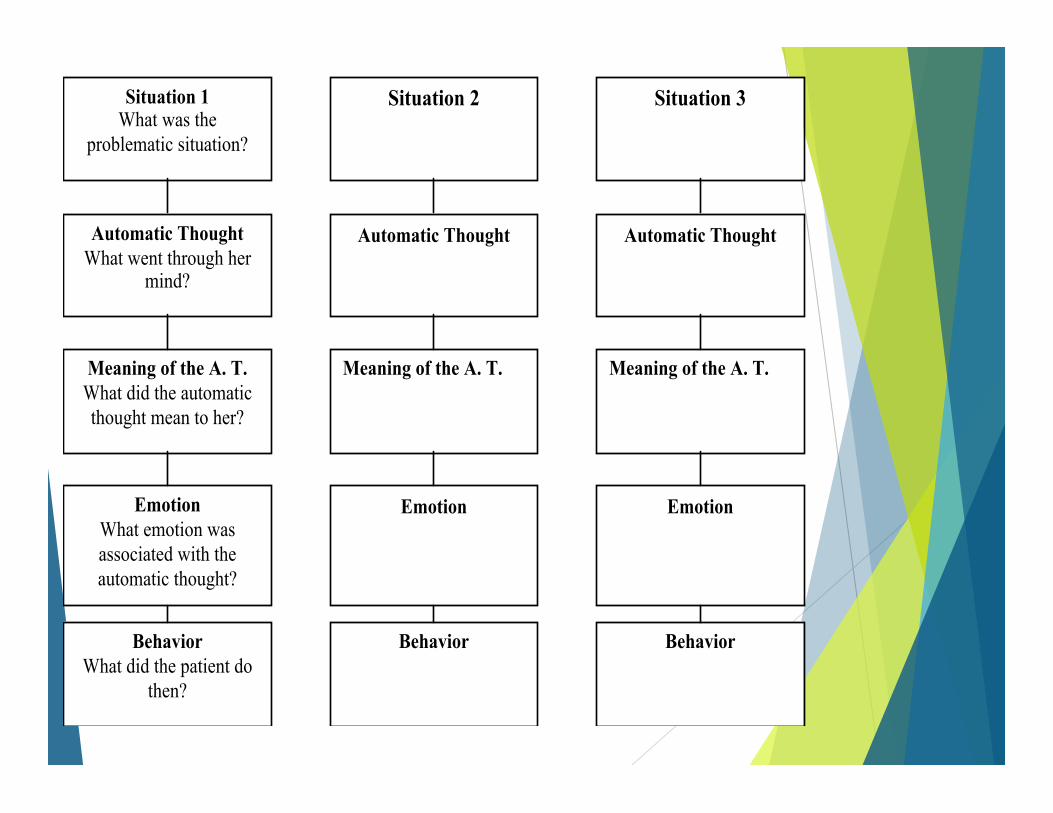
Situation 1 What was the
problematic situation?
Situation 2 Situation 3
Automatic Thought What went through her
mind?
Automatic Thought Automatic Thought
Meaning of the A. T. What did the automatic thought mean to her?
Meaning of the A. T.
Emotion What emotion was associated with the automatic thought?
Behavior What did the patient do
then?
Meaning of the A. T.
Emotion Emotion
Behavior Behavior
Identifying Automatic Thoughts/Emotional and Behavioral Patterns
u Ask the client to speak about a distressing situation.
u Notice a shift in affect and then prompt.
u “What went through your mind just then?”
u Take a feeling statement and reflect back as an absolute or a prediction. (“I worry I might fail the test.” -> “I am going to fail the test.”)
Melissa A. Novak, LCSW © 2016
“I wasn’t thinking anything.”
u Helpful questions to elicit “elusive” automatic thoughts. u Any hypotheses?
u Use another person.
u Emotions list
u Describe the physical state of feeling.
u Describe what you did
Melissa A. Novak, LCSW © 2016
Vignette: The Case of Jennifer u 40 something, white, cisgender, female requesting services to address recent break
up and apartment clutter.
u Has been on disability since being fired from job 15 years ago.
u Family Dynamic
u Middle child, lots of inter-sibling rivalry and fighting
u Mother and father had tumultuous relationship that ended; both had substance abuse issues
u Social
u Active in high school and academically successful
u Had friends but often felt left out and avoidant of bringing anyone home due to clutter and family
u Psych
u History of therapy with multiple providers
u Previous diagnosis of MDD, dysthymic disorder, ADHD
u Was on a cocktail of psychotropic meds which was reduced
u Obsessional, anxious, depressed, distrustful, defensive, hopeless and entitled

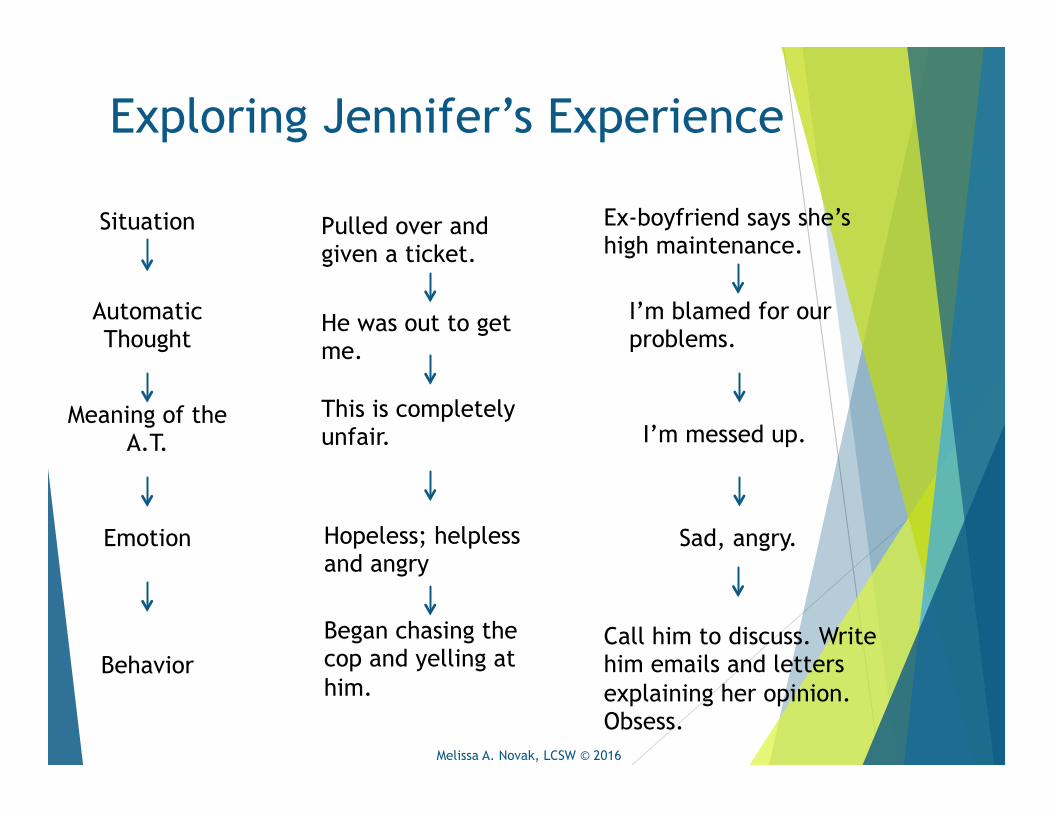
Exploring Jennifer’s Experience
Sad, angry.
I’m messed up.
I’m blamed for our problems.
Ex-boyfriend says she’s high maintenance.
Pulled over and given a ticket.
He was out to get me.
This is completely unfair.
Hopeless; helpless and angry
Began chasing the cop and yelling at him.
Call him to discuss. Write him emails and letters explaining her opinion. Obsess.
Situation
Automatic Thought
Meaning of the A.T.
Emotion
Behavior
Melissa A. Novak, LCSW © 2016
Assessing emotional intensity.
u LOW:
Cognitive/Insight Techniques
u Labeling distortions
u Thought logs u Hypothesis
testing u Reframes
u HIGH: Behavioral Techniques
u Sensory/Labeling u Exposures u Acting “as if” u Opposite Action u Emotion
Regulation u Distress
Tolerance u Activity Planning
Melissa A. Novak, LCSW © 2016
Challenging the Automatic Thoughts
u Are they true?
u Are they useful?
u Thought Logs
u Develop a hypothesis and test them (cognitive and behavioral options).
u Reframe and practice.
Melissa A. Novak, LCSW © 2016
Cognitive Distortions…
Challenging the Behavior and Emotion
u Acting “as if”
u Smiling/Posing
u Contrary Behavior
u Exposures
u Visualization
u Identifying needs
Melissa A. Novak, LCSW © 2016
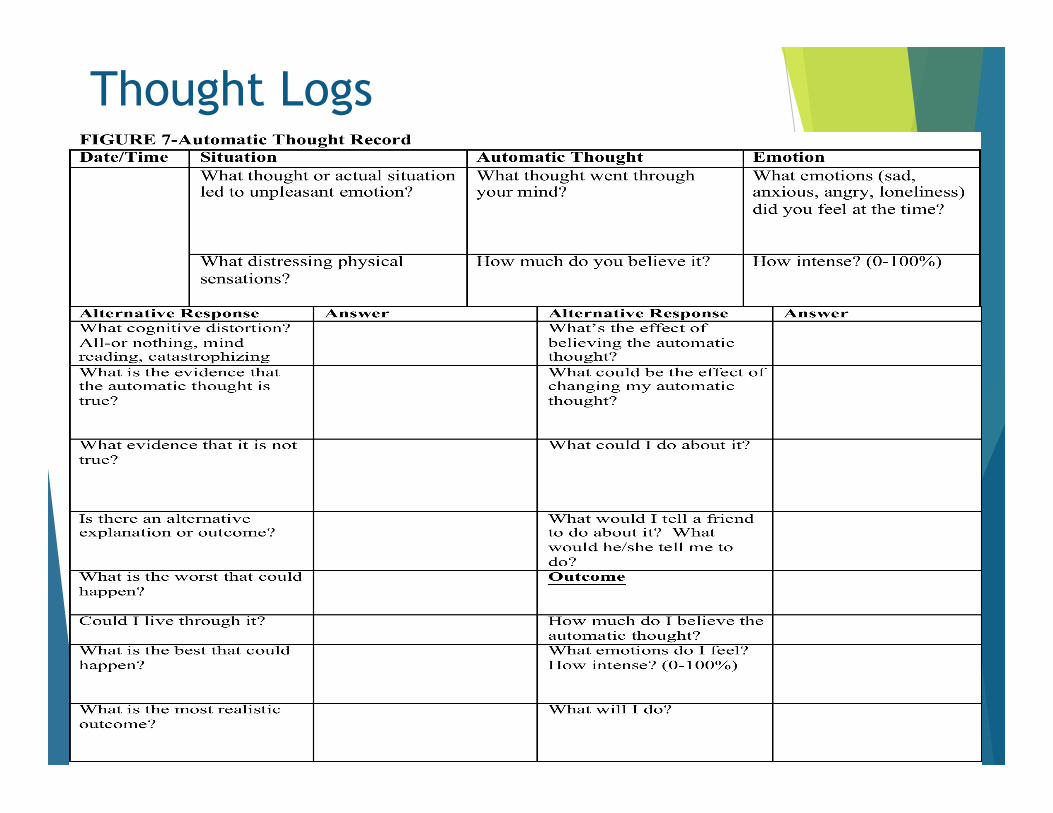
Thought Logs
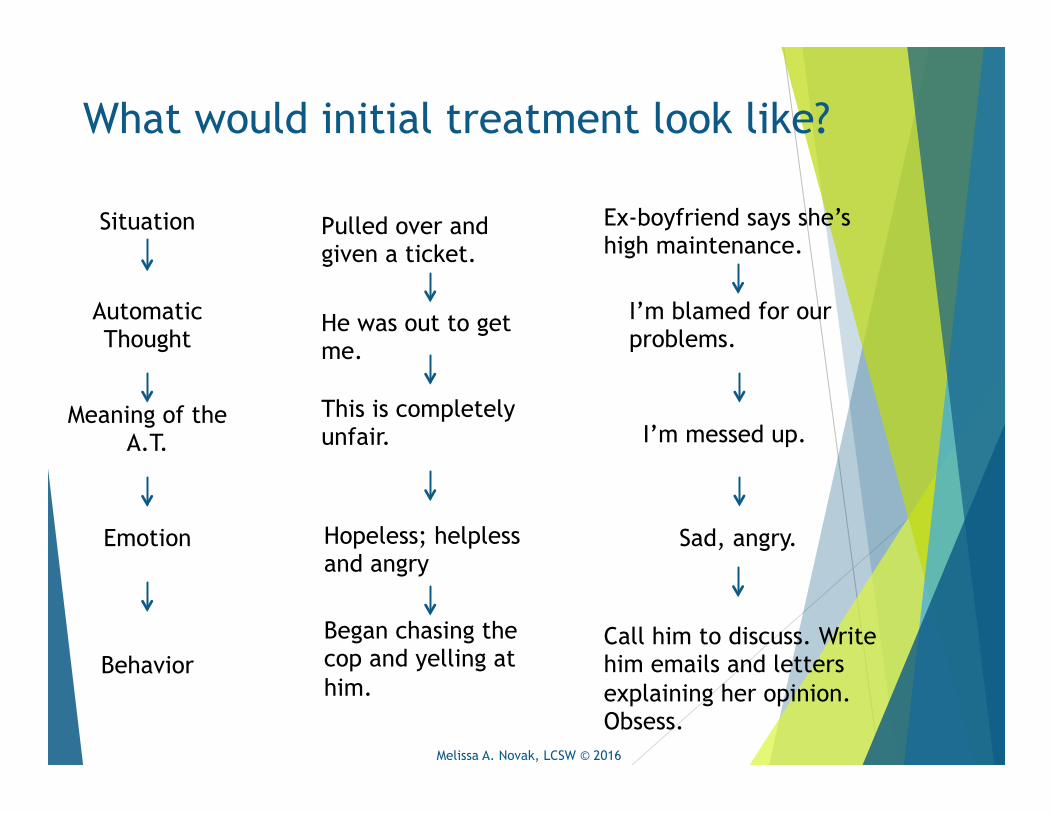
What would initial treatment look like?
Sad, angry.
I’m messed up.
I’m blamed for our problems.
Ex-boyfriend says she’s high maintenance.
Pulled over and given a ticket.
He was out to get me.
This is completely unfair.
Hopeless; helpless and angry
Began chasing the cop and yelling at him.
Call him to discuss. Write him emails and letters explaining her opinion. Obsess.
Situation
Automatic Thought
Meaning of the A.T.
Emotion
Behavior
Melissa A. Novak, LCSW © 2016
Situation 1 What was the
problematic situation?
Situation 2 Situation 3
Automatic Thought What went through her
mind?
Automatic Thought Automatic Thought
Meaning of the A. T. What did the automatic thought mean to her?
Meaning of the A. T.
Emotion What emotion was associated with the automatic thought?
Behavior What did the patient do
then?
Meaning of the A. T.
Emotion Emotion
Behavior Behavior
The meaning tells us why this matters and begins to help us see how the client sees herself, her world and her future. This is the beginning of downward arrow.
Exploring Jennifer’s Experience
Sad, angry.
I’m messed up.
I’m blamed for our problems.
Ex-boyfriend says she’s high maintenance.
Pulled over and given a ticket.
He was out to get me.
This is completely unfair.
Hopeless; helpless and angry
Began chasing the cop and yelling at him.
Call him to discuss. Write him emails and letters explaining her opinion. Obsess.
Situation
Automatic Thought
Meaning of the A.T.
Emotion
Behavior
Melissa A. Novak, LCSW © 2016
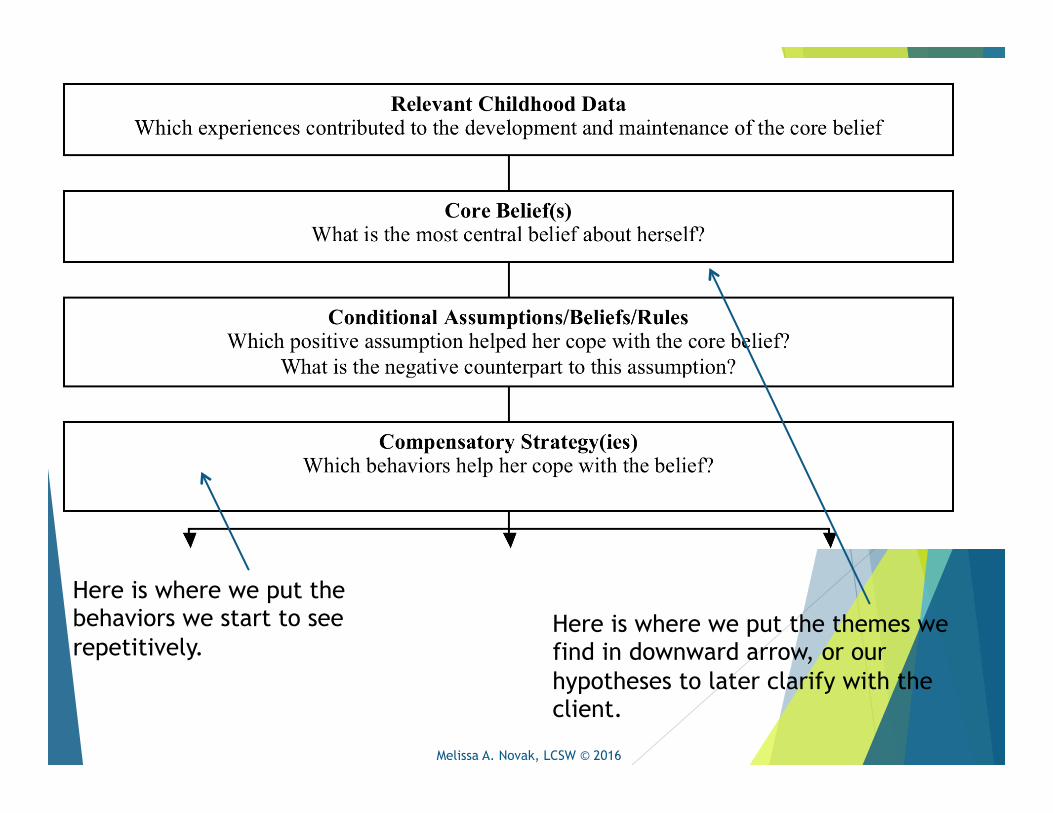
Here is where we put the themes we find in downward arrow, or our hypotheses to later clarify with the client.
Here is where we put the behaviors we start to see repetitively.
Melissa A. Novak, LCSW © 2016
Downward Arrow u Ask the client to examine what his/her thoughts mean, why they
matter?
u “And what if _______ happens?”
u “So what?”
u “What’s so bad about _________?”
u Compile themes of identified automatic thoughts.
u The client’s affect will typically significantly shift when you’ve identified the core belief.
u Often times clients will provide several distressing thoughts. Focus on one thought by having them select the one that is most charged.
Melissa A. Novak, LCSW © 2016
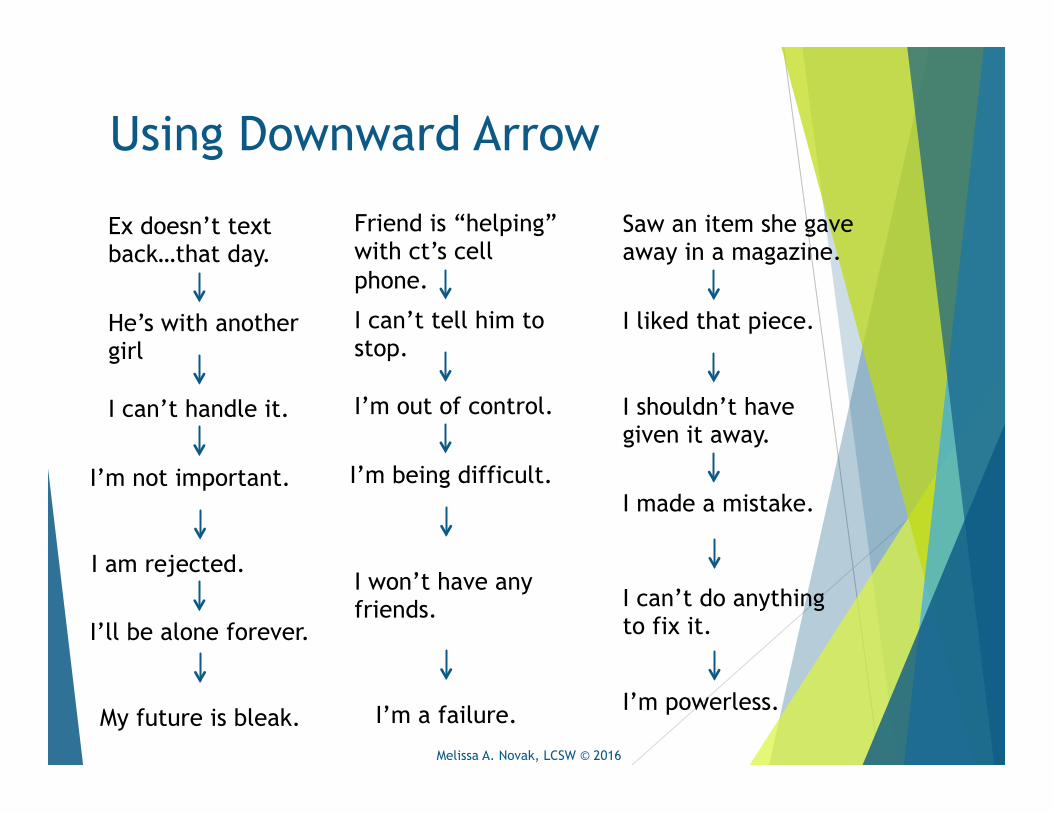
Using Downward Arrow
Ex doesn’t text back…that day.
He’s with another girl
I can’t handle it.
I’m not important.
I am rejected.
I’ll be alone forever.
My future is bleak.
Friend is “helping” with ct’s cell phone.
I can’t tell him to stop.
I’m out of control.
I’m being difficult.
I won’t have any friends.
I’m a failure.
Saw an item she gave away in a magazine.
I liked that piece.
I shouldn’t have given it away.
I can’t do anything to fix it.
I made a mistake.
I’m powerless.
Melissa A. Novak, LCSW © 2016
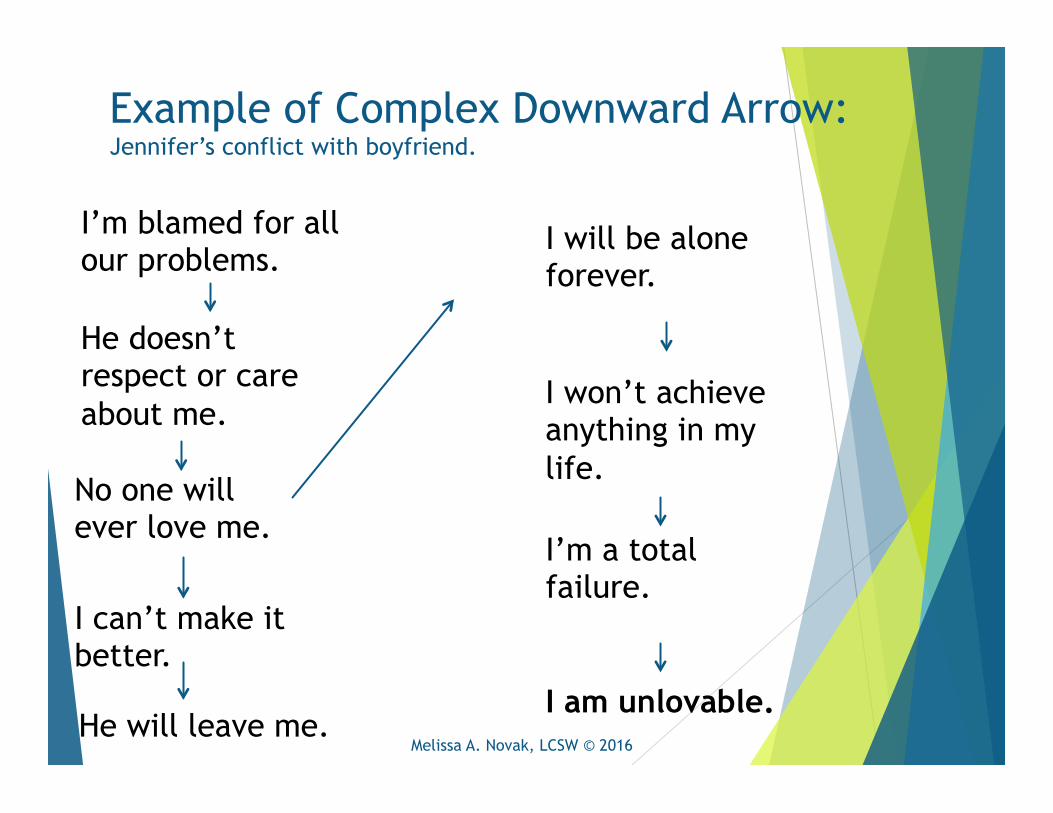
Example of Complex Downward Arrow: Jennifer’s conflict with boyfriend.
I’m a total failure.
I won’t achieve anything in my life.
I will be alone forever.
I’m blamed for all our problems.
He doesn’t respect or care about me.
He will leave me.
I can’t make it better.
No one will ever love me.
I am unlovable. Melissa A. Novak, LCSW © 2016
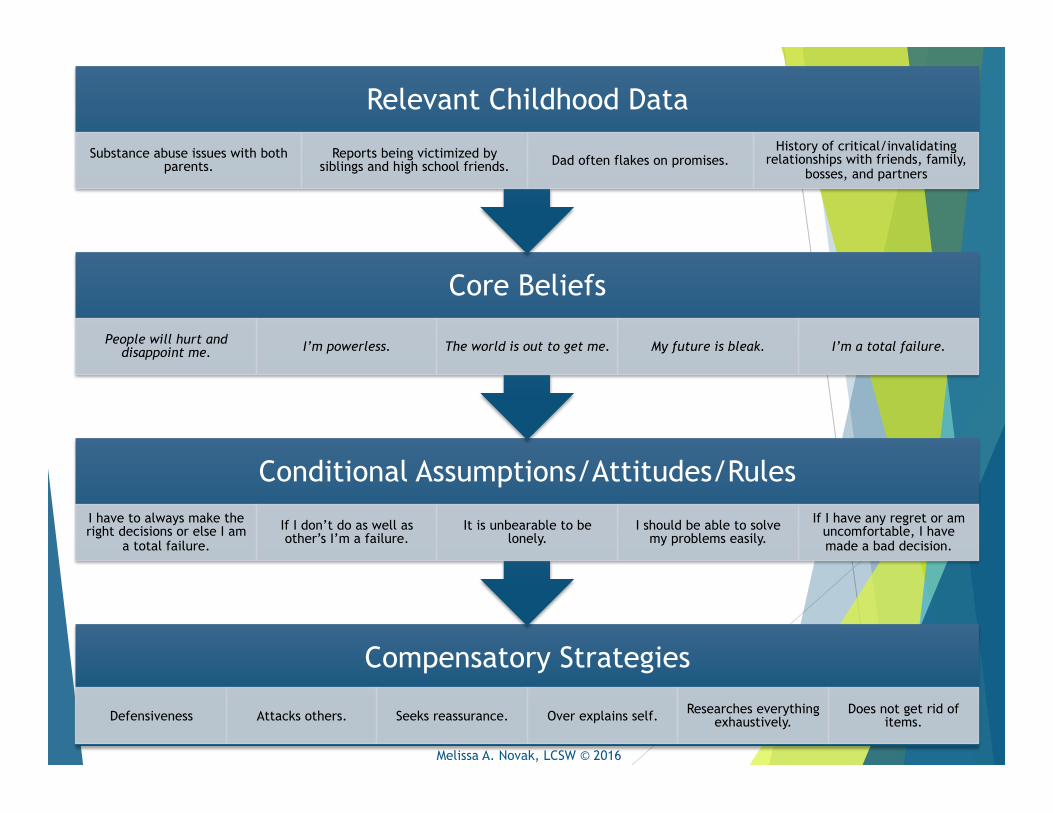
Compensatory Strategies
Defensiveness Attacks others. Seeks reassurance. Over explains self. Researches everything exhaustively.
Does not get rid of items.
Conditional Assumptions/Attitudes/Rules I have to always make the right decisions or else I am
a total failure.
If I don’t do as well as other’s I’m a failure.
It is unbearable to be lonely.
I should be able to solve my problems easily.
If I have any regret or am uncomfortable, I have made a bad decision.
Core Beliefs
People will hurt and disappoint me. I’m powerless. The world is out to get me. My future is bleak. I’m a total failure.
Relevant Childhood Data
Substance abuse issues with both parents.
Reports being victimized by siblings and high school friends. Dad often flakes on promises.
History of critical/invalidating relationships with friends, family,
bosses, and partners
Melissa A. Novak, LCSW © 2016
Cases & Goals
What are you taking with you? What are you going to try for every patient this week?
Cases…let’s do this!
Thoughts are not truths. They are not realities. They are not certainty. Yet, people often act as such. Thoughts are merely our perceptions habitually linked through charged language and experience.
Thoughts are the lenses to one’s experience. If they are covered in crap, then all you will see is crap.
Melissa A. Novak, LCSW © 2016
Questions?
u Academy of Cognitive Therapy: www.academyofct.org
u Beck, Judith. (1995). Cognitive Therapy: Basics and Beyond. New York: The Guiliford Press.
u Leahy, Robert L. (2003). Cognitive Therapy Techniques: A practitioner’s guide. New York: The Guliford Press
Resources and References:
Melissa A. Novak, LCSW © 2016