Embed Size (px)
Citation preview

Temporal and receptor correlates of the estrogen response in sheep
Frank C. Greiss, Jr., M.D., James C. Rose, Ph.D., Timothy E. Kute, Ph.D., Randall T. Kelly, M.D., and Lisa S. Winkler, B.S.
Winston-Salem, North Carolina
Uterine blood flow and uterine cytosol and nuclear estrogen receptors were measured at critical times during estradiol-induced vasodilatation in acute anesthetized and chronic conscious sheep preparations at
estradiol bolus injection frequencies from 1 to 24 hours. During acute experiments, the uterine blood flow response was muted and cytosol estrogen receptor replenishment did not occur whereas full replenishment occurred in 12 hours in conscious ewes. In ewes treated with daily estradiol that had a
stable daily uterine blood flow response, the uterine blood flow response 24 hours after uterine biopsy was similar to the preoperative one. Analysis of the duration of peak uterine blood flow levels and the rate of
uterine blood flow descent from peak levels showed that an interval of 18 hours between estradiol injections was necessary for the uterine blood flow response to approximate that observed after 24 hours. These observations suggest: (1) that uterine vascular receptor replenishment is delayed compared with
that of the total uterus; (2) that operative stress compromises cytosol estrogen receptor metabolism and possibly nuclear estrogen receptor function; (3) that the delayed maximum uterine blood flow response to
estradiol in ewes previously untreated with estradiol is due to a trophic uterine effect of daily estradiol stimulation. (AM J OeSTET GVNECOL 1986;154:831-8.)
Key words: Uterine blood flow, estrogen, estrogen receptors, uterine vasodilatation
The uterine blood flow response to estrogenic stimulation has been studied extensively in the oophorectomized ewe. When estradiol-17j3 is injected intravascularly, uterine blood flow is unchanged for 30 minutes. Then a progressive marked increase occurs and reaches peak levels after 1.5 to 2.0 hours. Thereafter, uterine blood flow gradually declines to control levels during 12 to 18 hours.' This response can be duplicated daily. Dose-response curves indicate that the maximum response occurs from 1 J-lg/kg given intravenously, 0.5 J-lg/kg intra-arterially, or 0.5 to 1.0 J-lg given directly into the uterine artery!' 3 If the estradiol injection is given during a continuous infusion of cycloheximide into the uterine artery, the response is ablated.' This observation and the latent phase before the increase in uterine blood flow have been interpreted to indicate that estradiol induces the formation of a vasodilator substance that mediates the vascular response. Although substances have been identified that can cause
From the Departments of Obstetrics and Gynecology, Physiology, and Biochemistry, Bowman Gray School of Medicine of Wake Forest University.
Supported by United States Public Health Service Grants No. HD-11339-21 and No. CA-12197.
Presented at the Fourth Annual Meeting of the American Gynecological and Obstetrical Society, Hot Springs, Virginia, September 4-7,1985.
Reprint requests: Frank C. Greiss,jr., M.D., Department of Obstetrics and Gynecology, Bowman Gray School of Medicine, 300 South Hawthorne Road, Winston-Salem, NC 27103.
a response quantitatively similar to that of estradiol, none of these has been shown to be the mediator per se. One other characteristic of the uterine blood flow response is pertinent. At ovine estrus, uterine blood flow increases from very low preestrous levels to
about half of those observed after maximum doses of estradiol, and these levels are maintained for 24 hours or more! Presumably, the uterine blood flow rise is caused by and lags about 6 hours behind a similar curve of estradiol secretion. However, in our laboratory and in experiments reported to date, a sustained increase in uterine blood flow has never been induced by exogenous estradiol administration except when the estradiol is given intramuscularly in oil. In fact, when estradiol is infused continuously at maximum pharmacologic doses, the uterine blood flow response is no different from that after a single injection! These observations suggest that when maximum pharmacologic doses of estradiol are given, a refractory phase occurs, which may be related to the metabolism of uterine estrogen receptors. To test this hypothesis, we have measured cytosol and nuclear receptors in serial uterine biopsy specimens obtained at critical times during the uterine blood flow response to estradiol in acute and chronic experiments in sheep. In addition, further knowledge of the refractory period has been achieved in conscious ewes by observation of the uterine blood flow response to various frequencies of intermittent estradiol injections.
831

832 Greiss et al.
Methods
Animal preparations Group 1. In a preliminary group of two ewes anes
thetized with pentobarbital sodium, biopsy specimens were obtained from the upper, middle, and lower thirds of the uterine horn and the animals were put to death. The biopsy specimens were analyzed for cytosol estrogen receptor content.
Group 2. Nonpregnant multiparous ewes were anesthetized with intravenous ketamine and supplemental pentobarbital sodium when necessary. Bilateral oophorectomy, implantation of an electromagnetic flow probe around the left middle uterine artery, and implantation of an aortic occlusion back loop were performed as previously described. 5
.6 Two catheters were
threaded via the mammary artery and vein into the descending aorta and inferior vena cava for blood pressure monitoring and estradiol injections. After the ewes recovered from operation, daily intravenous bolus injections of estradiol, 1 f.Lg/kg, prepared after the method of Killam et al. I were given and uterine blood flow was monitored until similar daily flow peaks occurred. Then a uterine biopsy specimen from the horn contralateral to the flow probe was obtained at laparotomy with the animal under ketamine anesthesia 24 hours after the previous estradiol injection. On recovery, daily estradiol doses were continued for 4 to 7 days. Then repeat uterine biopsy specimens were obtained in different animals 6, 12, and 18 hours after the last estradiol injection. Then the ewes were put to death. In a subset of this group biopsy specimens were obtained 24 hours after a previous biopsy and estradiol injection.
Uterine blood flow responses were analyzed as in group 4 described below and uterine biopsy specimens were analyzed for cytosol estrogen receptor and compared by means of analysis of variance and two-tailed Student's t test.
Group 3. Ewes were prepared as in group 2 and after repetitive daily estradiol-induced uterine blood flow peaks occurred, the following acute experiments were performed 24 to 27 hours after the preceding estradiol injection.
Ewes were paralyzed with curare, intubated while under topical anesthesia, and anesthetized with a 2: 1 mixture of nitrous oxide-oxygen. The rate and frequency of respirations were adjusted by a Harvard small animal respirator to maintain normal pH and blood gas levels. Supplemental curare was used as needed throughout the experiment. When uterine blood flow and maternal blood pressure were stable, the uterus was exposed via a midline incision and a control biopsy specimen (1 to 2 gm) from the uterine horn contralateral to the flow probe was obtained. Then an intravenous bolus of estradiol, 1 f.Lg/kg, was given. Repeat uterine biopsy specimens were obtained 5 and
April,1986 Am J Obstet Gynecol
30 minutes and 2, 6, 10, 14, and 18 hours later and the ewes were put to death. Between biopsies, the abdomen was closed to minimize trauma. Biopsy specimens were analyzed for cytosol estrogen receptor and nuclear estrogen receptors as described below. Since cytosol estrogen receptor depletions were similar to those observed in conscious ewes (group 2), control experiments to exclude an effect of operative stress were not performed.
Group 4. In a final group of ewes chronically prepared as in group 2, after daily estradiol-induced uterine blood flow peaks occurred, uterine blood flow responses were observed after the following regimens of intravenous estradiol, 1 f.Lg/kg, bolus injections: every hour for eight doses, every 2 hours for five doses, every 3 hours for four doses, every 4 hours for three doses, and every 6 hours for three doses. Further responses were observed after estradiol given 8, 10, 12, 14, 16, and 18 hours after the preceding estradiol dose. The various estradiol administration regimens were randomized so as to minimize the possible effect of time from initial operation on the observed responses. Five I-minute uterine blood flow levels were averaged every half hour during response periods and results were expressed as a percentage of the maximum flow observed during each individual response. Intraresponse levels at the various dose frequencies were compared after 4 hours with those of the 24-hour dose frequency by means of analysis of variance and the Mann -Whitney test for multiple comparisons.
Cytosol receptor assay Preparation of cytosol. The cytosol fractions were pre
pared by the method of Anderson et al. 7 All procedures were done at 4° C unless otherwise stated. Approximately 0.5 gm of frozen tissue was weighed out and minced into small fragments with a scalpel. The minced tissue was put in a Kontes glass grinder along with 2 ml of buffer A (10 mmol/L Tris, 1.5 mmol/L ethylenediaminetetraacetic acid, 10% glycerol, and 1.0 mmol/L monothioglycerol, pH 7.4 to 7.5) and homogenized. After the homogenate was transferred to a centrifuge tube, another 4 ml of buffer was added. The suspension was centrifuged at 1000 x g for 10 minutes to separate the nuclear and cytosolic fractions. The cytosolic fraction was mixed on a vortex mixer with a dextran-coated charcoal pellet (6 ml of 1.0% Norit A and 0.5% dextran) to remove endogenous estradiol and incubated for 10 minutes at 0° C. After the incubation period, the suspension was centrifuged at 120,000 x g for 30 minutes. The supernatant protein was measured by the Waddell method and normalized to 2 mg/ml for the binding study.
Cytosolic binding assay. The cytosol fraction was used in binding studies done by Scatchard analysis8 and the assay of Katzenellenbogen et al. 9 The Scatchard analysis uses 10 points with doses of tritiated estradiol varying

Volume 154 Number 4
c Q)
c o o .... c .8 'iii are UQ.. Q) •
c:: Cl _E g~ 00 >.E OLL Q) c '': Q)
5
1200
1000
600
400
200
0 ;-----l--t J I
0 5 30 2
Minutes
Responses to estrogen stimulation 833
1/ -----1-----1 I (4)
/ (4) I (4)
(4)/ P < .05 < .02 I
(3) (3) (3)
(3) I I I
6 12 18 24
Hours
Time After E2 Injection
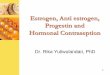
Fig. 1. Uterine cytosol estrogen receptor content (mean ± SEM) after intravenous estradiol injection (1 ILg/kg) in continuously anesthetized (e) and previously conscious (0) ewes. Numbers in parentheses indicate number of observations.
from 0.1 to 10 nmol ± 5 X 10~7 mol/L DES. The addition of DES is to correct for nonspecific binding. In the case of Scatchard analysis, the specific binding is defined as the total binding of receptors minus the nonspecific binding of receptors. The reactions were stopped with dextran-coated charcoal and analyzed by a computer program. IO
The assay of Katzenellenbogen et aI., which determined total binding in the cytosol, uses triplicates of 10 nmollL tritiated estradiol ± 10 x 1O~7 mollL DES. Cytosol was added to each vial and incubated for 1 hour at 00 C, then at 300 C for 18 hours. The reactions were then cooled to 00 C and stopped with dextran-coated charcoal. The calculations for the specific binding in this case were based on total binding minus nonspecific binding divided by the total protein concentration and reaction volume.
Nuclear binding assay. The nuclear fraction was assayed by the method described by Anderson et at. 7 The nuclear suspension was vigorously mixed on a vortex and 0.25 ml aliquots were transferred into two tubes containing 13 nmol/L tritiated estradiol and two tubes containing 13 nmol/L tritiated estradiol + 13 x 1O~7
mol/L estradiol. To each tube 0.25 ml of buffer was added and mixed on a vortex. These reactions were incubated in a 3T C shaking warm water bath for 1 hour. Then to remove any free steroid the reactions were washed three times with 1 ml of buffer A and centrifuged at 1000 x g for 10 minutes. The supernatant was discarded and the nuclear pellet resuspended in 1.0 ml of ethanol and incubated for 30 minutes at 300 C. Aliquots of 0.3 ml were taken from each tube and counted. The specific nuclear binding activity
Table I. Uterine cystosol estrogen distributions*
Hom location
Upper third Middle third Lower third
81-201
637 545 721
Ewe No.
*Femtomoles per milligram of protein.
81-202
1523 1664 1865
was calculated in femtomoles per gram of tissue and femtomoles per milligram of deoxyribonucleic acid (DNA)."
Results
Estrogen receptor responses. Cytosol estrogen receptor content in three different parts of the uterine horn were determined in two control ewes (group 1). These distributions are shown in Table I and indicate that receptor content in different areas of the ovine uterus is similar.
Uterine cytosol estrogen receptor responses were measured by analysis of specimens from timed biopsies during 18 hours in five anesthetized ewes (group 3). Complete results were obtained in only three ewes. Within 30 minutes of the estradiol bolus injection, cytosol estrogen receptor receptors decreased 57% from control, reached a nadir 75% below control levels after 2 hours, and stayed at this level for the remainder of the observation time (Fig. I, closed circles).
The time course of cytosol estrogen receptor replenishment in 10 ewes 2 to 10 days after prior operation and 6, 12, and 18 hours after estradiol injection are

834 Greiss et al.
'" 50 :::J (/) (/)
t= ci> E
'" 40 (5 E LL
0::
~ 30 8 o c. '" o £ 20 0::
'" '" e iii w
m 10 "0 :::J Z
'" 0::
I Mean±SEM
n=3
.~
5 OL5~--~3~0--7/)~-2~1---6~1--~1~~--~1~~--~1~~----(Min.) (Hrs.)
Time after E, Injection
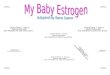
Fig. 2. Uterine nuclear estrogen receptor content after intravenous estradiol injection (I j.Lg/kg) in continuously anesthetized ewes.
also shown in Fig. 1 (open circles). The four assays at 24 hours were obtained 24 hours after a previous biopsy and estradiol injection.
Uterine nuclear estrogen receptor responses during 18 hours in three of the anesthetized ewes (group 3) are shown in Fig. 2. The nuclear estrogen receptor levels peaked 30 minutes after the estradiol injection and rapidly decreased to control levels within 6 hours.
Uterine blood flow responses. In four of the five ewes monitored before and during uterine biopsies while under anesthesia (group 3), the typical uterine blood flow response after estradiol occurred. However, the magnitude of the response was markedly reduced and achieved less than 50% of that evoked 24 hours earlier in the conscious state. In the one ewe in which no uterine blood flow response occurred, the cytosol estrogen receptor responses were similar to those in the other ewes.
During daily recordings of uterine blood flow re
sponses before and 24 hours after uterine biopsies in ewes in group 2, it was noted that peak uterine blood flow levels were approximately the same as those observed during the days preceding the biopsy. These are shown in Table II.
Eighty-six regimens of bolus doses of estradiol at varying hourly frequencies were administered to nine ewes. Composite uterine blood flow responses at 1-, 2-, 3-, 4-, and 6-hour dose frequencies are illustrated in Fig. 3. Panell shows the uterine blood flow response during hourly estradiol doses during 8 hours and the control response after 24 hours. Except for a more
April, 1986 Am J Obstet Gynecol
Table II. Postoperative uterine blood flow responses to estradiol after preoperative estradiol stabilization
Ewe No.
84-109 84-110
84-100
Range of preoperative responses*
80-105 89-100 89-100 83-107 83-107
24 hr postoperative response*
83 89 92 94 86
*Maximum uterine blood flow (milliliters per minute).
gradual descent of uterine blood flow from peak levels, the hourly dose response was similar to the 24-hour one. When estradiol was administered every 2 hours (paneI2, Fig. 3), the maximum response was reachieved I hour after the second dose but further doses only muted the waning response or caused a minimal uterine blood flow increase. Administrations every 3 hours (panel 3, Fig. 3) caused muted uterine blood flow increases 1 to 1 Y2 hours later but failed to alter the progressive descent from the maximum uterine blood flow levels induced by the first dose. When estradiol was administered every 4 hours (panel 4, Fig. 3), peak flow rates recurred transiently after the second dose but only a muted rise occurred after the third dose. It was not until estradiol was administered every 6 hours (panel
5, Fig. 3) that uterine blood flow peaks equal to those induced by the first dose could be reinduced regularly. However, the duration of the peak responses was shorter and the rate of uterine blood flow descent from peak levels was more rapid than after the first dose.
The uterine blood flow rates after estradiol injections timed 6, 8, 10, 12, 14, 16, 18, and 24 hours after the previous injection are illustrated in Fig. 4. As the estradiol dose interval increased, the rate of uterine blood flow descent from peak levels became slower and the sustained uterine blood flow rate between 1.5 and 2 hours reappeared. At the 18-hour dose frequency, although the uterine blood flow rates after 4 hours were slightly lower than the 24-hour ones, they were not significantly different whereas those at dose frequencies between 6 and 16 hours were different (p < 0.02).
Comment Current steroid response theory indicates that a
given response is dependent on the quantity of steroid exposed to a cell and the concentration of steroid-specific macromolecule receptors present in the cytosol of target cells. Upon formation of the steroid-receptor complex, it is translocated to the cell nucleus (nuclear receptor) where transcriptional events begin the process of effecting the various actions of the steroid. Since the initial concentration of cytosol receptor controls the

Volume 154 Number 4
" '" c: o a. '" " a: u. <D :::> E " E 'x .. ::< '0
n=9
n=9
16
Hours aiter Initial E, Injection
Fig. 3. Uterine blood flow responses after intravenous estradiol injections (I I1g/kg) ( t ) at different injection frequencies. Upper panel compares 24-hour dose frequency (solid line) with hourly dose frequencies (0' and 0----0).
nuclear receptor, a depletion of cytosol receptor will occur with translocation and the process of cytosol receptor replenishment must occur. Until a sufficient amount of cytosol receptor is replenished, the steroidinduced response will be blunted or erased depending on the degree of cytosol receptor depletion induced by the dose of administered steroid. This highly simplified description of a complex process provides the basis for using a continuously monitorable response to estradiol stimulation, uterine vasodilatation, to identify critical times for uterine biopsies for cytosol estrogen receptor assay and possibly to permit the response itself to give insight into cytosol estrogen receptor replenishment. We appreciated at the outset that cytosol estrogen receptor and nuclear estrogen receptor responses of samples of entire uterine tissues may not reflect those of the uterine vasculature but felt that such responses in the light of uterine blood flow changes may complement interpretation of responses. Since cytosol estrogen receptor contents were similar in different parts of the uterine horn, we felt that multiple biopsies from differing parts of the horn provided valid data for com
parison. It is clear from Fig. 1 that the intravenous dose of
estradiol necessary to evoke maximal uterine vasodilatation uses only 75% of available total uterine cytosol estrogen receptor. The uterine blood flow responses during injections of estradiol every hour and every 2 hours (Fig. 3) suggest that similar incomplete depletions in the cytosol estrogen receptor of the uterine vasculature occur; that is, since the period of maximal
Responses to estrogen stimulation 835
100
90
80
" '" 70 c: 0 a. '" " 60 a: u. f n <D :::> 50 E 24 8
" E 'x .. 40 6 ::< 6 '0 30 6 'if. 6
9 20 6 ....•
8 6
10
0 1.5 2.0 2.5 3.0 3.5 4.0
Hours aiter E, Injection
Fig. 4. Uterine blood flow responses after intravenous estradiol injections (I I1g/kg) at dose frequencies (f) between 6 and 24 hours. All of the responses at 4.0 hours are different from the 24-hour response (p < 0.02) except that after 18 hours.
dilatation can be prolonged or regained during the time of maximal initial depletion of cytosol estrogen receptor, it is likely that such responses are mediated by residual cytosol estrogen receptor. It would follow that recurrent uterine blood flow elevations after estradiol injections given 3, 4, and 6 hours after the initial injection would reflect the sum of residual and replenished cytosol estrogen receptor. In conscious unstressed ewes, cytosol estrogen receptor replenishment occurred within 12 hours of estradiol administration. These results are consistent with those reported in rat uteri by Clark and Peck. 12 However, the uterine blood flow responses suggest that cytosol estrogen receptor replenishment in the uterine vasculature proceeds at a slower pace than that in the uterus as a whole. For example, repetitive uterine blood flow peak flows could not be induced by estradiol until 6 hours after the preceding estradiol injection, a time when total uterine cytosol estrogen receptor replenishment was 39% of control. However, these peak flows were dissimilar from 24-hour controls in that the duration of the response was much shorter. This led us to look at the vasodilatory response from two aspects, its absolute magnitude and its magnitude over time. Methodologic limitations dictated the 4-hour observation period. Since duplication of uterine blood flow levels observed 24 hours after a preceding estradiol injection required an I8-hour interval, we have interpreted this to indicate that vascular cytosol estrogen receptor replenishment sufficient to duplicate control levels requires at least 18 hours. A longer time to full replenishment cannot be

836 Greiss et al.
excluded, however, SInce the control response was achieved presumably with < 100% of available cytosol estrogen receptor.
Investigators in this area have observed regularly that in animals under anesthesia, the estradiol vasodilatory response is muted and that after initial oophorectomy and flow probe implantation in ewes previously untreated with estradiol, at least 3 to 4 days of daily injections of estradiol is required to evoke a maximum repetitive uterine blood flow response. Anecdotally, both observations have been attributed to operative stress. This might be a function of operative and postoperative physiologic responses not only of the cardiovascular system but of estrogen receptor function as well. The present observations give possible insight into the explanations for these responses. Clearly, operative stress (anesthesia and operation) exerts immediate effects. In every case, the magnitude of the uterine blood flow response was blunted in comparison with responses in conscious unstressed animals and cytosol estrogen receptor replenishment did not occur (Fig. 1). Alternately uterine nuclear estrogen receptor responses were similar to those previously reported in rats. 12 Since cytosol estrogen receptor replenishment was obviously altered, it is possible that, although receptor translocation occurred normally, posttranslocational events were similarly compromised. Such an interpretation is supported by the observations of Lippe and Szego,13 who determined that the suppressive effect of actinomycin D on estrogen-induced uterine water imbibition is mediated by adrenocortical hyperactivity.
Twenty-four hours after uterine horn biopsy, cytosol estrogen receptor replenishment was apparently complete and when repetitive daily estradiol responses had been achieved before operation, uterine blood flow responses 24 hours later approximated the preoperative ones (Table II). We believe that uterine horn biopsy is at least as stressful as oophorectomy and implantation of a flow probe on the middle uterine artery. If this is true, then the initial low uterine blood flow levels observed after the latter procedure cannot be attributed to a prolonged effect on uterine estrogen receptor metabolism. Rather it would appear that late uterotropic responses (cellular hypertrophy and hyperplasia) permit a progressively greater uterine blood flow response to daily estradiol stimulation that would appear to maximize after 4 to 7 days.
The results presented herein further clarify events of the estradiol-induced vasodilatory response of the ovine uterus. Since most investigators of the estradiolinduced uterotropic responses address themselves to early and late metabolic and biosynthetic responses, we hoped that a continuously monitorable response might improve our understanding in this area. The observed
April, 1986 Am J Obstet Gynecol
results are consistent with known steroid-receptor interaction theory but the significance of the observations is only speculative because me tho do logic limitations preclude actual measurement of cytosol estrogen receptor and nuclear estrogen receptor in the uterine vasculature.
REFERENCES
1. Killam AP, Rosenfeld CR, Battaglia FC, Makowski EL, Meschia G. Effect of estrogen on the uterine blood flow of oophorectomized ewes. AM J OBSTET GYNECOL 1973; 115:1045.
2. Still JG, Greiss FC Jr. Effect of cis- and trans-clomiphene on the uterine blood flow of oophorectomized ewes. Gynecol Invest 1976;7:187.
3. Clewell WH, Stys S, Meschia G. Stimulus summation and tachyphylaxis in estrogen responses in sheep. AM J OBSTET GYNECOL 1980;138:485.
4. Greiss FC J r, Anderson SG. Uterine vascular changes during the ovarian cycle. AM J OBSTET GYNECOL 1969; 103:629.
5. Greiss FC Jr. A mechanical zero reference for implanted flowmeter systems. J Appl Physiol 1962; 17: 177.
6. Greiss FC Jr. The uterine vascular bed: effect of adrenergic drug stimulation. Obstet Gynecol 1963;21 :295.
7. AndersonJ, ClarkJH, Peck EJ Jr. Oestrogen and nuclear binding sites. Determination of specific sites by 'H-oestradiol exchange. J Biochem 1972; 126:561.
8. Scatchard G. The attraction of proteins for small molecules and ions. Ann NY Acad Sci 1949;51 :660.
9. Katzenellenbogen JA, Johnson HJ, Carlson KE. Studies on the uterine cytoplasmic estrogen binding protein. Thermal stability and ligand-dissociation rate. An assay of empty and filled sites by exchange. Biochemistry 1972; 12:4092.
10. Kute TE, Huske MS, Shore A, Rhyne AL. Improvements in steroid receptor assay including rapid computer analysis of data. Anal Biochem 1980;103:272.
11. Cesarone CF, Bolognesi C, Sonti L. Improved microfluorometric DNA determination in biological materials using 33258 Hoechst. Anal Biochem 1979;100:188.
12. ClarkJH, Peck EJ Jr. Female sex steroids, receptors and function. Berlin: Springer-Verlag, 1979: 100.
13. Lippe BM, Szego CM. Participation of adrenocortical hyperactivity in the suppressive effect of actinomycin-D on uterine stimulation by oestrogen. Nature 1965;207 :272.
Discussion DR. EDGAR L. MAKOWSKI, Denver, Colorado. Since
the observation by Markee l that uterine blood vessels become dilated after the administration of estrogens, many investigators have been interested in the steroid stimulus-uterine response relationship. In the current study by Greiss and his associates, this relationship was investigated in nonpregnant, oophorectomized sheep by monitoring uterine blood flow and uterine cytosol and nuclear receptors during estradiol-induced vasodilatation. Changes in uterine blood flow were determined by electromagnetic flow probes, and alterations of uterine receptors (cystosol and nuclear) were interpreted according to the classical "two-step" biochemical model of intracellular hormonal interaction.2 This model hypothesizes that the steroid binds with a soluble receptor in the cytoplasm of target cells. The receptorhormone complex is then translocated to the nucleus











![Study of Estrogen Receptor, Progesterone Receptor, …...[CANCER RESEARCH 49,4298-4304, August 1. 1989] Study of Estrogen Receptor, Progesterone Receptor, and the Estrogen-regulated](https://img.pdfslide.us/doc/110x75/5f95792bbdbd5e0915333803/study-of-estrogen-receptor-progesterone-receptor-cancer-research-494298-4304.jpg)