Embed Size (px)
Citation preview

TFP: CLINICAL ASSESSMENT
borderlinedisorders.com
Session 2: John F. Clarkin, Ph.D.

TAXONOMY OF PERSONALITY DISORDERS: CONTRASTING THE DSM AND OBJECT RELATIONS APPROACHES

1970s: Gunderson and Kernberg• Gunderson (Gunderson & Kolb, 1978): Collected clinical
descriptors manifested in the observable behavior of borderline patients; these would form the criteria for DSM-III (1980)
• Kernberg (1975): focused on the disturbed behaviors and the internal representations of self and others, suggesting these mental representations were identifiable, organized, and driving behavior
• In 1980, we began the investigation of TFP targeted to both the observable behaviors and the internal organization

Results of the Phenomenological Approach
• Search for the organization behind the 8-9 trait-like criteria in DSM
• Heterogeneity among those who met the criteria for the disorder
• Confused and unclear phenotype disrupts the search for underlying neurobiological factors

Ideas Behind the Development of DSM-5
• Notable difficulties with DSM-IV: heterogeneity within the PD diagnosis; rampant PD comorbidity; reliability but little validity
• Hyman(2011): • Too much emphasis on categories• Genes and neurobiology don’t result in clear categories• …schizophrenia and bipolar disorder might better be
conceptualized as interactions among continuous dimensions rather than well-bound categories
• Bring personality theory to bare on personality disorder diagnoses

Basic Emotional Systems (Pankseep, 2011)
PLAY/joy
PANIC/
separation
CARE/
nurturance
LUST/sexuality
FEAR/
anxiety
RAGE/anger
SEEKING/
expectancy system

Emotional Operating Systems Filtered Through Lens of Object Relations
Confllicted, intense
Interactions with others
Distorted cognitive appraisal
Negative affect
Deficient efforfful control

Personality Disorder: DSM-5, Section 3
• Moderate or greater impairment in personality (self/interpersonal) functioning
• One or more pathological personality traits• Negative affectivity vs emotional stability• Detachment vs. extraversion• Antagonism vs. agreeableness• Disinhibition vs. conscientiousness• Psychoticism vs. lucidity
• Impairments are relatively stable across time

Level of Self and Interpersonal Functioning: DSM-5, Section 3• Self-functioning
• Identity• Self-direction
• Interpersonal functioning• Empathy• Intimacy

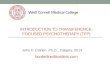
Levels (Least to Most Severe) of Personality Organization - Kernberg
Coping Rigidity
Identity Defenses Object Relations
Aggress-ion
Moral Values
Normal Flexibility Normal Normal Normal Modulat-ed
Present
Mild (Neurotic)
Rigidity Normal High Level Defenses
Conflicts Present
Severe (High Level BPO)
Inconsis-tent
Identity Diffusion
Primitive Defenses
Poor Varying degrees of aggress-ion
Variable
Most Severe (Low Level BPO)
Inconsis-tent
Identity Diffusion
Primitive Defenses
Poor Aggress-ion toward others
Lacking

FIGURE 1
Relationship between familiar, prototypic, personality types and structural diagnosis.
Severity ranges from mildest, at the top of the page, to extremely severe at the bottom. Arrows indicate range of severity.
Kernberg & Caligor (2005). A psychoanalytic theory of personality disorders. In: Major Theories of Personality Disorders, 2nd Ed. Eds: Clarkin & Lenzenweger. NY, Guilford, 115-156.

PERSONALITY DISORDERS: A TAXONOMY BASED ON THE OBJECT RELATIONS UNDERSTANDING OF PERSONALITY

Descriptive Features of Personality Disorder
Personality Disorders in general are distortions of normal personality characterized by:
• Rigidity or loss of flexibility of behavior patterns, resulting in poor adaptation
• Inhibition of normal behaviors• Exaggeration of certain behaviors• Chaotic alternation between inhibitory and impulsive
behavior patterns• Vicious circles develop: abnormal behaviors elicit
abnormal responses

Consequences of Personality Disorders:
- A reduction in the capacity to adapt to the psychosocial environment and to satisfy internal psychological needs (e.g., self-affirmation, sexuality, and dependency).
- In turn, personality disorders tend to be re-enforced by the pathological responses that patients elicit in their environment.

Axis II from a Personality Organization Point of View – Levels of OrganizationA mixed Categorical and Dimensional System
1-Normal flexibility and adaptation
2-Neurotic level of personality organization
3-Borderline level of personality organization:• High level borderline• Low level borderline
4-Psychotic level of personality organization

Borderline Personality OrganizationThe Defining Characteristics
• Identity Diffusion vs. integrated view of self and others (internal sense of continuity)• No integrated concept of self• No integrated concept of significant others
• Primitive Defenses• Splitting• Idealization/devaluation• Projective identification• Omnipotent control• Denial
• Variable Reality Testing

FIGURE 1
Relationship between familiar, prototypic, personality types and structural diagnosis.
Severity ranges from mildest, at the top of the page, to extremely severe at the bottom. Arrows indicate range of severity.
Kernberg & Caligor (2005). A psychoanalytic theory of personality disorders. In: Major Theories of Personality Disorders, 2nd Ed. Eds: Clarkin & Lenzenweger. NY, Guilford, 115-156.

Borderline Personality Organization: Clinical Implications
• Nonspecific ego weakness• Lack of impulse control, anxiety tolerance
• Disturbed object relations• Difficulties with work and love• Sexual pathology (Two levels: inhibition of all sexual
functioning; chaotic sexuality)• Pathology of moral functioning

LAYING THE FOUNDATION FOR TREATMENT: CLINICAL EVALUATION

BEGINNING TREATMENT
AssessmentSessions
Discussion of Dx and Contracting Sessions
FamilySession Therapy
Pre-Therapy
TherapyBegins(or not)N.B.:
Often a Sense of Urgency
Goal: To move from Acting Out to Transference

• Patients with personality pathology suffer from an internal structure that results in difficulties in work, friendships, and intimate relations
• Treatment structure is essential in the treatment of personality pathology, especially in mid to severe ranges of personality pathology
CLINICAL ASSESSMENT

• The human individual is organized at multiple levels
• Personality is an organization which enables the individual to function
• Personality organization enables the individual to function in the interpersonal sphere
• Treatment choice is guided by personality organization, not simply by symptoms or conflicts (see Kernberg & Caligor, 2004)
Guiding Ideas

•Definition of terms so they are used by all in the same way
•Assessment that is reliable; done the same by everyone
•Assessment leading to the application of TFP to patients for whom it is intended
Advantages to Your Group for a Standard Assessment

• Neurotic organization• High level borderline organization• Low level borderline organization
Review of Personality Disorders from a Personality Organization Point of View

Personality Organization
Figure 1Relationship between familiar, prototypic, personality types and structural diagnosis. Severity ranges from mildest, at the top of the page, to extremely severe at the bottom. Arrows indicate range of severity. *We include avoidant personality disorder in deference to the DSM. However, in our clinical experience, patients who have been diagnosed with avoidant personality disorder ultimately prove to have another personality disorder that accounts for avoidant pathology. As a result, we question the existence of avoidant personality as a clinical entity. This is a controversial question deserving further study.

Structural Interview (Kernberg, 1984)
• Focus on the patient’s thinking and functioning in the present time
• Begins with standard questions:• What brings you here?• What are your current difficulties?• What do you expect from treatment?• In general, where are you now?
• Key questions assessing representations of self and others:• Describe yourself as a unique individual• Describe a significant other in detail
• Interviewer’s stance: therapeutic neutrality• Sequential use of clarification, confrontation, beginning
interpretations

• Combination of traditional psychiatric interview, with assessment of personality organization
• Standard sequence to the interview• Yield from the interview:
• Psychiatric diagnoses• Personality organization
The Structural Interview

• Patient: 43 year old male• Chief complaint: Nothing to live for; girl friend taken away• Focus of assessment: level of personality pathology;
treatment options
Symphora Tape: Structural Interview

Mild (Neurotic) Personality Pathology
Identity; advanced defenses; low aggression, moral values
Severe (High Level BPO) Personality Pathology
Identity diffusion; primitive defenses
Most Severe (Low Level BPO) Personality Pathology
Aggression; relative absence of moral values
Levels of Pathology and Major Dimensions (Identity, etc)

Mild (Neurotic) Personality Pathology
Transference InterpretationsTherapeutic Neutrality
Severe (High Level BPO) Personality Pathology
Contract SettingTransference InterpretationsIn and out of Therapeutic Neutrality
Most Severe (Low Level BPO) Personality Pathology
Questionable use of treatment
Levels of Pathology and Treatment

• Combination of traditional psychiatric interview, with assessment of personality organization
• Standard sequence to the interview• Yield from the interview:
• Psychiatric diagnoses• Personality organization
• Example: Symphora tapes
The Structural Interview


• Theory driven• Relationship of personality organization to treatment selection
• Coverage of major constructs dictated by the theory
• Semi-structured interview format to ensure reliability
Semi-Structured Interview: STIPO

• Identity• Object relations• Primitive defenses• Coping/rigidity• Aggression• Moral values• Reality testing and perceptual distortions
Constructs in the STIPO

Investment in work How important is work to you? Would you say you are
ambitious with respect to work and career? Investment in free time
On weekends, or in your free time, what interests do you pursue?
Sense of self Tell me about yourself…describe yourself so that I get
a live and full picture of you Representation of others
Tell me about (most important person)…
Identity

1. Consolidated identity2. Some areas of deficit, e.g., mild superficiality or
instability in sense of self3. Mild to moderate instability or discontinuity in sense of
self and others4. Marked instability and superficiality in sense of self and
others5. Severe: contradictory, chaotic views of self and others
Overall Rating of Identity

Interpersonal relations Do you have close friends? Tell me about your
friendship…what do you share with one another? Intimate relations and sexuality
Have you been involved in any romantic relationships in the past 5 years?
Do you find it difficult to experience tender feelings while still enjoying sex?
Internal working model of relationships What is it like for you when people close to you are in
need of comfort, or are in emotional distress?
Object Relations

1. Durable, realistic, nuanced, satisfying object relations2. Some degree of impairment in intimate relations3. Attachments present but superficial, flawed, need
fulfillment, limited empathy4. Attachments few and flawed5. Paucity of attachments, no capacity for empathy nor
sustained interest in others
Overall Rating of Object Relations

Paranoia Would you consider yourself someone who is
cautious about what other people know about you? Erratic behavior Idealization/devaluation
Do your feelings for people run “hot and cold”, change quickly?
Black and white thinking Primitive denial Externalization Projective identification
Primitive Defenses

1. No evidence of primitive defenses
2. Some use of primitive defenses
3. Shifts in perception of self and others and related limited impairment in functioning
4. Shifts in perception of self and others severe and pervasive
5. Pervasive use of primitive defenses; radical shifts of perception of self and others
Overall Rating of Primitive Defenses

Anticipation When you are anticipating stressful events, do
you spend time planning ahead?SuppressionFlexibilitySelf-blameProactive copingPerfectionismShifting setsControlWorryingChallenges
Coping/Rigidity

1. Flexible, adaptive coping
2. Adaptive coping, but less consistency and efficacy
3. Inconsistent capacity for coping; vulnerable to stress and rigid coping
4. Rigid, maladaptive coping
5. Pervasive maladaptive and inflexible coping
Overall Rating of Coping/Rigidity

• Self-directed aggression
• Do you sometimes neglect your physical health?
• Do you at times do things that seem unwise and potentially dangerous, e.g. unprotected sex, heavy drinking or drug use?
• Other-directed aggression
• Do you lose your temper with others?• Have you at any time ever intentionally
seriously harmed someone physically?
Aggression

1. Control, modulation, integration of anger and aggression
2. Aggression through self-neglect, controlling interpersonal style
3. Self-directed , occasional tantrums, hostile verbal aggression
4. Aggression against others
5. Serious danger to safety of others and/or self
Overall Rating of Aggression

• Behavior
• Are there times when you deliberately deceive others?
• Have you ever done anything that is illegal?• Guilt
• Can you think of an example when you failed to live up to your personal code? How did you feel? Would you say that you felt guilty?
Moral Values

1. Appropriate concern for unethical behavior; internal moral compass
2. No antisocial behavior; some conflict around personal gain and ethical behavior
3. Some unethical/immoral behavior
4. Violent, aggressive antisocial behavior
5. Violent, aggressive antisocial behavior; no notion of moral values and guilt
Overall Rating of Moral Values

Prototypic Neurotic, High and Low Level BPO Patients

• Provides reliable assessment of level of personality organization
• Defines in concrete terms and questions psychoanalytic concepts such as identity
• Provides a method of empirically subgrouping patients (e.g., borderline, low level borderline)
• First step to measurement of change in personality organization
Uses of the STIPO

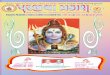
• Assessment of extraversion/intraversion, moral values, level and management of aggression, quality of object relations
Subtypes of BPD: Assessment Implications

0246810121416
NPO
BPO-High
BPO-Low
STIPO Profiles on SNAP Based Categories

Antisocial Paranoia Aggression
Group I Low Low Low
Group II Moderate High Low
Group III High Moderate High
Finite Mixture Modeling: Groups of BPD Patients

• Group I: high Constraint, high Social Closeness, low Physical Abuse, low Depression and Somatization
• Group II: low Social Closeness, high Sexual Abuse
• Group III: high Negative Affect, low Constraint, high Depression and Somatization, high Identity Diffusion
Associated Features of the Three Groups