Embed Size (px)
Citation preview

Psychological Reports, 1994, 7 4 , 1299-1306. O Psychological Reports 1994
TEACHING INTERPERSONAL SKILLS TO OCCUPATIONAL AND ENVIRONMENTAL HEALTH PROFESSIONALS
STANLEY RABINOWITZ MABEL FEINER JOSEPH RIBAK
Occupational Health and Rehabilitation Institute, Raanana Department of Family Medicine Department of Epidemiology
Sackler School of Medicine and Preventive Medicine Sackler School of Medicine
E l Aviv University
Summary.-An innovative course for teaching communication and interpersonal relationships was delivered to 29 environmental and occupational health professionals. This course aimed to highlight interpersonal and emotional aspects in the profession- al-client interaction and incumbent communication aspects when consulting team mem- bers, colleagues, and nonprofessionals in the occupational arena. Various experiential and other teaching techniques were used. Assessment showed that participants re- ported the positive features of such a course although Few changes in either psychoso- cial abilities or awareness were evident. Possible ramifications of the findings are dis- cussed.
Good practice of occupational medicine is based on an integrative ap- proach to the interaction between man and his occupational environment on the premise that improving quality of life and general well-being can lead to a decrease in the incidence of work accidents and morbidity and to an in- crease in the individual's productivity and general satisfaction in work and life in general (Henkin, 1990; Ribak, 1990).
Academic courses designed specifically to teach occupational health cov- er a wide range of subjects including toxicology, occupational medicine, hy- giene, and prevention. The contribution of the behavioral sciences to the teaching of occupational health includes (a) increasing awareness of psychoso- cial risk factors in the worksite and establishing the relationship between these factors and health-related symptoms and (b) teaching appropriate pre- ventive procedures applicable to the occupational health profession. Courses have included social psychology applied to occupational health and the work- ing population, stress-reduction procedures and interventions, and psycholog- ical aspects in health promotion and health behavior.
~ b m e studies have dealt with the promotion of effective interpersonal skllls in various health populations, taking cognisance of emotional aspects of the doctor-nurse relationship (Davidhizar & Cosgay, 1991; Lubbers & Roy, 1990; Maoz, Rabinowitz, Herz, & Katz, 1992; Rabinowitz, Herz, Granek,
'This study was supported by the Committee For Preventive Action and Research in Occu- pational Health, The Ministry of Labor and Social Affairs, Jerusalem, Israel. The authors thank p a Kasan for preparing the manuscript. Address requests for reprints to Dr. Stanley Rabinowitz, Occupational Health and Rehabili-
tation Institute at Loewenstein Hospital, P O Box 3, Raanana, Israel 43100.
1300 S. RABINOWITZ, ETA.!..
Lehmann, Pincus, & Maoz, 1989; Rabinowitz, Kushnir, & Ribak, in press, b; Sellick, 1991; Vore, 1991). However, the detection and treatment of psy- chosocial problems in occupational medicine, particularly the interaction between occupational health professionals and their clients, have not been adequately described.
Communication issues encountered by the occupational health profes- sional and a patient can be seen in a number of areas. (1) Health pro- fessionals working in an occupational setting as "specialists in occupational exposure to hazards and diseases in the work environment" (Ribak, 1990, p. 5 ) are in constant contact with workers and managers at the workplace. While this relationship may be smooth and problem-free, it can often be complex and fraught with obstacles.
Hill (1992) described the conflict between implementation of company policy and caring for the individual worker, while Gordon (1987) argued that occupational physicians are essentially company men malung clinical deci- sions, often guarding company policy by shielding the company from liti- gation over hazardous work practices. Here, the occupational health team may find it difficult to reconcile providing proper medical care for workers while showing adequate sensitivity to the implementation of company policy. The maintenance of professional confidentiality under these conditions may also be especially problematic, as outlined by Gordon (1987). Thus, effec- tive, sensitive communication skills are required to allay undue concerns and workers' suspicions of a management-aligned occupational health team effort.
(2) Another issue concerns ways of consulting with other professionals and nonprofessionals, i.e., to communicate and discuss results of professional investigations in a manner that is acceptable and comprehensible to other medical specialties and nonprofessionals (workers, management, policy mak- ers). This sometimes causes the occupational physicians discomfort and may affect effective free-flowing communication, for instance, confidentiality. Because of the interface between family medicine and occupational medi- cine, communication problems may also arise in consultations with profes- sional peers and communicating about patients' responsibility and over-all care.
( 3 ) Certain h n d s of interactions may lead to communication difficulties, for example, the malingerer who, motivated by monetary compensation, e.g., following a motor accident, may fabricate or exaggerate physical or psycho- logical symptoms for external gain. Malingerers often evoke a wide range of negative feelings in health professionals. Feelings of mistrust, anger, and h u d a t i o n are not uncommon and often threaten the traditional doctor-pa- tient relationship (Rabinowitz, Mark, Modai, & Margalit, 1990). Dissimula- tion may also pose problems. Occupational health physicians may be en- trapped by their feelings when patients who are motivated to work do not describe psychological or physical problems on examination.
HEALTH PROFESSIONALS: INTERPERSONAL SKILLS 1301
These are but a few of the areas in which the occupational health pro- fessional's feelings and interactions may necessitate appropriate communica- tion skills to allow effective relations with patients, colleagues, and the en- vironment.
Tel-Aviv University has developed a postgraduate continuing medical education course in occupational health for various medical specialties, in- cluding occupational physicians, nurses, industrial hygienists, and behavioral scientists working in occupational medicine. The master's program has been well described by Ribak, Noy-Man, Henkin, and Shapiro (1991). Teaching covers the main subjects for professional competency including epidemiology, biostatistics, principles of toxicology, physiology, industrial hygiene, and behavioral medicine. The latter includes social psychology, behavioral medi- cine, and occupational stress reduction. However, human interaction and communication skills have until now not been taught.
The Institute for Occupational Health at Tel-Aviv University Medical School has developed a course entitled "Communication Skills for the Oc- cupational Health Professional." Course objectives are (a) teaching commu- nication skills to enable the participants to detect emotional aspects in the professional-client encounter in the occupational arena, (b) helping the par- ticipants to understand reasons for emotional responses in emotionally loaded areas of occupational health to enable evaluation of the effects of these re- sponses on the professional-client or service receiver, and (c) demonstrating the communication aspects of teamwork and consultation both within and outside of the occupational medical setting.
Description of Course The semester course, consisting of 34 academic hours, was part of the
two-year master's program in Occupational Health at the Tel-Aviv University Medical School. I t was given to such professionals as occupational health physicians, industrial hygienists, and nurses or behavior scientists.
The course was divided into two sections, (1) communication between the health professional and the client and (2) communication between the health professional and his environment. In the first section topics included types of human communication, nonverbal communication, and doctor-pa- tient models. Different types of clients were discussed, including the nagging client, the angry client, the seductive client, and the malingerer. Specific rel- evant subjects were also taught. The second section covered communication with colleagues, including primary-care specialists, other health professionals, and management. These encounters often require the use of delicate com- munication skills. Topics raised included the loyalty issue, allegiance, con- fidentiality, and ways of communicating with these groups.
Various teaching techniques were used to foster active participation by the students. These included discussions based on case vignettes viewed on
1302 S. RABINOWITZ, ET AL.
videotape and simulated consultations, role playing, and individual case pre- sentations of communication issues encountered by health professional~. Relevant professional literature was also distributed, and participants were required to present the material actively in class. This stimulated lively dis- cussions. The relevance of all the material to the work arena was constantly emphasized. Similar to the work on industrial accident simulation by Ribak, et al. (1991), we wished to provide the students with "hands on" experien- tial learning in human communication.
An example of the videotaped vignette concerns a physician-patient di- alogue. The patient, a 45-yr.-old married working man with a moderate drinlung problem consults the physician. He tells the doctor that his wife has left him and he has severe financial problems. The 55-yt-old attending male physician has worked in the catchment area for a long time. His com- munication style is known to be forthright and direct. As the patient's story unfolds, the physician becomes increasingly irritable and fails to allay his fears, actively playing them down. As the consultation proceeds, he becomes more and more dominant until at the end he blurts out, "I warned you a long time ago of the danger of your wife leaving you and to watch your drinking, and that you risk losing your job. I told you, but you haven't lis- tened to me. Now I will tell you what to do . . ." The physician then proceeds to instruct him how to run his life. The patient by now has become passive and withdrawn.
A lively discussion ensued as to the doctor's expression of anger and irritability toward the patient, leading to a discussion of negative involve- ment with patients by other health professionals and ways of overcoming negative feelings and converting them into more appropriate professional ac- tion.
The purpose of the present study was to evaluate the efficacy of the course in contributing to increasing awareness and changing communication slulls and sensitivity to interpersonal processes and to evaluate at the end of the course the quality of its organization, teaching style, and group involve- ment.
Subjects The 29 professionals participating in the course comprised 11 hygien-
ists, 6 occupational physicians, and 12 behavioral scientists. All participants were actively working in a wide range of occupational health-related units in Israel.
Procedure Psychosocial professional efficacy was measured by the Psychological Med-
ical Inventory (Ireton & Sherman, 1988). Internal consistency was .88. The
HEALTH PROFESSIONALS: INTERPERSONAL SKILLS 1303
inventory was transIated into Hebrew by two thoroughly bilingual psycholo- gists. The questionnaire comprised 11 questions on a 7-point scale, nine as- sessing abilities in dealing with psychological aspects of patient care and two questions relating to sensitivity to patients' psychological needs, including confidence in dealing with interpersonal skills. An example of an abh ty question is "Ability to develop good professional-client relationships"; an ex- ample of a sensitivity question is "I am aware of how patients react to me." This questionnaire has been found to measure communication and relation- ship skills (Ireton & Sherman, 1988). The questionnaire has been adrninis- tered to over 100 Israeli health professionals. The total alpha value for all items was .85 and for the nine ability items .85. The two sensitivity items showed a correlation of .41 significant at the .0001 level.
The Social Support Questionnaire was an adapted version of the social support scale developed by Ezion (1984). Internal consistency was .75. The scale comprised 11 items on a 7-point scale. I t included items relating to feedback from others, unconditional support, and emotional social support. The social support score is the sum of scores on each of the individual items.
At the end of the course an evaluation questionnaire was given to the three groups. Internal consistency (alpha) of the questionnaire was .90. The questionnaire comprised 12 items on a 6-point scale ranging from 1 (low rel- evance) to 6 (high relevance) and evaluating various aspects of the course including course relevance, broadening professional skills and behavior, course delivery, content, and general satisfaction. Further, a question was asked as to how interested the participants were in participating in a similar course in the future.
The Psychological Medical Inventory and the Social Support Scale were given to the subjects before and after completion of the course. The course assessment questionnaire was given at the end of the course.
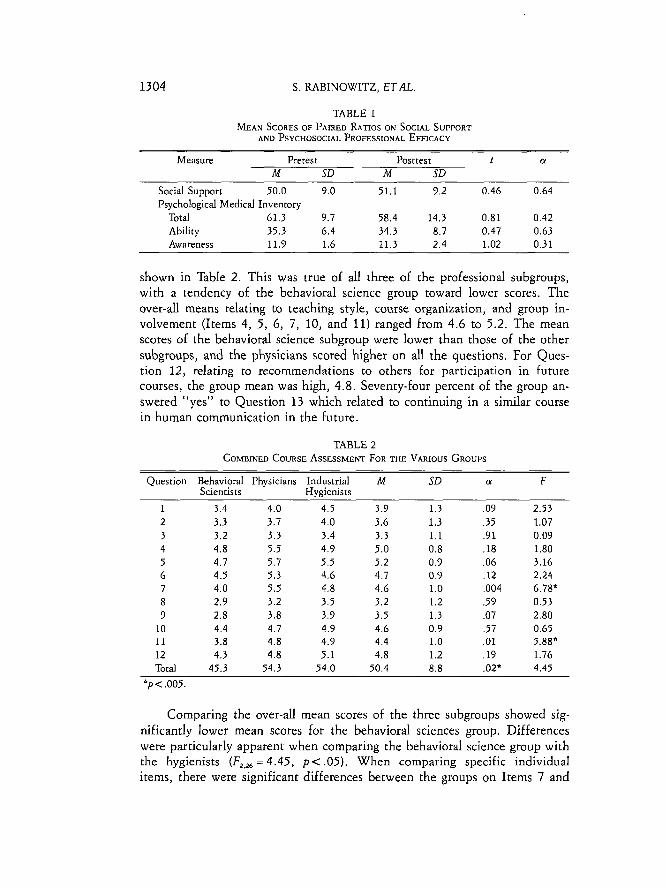
RESULTS As shown in Table 1, differences were found in social support before
and after the course, although these did not reach significance (mean of 50.0 increased to 51.1). However, it should be pointed out that the baseline mean of the present group was considerably higher than that of a previous group of family practice physicians who were exposed to a similar course (Rabinowitz, 1993).
For the professional psychosocial efficacy variables of the Psychological Medical Inventory which related to awareness of and sensitivity to psychoso- cial problems, there were no significant changes before and after the course, as shown in Table 1. However, it should be noted that the total over-all base- line scores were high (mean greater than 60 out of a possible 77).
O n the course assessment questionnaire, the over-all group means relat- ing to broad teaching aims (Items 2, 3, 8, and 9) ranged from 3.2 to 3.6, as
1304 S. RABINOWITZ, ET AL.
TABLE 1 MEAN SCORES OF P ~ E D h n o s ON SOCW SUPPORT
AND PSYCHOSOCIAL PROFESSIONAL EFFICACY
Measure Pretest Posttest t (Y
M SD M SD Social Support 50.0 9.0 51.1 9.2 0.46 0.64 Psychological Medical Inventory
Total 61.3 9.7 58.4 14.3 0.81 0.42 Ability 35.3 6.4 34.3 8.7 0.47 0.63 Awareness 11.9 1.6 11.3 2.4 1.02 0.31
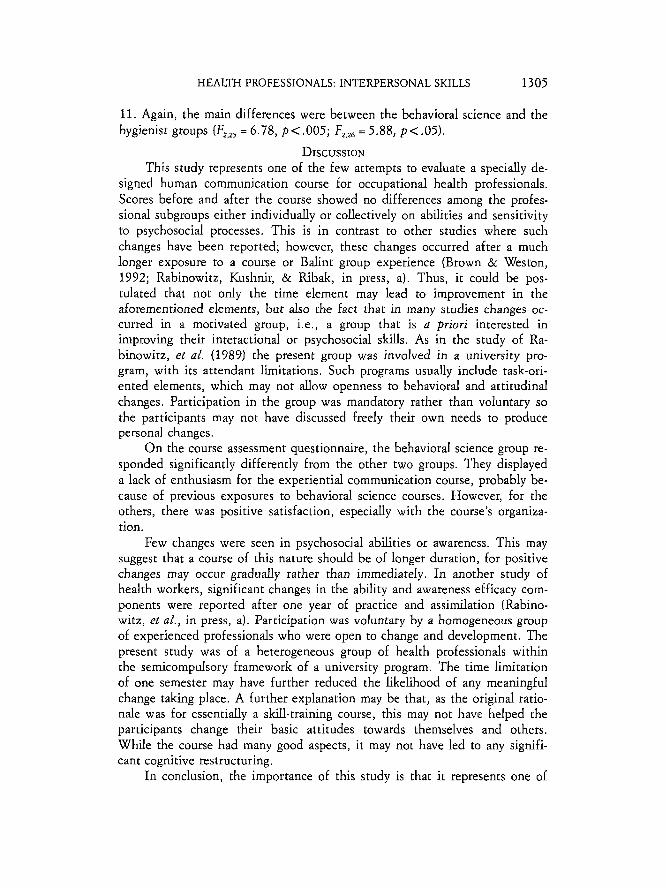
shown in Table 2. This was true of all three of the professional subgroups, with a tendency of the behavioral science group toward lower scores. The over-all means relating to teaching style, course organization, and group in- volvement (Items 4, 5, 6, 7, 10, and 11) ranged from 4.6 to 5.2. The mean scores of the behavioral science subgroup were lower than those of the other subgroups, and the physicians scored higher on all the questions. For Ques- tion 12, relating to recommendations to others for participation in future courses, the group mean was high, 4.8. Seventy-four percent of the group an- swered "yes" to Question 13 which related to continuing in a similar course in human communication in the future.
TABLE 2 COMBINED COURSE ASSESSMENT FOR THE VARIOUS GROUPS
Question Behavioral Physicians Industrial M SD a F Scientists Hygienists
1 3.4 4.0 4.5 3.9 1.3 .09 2.53 2 3.3 3.7 4.0 3.6 1.3 .35 1.07 3 3.2 3.3 3.4 3.3 1.1 .91 0.09 4 4.8 5.5 4.9 5.0 0.8 .18 1.80 5 4.7 5.7 5.5 5.2 0.9 .06 3.16 6 4.5 5.3 4.6 4.7 0.9 .12 2.24 7 4.0 5.5 4.8 4.6 1.0 ,004 6.78" 8 2.9 3.2 3.5 3.2 1.2 .59 0.53 9 2.8 3.8 3.9 3.5 1.3 .07 2.80
10 4.4 4.7 4.9 4.6 0.9 .57 0.65 11 3.8 4.8 4.9 4.4 1.0 .01 5.88" 12 4.3 4.8 5.1 4.8 1.2 .19 1.76 Total 45.3 54.3 54.0 50.4 8.8 .02* 4.45
* p < ,005.
Comparing the over-all mean scores of the three subgroups showed sig- nificantly lower mean scores for the behavioral sciences group. Differences were particularly apparent when comparing the behavioral science group with the hygienists (F,,,, = 4.45, p < .05). When comparing specific individual items, there were significant differences between the groups on Items 7 and
HEALTH PROFESSIONALS: INTERPERSONAL SKILLS 1305
11. Again, the main differences were between the behavioral science and the hygienist groups (F,,,, = 6.78, p < ,005; F,,, = 5.88, p < .05).
DISCUSSION This study represents one of the few attempts to evaluate a specidy de-
signed human communication course for occupational health professionals. Scores before and after the course showed no differences among the profes- sional subgroups either individually or collectively on abhties and sensitivity to psychosocial processes. This is in contrast to other studies where such changes have been reported; however, these changes occurred after a much longer exposure to a course or Balint group experience (Brown & Weston, 1992; Rabinowitz, Kushnir, & Ribak, in press, a). Thus, it could be pos- tulated that not only the time element may lead to improvement in the aforementioned elements, but also the fact that in many studies changes oc- curred in a motivated group, i.e., a group that is a priori interested in improving their interactional or psychosocial skills. As in the study of Ra- binowitz, et al. (1989) the present group was involved in a university pro- gram, with its attendant limitations. Such programs usually include task-ori- ented elements, which may not allow openness to behavioral and attitudinal changes. Participation in the group was mandatory rather than voluntary so the participants may not have discussed freely their own needs to produce personal changes.
O n the course assessment questionnaire, the behavioral science group re- sponded significantly differently from the other two groups. They displayed a lack of enthusiasm for the experiential communication course, probably be- cause of previous exposures to behavioral science courses. However, for the others, there was positive satisfaction, especially with the course's organiza- tion.
Few changes were seen in psychosocial abilities or awareness. This may suggest that a course of this nature should be of longer duration, for positive changes may occur gradually rather than immediately. In another study of health workers, significant changes in the ability and awareness efficacy com- ponents were reported after one year of practice and assimilation (Rabino- witz, et al . , in press, a). Participation was voluntary by a homogeneous group of experienced professionals who were open to change and development. The present study was of a heterogeneous group of health professionals within the semicompulsory framework of a university program. The time limitation of one semester may have further reduced the likelihood of any meaningful change taking place. A further explanation may be that, as the original ratio- nale was for essentially a skill-training course, this may not have helped the participants change their basic attitudes towards themselves and others. While the course had many good aspects, it may not have led to any signifi- cant cognitive restructuring.
In conclusion, the importance of this study is that it represents one of
1306 S. RABINOWITZ, ET AL
the few attempts at evaluating the effects of a course on human interaction and communication especially developed for occupational health profession- als. Although we did not demonstrate clear over-all differences, there were changes in the expected direction on the social support measure. Studies are needed to validate the results, with emphasis on longer-term group exposure to this type of training preferably outside of the compulsory, pressurized uni- versity setting. Further follow-up should be undertaken to investigate the efficacy of acquiring these skills for the occupational health professionals in their work setting. Finally, a limitation of the course concerned the central use of skill training as opposed to using it in combination with another ap- proach such as rational-emotive therapy. Adopting the latter approach from the outset may have indeed shown the trainees that their basic irrational be- liefs prevented them from unconditionally accepting themselves and the dif- ficult people with whom they work. Once this cognitive restructuring had been achieved, skill training could have followed.
REFERENCES BROWN, J. B., & WESTON, W. W. (1992) Training in psychosocial issues. Canadian Family
Physician, 38, 806-812. DAVIDFIIZAR, R., & COSGAY, R. (1991) Being an effective speaker. Today's OR Nurse, 13(8),
36-38. EZION, D. (1984) hloderatin effects of social support on the stress burnout relationsh~p.
Joitrnal o/ Appircd ~ s ~ c f o l o g ~ , 69, 615-622. GORDON, J. (1987) \%'orkplace health promotion: the right idea in the wrong place. Health Ed-
ucation Rrrrurch, 2 , 69-71. HENKM, I. (1990) Psychosocid aspects of occupational medicine. The Family Physician, 15,
31-35 . - - HILL, I. M. (1992) Health promotion in the British workplace: a suitable case for treatment.
Occupational Medicine, 42, 175-178. IRETON, H. , & SHERMAN, M. (1988) Self-ranngs ol graduating 6amily practice residents' psy-
chological medicine abilities. Family Prac!rcc Research Journal, 7, 236-244. L ~ B E R S , C. A,, & ROY, S. J. (1990) Commilnlcailon slulls for continuing education in nurs-
ing. Journal of Continuing Education in Nursing, 21, 109-112. IVIAOZ, B., ~ B I N O W I T Z , S., HERZ, M., & KATZ, C. (1992) Doctors and their feelings: a pharma-
cology of medical caring. New York: Praeger. RABINOWTZ, S. (1993) A communication course for farnily practitioners. (Unpublished report) RABINOWITZ, S., HERZ, M., GRANEK, M., LEHMANN, S., PINCUS, C., & MAOZ, B. (1989) The
doctor and his feelings: a course for residents in family medicine. Family Practice, 6, 199-202.
RABINOWTZ, S., KUSHNIR, T., & RKFIAK, J. (in press, a) Developing psychosocial mindedness and sensitivity to mental health issues among primary care nurses using the Balint Group method. Israel Journal of Psychiafry and Related Sciences.
RABINOWITZ, S., KUSHNIR, T., & R ~ M , J. (in press, b) The training of primary care nurses using the Balint method. Healrh and Social Care in the Communio.
RABINOWITZ, S., MARK, M., MODAI, I., & MARGALIT, C. (1990) Malingering in the clinical set- ting: practical suggestions for intervention. Psychological Reports, 67, 1315-1318.
~ A K , J. (1990) Occupational health. The Family Physician, 18, 7-10. RIBM, J., NOY-MAN, Y., HENKIN, I., & SHAPIRO, Y. (1991) Using industrial accident simula-
tion as a tool for teaching occupational and environmental medicine. Jozirnal of Occu- pational Medicine Singapore, 3, 41-44.
SELLICK, K. J. (1991) Nursing interpersonal behaviors and the development of helping skills. International Jonrnal of Nursing Shidies, 28, 3-1 1 .
VORE, A. L. (1791) Enhancing verbal communication skills and promoting effective socializa- tion of newly hired Spanish speaking registered nurses. Journal of Nursing Staff Devel- opment, 7 , 286-289.
Accepted March 28, 1794.





























