Embed Size (px)
Citation preview

Terence Ng MA, Charlene Harrington, PhD
Department of Social & Behavioral SciencesUniversity of California, San Francisco
3333 California Street, Suite 455San Francisco, CA 94118
415-502-6330 [email protected]
www.pascenter.orgFunded by: Kaiser Commission on Medicaid & the Uninsured, and National Institute on Disability & Rehabilitation Research (NIDRR)
PAS Center Webinar
MEDICARE AND MEDICAID IN LONG TERM CARE.

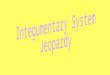
Total US Long-Term Care Expenditures, 2007$190.4 billion
Out-of-Pocket22%
Private Ins/ Other 11%
Medicare 25%
Medicaid/Other Public
42%

MEDICARE provides-Short-term post-acute care (after hospitalization) to aged and
disabled in nursing homes and by home health agencies -Hospice care at the end of life, in nursing homes, at home, or
in residential settings-Acute care, medical care, and other services to individuals
with chronic care and/or long-term care needs (not analyzed here)
Eligibility for nursing home and home health services -need for skilled care or therapy services for short periods (90
days or less)
After Medicare benefits are exhausted, these services paid for by out-of-pocket, by private insurance, or by the Medicaid program for those with low incomes and assets.
Introduction to Medicare Long Term Care

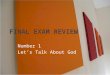
Medicare Home Health and Nursing Home Users, 1999 – 2007
0
1
2
3
4
5
6
1999 2004 2007
4 million4 million
38%
Nursing Homes
38%
Nursing Homes
63%63%
37%37%
62%
Home Health
62%
Home Health
34%34%
66%66%
4.9 million4.9 million

Medicare Home Health and Nursing Home Expenditures, 1999 – 2007
0
0
0
0
0
0
0
0
0
1999 2004 2007
$21.6 billion
$21.6 billion
60%
Nursing Homes
60%
Nursing Homes
41%41%
59%59%
40%
Home Health
40%
Home Health
54%54%
46%46%
$37.8 billion
$37.8 billion

Medicare pays for a growing proportion of total public nursing home expenditures
Medicare nursing home expenditures increased from 23 percent in 1999 to 32 percent of total nursing home expenditures in 2007
Medicare proportion of expenditures for home health remained about 80 percent over the same period
Medicare Long Term Care Trends

Medicaid - joint federal and state program managed by states-primary payer for long term care services for individuals with low
incomes and assets
Eligibility -Automatic for the Categorically Needy (those receiving
Supplemental Security Income [SSI] federal cash benefits), although 11 states have more restrictive standards.
-35 states plus the District of Columbia have medically needy programs, covering those who spend down by incurring medical expenses and meet the state’s income and asset requirements.
-Nursing home care and home health are mandatory benefits, while other long term care services such as those provided at home and in the community (HCBS) are optional.
Introduction to Medicaid Long Term Care

Medicaid Long Term Care Trends
Long term care represented about one-third of total Medicaid spending in 2007 and this has not changed over the study period.
Nursing home use has not kept pace with the growth in the aged population over the period (about 17 percent for age 65 and over and 30 percent for age 75 and over between 2000 and 2007 – while no change in nursing home use).
40% of institutional users consumed 61% of total Medicaid LTC expenditures in 2006

Medicaid HCBS Programs
Personal Care optional benefit
Optional, active in only 31 states (2007)
Must be statewide, available to Medicaid categorically eligible groups
HCBS 1915(c) waivers
Optional, provides range of HCBS e.g. personal care
Must be nursing home eligible, selective recipient groups
Slots, geography & expenditures can be limited
Financial & medical eligibility vary across states
Waiting lists can be established
Home Health
Mandatory in all states for those eligible for Medicaid institutional care

Medicaid HCBS Participants by Program, 1999 – 2006
1.9m
2.4m2.7m
2.9m

Medicaid HCBS Expenditures by Program, 1999 – 2006
$17b
$25b
$32b
$38b

Growth in Medicaid Home & Community Based Services
Many Reasons for HCBS Growth•Growing demand by individuals to remain in their homes rather
than in institutions.•US Supreme Court ruled in the Olmstead case in 1999 that
individuals have the right to live at home or in the community if they are able to and choose to do so, rather than to be placed in institutional settings by the government.
•Based on this ruling, states have expanded HCBS after lawsuits and establishment of Olmstead plans.
•Federal government has provided a number of initiatives and resources to assist states in complying with the Olmstead decision to increase access to HCBS, such as Money Follows the Person.

1915(c) Waiver Participants and Expenditures, By Target Group, 2006

Medicaid HCBS, Participant per 1,000 Pop.2006. US – 9.59

Medicaid HCBS, Expenditures per Capita2006. US - $127.80

Medicaid HCBS Policies and Cost Controls
Medicaid Home Health & State Plan Personal Care• Costs caps• Service caps• All eligibles must be served – no wait lists
Medicaid HCBS Waivers•Financial and Functional eligibility can vary•Cost caps•Service caps•Slots – limits on people served•Wait lists

Waiver Slots and Waiting Lists by Target Group, 2008
Total Slots: 1,362,624 Waiting List: Total 393,096

Medicaid HCBS Participation as a Percentage of Total LTC, 2006. US – 61%

Medicaid HCBS Expenditures as a Percentage of Total LTC, 2006. US – 39%

Complexity and Fragmentation of HCBS Programs
Many federal initiatives to expand HCBS such as
Real Choice Systems Change grants
Medicaid Section 1115 research and demonstration projects
Managed Care/Freedom of Choice Waivers (1915(b) waivers)
Money Follows the Person grants
Program of All-Inclusive Care for the Elderly (PACE)
Cash and Counseling
Deficit Reduction Act (DRA) of 2005 gave states increased flexibility in delivering LTC services in community-based settings.
But they, together with existing programs are fragmented among state departments such as social services or aged.
Many also have differing admin. & eligibility determination structure
= Costly and confusing to consumers

Coordination of Medicare and Medicaid Funding
Medicare and Medicaid are generally not coordinated or integrated when it comes to long term care.
Hospitals, with an incentive to discharge patients as soon as possible to reduce costs, often discharge before appropriate post-acute or LTC services can be arranged and may encourage expensive nursing home placement if HCBS not available at home.
High rates of expensive re-hospitalization is a serious problem for Medicare.
Greater effort needed to design effective discharge planning and post hospitalization follow-up programs.

General Discussion
Growth in Medicare short-term post-acute service use reflects short hospital stays and a growing demand for rehabilitation services. Many post-acute providers prefer the higher rates from Medicare than for Medicaid LTC services.
Medicaid has made progress since Olmstead in 1999 in expanding HCBS programs to a growing number of target groups and participants. These trends reflect a combination of changes in consumer preferences, state and federal policies to reduce institutional use, state limitations on Medicaid reimbursement rates, provider preferences for Medicare short-stay patients, and the growth in HCBS options and providers.
Wide inter-state variations in usage and expenditures and large waiting lists suggest inequities across states and limited access in many states. Variations among different target groups also suggest inequities in access within and across states.

General Discussion (2)
But amid growth, proportion of HCBS spending continues to be well below institutional spending. There are wide inter-state variations in efforts to ‘rebalance’ spending from institutional to HCBS, which may reflect differences in state resources, state policies, and commitments to rebalancing.
Policymakers concerned that waiver participants may not have been willing to use institutional services in the 1st place, with a “woodwork effect” of higher overall state costs. But recent study found that states that had well-established HCBS had less overall LTC spending growth compared to those with low HCBS spending because these states were able to reduce institutional spending over time.

General Discussion (3)
Studies have found new HCBS programs were associated with greater client and caregiver satisfaction.
The current budget crises at the national and state levels threaten the continued access to and spending on optional HCBS even as Medicaid enrollment increases and the population ages.
Policy changes are needed to align the incentives for the two programs. These findings suggest the need for structural reform of the LTC system.
Participant Thoughts?
The End




















![Untitled-1 [uralbeznarkotikov.ru]uralbeznarkotikov.ru/cat/paper/1-2016.pdf · 800 3333 118 8800 3333 118 "talbeznarkotihov.ru 8800 3333 8800 3333 118 8800 3333 118 B 800 3333 118](https://img.pdfslide.us/doc/110x75/5fa8ba52bd5e685c68532c8a/untitled-1-800-3333-118-8800-3333-118-talbeznarkotihovru-8800-3333-8800.jpg)





