Embed Size (px)
Citation preview

Targeting the Poor in Times of Crisis:
The Indonesian Health Card
Robert Sparrow
Institute of Social Studies
The Hague, The Netherlands
October 2006
Correspondence: Robert Sparrow, Institute of Social Studies, P.O Box 29776, 2502 LT
The Hague, The Netherlands. E-mail: [email protected].
Key words: Access, economic crisis, Indonesia, outpatient care, poverty, price subsidy,
targeting.

Abstract
This paper looks at targeting performance of the Indonesian health card programme that
was implemented in August 1998 to protect access to health care for the poor during the
Indonesian economic crisis. By February 1999, 22 million people had received a health
card. The health card provided a user fee waiver for public health care. Targeting of the
health card was pro-poor, but with considerable leakage to the non-poor. Utilisation of
the health card for outpatient care was also pro-poor, but conditional on ownership, the
middle quintiles were more likely to use the card.
Targeting of the health card followed a decentralised design combining
geographic targeting with community based targeting. This design facilitated the rapid
implementation of the programme, but targeting performance suffered from inadequate
information on the regional impact of the crisis, while at local level not all barriers to
accessing health care services were overcome by the health card. Indirect and direct costs
of seeking health care seem to be the main deterrent to using the health card, which are
higher in more remote areas.
Micro-simulations show that geographic targeting can contribute considerably to
improving targeting performance, but most of the targeting gains are to be made at the
community level.
This study highlights the need for adequate and up to date social welfare
indicators. In addition, further research would need to focus on how local knowledge can
be utilised for signalling poverty dynamics and local barriers to access.

Acknowledgements
I thank Menno Pradhan, Jan Willem Gunning, Marleen Dekker and Sudarno Sumarto for
helpful comments. A large part of this work was done while I was at the Vrije
Universiteit and Tinbergen Institute in Amsterdam, The Netherlands. Support from the
Netherlands Foundation for the Advancement of Tropical Research (NWO/WOTRO) is
gratefully acknowledged. All errors remain my own.

1
1. Introduction
In an attempt to protect access to health care utilisation for the poor during the Indonesian
economic crisis, a nationwide health programme was introduced in August 1998, as part
of the larger Indonesian Social Safety Net – Jaring Pengaman Sosial (JPS). This health
care programme included a targeted price subsidy that operated through the so called
health card – Kartu Sehat. Households that were thought to be most vulnerable to
economic shocks were allocated health cards, which entitled all household members to
the price subsidy at public health care providers. The programme followed a partly
decentralised targeting process, involving both geographic and community based
individual targeting.
The success of such crisis interventions critically depends on the ability to
identify and reach the poor, in particular those that are most vulnerable to the effects of a
crisis. Successful targeting requires information on welfare and crisis impact for
individual households. Typically, collecting such disaggregated information centrally is
costly. The administrative capacity for providing welfare details for each household (for
example, a centralised tax administration) is often not available in developing countries
like Indonesia. Moreover, short term information regarding the crisis effects for
individual households would be hard to retrieve even under a highly developed
administrative system. For example, in case of the Indonesian crisis, Skoufias et al. (2000)
find evidence of considerable movement in and out of poverty from 1997 to 1998,
hindering accurate targeting of the poor.
The decentralised design of the JPS programmes is meant to deal with this
targeting problem. The combination of multi-level geographic and community based

2
targeting provides an alternative infrastructure for gathering and processing information
locally, and disseminating this to higher administrative levels. Several authors have
argued that a decentralised design can benefit from local knowledge and community
participation, on the premise that local communities are more capable of identifying the
poor.1 Not only do local communities have better access to information on targeting
criteria, they are also more able to prioritise amongst the set criteria or even formulate
new local criteria that better reflect the need for assistance.
However, decentralisation has its weaknesses. Recently, a number of theoretical
and empirical studies have investigated the implications and pitfalls of different aspects
of decentralisation (e.g. regional political or fiscal autonomy). A main concern is that the
benefits of using local knowledge are offset against the loss of control over the allocation
process. Decentralised programmes are prone to local elite capture and suffer from
classic principal-agent dilemmas (e.g. Bardhan and Mookherjee 2000 and 2005, Galasso
and Ravallion 2005). In a comprehensive review of the empirical literature on targeting
Coady et al. (2004) find that geographic and community based targeting perform above
average, but with a large variation between the individual projects.
This paper deals with the targeting of the JPS health programme, in light of the
decentralised design. The objective is to investigate how the programme has been
implemented and who were the beneficiaries of the health cards. Has health card
allocation been pro-poor and is there evidence of leakage or local capture of benefits by
the non-poor? Particular focus will be on the effectiveness of regional targeting policy in
contrast to local (within-district) targeting by the allocation committees. What factors
underlie the observed patterns of benefit incidence? Has the centre been able to identify

3
the regions hit hardest by the crisis? What determines targeting at local level? Are there
barriers unabridged by the health card? Finally, a micro-simulation exercise will
decompose overall benefit incidence into geographic and local targeting performance.
The next section sets the context of the programme and contains a detailed
description of the programme design. Section 3 proposes the methodology and describes
the data. The results are presented and discussed in section 4, while section 5 concludes.
2. Background
The Indonesian economic crisis
The Indonesian economic crisis was triggered by a financial crisis that hit Southeast Asia
mid 1997. In addition, eastern Indonesia, Java and Sumatra were struck by El Niño
related droughts in the second half of 1997, while Sumatra, Kalimantan and eastern
Indonesia suffered large forest fires. In 1998 real GDP decreased by roughly 14 percent
and poverty rates had increased dramatically.2 According to estimates by the Indonesian
Bureau of Statistics (BPS) the poverty headcount increased from 17.7 percent in 1996 to
23.5 percent in 1999. Alternative estimates of poverty during the crisis abound,
unambiguously showing a daunting increase in poverty.3
The crisis saw a sharp decrease in the utilisation of outpatient health care from
1997 to 1998. Outpatient utilisation rates for modern health care drop from 0.193 visits
per person per month to 0.142 visits, with utilisation of public care declining from 0.095
to 0.064.4 This declining utilisation of public services was concentrated with local public
health clinics. A mayor cause of the decline in public health care utilisation was a
shortage of drugs and supplies during the crisis and a subsequent quality deterioration of

4
public care (Waters et al. 2003, Frankenberg et al. 1999, Knowles et al. 1999). Knowles
and Marzolf (2003) report cutbacks in public health spending due to reduced government
revenues during the crisis. The lack of operational funds and shortage of drugs disrupted
services in public health care facilities in 1998. In 1999 public health care utilisation
showed slight signs of recovery, which was partly attributed to the health card
programme (Pradhan et al. forthcoming).
The JPS health card programme
At the onset of the Indonesian financial crisis an important concern was whether the
achievements made in the social sectors over the past decades could be sustained. The
Indonesian government, with help of donors, reacted swiftly by introducing a social
safety net intervention aimed at safeguarding real incomes and access to social services
for the poor.
A main component of the social safety net was the revitalisation of the health card
programme, which started in the fall of 1998.5 This card existed before the onset of the
crisis, but its use had been negligible. A health card entitled a household to free services
at public health care providers consisting of (1) outpatient and inpatient care, (2)
contraceptives for women of child bearing age, (3) pre-natal care and (4) assistance at
birth. This study is limited to outpatient health care utilisation. The public health care
providers where the health cards could be used received budgetary support. These grants
were meant to compensate for the expected demand due to the health card and maintain
quality of health care. However, there was a loose relationship between the utilisation of
the health card and the compensation that the health care providers received in return.

5
Compensation was allocated based on the estimated number of households eligible for
the health card programme rather than actual utilisation of the health cards. The
1998/1999 budget for JPS health grants to primary health centres (Puskesmas) and village
midwives (Bidan di desa) amounted to US $ 29 million, financed by the Government of
Indonesia and the Asian Development Bank.
The JPS health programme followed a decentralised design, with part of the
targeting and allocation process delegated to district administrations, villages officials
and public health care providers. The number of health cards and the amount of
compensation to health care providers was determined by a prosperity measure for 307
district (urban kota and rural kabupaten), which was provided by the National Family
Planning Coordinating Agency – Badan Koordinasi Keluarga Berencana Nasional
(BKKBN). This prosperity measure is a poverty headcount ratio, defining a household as
poor if it fails one or more of the following 5 basic needs criteria: (i) households can
worship according to faith, (ii) eat basic food twice a day, (iii) have different clothing for
school/work and home/leisure activities, (iv) have a floor that is made out of something
other than earth, and (v) have access to modern medical care for children or access to
modern contraceptive methods. The BKKBN collects this information nationwide on a
census basis. The BKKBN prosperity measure has been criticised to be an unsuitable
allocation criterion for the JPS, since its components are fairly inflexible and
inappropriate for measuring economic shocks or the impact of a crisis. However, at the
time of implementation it was the only up to date welfare measure at hand. The BKKBN
prosperity measure was also used as allocation rule for both the budgetary support to
facilities and health cards to households.

6
Targeting within districts followed a two stage process. Special district
committees allocated compensation funds to public health care providers according to the
estimated number of health card eligible households living in the area served by the
provider. The transfer size was not influenced by the actual services provided to health
card owners, but based on BKKBN headcounts in the village or sub-district. Health cards
were allocated to villages, again based on the BKKBN measure, and subsequently
distributed to eligible households through local health centres and village midwives.
Eligible households were those that were considered poor following the BKKBN
classification. In addition, targeting of households relied heavily on local knowledge by
granting local leaders to define additional criteria according to their own insights
regarding the effects of the crisis.
3. Methodology and data
Benefit incidence analysis and targeting performance
The analysis starts with a benefit incidence analysis of health card allocation and
utilisation, and then investigates the factors driving observed benefit incidence patterns
by focusing on the targeting instruments and barriers at three layers of the targeting
process: the geographic unit (inter-district targeting), the community (intra-district
targeting) and the household (utilisation). Finally, geographic targeting performance is
linked to individual heath card allocation and utilisation by simulating targeting regimes.
The benefit incidence analysis describes the coverage and concentration of receipt
and allocation of health cards, and how this varies by economic status. Coverage reflects
the percentage of the population participating in the programme, while the concentration

7
measure indicates how the benefits are distributed across the population. Monthly
household expenditure per capita is used as indictor for economic welfare, by defining
quintiles. Following BPS poverty estimates, the poorest quintile roughly corresponds to
the share of the population living below the poverty line.
Table 1 shows the different targeting phases, with the main actors, decisions and
actions, targeting instruments and main barriers. In the first targeting phase the district
BKKBN measure was the main targeting instrument of the central management unit in
Jakarta. The main question here is whether the BKKBN prosperity measure adequately
reflects the poverty profile and the geographic heterogeneity of the crisis impact.
For the second targeting phase, the determinants of within-district targeting are
scrutinised by means of multivariate analysis, at household level. A probit is estimated
for the probability of receiving a health card (hcjk) conditional on geographic targeting
( ) ( ) ( )0Pr0Pr1Pr 321
* >+++=>== jkkkjkjkjk BKKBNBPSXhchc εααα (1)
where Xjk reflects the characteristics and village conditions for a household j (in district k)
that may be considered as local targeting criteria. BKKBNk contains targeting criteria for
sub-districts and districts. Although it was no an official targeting criterion, the model
also control for the BPS district poverty headcount, as irregularities in allocation were
correlated with the average level of poverty. The error term εjk reflects unobserved factors
affecting targeting. The marginal effects can be interpreted as reflecting intra-district
targeting since the district targeting rules have been controlled for.6

8
Even if households receive a health card, there may still be barriers to using it,
such as lack of information, regional shortage of providers, or opportunity costs
unabridged by the health card. Such barriers are likely to vary by households and are
likely to be higher for the poor. To this end, the third stage of the targeting process is
considered through probit analysis of the determinants of health card utilisation (hcuijk)
conditional on health card ownership
( ) ( ) ( ) 1if0Pr0Pr1Pr 321
* =>+++=>== jkijkijkkijkijkijk hcvBPSXhcuhcu λβββ (2)
The unit of analysis is the individual. Xijk contains the same variables as in equation (1),
in addition to gender and age of individual i. Since the model is estimated for health card
recipients, and health card allocation was not random, consistency of the β estimates is
typically compromised by selection effects. Sample selection is controlled for by the
selection term λ = E(ε | hc = 1). Under the normality assumptions of a probit analysis, λ is
the inverse Mills ratio computed from the health card allocation probit estimates.7 To
facilitate identification, the BKKBN district and sub-district targeting variables are
excluded in equation (2). These regional BKKBN indicators were used for geographic
targeting but should not play a role in the individuals’ decision to use the health card.8
Micro-simulation
To separate geographic from local targeting performance, I follow Alatas and Pradhan
(2003) who propose a micro-simulation based approach to attribute changes in targeting
performance to specific targeting stages. The estimation results from (1) and (2) are used

9
to simulate targeting outcomes under different geographic targeting regimes. The actual
targeting performance will be compared to that under geographic targeting following the
BPS indicators and a uniform regime where allocation to district simply depends on
population size. This will show how local targeting performs on its own, and whether
there is scope for geographical targeting to improve pro-poor allocation of health cards.
The simulation exercise comes down to using the probit estimates for ranking
households within districts in terms of eligibility. Households are selected into the
programme according to their eligibility rank until the district quota is reached.
Geographic targeting regimes are then imposed by changing the number of households
selected for the programme in each district, keeping the overall size of the programme
constant. That is, the districts’ share in the programme is altered, not the total amount of
health cards.
In order to rank households within districts, the probit estimates are not sufficient;
the unobserved errors are also needed. To see this, consider equation (1): hc* can be
interpreted as latent programme eligibility, where the eligibility threshold of selection is
normalised to zero. This latent eligibility can be constructed from the probit’s linear
prediction and the unobserved error term. Therefore the errors are drawn from a truncated
standard normal distribution, such that 0~ˆˆˆ 321 >+++ jkkkjk BKKBNBPSX εααα if
household j received a health card, and the opposite if otherwise.9 A similar approach is
taken for utilisation: conditional on health card allocation to households under a specific
geographic targeting regime, an individual’s utilisation behaviour is evaluated according
to the linear prediction of the utilisation probit (2) and error ijkv~ . In this way it is possible

10
to track the effects of regional redistribution of health cards to household level allocation
of health cards, and then to individual utilisation of the health card for outpatient care.
Data sources
The key source of data is Indonesia's main socioeconomic survey (Susenas). The Susenas
is conducted annually on a national scale, collecting information on health care utilisation,
socioeconomic background of individuals and households, and detailed information on
household expenditures. In 1999 a special JPS module was included, which covered
202,089 households and 822,607 individuals. This module provides information on
household and individual participation in each of the JPS programmes. The Susenas
survey is fielded in February, so the JPS module only reflects programme coverage
during the initial 6 months of implementation. The first health cards were distributed in
the fourth quarter of 1998. By February 1999, the health card programme covered about
11 percent of the population.
Household characteristics include demographic information such as household
composition and the gender of the head of household. Besides per capita expenditure
quintile and the five factors that determine BKKBN prosperity status, alternative
reflections of socioeconomic status include the main source of income for the household,
education of the head of household and living conditions. Household specific shocks are
partly reflected by employment status of the head of household and a variable indicating
whether daily activities of a household member was disrupted due to illness in the past
month. The Susenas also provides some information on the village characteristics where
the household resides, such as rural/urban and the IDT village classification.10

11
A 1996 village census (Podes), provides pre-intervention data on the availability
of health care facilities in each village (desa) and urban precinct (kelurahan) in Indonesia.
The Podes includes 66,486 of these communities and can be merged with the Susenas
data. The village variables used in the analysis reflect access to health care: the number of
public health facilities located in the village, the number of doctors and midwives that
live in the village (per 1,000 inhabitants), and a variable indicating the village leader's
opinion on accessibility of health facilities in the village.11
Finally, I use data on the geographic targeting criteria and consumption based
poverty. This includes the percentage of BKKBN poor households in districts (December
1997) and in sub-districts (January 1999). The consumption based poverty headcount
ratios are computed by BPS based on the 1996 and 1999 Susenas.12
4. Results and Discussion
Benefit incidence
The health card programme was already of a substantial magnitude in February 1999
with 10.6 percent of Indonesians living in a household with a health card. Health card
recipients show a higher utilisation of outpatient care than non-recipients. The difference
is largest with utilisation of public care. Amongst health card recipients, 15.1 percent
visited an outpatient provider during the 3 months prior to the survey. For non-health
card recipients this is lower, at 12.9 percent. Although health card owners tend to choose
public providers more often, they do not always use their health card. 3.7 out of 10.4
percent of the health card owners report not to use the health card when seeking care at a
public provides.

12
What could explain the weak link between ownership and utilisation? Providers
were not reimbursed based on actual services provided, but on the predicted demand.
Possibly, the providers themselves selected who they deemed in need for subsidised
services and did not always honour the rule that those who could present a health card
should be provided free services. Alternatively, rich household may decide to forgo the
option of free health care, preferring the higher quality private facilities instead of the
public health care centre.
Strauss et al. (2004) show that at some public health clinics not all services were
covered by the health card, but that this can not fully explain the under-usage of health
cards. Qualitative research by Soelaksono et al. (1999) find that at some public facilities,
the time allocated to patients with a health card was limited, and that in remote areas the
lack of access to the nearest public facility was a possible deterrent to use the health card.
They also found indications that patients perceived the care received using a health card
to be of lower quality than services and medicines obtained when not using the health
card. In addition, the public perception was that treatment at the public clinic was less
effective than at private sector.
Health cards are distributed pro-poor, as shown in Table 2. Amongst the poorest
20 percent of the population 18.5 percent had a health card. Incidence of health card
receipt drop as per capita expenditure increases, from 13.7 percent in the second quintile
to 3.7 in the richest quintile. The allocation shares for ownership and utilisation are
presented in columns 3 and 5 of Table 2. The poorest 20 percent of the population own
33.7 percent of the health cards. Still, there is considerable leakage to the more wealthy
households. Considering that about 11 percent of the population received a health card,

13
perfect targeting would imply that all health cards are concentrated with the poorest
quintile. However, the wealthiest 60 percent of the population own about 40 percent of
the health cards.
Utilisation of health cards for outpatient care shows a less pro-poor distribution
than allocation. Conditional on having a health card, the middle quintiles are more likely
to use it. That means that those who received benefits were on average wealthier than
those who received the card. Barriers of access to health care seem higher for the poor.
Even though the non-poor are more likely to use their health card when they have one,
most of the benefits still accrue to the poor. This is because the initial distribution of the
health card is distributed pro-poor. Almost three quarters of the health cards is distributed
in rural areas. But relative to this distribution, the use of the cards is similar between rural
and urban areas.
Geographical targeting and crisis impact
How well did the district targeting criteria reflect regional differences in poverty and
impact of the crisis? Several studies have raised concern about the lack of reliable data
available for geographic targeting (e.g. Ananta and Siregar 1999, Daly and Fane 2002,
Dhanani and Islam 2002, Pritchett et al. 2002). Given the heterogeneous nature of the
crisis, it is likely that criteria for regional targeting misjudged the degree of poverty in the
districts, since only pre-crisis information on regional poverty was available. There are
two reasons for this. First, the crisis has given rise to large relative price changes,
between products (especially food) and across regions (Cameron 1999, Frankenberg et al.
2003, Friedman and Levinsohn 2002). This variation is completely ignored in the

14
targeting process when pre-crisis poverty estimates are applied as allocation rule in 1999.
Second, the effects of the crisis varied strongly between regions and were only weakly
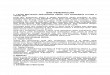
correlated with the initial level of poverty (Sumarto et al. 1998). This heterogeneity of the
crisis impact is shown in Figure 1, which plots 1996 consumption based poverty against
the change from 1996 to 1999. The difference between 1996 and 1999 estimates reflects
the impact of the crisis. It indicates the absolute change in the fraction of people that
moved into or out of poverty during the crisis. In line with Sumarto et al. (1998), there
appears to be no correlation between the initial level of poverty and the impact of the
crisis.
The BKKBN data are collected at more frequent intervals than the consumption
surveys. They can provide fairly up to date information, as far down as the household
level. The problem, however, is that the components of the BKKBN classification are
inflexible measures and inappropriate for capturing the degree of poverty when faced
with severe economic shocks of a crisis.13
Table 3 is illustrative for the difficulty of capturing the effect of the crisis using
pre-crisis data. The table shows the ranking of provinces (from low to high) according to
the 1999 (BPS99) and 1996 (BPS96) poverty headcount of BPS, the BKKBN measure.
The different welfare measures show different levels of poverty. As expected, the
consumption based poverty headcount estimates for 1996 are lower than for 1999.
Evaluating welfare by the basic needs criteria of the BKKBN yields a higher count of
deprived households. In itself this is not surprising. What is important is that the ranking
is different. The ranking following the BKKBN measure differs from both the levels and
changes of poverty, as measured by BPS.

15
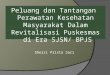
The differences between the welfare measures are further illustrated by a
graphical exposition. Figure 2 and Figure 3 plot the BKKBN targeting rule against the
poverty BPS estimates. The BKKBN prosperity score is strongly positively correlated
with the 1999 poverty headcount, but with a lot of variation around the trend. This is
expected since the BKKBN criteria are not solely based on household consumption.
There is a weakly positive correlation between the change in poverty and the BKKBN
measure for the main body of districts and a greater variation amount the mean. The trend
line is pulled up by a small number of districts that experienced a large increase in
poverty.
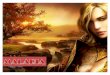
Actual allocation of health cards is less correlated with expenditure based poverty
than the BKKBN criteria are. There seems to be little correlation between BPS poverty
and the allocation of health cards reported in the Susenas data (Figure 4). This indicates a
fuzzy relationship between the BKKBN targeting criteria and actual allocation. This
could be due to delays in the implementation or regional difference in efficiency of the
programme. But if it is, then these irregularities are greater in relatively poor districts.
Community based targeting and health card utilisation
What are the key factors that determine targeting at the community level? Table 4 reports
probit estimates of the determinants for health card allocation as well as utilisation
conditional on ownership, at household level. The table reports marginal effects. The
standard errors have been adjusted for the stratified sampling design of the Susenas
survey.

16
There are significant negative effects of per capita consumption on the probability
of receiving a health card, confirming the pro-poor targeting found in the benefit
incidence analysis. For the use of the health card conditional upon owning one, the results
do not reflect the slightly non-poor pattern found in the benefit incidence. It could be that
observed utilisation differences between quintiles are too small to yield statistically
significant marginal effects in the multivariate analysis. Alternatively, it could be that the
non-poor bias in utilisation is not a direct wealth effect but follows from other
background characteristics, which are correlated with wealth.
Sector of employment affects both allocation and utilisation. The probability of
receiving a health card is lower for households for whom agriculture is the main source
of income, while they are also less likely to use it for outpatient care. This may indicate
that the opportunity costs of time spent at the health clinic or travelling are relatively
higher for farm households.
Supply and access of health care at village level plays an important role in the
targeting process. The number of auxiliary public clinics negatively affects the
probability of receiving a health card. But conditional on ownership the presence of
primary and auxiliary public clinics in the village strongly increases the use of health
cards for outpatient care. Further, utilisation of health cards is higher in villages where
the village leader views health care facilities to be easy or very easy to reach. Overall, the
results suggest that, while remote and less wealthy areas with little access to health care
receive priority in the targeting process, the direct and indirect costs of using the cards are
relatively high. On the other hand, the probability of selection increases as the number of
midwives living in the village increases. In addition, there is also a positive correlation

17
with utilisation. Since it is the medical staff of local clinics that actually distribute the
health cards to households, this might reflect the importance of informal contacts within
the village for awareness of, and participation in, social programmes.
The probit results confirm that health cards have been awarded to households
based on health status. The official allocation rules require health cards to be distributed
to the poor, irrespective of their health status. But the clearly positive effect on the
variable measuring whether any household member has its daily activities disrupted
through illness indicates that often health cards were given based on acute need. For
those who fall ill and do not own a health card, it is still possible to get a health card after
seeking medical care (Soelaksono et al. 1999).
Turning to household composition, the results show that (conditional on per capita
consumption) households with a relatively large share of children and elderly have a
higher probability of receiving and using a health card. Conditional on household
composition, larger households are less likely of receiving and using a health card.
Household headed by females have a significantly higher chance of receiving a health
card. There is a negative correlation between the education of the head of household and
the probability of receiving a health card. But controlling for other household variables,
the characteristics of the head of household seem less important for utilisation.
Women tend to use the cards more for outpatient care than men do. The outpatient
utilisation variable does not reflect the use of health cards for contraception and family
planning services. Nevertheless, it could be that the availability of these services under
the health card has raised awareness of its usefulness amongst women. Utilisation shows
a U-shaped age pattern as the young and the old use the card relatively more.

18
The results confirm that the BKKBN prosperity status variables have influenced
health card allocation. An increase in the district and sub-district BKKBN basic needs
measure increases the probability of receiving a health card. Amongst the individual
BKKBN criteria floor material is a strong predictor for health card ownership. Those with
an earth floor have a higher chance of receiving a health card, but a lower probability of
actually using it for outpatient care. Being able to worship according to faith decreases
the probability of receiving a health card. Interestingly, the individual’s perception of
freedom in practicing personal faith is positively correlation with utilisation of the health
card. Owning different sets of clothing for work and leisure decreases the probability of
using a health card. In contrast to the other BKKBN indicators, having access to modern
care does not yield the expected effect, as it increases both the chance of receiving a
health card and, conditional on ownership, the probability of using it. This suggests the
presence of two countervailing effects: accessibility to public providers increases
exposure to the programme, which outweighs the official targeting criterion.
Simulation results
The simulations are presented in Table 5. The table shows the actual outcome for the
sample used in the multivariate analysis and three counterfactual outcomes: geographic
targeting following BPS and BKKBN indicators, and uniform targeting. The table shows
concentration of health cards and utilisation, to make the performance of different
targeting regimes comparable.14
Not surprising, the actual outcome for the sample corresponds quite closely to a
geographical targeting regime that would follow the BKKBN rule strictly. However, the

19
BPS indicator would increase pro-poor targeting compared to the actual regime, as this
would redistribute 2.7 percent of the health cards to the poorest quintile. This may seem a
small change, but in terms of population it reflects roughly 600,000 people in the poorest
quintile that would move into the programme due to improved geographic targeting.
The uniform targeting regime shows the counterfactual outcome if a districts
share of health cards would be proportional to the relative population size. That is, if
purposive targeting would only occur within the districts. Compared to uniform
geographic targeting, the actual targeting regime increases the share of the poorest
quintile by 5.4 percentage points, from 28.9 to 34.1 percent. Considering that complete
random targeting at all levels would yield coverage of 20 percent per quintile, local
targeting alone increases health card concentration with the poorest by 8.8 percentage
points. Hence, for the poorest quintile the overall gain from decentralised targeting is an
additional 14.2 percent of the health card programme, 38 percent (i.e. 5.4 percentage
point) of which is due to geographic targeting and 62 percent (i.e. 8.8 percentage point) to
local targeting. The BPS targeting rule would increase this even further to a gain 16.9
percent, of which 48 percent (i.e. 8.1 percentage point) would be due to geographic
targeting.
The simulations for health card utilisation show very similar patterns, indicating
that improved targeting of health cards leads to a proportional improvement in targeting
of the benefits from the health card.
The results from the simulation exercise suggest that there is indeed scope for
geographic targeting. Under the BPS targeting rule almost half of the gain from targeting
would be due to geographic targeting. However, the results also show the limits to

20
geographic targeting. Coverage amongst the poorest quintile under the best performing
scenario is still only 37 percent, while perfect targeting would imply 53 percent coverage
(i.e. 10.6 percent / 20 percent). For this difference to be bridged community based
targeting would have to be improved. Moreover, barriers to access seem to be locally
determined and not much affected by geographic targeting.
5. Conclusion
There is clear evidence that the JPS health card programme was pro-poor in the sense that
the poor had a higher probability of receiving a health card and using it to obtain free
health services. However, despite pro-poor targeting, a considerable number of health
cards went to households in the richer quintiles.
The programme was implemented at the remarkable speed: by February 1999
approximately 22 million people (about 11 percent of Indonesians) lived in households
that received a health card. The decentralised programme design may well have
facilitated this swift reaction, by relying on existing administrative and operational
infrastructure within the districts. However, at such short notice there was no reliable data
on the impact of the crisis across districts. Geographic targeting criteria were therefore
based poverty estimates that reflect the actual level of poverty to some extent but do not
capture the impact of the crisis. There appears to be no correlation between the initial
level of poverty and the impact of the crisis.
A notable finding is that some health card owners did not use their health card
when obtaining care from public service providers. The particular design resulted in a
discrepancy between health card ownership and utilisation. Moreover, utilisation of

21
subsidised services is less pro-poor than ownership. Conditional on ownership, the
middle quintiles have a higher propensity to use their health card, suggesting that access
barriers to health care are not fully overcome by a user fee waiver. The main deterrent
seems to be the opportunity costs of seeking health care. The direct and indirect costs of
using the health card are relatively higher in the more remote, and rural villages with little
access to public health care providers. While the more remote areas were targeted
because of the lack of access to health care facilities, it is for the same reason that usage
rates are low.
Micro-simulations show that geographic targeting can contribute considerably to
improving targeting performance. Nevertheless, most of the targeting gains are to be
made at the community level.
In terms of policy implications for future safety nets and crisis responses, the need
for adequate information systems is apparent from this study. While the decentralised
design of the programme seems flexible in a crisis situation, up to date information and
early signalling of crisis effects are crucial. In addition, further research would need to
investigate how local information can best be exploited under decentralised and
community based targeting in signalling crisis related poverty dynamics and local
barriers to access.

22
Endnotes
1 See, for example, Alderman (2001 and 2002). Conning and Kevane (2002)
provide an extensive review of community based targeting.
2 For an account of the economic crisis in Indonesia see, amongst others, Cameron
(1999), Smith et al. (2002) and Frankenberg et al. (2003).
3 Using different data sources, Suryahadi et al. (2003) trace poverty movement
during the crisis and find that the poverty headcount has more than doubled from15.3
percent in February 1997 to 33.2 percent at the height of the crisis, late 1998.
4 Modern health care is here defined as public health care providers – hospitals,
health clinics (Puskesmas), village maternity posts (Polindes) and integrated health posts
(Posyandu) – and private providers – hospitals, doctors, clinics and paramedical services.
Traditional health care is not included.
5 The JPS further included an education, food security, labour creation and micro
credit programmes. Ananta and Siregar (1999) and Daly and Fane (2002) provide a good
overview of all the JPS programmes.
6 An alternative specification would be to include the observed health card coverage
in districts. However, this variable would be endogenous to the outcome variable.
7 Since the utilisation probit (2) is estimated for individuals, so is the first stage
allocation probit that is used for computing the selection term. The variables are the same
as those included in the household level analysis in (1) and the estimation results are very
similar. The results are available upon request.

23
8 Nevertheless, there may be reasons why the BKKBN indicators could still be
correlated with utilisation. The BKKBN indicators determined the amount of JPS
financial compensation to health facilities, and thus health care quality and supply.
Moreover, they might be correlated with local level of welfare (or deprivation), and thus
with health care demand. I therefore estimated equation (2) with the BKKBN variables
(without λ). Their marginal effects were small and statistically non significant. Although
this does not constitute a formal test, it is a strong indication that the exclusion restriction
is justified. The results are available upon request.
9 The errors are computed as ( )[ ])()()(~ 1 LLHu Φ+Φ−Φ⋅Φ= −ε where H and L are
the upper and lower truncation points, respectively. Ф reflects the standard normal cdf
and u is a drawn from a uniform distribution with a value between 0 and 1.
10 IDT refers to the Inpres Desa Tertinggal program, an anti-poverty programme for
economically less developed villages. For this program, each village or urban precinct in
Indonesia has been classified as either developed or less developed.
11 The Podes survey asks village leaders whether the closest public health clinics are
(i) very easy, (ii) easy, (iii) difficult or (iv) very difficult to reach by the majority of the
village population.
12 See BPS (2000) for details.
13 The main criticism in this respect is that the BKKBN measure is based on fixed
assets (type of floor and owning clothes) and non-economic questions regarding religious
practices. Sumarto et al. (2003) place further questions with interregional consistency of
the BKKBN measure as the village staff who collect the BKKBN data receive relatively
little training, and the figures are vulnerable to manipulation by local government

24
officials. Using data from a longitudinal survey in 100 villages, Suryahadi et al. (1999)
show that there is a high degree of mismatch between the BKKBN classification and
expenditure based poverty measures. For example, the BKKBN data classify 49 percent
of the households in the sample as poor. But according to per capita consumption, only
57 percent of these households rank with the poorest 49 percent of the population.
14 Some observations were lost due to a few missing values in the covariates, and
merging the Susenas and Podes data. The simulated programme sizes therefore differ
slightly from the actual observed size. Overall incidence varies between 10.7 and 10.9
percent, slightly above the observed 10.6 percent reported in Table 2. Comparing
coverage results could then be misleading if changes for quintiles are due to change in
programme size instead of redistribution. With the concentration measures the overall
size of the programme is normalised to 100 percent for all counterfactual regimes. The
coverage results are not reported here but are available upon request.

25
References
Alatas V and Pradhan MP. 2003. Geographic Targeting in Indonesia. World Bank,
Jakarta. Unpublished document.
Alderman H. 2001. Multi-Tier Targeting of Social Assistance: The Role of
Intergovernmental Transfers. The World Bank Economic Review 15: 33-53.
Alderman H. 2002. Do Local Officials Know Something We Don't? Decentralization of
Targeted Transfers in Albania. Journal of Public Economics 83: 375-404.
Ananta A and Siregar R. 1999. Social Safety Net Policies in Indonesia: Objectives and
Shortcomings. ASEAN Economic Bulletin 16: 344-359.
Bardhan P and Mookherjee D. 2000. Capture and Governance at Local and National
Levels. American Economic Review 90: 135-139.
Bardhan P and Mookherjee D. 2005. Decentralizing Antipoverty Program Delivery in
Developing Countries. Journal of Public Economics 89: 675-704.
BPS. 2000. Tingkat Kemiskinan Kabupaten. Jakarta. Unpublished document.
Cameron LA. 1999. Survey of Recent Developments. Bulletin of Indonesian Economic
Studies 35: 2-40.
Coady D, Grosh ME, and Hoddinott J. 2004. The Targeting of Transfers in Developing
Countries: Review of Experiences and Lessons. Washington, D.C: World Bank.
Conning J and Kevane M. 2002. Community-Based Targeting Mechanisms for Social
Safety Nets: A Critical Review. World Development 30: 375-394.
Daly A and Fane G. 2002. Anti-Poverty Programs in Indonesia. Bulletin of Indonesian
Economic Studies 38: 309-329.

26
Dhanani S and Islam I. 2002. Poverty, Vulnerability and Social Protection in a Period of
Crisis: The Case of Indonesia. World Development 30: 1211-1231.
Frankenberg E, Thomas D, and Beegle K. 1999. The Real Costs of Indonesia's Economic
Crisis: Preliminary Findings from the Indonesian Family Life Survey. Labor and
Population Program Working Paper 99-04, RAND, Santa Monica.
Frankenberg E, Smith JP, and Thomas D. 2003. Economic Shocks, Wealth, and Welfare.
Journal of Human Resources 38: 280-321.
Friedman J and Levinsohn J. 2002. The Distributional Impact of Indonesia's Financial
Crisis on Household Welfare: A "Rapid Response" Methodology. The World Bank
Economic Review 16: 397-423.
Galasso E and Ravallion M. 2005. Decentralized Targeting of an Antipoverty Program.
Journal of Public Economics 89: 705-727.
Knowles JC, Pernia EM, and Racelis M. 1999. Social Consequences of the Financial
Crisis in Asia. Economic Staff Paper Number 60, Asian Development Bank, Manila.
Knowles JC and Marzolf JR. 2003. Health Financing for the Poor in Indonesia. World
Bank, Washington D.C. Unpublished document.
Lanjouw P, Pradhan MP, Saadah F, Sayed H, and Sparrow R. 2002. Poverty, Education
and Health in Indonesia: Who Benefits from Public Spending? In: Morrisson C (ed).
Education and Health Expenditures, and Development: The cases of Indonesia and
Peru. Paris: Development Centre Studies, OECD Development Centre, pp. 17-78.
Pradhan MP, Saadah F, and Sparrow R. Forthcoming. Did the Health Card Program
Ensure Access to medical Care for The Poor During Indonesia's Economic Crisis?
The World Bank Economic Review.

27
Pritchett L, Sumarto S, and Suryahadi A. 2002. Targeted Programs in an Economic Crisis:
Emperical Findings from the Experience of Indonesia. SMERU working paper,
Jakarta.
Skoufias E, Suryahadi A, and Sumarto S. 2000. Changes in Household Welfare, Poverty
and Inequality during the Crisis. Bulletin of Indonesian Economic Studies 36: 97-
114.
Smith JP, Thomas D, Frankenberg E, Beegle K, and Teruel G. 2002. Wages, employment
and economic shocks: Evidence from Indonesia. Journal of Population Economics
15: 161-193.
Soelaksono B, Budiyati S, Hastuti et al. 1999. The Impact of the Crisis on the People's
Behavior and Perceptions of the Use and Effectiveness of Puskesmas, Posyandu,
and the Role of Midwifes. SMERU, Jakarta. Unpublished document.
Strauss J, Beegle K, Dwiyanto A et al. 2004. Indonesian Living Standards: Before and
After the Financial Crisis. Santa Monica: RAND.
Sumarto S, Wetterberg A, and Pritchett L. 1998. The Social Impact of the Crisis in
Indonesia: Results from a Nationwide Kecamatan Survey. SMERU working paper,
Jakarta.
Sumarto S, Suryahadi A, and Pritchett L. 2003. Safety Net or Safety Ropes? Dynamic
Benefit Incidence of Two Crisis Programs in Indonesia. World Development 31:
1257-1277.
Suryahadi A, Sumarto S and Pritchett L. 2003. The Evolution of Poverty During the
Crisis in Indonesia. Asian Economic Journal 17:221-241.

28
Suryahadi A, Suharso Y, and Sumarto S. 1999. Coverage and Targeting in the Indonesian
Social Safety Net Programs: Evidence from 100 Village Survey. SMERU working
paper, Jakarta.
Waters H, Saadah F, and Pradhan MP. 2003. The Impact of the 1997-98 East Asian
Economic Crisis on Health and Health Care in Indonesia. Health Policy and
Planning 18: 172-181.

29
Tables
Table 1 Targeting process of the JPS health card programme
Targeting phase
Actors
Objectives/decisions
Targeting instrument
Barriers
Phase 1:
CMU, Jakarta
Target districts
- BKKBN 1997
- No crisis information
- Welfare indicator quality
Phase 2:
District committees
Target public health care
providers and households
- Local BKKBN data
- Local knowledge
- Lack of crisis information of in
sub-districts, villages and
individual households
- Elite capture
Phase 3:
Households
Self targeting: utilisation
of health cards
- Self selection
- Needs
- Lack of access
- Perceptions
- Crowding out

30
Table 2 Distribution of health card allocation and utilisation for outpatient care during past three months, 1999
Health card allocation
(amongst Indonesian population)
Health card utilisation
(am
ongst health card recipients)
Incidence (%)
Share (%
) Incidence (%)
Share (%
)
Quintile 1 (poorest)
18.45
33.74
6.51
33.28
Quintile 2
13.71
25.68
6.54
25.43
Quintile 3
10.61
20.06
6.84
20.79
Quintile 4
7.09
13.41
6.78
13.77
Quintile 5 (richest)
3.71
7.10
6.25
6.72
Urban
7.23
26.79
6.65
26.89
Rural
12.82
73.21
6.62
73.11
All
10.62
100.00
6.63
100.00
Number of observations: 822,607.

31
Table 3 provinces ranked by poverty measures according to BPS and BKKBN headcount
Province BKKBN 1997 BPS 1996 BPS 1999 ∆BPS 99-96
% (rank) % (rank) % (rank) % (rank)
Aceh 51.65 (18) 12.72 (8) 14.75 (6) 2.03 (11)
North-Sumatra 27.56 (3) 13.23 (9) 16.74 (8) 3.51 (14)
West-Sumatra 33.89 (7) 9.84 (5) 13.24 (3) 3.40 (13)
Riau 35.97 (10) 12.62 (7) 14.00 (4) 1.38 (5)
Jambi 29.67 (4) 14.84 (11) 26.64 (17) 11.80 (25)
South-Sumatra 41.27 (12) 15.89 (12) 23.53 (14) 7.64 (20)
Bengkulu 43.22 (16) 16.71 (14) 19.79 (12) 3.08 (12)
Lampung 60.72 (22) 25.59 (21) 29.11 (20) 3.52 (15)
Jakarta 17.32 (2) 2.35 (1) 3.99 (1) 1.64 (9)
West-Java 33.25 (6) 11.06 (6) 19.78 (11) 8.72 (23)
Central-Java 54.30 (19) 21.61 (17) 28.46 (18) 6.85 (18)
Yogyakarta 34.57 (9) 18.43 (16) 26.11 (15) 7.68 (21)
East-Java 42.24 (14) 22.13 (18) 29.48 (21) 7.35 (19)
Bali 0.00 (1) 7.81 (2) 8.53 (2) 0.72 (3)
NTB 62.49 (23) 31.97 (23) 32.95 (23) 0.98 (4)
NTT 82.68 (26) 38.89 (24) 46.73 (25) 7.84 (22)
West-Kalimantan 46.82 (17) 24.21 (20) 26.18 (16) 1.97 (10)
Central-Kalimantan 42.71 (15) 13.50 (10) 15.05 (7) 1.55 (6)
South-Kalimantan 34.03 (8) 8.53 (3) 14.37 (5) 5.84 (16)
East-Kalimantan 32.14 (5) 9.73 (4) 20.16 (13) 10.43 (24)
North-Sulawesi 39.90 (11) 17.94 (15) 18.19 (9) 0.25 (1)
Central-Sulawesi 56.84 (20) 22.30 (19) 28.68 (19) 6.38 (17)
South-Sulawesi 41.53 (13) 16.71 (13) 18.32 (10) 1.61 (8)
South-East-Sulawesi 64.09 (24) 29.23 (22) 29.51 (22) 0.28 (2)
Maluku 60.21 (21) 44.56 (26) 46.14 (24) 1.58 (7)
Irian-Jaya 70.40 (25) 42.28 (25) 54.75 (26) 12.47 (26)
Indonesia 41.98 17.70 23.43 5.73

32
Table 4 Within-district targeting of JPS health cards to households, and determinants of
utilisation for outpatient treatment (probit marginal effects)
(1) (2)
Health card
allocation
Health card
utilisation
Unit of analysis Household Individual
Female 0.0172
[0.0017]**
Age -0.0021
[0.0002]**
Age squared 0.00004
[0.0000]**
Female head of household 0.0197 -0.0020
[0.0029]** [0.0045]
Education head of household
(reference = none / primary not completed)
Primary -0.0075 0.0078
[0.0019]** [0.0034]*
Junior secondary -0.0241 0.0002
[0.0023]** [0.0056]
Senior secondary -0.0407 0.0077
[0.0023]** [0.0079]
Higher -0.0474 -0.0031
[0.0035]** [0.0148]
Head of household unemployed 0.0152 -0.0055
[0.0086]+ [0.0112]
Member of household ill last month 0.0119 0.0821
[0.0019]** [0.0040]**
Log household size -0.0082 -0.0424
[0.0022]** [0.0047]**

33
(Table 4 continued)
(1) (2)
Household composition
(reference = share of males age 18-60)
Share of males age < 6 0.0313 0.0397
[0.0074]** [0.0141]**
Share of females age < 6 0.0269 0.0282
[0.0078]** [0.0145]+
Share of males age 6-12 0.0014 0.0401
[0.0063] [0.0122]**
Share of females age 6-12 0.0116 0.0213
[0.0065]+ [0.0124]+
Share of males age 13-17 0.0119 0.0020
[0.0069]+ [0.0143]
Share of females age 13-17 -0.0062 -0.0115
[0.0071] [0.0156]
Share of females age 18-60 0.0018 0.0044
[0.0057] [0.0130]
Share of males age > 60 0.0150 -0.0120
[0.0059]* [0.0125]
Share of females age > 60 0.0102 -0.0362
[0.0059]+ [0.0139]**
Agriculture main source of income -0.0090 -0.0056
[0.0021]** [0.0034]+
Per capita expenditure quintile
(reference = quintile 1, poorest)
Quintile 2 -0.0150 0.0009
[0.0024]** [0.0043]
Quintile 3 -0.0255 -0.0028
[0.0026]** [0.0050]

34
(Table 4 continued)
(1) (2)
Quintile 4 -0.0418 -0.0058
[0.0027]** [0.0066]
Quintile 5, richest -0.0657 -0.0112
[0.0029]** [0.0092]
BKKBN criteria
Can worship according to faith -0.0191 0.0140
[0.0041]** [0.0045]**
Eat basic food twice a day -0.0059 0.0108
[0.0079] [0.0086]
Different clothing school/work/leisure -0.0023 -0.0215
[0.0052] [0.0083]**
Floor made of material other than earth -0.0548 0.0123
[0.0033]** [0.0062]*
Access to modern medical care 0.0291 0.0337
[0.0025]** [0.0039]**
Living conditions
House made out of bamboo 0.0419 0.0031
[0.0036]** [0.0052]
Access to clean drinking water -0.0077 0.0106
[0.0029]** [0.0053]*
Closed sewer -0.0229 -0.0024
[0.0025]** [0.0047]
Access to electricity 0.0183 -0.0149
[0.0029]** [0.0056]**
Village characteristics
Rural area -0.0154 -0.0084
[0.0039]** [0.0061]
IDT village -0.0061 0.0083
[0.0035]+ [0.0046]+

35
(Table 4 continued)
(1) (2)
Nr. of primary health clinics -0.0058 0.0111
[0.0031]+ [0.0049]*
Nr. of auxiliary health clinics -0.0093 0.0159
[0.0026]** [0.0039]**
Nr. of doctors per 1,000 inhabitants 0.0067 0.0060
[0.0045] [0.0054]
Nr. of midwifes per 1,000 inhabitants 0.0066 0.0225
[0.0037]+ [0.0071]**
Health facilities easy to reach 0.0080 0.0139
[0.0062] [0.0070]*
Majority of inter village traffic by land 0.0212 0.0053
[0.0070]** [0.0116]
BKKBN poverty rate in sub-district 0.0982
[0.0075]**
BKKBN poverty rate in district 0.0178
[0.0098]+
BPS poverty rate 1999 -0.0008 0.0007
[0.0001]** [0.0002]**
Selection term -0.0070
[0.0166]
Observations 185,608 76,684
Pseudo R-squared 0.10 0.09
Robust standard errors in brackets
+ significant at 10%; * significant at 5%; ** significant at 1%

36
Table 5 Health card allocation and outpatient utilisation simulations under different geographic targeting regimes (percentage shares)
Health card allocation
(% share of total programme)
Health card outpatient utilisation
(% share of total utilisation)
Targeting regime
Current
BPS
BKKBN
Uniform
Current
BPS
BKKBN
Uniform
Quintile 1 (poorest)
34.21
36.90
33.43
28.84
33.43
37.11
33.94
28.11
Quintile 2
25.71
24.95
24.98
23.87
25.81
25.07
25.14
23.45
Quintile 3
19.76
18.91
19.50
20.51
19.94
17.97
18.45
20.61
Quintile 4
13.38
13.07
14.39
16.38
13.96
13.23
14.80
16.88
Quintile 5 (richest)
6.93
6.17
7.70
10.4
6.85
6.63
7.67
10.94
Urban
27.06
25.41
26.01
36.41
25.74
23.33
23.26
35.56
Rural
72.94
74.59
73.99
63.59
74.26
76.67
76.74
64.44
All
100.00
100.00
100.00
100.00
100.00
100.00
100.00
100.00

37
Figures
Lowess smoother, bandwidth = .8
Change BPS 1996-1999
BPS poverty rate 19960 .7089
-.0494
.2759
Figure 1 Correlation between initial poverty in 1996 and crisis impact on BPS poverty
headcount (locally weighted regression with 0.8 bandwidth)

38
Lowess smoother, bandwidth = .8BKKBN headcount
BPS poverty rate 1999.0109 .8009
0
.9655
Figure 2 Correlation between BKKBN headcount December 1997 and BPS 1999 poverty
rate (locally weighted regression with 0.8 bandwidth)

39
Lowess smoother, bandwidth = .8BKKBN headcount
Change BPS 1996-1999-.0494 .2759
0
.9655
Figure 3 Correlation between BKKBN headcount December 1997 and crisis impact on
BPS poverty rate (locally weighted regression with 0.8 bandwidth)

40
Lowess smoother, bandwidth = .8Health card coverage
BPS poverty rate 1999.0109 .8009
0
.517606
Figure 4 Correlation between health card coverage and BPS 1999 poverty rate (locally
weighted regression with 0.8 bandwidth)

i
Supplemental appendix
Table A.1. Within-district targeting of JPS health cards to households, and determinants of utilisation for outpatient treatment (probit
marginal effects)
(1)
(2)
(3)
(4)
(5)
Health card
Health card
(selection probit)
Utilisation
(selection term)
Utilisation
(no selection term)
Utilisation
(no exclusions)
Unit of analysis
Household
Individual
Individual
Individual
Individual
Fem
ale
0.0172
0.0172
0.0172
[0.0017]**
[0.0017]**
[0.0017]**
Age
-0.0021
-0.0021
-0.0021
[0.0002]**
[0.0002]**
[0.0002]**
Age squared
0.0000
0.0000
0.0000
[0.0000]**
[0.0000]**
[0.0000]**
Fem
ale head of household
0.0197
0.0185
-0.0020
-0.0015
-0.0015
[0.0029]**
[0.0031]**
[0.0045]
[0.0043]
[0.0043]
Education head of household
(reference = none / primary not completed)
Primary
-0.0075
-0.0052
0.0078
0.0077
0.0076
[0.0019]**
[0.0021]*
[0.0034]*
[0.0033]*
[0.0033]*
Junior secondary
-0.0241
-0.0219
0.0002
-0.0007
-0.0006
[0.0023]**
[0.0026]**
[0.0056]
[0.0050]
[0.0050]
Senior secondary
-0.0407
-0.0400
0.0077
0.0057
0.0056
[0.0023]**
[0.0024]**
[0.0079]
[0.0060]
[0.0060]
Higher
-0.0474
-0.0503
-0.0031
-0.0058
-0.0059
[0.0035]**
[0.0033]**
[0.0148]
[0.0125]
[0.0124]
Head of household unem
ployed
0.0152
0.0152
-0.0055
-0.0051
-0.0048
[0.0086]+
[0.0094]
[0.0112]
[0.0112]
[0.0112]
Mem
ber of household ill last month
0.0119
0.0125
0.0821
0.0826
0.0825
[0.0019]**
[0.0021]**
[0.0040]**
[0.0039]**
[0.0039]**
Log household size
-0.0082
-0.0129
-0.0424
-0.0429
-0.0429
[0.0022]**
[0.0026]**
[0.0047]**
[0.0044]**
[0.0044]**

ii
(Table A.1. continued)
(1)
(2)
(3)
(4)
(5)
Household composition
(reference = share of males age 18-60)
Share of males age < 6
0.0313
0.0298
0.0397
0.0408
0.0407
[0.0074]**
[0.0082]**
[0.0141]**
[0.0140]**
[0.0140]**
Share of females age < 6
0.0269
0.0234
0.0282
0.0291
0.0290
[0.0078]**
[0.0085]**
[0.0145]+
[0.0145]*
[0.0145]*
Share of males age 6-12
0.0014
-0.0008
0.0401
0.0400
0.0397
[0.0063]
[0.0070]
[0.0122]**
[0.0122]**
[0.0122]**
Share of females age 6-12
0.0116
0.0100
0.0213
0.0218
0.0215
[0.0065]+
[0.0071]
[0.0124]+
[0.0124]+
[0.0124]+
Share of males age 13-17
0.0119
0.0194
0.0020
0.0028
0.0026
[0.0069]+
[0.0077]*
[0.0143]
[0.0142]
[0.0142]
Share of females age 13-17
-0.0062
-0.0015
-0.0115
-0.0117
-0.0117
[0.0071]
[0.0080]
[0.0156]
[0.0156]
[0.0156]
Share of females age 18-60
0.0018
-0.0057
0.0044
0.0043
0.0044
[0.0057]
[0.0066]
[0.0130]
[0.0129]
[0.0129]
Share of males age > 60
0.0150
0.0056
-0.0120
-0.0119
-0.0117
[0.0059]*
[0.0071]
[0.0125]
[0.0125]
[0.0125]
Share of females age > 60
0.0102
0.0129
-0.0362
-0.0357
-0.0354
[0.0059]+
[0.0070]+
[0.0139]**
[0.0140]*
[0.0140]*
Agriculture main source of income
-0.0090
-0.0094
-0.0056
-0.0059
-0.0060
[0.0021]**
[0.0022]**
[0.0034]+
[0.0033]+
[0.0033]+
Per capita expenditure quintile
(reference = quintile 1, poorest)
Quintile 2
-0.0150
-0.0162
0.0009
0.0002
0.0001
[0.0024]**
[0.0025]**
[0.0043]
[0.0039]
[0.0039]
Quintile 3
-0.0255
-0.0284
-0.0028
-0.0039
-0.0041
[0.0026]**
[0.0027]**
[0.0050]
[0.0042]
[0.0042]
Quintile 4
-0.0418
-0.0454
-0.0058
-0.0077
-0.0079
[0.0027]**
[0.0028]**
[0.0066]
[0.0047]
[0.0047]+
Quintile 5, richest
-0.0657
-0.0663
-0.0112
-0.0141
-0.0145
[0.0029]**
[0.0028]**
[0.0092]
[0.0058]*
[0.0058]*

iii
(Table A.1. continued)
(1)
(2)
(3)
(4)
(5)
BKKBN criteria
Can worship according to faith
-0.0191
-0.0192
0.0140
0.0135
0.0134
[0.0041]**
[0.0044]**
[0.0045]**
[0.0043]**
[0.0043]**
Eat basic food twice a day
-0.0059
-0.0123
0.0108
0.0103
0.0102
[0.0079]
[0.0087]
[0.0086]
[0.0085]
[0.0086]
Different clothing school/work/leisure
-0.0023
-0.0019
-0.0215
-0.0216
-0.0217
[0.0052]
[0.0057]
[0.0083]**
[0.0083]**
[0.0083]**
Floor made of material other than earth
-0.0548
-0.0556
0.0123
0.0100
0.0108
[0.0033]**
[0.0036]**
[0.0062]*
[0.0037]**
[0.0038]**
Access to modern medical care
0.0291
0.0330
0.0337
0.0346
0.0346
[0.0025]**
[0.0028]**
[0.0039]**
[0.0034]**
[0.0034]**
Living conditions
House made out of bam
boo
0.0419
0.0415
0.0031
0.0045
0.0047
[0.0036]**
[0.0039]**
[0.0052]
[0.0043]
[0.0043]
Access to clean drinking water
-0.0077
-0.0071
0.0106
0.0104
0.0103
[0.0029]**
[0.0030]*
[0.0053]*
[0.0052]*
[0.0051]*
Closed sew
er
-0.0229
-0.0242
-0.0024
-0.0034
-0.0031
[0.0025]**
[0.0026]**
[0.0047]
[0.0042]
[0.0042]
Access to electricity
0.0183
0.0176
-0.0149
-0.0140
-0.0139
[0.0029]**
[0.0031]**
[0.0056]**
[0.0049]**
[0.0050]**
Village characteristics
Rural area
-0.0154
-0.0181
-0.0084
-0.0088
-0.0096
[0.0039]**
[0.0041]**
[0.0061]
[0.0060]
[0.0061]
IDT village
-0.0061
-0.0076
0.0083
0.0081
0.0077
[0.0035]+
[0.0037]*
[0.0046]+
[0.0045]+
[0.0045]+
Nr. of primary health clinics
-0.0058
-0.0055
0.0111
0.0108
0.0109
[0.0031]+
[0.0033]+
[0.0049]*
[0.0048]*
[0.0048]*
Nr. of auxiliary health clinics
-0.0093
-0.0081
0.0159
0.0156
0.0158
[0.0026]**
[0.0027]**
[0.0039]**
[0.0038]**
[0.0038]**
Nr. of doctors per 1,000 inhabitants
0.0067
0.0085
0.0060
0.0064
0.0065
[0.0045]
[0.0047]+
[0.0054]
[0.0053]
[0.0053]

iv
(Table A.1. continued)
(1)
(2)
(3)
(4)
(5)
Nr. of midwifes per 1,000 inhabitants
0.0066
0.0080
0.0225
0.0229
0.0230
[0.0037]+
[0.0040]*
[0.0071]**
[0.0074]**
[0.0073]**
Health facilities easy to reach
0.0080
0.0062
0.0139
0.0140
0.0141
[0.0062]
[0.0066]
[0.0070]*
[0.0070]*
[0.0070]*
Majority of inter village traffic by land
0.0212
0.0232
0.0053
0.0066
0.0063
[0.0070]**
[0.0073]**
[0.0116]
[0.0110]
[0.0111]
BKKBN poverty rate in sub-district
0.0982
0.0984
-0.0000
[0.0075]**
[0.0079]**
[0.0101]
BKKBN poverty rate in district
0.0178
0.0071
0.0122
[0.0098]+
[0.0101]
[0.0127]
BPS poverty rate 1999
-0.0008
-0.0007
0.0007
0.0007
0.0006
[0.0001]**
[0.0002]**
[0.0002]**
[0.0002]**
[0.0002]*
Selection term
-0.0070
[0.0166]
Observations
185,608
777,289
76,684
76,684
76,684
Pseudo R-squared
0.10
0.10
0.09
0.09
0.09
Robust standard errors in brackets; + significant at 10%; * significant at 5%; ** significant at 1%.

v
Table A.2. Health card allocation simulations under different geographic targeting regimes
Incidence
(% coverage am
ongst Indonesian population)
Share
(% share of total programme)
Targeting regime
Current
BPS
BKKBN
Uniform
Current
BPS
BKKBN
Uniform
Quintile 1 (poorest)
18.67
20.23
18.57
16.04
34.21
36.90
33.43
28.84
Quintile 2
13.69
13.34
13.53
12.94
25.71
24.95
24.98
23.87
Quintile 3
10.49
10.08
10.53
11.09
19.76
18.91
19.50
20.51
Quintile 4
7.14
7.00
7.81
8.90
13.38
13.07
14.39
16.38
Quintile 5 (richest)
3.69
3.30
4.17
5.65
6.93
6.17
7.70
10.4
Urban
7.29
6.87
7.12
9.98
27.06
25.41
26.01
36.41
Rural
12.95
13.30
13.37
11.50
72.94
74.59
73.99
63.59
All
10.70
10.75
10.89
10.90
100.00
100.00
100.00
100.00
Table A.3. Health card outpatient utilisation simulations under different geographic targeting regimes
Incidence
(% utilisation amongst health card recipients)
Share
(% share of total utilisation)
Targeting regime
Current
BPS
BKKBN
Uniform
Current
BPS
BKKBN
Uniform
Quintile 1 (poorest)
6.43
7.48
7.27
6.94
33.43
37.11
33.94
28.11
Quintile 2
6.57
7.46
7.19
6.92
25.81
25.07
25.14
23.45
Quintile 3
6.58
7.02
6.72
7.04
19.94
17.97
18.45
20.61
Quintile 4
6.80
7.47
7.28
7.21
13.96
13.23
14.80
16.88
Quintile 5 (richest)
6.27
7.83
6.97
7.26
6.85
6.63
7.67
10.94
Urban
6.35
7.11
6.57
6.98
25.74
23.33
23.26
35.56
Rural
6.60
7.50
7.31
7.07
74.26
76.67
76.74
64.44
All
6.53
7.41
7.12
7.04
100.00
100.00
100.00
100.00