Embed Size (px)
Citation preview

Team Collaboration: The Role of the SLP
Reggie Smith, M.A.,CCC-SLP
Speech-Language Pathologist
Presented at Comprehensive Stroke Conference
June 1, 2018
Whittier, CA

Disclosure and Acknowledgment
No conflicts of interest Reggie Smith is employed by PIH Health Hospital Reggie Smith is a volunteer treasurer for the Medical Speech
Pathology Council of California

Defenses to protect our airway
Epiglottis
FVFs
TVFs
Cough Reflex

4
Video Clip - Normal
• Video Clip
Role of the SLP: identifying aspiration risk and strategies to prevent PNA, dehydration, malnx,
pressure sores while collaborating with stroke team re: safe swallow guidelines.

Neurology of Swallowing & Associated Respiratory
Reflexes
S-M
Cortex
Prefrontal
Cortex
NTS &
Reticular
F.
V * Inter-
neurons
Sensory
Nucleus
VII XII
Nucleus
Ambiguus IX, X, XI
Thalamus Subcortical Sites
Central Pattern Generator
CN Motoneuron Pools
VII IX X Palate, pharynx,
larynx, mouth, tongue
Face mouth tongue
Jaw,
palate,
submental
Lips, face,
submental Palate,
pharynx,
larynx,
esophagus
Tongue
submental
Stretch receptors in lungs Diaphragm Intercostals
V
*Acts as a link between sensory/motor neurons
For educational use only and not for distribution: © complied/designed by Reggie Smith
Swallowing is everything but a simple process

Acute CVA: swallowing problems by site of lesion
1. Left or Right CVA (Cortical): If stroke is uncomplicated,
improvement in swallowing is with 1-3 weeks.
2. Medulla (lower brainstem): Improvement estimated from 1-2
weeks.
3. Pons (upper brainstem): Expect slow recovery from 1-4
weeks
4. Subcortical Stroke (Basal Ganglia): improvement in
swallowing is within 3-6 weeks.
5. Multiple Infarcts: Recovery patterns unpredictable.

Neurologic disease is 1 of 4
predisposing factors to aspiration Identification of Hospitalized Patients at Risk for Aspiration- Dr. Festic, Mayo Clinc, Jacksonville Florida, May 7, 2017

8
Video Clip- Abnormal
Role of the SLP: identifying aspiration risk and strategies to prevent PNA, dehydration, malnx,
pressure sores while collaborating with stroke team re: safe swallow guidelines.

Fails the nursing swallow screen Bedside Swallow Evaluation or VFSS (aka: MBSS) is requested
If h/o silent aspiration, SLP will jump right to a VFSS if
patient is appropriate
GOLD standard is a VFSS
Usually do NOT repeat a VFSS before 2 weeks
FEES will be suggested if question of impaired VF function
and dysphonia is present
Fact or Fiction: Is the VFSS a good test of airway function?

10
Acute CVA: Stats & Facts
Silent Aspiration Facts
“55% of stroke patients with
dysphagia demonstrate aspiration and
up to 40% silently aspirate.” -Source:
Shutter, L., (June 1, 2002). Advanced Issues In Dysphagia Management. Jo
Puntil Conference Handout, LBMMC, (2015) pp. 17-28. Respiratory
Infections in Acute Stroke: NG tubes/Immobility are stronger predictors than
Dysphagia - 2013
Dysphagia is present in…
30-65% of patients with acute ischemic stroke
Evidence points to multiple factors to develop PNA in the first week of CVA
Dysphagia present in 58% on admission; Dysphagia present in 1st week now to 30%; Overall respiratory infections = 11%.
[based on 536 CVA pts] Jo Puntil Conference Handout, LBMMC, 17-28.
Prevalence
Oropharyngeal dysphagia post-stroke – up to 78%
Persist 6 months after stroke in 50% of stroke patients

11
Acute CVA: Some Facts
Odds of liquid aspiration are significantly greater for CVA’s NOT oriented to person, place & time.
Odds of liquids/puree aspiration are significantly greater for CVA who cannot follow 1 step commands. (Leder, Suiter, Warner 2009)
Absence of gag reflex does NOT appear to be a predictor of dysphagia. (Leder 1996)
Myth buster: There are plenty of patients with a normal gag, but with severe dysphagia. Gag reflex is not related to swallowing. It is a primitive function and is not controlled by the cerebral cortex. It is a protective reflex.
Odds of liquids aspiration are significantly higher for individuals with reduced lingual ROM. (Leder,
Suiter, Murray, 2013)
Breathiness, hoarseness, harshness may be predictive of aspiration. (Daniels et al 1998)
Presence of dysarthria aspiration risk in stroke patients. (Daniels et. Al. &
McCollough et al 2005) - Motor movement problem (respiration, phonation, resonance, articulation)
Jo Puntil-Medically Fragile Issues Across the Lifespan – July 2015 – LBMMC Presentation

Stats and Facts re: PNA CDC (2011) – $22,875 was the average extra cost of treating one case of PNA
PNA occurs in 38% of all stroke
victims and is the most common
respiratory complication.
PNA contributes to 34% of all
stroke deaths (Stephens &
Addington, 1999)
Asp PNA is… due to
oropharyngeal dysphagia and the
most common form of HCAP
Risk of PNA ’d • 4x with observed laryngeal PEN
• 10x with observed aspiration
• 13x with “silent” aspiration
Gajic et al. AJRCCM 2011;183(4): 462-70
Aspiration
Dysphagia
Poor cough reflex
Silent aspiration
Poor oral care
Bacterial contamination
Oropharyngeal secretion
Gastric secretion GER
Pneumonia
Fact or Fiction: Does a PEG prevent PNA?

Abnormal Esophageal Phase
with the hx of L-CVA
DYSPHAGIA
What are we looking at?
Cognitive ability – attention, impulsivity, awareness, ability to
follow directions
Oropharyngeal phases & overt s/s of aspiration/penetration
with trials if appropriate
Respiratory status
How fragile and/or how ambulatory is the patient
Does patient have h/o dysphagia

Treatment Approaches
NMES with sEMG
Postural techniques
Swallow maneuvers
Neuromuscular
Re-education
Food/Liquid
modifications

Education and Care Provider
Training, including stroke team
Safe swallow guidelines
• sitting posture
• oral care check
• tray set up
• bolus size
• postural techniques
• swallow maneuvers
• assist needed
• adaptive equipment

Education and Care Provider
Training, including stroke team
See Handout re:
Oral hygiene guidelines
Resources: www.swallowstudy.com/oral-care-procedures
Dysphagia after acute stroke
Consequences of missed swallowing impairment by the stroke team members:
• Pulmonary compromise
• Intubation
• Antibiotics
• Alternate feeding method
• LOS by 3.8 days longer than non-dysphagic inpatients
• 33% higher inpatient care costs
• 2.8% times more likely to require post acute care services
• 1.7 fold high odds of dying in the hospital vs. non-dysphagic
patients.
Bottomline: A dx of dysphagia appears to be an indicator of
worse outcomes/higher costs. Patel et al (2018) – Economic/survival burden of dysphagia among inpatients in the United States.
Diseases of the Esophagagus
Patel D A, Krishnaswami S, Steger E, et al. Economic and survival burden of dysphagia among hospitalized patients. Diseases of the Esophagus 2017; 31: 1-7.
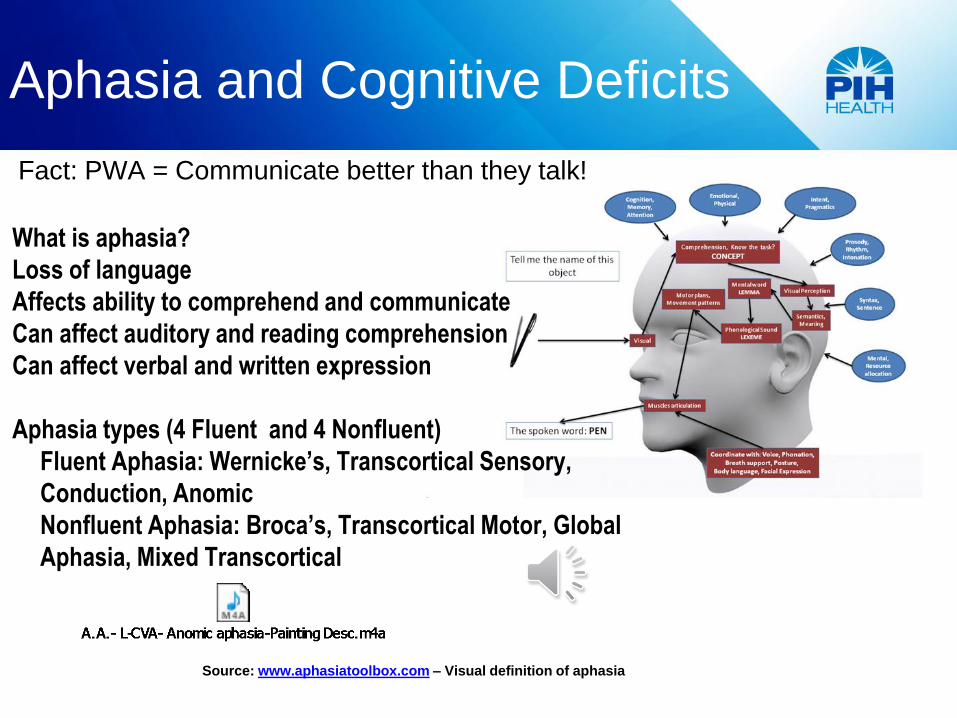
Aphasia and Cognitive Deficits
Source: www.aphasiatoolbox.com – Visual definition of aphasia
What is aphasia?
Loss of language
Affects ability to comprehend and communicate
Can affect auditory and reading comprehension
Can affect verbal and written expression
Aphasia types (4 Fluent and 4 Nonfluent)
Fluent Aphasia: Wernicke’s, Transcortical Sensory,
Conduction, Anomic
Nonfluent Aphasia: Broca’s, Transcortical Motor, Global
Aphasia, Mixed Transcortical
Fact: PWA = Communicate better than they talk!


Aphasia Stats & Facts
Prevalence
• Up to 38 % of stroke patients have aphasia
• Approximately, 1/3rd will fully recover
• Initial severity, early recovery, and site/size of lesion are
good predictions of outcome (Plowman et al., 2011)
• Spontaneous recovery is best during the first 6 months
• PWA can continue to improve years after onset with speech
therapy that focuses on the patient’s environment and
activities of personal relevance for self-management.
NOTE: Most PWA will have some trouble with speaking,
writing, understanding, and/or reading. Some will have
dysarthria (slur/nasality) and/or apraxia (mix up sounds in
words, say the wrong sounds, struggle to say sounds-motor
planning/programming problem).

Cognitive Impairments Post Stoke
Definition: Cognition is an impairment in speed of processing
heard/seen information, attention, verbal/visual memory, executive function
is an umbrella term for lots of cognitive processes having to do with
inhibition (e.g., verbal perseveration), and working memory.
• 75% of acute stroke patients have cognitive impairments
• Cognitive impairment influences spontaneous recovery in the first 12
months
• Cognitive impairments have to do with poor functional outcomes
• If cognition (memory, self-regulation) are faulty, patients may have
difficulty keeping those gains made in therapy over time
• Predictors of response to speech therapy includes: visual-spatial
memory; attention, executive function; and verbal learning (ability to learn
new words, novel words for objects and this correlates with tx outcome)

Aphasia – Role of SLP
Assess language (aphasia), cognition, and motor speech
(dysarthria, apraxia)
Utilize informal and formal measures
Provide intervention (direct and/or indirect)
Provide education to patient and family members
Collaborate with the stroke team
First step: Fluency
Is patient fluent?
Speech is fluent when the patient can say six or more words in a
sentence
To determine fluency
Ask the patient, “Why are you here?
If he answers with six or more words in a sentence, by definition he
is fluent.
Ask patient to repeat simple words, then phrases, then complex
sentences
Repeat after me… Fork, Table, Answer to phone, Eastern
Pentecostal, The neighbor sheared the sheep.

Next step: Auditory Comprehension
Can she understand what she hears?
Begin with one step commands and then advance to more complex
commands
One-step command: Touch ________(eyes, nose, or ears)
Two-step direction: Point to the ceiling, then to the floor or Touch your
nose, then your knee.
Multi-step command: Tap each shoulder twice with two fingers,
keeping your eyes shut.
Can assess with yes/no questions? Are you in a bank?
Are you in a hospital? Are you a woman? Is your name…?

Education and Care Provider
Training, including stroke team
General Communication Guidelines…Simplify
• Handle only one ideas at a time.
• Use short sentences with simple, common
words.
• Repeat or rephrase direction as needed.
• Ask simple, personal yes/no questions.
Are you hot? Are you in pain?

Education and Care Provider
Training, including stroke team
-Slow down and allow time.
-Clue him in.
-Do not assume he understands
everything.
-Guess and confirm.
-Be clear and validate.
-Respect.
-Be flexible.
-Helpful hints. • Be direct, concise.
• Explain what and why you are doing something