Embed Size (px)
Citation preview

The 2019 Yorkshire Turner-Warwick Lecture
Daniel Pan
NIHR Academic Clinical Fellow in Infectious Diseases and Medicine
Department of Respiratory Sciences, University of Leicester
Three important considerations for the general physician when
managing patients admitted to hospital with heart failure

Contents of talk
I have no conflicts of interest.
All views are my own.
Part 1: Three important considerations to take into account when
assessing the heart failure inpatient
Part 2: Prognostic value of the chest x-ray in the heart failure
inpatient

A case..

Isselbacher et al. Case 38 – 2018: A 54-Year-Old Man with New Heart Failure. New England
Journal of Medicine. 2018; 379:24 p2362-2372

Investigations
Haemoglobin: 14.6g/dL
WCC: 8.4 x103 per mm3
Platelets: 290 x103 per mm3
NT-pro BNP 8,352 pg/ml
Troponin: 71 ng/ml (non-dynamic)

Management
A diagnosis of heart failure, with volume overload is made.
Intravenous diuretics – Furosemide 40mg BD
Inpatient transthoracic echocardiogram
Heart failure nurse referral

Thomas et al. Calculation of left ventricular volumes and ejection fraction from biplane
Simpson’s formula using 2D echocardiography. J Nucl Med 2015;56:31S-38S

Over the course of the next week…
Oedema has improved.
Patient no longer symptomatic.
Passed mobility assessment by physiotherapy and occupational therapy
Furosemide switched to oral.
Prognostic medication – beta-blocker, ACE-inhibitor commenced and
uptitrated
Discharge – with heart failure follow-up in community



Before discharge…
‘Doctor, what is heart failure? Is it bad?’
-

Heart failure is increasing
British Heart Foundation

Heart failure is increasing
Conrad N et al. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million
individuals. Lancet 2018;391:572–580.

A large proportion of patients admitted to hospital with heart
failure are looked after by general medicine
National cardiac audit programme. National Heart Failure Audit 2016-2017 summary report

Patients with heart failure have a high readmission rate within 30
days of discharge, before they can get seen by a heart failure
nurse
National cardiac audit programme. National Heart Failure Audit 2016-2017 summary report

Prognosis of patients with heart failure, especially those admitted
to hospital continues to be poor
Taylor et al. Trends in survival after a diagnosis of heart failure in the
United Kingdom 2000-2017: population based cohort
study BMJ 2019; 364 :l223
Grothey et al. Duration of adjuvant chemotherapy for stage II colon
cancer. New England Journal of Medicine 2018; 378;13 p 1177-1188.

Prognosis of heart failure is worse than some cancers
Mamas et al. Do patients have worse outcomes in heart failure than in cancer? A primary care‐based cohort study with 10‐year
follow‐up in Scotland. Eur J Heart Fail 2017, 19: 1095-1104.

What are patient’s perceptions of heart failure?
Plotka et al. Patients’ knowledge of heart failure and perception of the
disease. Patient Preference and Adherence 2017:11 1459-1467

Patients understanding, in their own words, of the term ‘heart failure’ at the time of the
survey (months after diagnosis was made).
P Banerjee et al. Clin Med 2010;10:339-343
0
10
20
30
40
50
60
Blood clot to
coronary
Damaged heart
muscle
Breathlessness No
understanding
No answer
Percentage
Percentage

Response to the questions ‘Did you understand the meaning of the term “heart
failure” at the time of diagnosis?’ and ‘Who gave you the diagnosis?’.
P Banerjee et al. Clin Med 2010;10:339-343
0
5
10
15
20
25
30
35
40
Yes No Do not
know
No
answer
General
practitioner
Hospital nurse
Hospital doctor
Other
Do not know
Did not answer

Point 1: Consider spending time to educate
patients about heart failure and its prognosis

What is heart failure?
Ponikowski et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart
failure. European Heart Journal 2016;37:2128-2200

Cowie et al. Improving care of patients with acute heart failure: before, during and after
hospitalization. ESC Heart Failure 2014:; 110-145.
‘Acute’ heart failure has many different causes
De Novo Acute
decompensation

Cowie et al. Improving care of patients with acute heart failure: before, during and after
hospitalization. ESC Heart Failure 2014:1; 110-145.
‘Acute’ heart failure may just be the natural history of
chronic heart failure

Rheumatic heart disease
Acute coronary syndrome
Post PCI/CABG
Age!
Multimorbidity
1970 2019
‘Acute’ heart failure 50 years ago is different to
‘acute’ heart failure today

The definition of heart failure itself is changing
Pre-1980s
‘Non-pharmacologic
era’
- Fluid restriction
- Bedrest
- Diuretics
1980s: Pharmacologic era
- Digitalis
- Diuretics
- Vasodilators
- Inotropes
1990s: Age of ACE
- ACEi
- Beta blockers
- Spironolactone
2000s: Decade of devices
- CRT, ICDs and
LVAD
Professor Andrew L Clark:
Heart failure with preserved ejection
fraction?
Or heart failure with normal ejection
fraction?
Now: Age of ARNIs
Return of the Diuretics?
Transplantation

Point 2: Don’t think acute heart failure – think
patients admitted to hospital with heart failure

Cowie et al. Improving care of patients with acute heart failure: before, during and after
hospitalization. ESC Heart Failure 2014:; 110-145.
‘Acute’ heart failure is not a single entity
Congestion

Residual congestion as an inpatient is related to worse prognosis
Rubio-Gracia et al. Prevalence, predictors and clinical outcome of residual congestion in acute
decompensated heart failure. International Journal of Cardiology 2018; 258. 185-191.

Congestion and relation to prognosis
Hasselblad et al. Relation between dose of loop diuretics and outcomes in a heart failure
population: Results of the ESCAPE Trial. European Journal of Heart Failure 2007, 9:1064-1069.

Pellicori et al. Prevalence, pattern and clinical relevance of ultrasound indices of congestion in
outpatients with heart failure. European Journal of Heart failure 2019, 21; 904-916

Congestion and relation to prognosis
McMurray et al. Dapaglifozin in patients with heart failure and reduced ejection fraction. The New
England Journal of Medicine September 2019
Is it simply just a diuretic effect?

Point 3: Although loop diuretics have not been
proven to relate to mortality, congestion is.

Treatment strategies
Identify the cause of the heart failure
Is this a traffic jam problem?
DISCLAIMER: my own view
Is this a mileage problem?

Heart failure ++ congestion = decongest
Heart failure + congestion = uptitrate
medications
The traffic jam problem
The heart is not working well, but the patient
is severely, acutely congested.

Heart failure ++ congestion = decongest
Heart failure + congestion = uptitrate
medications
The mileage problem
The patient is congested because the heart is
not working well.


Mullens et al. The use of diuretics in heart failure with congestion – a position statement from the Heart Failure
Association of the European Society of Cardiology. European Journal of Heart Failure 2019; 21(2): 137-155

Chest x-ray in acute heart failure
Battler. The Initial Chest X-ray in Acute Myocardial Infarction Prediction of Early and Late Mortality and
Survival. Circulation 1980:1004–10

Chest x-ray in acute heart failure
Core investigation in breathless patients.
Not considered a ‘diagnostic test’ for HF.
Little relation between cardiothoracic ratio and left ventricular systolic
function. (1)
Not all patients with acute HF have pulmonary congestion. (2)
Only studies investigating prognosis are those 20-40 years ago, when
most patients with pulmonary congestion had acute myocardial
infarction. (3-7)
(1) Clark et al.. Unreliability of cardiothoracic ratio as a marker of left ventricular impairment: Comparison with radionuclide ventriculography and echocardiography. Postgrad Med J 2000;76:289–91
(2) Allen et al. Improving Time to Diagnosis How to Improve Time to Diagnosis in Acute Heart Failure – Clinical Signs and Chest X-ray Improving Time to Diagnosis. 2015;:69–74
(3) Petrie et al. It cannot be cardiac failure because the heart is not enlarged on the chest x-ray. Eur J Heart Fail 2003;5:117–9
(4) Roguin et al.. Long-term prognosis of acute pulmonary oedema--an ominous outcome. Eur J Hear Fail J Work Gr Hear Fail Eur Soc Cardiol 2000;2:137–44
(5) Battler et al. The Initial Chest X-ray in Acute Myocardial Infarction Prediction of Early and Late Mortality and Survival. Circulation 1980:1004–10
(6) Brezins et al. Left ventricular function in patients with acute myocardial infarction, acute pulmonary edema, and mechanical ventilation: Relationship to prognosis. Crit Care Med 1993;21:380–5
(7) Lin et al.. Reappraisal of continuous positive airway pressure therapy in acute cardiogenic pulmonary edema: Short-term results and long-term follow-up. Chest 1995;107:1379–86

Study aim
To investigate the prevalence and
prognostic significance of signs of heart
failure on the chest radiograph, in patients
admitted to hospital with acute heart failure

OPERA-HF
Observational study to PrEdict ReAdmission for Heart Failure patients
Prospective observational study (October 2012-November 2016)
Inclusion criteria:
- Age >18 years of age
- Usual residence in the region
- Hospitalisation with heart failure
- Treatment with loop diuretics
And one of the follow:
-Left ventricular ejection fraction ≤40%
-Left atrial dimension≥4.0cm
-N-terminal pro-B-type natriuretic peptide (NT-proBNP)>400 pg/mL (if in sinus rhythm) or
>1200 pg/mL (if in atrial fibrillation – AF) ISRCTN96643197

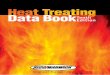
Kerley B lines
• Short horizontal lines
situated perpendicularly to
the pleural surface and
between the lung lobes in
the interstitium
Alveolar oedema
• Fluffy shadowing in the
lung fields. Severe is
defined as present
throughout all lung fields.
Pleural effusion
• Costophrenic and
cardiophrenic angle
blunting
Cardiothoracic ratio = A+B/2C
Chest x-ray projection
• Posterior-anterior
• Anterior-posterior
C B
A
Pulmonary venous congestion
• Increase in proportion of
vessels in the upper lung zones
compared to lower lung zones
Danzer CS. The cardio-thoracic ratio: An index of cardiac enlargement. Am J Med Sci 1919; 157:513-52
Illustration: Pan et al. 2019 Unpublished.

Enrolled in OPERA-HF: 1145 patients
No CXR during admission: 70 patients
Remaining: 1075 patients
CXR grossly rotated: 59 patients
No erect CXR: 41 patients
Remaining: 975 patients
Pan et al 2019. Unpublished
Clinical variables
Age
Gender
Hospitalised for HF
in previous year
Prior MI
Prior CABG
Malignancy
Diabetes
COPD
ACS on admission
SBP/DBP
Degree of
breathlessness
Investigation variables
Presence/absence of LVSD
AF
QRS duration
Heart rate
Cardiothoracic ratio
Film projection (AP/PA)
Alveolar oedema
Kerley B lines
Pleural effusion
Pulmonary venous congestion
Laboratory variables
Sodium
Potassium
Urea
Troponin T
NT-proBNP
Hb
Chloride
Albumin
Outcomes
In-hospital mortality
30 day mortality
Readmission to
hospital within 30
days of discharge
All-cause mortality
at end of followup

x975
Research is not a piece of cake…

Most patients with AHF did not present with ACS
Median age: 77 (68-83)
Median NT-proBNP: 5047 pg/ml (2337-10945) (26% did not have one taken
on admission)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Male Hospitalised for
heart failure in the
previous year
Presented with
acute coronary
syndrome
Breathlessness at
rest
Atrial fibrillation Reduced left
ventricular
ejection fraction
Study demographics
Yes NoPan et al 2019. Unpublished

The traffic jam

Mileage

Don’t think acute heart failure – think patients
admitted to hospital with heart failure

Pulmonary congestion is common in AHF
Median cardiothoracic ratio: PA films: 0.57 (0.55-0.64);
AP films: 0.60 (0.55-0.64)
Cardiomegaly present in 67%; unmeasurable in 6%.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Film projection (A -
AP, B - PA)
Alveolar oedema (A -
present, B - absent)
Kerley B lines (A -
present, B - absent)
Pleural effusions (A-
present, B - absent)
Pulmonary venous
congestion - (A -
present, B - absent)
Chest x-ray findings (N=975)
A B

33%
No congestive features 5%
Pulmonary venous
congestion
Kerley B lines
Pleural effusions 4%
4%
2%
3%
1%
1%
3%
2%
3%
9%
7%
8%
5% 10%
Alveolar oedema
Features of pulmonary congestion occur together
Sensitivity = probability
of a positive test given the
patient has a disease
= 95%

Pulmonary congestion gets worse in AP films,
with larger cardiothoracic ratios

Follow-up results
Median followup – 671 days (1.8 years)
440 (45% patients died)
41 during index admission
19% of patients were readmitted with worsening HF within
30 days of discharge from index admission.
Chest x-ray findings had no relation to short term outcomes

Consider spending time to educate patients
about heart failure and its prognosis





Although loop diuretics have not been proven to
relate to mortality, congestion is.

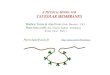
Creation of a chest x-ray prognostic score
Assessment of whether the score is related to prognosis when considered in a multivariable analysis
Assessment of whether the score is additionally useful in assessment of prognosis in addition to other variables
Statistical analysis strategy

Outcome: all-cause
mortality
Hazard ratio
(95% CI)
Wald X2 P value Hazard ratio (95%
CI)
β-coefficient Score
Alveolar oedema
Absent Referent Referent Referent Referent Referent 0
Present 1.20 (0.98-1.47) 1.71 0.09 1.04 (0.84-1.31) 0.05 1
Severe 1.67 (1.22-2.28) 3.20 0.001 1.35 (0.97-1.88) 0.30 3
Kerley B lines
Absent Referent Referent Referent Referent Referent 0
Present 1.28 (1.04-1.59) 2.30 0.02 1.21 (0.98-1.51) 0.19 2
Cardiothoracic ratio
≤0.55 Referent Referent Referent Referent Referent 0
0.55-0.70 1.21 (0.96-1.52) 1.62 0.10 1.12 (0.89-1.41) 0.12 1
>0.70/unmeasurable 1.84 (1.35-2.50) 3.84 <0.001 1.60 (1.16-2.19) 0.46 5
Chest x-ray projection
Posterior-anterior Referent Referent Referent Referent Referent 0
Anterior-posterior 1.13 (1.07-1.20) 4.28 <0.001 1.47 (1.17-1.86) 0.38 4
Pleural effusions
Absent Referent Referent Referent Referent Referent 0
Present 1.29 (1.05-1.59) 2.47 0.01 1.12 (0.89-1.40) 0.11 1
Pulmonary venous congestion
Absent Referent Referent Referent N/A N/A N/A
Present 1.06 (0.85-1.33) 0.53 0.60 N/A N/A N/A
Chest x-ray score
Chest x-ray score 1.10 (1.07-1.13) 6.15 <0.001 N/A N/A N/A
Austin PC et al. Developing points-based risk-scoring systems in the presence of competing risks. Stat Med 2016;35:4056–72
Pan et al. 2019 Unpublished
Creating the chest x-ray score


Relation of chest x-ray score to patient demographics
Older age
Female
Prior CABG
Worsening
breathlessness Increasing potassium
Increasing urea
Increasing creatinine
Increasing NT-proBNP
Decreasing albumin
Decreasing haemoglobin
Increasing chest x-ray score
(univariable analysis)
Decreasing diastolic BP

Relation to death (Univariable Cox analysis)
Older age
Lower diastolic BP
Prior CABG
Increasing potassium Increasing urea
Increasing creatinine
Increasing NT-proBNP
Decreasing albumin
Decreasing
haemoglobin
Female
Worsening
breathlessness

Chest x-ray score is related to death on multivariable
Cox regression
0.5 1 1.5
Age (per year increase)
Systolic blood pressure – mmHg (per 10 unit increase
Heart rate – beats/minute (per 10 unit increase)
Sodium – mmol/L– beats/minute (per 10 unit increase)
Urea – mmol/L– beats/minute (per 10 unit increase)
Chloride – mmol/L– beats/minute (per 10 unit increase)
Albumin– mmol/L– beats/minute (per 10 unit increase)
Chest x-ray score – mmol/L (per 10 unit increase
Hazard ratio
Base model

….but it does not offer any additional prognostic
value compared to other routinely collected variables

Return of the chest x-ray - main findings
Radiological evidence of congestion is very common in patients
presenting to hospital with heart failure.
Patients presenting with breathlessness as their dominant
symptom, have a higher chest x-ray score
Increasing pulmonary congestion on the chest x-ray score is
related to worsening heart failure as assessed by other clinical
measures and all-cause mortality.

Applications
Everyone gets a chest x-ray. This could used a systematic way of
grading chest x-rays in clinical trails
Evaluation of different phenotypes of pulmonary congestion and
association with prognosis
Anterior-posterior films. Why are they related to a worse
prognosis?

Limitations
Single – centre study
Most patients – Caucasian ethnicity
Previous congestion scores exist, but are more research
orientated, clunky to use.
Needs validation
No radiologists..

Considerations for the general physician
Educating patients about heart failure prognosis
is every general physician’s responsibility
Don’t think acute heart failure – think patients
admitted to hospital with heart failure
Although loop diuretics have not been shown to
relate to prognosis, congestion is.

Back to our patient
Regional wall motion abnormalities on the echo.
Normal other results – diagnosis of HF-rEF was
made, secondary to ischaemic heart disease.
Patient was also commenced on antiplatelet
therapy.
The diagnosis and prognosis of heart failure was
explained. Strict uptitration of heart failure
medications emphasized.

“The way to lead a long life is to get a chronic disease and take
care of it.”
Sir William Osler

Thank you! Contact: [email protected]
Academic Cardiology team at Castle Hill
Hospital
Supervision
Professor Andrew Clark – taught me how to
really calculate the cardiothoracic ratio
Dr Pierpaolo Pellicori
Data collection
Dr Alessia Urbinati
Dr Ioanna Sokoreli
Dr Shirley Sze
Dr Oliver Brown
Statistics advice
Professor Alan Rigby
Research database management
Syed Kazmi
General advice:
Dr Jarno Riistama
Professor John Cleland
Heart failure nurses
Karen Dobbs
Jeanne Bulemfu