Embed Size (px)
Citation preview

Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/44640993
Ten-yeartrendsinhospitaladmissionsfor
adversedrugreactionsinEngland1999-2009
ArticleinJournaloftheRoyalSocietyofMedicine·June2010
DOI:10.1258/jrsm.2010.100113·Source:PubMed
CITATIONS
66
READS
65
7authors,including:
Tai-YinWu
20PUBLICATIONS199CITATIONS
SEEPROFILE
Min-HuaJen
ImperialCollegeLondon
26PUBLICATIONS447CITATIONS
SEEPROFILE
MariamMolokhia
King'sCollegeLondon
111PUBLICATIONS2,335CITATIONS
SEEPROFILE
DerekBell
ImperialCollegeLondon
167PUBLICATIONS1,952CITATIONS
SEEPROFILE
Allin-textreferencesunderlinedinbluearelinkedtopublicationsonResearchGate,
lettingyouaccessandreadthemimmediately.
Availablefrom:DerekBell
Retrievedon:18August2016

Ten-year trends in hospitaladmissions for adverse drugreactions in England 1999–2009
Tai-Yin Wu1,2,3 + Min-Hua Jen4 + Alex Bottle4 +Mariam Molokhia5 + Paul Aylin4 + Derek Bell6 + Azeem Majeed1
1 Department of Primary Care and Public Health, Imperial College London, Charing Cross Campus, London W6 8RP, UK2 Department of Family Medicine, Taipei City Hospital, Renai Branch, Taipei, Taiwan3 Institute of Preventive Medicine, National Taiwan University, Taipei, Taiwan4 Dr Foster Unit at Imperial College, Department of Primary Care and Public Health, Imperial College London, London
EC1A 9LA, UK5 Non-Communicable Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine, London WC1E 7HT, UK6 Department of Medicine, Imperial College London, Chelsea and Westminster Campus, London SW10 9NH, UK
Correspondence to: Tai-Yin Wu. E-mail: [email protected]
Summary
Objectives Adverse drug reactions (ADR) are an important cause ofmorbidity and mortality. We analysed trends in hospital admissionsassociated with ADRs in English hospitals between 1999 and 2008.
Design Data from the Hospital Episode Statistics database were examinedfor all English hospital admissions (1999–2008) with a primary or secondarydiagnosis of an ADR recorded.
Setting All NHS (public) hospitals in England.
Main outcome measures The number of admissions and in-hospitalmortality rate with a primary (codes including ‘adverse drug reaction’, ‘drug-induced’, ‘due to drug’, ‘due to medicament’ or ‘drug allergy’) or secondarydiagnosis of ADR (ICD-10 Y40-59) were obtained and analysed. Furtheranalysis for the year 2008–2009 was performed with regard to age, gender,proportion aged >65 yrs and total bed-days.
Results Between 1999 and 2008, there were 557,978 ADR-associatedadmissions, representing 0.9% of total hospital admissions. Over this periodthe annual number of ADRs increased by 76.8% (from 42,453 to 75,076), andin-hospital mortality rate increased by 10% (from 4.3% to 4.7%). In 2008,there were 6,830,067 emergency admissions of which 75,076 (1.1%) weredrug-related. Systemic agents were most commonly implicated (19.2%),followed by analgesics (13.3%) and cardiovascular drugs (12.9%).There hasbeen a near two-fold increase in nephropathy and cardiovascularconsequences secondary to drugs and a 6.8% fall in mental and behaviouraldisorders due to drugs.
Conclusions ADRs have a major impact on public health. Our data suggestthe number of ADR admissions has increased at a greater rate than the increasein total hospital admissions; some of this may be due to improved diagnostic
DECLARATIONS
Competing interests
None declared
Funding
The Dr Foster Unit is
funded by Dr Foster
Intelligence.
Imperial College
London is grateful
for support from the
NIHR Biomedical
Research Centre
scheme and the
NIHR Collaboration
for Leadership in
Applied Health
Research & Care
(CLAHRC) scheme.
MM is funded by an
NIHR postdoctoral
award and is an
investigator for the
EU-ADR FP7 and
Serious Adverse
Events Consortium
(SAEC) projects on
adverse drug
reactions
RESEARCH
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113 239

coding. However, in-hospital mortality due to ADR admissions also increasedduring the period. Our findings should prompt policymakers to implement furthermeasures to reduce ADR incidence and their associated in-hospital mortality, andmethods to improve the recording of ADRs.
Introduction
An adverse drug reaction (ADR) is an undesirableeffect of a drug beyond its anticipated therapeuticeffects occurring during clinical use,1 and is one ofthe major causes of iatrogenic disease.2 ADRscause significant morbidity and mortality and in-crease the length of hospital stays. The economicburden of ADRs on the British NHS is also high,accounting for considerable extra NHS costs.3
ADRs may be on target (where there is a clear doserelationship) and may be reversible on reducing orwithdrawing the drug,1,4 or off target (where there isuncertain dose response relationship). IdiosyncraticADRs which are largely unpredictable, can dependon the genetic susceptibility of the individual and areoften more serious (sometimes fatal). The benefit–harm relationships of ADRs are complex and shouldalways be taken into account when prescribing.
From the patients’ perspective, ADRs affectsquality of life, confidence in treatment, influenceadherence to medications, and increase costs ofcare.1 The manifestation of ADRs may also mimica disease process and, therefore, lead to furtherinvestigations and treatments.
Older people or those with multiple long-termdiseases are more susceptible to ADRs.5 As co-morbidity increases with increasing age, poly-pharmacy (use of more than four prescriptiondrugs6) is seen more frequently in older patients.7,8
Moreover, between 14 and 24% of older adultsreceive potentially inappropriate medications.9
For example, long-acting benzodiazepines have ahigh potential for severe adverse outcomes inolder patients, according to Beers criteria (a list ofinappropriate medications for the elderly).10 Poly-pharmacy increases the likelihood of drug-druginteraction and adverse drug reactions.11 ADRsthen in turn prompt the patient to seek furthermedical help and multiple primary and secondarycare visits may ensue.12
Despite the clinical impact of adverse drug re-actions, methods for monitoring them remainedlimited. Databases derived from electronic healthrecords such as the General Practice Research
Database (GPRD) or QResearch are also beingincreasingly used to monitor ADRs. Other ap-proaches include: clinical trials, prescription eventmonitoring, spontaneous reporting, and linked ad-ministrative databases. However, where an ADR israre, clinical trials lack power to detect associ-ations. Prescription event monitoring examinesrisk in newly-marketed drugs but has a relativelyshort follow-up and difficulty in selecting appro-priate controls. Spontaneous reporting is donethrough pharmacovigilance reporting such as theMHRA (Medicines and Healthcare Products Regu-latory Agency) Yellow Card Scheme in the UK,although under-reporting remains a significantissue.
Consequently, when a drug is first marketed,there is often limited information about its safetyin routine clinical use,13 although under the blacktriangle scheme new medicines are intensivelymonitored by the Commission on Human Medicines(CHM) and the MHRA. Drug safety assessmentshould be considered an integral part of everydayclinical practice,1 as well as necessity for phase IV(post-marketing surveillance) trials. Under suchpost-marketing surveillance, drugs continue to bewithdrawn from the market due to safety concerns;for example, the withdrawal of rofecoxib in 200414
due to concerns about cardiovascular safety (MI andstroke) and, more recently, efalizumab in 2009, a re-combinant humanized monoclonal antibody used totreat psoriasis, due to potential risk of progressivemultifocal leukoencephalopathy (PML).
We analysed hospital admissions associatedwith ADRs in all NHS (public) English hospitals inthe past 10 years, using the Hospital Episode Sta-tistics database. We examined the epidemiology ofhospital admissions for ADRs including temporaltrends, in-hospital mortality, the age and genderdistribution of these admissions, and differences inADR rates between individual hospitals.
Methods
Hospital Episode Statistics (HES) is an administra-tive database produced by the Department of
Ethical Approval
We have approval
from St Mary’s
Hospital Local
Research Ethics
Committee to use
routinely collected
hospital
administrative data
for research. Also,
we have been
granted permission
by the Patient
Information Advisory
Group under Section
251 of the NHS Act
2006 (originally
enacted under
Section 60 of the
Health and Social
Care Act 2001) to
use routinely
collected hospital
administrative data
to provide measures
of quality of delivery
of healthcare by
provider
Guarantors
T-YW and AM
Contributorship
T-YW extracted the
relevant ICD-10
codes, carried out
the literature review
and drafted the
manuscript. M-HJ
and AB obtained and
analysed the data
and prepared the
Journal of the Royal Society of Medicine
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113240

Health for England.15 It is available for every yearfrom 1989 onwards and comprises data gatheredlocally from each NHS hospital’s Patient Admin-istration System or Hospital Information System.4
It covers all inpatient and day-case activity deliv-ered by NHS hospitals in England, and containsdemographic, administrative and clinical infor-mation. The data-set contains over 300 fields in-cluding age, gender, admission method, primaryand secondary diagnosis fields, length of stay, andmethod of discharge (including in-hospital death).The basic unit of the data-set is the consultantepisode, covering the continuous period of timeduring which a patient was under the care of oneconsultant. Episodes of care were linked into ad-missions and those ending in transfer to anotherhospital were linked together to avoid multiplecounting. The 10th International Classification ofDiseases (ICD-10) is used for diagnosis coding.
For each financial year from 1999–2000 to 2008–2009, we obtained HES records in which there wasan ICD-10 code containing the following key-words: ‘adverse drug reaction’, ‘drug-induced’,‘due to drug’, ‘due to medicament’ or ‘drug al-lergy’. For comprehensiveness, we also searchedfor ICD-10 codes relevant to ADRs containing theword ‘immunization’, since vaccines were consid-ered as a form of medication. We then divided themain diagnostic codes into chapters based on ICD-10, as shown in Appendix 1 online (see http://jrsm.rsmjournals.com/cgi/content/full/103/6/239/DC1). We also analysed codes in the range Y40–59,which are known as ‘external cause’ codes or‘secondary diagnoses’. In this way, we excludedaccidental or intentional poisoning due to drugs.We analysed those codes that explicitly stated thatthe admission was caused by a certain drug.
HES records contain one main diagnosis codeand 13 (six up to 2000) secondary diagnosis codes.We flagged all the emergency admissions withADR-related ICD-10 codes in either the primarydiagnoses or secondary diagnoses fields. We calcu-lated the frequency of each three-digit external Ycodes and of related ADRs ICD-10 codes of eachchapter for each financial year. We excluded poss-ible duplications in coding; an admission codingboth ADR-related primary and secondary diag-noses is only counted once, as shown in Table 1.When analysed by individual ICD-10 chapters orcategories in Tables 2–5, these admissions might becounted twice or more. However, the majority of the
admissions (99.5% for year 2008–2009) only had oneADR-related ICD-10 code in their diagnosis.
For the latest year, 2008–2009, we examined thenumber of admissions by age, gender, proportionof older people (age >65 yrs), total bed-days andin-hospital mortality of each category of ADR. Weshowed the distribution of hospital-level ADRrates on a funnel plot. Statistical analysis wasperformed with SAS software (version 9.2). Forall analyses, only data for emergency (unplanned)admissions were used.
ResultsOverall hospital admissions for ADRs
Table 1 summarizes the annual number of totalhospital admissions, the number of admissions as-sociated with ADRs and in-hospital mortalityrates. In our 10-year study period, there were59,718,694 total emergency hospital admissionsand 557,978 admissions with a diagnostic code in-dicative of ADRs (0.9%). Of these, 188,024 wereprimary diagnoses and 444,780 were of ‘externalcause’. There were 26,399 in-hospital deaths inADR admissions, a case-fatality rate of 4.7%.
Ten-year trends in hospital admissions forADRs
Between 1999 and 2008, the total number of hospi-tal admissions increased by 28.3%, but the totalnumber of admissions due to ADRs increased by76.8%. The majority of the latter was due to anincrease in external cause codes. The in-hospitalmortality rate of ADR admissions increased by10%, from 4.3% to 4.7%, although this stabilizedfrom 2004 onwards (Table 1).
Tables 2 and 3 describe the burden of ADRsaccording to ICD-10 code. The number of ADRswith a primary diagnosis increased by 36.8%during this study. Nephropathy due to drugs(from 109 to 303 admissions), cardiovascular con-sequences (from 1238 to 3399 admissions) anddrug-induced lung disorders (from 64 to 157admissions) were the three fastest growing ADRsas a primary diagnosis (Table 2). Mental and be-havioural disorders due to drugs decreased 6.8%during the 10-year period, although the categorybore the highest admission burden (57,096 diag-noses in the study period). Drug-induced anaemia(−21.8%) and complications following injection,
tables and figure.
AM, PA, DB and MM
conceived the study,
mentored the other
authors and made
critical contributions
to the manuscript at
each stage
Acknowledgements
None
Reviewer
David Henry
Ten-year trends in hospital admissions for adverse drug reactions in England 1999–2009
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113 241

immunization or anaesthesia (−7.0%) declinedduring the years 2004–2008.
The number of ADRs recorded in any second-ary diagnosis field increased 105.8% during thestudy period (Table 3).The three fastest growingADRs as external causes were drugs related to:gastrointestinal system (from 302 to 854 admis-sions); water-balance (from 2081 to 5789 admis-sions); and systemic agents (from 5146 to 12,667admissions). In contrast, the only reported ratewhich showed a decrease was under the categoryof bacterial vaccines (from 297 to 153 admissions).
General description for year 2008–2009
In 2008–2009, the total number of emergencyadmissions in England was 6,830,067, of which75,076 (1.1%) were drug-related (Table 1). Thetotal admission rate in England was 13,726 per100,000 person-years and the ADR admissionrate in England was 146 per 100,000 person-years(data not shown). Mental and behavioural dis-orders due to drugs (24.5%), cardiovascular con-sequences (15.1%) and complications followinginjection, immunization or anaesthesia (14.8%)were the most frequent manifestations of ADRs(Table 4). Systemic agents were the most impli-cated class (Y43, 19.2%), followed by analgesics,antipyretics and anti-inflammatory drugs (Y45,13.3%) and cardiovascular drugs (Y52, 12.9%)(Table 5). Systemic agents (Y43) were primarilyantineoplastic or immunosuppressive drugs.
The admission burden was highest for mentaland behavioural disorders due to drugs (94,579total bed-days), but in-hospital mortality rate washighest for lung disorders due to drugs (17.2%)(Table 4). The highest admission burden wasassociated with systemic agents (Y43, 112,667 totalbed-days), but the in-hospital mortality rate washighest among ADR due to agents affecting bloodconstituents (Y44, 9.4%).
Age distribution for year 2008–2009
Most hospital admissions associated with adversedrug reactions occurred in older patients. In 2008–2009, 58.5% of hospital admissions in which therewas an external ICD-10 code for ADR occurred inpeople aged 65 years and over. The median age ofADRs with an external code was 70 (Table 5). ADRsdue to bacterial vaccines (Y58) usually occurred in Ta
ble
1To
taln
umbe
rof
emer
genc
yad
mis
sion
sfo
rw
hich
ther
ew
asa
prim
ary
diag
nosi
sor
‘ext
erna
lcau
se’o
fAD
Rfr
om19
99to
2008
Year
1999
–200
020
00–2
001
2001
–200
220
02–2
003
2003
–200
420
04–2
005
2005
–200
620
06–2
007
2007
–200
820
08–2
009
Cha
nge
(%)
1999
–200
8Ch
ange
(%)
2004
–200
8
Tota
lnum
ber
ofad
mis
sion
s5,
321,
796
5,31
9,79
15,
337,
034
5,49
4,06
65,
818,
057
6,11
6,50
76,
423,
646
6,49
6,94
56,
560,
785
6,83
0,06
728
.311
.7N
umbe
rwith
drug
-indu
ced
code
s16
,434
16,2
3717
,151
16,6
4518
,307
19,6
5220
,465
20,0
0920
,685
22,4
3936
.514
.2N
umbe
rwith
exte
rnal
caus
eco
des
31,4
8632
,641
33,8
4236
,617
41,7
2244
,745
50,0
6353
,198
56,8
8363
,583
101.
942
.1To
tala
dmis
sion
sdu
eto
AD
Rs
42,4
5343
,288
45,5
1847
,455
53,2
1856
,629
61,9
3164
,536
67,8
7475
,076
76.8
32.6
In-h
ospi
talm
orta
lity
ofA
DR
ad-
mis
sion
s18
1618
7922
5924
8026
7226
7928
7830
1331
8935
3494
.631
.9
In-h
ospi
talm
orta
lity
rate
ofA
DR
adm
issi
ons
4.3
4.3
5.0
5.2
5.0
4.7
4.6
4.7
4.7
4.7
10.0
−0.5
Journal of the Royal Society of Medicine
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113242

Tabl
e2
Ann
ualn
umbe
rof
emer
genc
yad
mis
sion
sw
ith
apr
imar
ydi
agno
sis
for
anA
DR
ICD
-10
chap
ters
Des
crip
tion
1999
–20
0020
00–
2001
2001
–20
0220
02–
2003
2003
–20
0420
04–
2005
2005
–20
0620
06–
2007
2007
–20
0820
08–
2009
Cha
nge
(%)1
999–
2008
Cha
nge
(%)2
004–
2008
DD
rug-
indu
ced
anae
mia
155
138
145
162
143
316
259
178
194
247
59.4
−21.
8E
Dru
g-in
duce
dm
etab
olic
diso
rder
s85
782
482
195
410
1411
2511
8412
1813
1615
6182
.138
.8
FM
enta
land
beha
viou
ral
diso
rder
sdu
eto
drug
s59
3754
6655
1757
0359
0560
4459
8956
0353
9955
33−6
.8−8
.5
GD
rug-
indu
ced
neur
omus
cula
rdi
sord
ers
889
873
864
812
933
1042
1188
1266
1304
1578
77.5
51.4
HD
rug-
indu
ced
cata
ract
and
hear
ing
loss
2712
1010
2128
3140
2242
55.6
50.0
IC
ardi
ovas
cula
rco
nseq
uenc
esdu
eto
drug
s12
3813
8714
3814
8317
7620
7623
7424
9229
9633
9917
4.6
63.7
JD
rug-
indu
ced
lung
diso
rder
s64
4853
8880
103
101
123
110
157
145.
352
.4K
Toxi
cliv
erdi
seas
e43
844
643
848
754
949
357
853
053
361
440
.224
.5L
Der
mat
itis
due
todr
ugs
1870
1829
1866
1935
2183
2392
2719
2713
2842
3213
71.8
34.3
MD
rug-
indu
ced
imm
une
diso
rder
s19
4622
2233
0723
3822
9823
2923
6123
8024
9725
6431
.810
.1N
Nep
hrop
athy
due
todr
ugs
109
134
163
149
183
208
207
202
298
303
178.
045
.7T
Com
plic
atio
nsfo
llow
ing
inje
ctio
n,im
mun
izat
ion
oran
aest
hesi
a29
5629
3026
1426
0833
2235
9335
8933
5732
8933
4313
.1−7
.0
Tota
l16
,486
16,3
0917
,236
16,7
2918
,407
19,7
4920
,580
20,1
0220
,800
22,5
5436
.814
.2
Ten-year trends in hospital admissions for adverse drug reactions in England 1999–2009
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113 243

Tabl
e3
Ann
ualn
umbe
rof
emer
genc
yad
mis
sion
sw
ith
an‘e
xter
nalc
ode’
for
anA
DR
ICD
-10
code
sD
escr
iptio
n19
99–
2000
2000
–20
0120
01–
2002
2002
–20
0320
03–
2004
2004
–20
0520
05–
2006
2006
–20
0720
07–
2008
2008
–20
09C
hang
e(%
)199
9–20
08
Cha
nge
(%)2
004–
2008
Y40
Sys
tem
ican
tibio
tics
3364
3510
3439
3719
4446
5065
5738
5976
6297
6996
108.
038
.1Y
41O
ther
syst
emic
anti-
infe
ctiv
esan
dan
tipar
asiti
cs63
571
267
675
784
396
710
6412
0512
4113
6411
4.8
41.1
Y42
Hor
mon
esan
dth
eir
synt
hetic
subs
titut
esan
dan
tago
nist
s20
8921
5420
6423
7126
3227
8530
4121
0134
9643
5210
8.3
56.3
Y43
Prim
arily
syst
emic
agen
ts51
4352
6861
6266
6368
9273
3284
4797
8911
,175
12,6
6714
6.2
72.8
Y44
Age
nts
prim
arily
affe
ctin
gbl
ood
cons
titue
nts
2939
2973
3083
3363
4003
2904
2993
2992
3055
3171
7.9
9.2
Y45
Ana
lges
ics,
antip
yret
ics
and
anti-
infla
mm
ator
ydr
ugs
4364
4385
4302
4788
5328
6078
7054
7375
7857
8747
100.
443
.9
Y46
Ant
iepi
lept
ics
and
anti-
Park
inso
nism
drug
s96
292
710
0410
2511
0612
2212
9613
1613
5414
9255
.122
.1
Y47
Sed
ativ
es,h
ypno
tics
and
anti-
anxi
ety
drug
s29
335
234
635
645
046
251
956
159
862
411
3.0
35.1
Y48
Ana
esth
etic
san
dth
erap
eutic
gase
s18
519
415
116
720
820
626
524
828
935
089
.269
.9Y
49Ps
ycho
trop
icdr
ugs,
note
lsew
here
clas
sifie
d13
7315
6314
8514
6917
9819
3519
6221
3322
5624
2276
.425
.2
Y50
Cen
tral
nerv
ous
syst
emst
imul
ants
,not
else
whe
recl
assi
fied
5264
5658
6371
111
6883
8869
.223
.9
Y51
Dru
gspr
imar
ilyaf
fect
ing
the
auto
nom
icne
rvou
ssy
stem
1698
1834
1981
2135
2559
2866
3164
3178
3331
3591
111.
525
.3
Y52
Age
nts
prim
arily
affe
ctin
gth
eca
rdio
vasc
ular
syst
em35
8740
4041
6445
2451
4759
4965
8871
0077
2385
1813
7.5
43.2
Y53
Age
nts
prim
arily
affe
ctin
gth
ega
stro
inte
stin
alsy
stem
302
338
293
321
411
457
579
584
670
854
182.
886
.9
Y54
Age
nts
prim
arily
affe
ctin
gw
ater
-bal
ance
and
min
eral
and
uric
acid
met
abol
ism
2081
2258
2613
3115
3833
4316
4946
5109
5115
5789
178.
234
.1
Y55
Age
nts
prim
arily
acts
moo
than
dsk
elet
alm
uscl
ean
dre
spir
ator
ysy
stem
292
308
270
272
329
352
383
405
416
485
66.1
37.8
Y56
Topi
cala
gent
prim
arily
affe
ctin
gsk
in/
muc
ous
mem
bran
esan
dop
th/o
t-rh
-lary
/de
ntal
drug
s
784
639
719
705
743
808
864
909
873
1020
30.1
26.2
Y57
Oth
eran
dun
spec
ified
drug
san
dm
edic
amen
ts12
9712
8013
4613
6814
4817
3821
1523
2925
4328
9212
3.0
66.4
Y58
Bac
teri
alva
ccin
es29
721
816
017
231
125
017
217
816
315
3−4
8.5
−38.
8Y
59O
ther
and
unsp
ecifi
edva
ccin
esan
dbi
olog
ical
subs
tanc
e32
926
622
221
734
035
938
033
133
641
225
.214
.8
Tota
l32
,069
33,2
8334
,536
37,5
6542
,890
46,1
2251
,681
53,8
8758
,871
65,9
8710
5.8
43.1
Journal of the Royal Society of Medicine
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113244

Tabl
e4
Num
ber
ofH
ESem
erge
ncy
adm
issi
ons
wit
ha
prim
ary
diag
nosi
sfo
ran
AD
Rin
2008
–09:
med
ian
age
ofad
mis
sion
s,ol
dag
ean
dge
nder
dist
ribu
tion
ofad
mis
sion
s,to
talb
ed-d
ays
and
mor
talit
y
ICD
-10
chap
ters
Des
crip
tion
Tota
l(%
)M
en(%
)M
edia
nag
eA
ge65
+(%
)To
talb
ed-
days
In-h
ospi
tal
mor
talit
yra
te
DD
rug-
indu
ced
anae
mia
1.1
44.1
6857
.128
987.
7E
Dru
g-in
duce
dm
etab
olic
diso
rder
s6.
944
.872
62.5
19,0
786.
2F
Men
tala
ndbe
havi
oura
ldis
orde
rsdu
eto
drug
s24
.568
.933
3.5
94,5
791.
0G
Dru
g-in
duce
dne
urom
uscu
lar
diso
rder
s7.
044
.470
60.7
32,3
896.
7H
Dru
g-in
duce
dca
tara
ctan
dhe
arin
glo
ss0.
242
.952
28.6
454
4.8
IC
ardi
ovas
cula
rco
nseq
uenc
esdu
eto
drug
s15
.146
.578
80.5
36,4
303.
8J
Dru
g-in
duce
dlu
ngdi
sord
ers
0.7
55.4
7368
.221
3017
.2K
Toxi
cliv
erdi
seas
e2.
742
.743
24.4
10,4
3011
.4L
Der
mat
itis
due
todr
ugs
14.2
41.2
6041
.942
,801
4.2
MD
rug-
indu
ced
imm
une
diso
rder
s11
.456
.469
60.9
31,5
1812
.5N
Nep
hrop
athy
due
todr
ugs
1.3
58.1
6655
.846
329.
6T
Com
plic
atio
nsfo
llow
ing
inje
ctio
n,im
mun
izat
ion
oran
aest
hesi
a14
.840
.957
30.2
26,7
172.
9
Tota
l22
,554
100.
051
.459
41.5
302,
574
4.8
Ten-year trends in hospital admissions for adverse drug reactions in England 1999–2009
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113 245

Tabl
e5
Ann
ualn
umbe
rof
emer
genc
yad
mis
sion
sw
ith
an‘e
xter
nalc
ode’
for
anA
DR
in20
08–0
9:m
edia
nag
eof
adm
issi
ons,
old
age
and
gend
erdi
stri
buti
onof
adm
issi
ons,
tota
lbed
-day
san
dm
orta
lity
ICD
-10
code
sD
escr
iptio
nTo
tal(
%)
Men
(%)
Med
ian
age
Age
65+(
%)
Tota
lbed
-da
ysIn
-hos
pita
lm
orta
lity
rate
Y40
Sys
tem
ican
tibio
tics
10.6
40.5
6447
.482
,684
4.3
Y41
Oth
ersy
stem
ican
ti-in
fect
ives
and
antip
aras
itics
2.1
30.6
6449
.115
,620
2.8
Y42
Hor
mon
esan
dth
eir
synt
hetic
subs
titut
esan
dan
tago
nist
s6.
644
.567
54.6
53,0
656.
9
Y43
Prim
arily
syst
emic
agen
ts19
.242
.561
38.2
112,
667
5.4
Y44
Age
nts
prim
arily
affe
ctin
gbl
ood
cons
titue
nts
4.8
46.2
7675
.945
,865
9.4
Y45
Ana
lges
ics,
antip
yret
ics
and
anti-
infla
mm
ator
ydr
ugs
13.3
44.0
6957
.193
,656
4.4
Y46
Ant
iepi
lept
ics
and
anti-
Park
inso
nism
drug
s2.
348
.064
49.2
22,4
882.
1Y
47S
edat
ives
,hyp
notic
san
dan
ti-an
xiet
ydr
ugs
0.9
44.6
6649
.788
754.
5Y
48A
naes
thet
ics
and
ther
apeu
ticga
ses
0.5
44.9
4427
.728
612.
9Y
49Ps
ycho
trop
icdr
ugs,
note
lsew
here
clas
sifie
d3.
738
.172
61.6
36,7
673.
5Y
50C
entr
alne
rvou
ssy
stem
stim
ulan
ts,n
otel
sew
here
clas
sifie
d0.
153
.449
35.7
822
3.4
Y51
Dru
gspr
imar
ilyaf
fect
ing
the
auto
nom
icne
rvou
ssy
stem
5.4
49.6
7881
.827
,746
1.8
Y52
Age
nts
prim
arily
affe
ctin
gth
eca
rdio
vasc
ular
syst
em12
.953
.178
81.3
80,5
703.
3Y
53A
gent
spr
imar
ilyaf
fect
ing
the
gast
roin
test
inal
syst
em1.
337
.275
62.2
8790
3.9
Y54
Age
nts
prim
arily
affe
ctin
gw
ater
-bal
ance
and
min
eral
and
uric
acid
met
abol
ism
8.8
35.6
8086
.871
,974
5.4
Y55
Age
nts
prim
arily
acts
moo
than
dsk
elet
alm
uscl
ean
dre
spir
ator
ysy
stem
0.7
34.6
5130
.932
823.
3
Y56
Topi
cala
gent
prim
arily
affe
ctin
gsk
in/m
ucou
sm
embr
anes
and
opth
/ot-
rh-la
ry/d
enta
ldru
gs1.
541
.758
39.6
8061
3.8
Y57
Oth
eran
dun
spec
ified
drug
san
dm
edic
amen
ts4.
443
.369
55.6
33,8
664.
5Y
58B
acte
rial
vacc
ines
0.2
54.9
<17.
262
30.
0Y
59O
ther
and
unsp
ecifi
edva
ccin
esan
dbi
olog
ical
subs
tanc
e0.
647
.157
17.0
2070
1.5
Tota
l65
,987
100
42.9
7058
.568
0,83
34.
6
Journal of the Royal Society of Medicine
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113246

infants (median age <1), and younger patientstended to have ADRs from anaesthetics and thera-peutic gases (Y48, median age 44) or CNS stimu-lants (Y50, median age 49). Older patients (>65 yrs)tended to have ADRs due to water-balance drugs(Y54, median age 80), drugs affecting the auto-nomic nervous system (Y51, median age 78) or thecardiovascular system (Y52, median age 78).Agents primarily affecting water-balance and min-eral and uric acid metabolism (Y54) includedmineralocorticoids, diuretics, agents affecting cal-cification or uric acid metabolism, and mineralsalts.
Younger people tended to manifest ADRs asmental and behavioural disorders (median age 33)or toxic liver disease (median age 43). By contrast,those aged >65 yrs tended to have a clinical pictureof cardiovascular consequences (median age 78),lung disorders (median age 73) or metabolic dis-orders (median age 72) (Table 4).
Gender distribution for year 2008–2009
There was little gender difference in admissionswith a primary code of ADR (51.4% men) (Table 4).However, female patients predominate in admis-sions with an external cause code of ADR (42.9%men) (Table 5). Men were more likely to suffer frommental and behavioural disorders (68.9% men)and women were more likely to suffer from com-plications following injection, immunization oranaesthesia (40.9% men) (Table 4). Women appearmore likely to be affected by ADRs due to systemicanti-infectives and antiparasitics (Y41, 30.6% men),agents primarily acting on smooth and skeletalmuscle and respiratory system (Y55, 34.6% men) orwater-balance agents (Y54, 35.6% men) (Table 5).
Socioeconomic status and ADR
We analysed ADR rate per 1000 admissions bypopulation-weighted quintiles based on the Car-stairs deprivation index allocated via the postcodeto a small geographical area (‘output area’). How-ever, there was no simple socioeconomic gradientin ADR rates per 1000 admissions, which were9.9, 10.7, 10.4, 9.9 and 9.1 from quintile 1 (leastdeprived) through quintile 5 (most deprived).
Individual performance of NHS acutehospital trusts
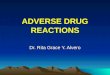
We analysed the relationship between total emer-gency admissions and the percentage of ADR-related admissions for NHS acute hospital trusts,as shown in Figure 1. There were two trusts withunusually high rates: one with the proportion of12% (3393 admissions) and the other with 34%(1134 admissions). Both of them were not includedin the funnel plot. However, there was still widevariation in ADR-related admission percentagesbetween individual NHS trusts, with many rateslying outside the control limits despite excludingthese two trusts.
Discussion
Characteristics of this study
This study on hospital admissions for adversedrug reactions is unique in several aspects. Thestrengths of this study included its comprehen-siveness in covering all NHS hospital admissionsin England and its time trends.
Building on previous work using HES,4,16 wehave tried to be systematic in capturing all ADR-related ICD-10 codes. We had access to mortalitydata associated with hospital admissions, whichgave us a further insight into the severity of ADR-related admissions and we accessed patient-levelrather than aggregate data. A prior study con-ducted by Pirmohamed and colleagues analysedadmissions due to ADRs in two North-WestEnglish hospitals.3 However, their sample size(18,820 admissions) was substantially less thanin this nationwide survey.
Limitations of this study
The main limitation of our study is that HospitalEpisode Statistics data have the weaknesses associ-ated with all routinely collected data; namely miss-ing, incomplete or inaccurate data. Differences incoding practice between hospitals or populationscovered make comparisons at hospital level diffi-cult and will be one key explanation of the vari-ation seen in Figure 1. We were also unable to ruleout changes in coding as a result of behavioural orpolicy change as an explanation for our findings. Ifsuch variation occurs between hospitals, it is also
Ten-year trends in hospital admissions for adverse drug reactions in England 1999–2009
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113 247

likely within hospitals over time, which is a poss-ible explanation for some of the trends observed.Nevertheless, HES represents one of several im-portant resources for monitoring ADRs because ofits size, national coverage and relatively standard-ized recording regulations.
We do not have data on the pre-hospital utiliza-tion of drugs (or over-the-counter drug usage), nordo we have details on the number of drugs pre-scribed or taken by patients before admission.There is no indication on the HES record whetherthe recorded ADRs were present on admission, oroccurred during a patient’s stay in hospital. Ifgiven as a primary diagnosis, in the first episode ofcare, then it is perhaps more likely that the ADRoccurred prior to admission, and if given as a sec-ondary diagnosis, then perhaps more likely tohave occurred in hospital. However, this inter-pretation is limited, as there will be some consider-able blurring between these two scenarios.
We do not have data from general practice oroutpatient visits, and we are unable to link ADRsto consultations.12 Minor ADRs which might affectthe patient’s quality of life but not to the extent ofhospital admission were not covered by our study.We were also unable to obtain data regarding riskbenefit calculations of ADRs. Hence, given thelimitations of our data, we must interpret the re-sults with caution.
Overall trends
Our study showed that the number of admissionsdue to ADRs has increased significantly over thetime period examined. The reported increase ofADR admissions by 76.8% may be due to im-proved record keeping and increased publicawareness. Population ageing also added to thistrend,17 since ADRs are most frequently encoun-tered in older people with multiple long-termconditions.
In this study, we included immunization aspart of our analysis. Complications following in-jection, immunization or anaesthesia accountedfor 31,601 admissions in the study decade, 26,717bed days in year 2008–2009, and an in-hospitalmortality rate of 2.9%. Most of the admissionsoccurred in infants.
The majority of the increase in ADR admissionswas due to increases in admissions with an ADR-related external code (105.8% change in the studyperiod). These are most likely to have developedas a result of treatments in hospital, in contrastto admissions with a primary diagnosis of ADR,which may be due to drugs prescribed in the com-munity or from a previous hospital admission.
Comparison with other studies
Pirmohamed et al. estimated that in England,ADRs were responsible for 6.5% of all emergencyhospital admissions in adults and at least 5000deaths per year.3 However, this study excludedsome categories of patients. Howard et al. sug-gested that the percentage of preventable drug-related admissions to hospitals was 3.7%.18,19 Inour study, ADR admissions accounted for only0.8–1.1% of all annual admissions for 1999–2008,and the in-hospital mortality for ADR admissionsfor 2008–2009 was 3534, which was substantiallyless than suggested in previous literature. Thereare two possible explanations for this inconsist-ency. First, this may suggest a suboptimal record-ing of ADRs in the HES database because ofunder-recognition and under-reporting of ADRs inroutine hospital activity data.16 Conversely, ourstudy is based on a comprehensive nationwidedata-set, which might also be more close to thereality than previous extrapolations from smallerscale studies.
Contradictory to some prior expectations,4 the in-troduction of the Quality and Outcome Framework
Figure 1Funnel plot of the relationship between the total emergencyadmissions and the cases of ADRs as percentage of totalemergency admissions for NHS acute hospital trusts
Journal of the Royal Society of Medicine
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113248

(QOF) on 1 April 2004 in England did not seem toaggravate the burden of ADRs. Instead, the in-hospital mortality in ADR admissions stabilized at4.7% from 2004 onwards. Drug-induced anaemiaand complications following injection, immuniz-ation or anaesthesia increased for the years 1999–2004, culminated in year 2004–2005, and thendecreased thereafter.
There is an association between increasing ageand ADR risk,20 and elderly people are more suscep-tible to ADRs. Previous studies suggested thatdiuretics and antiplatelets are often used in elderlypatients and accounted for 5.3% and 4.0%, respect-ively, of all primary care prescriptions in England.18
This study also showed similar findings, in whichagents primarily affecting water-balance (Y54) andcardiovascular system (Y52) are the most implicatedcategories in ADRs in older people.
Pirmohamed et al. reported that 59% of thepatients admitted with an ADR were female.3 Ourstudy also showed that 57% of hospital admissionswith a secondary code of ADR are female. Thepharmacokinetics and pharmacodynamics of drugmetabolism differ between the two sexes and areinfluenced by gender-specific factors such as bodybuild, hormonal transitions, or medical-seekingbehaviour.21 We cannot tell from this study if thesedifferences are due to true discrepancies in ADRoccurrence rates or are consequences of genderdifferences in prescription, consultation and usagepatterns.
As to the drug types most implicated in ADR,our study showed that systemic agents are respon-sible for one-fifth of total ADR admissions in year2008–2009, followed by analgesics and cardiovascu-lar drugs. Systemic agents are also the third fastestgrowing agent in ADR-related admissions duringthe study period. These findings are similar to pre-vious works by Waller et al.,16 but other studies alsoshowed that low-dose aspirin, diuretics, warfarin,and non-steroidal anti-inflammatory drugs werethe most commonly implicated drugs in ADR.3,8,18
Our results differed from this, and this can be ex-plained by the different classification system of thedrugs we used. We examined ICD-10 external causecodes to infer to the drug class, instead of individualgeneric name drugs. Broad groupings of drugs areused in this study, as exemplified by the systemicagent category, which includes antineoplasticdrugs, immunosuppressive agents, enzymes, anti-allergic and anti-emetic drugs.
Conclusions
The advent of modern medicine has brought hopeto many people with previously untreatable diseases,such as the use of penicillin to treat syphilis, or com-bination therapy to treat HIV infection. Nevertheless,ADRs are unwanted events following drug prescrip-tion and should be considered as part of a risk-benefitapproach when prescribing medicines, particularly invulnerable groups. Although ADRs continue to be amajor public health problem resulting in a consider-able use of NHS hospital resources and a significantnumber of deaths, their impact is often overlooked.Hospital admissions showed an apparent rise in rela-tion to ADRs; however, this may be a consequence ofimproved recording.
There are several initiatives exploring suscepti-bility to ADRs through international collabora-tions (such as FP7-funded EU-ADR, The SeriousAdverse Event Consortium, among others). Spon-taneous reporting is important in identifying pre-viously undetected ADRs, mostly type-B reactions,to allow appropriate drug regulatory action to betaken but frequently is unable to detect rare eventsuntil after years of patient use, with less than 10%reported.2 It is also a passive reporting policy andwould benefit from being linked to other data-bases. More active drug surveillance schemesmight be a potential strategy to address the highmortality associated with ADR admissions (4.7%in this study).
Other current strategies to improve drug safetyinclude stringent safety testing; nationwide imple-mentation of updated prescribing software to reduceprescribing errors;22,23 medicines reconciliation onadmission and discharge from hospital to minimizepolypharmacy;24 financial incentives for clinicians toreport ADRs to address under-recording; and fund-ing for research to decipher the complex multifacto-rial pathogenesis of idiosyncratic ADRs.25
Because of the wide range of medications avail-able, ADRs vary in manifestations and organsystem. Heightened awareness of pharmaco-vigilance by clinicians in diagnosing ADRs is crucialfor continued drug safety monitoring. Over 70%of adverse drug reactions were possibly avoidable3
and preventable through simple improvements inprescribing, e.g. increased awareness of warningprompts of possible drug interactions and high-riskpatient groups, prescribing a drug at the lowest dosenecessary to achieve the therapeutic target.
Ten-year trends in hospital admissions for adverse drug reactions in England 1999–2009
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113 249

Developed countries worldwide tend to haveprogressively older populations. In the UK, thenumber of people age 65 years and over is esti-mated to increase by 53% between 2001 and 2031.17
This increase will result in a rise in the number ofpeople at higher risk of suffering from ADRs,which are more likely to be severe in this group.26
In our study, we also noticed that most ADR in-creases occur in those over the age of 65.
In this study, systemic agents were the mostimplicated and the third fastest growing agent inADR-related admissions. This is also correlatedwith the rapid ageing of the English population,since systemic anti-cancer therapy (SACT) is tar-geted at malignancies whose risk increases withage. According to NCEPOD report 2008,27 43% ofcancer cases suffered from clinically significanttreatment-related toxicities.
Our data suggest that the number of ADR ad-missions may have increased at a greater rate thanthe increase in total hospital admissions, but it isunclear whether this could also be due to increasedrecording. Also, the percentage of ADR-related ad-missions varied considerably between individualNHS trusts. This study should prompt policy-makers toward implementing further measures toreduce ADR incidence and their associated in-hospital mortality; and to make greater use of rou-tinely collect NHS data, such as Hospital EpisodeStatistics, to monitor the epidemiology of ADRsand identify potentially avoidable aetiological fac-tors, and to improve the completeness, accuracyand standardization of coding across hospitals.
References1 Pirmohamed M, Breckenridge AM, Kitteringham NR,
Park BK. Adverse drug reactions. BMJ 1998;316:1295–82 Pirmohamed M, Park BK. Adverse drug reactions: back to
the future. Br J Clin Pharmacol 2003;55:486–923 Pirmohamed M, James S, Meakin S, et al. Adverse drug
reactions as cause of admission to hospital: prospectiveanalysis of 18,820 patients. BMJ 2004;329:15–19
4 Patel H, Bell D, Molokhia M, et al. Trends in hospitaladmissions for adverse drug reactions in England:analysis of national hospital episode statistics 1998–2005.BMC Clin Pharmacol 2007;7:9
5 Chutka DS, Takahashi PY, Hoel RW. Inappropriatemedications for elderly patients. Mayo Clin Proc2004;79:122–39
6 Viktil KK, Blix HS, Moger TA, Reikvam A. Polypharmacyas commonly defined is an indicator of limited value inthe assessment of drug-related problems. Br J ClinPharmacol 2007;63:187–95
7 Willlams CM. Using medications appropriately in olderadults. Am Fam Physician 2002;66:1917–24
8 Davies EC, Green CF, Taylor S, Williamson PR, MottramDR, Pirmohamed M. Adverse drug reactions in hospitalin-patients: a prospective analysis of 3695 patient-episodes. PLoS One 2009;4:e4439
9 Pham CB, Dickman RL. Minimizing adverse drug eventsin older patients. Am Fam Physician 2007;76:1837–44
10 Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR,Beers MH. Updating the Beers criteria for potentiallyinappropriate medication use in older adults: results of aUS consensus panel of experts. Arch Intern Med2003;163:2716–24
11 O’Mahony D, Gallagher PF. Inappropriate prescribing inthe older population: need for new criteria. Age Ageing2008;37:138–41
12 Chan DC, Hao YT, Wu SC. Characteristics of outpatientprescriptions for frail Taiwanese elders with long-termcare needs. Pharmacoepidemiol Drug Saf 2009;18:327–34
13 Murray MD, Callahan CM. Improving medication use forolder adults: an integrated research agenda. Ann InternMed 2003;139:425–9
14 Konstam MA, Weir MR, Reicin A, et al. Cardiovascularthrombotic events in controlled, clinical trials of rofecoxib.Circulation 2001;104:2280–8
15 HES Online London: Department of Health; 2009. Seehttp://www.hesonline.nhs.uk/Ease/servlet/ContentServer?siteID=1937&categoryID=658&keyword=validation
16 Waller P, Shaw M, Ho D, Shakir S, Ebrahim S. Hospitaladmissions for ‘drug-induced’ disorders in England: astudy using the Hospital Episodes Statistics (HES)database. Br J Clin Pharmacol 2005;59:213–19
17 Majeed A, Aylin P. The ageing population of the UnitedKingdom and cardiovascular disease. BMJ 2005;331:1362
18 Howard RL, Avery AJ, Slavenburg S, et al. Which drugscause preventable admissions to hospital? A systematicreview. Br J Clin Pharmacol 2007;63:136–47
19 Howard RL, Avery AJ, Howard PD, Partridge M.Investigation into the reasons for preventable drug relatedadmissions to a medical admissions unit: observationalstudy. Qual Saf Health Care 2003;12:280–5
20 Routledge PA, O’Mahony MS, Woodhouse KW. Adversedrug reactions in elderly patients. Br J Clin Pharmacol2004;57:121–6
21 Seeman MV. Gender differences in the prescribing ofantipsychotic drugs. Am J Psychiatry 2004;161:1324–33
22 Pollock M, Bazaldua OV, Dobbie AE. Appropriateprescribing of medications: an eight-step approach. AmFam Physician 2007;75:231–6
23 Kaushal R, Barker KN, Bates DW. How can informationtechnology improve patient safety and reduce medicationerrors in children’s health care? Arch Pediatr Adolesc Med2001;155:1002–7
24 NICE, NPSA. Technical patient safety solutions formedicines reconciliation on admission of adults tohospital. 2007. See http://www.nice.org.uk/nicemedia/pdf/PSG001Guidance.pdf.
25 Pirmohamed M. Genetic factors in the predisposition todrug-induced hypersensitivity reactions. AAPS J2006;8:E20–6
26 McLean AJ, Le Couteur DG. Aging biology and geriatricclinical pharmacology. Pharmacol Rev 2004;56:163–84
27 NCEPOD. For better, for worse? A review of the care ofpatients who died within 30 days of receiving systemicanti-cancer therapy. 2008. See http://www.ncepod.org.uk/2008report3/Downloads/SACT_report.pdf.
Journal of the Royal Society of Medicine
J R Soc Med 2010: 103: 239–250. DOI 10.1258/jrsm.2010.100113250