Embed Size (px)
Citation preview
TEM FOR EARLY RECTAL CANCER
M. MorinoDigestive, Colorectal and Minimal
Invasive SurgeryUniversity of Torino - Italy
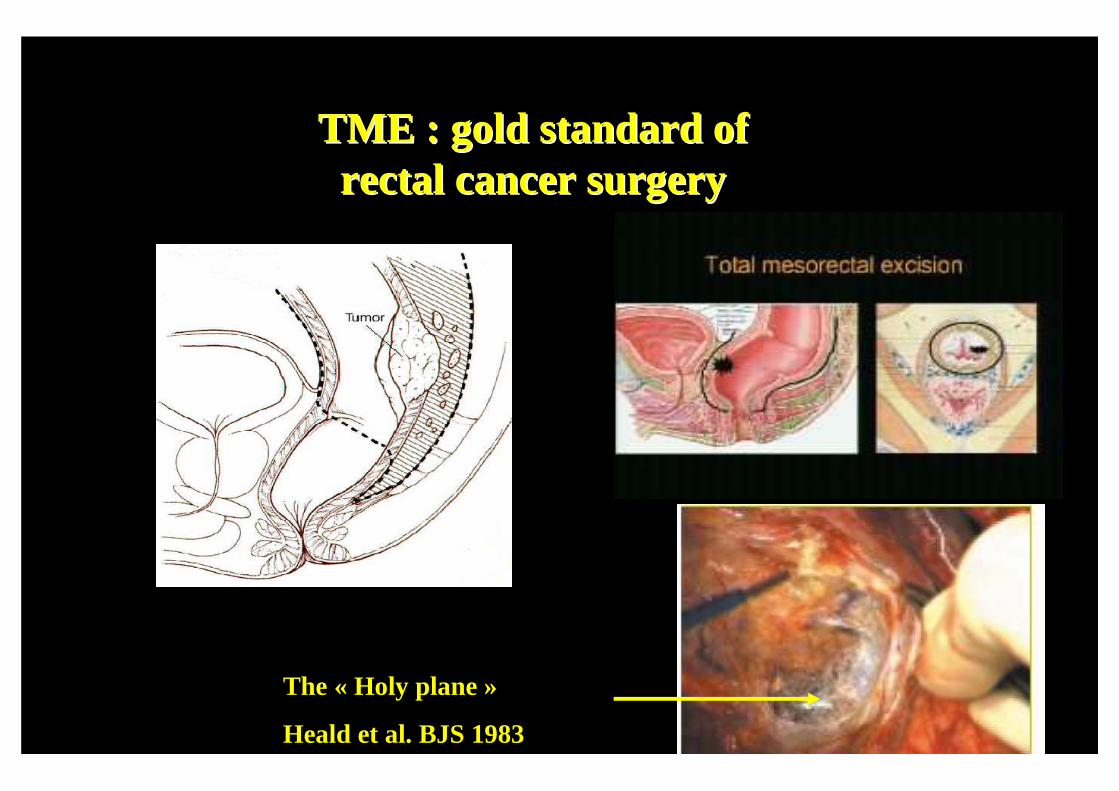
TME : gold standard ofTME : gold standard ofrectal cancer rectal cancer surgerysurgery
The « Holy plane »
Heald et al. BJS 1983
TME for rectal cancer:Literature Review 2000-10
• MORTALITY 2-7%
• MORBIDITY 26-53%
• TEMPORARY STOMA 50-100%
• DEFINITIVE STOMA 5-30%
• SEXUAL DYSFUNCTIONS 10-52%
• URINARY DISFUNCTIONS 5-27%
22
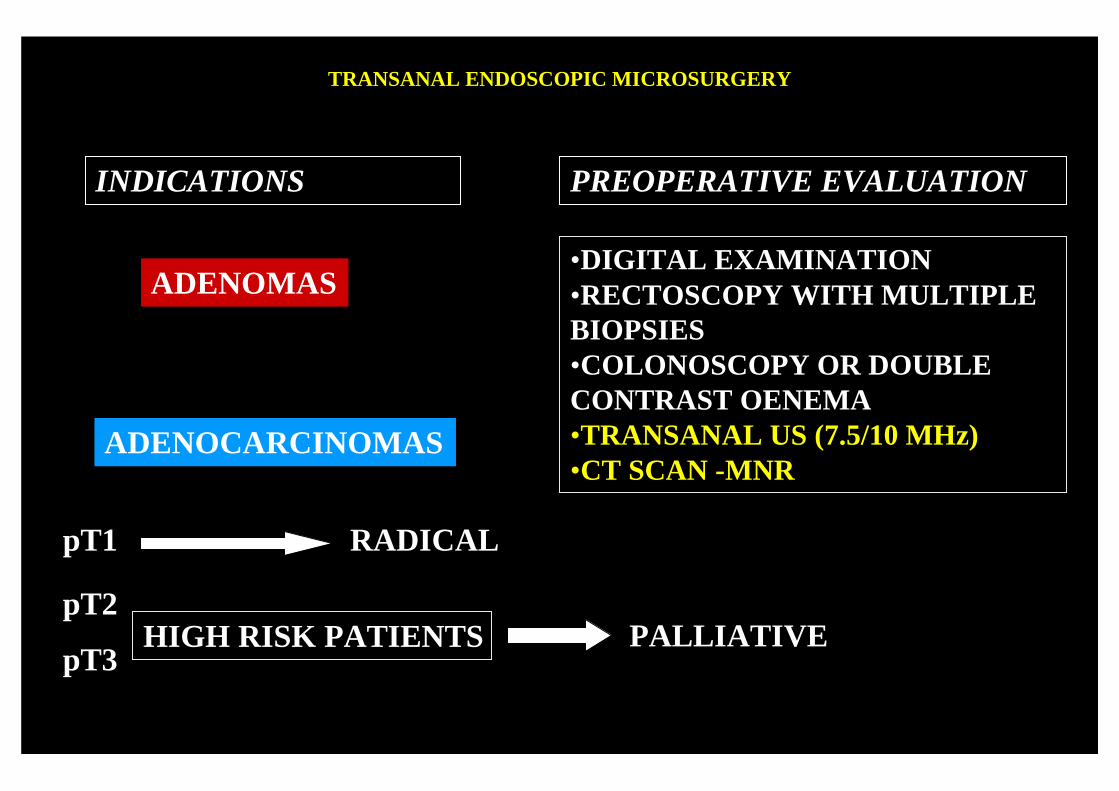
TRANSANAL ENDOSCOPIC MICROSURGERY
•DIGITAL EXAMINATION•RECTOSCOPY WITH MULTIPLE BIOPSIES•COLONOSCOPY OR DOUBLECONTRAST OENEMA•TRANSANAL US (7.5/10 MHz)•CT SCAN -MNR
PREOPERATIVE EVALUATIONINDICATIONS
ADENOMAS
ADENOCARCINOMAS
pT1 RADICAL
pT2
pT3HIGH RISK PATIENTS PALLIATIVE
Dis Colon Rectum 2009; 52: 1831-1836
Surgical Endoscopy 2011; published online 7 june
Risk factors for recurrence after TEM for rectal malignantneoplasm.M.Morino, M.Allaix, M.Caldart, G.Scozzari, A.Arezzo
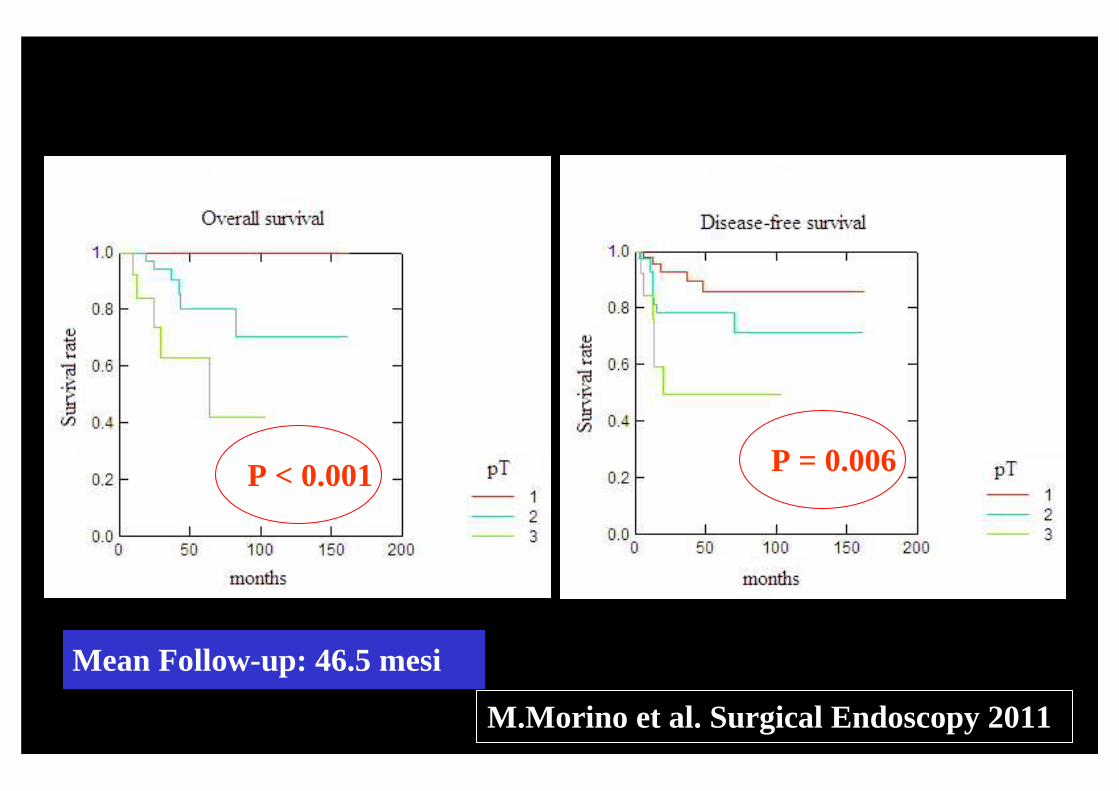
Mean Follow-up: 46.5 mesi
P < 0.001 P = 0.006
M.Morino et al. Surgical Endoscopy 2011
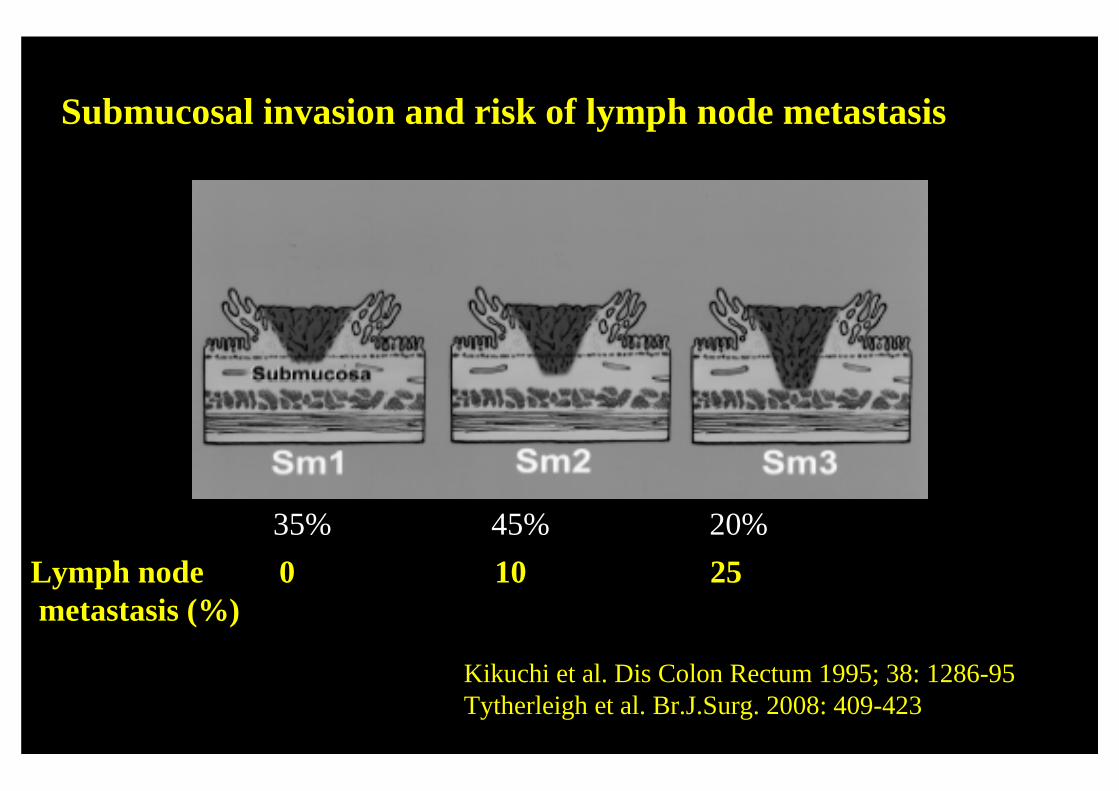
35% 45% 20%
Lymph nodemetastasis (%)
0 10 25
Submucosal invasion and risk of lymph node metastasis
Kikuchi et al. Dis Colon Rectum 1995; 38: 1286-95Tytherleigh et al. Br.J.Surg. 2008: 409-423
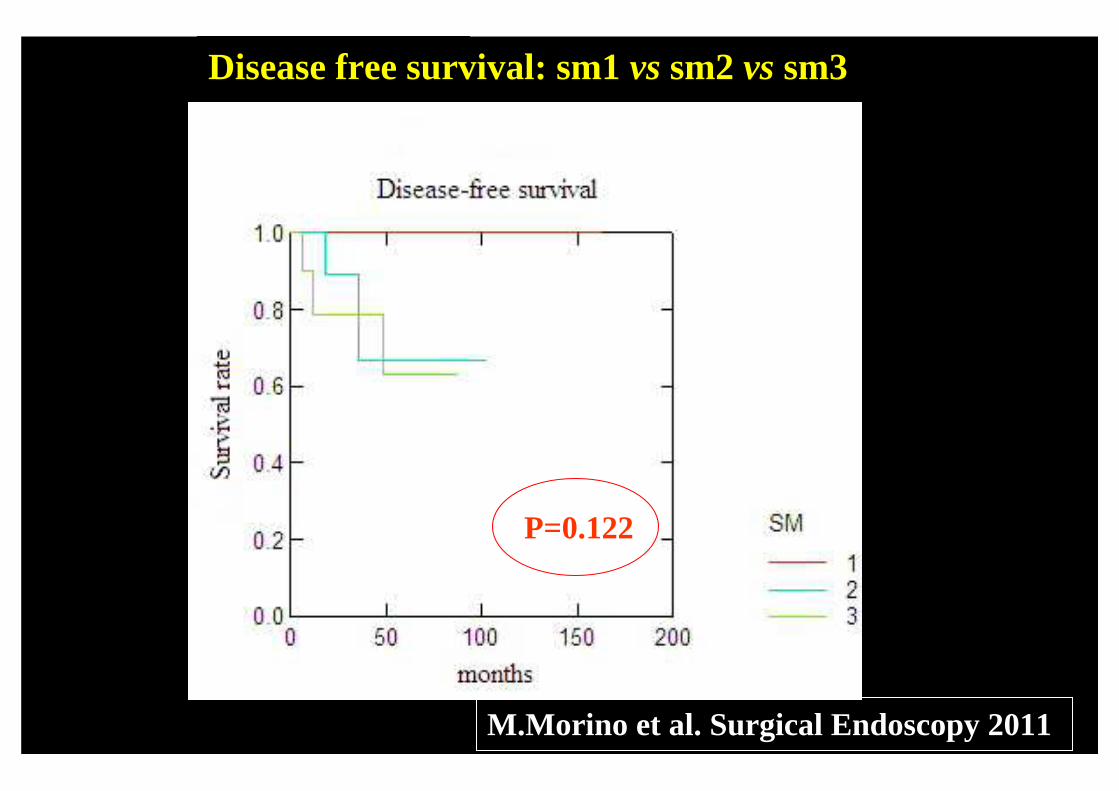
Disease free survival: sm1 vs sm2 vs sm3
P=0.122
M.Morino et al. Surgical Endoscopy 2011
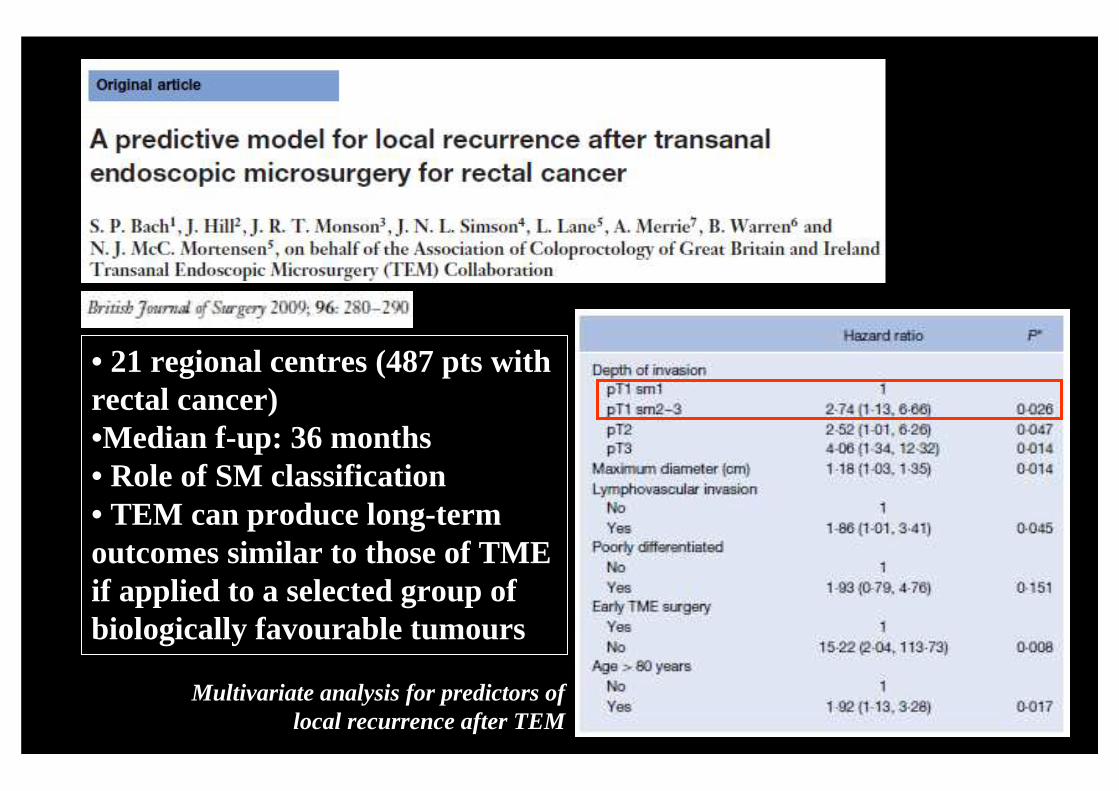
• 21 regional centres (487 pts withrectal cancer)•Median f-up: 36 months• Role of SM classification• TEM can produce long-termoutcomes similar to those of TME if applied to a selected group ofbiologically favourable tumours
Multivariate analysis for predictors oflocal recurrence after TEM
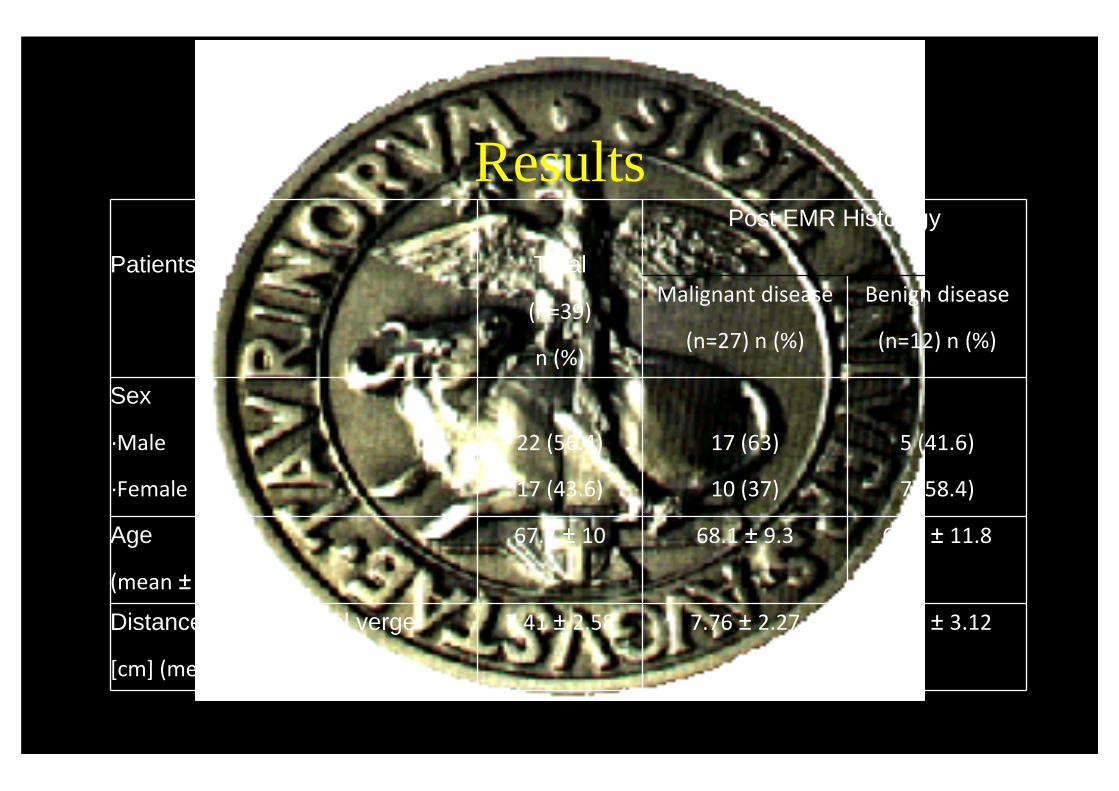
Results
Patients Total
(n=39)
n (%)
Post EMR Histology
Malignant disease
(n=27) n (%)
Benign disease
(n=12) n (%)
Sex
·Male
·Female
22 (56.4)
17 (43.6)
17 (63)
10 (37)
5 (41.6)
7 (58.4)
Age
(mean ± DS)
67.7 ± 10 68.1 ± 9.3 66.8 ± 11.8
Distance from the anal verge
[cm] (mean ± DS)
7.41 ± 2.58 7.76 ± 2.27 6.63 ± 3.12
Results

ResultsMean operative time 64.2 +/- 31.2 min (range 25-150)
Peritoneal opening 1/39 (2.7%)
Conversion rate 0/39
Diverting stoma 0/39
Blood transfusions 0/39
30 days mortality 0/39
30 days morbidity 1/39 (2.7%)Grade IIIa: rectal bleedingEndoscopic clip positioning
Mean post operative stay 4.1 +/- 1.2 days (range 2-7)
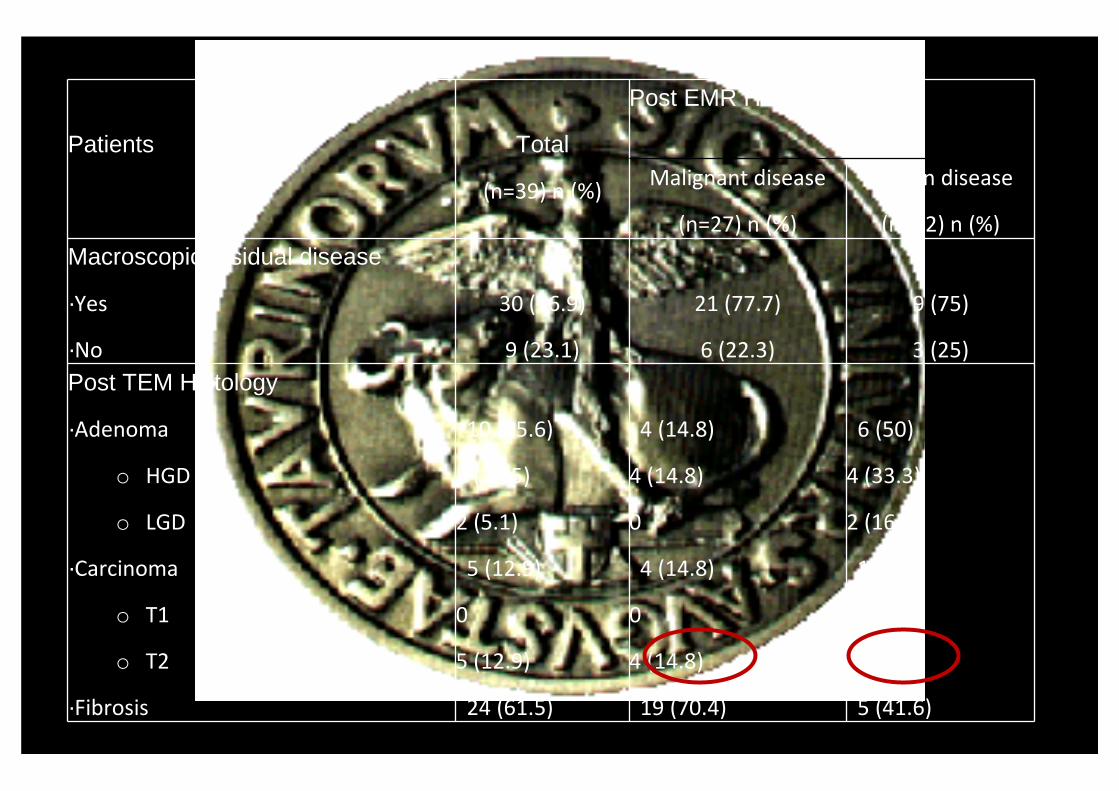
Patients Total
(n=39) n (%)
Post EMR Histology
Malignant disease
(n=27) n (%)
Benign disease
(n=12) n (%)
Macroscopic residual disease
·Yes
·No
30 (76.9)
9 (23.1)
21 (77.7)
6 (22.3)
9 (75)
3 (25)
Post TEM Histology
·Adenoma
o HGD
o LGD
·Carcinoma
o T1
o T2
·Fibrosis
10 (25.6)
8 (20.5)
2 (5.1)
5 (12.9)
0
5 (12.9)
24 (61.5)
4 (14.8)
4 (14.8)
0
4 (14.8)
0
4 (14.8)
19 (70.4)
6 (50)
4 (33.3)
2 (16.7)
1 (8.4)
0
1 (8.4)
5 (41.6)
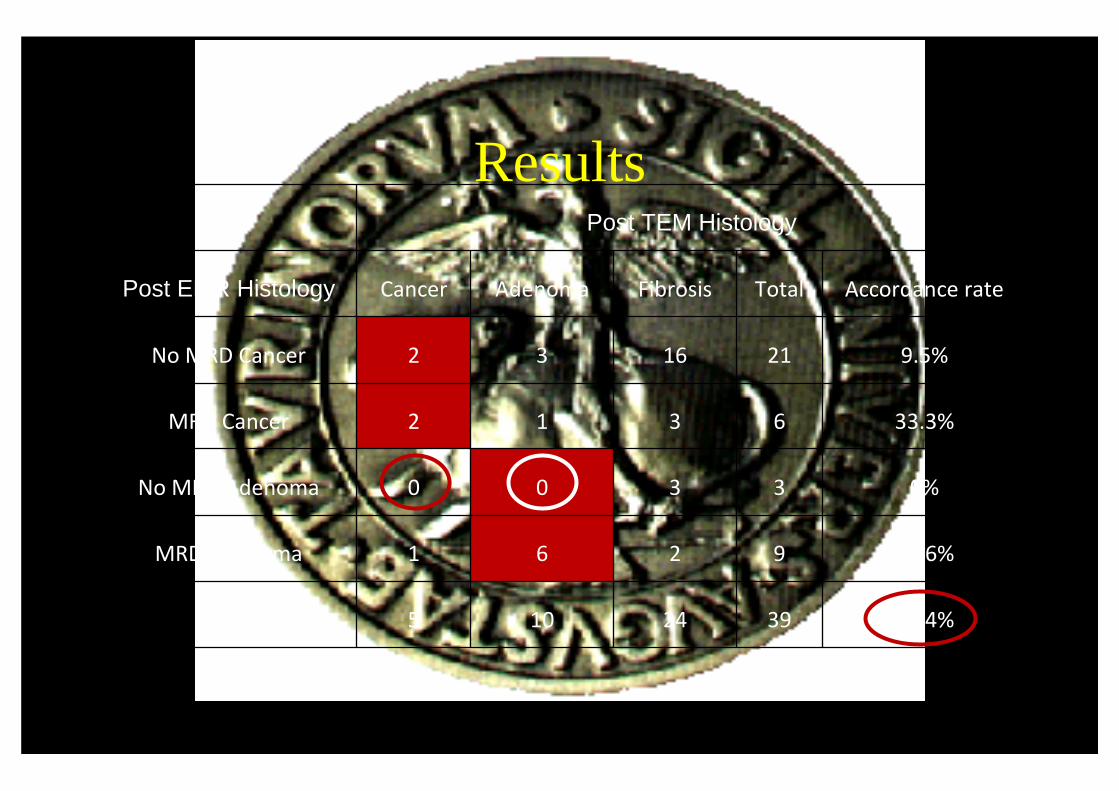
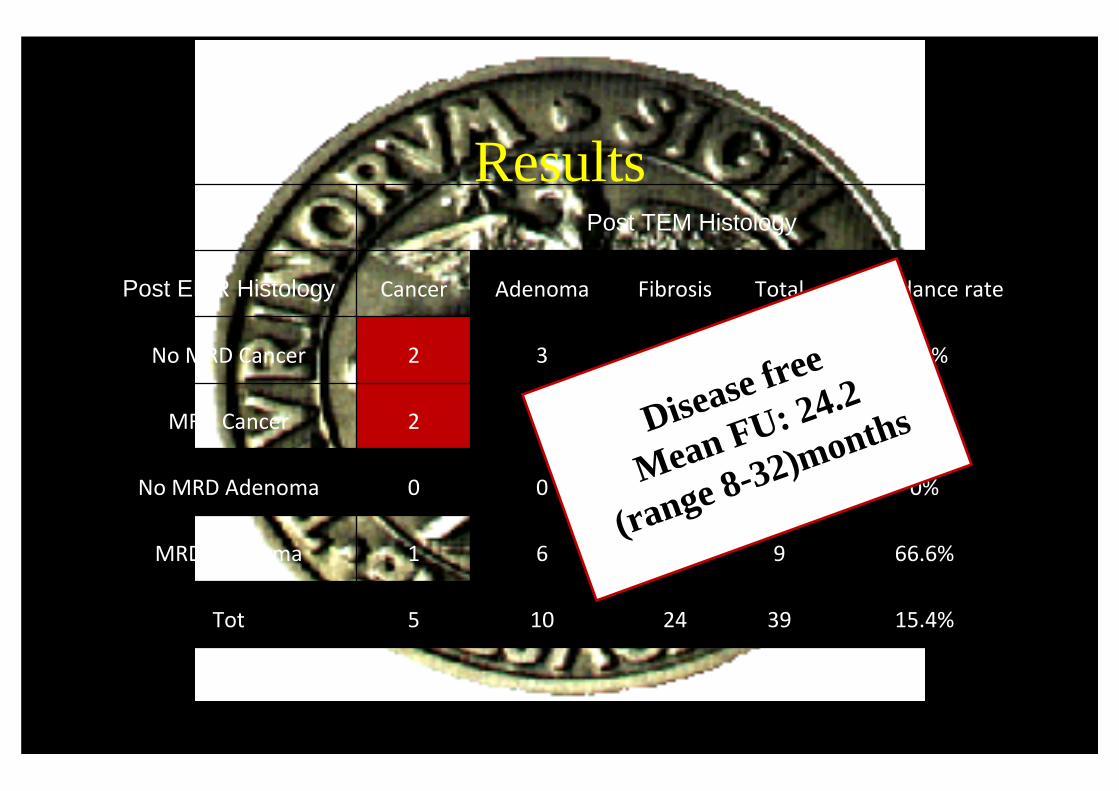
ResultsPost TEM Histology
Post EMR Histology Cancer Adenoma Fibrosis Total Accordance rate
No MRD Cancer 2 3 16 21 9.5%
MRD Cancer 2 1 3 6 33.3%
No MRD Adenoma 0 0 3 3 0%
MRD Adenoma 1 6 2 9 66.6%
Tot 5 10 24 39 15.4%
ResultsPost TEM Histology
Post EMR Histology Cancer Adenoma Fibrosis Total Accordance rate
No MRD Cancer 2 3 16 21 9.5%
MRD Cancer 2 1 3 6 33.3%
No MRD Adenoma 0 0 3 3 0%
MRD Adenoma 1 6 2 9 66.6%
Tot 5 10 24 39 15.4%
Disease free
Mean FU: 24.2
(range 8-32)months
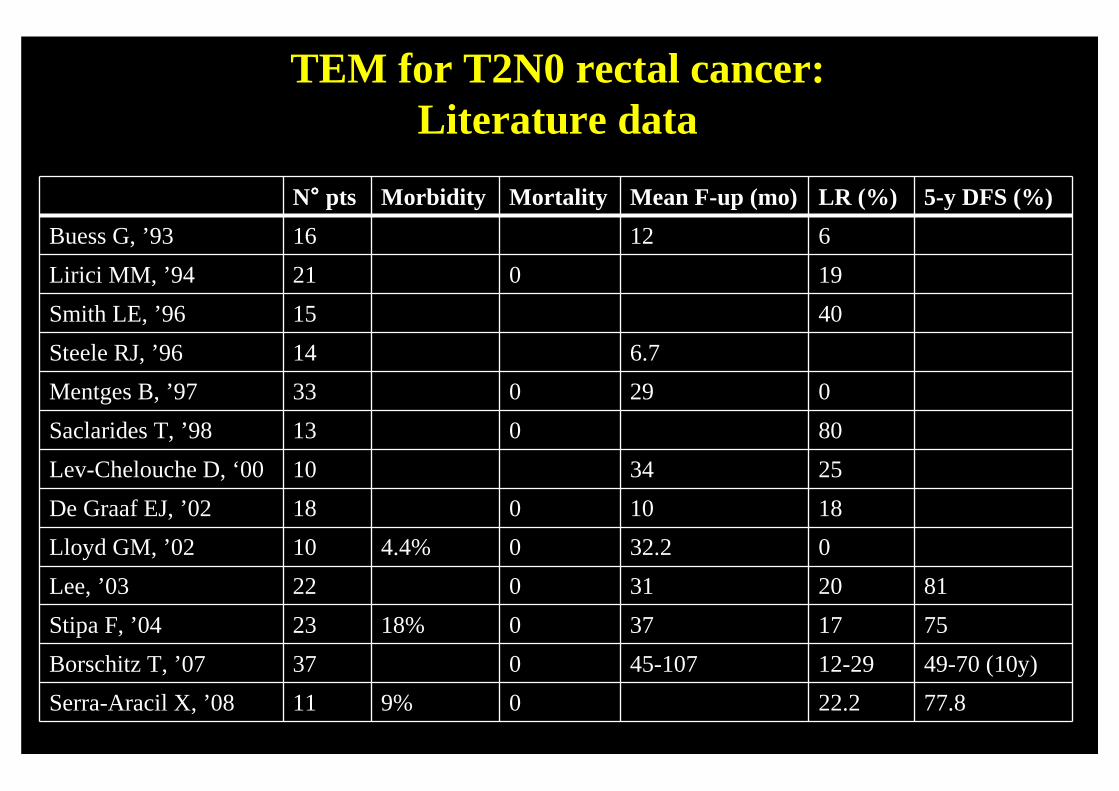
TEM for T2N0 rectal cancer: Literature data
N°°°° pts Morbidity Mortality Mean F-up (mo) LR (%) 5-y DFS (%)
Buess G, ’93 16 12 6
Lirici MM, ’94 21 0 19
Smith LE, ’96 15 40
Steele RJ, ’96 14 6.7
Mentges B, ’97 33 0 29 0
Saclarides T, ’98 13 0 80
Lev-Chelouche D, ‘00 10 34 25
De Graaf EJ, ’02 18 0 10 18
Lloyd GM, ’02 10 4.4% 0 32.2 0
Lee, ’03 22 0 31 20 81
Stipa F, ’04 23 18% 0 37 17 75
Borschitz T, ’07 37 0 45-107 12-29 49-70 (10y)
Serra-Aracil X, ’08 11 9% 0 22.2 77.8
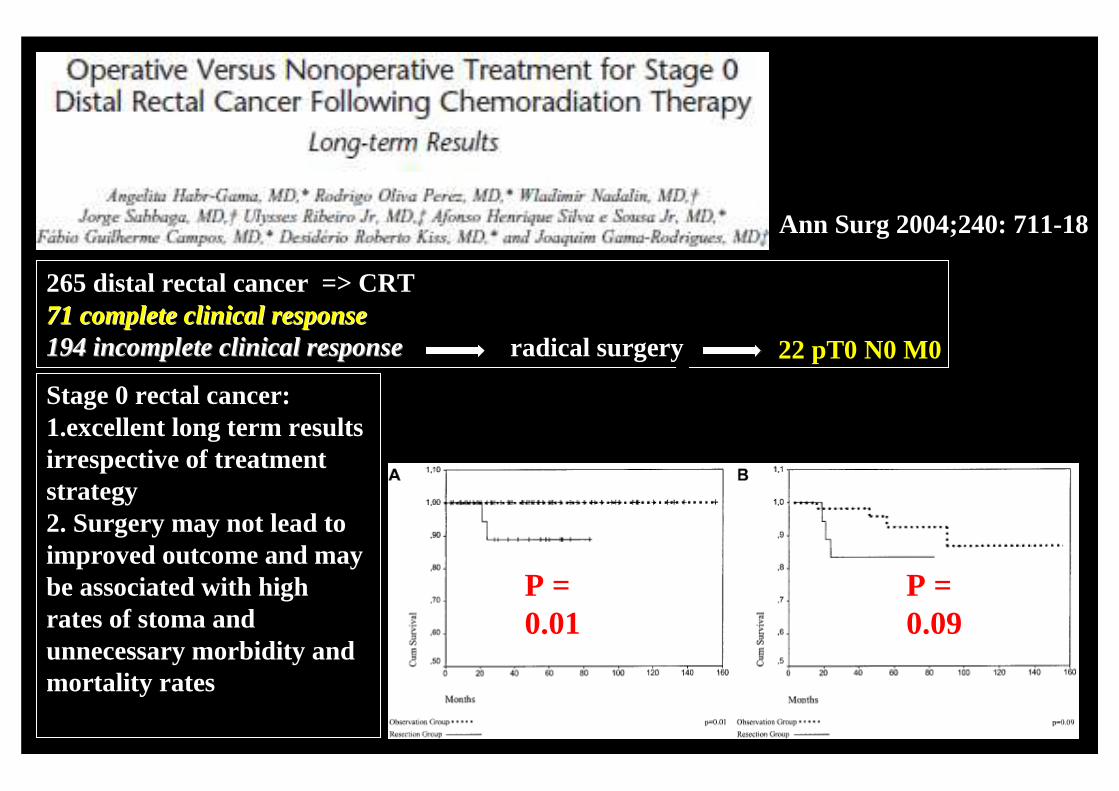
Ann Surg 2004;240: 711-18
P = 0.01
P = 0.09
265 distal rectal cancer => CRT71 complete 71 complete clinicalclinical responseresponse194 incomplete 194 incomplete clinicalclinical responseresponse
7radical surgery 22 pT0 N0 M0
Stage 0 rectal cancer:1.excellent long term resultsirrespective of treatment strategy2. Surgery may not lead toimproved outcome and maybe associated with high rates of stoma and unnecessary morbidity and mortality rates
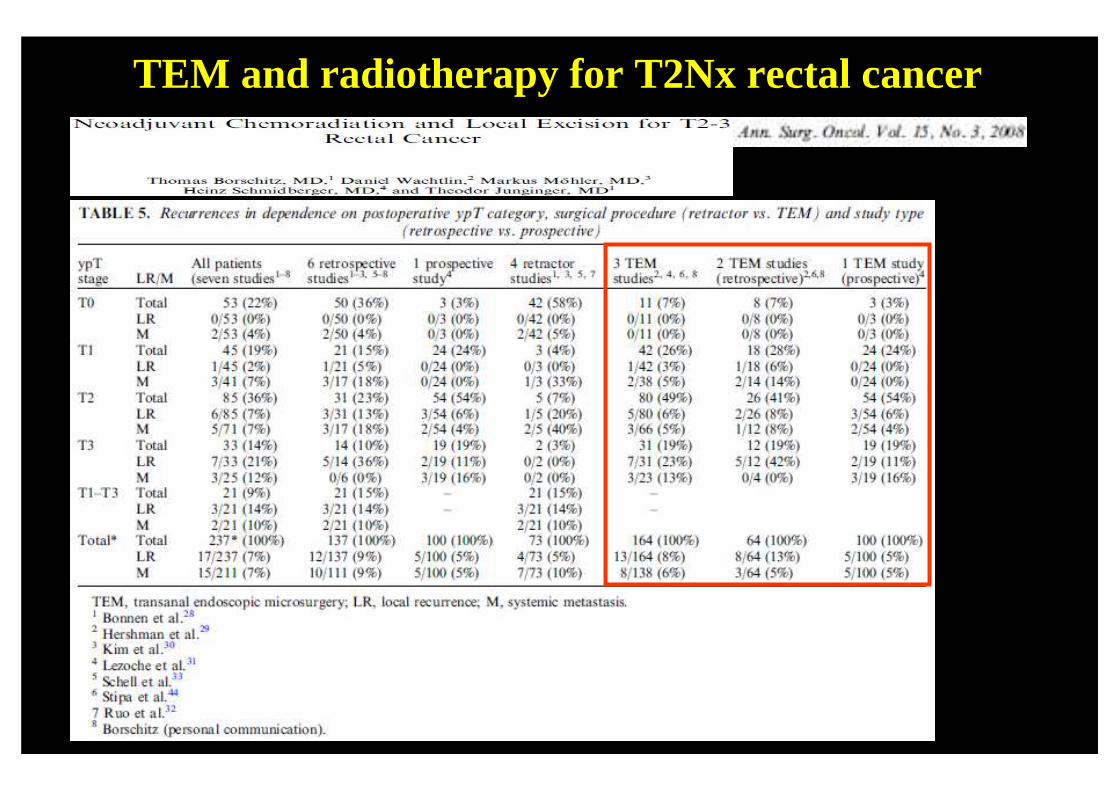
TEM and radiotherapy for T2Nx rectal cancer
TEM and preop radiotherapy forT2Nx rectal cancer
Surg Endosc. 2010 Oct 7. [Epub ahead of print]
Prospective study84 T2N0M0Median operative: 95 (65-120) min Minor complications: 9%Major complications: 1.5% (1 ileostomy for perianal phlegmon)Median follow-up: 97 (55-193) months
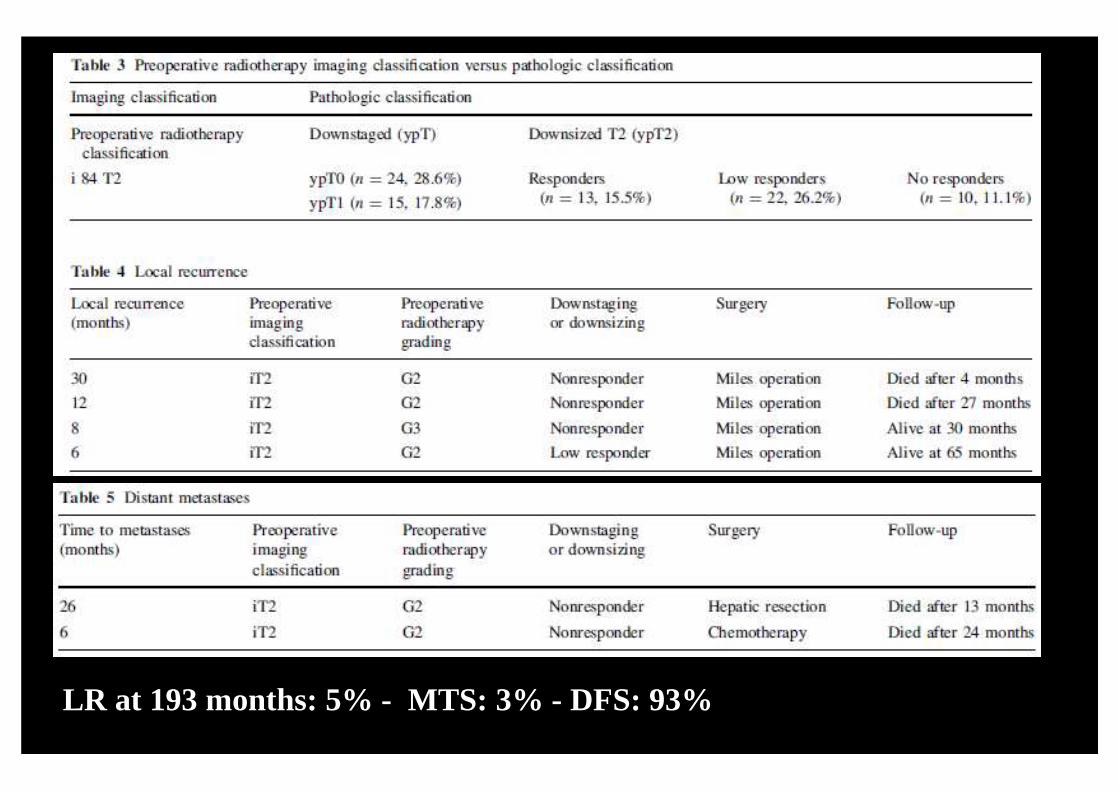
LR at 193 months: 5% - MTS: 3% - DFS: 93%
TEM and radiotherapy for T2Nx rectal cancer
RCT35 TME vs 35 TEMMedian follow-up: 84 (72-96) min LR TEM 5.7% vsvs LR TME: 2.8%MTS TEM 2.8% vsvs 2.8%DFS: 94% vsvs 94%
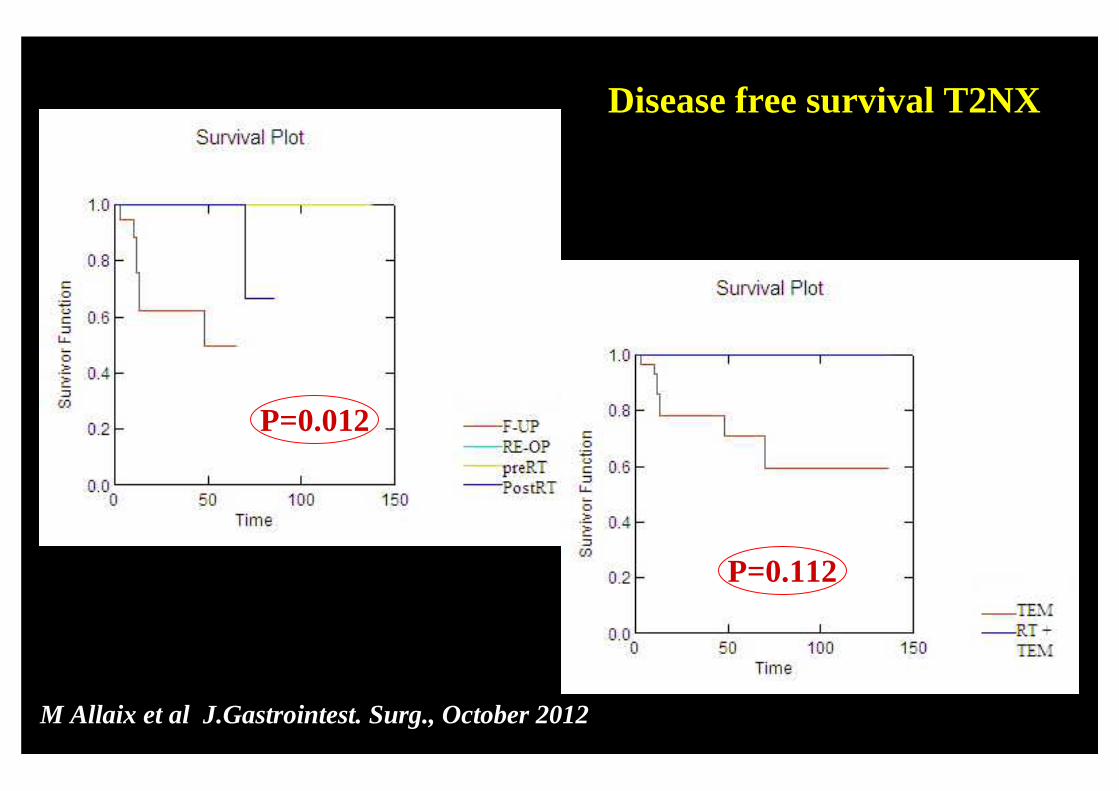
P=0.012
P=0.112
JM Allaix et al J.Gastrointest. Surg., October 2012
Disease free survival T2NX
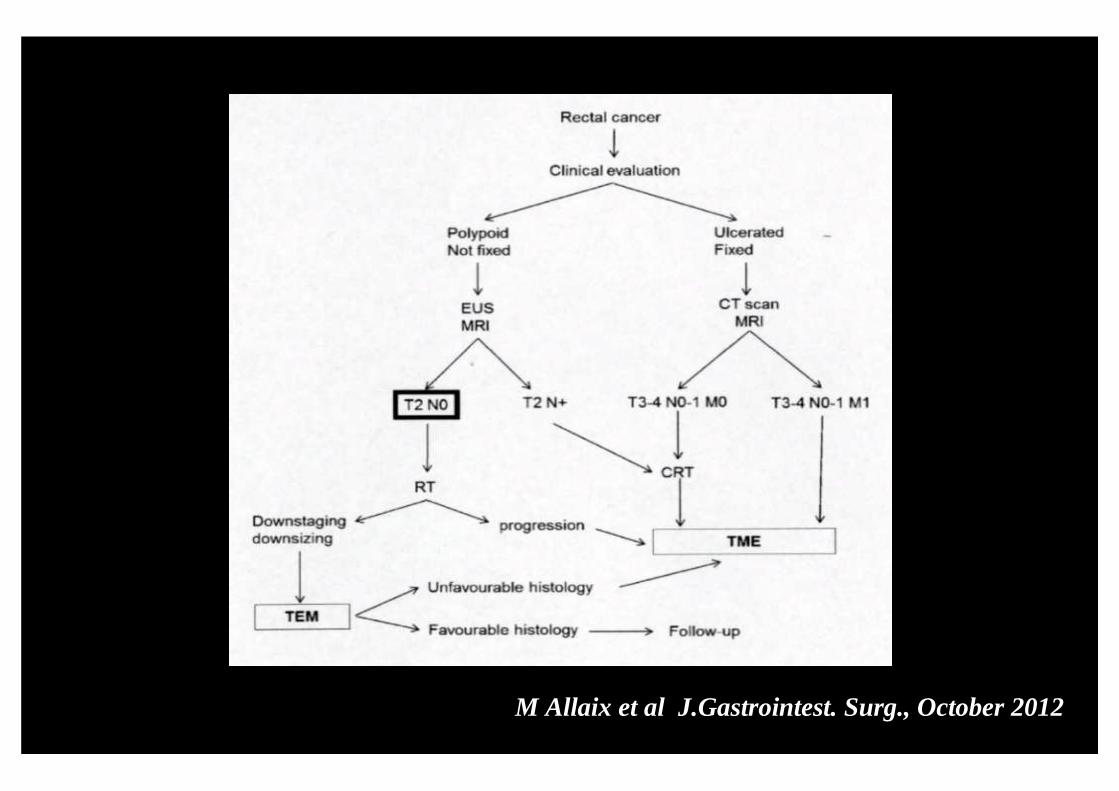
JM Allaix et al J.Gastrointest. Surg., October 2012
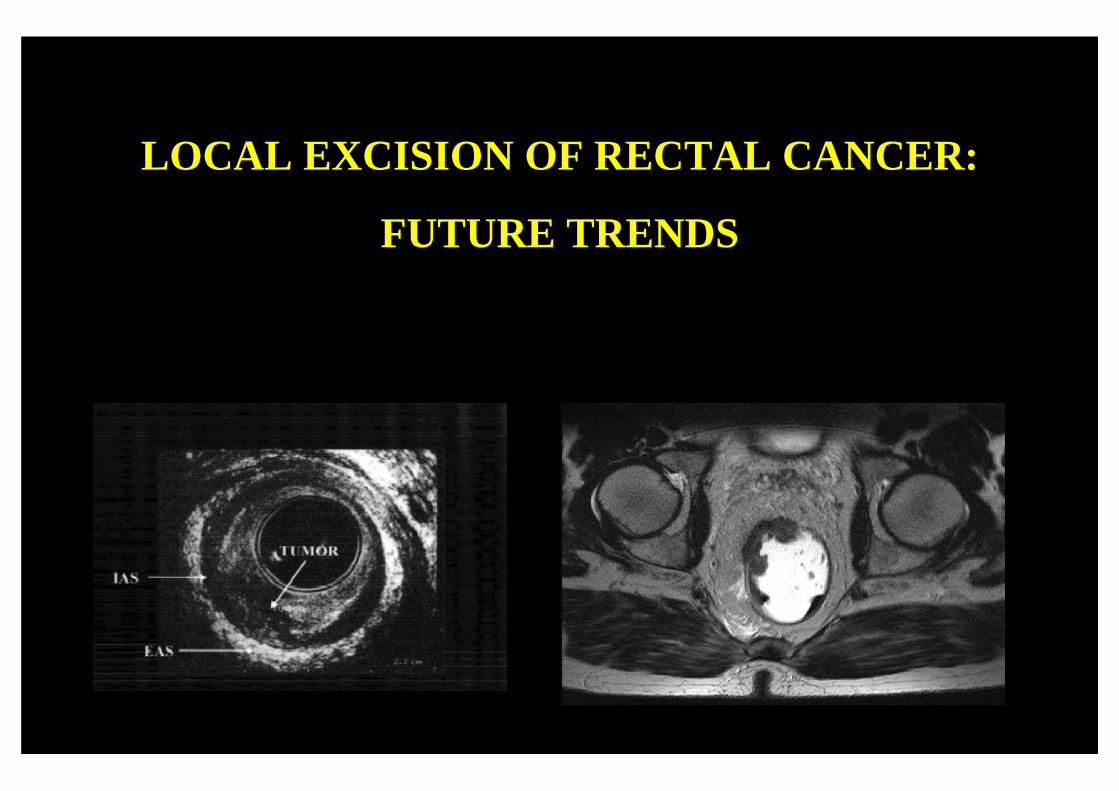
LOCAL EXCISION OF RECTAL CANCER:
FUTURE TRENDS
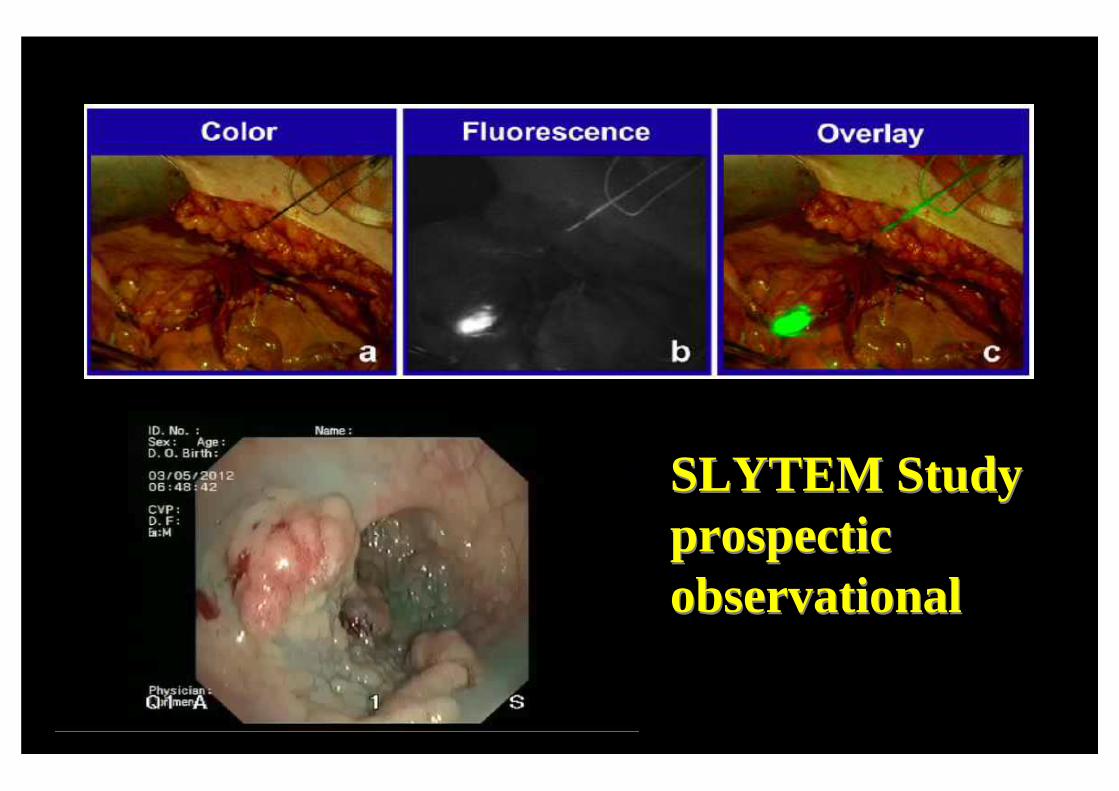
SLYTEM Studyprospecticobservational
SLYTEM Studyprospecticobservational
SLYTEM Studyprospecticobservational
SLYTEM Studyprospecticobservational
CONSENSUS CONFERENCE:EARLY RECTAL CANCER
Aim
To assess the the resultsof TEM after incompleteendoscopic polypectomyin terms of residual disease,recurrence and need offurther surgery
Methods• TEM within 3 months after endoscopic polypectomy
– Partial polypectomy(Confirmed by rigid rectal endoscopy and multiple biopsies)
– Complete endoscopic resection(Malignant polyps or HGD adenomas)
• Preoperative assessment– Rectal digital examination
– Rigid rectal endoscopy
– Complete colonoscopy
– Endorectal UltraSonography (EUS)
• Full thickness TEM
MethodsPost TEM histology
– locally advanced rectal cancer → TME
– no residual malignant disease or pT1sm1 → FU
• clinical examination• flexible rectal endoscopy• neoplastic markers
Every 3 monthsfor 2 years
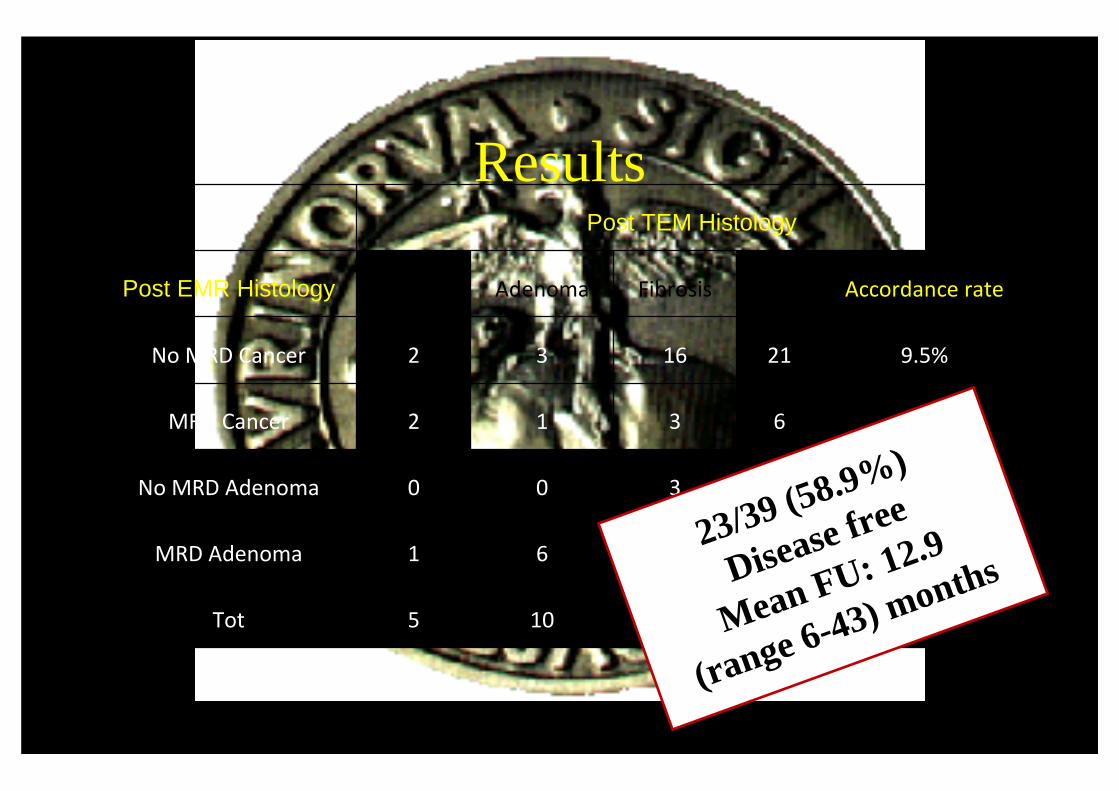
ResultsPost TEM Histology
Post EMR Histology Cancer Adenoma Fibrosis Total Accordance rate
No MRD Cancer 2 3 16 21 9.5%
MRD Cancer 2 1 3 6 33.3%
No MRD Adenoma 0 0 3 3 0%
MRD Adenoma 1 6 2 9 66.6%
Tot 5 10 24 39 15.4%
23/39 (58.9%)
Disease free
Mean FU: 12.9
(range 6-43) months
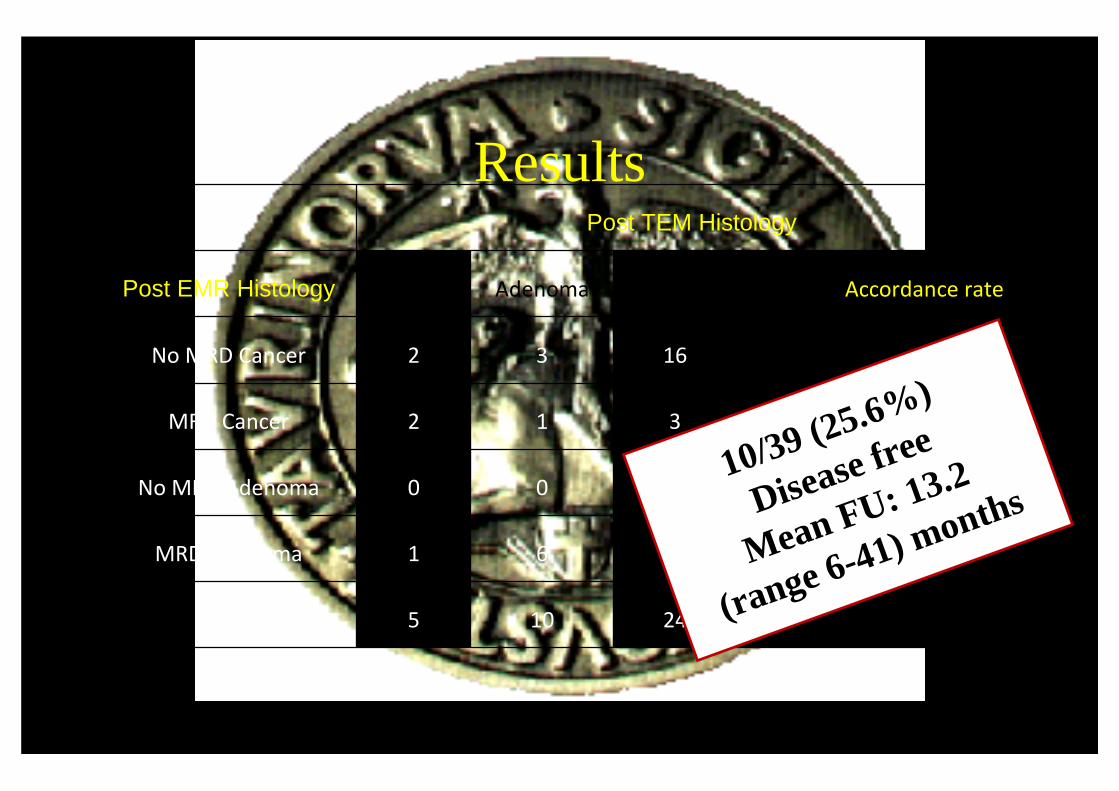
ResultsPost TEM Histology
Post EMR Histology Cancer Adenoma Fibrosis Total Accordance rate
No MRD Cancer 2 3 16 21 9.5%
MRD Cancer 2 1 3 6 33.3%
No MRD Adenoma 0 0 3 3 0%
MRD Adenoma 1 6 2 9 66.6%
Tot 5 10 24 39 15.4%
10/39 (25.6%)
Disease free
Mean FU: 13.2
(range 6-41) months
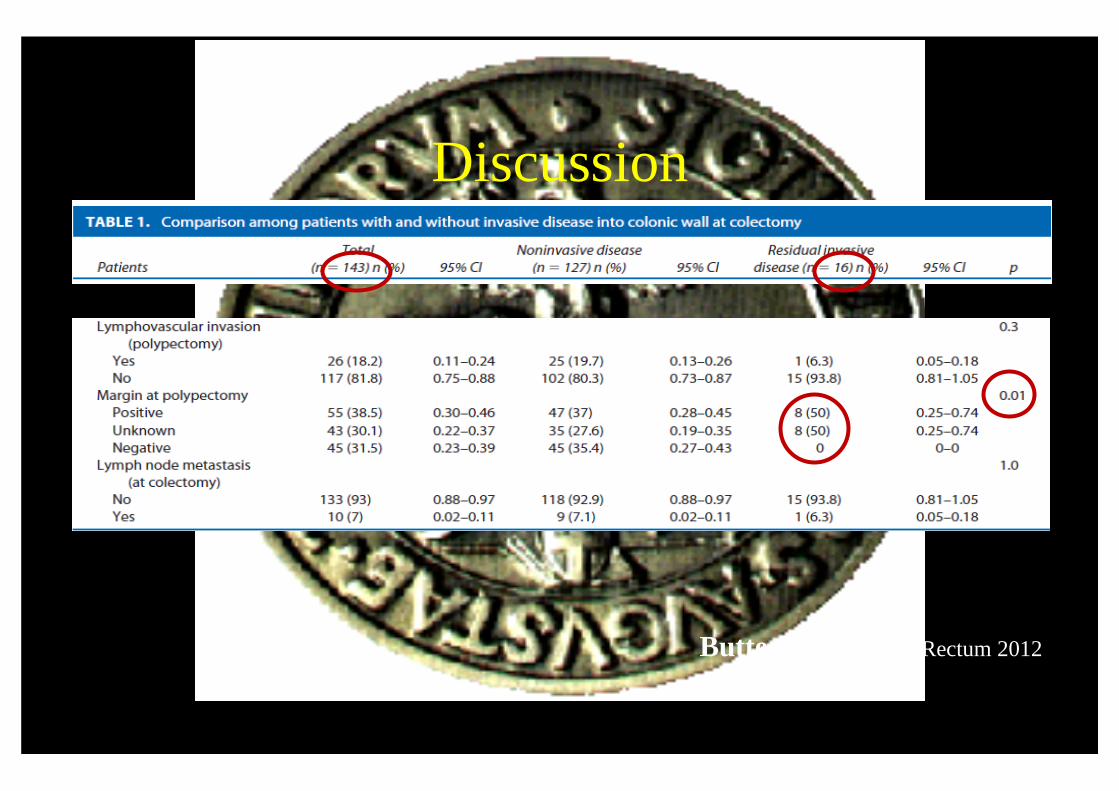
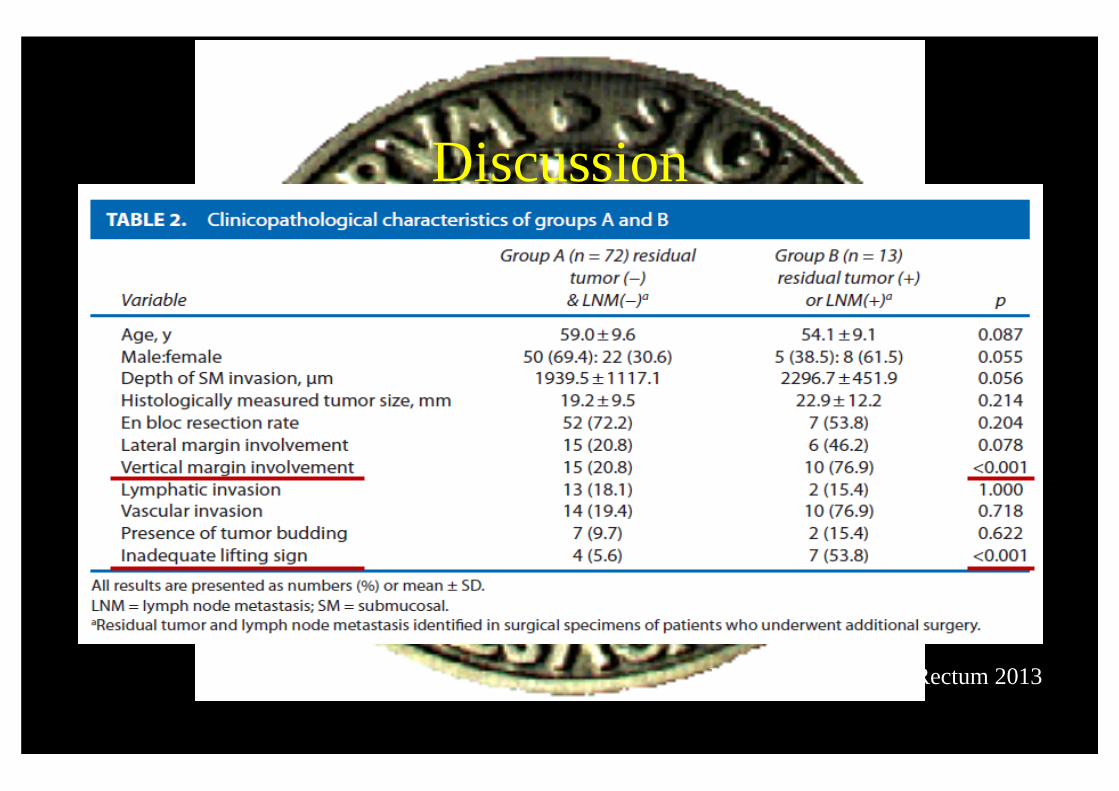
Discussion
Butte et al, Dis Colon Rectum 2012
Discussion
Kim et al, Dis Colon Rectum 2013
ConclusionsRectal polyps > 2 cm
Full Thickness TEM
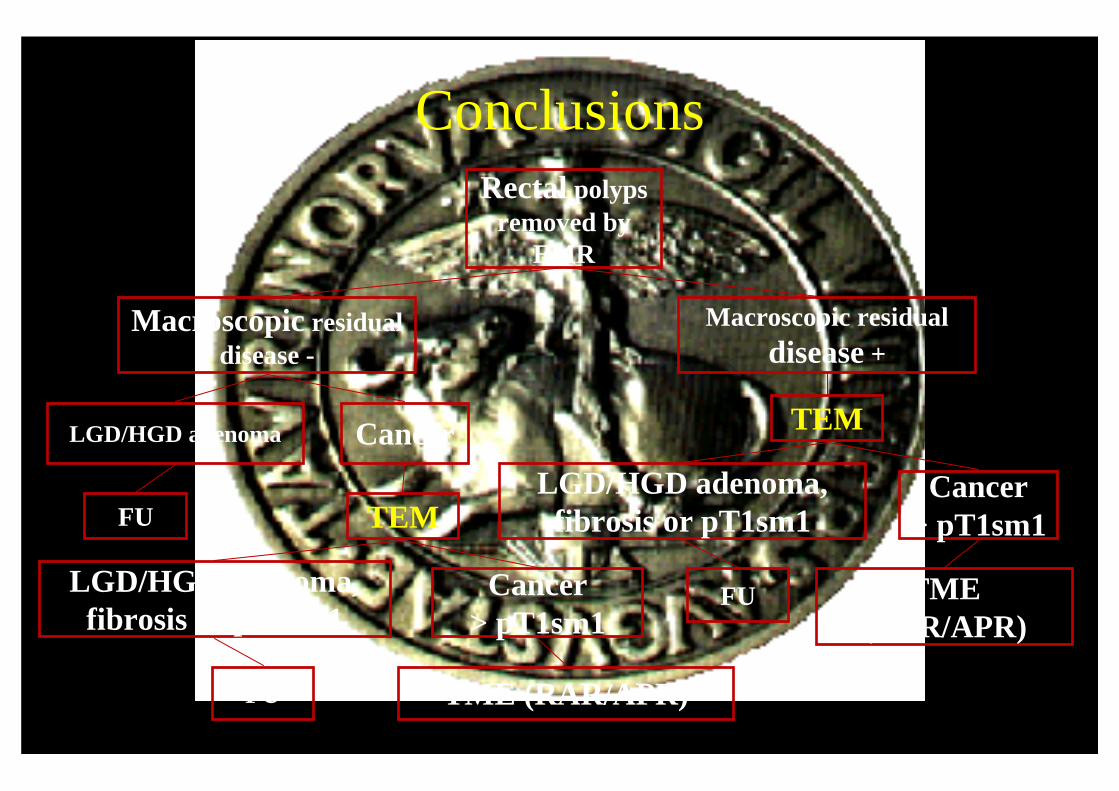
ConclusionsRectal polyps
removed byEMR
Macroscopic residualdisease -
Macroscopic residualdisease +
TEMLGD/HGD adenoma Cancer
FU TEM
LGD/HGD adenoma, fibrosis or pT1sm1
Cancer> pT1sm1
LGD/HGD adenoma, fibrosis or pT1sm1
Cancer> pT1sm1
TME (RAR/APR)
FU
TME (RAR/APR)FU












![Transanal endoscopic microsurgery for radical resection of ...Transanal endoscopic microsurgery in sigmoid cancer 1451 JBUON 2019; 24(4): 1451 large rectal polyps by TEM [11]. However,](https://img.pdfslide.us/doc/110x75/60f7e35c60455642d5494ef7/transanal-endoscopic-microsurgery-for-radical-resection-of-transanal-endoscopic.jpg)
















